
© 2016 American Dental Association All Rights Reserved. March 2016
The Per-Patient Cost of Dental Care, 2013:
A Look Under the Hood
Authors: Thomas Wall, M.A., M.B.A.; Albert Guay, D.M.D.
Introduction
Recent studies have shown that cost is the most significant barrier to receiving dental
services.
1
,
2
Studies have also reported that cost barriers to dental care are considerably
higher than for other types of health care services.
3
According to a recent study of non-
elderly adults with health insurance, dental care ranked number one among health care
services that people are skimping on because of cost.
4
This may seem surprising considering that in 2013, dental expenditures accounted for 4.5
percent of total health care spending, down from 8.5 percent in 1960.
5
According to another
study, average per-patient dental expenditures were $666 in 2011, an amount that would not
appear to qualify as a “budget buster” for most dental patients.
6
In this brief, we focus on the cost of dental care measured in terms of annual per-patient
dental expenditures. We look at expenditures for services provided by general practice (GP)
dentists and dental specialists. We also consider dental expenditures in the context of other
health care services, including the percentage of expenditures paid for out of pocket.
Key Messages
Average annual per-patient dental expenditures in the U.S. were $685 in 2013.
Average expenditures for patients in the 90th percentile were $1,624. Expenditures at
this level and above could represent a financial burden to dental patients.
Contributing to this burden are out-of-pocket expenditures which, as a percentage of the
total expenditure, are higher for dental services compared to other sectors of the health
care system.
Patients with high dental expenditures represent a relatively small percentage of the U.S.
population, and the services they receive are not usually required annually.
Research Brief
The Health Policy Institute (HPI)
is a thought leader and trusted
source for policy knowledge on
critical issues affecting the U.S.
dental care system. HPI strives
to generate, synthesize, and
disseminate innovative research
for policy makers, oral health
advocates, and dental care
providers.
Who We Are
HPI’s interdisciplinary team of
health economists, statisticians,
and analysts has extensive
expertise in health systems
policy research. HPI staff
routinely collaborates with
researchers in academia and
policy think tanks.
Contact Us
Contact the Health Policy
Institute for more information on
products and services at
call 312.440.2928.
2
Research Brief
Results
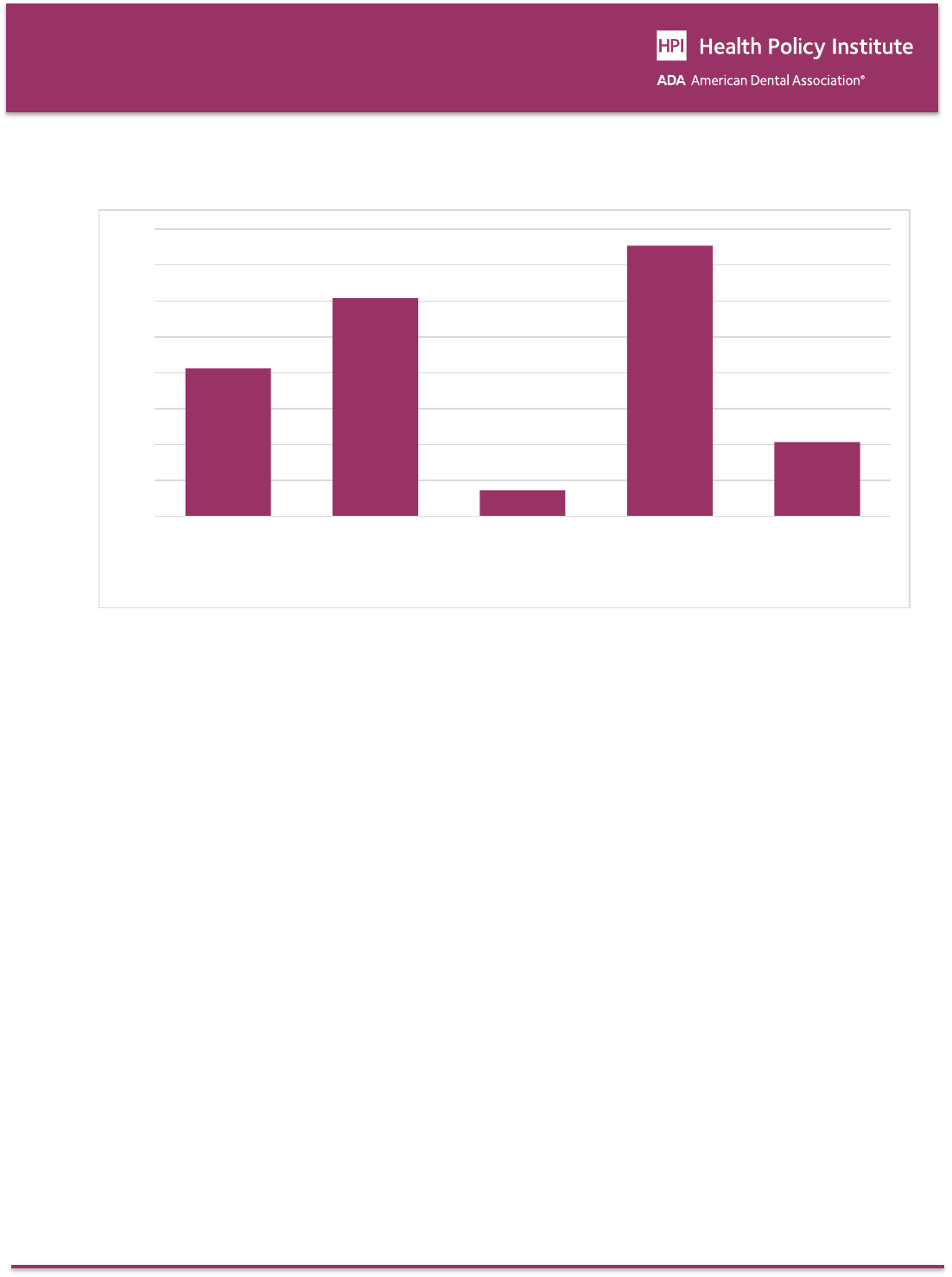
According to the Medical Expenditure Panel Survey
(MEPS), average annual dental expenditures among
those with a visit were $685 in 2013 (Figure 1). Among
those with a visit to a GP dentist, average expenditures
were $514. Among those with a visit to a dental
specialist, average dental expenditures were $1,755.
As an example of dental services provided by
specialists, average dental expenditures for services
provided by orthodontists were $1,440.
Table 1 shows the percentile distribution for annual
dental expenditures (i.e., all dentists) in 2013. The
lowest 10th percentile of dental patients reported
expenditures of $74 or less, while those in the 90th
percentile reported expenditures of $1,624. Patients at
the 50th percentile, or median, reported expenditures
of $254. Note that the mean ($685) is much higher
than the median ($254) because the distribution of
dental expenditures is positively skewed. Patients
falling into the 90th percentile and above represented
13.4 million persons, or 4.2 percent of the U.S.
population, in 2013.
Table 2 shows total health care spending in 2013,
broken down by type of service. As shown in Figure 2,
mean dental spending per person with an expense was
$707.
7
However, as shown in Figure 3, the percentage
out of pocket was highest for dental (45.1 percent).
The percentage out of pocket was lowest for hospital
inpatients (3.2 percent), but due to very high per-
patient expenditures ($16,943), the amount out of
pocket was $544 (Figure 4). Finally, it is worth noting
that the percentage of the population reporting an
expense for hospital inpatient services (7.3 percent)
was much lower than the percentage with an expense
for dental services (41.2 percent). See Figure 5.
Discussion
We found that average per-patient dental costs were
$685 in 2013 and median (i.e., 50th percentile)
expenditures were $254. Expenditures for patients in
the 90th percentile were $1,624. Patients in the 90th
percentile and above represented 13.4 million persons,
or 4.2 percent of the U.S. population, in 2013.
Relatively high dental expenditures, like those in the
90th percentile or above, are likely to represent
services provided by dental specialists or high cost
restorative procedures performed by GP dentists (e.g.,
crowns, implants). Expenditures of this amount could
represent a financial burden even for those with private
dental insurance, and those without coverage are
required to pay the entire cost out of pocket. On the
other hand, high cost dental procedures are not usually
required annually. For example, most orthodontic
treatments can be completed in 18 to 24 months
without need for subsequent comprehensive treatment.
Contributing to this financial burden are higher out-of-
pocket expenditures as a percentage of total
expenditures for dental care compared to other health
care services. This is due, in part, to the relatively high
percentage of the U.S. population with no dental
benefits. For example, in employer-based insurance, a
smaller share of workers have access to dental
coverage through work than have access to health
coverage through work; 45 percent of workers in
private industry were offered dental benefits in 2012
compared with 70 percent who were offered health
benefits.
8
Also, those with private dental insurance are
subject to annual caps and copayments.
9
Dental
benefits are typically capped at $1,000 or $1,500 each
year, according to the National Association of Dental
Plans.
10
Regular office visits for cleanings and X-rays
are generally covered at 100 percent, while fillings and
other basic procedures are covered at 80 percent.

3
Research Brief
Plans typically pay just half of the cost of major
procedures such as crowns and inlays.
As mentioned in the introduction, recent studies have
shown that cost is the most significant barrier to
receiving dental services.
1,2
Although the percentage
of the U.S. population reporting cost barriers to dental
care declined each year from 2010 to 2013, cost
barriers for dental care remain significantly higher than
for other segments of the health care system.
3
However, we found that mean out-of-pocket
expenditures for hospital inpatient services were
considerably higher than mean out-of-pocket dental
expenditures.
Studies of the demand for health care services have
found that the demand for hospital care is among the
least price-responsive while the demand for dental
care is among the most price-responsive.
11
The
patterns of demand correspond to intuition about
“medical necessity” and urgency. This tendency of
patients to place a lower value on dental services than
other health care services may make them more
sensitive to out-of-pocket expenditures for dental
services and more likely to see the cost as a barrier to
care. Because of dental care’s greater sensitivity to
cost (elasticity), the imposition of out-of-pocket patient
costs for dental care can be employed by payers to
manage their financial risks by discouraging the
utilization of care.
12
On the other hand, for half of all dental patients, annual
costs were $254 or less, and those with private dental
insurance paid even less out of pocket. This reflects
improvements in the oral health of the U.S.
population
13
and the shift in the dental services mix
from relatively high cost restorative services to lower
cost diagnostic and preventive services.
14
In 2004,
approximately 73 percent of dental procedures were
either diagnostic (42.5 percent) or preventive (30.4
percent).
15
We have introduced “cost” into the discussion because
the out-of-pocket costs that patients pay for their care
are, in reality, the “price” patients must contend with.
This is regardless of the price providers charge for their
services because of the partial insulation from the true
price providers receive by the various subsidies
delivered by third party payers. The costs to patients
must include opportunity and acquisition costs, such as
transportation, child care, time lost from work, etc. In
other words, a price of zero would still leave costs to
patients when personal considerations are factored in.
On the surface, it appears to be incongruous that oral
health care consumes the smallest portion of health
care spending but dental patients pay the greatest
share of the costs for care out of pocket. The impact of
out-of-pocket spending on the amount of all health
spending is small; however, the impact on seeking
care by individual patients can be significant.
Meaningful reduction of the financial barriers to oral
health care must include moderating out-of-pocket
costs for patients and consideration of opportunity and
acquisition costs to patients beyond the price for
services.
4
Research Brief
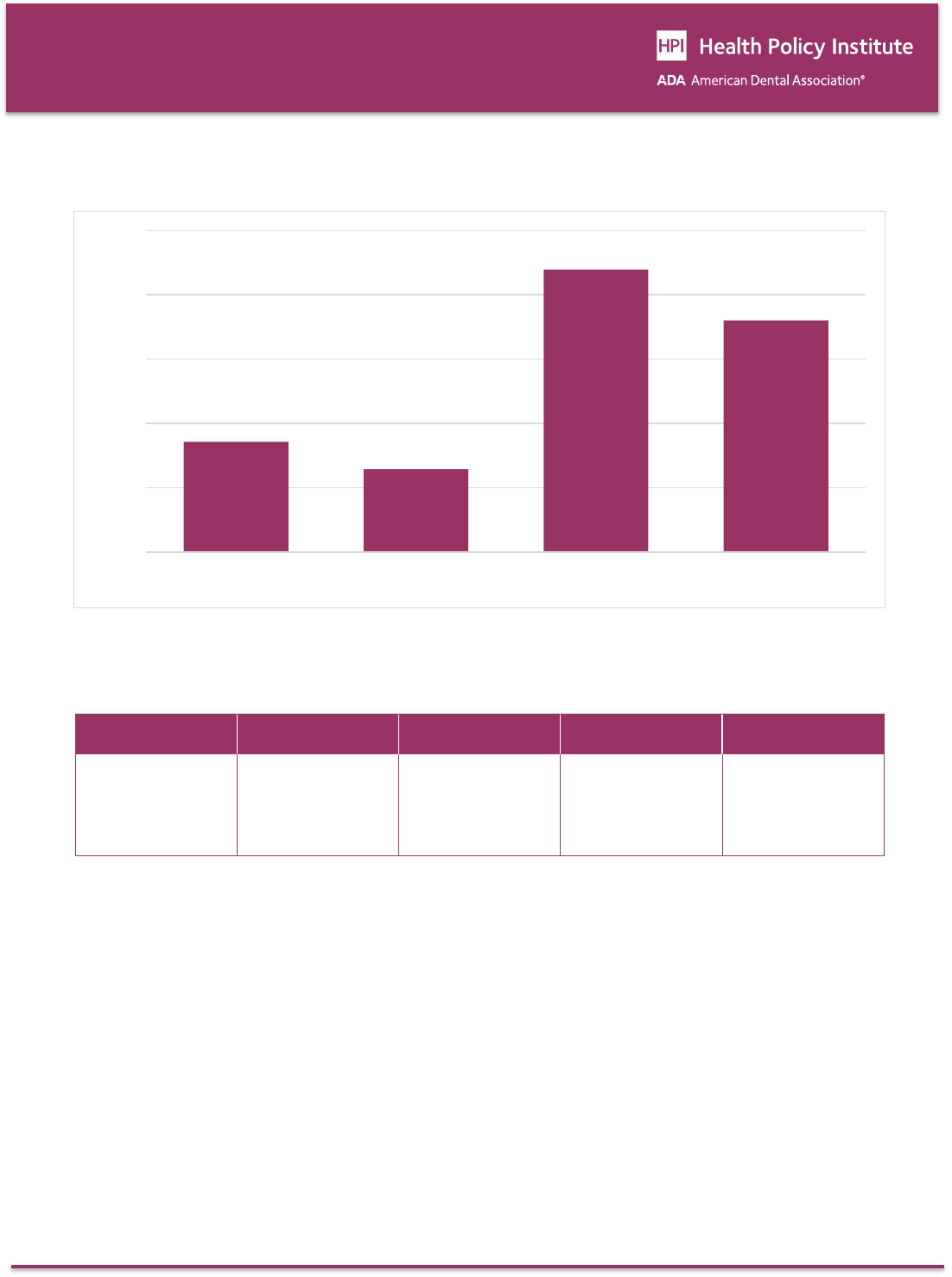
Figure 1: Average Annual Expenditures Among Those with a Visit by Visit Type, 2013
Source: 2013 Medical Expenditure Panel Survey.
Table 1: Annual Expenditures for Dental Services Provided by All Dentists, 2013
10th percentile
25th percentile
50th percentile
75th percentile
90th percentile
$74
$127
$254
$595
$1,624
Source: 2013 Medical Expenditure Panel Survey.
$685
$514
$1,755
$1,440
$0
$400
$800
$1,200
$1,600
$2,000
All dental services Services provided by GP
dentists
Services provided by all
dental specialists
Services provided by
orthodontists
5
Research Brief
Table 2: Health Care Spending by Type of Service, 2013
Mean
(per person
with an
expense)
Percentage
with an
expense
Percentage
out of pocket
Mean
out of pocket
Total
out of pocket
(billions)
Percentage
of total out of
pocket
Total
expenditures
(billions)
Percentage
of total
expenditures
Dental
$706.73
41.2%
45.1%
$318.85
$41.4
21.5%
$91.8
6.6%
Prescription
Drugs
$1,606.63
60.7%
16.5%
$264.84
$50.7
26.3%
$307.8
22.0%
Hospital
Inpatient
$16,942.66
7.3%
3.2%
$544.18
$12.6
6.5%
$390.9
27.9%
Ambulatory
Services
$2,231.93
75.3%
12.7%
$283.39
$67.4
34.9%
$530.6
37.9%
Home Health
Care and
Other Medical
Services and
Equipment
$1,213.51
20.7%
26.3%
$318.50
$20.9
10.8%
$79.4
5.7%
Total Health
Care
$5,255.95
84.4%
13.8%
$724.07
$192.9
100.0%
$1,400.5
100.0%
Source: 2013 Medical Expenditure Panel Survey. Note: Expenditures include total direct payments from all sources to hospitals, physicians, home
health providers (agency and independent providers), dental providers, other types of health care providers (e.g., physical therapists, chiropractors,
optometrists, etc.), and pharmacies for services reported by respondents in the MEPS. Expenditures for hospital-based services include those for
both facility and separately billed physician services. Estimates are for the U.S. civilian non-institutionalized population.
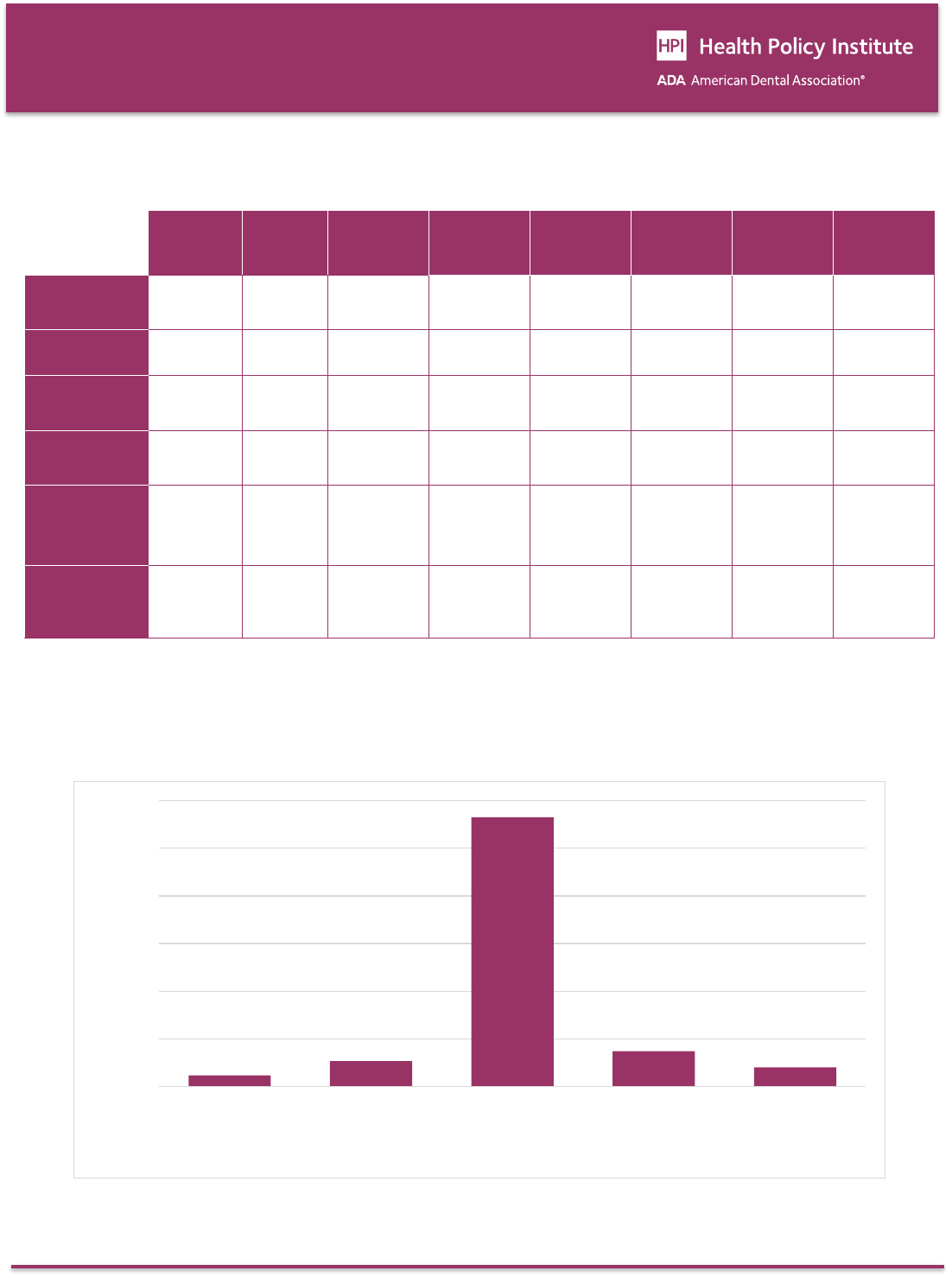
Figure 2: Average Annual Expenditures Per Person With an Expense, 2013
Source: 2013 Medical Expenditure Panel Survey.
$707
$1,607
$16,943
$2,232
$1,214
$0
$3,000
$6,000
$9,000
$12,000
$15,000
$18,000
Dental Prescription Drugs Hospital Inpatient Ambulatory
Services
Home Health Care
and Other Medical
Services and
Equipment
6
Research Brief
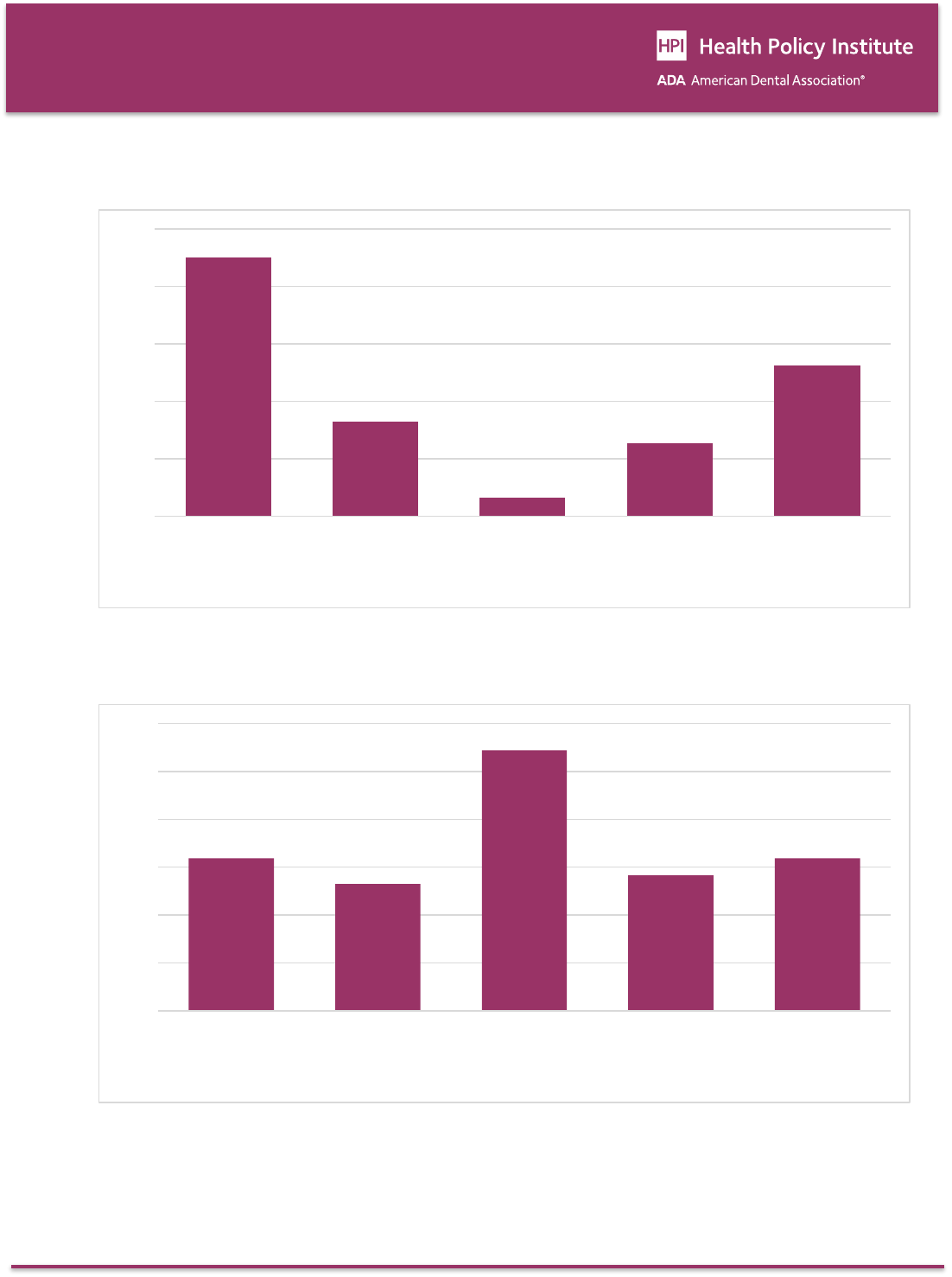
Figure 3: Percentage of Annual Expenditure Paid for Out of Pocket, 2013
Source: 2013 Medical Expenditure Panel Survey.
Figure 4: Average Out-of-Pocket Expenditure, 2013
Source: 2013 Medical Expenditure Panel Survey.
45.1%
16.5%
3.2%
12.7%
26.3%
0%
10%
20%
30%
40%
50%
Dental Prescription Drugs Hospital Inpatient Ambulatory Services Home Health Care
and Other Medical
Services and
Equipment
$319
$265
$544
$283
$319
$0
$100
$200
$300
$400
$500
$600
Dental Prescription Drugs Hospital Inpatient Ambulatory Services Home Health Care
and Other Medical
Services and
Equipment
7
Research Brief
Figure 5: Percentage of the Population with an Expense, 2013
Source: 2013 Medical Expenditure Panel Survey.
Data & Methods
We analyzed data from the Medical Expenditure Panel
Survey (MEPS) that is managed by the Agency for
Healthcare Research and Quality (AHRQ). We focused
on the year 2013, the most recent year for which data
are available (data for 2013 were released in
September 2015). The MEPS provides nationally
representative estimates of health care use,
expenditures, sources of payment, and health
insurance coverage for the U.S. civilian non-
institutionalized population. Studies have documented
differences between the MEPS and National Health
Expenditure Accounts (NHEA) regarding health care
expenditure estimates.
16
We present annual dental expenditure estimates for all
dental services, dental services provided by general
practice (GP) dentists, and dental services provided by
dental specialists. Dental specialists include the
following categories in the MEPS: (1) dental surgeon,
(2) orthodontist, (3) endodontist, (4) periodontist and
(5) other dental specialist.
We also examine expenditures for dental care in the
context of other categories of health care expenditures
included in the MEPS, including prescription drugs,
hospital inpatient services, ambulatory services
(includes hospital out-patient visits, office-based
medical provider visits, and hospital ED visits), and
home health care and other medical services and
equipment. We include per-patient and total
expenditures as well as out-of-pocket expenditures as
a percentage of the total.
41.2%
60.7%
7.3%
75.3%
20.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Dental Prescription Drugs Hospital Inpatient Ambulatory Services Home Health Care
and Other Medical
Services and
Equipment

9
Research Brief
References
1
Wall T, Nasseh K, Vujicic M. Most important barriers to dental care are financial, not supply related. Health Policy
Institute Research Brief. American Dental Association. October 2014. Available at:
http://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1014_2.ashx. Accessed February
26, 2016.
2
Yarbrough C, Nasseh K, Vujicic M. Why adults forgo dental care: evidence from a new national survey. Health Policy
Institute Research Brief. American Dental Association. November 2014. Available at:
http://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1114_1.ashx. Accessed February
26, 2016.
3
Nasseh K, Wall T, Vujicic M. Cost barriers to dental care continue to decline, particularly among young adults and the
poor. Health Policy Institute Research Brief. American Dental Association. October 2015. Available at:
http://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1015_2.ashx. Accessed February
26, 2016.
4
Urban Institute. Health Policy Center. QuickTake: the forgotten health care need: gaps in dental care for insured
adults remain under ACA. September 2015. Available at: http://hrms.urban.org/quicktakes/Gaps-in-Dental-Care-for-
Insured-Adults-Remain-under-ACA.html.
5
Centers for Medicare & Medicaid Services. National Health Expenditure Data. National Health Expenditures by type of
service and source of funds. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-
Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html.
6
Wall T, Nasseh K, Vujicic M. U.S. dental spending remains flat through 2012. Health Policy Institute Research Brief.
American Dental Association. January 2014. Available at:
http://www.ada.org/sections/professionalResources/pdfs/HPRCBrief_0114_1.pdf. Accessed February 26, 2016.
7
Mean per-patient dental expenditures in Table 2 are based on those patients in the MEPS with an expense. Mean per-
patient dental expenditures in Figure 1 are somewhat lower and include some patients in the MEPS with no
expenditures.
8
Wiatrowski WJ. 2013. Employment-based health benefits in small and large private establishments. Beyond the
Numbers. 2013;2(8). Washington, DC: Bureau of Labor Statistics.
9
Kaiser Health News. Adults with insurance often still have unmet dental needs, survey finds. October, 2015. Available
at: http://khn.org/news/adults-with-insurance-often-still-have-unmet-dental-needs-survey-
finds/?utm_campaign=KHN%3A+Daily+Health+Policy+Report&utm_source=hs_email&utm_medium=email&utm_conte
nt=22533884&_hsenc=p2ANqtz-8jWv6yFlEeg_QTT1JHQH4R-hbfjpxOOTOHArSwVUNCb_xzUfyW1Jfr2qgt9gjg-
PGYcK5LRTrozFU8phVIgVwEjset1g&_hsmi=22533884.
10
National Association of Dental Plans. What do dental plans normally cover? Available at:
http://www.nadp.org/Dental_Benefits_Basics/Dental_BB_3.aspx.
11
Phelps CE. Health Economics. Reading, MA: Addison Wesley Educational Publications, 1997.
12
Manning WG, Phelps CE. The demand for dental care. Bell Journal of Economics. 1979;10(2):503-525.
13
Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton-Evans G, et al. Trends in oral health status: United States,
1988–1994 and 1999–2004. National Center for Health Statistics. Vital Health Stat. 2007;11(248):1-92.
14
Eklund SA, Pittman JL, Smith RC. Trends in dental care among insured Americans, 1980 to 1995. JADA.
1997;128(2):171-78.
15
Manski, RJ, Brown E. Dental use, expenses, private dental coverage, and changes, 1996 and 2004. Agency for
Healthcare Research and Quality. 2007. MEPS Chartbook No. 17. Available at:
http://www.meps.ahrq.gov/mepsweb/data_files/publications/cb17/cb17.pdf.
16
Sing et al. Reconciling medical expenditure estimates from the MEPS and NHEA, 2002. Health Care Financing
Review. 2006;28(1):25-40.
10
Research Brief
Suggested Citation
Wall T, Guay A. The per-patient cost of dental care, 2013: a look under the hood. Health Policy Institute Research Brief.
American Dental Association. March 2016. Available from: https://www.ada.org/-/media/project/ada-
organization/ada/ada-org/files/resources/research/hpi/hpibrief_0316_4.pdf.
