ODYSSEY 2012
14
asl/english
bimodal
bilingual program
During the past few years, the teachers and staff at Kendall Demonstration
Elementary School (KDES) have reviewed research to identify factors that
positively impact language development for deaf and hard of hearing
children, and established language and communication practices to reflect
what we have learned. Based on the research, which details the advantages of
early accessible visual language (Baker, 2011) and documents the variations
in spoken language outcomes regardless of the use of hearing aids and
cochlear implants (Yoshinaga-Itano, 2006), we have examined how an
American Sign Language (ASL)/English bilingual program can be designed
to benefit children with a wide range of characteristics—from children who
have minimal access to spoken language through hearing aids and cochlear
implants to those who benefit greatly from these technologies. We refer to
this as an ASL/English bimodal bilingual approach, which includes
establishment of language foundations and access to learning through two
modalities, e.g., auditory and visual, and two languages, e.g., ASL and
English (Berent, 2004; Bishop, 2006; Emmorey, Bornstein, & Thompson,
2005). Through our experience in establishing a bimodal bilingual program
at KDES and through our consultations with schools and programs
throughout the United States, we are finding that with purposeful planning
this multisensory approach can be implemented to effectively support the
overall development of deaf and hard of hearing children.
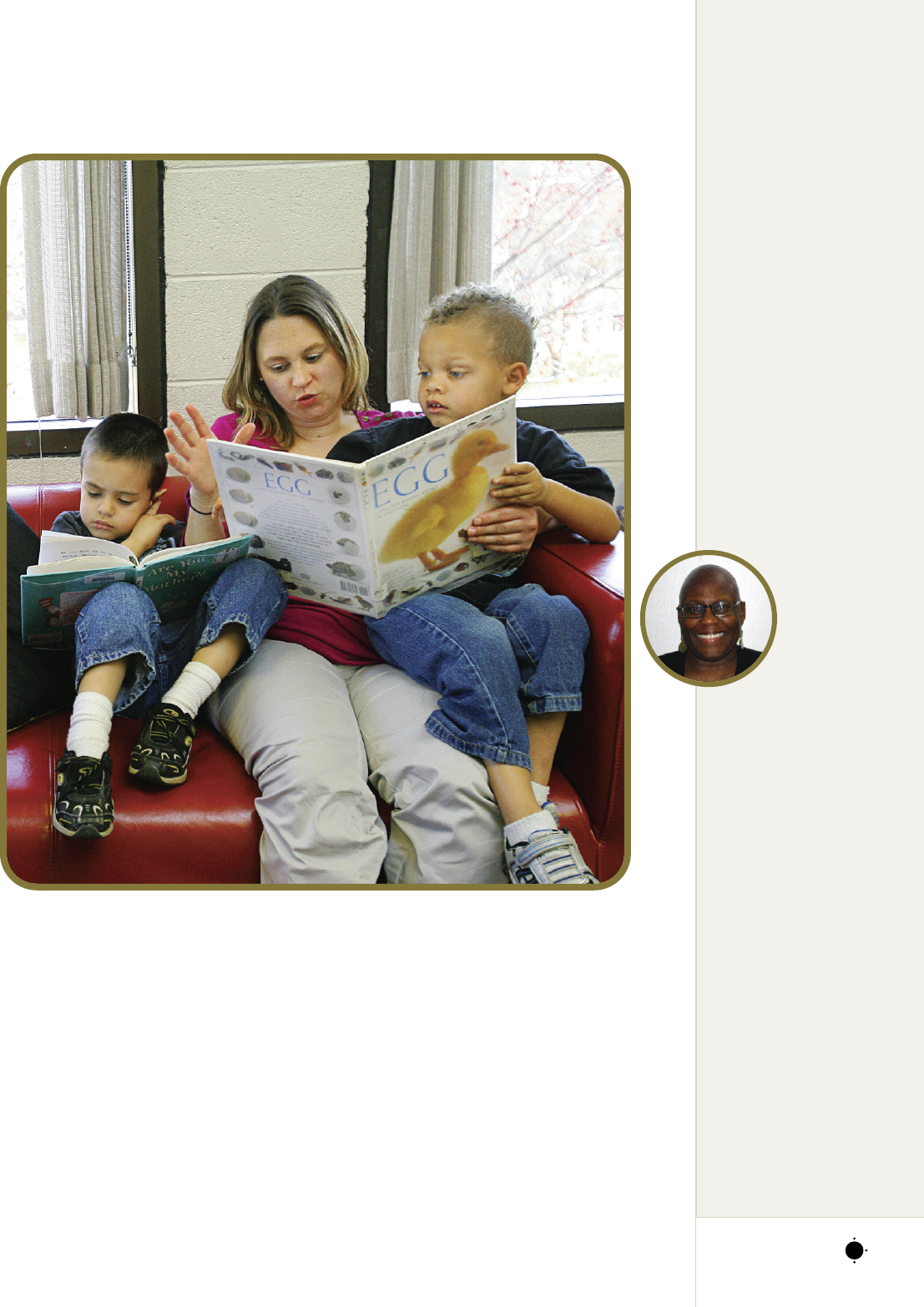
Photos by John T. Consoli
Debra Berlin
Nussbaum, MA, is
coordinator of the
C
ochlear Implant
Education
Center (CIEC)
at the Laurent
Clerc National
Deaf Education
Center at Gallaudet
University. She earned her
master’s degree in
audiology from George
Washington University
and has worked at the
Clerc Center since 1977,
first as a pediatric
audiologist and since
2000 as coordinator of the
CIEC. She has
spearheaded national
efforts to address how
spoken language and
signed language can be
included in the education
of children who are deaf or
hard of hearing. She has
also developed numerous
resource materials and
professional training
workshops; she speaks
nationally and
internationally on this
topic.
Susanne Scott, MS,
is a cochlear
implant/bilingual
specialist at the Laurent
Clerc National Deaf
Education Center at
Gallaudet University.
With a degree in
audiology from
Gallaudet
University, she has
worked at Gallaudet
University and the
Clerc Center since 1980,
first as an educational
audiologist and then as a
By Debra Berlin Nussbaum, Susanne Scott, and Laurene E. Simms
T H E “ W H Y ” A N D “ H O W ” O F A N
2012 ODYSSEY
15
clinical educator in the
Department of Hearing,
S
peech and Language
Sciences. In 2003 Scott
joined the Cochlear
Implant Education
Center, where she provides
expertise in cochlear
implants and ASL/English
bilingual programming
for professionals, students,
and families at the Clerc
Center and throughout
the nation.
Laurene E. Simms,
PhD, is a professor in the
Department of Education
at Gallaudet University.
After graduating from the
Indiana School for the
Deaf, she earned her
bachelor’s and
master’s degrees
in elementary
education from
the University of
Nebraska, Lincoln
and Western
Maryland College (now
McDaniel College),
respectively. She received
her doctorate in language,
reading, and culture from
the University of Arizona.
An acknowledged expert
in ASL/English
instruction, Simms has
implemented
bilingual/multicultural
educational environments
for diverse deaf and hard
of hearing children.
The authors welcome
questions and comments
about this article at
Debra.Nussbaum@gallaudet
.edu, Susanne.Scott@
gallaudet.edu,and Laurene.
respectively.
Research Support for a
Bimodal Bilingual Approach
For children who are deaf or hard of hearing
and cannot fully access linguistic meaning
through audition, the use of ASL has been
documented to promote linguistic,
communication, cognitive, academic, and
literacy development as well as social-
emotional growth and identity formation
(Baker, 2011; Cummins, 2006; Grosjean,
2008; Morford & Mayberry, 2000; Yoshinaga-
Itano, 2006). Evidence also indicates that there
is a risk of language delay if an accessible
language is not used as early as possible, even
for children who have some level of access to
spoken language through a hearing aid or
cochlear implant (Mayberry, 1993, 2007;
Mayberry & Eichen, 1991; Mayberry, Lock, &
Kazmi, 2002; Schick, de Villiers, de Villiers, &
Hoffmeister, 2007). The brain has the capacity
to acquire both a visual and a spoken language
without detriment to the development of
either (Kovelman et al., 2009; Petitto et al.,
2001; Petitto & Kovelman, 2003), and there is
no documented evidence demonstrating that
ASL inhibits the development of spoken
English (Marschark & Hauser, 2012). An
ASL/English bimodal bilingual approach has
the characteristics to be advantageous to
language acquisition and learning. The child
ODYSSEY 2012
acquires language through his or her
intact visual modality while developing
spoken English to the maximum extent
possible. This approach is “additive”; it
builds upon a child’s strength in one
language while adding a second
language (Baker, 2006).
Evolution of an ASL/English
Bimodal Bilingual Approach
Use of a bilingual approach, which
addresses the acquisition and use of both
ASL and English, emerged during the
1980s. Referred to as the
bilingual/bicultural (“Bi-Bi”) approach,
this model reflects the importance of
including the language accessibility
needs as well as the cultural and identity
needs of deaf learners. ASL is
recommended as a first language and
major medium of communication, with
English addressed primarily through
reading and writing (Nover, 1995;
Nover, Christensen, & Cheng, 1998;
Reynolds & Titus, 1991; Vernon &
Daigle, 1994). A framework later
emerged emphasizing the development
of ASL and English, including the
development of spoken English
commensurate with a child’s potential
for oral/aural development (Garate,
2011; Nover, Christensen, & Cheng,
1998). As growing numbers of children
demonstrate the potential to access
language and learning through audition
via improved digital hearing aids and
cochlear implants, increasing numbers of
educational programs have moved
towards designing and implementing an
ASL/English bilingual program that is
also bimodal.
Planning and Implementing a
Bimodal Bilingual Program
The key to designing and implementing
a successful bimodal bilingual program
is planning (Knight & Swanwick, 2002;
Nover, 2004). Regardless of whether
this approach is implemented in schools
for deaf students or in public or private
school settings, three components are
integral: school-wide planning,
individualized planning, and teacher
implementation planning.
School-wide planning is the first
step. It is critical that the school
administration define and share with
the school community the school’s
philosophy and guiding principles
surrounding the development and use of
ASL and spoken and written English
(Muhlke, 2000). (See sidebar on
“Guiding Principles for Bilingual
Planning at the Clerc Center.”) An
effective planning process should
include teachers, staff, and families. A
strategic plan to identify resources for
ongoing professional development and
family education and a system to
monitor program effectiveness is also an
important part of the process. From our
experience, it has been beneficial to have
a designated person(s) responsible for
oversight of the school-wide planning
and implementation process.
Individualized planning, the
development of a language and
communication plan for each child, is
the second key component. The
individualized plan should include the
child’s profile (based on informal and
formal assessment) and his or her
functioning in both ASL and spoken
English (Easterbrooks & Baker, 2002); it
should also include recommendations for
individual goals to facilitate
development and use of each language
and a system to monitor each child’s
progress. (See sidebar on “Planning to
Implementation: A Look at Tommy’s
Day.”) The plan can be tailored to reflect
the needs of children who:
•
Are from families that are culturally
deaf
•
Have additional disabilities
•
Are in the early language
development stages
•
Are beyond the early language
development years
•
Use and benefit from hearing aids or
cochlear implants
•
Do not use or benefit from hearing
aids or cochlear implants
As part of the individualized planning
process, the Clerc Center has developed
and is utilizing a Language and
Communication Profile. This profile
includes a variety of tools we have
chosen to document a child’s language
and communication characteristics and
reflects a child’s use of language in
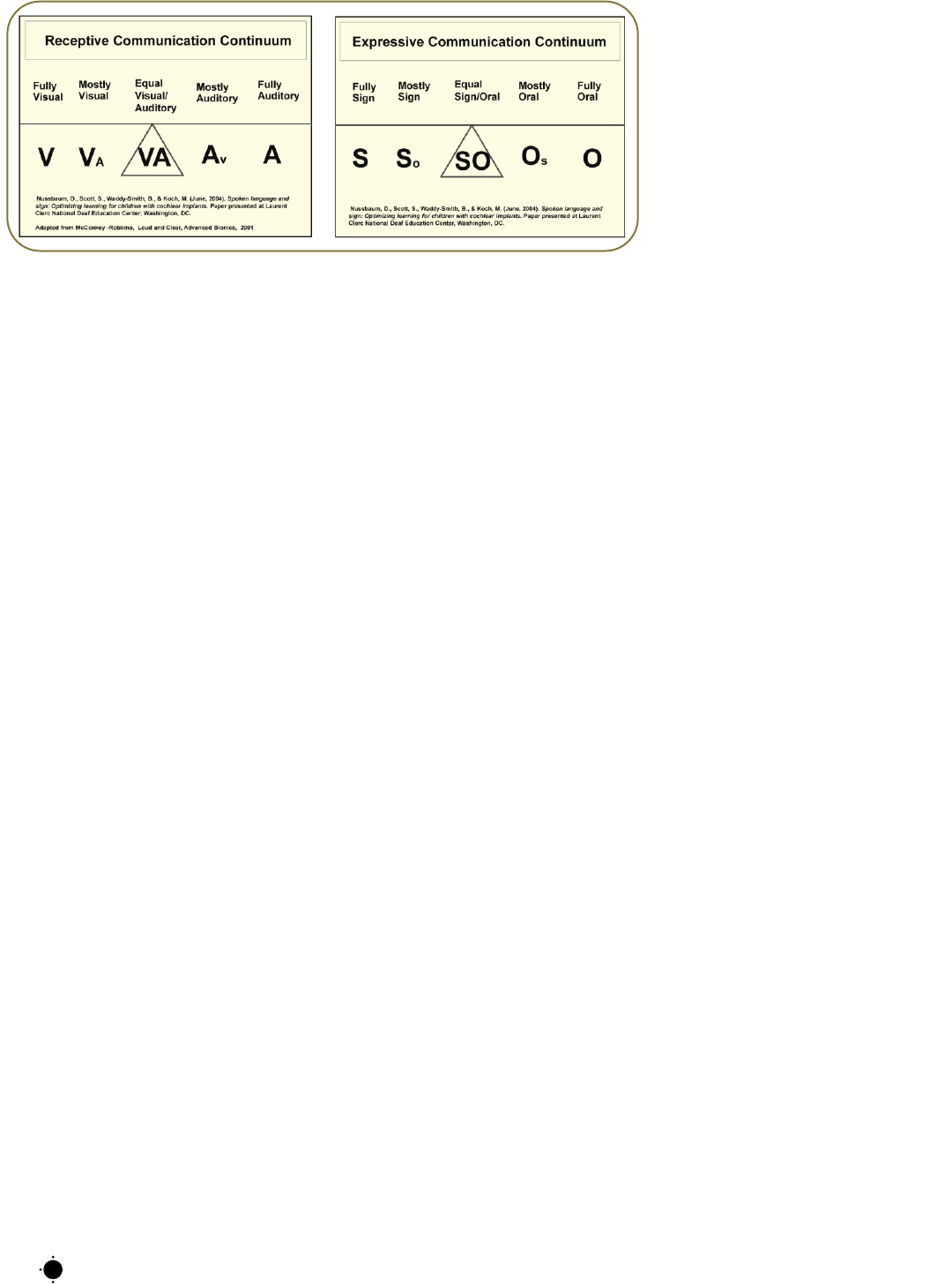
varied environments. One part of the
profile includes a description of the
child’s functioning along two
continuums (see Figure 1): a receptive
continuum for how a child accesses
language—visually, aurally, or
somewhere in between; and an
expressive continuum for how a child
expresses language—signed, spoken, or
somewhere in between (Nussbaum &
Scott, 2011). As placements within
these continuums are incorporated into
developing an individualized plan, it is
important to emphasize the following:
•
How a child functions on either
continuum may differ in varied
settings (e.g., social settings, large
classrooms, small groups, 1-1
situations, noisy environments,
complicated fast-paced language
situations). Language use decisions
should reflect a child’s needs in each
of these settings.
•
How a child functions in
understanding ASL and spoken
language may differ from how he or
she functions in generating either
language. For example, a child may
be able to readily understand
spoken language or ASL; however,
16
Figure 1: Continuums used at the Clerc
Center to document receptive and expressive
communication as part of the individualized
language planning process
2012 ODYSSEY
he or she may not demonstrate the
ability to express him- or herself at
t
he same level through either
language.
Regardless of which assessment tools
or documentation system a school uses,
the individualized plan should be
developed by a team of professionals
working with the child, including his or
her teacher, speech language specialist,
audiologist, ASL specialist, etc.
Gathering family input related to a
child’s use of language and
communication in the home, as well as
family goals related to the development
and use of each language, is an integral
part of developing the individualized
plan. If professionals or specialists
outside of the school are involved with
the child, they should also be included
in the planning process.
Teacher implementation planning,
the third step in the process, should be
coordinated by the child’s teacher and
include feedback from other support
professionals and the family. It should
reflect language use for each activity
throughout the day, identify who will
use each language to facilitate the
activity, and determine how to group
children with similar language and
communication characteristics and goals
(Swanwick & Tsverik, 2007; Garate,
2011). Part of the plan can also include
recommendations for families regarding
how and when to use each language in
the home.
At KDES, two of the practices used
for implementing individual language
and communication plans are language
immersion and classroom integration:
•
Language immersion is the targeted
use of either ASL or spoken English
for a dedicated period of time
guided by the activity, the person
facilitating the activity, and/or the
place of the activity. This practice
provides an opportunity for children
to acquire and experience a distinct
separation between ASL and spoken
English (Baker, 2006). Language
use during immersion activities is
purposeful, meaningful, and
developmentally appropriate,
allowing language acquisition to
proceed in a way that is natural and
incidental. For example, in a
preschool classroom, an art activity
may be facilitated through spoken
English in one area of the classroom
and through ASL in another area of
the classroom. Other immersion
opportunities we have implemented
include lunchtime, facilitated in
ASL or spoken English at separate
tables, and read-aloud stories,
facilitated either in ASL or spoken
English. For children in
kindergarten through eighth grade,
ASL immersion occurs via a
dedicated ASL language arts class.
•
Classroom integration is the use of ASL
and English within a lesson, activity,
or interaction to facilitate
development of skills in ASL and
spoken English. Classroom
integration provides structured
opportunities to address each child’s
individual language and
communication goals. For example,
while working on curriculum
content in class, one group of
children may be with a speech-
language specialist and/or teacher to
develop spoken English skills and
17
Guiding Principles for Bilingual
Planning at the Clerc Center
B
ELIEF STATEMENT ON LANGUAGE:
We believe that early access to and acquisition of linguistic proficiency
i
n ASL and English are integral to a deaf or hard of hearing
student’s overall development.
GUIDING PRINCIPLES:
•
Early, unrestricted access to language is critical to linguistic and cognitive
development.
•
Bilingual development of ASL and English is critical to deaf and hard of
hearing children establishing early communication with their parents,
developing their cognitive abilities, acquiring world knowledge,
communicating fully with the surrounding world, and acculturating into the
world of the hearing and of the deaf. (Grosjean, 2008)
•
Accessible and consistent ASL and English adult and peer language models are
integral to fostering language acquisition and learning.
•
Use of visual language, including ASL and a rich English print environment,
is critical for access, acquisition, and development of both languages.
•
Spoken English is valued, encouraged, and incorporated specific to an
individual child’s characteristics and goals.
•
Family involvement and competence in facilitating early accessible language
and communication is critical to a child’s cognitive and social-emotional
development.
a
nother group of children may be
with an ASL specialist and/or teacher
to develop ASL skills. Skill
development in each language can
also be integrated through use of
learning centers (Garate, 2011).
During both immersion and
integration opportunities, bilingual
strategies can be used to link ASL and
spoken English, including:
•
Sandwiching—Saying it-signing it-
s
aying it, or signing it-saying it-
signing it
•
Chaining—Signing it-fingerspelling
it-using picture support-saying it
While research exists to support the
bimodal bilingual approach, research has
not yet formally documented student
outcomes. However, at KDES we have
witnessed positive outcomes in both ASL
and spoken English for our students. We
have also experienced the benefit to our
s
chool community, families, and students
of using a language planning process that
is reflective of research and driven by
individualized student assessment. While
a bimodal bilingual program requires
dedicated planning and coordination, we
are optimistic that its potential to
positively impact the development of
linguistic competence of deaf and hard of
hearing children will offer strong
motivation for educational settings to
implement this approach.
ODYSSEY 201218
Planning to Implementation: A Look at Tommy’s Day
B
ACKGROUND:
Tommy is 5 years old and enrolled in an ASL/English bilingual kindergarten class. He is one of 12 students with varying
degrees of hearing levels, varied use and benefit from listening technologies (e.g., hearing aids, cochlear implants), and varied skills in ASL and
spoken English. He has a teacher who is hearing and bilingual in ASL and English as well as an instructional aide who is a native ASL user.
Tommy has a bilateral, moderate to severe sensorineural hearing loss that was identified via newborn hearing screening. Tommy’s
parents are hearing and he has a 2-year-old sister who is also hearing. He started receiving early intervention services at 4 months of age.
At that time he was fitted with digital hearing aids that he uses consistently, and his parents started learning and using ASL. The
primary language of the home is spoken English; however, the family also uses ASL. Based on the results of formal and informal
assessments, Tommy’s language and communication functioning is as follows:
•
ASL: Tommy understands simple, familiar information when language is context embedded and predictable. He demonstrates the
emerging potential to understand and use ASL for increasingly complex new information in one-on-one or small group settings.
His signing is generally understood by family members, teachers, and peers.
•
SPOKEN ENGLISH: Tommy receives significant benefit from his hearing aids
and is able to understand and use spoken English for complex new
information in a variety of settings. He has few articulation errors, and his
speech is generally understood by family members, teachers, and peers.
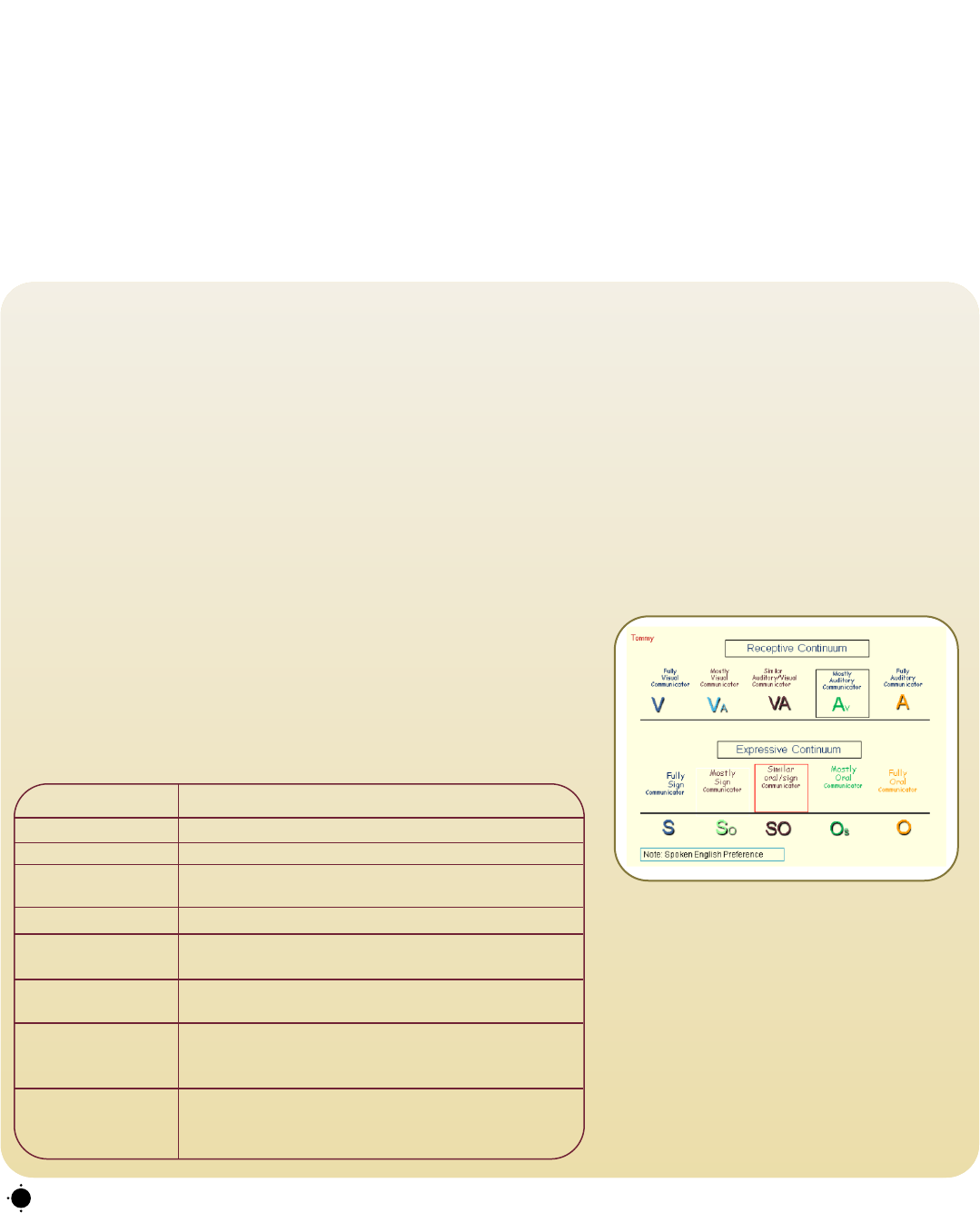
Communication Continuum:
Tommy’s primary language for communication in
most situations is spoken English; however, he is
comfortable using ASL with his peers and for
specific class activities. On the receptive
continuum Tommy is rated “Av,” indicating that
he primarily accesses information through
listening but benefits from visual clarification
through signs in noisy situations or when content
is unfamiliar. Expressively he is rated “SO,”
suggesting that he has equal ability to use spoken
language and ASL.
Below: A description of Tommy’s individualized plan to address how and when to use ASL
and spoken English.
ACTIVITY IMPLEMENTATION PLAN
Arrival/Breakfast Daily hearing aid check
Morning Meeting ASL used for full class
Language Arts Spoken English used to facilitate activities; Tommy grouped
with peers having similar access and skills for spoken English
Math ASL used for full class
Lunch Spoken English used at lunch table; Tommy grouped with
peers having similar access and skills for spoken English
ASL Language Arts ASL immersion*
*ASL taught as a content class
Social Studies/Science ASL integration*: 2x a week
Spoken English integration*: 2x a week
*Skill development in each language using classroom content
Additional Supports Spoken language habilitation services: 2x a week for 30
minutes. Family ASL class once a week
Development of a family plan for language use in the home
References
B
aker, C. (2006). Foundations of bilingual education and bilingualism
(4th ed.). Clevedon, England: Multilingual Matters.
Baker, S. (2011). Advantages of early visual language. Available from
the Visual Language & Visual Learning website,
http://vl2.gallaudet.edu/assets/section7/document104.pdf
Berent, G. P. (2004). Sign language-spoken language bilingualism:
Code mixing and mode mixing by ASL-English bilinguals. In W. C.
Ritchie & T. K. Bhatia (Eds.), The handbook of bilingualism (pp. 312-
335). San Diego, CA: Academic Press.
Bishop, M. (2006). Bimodal bilingualism in hearing, native users of
American Sign Language. Unpublished dissertation, Gallaudet
University, Washington, D.C.
Cummins, J. (2006). The relationship between American Sign Language
proficiency and English academic development: A review of the research.
Unpublished paper for the Ontario Association of the Deaf, Toronto,
Ontario, Canada.
Easterbrooks, S., & Baker, S. (2002). Language learning in children who
are deaf and hard of hearing: Multiple pathways. Boston: Allyn and
Bacon.
Emmorey, K., Bornstein, H. B., & Thompson, R. (2005). Bimodal
bilingualism: Code-blending between spoken English and American
Sign Language. In J. Cohen, K. T. McAlister, K. Rolstad, & J.
MacSwan (Eds.), ISB4: Proceedings of the 4th international symposium on
bilingualism (pp. 663-673). Somerville, MA: Cascadilla Press.
Garate, M. (2011). Educating children with cochlear implants in an
ASL/English bilingual classroom. In R. Paludneviciene & I. Leigh
(Eds.), Cochlear implants evolving perspectives (pp. 206-228).
Washington, DC: Gallaudet University Press.
Grosjean, F. (2008). Studying bilinguals. New York: Oxford University
Press.
Knight, P., & Swanwick, R. (2002). Working with deaf pupils: Sign
bilingual policy into practice. London: David Fulton.
Kovelman, I., Shalinsky, M. H., White, K. S., Schmitt, S. N.,
Berens, M. S., Paymer, N., et al. (2009). Dual language use in sign-
speech bimodal bilinguals: fNIRS brain-imaging evidence. Brain &
Language, 109, 112-123. doi: 10.1016/j.bandl.2008.09.008
Marschark, M., & Hauser, P. (2012). How deaf children learn: What
parents and teachers need to know. New York: Oxford University Press.
Mayberry, R. I. (1993). First-language acquisition after childhood
differs from second-language acquisition: The case of American Sign
Language. Journal of Speech & Hearing Research, 36(6), 1258-1270.
Mayberry, R. I. (2007). When timing is everything: Age of first-
language acquisition effects on second-language learning. Applied
Psycholinguistics, 28(3), 537-549. doi: 10.1017/S0142716407070294
Mayberry, R. I., & Eichen, E. B. (1991). The long-lasting advantage
of learning sign language in childhood: Another look at the critical
period for language acquisition. Journal of Memory and Language,
30(4), 486-512. doi: 10.1016/0749-596X(91)90018-F
M
ayberry, R. I., Lock, E., & Kazmi, H. (2002). Linguistic ability and
early language exposure. Nature, 417(6884), 38.
doi:10.1038/417038a
Morford, J. P., & Mayberry, R. I. (2000). A reexamination of “early
exposure” and its implications for language acquisition by eye. In C.
C
hamberlain, J. Morford, & R. Mayberry (Eds.), Language acquisition
by eye (pp. 111-127). Mahwah, NJ: Lawrence Erlbaum.
Muhlke, M. (2000, Winter). The right to language and linguistic
development: Deafness from a human rights perspective. Virginia
Journal of International Law, 40, 705-760.
Nover, S. (1995). Politics and language: American Sign Language
and English in deaf education. In C. Lucas (Ed.), Sociolinguistics in deaf
communities (pp. 109-163). Washington, DC: Gallaudet University
Press.
Nover, S. M. (2004). A theoretical framework for language planning in
ASL/English bilingual education. Manuscript in preparation.
Nover, S. M., Christensen, K. M., & Cheng, L. L. (1998).
Development of ASL and English competence for learners who are
deaf. Topics in Language Disorders, 18(4), 61-72.
Nussbaum, D., & Scott, S. (2011). The Cochlear Implant Education
Center: Perspectives on effective educational practices. In R.
Paludneviciene & I. Leigh (Eds.), Cochlear implants evolving perspectives
(pp.175-205). Washington, DC: Gallaudet University Press.
Petitto, L. A., Katerelos, M., Levy, B. G., Gauna, K., Tetreault, K., &
Ferraro, V. (2001). Bilingual signed and spoken language acquisition
from birth: Implications for the mechanisms underlying early
bilingual language acquisition. Journal of Child Language, 28, 453-
496.
Petitto, L. A., & Kovelman, I. (2003). The bilingual paradox: How
signing-speaking bilingual children help us resolve bilingual issues
and teach us about the brain’s mechanisms underlying all language
acquisition. Learning Languages, 8, 5-18.
Reynolds, D., & Titus, A. (1991). Bilingual/bicultural education:
Constructing a model for change. Paper presented at the 55th Biennium
Meeting of the Convention of American Instructors of the Deaf, New
Orleans, Louisiana.
Schick, B., de Villiers, J., de Villiers, P., & Hoffmeister, R. (2007).
Language and theory of mind: A study of deaf children. Child
Development, 78(2), 376-396.
Swanwick, R., & Tsverik, I. (2007). The role of sign language for
deaf children with cochlear implants: Good practice in sign bilingual
settings. Deafness and Education International, 9(4), 214-231.
Vernon, M., & Daigle, B. (1994). Bilingual and bicultural education.
In M. Garretson (Ed.), Deaf American monograph, 44 (pp. 121-126).
Silver Spring, MD: National Association of the Deaf.
Yoshinaga-Itano, C. (2006). Early identification, communication
modality, and the development of speech and spoken language skills:
Patterns and considerations. In P. E. Spencer & M. Marschark (Eds.),
Advances in the spoken language development of deaf and hard-of-hearing
children (pp. 298-327). New York: Oxford University Press.
2012 ODYSSEY
19
