Paid Maternity + Parental Leave
Nursing Loan Repayment Program
Voluntary Benefit Offerings
2023 Benets Highlights
for Main Campus Residents and Fellows
2
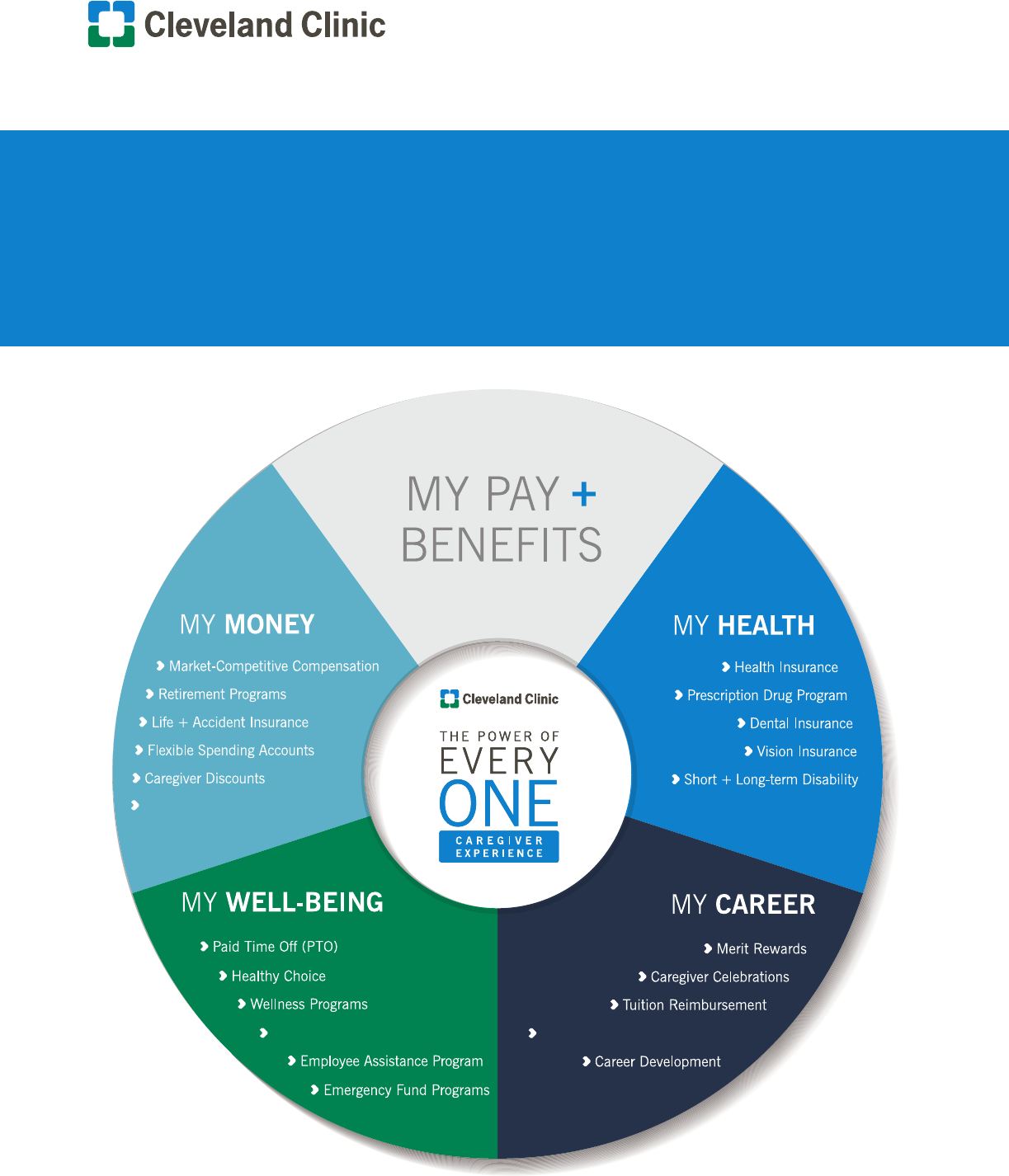
Empowering You to Choose
Cleveland Clinic knows your needs may differ from those of your colleagues, and your preferences
can change at any stage of your life.
This is why we offer comprehensive benets options as part of your My Pay + Benets package.
With more opportunities to choose, you can determine how our benets offerings can best help
you thrive every day.
Take a few moments to review these benets highlights. Detailed summary plan descriptions are
available on the ONE HR Portal. Making informed decisions about the benets you elect protects
you and your family, supports your health and well-being, and improves your caregiver experience.
Thank you for your dedication to our patients, our communities and your fellow caregivers.
Eliane Seeman
Executive Director, Total Rewards
Table of Contents
HOW TO ACCESS THE ONE HR PORTAL ... 3
ELIGIBILITY ......................................... 3
BENEFITS ENROLLMENT ...................... 4
MY HEALTH
Employee Health Plan (EHP) ................... 5
Dental Plan Options ............................. 10
Vision Plan Options .............................. 12
Disability ............................................. 13
MY MONEY
Life Insurance ...................................... 14
Loan Program ...................................... 14
On Call Meals ...................................... 14
Retirement Program .............................. 14
Travel Benet........................................ 15
Uniform Information .............................. 15
Voluntary Benet Programs .................... 15
Flexible Spending Accounts (FSAs) ......... 18
MY WELL-BEING
Well-Being Programs ............................ 19
Employee Assistance Program ............... 19
Adoption Assistance ............................. 19
Bereavement Leave .............................. 19
Maternity and Parental Leave ................ 20
Medical Leave of Absence ..................... 20
Military Leave of Absence (FMLA) .......... 20
Paid Personal Days ............................... 20
Personal Leave ..................................... 20
Vacation Days ...................................... 20
Caregiver Leave ................................... 21
Healthy Choice Program ....................... 21
BENEFIT COSTS ................................. 22
TERMS AND DEFINITIONS .................. 23

3
How to Access the ONE HR Portal
Everything you need to know about your benets is in one place – the ONE HR Portal – and you’re there in just a few clicks!
• Visit https://www.ccf.org/ONEHR
• Select “Current Caregiver” to log in to Workday
• Under “Announcements” in the bottom right, click “Access the ONE HR Portal”
• Press the blue button, “Click HERE to Access the ONE HR Portal.”
• If you need assistance call the ONE HR Service Center at 877.688.CCHR
To review benet offerings from home follow these steps to install the Workday app on your Android, iPhone or iPad devices.
Access Workday
from Home
Install and Log In to Workday from your
Android, iPhone and iPad
Eligibility
In general, the benets described in this summary are extended to active residents and fellows at Cleveland Clinic main
campus.
Dependent Eligibility
Dependents eligible for coverage under the Cleveland Clinic health, dental, vision and life insurance benet programs
include:
• A caregiver’s lawful spouse (not divorced or legally separated)
• The following child(ren) of a caregiver or caregiver’s spouse:
• a natural or legally adopted child
• a child placed for adoption with the caregiver or spouse
• a child for whom the caregiver or spouse has been appointed by a court as the legal guardian
• a child for whom the caregiver or spouse is required to provide coverage under a qualied medical
support order (as dened in Section 609 of ERISA)
provided the child is less than 26 years old, or if prior to age 26 the child is determined by the Social Security
Administration to be physically or mentally incapable of self-support and is receiving principal nancial support from the
caregiver and/or spouse and is enrolled in the plan(s) at the time they turn 26.
4
Benets Enrollment
New Hires and Newly Eligible
Newly hired or newly eligible caregivers can enroll in benets in Workday beginning on their start date and will have 31 days
from their start date to enroll. Failure to enroll in benets within this 31 day period will result in waiving coverage under the
health, dental, vision, exible spending accounts (FSAs) and supplemental/dependent life insurance benet programs.
New hire and newly eligible benet elections become effective retroactively to the caregiver’s start date. Caregivers
are required to provide dependent verication documentation after adding a dependent to benet programs as part of
this enrollment process. After enrollment has been completed caregivers will be contacted by Willis Towers Watson via
postal mail with instructions on what documentation is required and where to send it. Failure to provide the requested
documentation will result in the dependent(s) being removed from coverage under each benet program they were originally
added on to.
Life Events
Caregivers may be able to make benet election changes after experiencing a qualifying life event change. The IRS denes
life events as follows:
• Change in marital status
• Birth/adoption/legal guardianship of a child
• Death of a dependent
• Loss or gain of outside coverage
• Employment status change (full-time to part-time, vice versa)
• Qualied medical support order (QMSO)
• Change in the place of residence or work
Caregivers who experience a life event which would necessitate a change in benets elections can initiate a life event benet
change in Workday within 31 days of the qualifying event. Any change in benet elections must be consistent with the life
event, and documentation must be provided to support the life event change request.
Annual Open Enrollment
Caregivers have the opportunity to make changes to benet elections each year during the annual open enrollment period.
Open enrollment takes place in the fall of each year (end of October through early November). Benet election changes are
made in Workday during the open enrollment period, and changes become effective January 1 of the following calendar
year. Caregivers are required to provide dependent verication documentation after adding a dependent to benet programs
as part of the open enrollment process. Failure to provide the requested documentation will result in the dependent(s) being
removed from coverage under each benet program they were added on to during open enrollment.
5
MY HEALTH
Employee Health Plan (EHP)
The Cleveland Clinic Employee Health Plan (EHP) provides comprehensive healthcare benets for plan members. The EHP
includes a 2 tier network of providers. Benets are maximized when members use Tier 1 Cleveland Clinic Quality Alliance
network providers.
Tier 1 Network
The Tier 1 provider network is the Cleveland Clinic Quality Alliance (QA) network. This network includes Cleveland Clinic
facilities and employed physicians as well as contracted community physicians and facilities in northeast Ohio. Tier 1
providers can be found online at employeehealthplan.clevelandclinic.org.
Highlights of the Tier 1 network include:
• No annual deductible
• No co-pays or co-insurance for primary care ofce visits (Internal Medicine, Family Practice, OB-GYN and Pediatrics)
• No co-pays or co-insurance for all virtual visits (includes, Express Care Online app and real time virtual visits)
• $35 specialist ofce visit co-pay
• $350 co-pay for inpatient services (prior authorization is required), including labor and delivery
In the Tier 1 network, the services listed above are covered 100% after the applicable copays have been paid.
Tier 2 Network
The Tier 2 provider network is the Aetna Select Open Access Network. Note: The University Hospital System,
University Hospital Case Medical Center, Summa Health System, Aultman Hospital and their employed physicians
and their afliates are not considered in the EHP or Aetna networks. Tier 2 providers can be accessed by visiting
employeehealthplan.clevelandclinic.org.
Services from Tier 2 providers are subject to a $500 annual deductible and most medically necessary services are covered
70% thereafter. Routine health examinations, routine screening tests, and certain other medical services are not covered
in Tier 2.
Emergency and Urgent Care
Emergency care and urgent care visits are covered 100% (after applicable copay) regardless of which provider is used.
Emergency department visits are subject to a $250 copay and urgent care visits are subject to a $50 copay.
Additional Information
The charts on pages 6 and 7 outline the medical benet coverage for the EHP. Complete coverage information, including
exclusions and limitations, can be referenced in the EHP Summary Plan Description (SPD), which can be accessed through
the EHP website at employeehealthplan.clevelandclinic.org.
See page 22 for health plan costs.
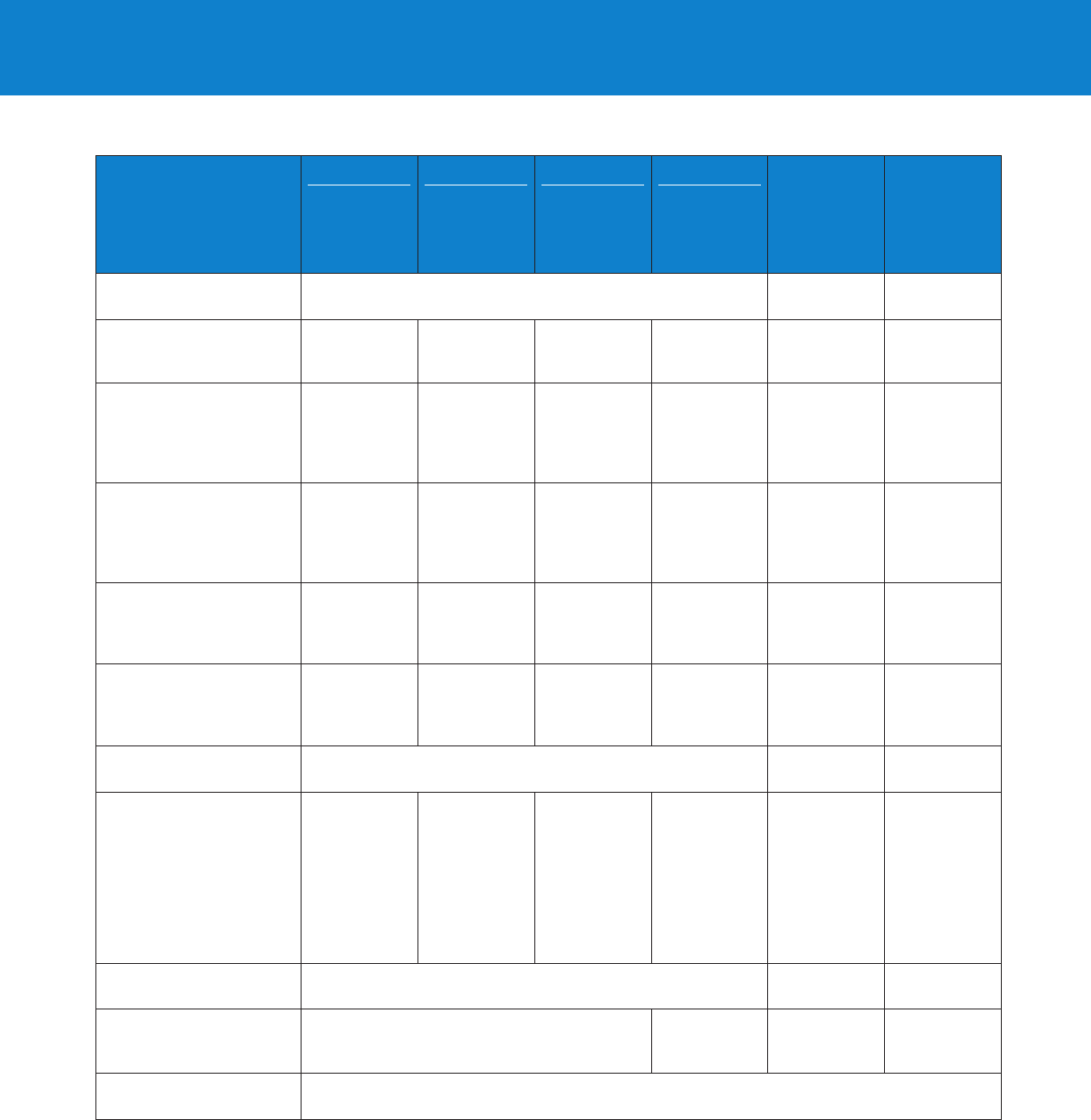
6
MY HEALTH
Benet Program Features
TIER 1
Cleveland Clinic
Quality Alliance Network
TIER 2
Aetna Select
Open Access Network
Annual Deductible
Single
Family
Out-of-Pocket Maximum
Single
Family
None
None
$3.950
$7,900
$500
$1,500
$4,750
$9,500
Medical Benet Program Features
PCP Ofce Visit (Family Practice, Internal
Medicine, Gynecology, Obstetrics and Pediatrics)
100% of Allowed Amount
$25 co-pay, then 70% of Allowed
Amount (after deductible)
PCP Virtual Visits 100% of Allowed Amount
$25 co-pay, then 70% of Allowed
Amount (after deductible)
Specialist Ofce Visits
100% of Allowed Amount after $35 copay
(no referral required)
$50 co-pay, then 70% of
Allowed Amount (after deductible)
Specialist Virtual Visits 100% of Allowed Amount
$50 co-pay, then 70% of
Allowed Amount (after deductible)
Maternity Care
$350 co-pay/admission, then 100% of
Allowed Amount
$350 co-pay/admission, then 70% of
Allowed Amount (after deductible)
Routine (Annual) Physical Exam by
Primary Care Physician
Routine (Annual) Vision Exam
100% of Allowed Amount
100% of Allowed Amount after $35 co-pay
Not Covered
Not Covered
Inpatient Hospital Services
1
$350 co-pay/admission, then 100% of
Allowed Amount
$350 co-pay/admissions, then 70% of
Allowed Amount (after deductible)
Outpatient Hospital Services
Radiology –
MRI/CT Scans (non-emergent)
1
100% of Allowed Amount
100% of Allowed Amount
$75 co-pay, then 100% of Allowed Amount
70% of Allowed Amount (after deductible)
70% of Allowed Amount (after deductible)
$75 co-pay, then 70% of Allowed Amount
(after deductible)
Laboratory/Diagnostic Tests 100% of Allowed Amount 70% of Allowed Amount (after deductible)
Emergency Department
Emergency Care
Urgent Care
100% after $250 co-pay
100% after $50 co-pay
100% after $250 co-pay
100% after $50 co-pay
Medical Supplies and Durable
Medical Equipment
80% of Allowed Amount
80% of Allowed Amount
(after deductible)
Skilled Nursing Care
1
60 Days per Benet Year
$350 co-pay/admission, then 100% of
Allowed Amount
$350 co-pay/admission, then 70% of
Allowed Amount (after deductible)
Acute Inpatient Rehab
1
60 Days per Benet Year
$350 co-pay/admission, then 100% of
Allowed Amount
Not Covered
Long-Term Acute Care
1
60 Days per Benet Year
$350 co-pay/admission, then 100% of
Allowed Amount
Not Covered
Hospice
Symptom Management
Respite Care
100% of Allowed Amount
100% of Allowed Amount
100% of Allowed Amount
100% of Allowed Amount
100% of Allowed Amount
100% of Allowed Amount
Home Health Care
1
60 Visits per Benet Year
100% of Allowed Amount 70% of Allowed Amount (after deductible)
Acupuncture
Maximum of 10 Visits/Benet Year
50% of Allowed Amount Not Covered
Chiropractic
Maximum of 30 Visits/Benet Year
100% of Allowed Amount after $35 co-pay Not Covered
EHP Benets Summary
1. Precertication required.

7
MY HEALTH
EHP Benets Summary (continued)
Medical Benet Program Features
TIER 1
Cleveland Clinic
Quality Alliance Network
TIER 2
Aetna Select
Open Access Network
Therapy Services (Rehabilitative)
Occupational/Speech/Physical
100% of Allowed Amount after a $10 copay.
30 Visits per Therapy per Calendar Year
Not Covered
Therapy Services (Habilitative)
Physical/Occupational/Speech
a. Developmental Delay, Cerebral Palsy, Apraxia
b. Autism and Autism Spectrum Disorder
100% of Allowed Amount
30 Visits per Therapy per Calendar Year
100% of Allowed Amount (No visit limitation)
Not Covered
Dental – Surgical extractions for soft/bony
impactions, or dental implants for certain medical
conditions or recent accidents/injuries
100% of Allowed Amount Not Covered
Family Planning
2
(See Coverage Clarications)
Voluntary Abortion
100% of Allowed Amount
100% of Allowed Amount
Not Covered
100% of Allowed Amount
Infertility Treatment
1
100% of Allowed Amount
LTM: ($15,000 Medical, $6,000 Pharmacy)
Not Covered
Hearing Aids
5
50% of Charge up to $3,500/Ear –
Limited to one aid per Ear every 3 years
Not Covered
Organ Transplant
1
Transplant Lifetime Maximum
Out-of-Pocket Maximum
100% of Allowed Amount
Unlimited
See previous page
Not Covered
Behavioral Health Benet Program Features
Outpatient Coverage
Outpatient (OP Visits)
3
Ofce Visits
Psychological and Neuro-Psychological Testing
4
100% of Allowed Amount
$35 co-pay, then 100% of Allowed Amount
100% of Allowed Amount
100% of Allowed Amount (after deductible)
$50 co-pay, then 70% of Allowed Amount
(after deductible)
Not Covered
Outpatient Telemedicine/Virtual Consultation 100% of Allowed Amount 100% of Allowed Amount (after deductible)
Inpatient Coverage
1
$350 co-pay/admission, then 100% of
Allowed Amount
$350 co-pay/admission, then 70% of
Allowed Amount (after deductible)
Intensive Outpatient (OP)
1
100% of Allowed Amount 70% of Allowed Amount (after deductible)
Partial Hospitalization Programs (PHP)
1
100% of Allowed Amount 70% of Allowed Amount (after deductible)
Residential Treatment
1
$350 co-pay/admission, then 100% of
Allowed Amount
Not Covered
Transcranial Magnetic Stimulation (TMS)
1
36 Therapy Related Visits per Benet Year
100% of Allowed Amount Not Covered
For Tier 1, co-payments and co-insurance listed on this chart accumulate to your out-of-pocket maximum
with the exception of co-payments for bariatric surgery and the Autism School.
1. Precertication required.
2. Marymount and Mercy Hospital employees are subject to Religious Exemption and are not eligible for the
following: transgender services and family planning services which include infertility treatment, abortion,
vasectomy, contraceptive implants, Depo Provera, IUE, tubal ligation, and oral contraceptives, except if
clinically appropriate.
3. The Outpatient coverage for the Behavioral Health Benet Program includes any outpatient services
provided by a behavioral health practitioner for chronic pain management, sleep disorder, aftercare groups
for substance abuse, and/or pre and post gastric surgery visits. There is no coverage for school meetings by
outpatient behavioral health practitioners.
4. Psychological and Neuro Psychological Testing: Up to eight hours testing are automatically covered without
precertication. Neuro-Psychological Testing: Testing is covered in Tier 1 only, by trained Behavioral Health
Specialists.
5. Hearing aids are only covered when provided by a Cleveland Clinic provider. There is no coverage for any
other provider.
Note: Prior authorization, precertication and prior approval are often used interchangeably.
Any unauthorized programs, services or visits will not be covered by the HBP
under any circumstances and the subsequent charges will be the nancial responsibility
of the member. This applies to any unauthorized out-of-network and out-of-area
providers and facilities, with the only exception being for emergency care.
8
MY HEALTH
Prescription Drug Benet
The prescription drug benet is included with the EHP and provides coverage for prescriptions obtained through Cleveland
Clinic and CVS Pharmacies. Highlights of the prescription drug benet include:
• No deductible on generic medications obtained at Cleveland Clinic Pharmacies
• $200 deductible for brand name medications obtained at any in-network pharmacy, or generics obtained at CVS
Pharmacies
• Preferred generics covered at 85% at Cleveland Clinic Pharmacies and 80% at CVS Pharmacies
• Preferred brands covered at 75% at Cleveland Clinic Pharmacies and 70% at CVS Pharmacies
• 90 day supplies and routine maintenance medications can only be lled at Cleveland Clinic Pharmacies or through
Cleveland Clinic or CVS Mail Order Pharmacies
A summary overview of the prescription drug benet for 2023 is on page 9. Additional information on the prescription drug
benet, including a full listing of Cleveland Clinic locations, can be found in the Cleveland Clinic Employee Health Plan
Summary Plan Description which can be accessed through the EHP website at employeehealthplan.clevelandclinic.org.
9
MY HEALTH
The Following Is a Summary Overview of the Prescription Drug Benet for 2023
Categories
TIER 1
Preferred
Generics
(Non-Specialty)
TIER 2
Preferred
Brands
(Non-Specialty)
TIER 3
Non-Preferred/
Non-Formulary
Brands and
Generics
TIER 4
Specialty Brand/
Generic Drugs
(Hi-Tech)
Drugs & Items
at Discounted
Rate
Non-Covered
Drugs & Items
Annual Deductible
$200 Individual (Waived for generic prescriptions if obtained
$400 Family from a Cleveland Clinic Pharmacy)
No No
Member % Co-insurance
Cleveland Clinic Pharmacies:
up to 90-Day Supply
15% 25% 45% 20%
Member Pays
100% of the
Discounted Price
Not Available
through Rx Plan
Member % Co-insurance
CVS Store Pharmacies:
30-Day Supply
Mail Service Program:
90-Day Supply
20% 30% 50% 20%
Member Pays
100% of the
Discounted Price
Not Available
through Rx Plan
Cleveland Clinic Pharmacies
including Specialty & Home
Delivery:
Is there a Minimum or Maximum to
the Rx % Co-insurance?
Yes
$3 Minimum/
$50 Maximum
per Month Supply
Yes
$3 Minimum/
$50 Maximum
per Month Supply
No
Yes
No Minimum/
$50 Maximum
per Month Supply
No No
Retail Pharmacies:
Is there a Minimum or Maximum to
the Rx % Co-insurance?
Yes
$5 Minimum/
$50 Maximum
per Month Supply
Yes
$5 Minimum/
$50 Maximum
per Month Supply
No N/A No No
CVS/caremark Mail Service
Program:
Is there a Minimum or Maximum to
the Rx % Co-insurance?
Yes
$15 Minimum/
$150 Maximum
90-Day Supply
Yes
$15 Minimum/
$150 Maximum
90-Day Supply
No
Yes
No Minimum/
$100 Maximum
per Month Supply
No No
Is there an Annual
Out-of-pocket Maximum?
After Deductible Has Been Met: $3,950 Individual / $7,900 Family
Combined Maximums for Retail, Specialty and Home Delivery
No No
Components of
Each Category
Brand Name
Drugs
See the
EHP Prescription
Drug Benet
Formulary
Specialty Drugs
6,7
Complete list of
Specialty Drugs
and Copay
Card Assistance
Program in the
EHP Prescription
Drug Benet
Formulary
Lifestyle Drugs
See the
EHP Prescription
Drug Benet
Formulary
Over-the-Counter
Drugs
See the
EHP Prescription
Drug Benet
Formulary
Pre-certication Required
See the EHP Prescription Drug Benet Formulary for list of pharmaceuticals
requiring precertication
No N/A
Diabetic Supplies
8
Asthma Delivery Devices
8
and Prescription Vitamins
9
Co-insurance 20% No No N/A
Pharmacies
10
in the Retail
Network
Cleveland Clinic Pharmacies ClevelandClinic Specialty Pharmacy, Cleveland Clinic Home Delivery Pharmacy, CVS store
pharmacies (including CVS pharmacieslocated in Target stores), CVS/caremark Mail Service, CVS/specialty Pharmacy
Note: Benet Program includes: generic oral contraceptives – covered for Marymount and Mercy Hospital
caregivers for clinical appropriateness only under the HBP.
6. Certain specialty medications are included in the Copay Card Assistance Program. Please refer to the
Prescription Drug Formulary Handbook.
7. There are 3 options for obtaining medications in the category listed above. The options are: 1. Cleveland
Clinic Pharmacies, 2. Cleveland Clinic Specialty Pharmacy, and 3. CVS/caremark Specialty Drug Program.
Specialty Drug prescription orders (rst ll and rells) are limited to a one month supply.
8. Diabetic Supplies – All diabetic supplies covered, except for most insulin pumps and insulin pump
supplies (with the exception of Omnipod Dash), continuous glucose monitors (with the exception of FreeStyle
Libre products), and continuous glucose monitor supplies (which are covered under the medical benet).
Diabetic supplies covered under the prescription drug benet include: needles purchased separately, test
strips, lancets, glucose meters, syringes, lancing devices, injection pens, FreeStyle Libre products, and
Omnipod Dash. Members with type 1 diabetes who are under 18 years of age will have no out-of-pocket
expense for their insulins and diabetic supplies covered under the prescription drug benet. Asthma Delivery
Devices – Includes spacers used with asthma inhalers.
9. Refers to vitamins that require a prescription from your healthcare provider.
10. Members can use any Cleveland Clinic pharmacy or any CVS store pharmacy for obtaining acute care
medications (e.g. single course of antibiotic therapy) and for the rst ll of maintenance medications
but must use a Cleveland Clinic Pharmacy or CVS/caremark Mail Service Program for all maintenance
medications.
10
MY HEALTH
Dental Plan Options
There are four dental plan options administered by Cigna.
Cigna Dental HMO
• Narrowest network – you can only utilize Cigna HMO providers such as Aspen Dental, Hudec Dental and Bright Now.
Cleveland Clinic and Mercy dental providers are not included in this plan.
• Includes coverage for routine cleanings/x-rays, restorative care and adult/child orthodontia
Preventive Dental Plan
• Includes coverage for routine cleanings/x-rays and minor restorative care such as llings
• Does not cover major restorative care or orthodontia
Traditional Dental Plan
• Includes coverage for routine cleanings/x-rays, minor/major restorative care and child orthodontia
(up to age 23)
• Most popular plan for Cleveland Clinic caregivers
Enhanced Dental Plan
• Includes coverage for routine cleanings/x-rays, minor/major restorative care and adult/child orthodontia
• Highest annual maximum benet
Costs for each plan can be found on page 22. Summary Plan Descriptions with complete details are available on the ONE
HR Portal. A directory of Cigna providers can be found at www.cigna.com or by calling 800.244.6224. The following chart
highlights some of the services covered under each dental plan.
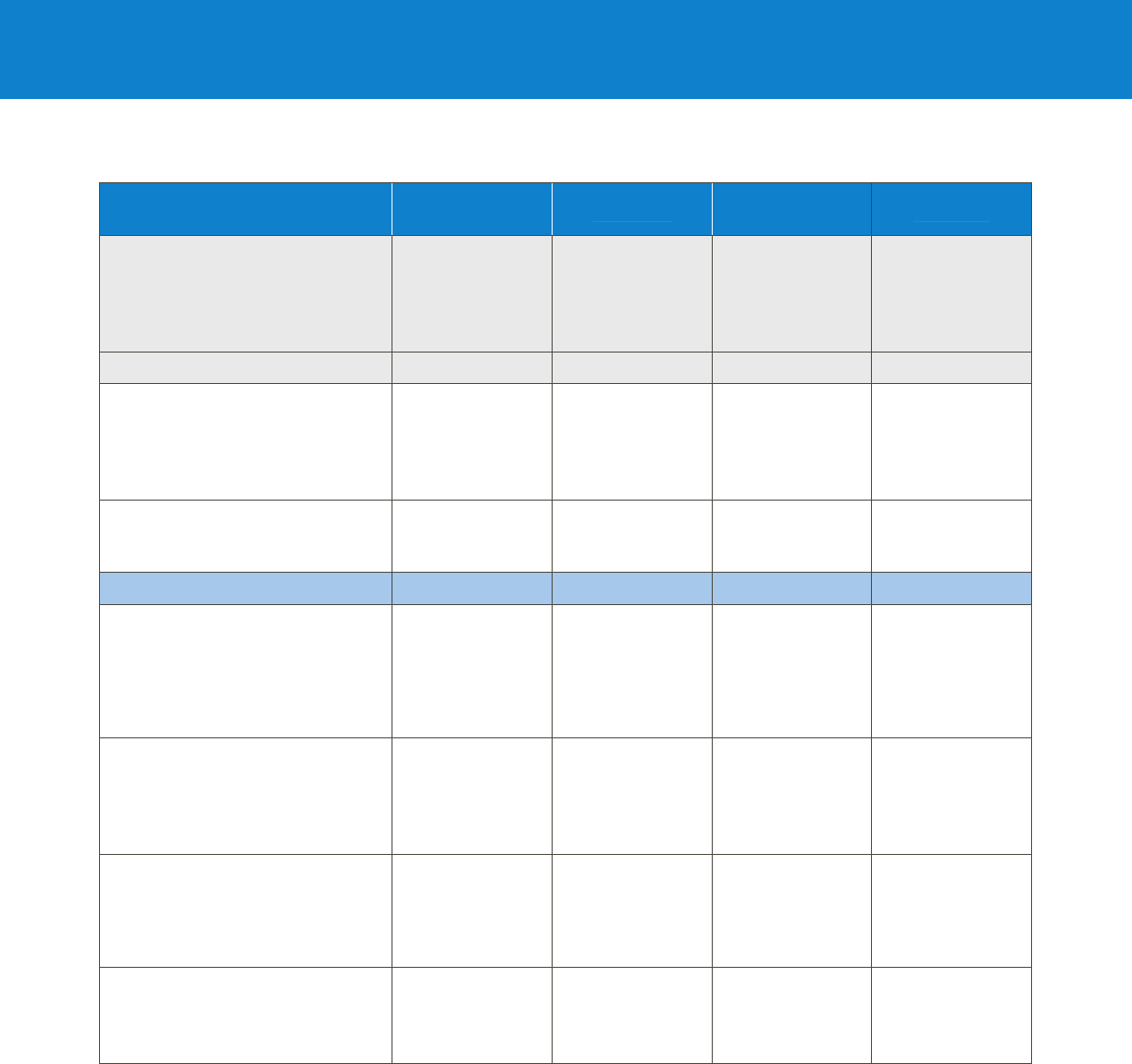
11
HMO
1
Preventive Traditional Enhanced
Network
Cigna Dental
HMO Providers
(e.g., Aspen,
Hudec, Bright
Now)
Total Cigna DPPO
Providers
Cigna DPPO
Advantage and
Cigna DPPO
Providers
Total Cigna
DPPO Providers
Out of Network Coverage None Yes
2
Yes
2
Yes
2
Calendar Year Maximum Benet None $500
$1,250 Cigna
DPPO Advantage
Providers
$1,000 all other
providers
$1,500
Annual Deductible
Individual
Family
None $50
$150
$50
$150
$50
$150
SERVICES Your Charge Plan Pays Plan Pays Plan Pays
Preventive and Diagnostic Care
Oral Exams
Routine Cleanings
X-Rays
Fluoride Application
Sealants
$0
$0
$0
$0
$12/tooth
100% 100% 100%
Basic Restorative Care
3
Fillings – Amalgam
Simple Extractions
$0
$12–$115
80%
80% Cigna
DPPO Advantage
providers
70% all other
providers
80%
Major Restorative Care
3
Crowns
Dentures
Bridges
Inlays/Onlays
$150–$490/tooth
$625–$715
$150–$470/tooth
$150–$470/tooth
Not covered 50% 60%
Orthodontia
3
Adults – $2,376
Children under 19
– $2,040
Not covered
50%
$1,250 max
covered for
children to age 23
80%
$2,500 max
covered for
children & adults
1. This grid is a sample of services covered under the Cigna Dental HMO Benet Program. For a complete list of all services you will need
to review the Cigna Dental Care Patient Charge Schedule. You can nd this on the ONE HR Portal which is accessed through Workday.
2. Out of network claims are reimbursed based on reasonable and customary fees, which may result in your costs being higher than if you
go to a CIGNA DPPO provider.
3. Subject to annual deductible.
MY HEALTH
Dental Plan Options
12
MY HEALTH
Vision Plan Options
There are two vision plan options administered by EyeMed. The Basic and Enhanced Vision Plans provide a benet for either
eyeglasses (frames & lenses) or contact lenses once per calendar year. Additional eyewear can be purchased at a discount.
Benets under each plan are maximized when EyeMed Access Network providers are used. A full directory of providers can
be found at www.eyemedvisioncare.com. The following chart highlights benets under each vision plan. Visit the ONE HR
Portal for additional details. Costs for each plan can be found on page 22.
Note: EyeMed Vision Plans cover materials only; coverage for an eye exam is included in the EHP if enrolled.
BASIC VISION PLAN ENHANCED VISION PLAN
In-Network
Member Cost
Out-of-Network
Member
Reimbursement
In-Network
Member Cost
Out-of-Network
Member
Reimbursement
FRAME $0 copay; 20% off
balance over $130
allowance
Up to $35
$0 copay; 20% off
balance over $180
allowance
Up to $65
STANDARD PLASTIC LENSES
Single Vision
Bifocal
Trifocal
Progressive – Standard
Progressive – Premium Tier 1–4
$0 copay
$0 copay
$0 copay
$65 copay
$85–175 copay
Up to $25
Up to $40
Up to $55
Up to $40
Up to $40
$0 copay
$0 copay
$0 copay
$10 copay
$85–175 copay
Up to $25
Up to $40
Up to $55
Up to $40
Up to $40
LENS OPTIONS
Anti Reective Coating:
Standard
Premium Tier 1–2
Premium Tier 3
Photochromic – Non-Glass
Polycarbonate – Standard
Scratch Coating – Standard Plastic
Tint – Solid or Gradient
UV treatment
All Other Lens Options
$45
$57–68
20% off retail price
20% off retail price
$40 ($0 if
< 19 yrs of age)
$0 copay
$15
$15
20% off retail price
Not covered
Not covered
Not covered
Not covered
Up to $20
Up to $8
Not covered
Not covered
Not covered
$0 copay
$12–23
20% off retail price
20% off retail price
$0 copay
$0 copay
$0 copay
$0 copay
20% off retail price
Up to $23
Up to $23
Not covered
Not covered
Up to $20
Up to $8
Up to $8
Up to $8
Not covered
CONTACT LENSES
Contacts – Conventional
Contacts – Disposable
Contacts – Medically Necessary
$0 copay; 15% off
balance over $130
allowance
$0 copay; 100% of
balance over $130
allowance
$0 copay; paid in full
Up to $70
Up to $70
Up to $70
$0 copay; 15% off
balance over $180
allowance
$0 copay; 100% of
balance over $180
allowance
$0 copay; paid in full
Up to $104
Up to $104
Up to $200

13
MY HEALTH
Disability
Cleveland Clinic provides and fully pays for a group long-term disability policy for all clinical trainees appointed through the
Graduate Medical Education Department. The plan covers 70% of salary, to a $3,000 maximum monthly benet. A benet
is paid after you are disabled for 90 days and will continue for the length of the total disability until Social Security normal
retirement age. There is no health exam required for this coverage nor are pre-existing conditions excluded from the policy.
The plan includes partial disability benets, survivor benets, a loan payout benet of $100,000 and a delayed cost of living
benet. The insurance is provided at no cost to the clinical trainee with premiums paid by Cleveland Clinic. Enrollment in the
program is automatic with coverage beginning on the rst day of employment.
As a Cleveland Clinic GME trainee, you also have the unique opportunity to supplement your group long-term disability with
an individual disability policy. This opportunity is medically guaranteed and requires no health questions or medical exams.
The Guaranteed Standard Issue (GSI) program allows you to apply for up to $7,500 of monthly benet with future increases
up to $10,000 and protects you in your specialty with strong enhanced true own occupation contractual language. The
GSI also provides a student loan protection option and the policy and its discounts are fully portable once you leave your
Cleveland Clinic training program. You have the option to enroll in the GSI program any time during your training, or up to
six months after. For more information or questions, please contact:
Amy P. Dickenson Rory Bixel Lough
Dickenson & Associates, LLC. Arthur J. Gallagher & Co.
440.505.6007 440.974.4040
14
MY MONEY
Life Insurance
Cleveland Clinic provides a $25,000 group term life insurance benet at no cost. You are automatically enrolled on your
start date.
Life Insurance Beneciary Designations
Beneciary designations are made on MedMutual Life’s web portal, which can be accessed in Workday by clicking the
Benets link, then clicking the MedMutual Life Beneciary Designation option under the External Links heading. A job aid
is posted on the ONE HR Portal to walk you through the process.
Loan Program
An emergency loan fund is available for clinical trainees, not to exceed $2,400. Outstanding loans must be paid in full
before a new loan may be requested. Loans must be paid in full when clinical trainees leave the Cleveland Clinic. Loan
Repayment Options:
1. 6 months: 12 equal payments (up to $200/pay for a $,2400 loan)
2. 1 year: 24 equal payments (up to $100/pay for a $2,400 loan)
3. 2 years: 48 equal payments (up to $50/pay for a $2,400 loan)
4. 2 years with deferral: 1st year payment deferred, 2nd year 24 equal payments (up to $100/pay for a $2,400 loan)
Please contact Graduate Medical Education (meded@ccf.org or 216.444.5690) for additional information and application.
On Call Meals
Clinical trainees that are in programs that require them to be on in-house overnight call are provided an on-call meal
allowance. This does not include trainees taking call from home. In order to use the on-call meal allowance you must complete
the Cleveland Clinic Payroll Deduction Food Purchase Authorization Form. Cleveland Clinic uses a debit system; funds will be
loaded on your ID Badge in six month increments based on projected number of calls designated by your program.
Retirement Program
Caregivers are automatically enrolled in the Savings & Investment Plan (SIP) managed by Fidelity Investments:
The SIP is funded with your own pre-tax, Roth, and/or after-tax contributions. All newly hired and newly eligible caregivers
will be automatically enrolled to contribute 3% of pay on a pre-tax basis 31 days after their start date. You can change
or stop your contribution percentage at any time online at www.netbenets.com/clevelandclinic or by calling Fidelity at
888.388.2247. In 2023 you can contribute up to $22,500 on a pre-tax or Roth basis (up to $30,000 if age 50 or older).
Contributions to the SIP are invested in a default target date fund based on your age. You can change your investment
allocations at any time on Fidelity’s website (www.netbenets.com/clevelandclinic).
Assistance in Managing Your Retirement Accounts
To support your nancial well-being, Fidelity representatives are available to discuss your retirement program at no cost.
They can translate all the “nancial lingo” to help you understand your choices and create a plan for saving. To schedule
time with a representative, visit www.netbenets.com/clevelandclinic or call 866.715.2059.
15
MY MONEY
Travel Benet
Cleveland Clinic strongly encourages their clinical trainees to participate in scholarly/research activities; these activities are
mandatory in many training programs. The Education Institute with the recommendation of the Graduate Medical Education
Council (GMEC) has set aside funds to allow trainees in accredited programs at a PGY-2 level or above to attend academic
meetings for the purpose of presenting or engaging in leadership roles within national societies.
Eligibility for individual trips will be determined by each program director after reviewing the meeting for educational value
and the presentation for content. In addition, the trainee must be listed as rst author on the poster or presentation and be
the “presenter”. Trainees who meet the above criteria will qualify for one annual Education Institute sponsored trip with a
maximum reimbursement of $1,500.00.
Uniform Information
Monogrammed lab coats and OR scrubs are provided to clinical trainees and laundered by Cleveland Clinic.
Voluntary Benet Programs
Cleveland Clinic offers voluntary benets to provide choices that cover as many of your life needs as we can. Identity
protection, legal, auto, home and pet insurance help reduce the nancial risk of unexpected events. Details can be found on
the ONE HR Portal. If you enroll in these programs premiums will be deducted from each paycheck.
To learn more scan the QR code below
MetLife Auto & Home
With MetLife Auto & Home
®
, you can get insurance tailored to your needs and access to special savings and benets you
won’t nd anywhere else. Caregivers can enroll in this program at any time during the year.
Auto Insurance
With custom t coverages, you can drive your own auto insurance policy, while enjoying savings and benets like:
• Special group discounts
• Automated payment options
• Claim-free driving rewards
• Car rental
• No deductible windshield repair
• Roadside assistance
• Guaranteed auto repairs for covered losses
16
MY MONEY
Home Insurance
4
Quality home insurance coverage means you can rest easy knowing your most valuable asset is truly protected, along with
savings and benets, like:
• Special group discounts
• Replacement cost coverage
• Referral networks
• Automated payment options
MetLife Pet Insurance
Every individual and their pet have unique needs. MetLife pet insurance provides exible coverage with up to 100%
reimbursement and the freedom to visit any U.S. licensed vet, optional Preventive Care coverage, 24/7 access to Telehealth
Concierge Services, and discounts and offers on pet care. Some limitations apply; refer to MetLife product overview on the
ONE HR Portal. Caregivers can enroll in this program at any time during the year.
To get a quote or enroll in auto, home or pet insurance, visit https://www.metlife.com/info/cleveland-clinic/, call 1.800.GET.
MET8, or scan the QR code below.
MetLife Legal Plan
MetLaw is an affordable, easy-to-use plan that offers you and your family value and comfort in knowing you can access
legal services for almost all personal legal matters. You can have a team of top attorneys ready to help you take care of
life’s planned and unplanned legal events – for a at monthly fee. The plan provides coverage for you, your spouse/domestic
partner and dependent children. You can also elect to provide coverage for parents and parents-in-law.
Covered services include
5
• Estate planning documents, including Wills and Trusts
• Real estate matters
• Financial matters, such as debt collection defense
• Trafc offenses
• Document review and preparation
• Family law, including adoption and name change
• Advice and consultation on personal legal matters
• Divorce, Custody Order
• Enforcement or Modication of Support Order
• Reproductive Assistance Law (20 hours)
• Habeas Corpus, Misdemeanor Defense
• Insurance Claims, Tax Preparation
• LifeStages Identity Restoration Services
• Eight hours of network attorney time and services for
non-covered matters
4. Home insurance has limited availability in the state of MA and is not available in the state of FL.
5. Some limitations apply; refer to MetLife product overview on the ONE HR Portal.

17
MY MONEY
Allstate Identity Protection
Allstate Identity Protection delivers comprehensive fraud monitoring and powerful mobile and desktop cybersecurity to help
protect you, your family, and your nances from emerging threats. Family members are covered under the program if they
are dependent on you nancially or live in your home (including parents, in-laws and grandparents age 65+). Should fraud
or identity theft occur, Allstate’s highly-trained and certied experts are available 24/7 to handle and remediate every type of
identity fraud case and fully manage restoration cases.
Covered services include:
• Allstate Digital Footprint
SM
• Comprehensive identity and credit monitoring
• Dark web monitoring
• Financial transaction monitoring
• Social media monitoring
• Data breach notications
• Remediation of pre-existing identity theft covered at no
additional cost
• Mobile safe browsing and phishing protection
• Wi-Fi network scan and alerts
• Mobile device locator and theft alerts
• Coverage available for family
• Full service, U.S.-based remediation support
• Stolen fund reimbursement
• Tax fraud refund advance
• 401(k) and HSA reimbursement
• Up to $1 million identity theft expense reimbursement
Trustmark Long-Term Care Insurance
Long-term care (LTC) planning is an important aspect of a personal nancial plan. LTC services are not covered by your
health insurance, disability insurance, or Medicare. Today, the average cost of home health care is around $43,000/year or
more.
6
Trustmark’s LTC benets help protect your retirement savings, ease the burden of caregiving by your loved ones, and
allow you to choose the setting where you receive care.
The Trustmark program offers two benets in one policy:
1. Permanent life insurance protection for your family, and
2. Long-term care protection if you happen to need care.
Benets are payable as long as your coverage is active and premiums are paid up.
With this program:
• You choose a life insurance benet up to $200,000
• You can access 4% of the selected life insurance benet per month if you need covered LTC services
• The LTC benet keeps paying up to twice the life insurance benet if you continue to need care
• A death benet is payable to a beneciary even if you access your LTC benets
Example: If you select a life insurance benet of $50,000, your monthly LTC benet would be $2,000 (4% of $50,000) and
your maximum LTC benet is $100,000.
A special enrollment period is tentatively planned for August 2023 whereby eligible caregivers will be offered guaranteed
acceptance (which means you cannot be turned down because of your health). Watch for communications this summer.
6. US Department of Health & Human Services

18
MY MONEY
Flexible Spending Accounts
Cleveland Clinic offers two distinct exible spending accounts (FSAs) administered by Payex:
1. Healthcare FSA – used to pay for eligible out-of-pocket healthcare-related expenses for you and your dependents with
pre-tax dollars.
2. Dependent Care FSA – used to pay for eligible out-of-pocket childcare and/or adult daycare-related expenses for your
dependents with pre-tax dollars.
Healthcare FSA
• Minimum election of $100 (if you choose to enroll) up to a maximum election of $3,050 in 2023
• Your account will come preloaded with the amount you elect and can be spent right away
• Payex will issue a debit card that you can use to pay for qualied out-of-pocket expenses
• You should save receipts and Explanation of Benet (EOB) statements for qualied purchases in case Payex needs to
verify the eligibility of your expenses
Dependent Care FSA
• Minimum election of $100 (if you choose to enroll) up to a maximum election of $5,000 (if your salary is $135,000 or
higher, the maximum annual election is $1,500)
• Your account is funded through payroll deduction deposits (the account is not preloaded with your full annual election)
A full listing of eligible expense items under the Healthcare and Dependent Care FSAs can be found at www.payex.com.
Reimbursement Deadline
Eligible expenses must be incurred during the plan year and subsequent grace period. The plan year is January 1, 2023 (or
the effective date of your enrollment as a new hire or due to a life event change, if later) through December 31, 2023 (or
the date your employment terminates, if earlier). The grace period runs from January 1, 2024 through March 15, 2024.
Expenses incurred during the plan year and subsequent grace period must be submitted to PayFlex for reimbursement
by April 30, 2024. This is referred to as the “run-out period”. This means that expenses incurred from January 1, 2023
through March 15, 2024 (or your termination date, if earlier) must be submitted to PayFlex for reimbursement by April 30,
2024, otherwise they will be denied.
You must re-enroll in the FSAs each year during annual open enrollment as your annual election will revert back to $0 at the
end of each calendar year.
19
MY WELL-BEING
Well-Being Programs
Cleveland Clinic is committed to offering opportunities to improve your holistic well-being and provides access to resources
available to all caregivers along the Physical, Emotional, Financial, Making Connections, and Lifelong Learning dimensions.
A full spectrum of programs aim at helping our caregivers achieve fulllment, live healthier lifestyles and improve quality of
life. Additional information on these programs can be found on the ONE HR Portal accessed through Workday and on the
Caregiver Well-Being site in Connect Today. The Caregiver Well-Being Connect Today site is accessible whether you are on or
off-site. Connect via your personal mobile device (use QR code) or computer (use web address). No need for a CCF device or
network connection!
Employee Assistance Program
Cleveland Clinic offers a full-service employee assistance program (EAP) dedicated to providing resources and support for
caregivers are facing challenging issues both inside and outside of the workplace. These services are provided at no cost to
the caregiver and can assist with items such as:
• Work problems
• Family issues
• Emotional problems
• Alcohol and drug use
• Legal matters
• Marital problems
• Parenting issues
• Loss/bereavement
• Financial pressures
Additional information can be found on the Connect Today site at https://ccf.jiveon.com/community/caring-for-caregivers or
on the ONE HR Portal which can be accessed through Workday.
Adoption Assistance
Cleveland Clinic provides nancial assistance of up to $5,000 for a legal adoption ($10,000 lifetime maximum benet).
Caregivers must be employed for 12 months to become eligible. Additional information can be found on the ONE HR Portal
which can be accessed through Workday.
Bereavement Leave
Employees are eligible for three (3) bereavement days for a death in the immediate family.

20
MY WELL-BEING
Maternity and Parental Leave
Cleveland Clinic provides caregivers with paid maternity and parental leave:
• 100% pay for 8 weeks of maternity leave for mothers following childbirth
• 100% pay for 4 weeks of parental leave for both parents following the birth or adoption of a child
Caregivers are eligible for this benet effective upon their hire date. For additional information please visit the ONE HR Portal
accessed in Workday (www.ccf.org/onehr).
Medical Leave of Absence
If a clinical trainee is temporarily unable to work due to illness or accident as determined by their primary care physician and
is unable to carry on duties and responsibilities as required in the training program, salary and benets will continue for 90
days, the duration of the illness or the remainder of the contract; whichever is shorter. If the illness continues and the clinical
trainee holds a valid appointment he/she will continue to receive Cleveland Clinic benets; however, in lieu of a salary they
will receive payments from the disability plan.
Military Leave of Absence (FMLA)
Pursuant to the Family and Medical Leave Act (FMLA), Cleveland Clinic allows eligible employees time off from work for up
to 12 weeks in a leave year, due to any qualifying exigency arising out of the fact that the employee’s spouse, son, daughter
or parent is a covered military member on active duty (or has been called to active duty) in support of a contingency
operation and allow eligible employees up to 26 weeks in a single leave year to care for a covered service member with a
serious injury or illness if the employee is the spouse, son, daughter, parent or next of kin of the service member.
Paid Personal Days
Trainees are eligible for up to 5 personal days per year. Personal days can be used for taking board or USMLE exams, when
too ill to work or as interview days. Personal days should be requested in advance whenever possible. Please refer to your
specic program’s time away policy for additional information.
Personal Leave
It is the policy of the Cleveland Clinic to grant residents and fellows a leave of absence (without pay) for urgent or emergency
situations that personally affect the trainee and cannot be handled in any other way. Program Directors have the nal
approval for all personal leave of absence requests.
Vacation Days
Residents and fellows are given three weeks (15 working days) of vacation per academic year.

21
MY WELL-BEING
Caregiver Leave
Cleveland Clinic provides trainees with up to 6 weeks paid caregiver leave over the course of their training program to care
for an immediate family member (i.e., spouse, child, or parent) with a serious health condition. Trainees are eligible for this
benet effective upon their hire date
Healthy Choice Program
7
The Healthy Choice Program is a voluntary premium discount program from the Employee Health Plan (EHP) that rewards
you for taking action to manage your health. The program also provides resources to help you save on health care costs and
support your overall wellbeing. When you participate and meet your goals, you’ll become eligible for big savings on your
health plan premiums – up to 30%. Have a spouse on your health plan? They can participate too, and together you could
achieve your best discount.
The program begins each year in January. To get started, you’ll need to create your personalized Healthy Choice portal
account so that you can view your health status, submit some health information and follow your personal program
requirements. If you join and participate for at least six months and achieve all of your goals by the nal deadline, you’ll
be eligible for a discount the following year.
For your convenience, you can download the EHP Healthy Choice app right to your phone for quick, easy access to all your
information. Your portal account is a critical tool to help you stay on track and meet your goals. Don’t have an account? Use
your health plan ID and date of birth to create your account and login. You can nd more information about the Healthy
Choice Program by visiting employeehealthplan.clevelandclinic.org or by scanning the Healthy Choice QR code below.
7. As a resident/fellow you are not eligible for Healthy Choice premium discounts as you are already receiving a signicant health plan
premium discount (you pay half of the bronze full-time rate). However, if you were to be promoted to a staff position in the following
calendar year your successful participation in the Healthy Choice Program this year could allow you to receive discounted health plan
premiums upon your appointment to the professional staff.
22
BENEFIT COSTS
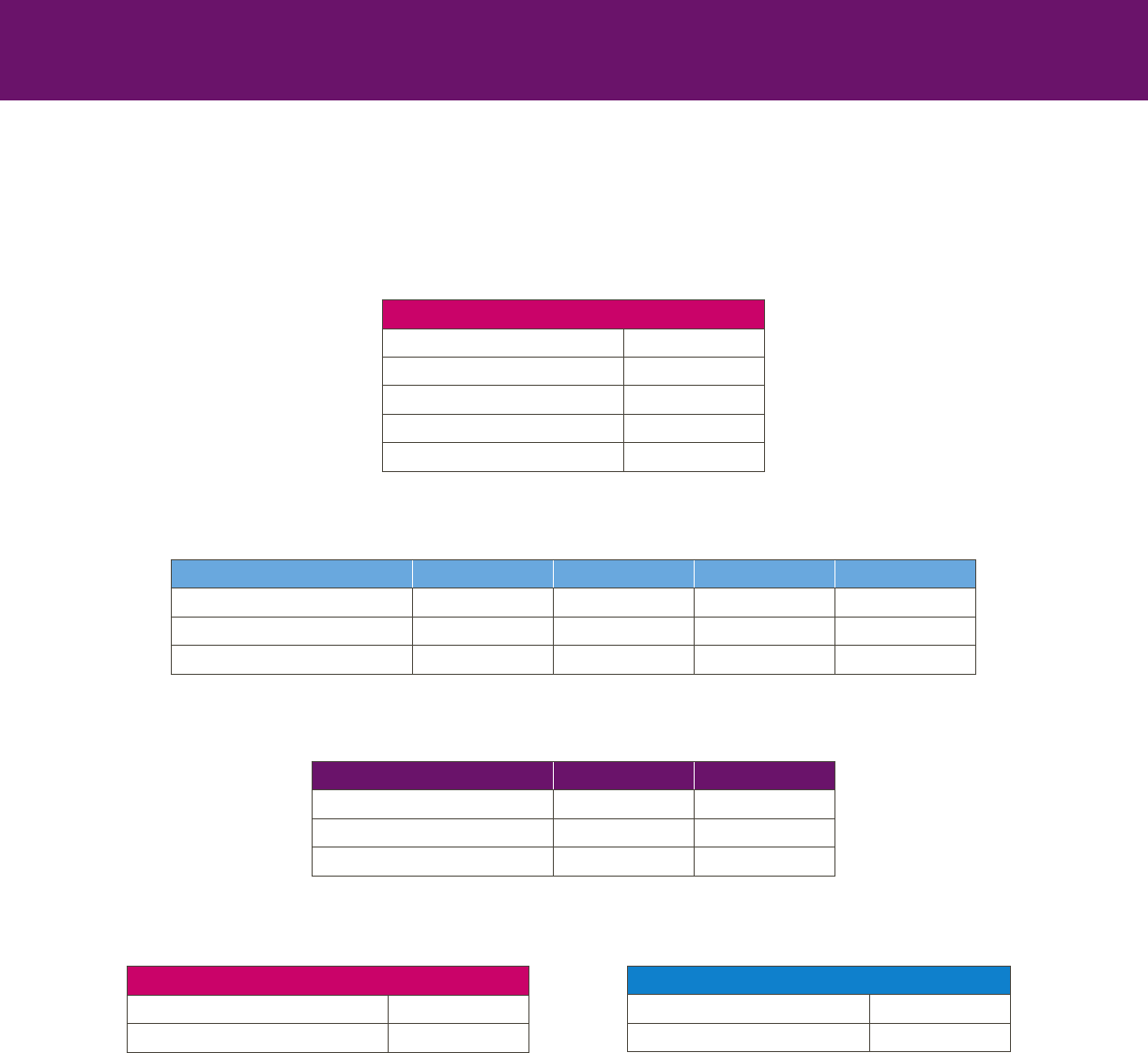
* After completing one year of service, DHMO, Preventive and Traditional plans are fully paid by department. If Enhanced is elected,
employee pays difference between Enhanced and Traditional.
2023 Benet Costs Per Paycheck
Semi-Monthly (24 pays per year)
EHP (PRE-TAX)
Employee Only $36.58
Employee + Child $66.50
Employee + Spouse $86.79
Family I (2-3 Dependents) $109.67
Family II (4+ Dependents) $121.54
DENTAL PLANS* (PRE-TAX)
DHMO Preventive Traditional Enhanced
Employee Only $6.00 $7.38 $10.83 $14.79
Employee + 1 $9.88 $12.33 $21.88 $31.38
Employee + Family $17.04 $21.58 $36.54 $52.96
VISION PLANS (PRE-TAX)
Basic Enhanced
Employee Only $2.42 $5.38
Employee + 1 $4.88 $10.71
Employee + Family $6.71 $14.75
METLIFE LEGAL (POST-TAX)
Employee + Family $7.65
Employee + Family + Parents $10.15
ALLSTATE IDENTITY PROTECTION (POST-TAX)
Employee Only $3.38
Employee + Family $6.38
23
Terms and Denitions
General
FTE: This means “full-time equivalent” and is used to describe your employment status. If you work 100% full-time, your
employment status is 1.0 FTE. If you work 50% time, your employment status is 0.5 FTE.
PRN: PRN stands for the Latin term “pro re nata” which means “as needed.” A “PRN” employee is an employee who is
utilized on an “as needed” basis.
Health, Dental and Vision Plans
Co-insurance: The percentage of the cost of covered charges that you are responsible to pay when coverage is less than
100%. For example, if a service is covered 80%, your co-insurance is 20% of the covered charges.
Co-payment, or Co-pay: A dollar amount that you are required to pay at the time you receive services.
Covered Charges: Charges for medical services or procedures that are covered by the health and dental plans.
Deductible: A dollar amount that you are responsible to pay each year before the benet plan will start to provide
reimbursement
Maximum Benet (Dental Plans): This is the maximum amount the dental plan pays for covered services each calendar
year.
Network Provider: A participating provider who has agreed to accept a contracted amount for covered services they provide
(after you pay the applicable co-payment or co-insurance). When you receive services from a network provider, you are not
responsible to pay any amount that exceeds the contracted rate.
Out-of-Pocket Maximum: This is the maximum amount of accrued co-pay and co-insurance amounts that you pay in a
calendar year.
Primary Care Providers (PCP): Physicians expert in providing diagnosis and treatment of illness and provision of preventive
care; they also serve as coordinators of the overall care of their patients.
Provider: A person or organization responsible for furnishing health, dental or vision services.
Reimbursement: This refers to the dollar amount paid by the benet plan.
Specialist, or Specialty Care Provider: A physician with expertise in a specic medical specialty or sub-specialty.
Retirement Programs
Pre-tax Contribution: A pre-tax contribution is one that is made before any taxes are paid on the amount. An advantage of
pre-tax contributions to your retirement accounts is that they can reduce your income taxes for the current year. You pay
income taxes on the contributions and earnings when you make withdrawals from your retirement account.
Roth Contribution: A Roth contribution is made to your retirement account with post-tax dollars. Earnings then grow tax-free.
When you make withdrawals from your account, you do not pay income taxes, since income taxes were already applied to
your contributions.
Target Date Fund: A mutual fund that mixes several different types of stocks, bonds and other investments to help you take
more risks when you’re young, and gradually get more conservative in your investment strategy as you approach retirement.
Vested: After meeting the vesting period, you have a non-forfeitable right to your full account balance, including any
employer contributions. (All of the money in your account belongs to you.)
Vesting Period: The amount of time you must work for Cleveland Clinic in order to become vested in your full account
balance, including any employer contributions.

24
Copyright (© 2022 Cleveland Clinic)
This summary is intended to provide a high level overview of Cleveland Clinic benet programs. By its nature, this is
not a legal document. Benet program details are covered in summary plan descriptions (SPDs) and controlling legal
documents. SPDs can be found on the ONE HR Portal, which can be accessed through Workday, or by contacting the
ONE HR Service Center at 216.448.2247. This summary does not create a contract between Cleveland Clinic and its
caregivers for either employment or any other benet program offered. Cleveland Clinic routinely reviews the benet
programs offered and has the right to change or terminate these offerings at its own discretion at any time.
