(mvphealth
Vermont Health Connect
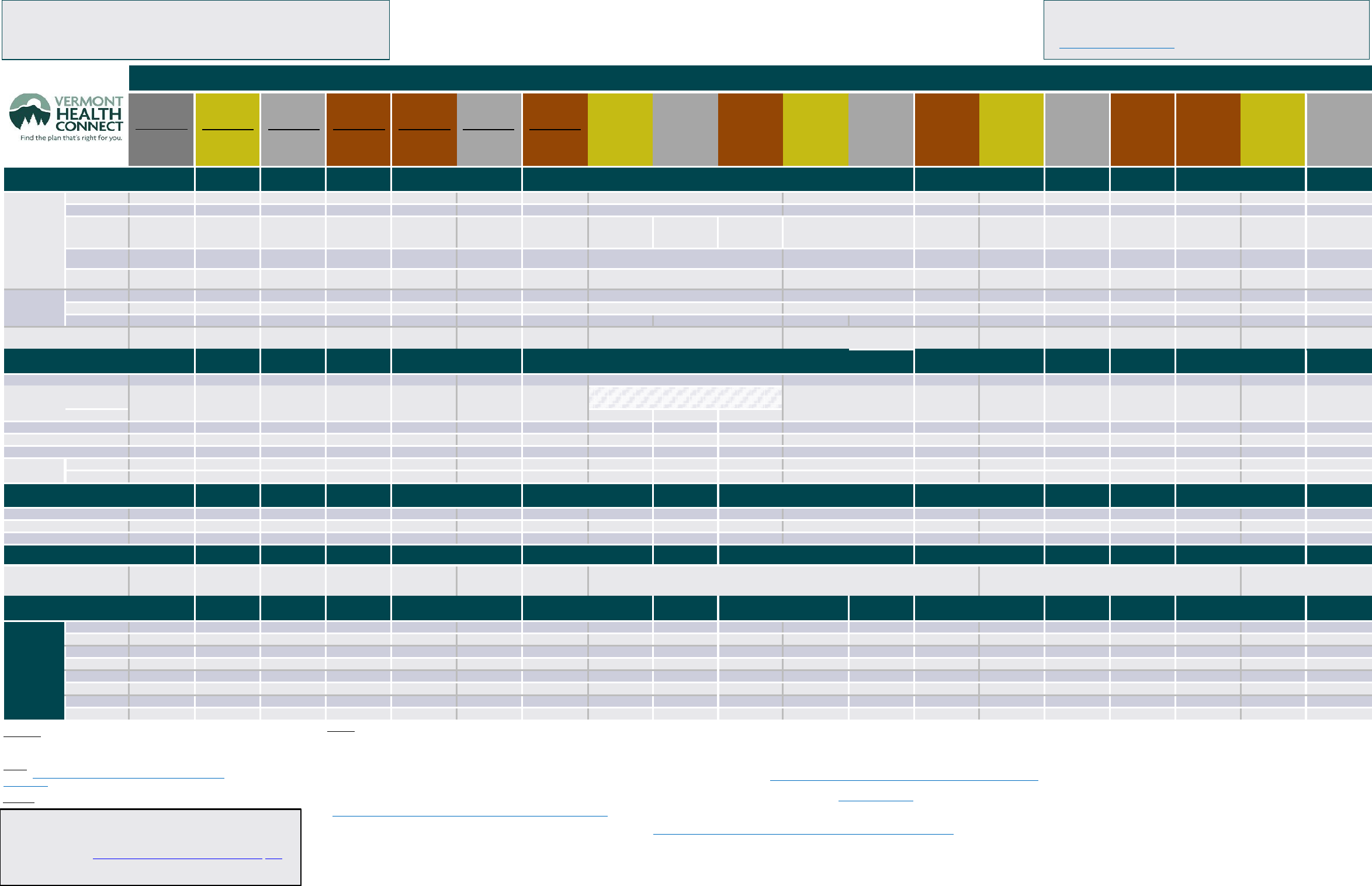
2023 Plan Designs & Premiums for Individuals and
Families*
(before any subsidies)
Standardized Plans Standardized Plans
BCBSVT Plans Only
BCBSVT Plans Only
MVP Plans Only
MVP Plans Only
(same coverage for both insurance carriers) (high deductible ‐ can pair with HSA) (CDHP ‐ can pair with HSA) (HDHP ‐ can pair with HSA)
BCBSVT
Platinum Plan
MVP
Platinum 1
BCBSVT
Gold Plan
MVP VT
Gold 1
BCBSVT
MVP VT
Silver 3
BCBSVT
Bronze Plan
MVP VT
Bronze 2
BCBSVT
Bronze Integrated
Plan
MVP VT
Bronze 4
BCBSVT Silver
CDHP Plan
MVP VT
Silver 4 HDHP
BCBSVT Bronze
CDHP Plan
MVP VT
Bronze 3 HDHP
BCBSVT
Vermont
Preferred Gold
Plan
BCBSVT
Vermont
Preferred Silver
Plan
BCBSVT
Vermont
Preferred Bronze
Plan
BCBSVT
Vermont Select
Gold CDHP Plan
BCBSVT
Vermont Select
Silver CDHP Plan
BCBSVT
Vermont Select
Bronze CDHP Plan
MVP VT Plus
Gold 2
MVP VT Plus
Silver 1
MVP VT Plus
Bronze 1
MVP VT Plus
Bronze 5
MVP VT Plus
Gold 3 HDHP
MVP VT Plus
Silver 2 HDHP
Deductibles & Out‐of‐
Pocket Limits
Individual / Family Individual / Family Individual / Family
Individual / Family Individual / Family Individual / Family Individual / Family
Individual / Family Individual / Family Individual / Family
Individual / Family Individual / Family Individual / Family Individual / Family Individual / Family Individual / Family
Individual / Family Individual / Family Individual / Family
Deductible (Ded.)
Integrated Ded.?
N
N
N
N
$9,000/$18,000 $2,100/$4,200
$5,800/$11,600
$1,250/$2,500 $3,200/$6,400 $8,950/$17,900 $2,675/$5,350 $5,125/$10,250 $7,150/$14,300
N
N
N
$9,100/$18,200
$3,200/$6,400
$5,500/11,000
Medical Ded.
$425/$850 $1,400/$2,800 $4,000/$8,000
$6,450/$12,900
See above
See above
See above
See above
See above
See above
See above
See above
See above
$850/$1,700 $2,100/4,200
$7,250/$14,500
See above
See above
See above
Waived
1
for:
(see Services
below)
Prev, OV, UC, Amb,
Den1, Vision
Prev, OV, UC, Amb,
Den1, Vision
Prev, OV, UC, Amb,
Den1, Vision
Prev, Den1 Prev, OV, Den 1 Prev Prev
Prev,
4 PCP/MH/Qualified
Specialist OV, Den1
11
Prev,
4 PCP/MH/Qualified
Specialist OV, Den1
11
Prev,
4 PCP/MH/Qualified
Specialist OV, Den1
11
Prev Prev Prev
Prev, UC, OV,
Den1
10
Prev, 3 PCP/MH,
Den1
Prev, Den 1
Prev,
3 PCP/MH OV,
Den1
Prev Prev
Prescription (Rx)
Ded.
$0 $200/$400 $500/$1,000 $1,100/$2,200 See above See above See above
See above See above See above See above See above See above $350/$700 $850/1,700 $700/$1,400 See above See above See above
Waived for:
N/A ($0 Ded.) Rx Generic Rx Generic Rx Generic
Rx Generic
1
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx Wellness
8
Rx VBID,
Rx Generic
Rx VBID
Rx VBID,
Rx Generic
Rx VBID,
Rx Tier 1
Rx Wellness Rx Wellness
Max.
Out‐of‐Pocket
(MOOP)
Integrated?
N
N
$9,100/$18,200 $9,100/$18,200 $9,000/$18,000 $7,050/$14,100 $7,100/$14,200
$5,150/$10,300
$8,550/$17,100 $8,950/$17,900 $2,675/$5,350 $5,125/$10,250 $7,150/$14,300
N
N
$8,400/$16,800
$9,100/$18,200
$3,200/$6,400
$5,500/11,000
Medical
$1,500/$3,000 $5,600/$11,200
See above
See above
See above
See above
See above
See above
See above
See above
See above
See above
See above
$6,600/$13,200 $7,000/14,000
See above
See above
See above
See above
Prescription (Rx)
$1,400/$2,800
$1,400/$2,800
$1,400/$2,800
$1,400/$2,800
See above
$1,500/$3,000 $1,500/$3,000 $1,500/$3,000 $1,500/$3,000
See above
$1,500/$3,000 $1,500/$3,000
See above
$1,400/$2,800
$1,400/$2,800
See above
See above
$1,500/$3,000 $1,500/$3,000
Stacked, Embedded, or Aggregated
6
Stacked
6
Stacked
6
Stacked
6
Stacked
6
Stacked
6
Aggregate
6,9
Embedded
Aggregate
6,9
Embedded
Aggregate
6,9
Embedded
Individual OOPM of $9,100
Aggregate
6
Aggregate
6,9
Embedded
Individual OOPM of $9,100
Stacked
6
Stacked
6
Stacked
6
Stacked
6
Aggregate
6
Stacked
6
Service Category
Co‐insurance
(%)
/
Co‐insurance
(%)
/
Co‐insurance
(%)
/
Co‐insurance
(%)
/
Co‐insurance
(%)
/ Co‐insurance
(%)
/
Co‐insurance
(%)
/
Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) / Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) /
Co‐insurance (%) / Co‐insurance (%) /
Co‐insurance (%) /
(Examples)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($) Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($) Co‐pay ($)
Co‐pay ($)
Co‐pay ($)
Co‐pay ($) Co‐pay ($)
Co‐pay ($)
Preventive (Prev)
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
$0
Office Visit
(OV)
PCP or Mental
Health (PCP/MH)
$15*
$40
$20*
$50
$40*
$90
Ded., then $35
Ded., then $90
$40*
$100
Ded., then 10%
Ded., then 30%
Ded., then 50%
Ded., then 50%
4 combined visits with no cost‐share; then deductible applies,
then co‐pay: $20 (Gold), $30 (Silver), $0 (Bronze)
11
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
$20
$45
$30 x3, then ded.,
then $30
12
Ded., then $60
Ded., then $40
Ded., then $100
0% x3, then ded.,
then 0%
12
Ded., then 0%
Ded., then 0%
Ded., then 0%
Ded., then 0%
Ded., then 0%
Specialist
2
Ded., then $40
11
Ded., then $50
11
Ded., then $0
11
Urgent Care (UC)
$50
$60
$100
Ded., then $100
Ded., then $0
Ded., then 30%
Ded., then 50%
Ded., then $40
Ded., then $50
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
$30
Ded., then $60
Ded., then $100
Ded., then 0%
Ded., then 0%
Ded., then 0%
Ambulance (Amb)
$60
$70
$100
Ded., then $100
Ded., then $0
Ded., then 30%
Ded., then 50%
Ded., then $40
Ded., then $50
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $50
Ded., then $100
Ded., then $100
Ded., then 0%
Ded., then 0%
Ded., then 0%
Emergency Room (ER)
3
Ded, then $100
Ded, then $150
Ded., then $500
Ded., then 50%
Ded., then $0
Ded., then 30%
Ded., then 50%
Ded., then $250
Ded., then $450
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $250
Ded., then $400
Ded., then 50%
Ded., then 0%
Ded., then 0%
Ded., then 0%
Hospital Services
4
Inpatient
Ded., then 10%
Ded., then 30%
Ded., then 50%
Ded., then 50%
Ded., then $0
Ded., then 30%
Ded., then 50%
Ded., then $750
Ded., then $1,750
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then 20%
Ded., then 50%
Ded., then 50%
Ded., then 0%
Ded., then 0%
Ded., then 0%
Outpatient
Ded., then 10%
Ded., then 30%
Ded., then 50%
Ded., then 50%
Ded., then $0
Ded., then 30%
Ded., then 50%
Ded., then $750
Ded., then $1,750
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then 20%
Ded., then $1,400
Ded., then 50%
Ded., then 0%
Ded., then 0%
Ded., then 0%
Prescription (Rx) Drug Coverage
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
30‐day
supply
Rx Generic
5
$10
$12
$20
$15
$30
Ded.
8
, then $10
Ded.
8
, then $12
Ded., then $5
Ded., then $5
Ded.
8
, then $0
Ded., then $0
Ded., then $0
Ded., then $0
$15
Ded., then $5
$25
$35
Ded.
8
13
then 0%
Ded.
8
, then 0%
Rx Preferred Brand
5
$50
Ded., then $55
Ded., then $70
Ded., then $85
Ded., then $0
Ded.
8
, then $40
Ded.
8
, then 40%
Ded., then 40%
Ded., then 40%
Ded.
8
, then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $40
Ded., then 50%
Ded., then $100
Ded., then 0%
Ded.
8
13
then 0%
Ded.
8
, then 0%
Rx Non‐Preferred Brand
5
50%
Ded., then 50%
Ded., then 50%
Ded., then 60%
Ded., then $0
Ded.
8
, then 50%
Ded.
8
, then 60%
Ded., then 60%
Ded., then 60%
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then $0
Ded., then 50%
Ded., then 50%
Ded., then 60%
Ded., then 0%
Ded.
8
13
then 0%
Ded.
8
, then 0%
Additional Benefits
Wellness/Other Benefits
N/A N/A N/A N/A N/A N/A
N/A
Individualized online wellness portal
Up to $600 in Well-Being Reimbursements Gold and Silver VBID RX Co‐
pay $1; Bronze VBID RX Co‐pay $3; $0 Generics to age 10. Gia
®
Virtual Care Services; $500 Acupuncture Allowance
14
Up to $600 in Well-Being Reimbursements;
Gia
®
Virtual Care Services; $500
Acupuncture Allowance
14
Premiums by Tier
Cost before Cost before Cost before Cost before Cost before Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
Cost before
(monthly cost)
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
subsidy
Single
BCBSVT
$1,134.56 $941.63 $848.31 $640.78 $660.98 $875.58 $663.06 $894.00 $841.08 $653.11 $913.28 $837.38 $645.48
N/A
N/A
N/A
N/A
N/A
N/A
MVP
$1,138.38
$939.60
$854.37 $674.76 $706.61 $867.56 $685.66
N/A
N/A
N/A
N/A
N/A
N/A
$989.35 $847.85
$672.82 $678.90 $972.69 $872.57
Couple
BCBSVT
$2,269.12
$1,883.26
$1,696.62
$1,281.56
$1,321.96 $1,751.16 $1,326.12 $1,788.00 $1,682.16
$1,306.22
$1,826.56
$1,674.76 $1,290.96
N/A
N/A
N/A
N/A
N/A
N/A
MVP
$2,276.76 $1,879.20 $1,708.74 $1,349.52
$1,413.22
$1,735.12 $1,371.32
N/A
N/A
N/A
N/A
N/A
N/A
$1,978.70 $1,695.70
$1,345.64
$1,357.80
$1,945.38 $1,745.14
Parent and
BCBSVT
$2,189.70 $1,817.35 $1,637.24 $1,236.71 $1,275.69 $1,689.87 $1,279.71 $1,725.42 $1,623.28
$1,260.50 $1,762.63
$1,616.14
$1,245.78
N/A
N/A
N/A
N/A
N/A
N/A
Child(ren)
MVP
$2,197.07 $1,813.43
$1,648.93 $1,302.29 $1,363.76
$1,674.39 $1,323.32
N/A
N/A
N/A
N/A
N/A
N/A
$1,909.45
$1,636.35 $1,298.54 $1,310.28
$1,877.29 $1,684.06
Family
BCBSVT
$3,188.11
$2,645.98
$2,383.75 $1,800.59
$1,857.35
$2,460.38
$1,863.20
$2,512.14 $2,363.43 $1,835.24
$2,566.32 $2,353.04 $1,813.80
N/A
N/A
N/A
N/A
N/A
N/A
MVP
$3,198.85
$2,640.28
$2,400.78 $1,896.08 $1,985.57 $2,437.84 $1,926.70
N/A
N/A
N/A
N/A
N/A
N/A
$2,780.07 $2,382.46 $1,890.62 $1,907.71 $2,733.26 $2,451.92
Abbreviations
‐‐
Ded
: Deductible,
Rx
: Prescription Drugs,
OV
: Office Visits,
UC
:
Urgent Care,
Amb
: Ambulance,
VBID
: Value‐Based Insurance Design,
Den1
:
Pedatric Dental Class 1 Series,
ER
: Emergency Room.
Glossary
‐‐ Find definitions for
VBID
,
Stacked
,
Aggregated
,
Integrated
, and other
terms at https://info.healthconnect.vermont.gov/learn‐more/health‐insurance‐
basics/list‐terms
Plan details
‐‐ Different plans cover specific drugs and services in different ways.
Footnotes
1
Medical Deductible waived for: Preventive, Office Visit, Urgent Care, Ambulance, Emergency Room, Vision, Pediatric Dental Class 1 Series (as indicated by plan).
2
Specialist co‐pay also applies to ST, OT, and any alternative medicine benefits, as appropriate. PT/Chiro have separate cost share.
3
ER co‐pay is waived if admitted.
4
Hospital Services are Inpatient (including surgery, ICU/NICU, maternity, SNF and MH/SA); Outpatient (including ambulatory surgery centers); and Radiology (MRI, CT, PET). This cost‐sharing will also include physician and anesthesia costs, as appropriate.
5
Each insurance carrier classifies drugs according to its own formulary. To see if a specific drug qualifies for the Generic or Preferred co‐pay, view the formularies at https://info.healthconnect.vermont.gov/compare‐plans/qualified‐health‐plans/covered‐prescriptions or contact BCBSVT (800‐247‐2583) or MVP (844‐865‐0250).
6
With an aggregate family deductible, your family must meet the family deductible before the plan pays benefits. With a stacked deductible, the plan pays benefits once you meet either your individual deductible or your family deductible.
7
If you purchase a silver plan and your income qualifies for cost‐sharing reductions your deductible and max. out‐of‐pocket could be lower than the figures stated above. To learn more, go to VermontHealthConnect.gov and click on "Compare Plans."
8
With MVP High Deductible Health Plans (HDHP), BCBSVT Vermont Select CDHP, BCBSVT CDHP and Vermont Preferred plans, might have deductibles for Wellness prescriptions before cost‐shares apply. See the BCBSVT and MVP lists of Wellness drugs at
https://info.healthconnect.vermont.gov/compare‐plans/qualified‐health‐plans/covered‐prescriptions.
9
Some aggregate family deductibles have an embedded individual maximum out‐of‐pocket of $9,100 to prevent one individual from paying the full family maximum out‐of‐pocket when it exceeds the federal maximum out‐of‐pocket of $9,100 for an individual.
10
This plan includes deductible‐waived vision care for qualifying children. See Summary of Benefits and Coverage for details: https://info.healthconnect.vermont.gov/compare‐plans/qualified‐health‐plans/summaries‐benefits‐and‐coverage.
11
BCBSVT VT Preferred provides 4 additional pre‐deductible visits with certain specialists, plus unlimited nutritional counseling for heart disease & diabetes patients.
12
Benefit covers three (3) visits at indicated cost share, for each plan member, before the deductible.
13
Preventive drugs on the MVP VT Plus Gold 3 HDHP plan are $10/$15/5% before the deductible.
14
See plan documents for more information about these benefits
.
* First 3 visits per member covered in full
Updated 09/29/2022
*n 2023, qualified health plans have the same plan designs but different premiums
for small group. You can find the small group market premiums here:
•
Blue Cross and Blue Shield of Vermont 2023 Small Group Plans &
Premiums Chart (bluecrossvt.org/smallbusiness).
•
MVP Health Care® MVP Product Placemat Vermont Small Group 2023 Plans
(mvphealthcare.com)
To
enroll in small group plans, contact BCBSVT or MVP
Interested in the cost after subsidy?
Most Vermonters who use Vermont Health Connect qualify for financial help
to reduce their costs. To see if you qualify, visit the Plan Comparison Tool
at https://vt.checkbookhealth.org or call 1‐855‐899‐9600.
All Vermont Health Connect plans cover the same set of Essential Health Benefits.
The difference lies in the plan designs, which determine how you pay for those benefits.
Standardized plans have the same designs across insurance carriers, while the other QHPs
(Qualified Health Plans) were uniquely designed by the carriers.
Aggregate
6,9
Embedded
Individual OOPM of $9,
100
Aggregate
6,9
Embedded
Individual OOPM of $9,100
Aggregate
6,9
Embedded
Individual OOPM of $9,100
Silver Plan
