Temporary Duty (TDY)
Travel Voucher Guide
How to Complete the DD 1351-2
created April 2015
Thank you for your service to our nation and thank you in advance for referring to
this guide as you prepare your travel vouchers.
This “How to” guide is intended for all service members and civilian employees
serviced by DFAS Rome Travel Pay Services. It provides step-by-step procedures in
preparing a travel voucher so it is “pay ready” upon submission. Submitting “pay
ready” vouchers will assist us in providing you a timely and accurate payment.
Defense Finance and Accounting Service
Travel Pay Operations
Rome, New York
www.dfas.mil/militarymembers/travelpay/armyactivetdy
www.dfas.mil/civilianemployees/travelpay/tdy

Instructions for completing a DD Form 1351-2
The DD Form 1351-2 is the primary form used to record travel itineraries and claim expenses for
government travel. As with tax forms there is a correct way to fill out the DD 1351-2, regardless
of the type of travel you are performing. The following is a step-by-step guide to ensure that you
are filling the form out correctly. The numbers listed below correspond to the numbers shown in
the blocks on the DD 1351-2.
Block 1: PAYMENT - Choose direct deposit, also known as Electronic Funds Transfer
(EFT). Service members and civilian employees are required by your chain of
command to use EFT for travel. If you are an Active Duty, Guard, or Reserve
service member you are required to file EFT information. Login to your myPay
account to set up your EFT account information.
Choose “Payment by Check” if you are a civilian on invitational travel orders with
the government (such as a court martial appearance or medical attendant for a
service member) or will, to the best of your knowledge, be traveling very rarely
with the government. If you are a civilian government employee or service member,
please include your EFT/bank account information.
SPLIT DISBURSEMENT – Check the box and indicate how much of your total
entitlement you would like to be paid directly to your government travel card. If
you chose “Payment by Check” in step 1, above that overrides this option; your
entire entitlement will be paid in check form. Please make sure that the split amount
adequately covers charges you’ve placed on your credit card.
Block 2: NAME – Fill in your last name, first name and middle initial.
Block 3: GRADE - If you are a civilian employee, write “C” in Box 3. If you are a service
member, write in your current rank or grade.
Block 4: SSN - Please use your complete nine digit social security number. We can process
claims with only the last four digits on the 1351-2 when your full social security
number is clearly shown on the travel order. For civilian government employees,
we can accept the last four digits on the 1351-2, provided the full social security
number appears on another official government document. But, if the social security
number is illegible we will return your claim.
Block 5: TYPE OF PAYMENT – Select “TDY” and “Member/Employee.”
Block 6a - d: ADDRESS - Your most current mailing address. If we need to contact you about
changes or corrections to your travel claim, we will do so via e-mail or telephone,
but we still need your full mailing address.
Block 6e: E-MAIL ADDRESS - This is EXTREMELY important. Your e-mail address will
be our primary means of communication in the event we have any questions about
your travel claim or corrections need to be made. Choose your primary duty or
official e-mail address, an e-mail address you will access regularly while TDY and
at home.
Block 7: DAYTIME TELEPHONE NUMBER AND AREA CODE - Your primary duty
phone or a telephone number where you can be reached.
Block 8: TRAVEL ORDER/AUTHORIZATION NUMBER – You’ll find this number on
the upper left hand corner of your orders, if TCS orders, or from Box 22 of your DD
Form1610. Invitational travel orders should have this number clearly indicated on
the orders.
Block 9: PREVIOUS GOVERNMENT PAYMENTS/ADVANCES - Have you received any
advances or other payments for the specific TDY trip you are filing this claim for?
If so, write the amounts in this box. If not, or if you are unsure, leave this box blank.
Block 10: FOR D.O. USE ONLY - This box is rarely used in full. Block 10d can be used to
indicate annual leave taken while on TDY travel. Please write in the dates of your
leave and indicate type of leave, for example “Annual Leave, 10-15 APR 2014.”
Block 11: ORGANIZATION AND STATION - Write in your unit or organization name. For
example, A CO, 4 BN, 5 RGT; Defense Information Systems Agency, etc.
Block 12: DEPENDENT(S) – Mark the “unaccompanied” box since TDY travel does not
authorize dependents.
Block 13: DEPENDENTS’ ADDRESS ON RECEIPT OF ORDERS – Leave blank since
dependent travel is not authorized on TDY travel.
Block 14: HAVE HOUSEHOLD GOODS BEEN SHIPPED - TDY travel rarely involves
shipment of household goods, so this box can usually be marked “No”. Claim
storage of household goods while TCS (temporary change of station) separately on
another DD 1351-2.
Block 15a-f: ITINERARY – You must fill out in chronological order. If for any reason the dates
are not in chronological order, illegible or missing then you will only be reimbursed
for travel that has occurred prior to the error.
For example, if the traveler mistakenly writes ARR Kandahar Afghanistan
15DEC2014 and DEP Kandahar Afghanistan 8DEC2014, the traveler can only be
reimbursed up to Dec. 8. The traveler will have to file a corrected supplemental
claim to be reimbursed past Dec. 8.
Block 15a: Write only the full year in which the travel began even when the travel crosses into
the next calendar year. For example, if your travel began 22Nov2014 and ended
15Feb2015 write 2014 as the year.
Write in every stop to/from your temporary duty location and home using the
“DEP” and “ARR” rows to make sure you are paid correctly for all stops, including
any overnight stays while en route.
Also, it is imperative that you return to your permanent duty station (PDS) or home
of record (HOR) by the final day on your travel order. For example, the traveler
goes TCS to Afghanistan and is authorized 270 days out. The traveler leaves the
area of responsibility (AOR) on day 270 but it takes 3 days to return to his PDS
bringing the total number of days out to 273. The traveler must obtain an
amendment and file a supplemental claim to be reimbursed for travel on those 3
days. Otherwise he will only be paid for the 270 days. Contact the command who
issued the original orders to get the amendment.
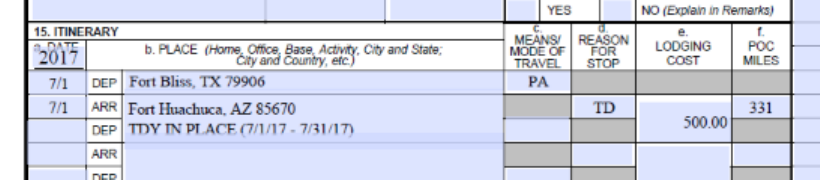
Block 15b: PLACE - PLACE - Each box in this section should only have one location per box.
When submitting an Accrual Voucher, below where you have indicated your arrival
to the TDY location enter the following into 15b “TDY in Place (Insert date range
being claimed on the voucher)” For example:.
Block 15c: MEANS/MODE OF TRAVEL - The second page of your DD Form 1351-2 lists the
two-letter codes under the instructions section that indicate which form of
transportation used en route. For example, code “GP” is Government Plane; code
“PA” is Privately Owned Auto, etc.
Block 15d: REASON FOR STOP - The second page of your DD Form 1351-2 lists the
“reasons for stop” under the instructions section. Please note that for TCS orders,
the “reason for stop” is limited to the following:
• AD – Authorized delay, for layovers while en route to the AOR. You are
authorized up to 14 days in active duty (AD) status. Beyond that, you need an
amendment authorizing any additional time.
• TD – Temporary Duty, for the TD location(s) authorized in your orders.
• MC – Mission Complete, for the date you return to your PDS or HOR.
Block 15e: LODGING COST - If your trip involved an overnight stay with lodging costs for
the location you wrote in block 15b and you are entitled to reimbursement for those
lodging costs, write that dollar amount in the space. Also, don’t forget to send in
lodging receipts or a Statement in Lieu of Receipt. The receipt needs to show the
following:
1)
lodging name and address
2)
your name
3)
check-in/check-out dates
4)
means of payment (VISA, Mastercard, etc...)
5)
dollar amount with charges itemized
6)
a zero balance (proof that you paid for your entire stay)
For example: Holiday Inn, 12345 Main Street, Smithville, TN, 22587
Check in – 05/14/214
Check out – 05/15/2014
Guest name: John Smith
Room rate:
68.00
State tax:
3.00
County tax:
2.00
Service fee:
.75
Total:
$73.75
Paid in full:
$0.00 balance
Method of payment: visa
Please note, you MUST include a receipt for both lodging and
rental car (if authorized), regardless of the amount. Receipts for items $75 and over
are required, but we highly recommend you keep and submit copies of all receipts.
If your receipts are lost or destroyed, please submit a Statement in Lieu of a
Receipt.
Block 15f: POC MILES - Did you drive to your TDY location in your personal vehicle? If so,
write in the number of miles to your TDY location. Did you drive to the airport in
your personal vehicle? Write in the number of miles to the airport. Do the same
when departing your TDY location or the airport to reach your final (MC)
destination.
Block 16: POC TRAVEL - Please note, you must check the box before “Own/Operate” to be
reimbursed for the POC miles you list in column 15f.
Block 17: DURATION OF TRAVEL - Check the approximate duration of your TD travel. If
travel was less than 12 hours you will not receive per diem for that day. If it is
between 12-24 hours you will receive partial per diem. If more than 24 hours you
will receive full Per Diem.
Block 18: REIMBURSABLE EXPENSES - This is an itemized list for a number of expenses,
such as airline tickets, rental car and fuel, public transportation or taxi fare, excess
baggage, baggage cart charges, etc. For this section please include receipts for all
expenses $75.00 and over. Also, the expense must have been incurred during the
period of actual TDY travel. For example, if SGT Pepper began TDY travel on May
11 SGT Pepper cannot be reimbursed for a taxi fare incurred on May 8.
Another rule to note is that aside from lodging, which should listed in Block 15e, all
other non-meal expenses should be listed in Block 18. If you don’t claim it we can’t
pay it, even if you are entitled to it. The one exception is your meal rate. If you are
entitled to a certain meal rate and it is clearly indicated on your orders, you don’t
need to list the cost or include receipts. The system will calculate that meal rate
automatically.
Block 19: GOVERNMENT/DEDUCTIBLE MEALS – You may be entitled to the local
commercial rate for meals but be required to dine in a dining facility (DFAC) or
other government facility during your stay. If so, write the date and number of
meals you purchased at the dining facility. Example: SGT Pepper is sent TDY to
Kuwait and is authorized the local commercial meal rate for Kuwait. However, as
part of the TDY, SGT Pepper must visit several forward operating bases (FOB) in
Afghanistan which only have government dining facilities. The date and number of
meals go in this block.
Block 20a: SIGNATURE - As simple as this box may be to fill out, it is one of the largest
problem areas. You must sign your DD 1351-2 or it will be returned for corrections.
“Claimant” refers to you as the person on TDY travel.
Block 20b: DATE - This box must contain the MONTH, DATE, and YEAR (all three items) to
be considered valid or your DD 1351-2 will be returned automatically. Many
choose to sign their DD 1351-2 electronically, which is permitted, but DO NOT
rely on the date in the electronic signature to remain legible throughout the
processing life of your claim. It is highly recommended that you include the date,
typed or hand-written, in Box 20b to avoid delays in processing your claim.
Also, the date must be on or after the mission complete (MC) date provided in the
itinerary above.
Block 20c: REVIEWER’S PRINTED NAME - Your reviewer should be your commander or
supervisor who has knowledge of the travel and can confirm accuracy. You cannot
sign as the reviewer; your claim will be returned.
Block 20d: REVIEWER’S SIGNATURE – Your claim must have the signature of your
commander or supervisor.
Block 20f: DATE – Be sure the date in Block 20f is on the same day or after the date in Block
20b. If the reviewer signs and dates your claim before you sign/date it your claim
will be returned for corrections.
Block 21a: APPROVING OFFICIAL’S PRINTED NAME - An approving official must sign
and date attesting to the validity of, and approving payment for, any additional
items not originally authorized on the orders. You must include a remark in the
remarks section, Block 29, page 2 of DD 1351-2, explaining what additional items
are being approved.
Block 21b: APPROVING OFFICIAL’S SIGNATURE – Your claim must have the approving
official’s signature to be complete. Note, only needed if approving additional items
as described above. Reviewer and Approving Official cannot be the same person.
Block 21d: DATE – Be sure the date in Block 21d is on or after the date in Block 20f.
Pay attention to the dates. If the signature dates are not in chronological order and
on/after the MC date, your claim will be returned for corrections.
Blocks 22 - 28: Do not complete. These are to be filled out by your S1 or finance officer.
Block 29: REMARKS (on second page): Claim items authorized by the Authorizing Official
(Block 21a) in this additional space. You may also use to list leave dates, though
leave dates can also be listed in Block 10.
Temporary Duty Travel Customer Service Inquiries
Please contact the agency or official issuing your travel orders for specific assistance with your
travel order, DD Form 1610.
Check the status of your voucher with the Online Payment Status Tool.
Simply enter your Travel Order/Authorization Number and email
address and you'll receive an email within minutes telling you the
status of your voucher.
For information regarding the processing of or explanation of payment for TDY travel vouchers
processed by DFAS Rome Travel Pay Services contact us at:
Toll Free: 1-888-332-7366
Email, questions only: [email protected]
Voucher submission by email: dfas.rome.jft.mbx.army-travel@mail.mil
Voucher submissions by fax: 1-317-275-0329

Important Information
Incomplete information will stop your claim from being paid! Don’t make these common mistakes
when completing your DD Form 1351-2 travel voucher.
1.
Incomplete/incorrect Itinerary
Fill out block 15 completely and accurately describing your travel stops. Include complete dates (MM/DD) in
block 15a for each travel leg shown in itinerary. Annotate “place” location in block 15b by City/State, Military
Installation/State, or City/Country. Use the correct two-digit characters (codes) for block 15c and 15d. The
correct codes are listed on the second page of the DD 1351-2.
2.
Missing supporting documentation
Receipts must be included for lodging or any expense of $75 or more.
3.
Proof of Paid Receipts
Receipts do not show a zero balance or state “paid in full.” See information on next page under “Receipts.”
4.
Using an Individually Billed Account (IBA) without Authorization
Travel orders must authorize use of an “IBA” in order for the traveler to be reimbursed airfare charged to their
government credit card.
5.
Missing Traveler’s Signature and Date
Your signature is required under penalty of perjury and fraud. A parent or legal guardian should sign the travel
voucher for a dependent minor (see signing vouchers on behalf of a minor
).
6.
Missing Reviewer’s Signature and Date
The Reviewer must verify their knowledge of the travel and review the voucher for completeness and accuracy
by signing the DD Form 1351-2.
7.
Missing Orders or Amendments
Travel orders are required with the travel voucher submission. Orders must cover the period of travel claimed.
If the original travel order was amended, then the amended order is required.
8.
Group Order Annex Missing
If you are traveling on a Reserve Group Order then the annex order/roster must be included in the voucher
submission. The annex order/roster must contain the verbiage authorizing per diem and/or travel day expense
(inside or outside of commuting distance).
9.
Failure to provide Line of Accounting
Line of Accounting on travel order is missing, incomplete or invalid.
•
Reserve Orders missing 21T in Line of Accounting (LOA), the LOA must include a 21T line. This LOA
authorizes travel and transportation allowances. Please have your orders amended to incorporate the 21T in
the LOA.
10.
Missing Signature Block on Reserve Orders
All reserve component travel orders must include a signature brief block to validate that it is an official
document.
11.
Inside Commuting Distance (Reserve Travel Exclusive)
If your order states you are “inside commuting distance,” then you are entitled to one roundtrip mileage
reimbursement. Per diem is not payable inside commuting distance.
12.
National Guard Vouchers
Claims are paid for National Guard members only when traveling in support of contingency operations. All
other National Guard vouchers should be submitted to the traveler’s servicing state United States Property
Fiscal Office (USPFO).
13.
Illegible Documents
All documents submitted must be easy to read.

Helpful Hints
Visit our website at www.dfas.mil to take advantage of the online resources. These resources
make it easier to fill out your voucher, send it in and check the status of your payment.
The SmartVoucher makes it easier for you to complete travel
vouchers error-free. It guides you step-by-step through a series
of questions then l generates a completed DD Form 1351-2
travel voucher.
Upload your travel voucher and supporting documents online
with the Travel Voucher Direct. For all travel claims computed
and paid by DFAS. Not for those using DTS (Defense Travel
System) for their travel vouchers.
With the Online Payment Status Tool simply enter your Travel
Order/Authorization Number and email address. You'll receive an
email within minutes telling you the status of your voucher.
Receipt Helpful Hints
Any and all receipts submitted with a claim should contain the following:
1)
business name and address
2)
your name
3)
check-in/check-out dates(if applicable)
4)
means of payment (VISA, Mastercard, etc...)
5)
dollar amount with charges itemized
6)
a zero balance (proof that you paid for your entire stay) – Please note, if receipt does not
show a zero ($0.00) balance but states the amount will be paid to the traveler’s IBA, you need to
submit a Statement in Lieu of Receipt.
For example: Holiday Inn, 12345 Main Street, Smithville, TN, 22587
Check in – 05/14/214
Check out – 05/15/2014
Guest name:
John Smith
Room rate:
$68.00
State tax:
3.00
County tax:
2.00
Service fee:
.75
Total:
$73.75
Paid in full:
$0.00 balance
Method of payment: visa

Please note, you MUST include a receipt for both lodging and rental car (if authorized),
regardless of the amount.
If for any reason a receipt is illegible, missing, or was not provided for the goods or services in
question, please submit a Statement In Lieu of Actual Receipt. The Statement in Lieu of Actual
Receipt must include the dates the expenses were incurred, as well as the signature date.
ActivedutyTDY- 1351-1CHECKLIST -- forTravelers
DDForm1351-Z(v.May 2011). Usuniakpen,typewtilti;oc, -'t>rlzuwtocompi.teyoorform.
D Blockl Select method of payment. D BlocklSc Usecorrect means/mode oflravelcode
D Blockl Enter fullname. (see second pageof DD 1351-2).
D Block3 Entergrade or rank.
D
BlocklSd
Use correct code for reason forstop (see
D Block 4 Enternine-digitSocial Security Nwnber.
D Block S Select typeof paymen,tfor active duty
travel "TDY"and"Member/Employee" is correct.
D Block 6a-d Provide current mailingaddress.
secondpageof DD1351-2).
D BlocklSf If authorized,enter thenwnberof miles
traveled byPOC.
D Block16 If POC miles claimed in 15f,select
D Block 6t Makesureyour email address is correct
andlegli>le. Voucherstatusemail notifications are
sent tothis
emailaddress.
D Block7 Provide your daytime(duty) telephone
number.
D Block8 Enteryour travel order/authorization
number.
D Block9 List theamount of anyadvanceand/or
partial payments you received. Write"NONE" if
you
didn't
receive anad\iance DonotindicateATM
cash withdrawals here.
D
Block
IO
Write
"annual l
eave"
ifapplica
b
le
under
"d.
computations".
D Block11 Provide organization nameand dnty
stationyou traveledto.
D Blockll Select "unaocompanied".
D
Block 13
Not applicabk
D Block 14 Select"no".
D BlocklSa Listall traveldates in chronological
order.
D Block1Sb Listall stop locations, oneperbox.
Before
submittill:g
yourclaim,
makesure
your
cwm package
iDcludes
thefollowing:
C CompleredDD Form 1351-2
sigoed.fdaredby }'t'IU
in blocks
20a/20bmd by yourrevieweris blocks20dl20f
C Complececopiesof all IDYordersmi, , .,.d ,enrs
C Supples:nemal formsand
do,
an
lffltation
as
described
abo\.-e
a R«eipcsforreimbursable expensesof$7Sormoremi all
IDdpllgODdlo,"""'I
an
e,q,emes
(if
...-imd)
a
If)'OUrmrett
depo,it(elec1nmic
flms
l!Ulsfer,
BFI)
accOODt
baschaDgedsinceyourlast tra\ieJcl aim,iDdudea,'Oided
cbec.k or
SFJ199A.
Sad via t1Uil: dfas.rome..jft.JObLarm y -tran l mail.lllil
or
fax: 317-275-0329
"o
wn/
o
pe
rate
"
.
.
D
Block17 Select thedurationof your travel.
D Block18a-d Listdates andreimbursable expenses.
All lodgingand anysingleexpenseover$75 must
D have a receipt.
Block19
Listall
govemment mealsand thedate
D
provided.
BlockZOa
Tra v eler 's si gnaturegoes in the
D
"claimantsignature" box.
Block20b DatemtLst be onor after the"mission
D
complete" date in the itinerary.
Block20c-f Reviewer's name, signature,phone
numberanddate
is required; mnstbe onor after
D traveler's s ignature/date.
Blocklla-d Get approving official' s name,
s ignature,phone nwnberand date
(if required;) mnst
0
be
onorafter thereviewers signature/date
Block29a Did you take leave inconjunctionwith
the travel? If so, include in block 15 or block 10d
portionand indicate thedates on second pageof
1351-2 in block 29a. Also, listhereitem, claimed
but notauthorized in original orders needapproving
official'ssignaturein block 2 la-d.
Note: Voucherssubmitted,ia email mustbeio PDFformat. We
cannotaccepteocrypted
e.ocapsulatedemailsorpassword
protectedfiles.Make swe youremail address(block 6e) is legible.
\li.'itbin 2448 bounreceipt
DOCific.atioDs
aresemas yourclaimis
loggedintooursystem. Pleasesubmiteachclaimooce. Multiple
submissionsof
ibe
same\
1
oucher
could
slow
processing
of
y
our
claim.
IfyoudoDO( recei\,e the"ootincatioa of receipr'' after 48 hours,
pleasec0ctactourCUstomer Care Center.
J-l!38-332-7366
dfas.rome.jftmbx.ccc.ttave.lpay@mail.mil
(seodquestions
OWy,
oot
tta\--el
claimsto thisaddress)
http://go.US3.go v/9Sx
