Inquest into the deaths of Kate Goodchild,
Luke Dorsett, Cindy Low & Roozbeh
Araghi at Dreamworld, October 2016
Findings and Recommendations
February 2020
CORONERS COURT OF
QUEENSLAND

CORONERS COURT OF QUEENSLAND
INQUEST INTO THE DEATHS OF KATE LOUISE GOODCHILD, LUKE
JONATHAN DORSETT, CINDY TONI LOW, & ROOZBEH ARAGHI
Coroner, Southern Region
Credit for the above photograph is given to Mr. Richard Gosling, Newspix

CORONERS COURT OF QUEENSLAND
FINDINGS OF INQUEST
CITATION: Inquest into the deaths of Kate Louise GOODCHILD,
Luke Jonathan DORSETT, Cindy Toni LOW, &
Roozbeh ARAGHI
TITLE OF COURT: Coroners Court
JURISDICTION: SOUTHPORT
FILE NO(s): 2016/4486, 2016/4485, 2016/4480, 2016/4482
DELIVERED ON: 24 February 2020
DELIVERED AT: BRISBANE
HEARING DATE(s): 18 June 2018 to 29 June 2018
8 October to 19 October 2018
12 November to 22 November 2018
6 & 7 December 2018
FINDINGS OF: James McDougall, Coroner
CATCHWORDS: Coroners: inquest, Dreamworld, amusement device,
Theme Park, safety management systems, ride
maintenance, training, amusement device
regulation, amusement device designer, amusement
device modification, external safety audits.
REPRESENTATION:
Counsel Assisting
Mr Ken Fleming, QC
Ms Rhiannon Helsen, CCoQ
Family of Cindy Low
Mr Matthew Hickey, Counsel instructed by Clayton Utz
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
i
Families of Kate Goodchild & Luke Dorsett
Mr Steven Wybrow, Counsel instructed by Aulich Civil
Law
Family of Roozbeh Araghi
Mr Toby Nielsen, Counsel instructed by Gordon & Barry
Law
Mrs Kim Dorsett (mother, Kate & Luke)
Mr Robert Davis, Counsel instructed by Sneddon, Hall &
Gallop Lawyers
Office of Industrial Relations (Workplace Health & Safety Queensland)
Mr Stephen Gray, Counsel instructed by Crown Law
Ms Courtney Williams
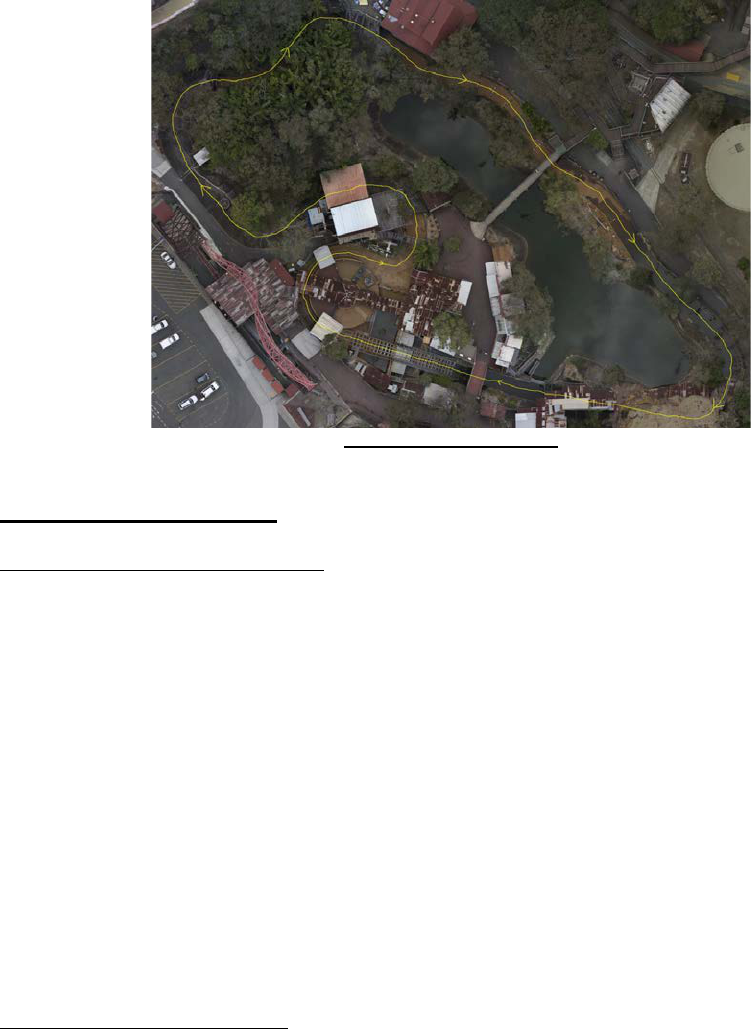
Mr Peter Callaghan SC, instructed by Gilshennan &
Luton
Ms Chloe Brix, Ms Sarah Cotter, Mr Wayne Cox,
Ms Amy Crisp, Mr Generic Cruz, Mr Francoire De Villiers,
Mr Christopher Deaves, Mr Quentin Dennis, Mr Andrew Fyfe,
Mr Peter Gardner, Mr Mark Gordon, Ms Nichola Horton,
Mr Jason Johns, Ms Jennie Knight, Mr John Lossie,
Mr Troy Margetts, Mr Steven Murphy, Mr Grant Naumann,
Mr Peter Nemeth, Mr Kamlesh Prasad, Mr Scott Ritchie,
Mr Matthew Robertson, Mr Michael Stead,
Mr Mark Watkins, Mr Timothy Williams, Mr Jacob Wilson
Mr Ralph Devlin QC & Mr Liam Dollar, Counsel
instructed by K & L Gates LLP
Ardent Leisure Ltd trading as Dreamworld
Mr Bruce Hodkinson QC & Mr James Bell QC, instructed
by Baker McKenzie Lawyers & DWF (Australia)
CEO, Dreamworld, Craig Davidson
Mr Gavin Handran, Counsel instructed by Quinn,
Emanuel, Urquhardt & Sullivan LLP
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
ii
Queensland Police Service
Mr Adrian Braithwaite, Counsel instructed by QPU Legal
Group
DANFOSS Australia (Mr Eduardo Gie)
Mr Sean Farrell, Counsel instructed by Mills Oakley
Mr John Clark, Mr Shane Green, Mr Benjamin Hicks,
Mr Nigel Irwin, Ms Rebecca Ramsay, Mr Mark Thompson
Mr Anthony Harding, Counsel instructed by Rankin & Co
Lawyers
Mr Angus Hutchings
Mr Craig Eberhardt, Counsel instructed by Robertson
O’Gorman Solicitors
Mr Tom Polley (Danski Pty Ltd)
Ms Polina Kinchina, Counsel instructed by Colin,
Biggers, Paisley Lawyers
Mr Bob Tan
Mr John Bremhorst, Counsel instructed by Australian
Business Lawyers & Advisors
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
iii
CONTENTS
INTRODUCTION ....................................................................................................................... 6
ISSUES FOR INQUEST ............................................................................................................ 7
ABOUT THE DECEASED PERSONS ...................................................................................... 7
BRIEF SUMMARY OF THE INCIDENT .................................................................................... 8
POST MORTEM FINDINGS .................................................................................................... 10
Kate Goodchild .................................................................................................................... 10
Luke Dorsett ........................................................................................................................ 10
Cindy Low ............................................................................................................................ 10
Roozbeh Araghi ................................................................................................................... 10
DREAMWORLD STRUCTURE & OVERVIEW ...................................................................... 11
THUNDER RIVER RAPIDS RIDE (TRRR) ............................................................................. 15
Configuration of the TRRR .................................................................................................. 16
Forensic Crash Unit Investigation .................................................................................................. 16
Configuration of the TRRR at the Time of the Incident .................................................................. 17
Operating Control System ............................................................................................................. 17
Trough ........................................................................................................................................... 18
Raft Supporting Rails ..................................................................................................................... 18
Conveyor System .......................................................................................................................... 19
Water Pumps ................................................................................................................................. 21
Rafts .............................................................................................................................................. 22
Pneumatic Gates ........................................................................................................................... 23
Safety Features of the TRRR .............................................................................................. 24
Emergency Stops (E-Stops) .......................................................................................................... 24
Raft Safety Stop ............................................................................................................................ 25
Chain Break Safety........................................................................................................................ 25
Anti-Roll Back Gates ..................................................................................................................... 25
Water levels ................................................................................................................................... 25
History & Modifications to the TRRR Since 1986................................................................ 25
Issues with the Conveyor and Removal of Slats ........................................................................... 26
Turntable Removal ........................................................................................................................ 28
Pumps ........................................................................................................................................... 29
Raft Collar Quote ........................................................................................................................... 30
General Feasible Improvements ................................................................................................... 31
Changes to the Unload Area ......................................................................................................... 31
Raft Track ...................................................................................................................................... 31
Conveyor Chain Break and Raft Slip Monitoring ........................................................................... 32
PFI Modifications to the Log Ride in 2013 ..................................................................................... 36
Other Suggested Modifications to the TRRR ...................................................................... 37
Automated Raft Rotation System .................................................................................................. 37
Single Button Shutdown ................................................................................................................ 38
Sourcing Further Wood for Conveyor in 2016 ............................................................................... 38
TRAINING & OPERATOR PROCEDURES ............................................................................ 39
TRRR Position Responsibilities and Training ..................................................................... 41
Ride Operator Level 1 (No. 3) Deckhand ...................................................................................... 43
Ride Operator Level 2 (No. 2) Load Operation .............................................................................. 45
Ride Operator Level 3 (No. 1) ....................................................................................................... 51
Memorandums for the TRRR .............................................................................................. 55
12 February 2016 .......................................................................................................................... 56
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 1 of 274
29 May 2016 .................................................................................................................................. 57
18
October 2016 ............................................................................................................................ 57
Pre-ride Checks on the TRRR............................................................................................. 58
Emergency Scenario Training ............................................................................................. 59
PAST INCIDENTS ON THE TRRR ......................................................................................... 60
18 January 2001 – H101/0019 – Property Damage ........................................................... 60
Incident Report .............................................................................................................................. 61
Recommendations ........................................................................................................................ 63
Comments About the Incident ....................................................................................................... 63
7 October 2004 .................................................................................................................... 63
Further Consideration and Implementation of the Recommendations by Dreamworld .................. 65
Comments about the Incident ........................................................................................................ 67
28 August 2005 ................................................................................................................... 67
26 February 2008 ................................................................................................................ 68
6 November 2014 – ‘The BUSS Incident’ ........................................................................... 69
13 November 2014 - Bob Tan Email to Leadership Team .................................................. 71
Further Incidents Recorded in Log Reports ........................................................................ 72
DREAMWORLD SAFETY DEPARTMENT ............................................................................. 73
Figtree Reporting System .................................................................................................... 75
TRRR Risk Assessments .................................................................................................... 75
ENGINEERING & TECHNICAL (E&T) DEPARTMENT ......................................................... 78
Safety Issues Identified by E&T Staff .................................................................................. 80
Training for E&T Department Staff ...................................................................................... 81
Role of Junior Engineer ....................................................................................................... 81
Mr. Bob Tan’s Role .............................................................................................................. 82
E&T Department Knowledge of the Design, Modifications and Incidents on the TRRR..... 84
RIDE MAINTENANCE AT DREAMWORLD ........................................................................... 86
Daily Inspection ................................................................................................................... 88
Daily Operator Pre Start Up and Post Operation Shutdown Sheets .............................................. 89
Breakdown Procedure ......................................................................................................... 89
Park Technician Procedure ................................................................................................. 91
TRRR YEARLY PREVENTATIVE MAINTENANCE INSPECTION ....................................... 93
Shutdown June 2016 ........................................................................................................... 93
RECENT BREAKDOWNS OF THE TRRR ............................................................................. 94
19
October 2016 .................................................................................................................. 94
22 October 2016 .................................................................................................................. 95
23 October 2016 .................................................................................................................. 96
Day of the Incident – 25 October 2016 ............................................................................... 97
TIMELINE OF EVENTS ON 25 OCTOBER 2016 ................................................................... 97
Immediate Response to the Tragic Incident ...................................................................... 109
Further Evidence from Ms. Williams ................................................................................. 110
Further Evidence of Mr. Nemeth ....................................................................................... 112
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 2 of 274
Discussion with QPS, OIR & Dreamworld Management on 25 October 2016 ................. 113
TECHNICAL CAUSE & CIRCUMSTANCES OF THE INCIDENT ....................................... 114
Plank Damage and Observations ..................................................................................... 118
Reconstruction of the Incident ........................................................................................... 118
FCU Investigation Findings as to Causation ..................................................................... 119
EARTH FAULT AND PUMP DRIVES EXAMINATION ........................................................ 122
History of VSDs at Dreamworld ......................................................................................... 122
Testing on drives post incident .......................................................................................... 123
Recommended Course of Action in Response to an Earth Fault ..................................... 125
Mr. Ritchie’s Assessment of the Fault Prior to the Tragic Incident ................................... 126
HISTORY OF EXTERNAL SAFETY AUDITS AT DREAMWORLD ..................................... 127
JAK Leisure Company Audits ............................................................................................ 127
May 2003 – Inspection ................................................................................................................ 130
November 2004 – Inspection ....................................................................................................... 132
July 2006 – Inspections ............................................................................................................... 135
September 2009 – Inspections .................................................................................................... 139
March 2013 – Inspections ........................................................................................................... 142
Comments about JAK / Ocean Embassy Safety Audits .............................................................. 144
DRA Safety Management Audits ...................................................................................... 147
February 2013 Audit .................................................................................................................... 148
2014 Audit ................................................................................................................................... 151
Consultancy Visits 2014 .............................................................................................................. 153
2015 Audit ................................................................................................................................... 153
Consultancy Visit - April 2015 ...................................................................................................... 154
Consultancy Visit - December 2015 ............................................................................................ 155
Consultancy Visit - April 2016 ...................................................................................................... 155
Dreamworld’s Response to DRA Audits ...................................................................................... 157
Dreamworld Safety Auditing Strategy FY15 ...................................................................... 157
CHANGES AT DREAMWORLD FOLLOWING THE INCIDENT .......................................... 159
AMUSEMENT PARK REGULATION IN QUEENSLAND .................................................... 161
Brief History of WHS Legislation - Past Decade ............................................................... 162
2011 WHS Act – Regulator Responsibilities ..................................................................... 162
Administrative Functions as of October 2016 ................................................................... 162
Plant Design Registration ............................................................................................................ 163
Plant Registration Renewal ......................................................................................................... 163
Safety Regulations for Plant ........................................................................................................ 164
Compliance Monitoring and Engagement ......................................................................... 168
Industry Guidance & Engagement Activity ........................................................................ 169
AALARA Forum ........................................................................................................................... 170
Annual Amusement Device Stakeholders Forum ........................................................................ 170
Functional Safety Forum ............................................................................................................. 170
Published Guidance Material ....................................................................................................... 170
Enforcement & Sanctions .................................................................................................. 171
Compliance Notices..................................................................................................................... 171
Investigations .............................................................................................................................. 172
Prosecutions ................................................................................................................................ 172
Regulatory Focus on Mobile Amusement Rides .......................................................................... 172
Previous Notifications Made to OIR in Relation to the TRRR by Dreamworld .................. 173
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 3 of 274
CLASS 2 RIDES INSPECTION & REGISTRATION ............................................................ 173
Dreamworld’s Compliance with the Requirement for Renewal of Plant Registration ....... 173
2016 Dreamworld Plant Registration ........................................................................................... 175
Certificate Issued for TRRR ......................................................................................................... 178
Draft Report for all Class 2 Rides ................................................................................................ 179
OIR INSPECTOR AUDITS OF DREAMWORLD PRIOR TO THE INCIDENT ..................... 181
OIR TECHNICAL ADVICE ABOUT THE INCIDENT ............................................................ 184
Technical Advice - Principal OIR Adviser (Mechanical), Mr. David Flatman .................... 184
Inspections and Testing ............................................................................................................... 184
Control Measures ........................................................................................................................ 187
Ride Modifications ....................................................................................................................... 188
Previous Incidents on TRRR ....................................................................................................... 189
Maintenance and Inspections ...................................................................................................... 189
Conclusions ................................................................................................................................. 190
Technical Advice - OIR Principal Inspector, Mr. Ian Stewart ............................................ 190
Issue 1 - Reliance on Administrative Control in Emergency Situations ....................................... 191
Issue 2: Limitations of the Ride Emergency Controls, Systems and Procedures Provided for the
Operator to Respond to Emergencies ......................................................................................... 193
Issue 3 - Monitoring and Prevent of Rafts Colliding in the Unloading Area ................................. 194
Issue 4 – Water Level Monitoring ................................................................................................ 194
Issue 5 – Gap at the End of the Conveyor at the Unloading Area ............................................... 195
PROHIBITION NOTICE – ARDENT LEISURE ..................................................................... 197
REGULATORY RESPONSE FOLLOWING THE INCIDENT ............................................... 198
2016 Audit Campaign ........................................................................................................ 198
2017 Audit Campaign ........................................................................................................ 199
Best Practice Review of OIR ............................................................................................. 200
OIR Plant Inspectors (Amusement Devices) Subgroup ............................................................... 202
Plant Item Registration Working Group ....................................................................................... 203
Amusement Devices Stakeholders and Regulators Forum ......................................................... 204
PROPOSED REGULATORY AMENDMENTS ..................................................................... 204
Draft Further Amendments to the Regulations .................................................................. 204
Major Amusement Parks and the Proposed Safety Case Licensing System ............................... 205
Mandatory Major Inspections of Amusement Devices ................................................................. 206
Operators of Amusement Devices ............................................................................................... 207
Amusement Device Log Books ................................................................................................... 207
Purpose of the New Proposed Safety Case Regime ........................................................ 208
INDUSTRY RESPONSE & INFORMATION ......................................................................... 209
Submission by the Safety Institute of Australia ................................................................. 209
OIR Response to SIA Submission .................................................................................... 211
VILLAGE ROAD SHOW SAFETY SYSTEMS ...................................................................... 214
EXPERT EVIDENCE ............................................................................................................. 217
Engineering Expert Advice ................................................................................................ 217
Report on the Design of the Conveyor System by Dr Frank W. Grigg, Forensic Engineering
Consulting Pty Ltd ....................................................................................................................... 217
Safety Related Control Systems, Summary Report 170326GRa, Expert Report by George
Rutherford, 26 March 2017 .......................................................................................................... 220
Report by Dr Duncan Gilmore, Managing Director and President of Gilmore Engineers Pty Ltd 222
ENGINEERING EXPERT CONCLAVE ................................................................................. 230
Joint Engineering Expert Advice ....................................................................................... 230
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 4 of 274
Expert’s Response to the Proposed Draft Regulations ..................................................... 247
Mr. Chan’s Response to the Expert Evidence .................................................................. 247
FURTHER EXPERT ADVICE ............................................................................................... 248
Human Factors Report on Fatal Incident, Professor Penelope Sanderson ...................... 248
Expert Report by Principal Naval Architect, Mr. Mark Devereaux .................................... 254
Dreamworld Ride Velcro Seatbelt Test, APV Engineering & Testing Service, Mr. Jose de
Freitas ................................................................................................................................ 255
ANALYSIS OF THE CORONIAL ISSUES ............................................................................ 256
The Findings required by s.45 of the Coroners Act 2003 ................................................. 256
Examination of the Thunder River Rapids Ride at the Dreamworld Theme Park, including
but not limited to, the construction, maintenance, safety measures, staffing, history and
modifications. .................................................................................................................... 256
Records ....................................................................................................................................... 261
Technical Circumstances ............................................................................................................ 262
Lack of Automation ...................................................................................................................... 263
Operators Account of the Incident ............................................................................................... 263
Operator Responsibilities ............................................................................................................ 264
Response to the South Pump ‘Earth Fault’ .................................................................................. 265
Examination of the sufficiency of the training provided to staff in operating the Thunder
River Rapids Ride. ............................................................................................................ 266
Consideration of the regulatory environment and applicable standards by which
Amusement Park rides operate in Queensland and Australia, and whether changes need to
be made to ensure a similar incident does not happen in the future. ............................... 267
Mr. Polley’s Conduct.................................................................................................................... 269
Changes Made at Dreamworld Following the Incident ..................................................... 270
What further actions and safety measures could be introduced to prevent a similar future
incident from occurring? .................................................................................................... 270
RECOMMENDATIONS IN ACCORDANCE WITH s.46 ....................................................... 271
DISCRETION TO REFER IN ACCORDANCE WITH s.48 (4) .............................................. 273
Referral of Ardent Leisure Limited to the OIR ................................................................... 274
Mr. Polley ........................................................................................................................... 274
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 5 of 274
INTRODUCTION
1. At around 2:05 pm on 25 October 2016, a tragic incident occurred on the Thunder
River Rapids Ride (TRRR) at Dreamworld Theme Park, Coomera, which claimed
the lives of Ms. Kate Goodchild, Mr. Luke Dorsett, Ms. Cindy Low and Mr.
Roozbeh Araghi. A joint inquest into the circumstances of this tragedy was
convened over a six-week period at various dates in June, October, November
and December 2018, in the Coroners Court of Queensland at Southport.
2. The gravity, complexity and scope of this tragedy at Australia’s largest Theme
Park was reflected in the comprehensive and professional investigations
conducted by the Queensland Police Service (QPS) and the Office of Industrial
Relations, formerly Workplace Health and Safety Queensland (OIR), as well as
the voluminous documentary, photographic and video exhibits obtained during
the course of the inquiry. During the hearing, oral evidence was taken from 59
witnesses, with an expert engineering conclave convened to provide evidence
concurrently.
3. The impact of this tragedy on the community, whilst paling in comparison to that
on the loved ones of those who lost their lives, has been undeniably significant.
Accordingly, the in-depth nature of this inquiry was intended to ensure that such
a tragic event does not happen again.
4. I would like to commend the work of all of those involved in the investigation of
this tragic incident. The investigation was conducted to an exceptionally high
standard, with a great deal of compassion, expertise and dedication by the
Queensland Police Service and Office of Industrial Relation (OIR) officers
involved. The gravity, scope and complexity of this tragedy at Australia’s largest
Theme Park is unparalleled in Queensland’s history, and was carried out to a
remarkable standard under great public scrutiny, with the eyes of the world
watching.
5. Whilst the investigation and ongoing preparation of this inquiry was certainly
collaborative, I would like to make particular commendations to the following
Queensland Police Investigators for their remarkable efforts.
6. I am grateful for the tireless and outstanding work undertaken by Detective
Sergeant Nicola Brown, the lead investigator for this tragic incident. Her standard
of work and dedication has been exceptional, and of great assistance to my
inquiry. The task of investigating such a unique and high-profile incident was
immense, and undertaken by Detective Sergeant Brown in a professional,
diligent, compassionate and comprehensive manner. I am thankful for all her
efforts during the course of these proceedings.
7. The skillful and detailed analysis conducted by Senior Constable Steven
Cornish, the lead Forensic Crash Unit Investigator, with respect to the
mechanical and technical aspects of this tragedy was pivotal to this inquiry. His
dedication and attention to detail ensured that this unique and catastrophic
incident was properly, and with the requisite expertise, investigated and
considered. I am grateful for all his tireless work and commitment.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 6 of 274

ISSUES FOR INQUEST
8. On 3 April 2018 and 25
May 2018, at pre-inquest hearings, the following issues
for the inquest were determined:
a. The findings required by s.45 (2) of the Coroners Act 2003; namely the
identity of the deceased person, when, where and how they died and
what caused the death.
b. The circumstances and cause of the fatal incident on the Thunder River
Rapids Ride at the Dreamworld Theme Park, which occurred on 25
October 2016.
c. Examination of the Thunder River Rapids Ride at the Dreamworld Theme
Park, including but not limited to, the construction, maintenance, safety
measures, staffing, history and modifications.
d. Examination of the sufficiency of the training provided to staff in operating
the Thunder River Rapids Ride.
e. Consideration of the regulatory environment and applicable standards by
which Amusement Park rides operate in Queensland and Australia, and
whether changes need to be made to ensure a similar incident does not
happen in the future.
f. What further actions and safety measures could be introduced to prevent
a similar future incident from occurring?
ABOUT THE DECEASED PERSONS
9. Ms. Kate Louise Goodchild was born on 3 August 1984 in Canberra. She resided
with her partner of 15 years, David Turner, and their two children, Ebony and
Evie in Ngunnawal, ACT. She was a dedicated wife and mother, who had a
wonderful sense of humour.
1
She had three siblings, Luke Dorsett, Jeremy
Goodchild and Peta Harrison. At the time of her death, Ms. Goodchild worked for
the Department of Human Services, having previously worked in various public
service and private organisations.
10. Mr. Luke Johnathan Dorsett was born on 28 March 1981 in Canberra, and is Ms.
Kate Goodchild’s older brother. He resided with his adored partner of 10 years,
Mr. Roozbeh Araghi in the ACT. He worked for the Department of Human
Services. Like his sister Kate, Mr. Dorsett was dedicated to his role in the public
service and had an immense work ethic. He was described as an extraordinary
role model to those around him.
2
11. Mrs. Cindy Toni Low was born in Whakatane, New Zealand on 19 May 1974.
She and her husband, Mr. Mathew Low travelled to Sydney and settled there in
2001. They had two children, Keiran Elijah Low and Isla Grace Low. Mrs. Low
was a dedicated wife and mother, who was described by her family as vibrant,
intelligent and social.
3
She lived at East Gosford and worked as a personal
assistant at a property valuation company.
1
Ex B1, pg. 11
2
Ex B1, pg. 12
3
Ex B1, pg. 11
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 7 of 274

12. Mr. Roozbeh Araghi was born on 7 September 1978 in Iran to parents Behrooz
Araghi and Vivien Hadden Araghi. He had two siblings, Simon Sirus Araghi and
Darius Araghi and was the father of Zachary Araghi Dawson and Harrison Araghi
Dawson. He resided in the ACT with his loving partner of 10 years, Mr. Dorsett.
He held a Bachelor of Arts (Honours) from Sydney University and worked for the
Australian Bureau of Statistics. He was known amongst his friends and
colleagues as a ‘tireless defender of the under privileged’.
4
BRIEF SUMMARY OF THE INCIDENT
13. On Tuesday 25 October 2016, Dreamworld opened as usual at 10:00 am. The
Thunder River Rapids Ride (TRRR) commenced operating with nine rafts in
circulation and two Ride Operators. This is the maximum number of rafts allowed
in circulation for a two Operator model.
5
14. At around 2:00 pm on 25 October 2016, Cindy Low and her son Kieran, Kate
Goodchild and her daughter Ebony Turner, along with Kate’s brother, Luke
Dorsett and his partner Roozbeh Araghi, boarded Raft 5 of the TRRR. At the
time, the weather was dry and clear.
15. The TRRR, which is no longer in commission, was an aquatic based family
orientated ‘moderate thrill ride’, which was suitable for patrons over the age of
two. It was designed to simulate white water rafting for six patrons, with the option
of having three children seated on an adult’s lap, within a circular raft.
Statistically, it was the most popular ride in the Theme Park.
6
16. Raft 5 travelled through the water course without incident before being picked up
by the conveyor at the end of the ride and moved towards the elevated unloading
area. At this time, Raft 6, which was dispatched in front of Raft 5, became
stranded on the steel support rails situated at the end of the conveyor near the
unloading area. Raft 5 continued to travel on the conveyor where it collided with
Raft 6 before being lifted and pulled vertically into the conveyor mechanism.
Ebony and Kieran, who were seated at the top of Raft 5, were able to free
themselves and escape to safety. Ms. Goodchild, Ms. Low, Mr. Dorsett and Mr.
Araghi were caught in the mechanism of the ride, and were either trapped in the
raft or ejected into the water beneath the conveyor.
17. The Ride Operators and some patrons immediately responded to the incident,
attempting to assist those trapped in the raft and in the watercourse. Emergency
services were contacted, and various Dreamworld staff responded to the
incident. Unfortunately, all attempts to provide medical assistance to Ms.
Goodchild, Mr. Dorsett, Ms. Low and Mr. Araghi were unsuccessful, and they
were declared deceased at the scene.
18. A major investigation code named ‘Operation Oscar Holocene’ was immediately
commenced by QPS, which included support from various internal specialty
units, including the Forensic Crash Unit, who carried out testing and an expert
analysis of the scene and circumstances of the incident. Given the scale of the
investigation and nature of the incident, support was also provided by the State
Crime and Intelligence, Counter-Terrorism and Major Events Command.
4
Ex B1, pg. 12
5
Ex B1
6
Ex B3C(50), pg. 20
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 8 of 274
19. The scope of the QPS investigation was twofold. Firstly, to determine whether
there was any criminal negligence or criminal responsibility under the Criminal
Code 1899, and also to identify, report and obtain evidence, which could assist
the South Eastern Coroner in his investigation of the incident, establish a cause
of death, make the requisite findings under the Coroners Act 2003 and identify
any possible preventative recommendations. In addition to undertaking an expert
forensic examination and search of the incident scene, a multitude of witnesses
were interviewed, including eye witnesses, Ride Operators, Dreamworld
management staff, maintenance workers, current and former Dreamworld
employees, Queensland Ambulance Service (QAS) officers, and Dreamworld
patrons. Relevant evidence from the scene was seized, extensive photographs
of the incident site taken, and various external and internal subject matter experts
were engaged in order to comprehensively canvas all of the pertinent issues
associated with the tragedy, and to ensure a thorough and expert analysis was
conducted of the incident and scene.
20. Due to the nature of the coronial investigation, its gravity and scope, OIR, whilst
undertaking their own separate statutory investigation, assisted QPS in
examining the incident. Various interviews and evidence was obtained pursuant
to s.171 of the Work Health and Safety Act 2011, for an array of potential
witnesses, who refused to provide voluntary statements to QPS, however, were
highly relevant to provide context, evidence, information regarding training,
maintenance, safety and the history of the TRRR.
21. The OIR investigation into the circumstances of the tragedy was also extensive,
and various professionals and experts were employed to provide comment as to
components of the incident, the ride and regulatory history. OIR officers attended
site immediately following the incident and continued to work concurrently with
QPS investigators throughout the course of the inquiry.
22. Extensive documentary evidence was also sought from Ardent Leisure, as well
as other external parties, by way of numerous coronial directions. As a result,
voluminous records pertaining to a myriad of issues, including the TRRR,
modifications made, training, maintenance, job descriptions, operations at
Dreamworld, certifications, workplace health and safety related issues, meeting
minutes, safety decisions, policies and procedures, directions and complaints,
were obtained.
23. Ultimately, comprehensive coronial reports with extensive annexures, including
statements, interviews and documentary exhibits, were furnished by Detective
Sergeant Nicola Brown, Gold Coast Criminal Investigation Branch and Senior
Constable Steven Cornish, Forensic Crash Unit (FCU), Coomera.
24. As Coroner I attended the scene of the tragedy and was briefed by officers
approximately two hours after the event and before the forensic pathologists
attended. I also attended the day of testing and reconstruction, in company with
my Counsel Assisting, Ms. Rhiannon Helsen and my Investigations Officer, Mr.
Mark Ozolins.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 9 of 274
POST MORTEM FINDINGS
Kate Goodchild
25. An external and full internal post-mortem examination was carried out on 26
October 2016 by Pathologist, Dr Dianne Little. A CT scan and toxicological
testing was also conducted.
7
26. The post-mortem examination revealed the presence of severe chest and
abdominal injuries. A band of abrasions and bruising were found across the
upper and mid trunk, as well as the corresponding area across the left upper
arm. Internal injuries found included multiple rib fractures, fragmentation of the
liver, transection of the duodenum and torn blood vessels to the right kidney.
These injuries were the direct cause of death and suggestive of a crushing blow
to this area of the body. There was no evidence of drowning.
Luke Dorsett
27. An external and full internal post-mortem examination was carried out on 26
October 2016 by Pathologist, A/Professor Alex Olumbe. A CT scan and
toxicological testing was also conducted.
8
28. The external examination revealed extensive bruising and abrasions over the
entire body. Multiple severe contusions and crushing injuries to the neck, spine
and ribs, as well as the liver, were found following the internal examination.
These injuries were consistent with having been caused by multiple compressive
impacts, particularly to the cervical area, and upper section of the thoracic spinal
column, resulting in severing of the brain stem, as well as other injuries. Death
would have been rapid. There was no evidence of drowning.
Cindy Low
29. An external and full internal post-mortem examination was carried out on 25
October 2016 by Pathologist, Dr Dianne Little. A CT scan and toxicological
testing was also conducted.
9
30. Extensive multiple injuries were observed to the head, chest, abdomen, pelvis
and limbs, the combined effect of which was found to be the cause of death.
Roozbeh Araghi
31. An external and full internal post-mortem examination was carried out on 25
October 2016 by Pathologist, A/Professor Alex Olumbe. A CT scan and
toxicological testing was also conducted.
10
32. The cause of death was extensive disruptive chest injuries evidence of which
was evident internally and externally. The mechanism of death was found to be
a single disruptive compressive impact to the middle section of the chest due to
a rapid movement by an implement. Death would have been rapid. There was
no evidence of drowning.
7
Ex A3 & A4
8
Ex A7 & A8
9
Ex A11 & A12
10
Ex A15 & A16
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 10 of 274

DREAMWORLD STRUCTURE & OVERVIEW
33. The Dreamworld Theme Park is located on the Gold Coast at 1 Dreamworld
Parkway, Coomera. It was developed by John Longhurst and was officially
opened to patrons on 15 December 1981. Over the years, Dreamworld has
expanded, and is now Australia’s largest Theme Park comprised of various
themed rides, wildlife and television branded attractions. Ardent Leisure Group,
an Australian based leisure company, currently owns and operates Dreamworld,
having acquired the park in 1998 from the Macquarie Leisure Trust.
11
Ardent
Leisure operates Dreamworld along with the adjacent Whitewater World,
Skypoint, AMF Bowling, Kingpin Bowling, and Good Life Health Clubs throughout
Australia, New Zealand and the United States of America.
12
Ardent Leisure
Limited was incorporated on 28 April 2003 and took over the ownership,
management and responsibility of the Dreamworld assets from that date. The
TRRR had long been in operation at that time. The documentation Ardent
inherited in 2003 could well be described as “scant”. They commenced their own
record keeping from that date.
34. Within Dreamworld, under the command of the Chief Executive Officer (CEO),
are the following Departments:
13
• Operations;
• Engineering and Technical (E&T);
• Life Sciences;
• Retail;
• Sales and Marketing;
• Food and Beverage;
• Safety;
• Finance and Administration; and
• Employee relations.
35. The CEO of Dreamworld, at the time of the tragic incident, was Mr. Craig
Davidson. All General Managers of the above Departments, and the Chief
Financial Officer reported directly to him.
14
He held the ultimate decision making
authority for Dreamworld, and liaised directly with the Ardent Leisure Board as
to all relevant matters, including safety, expenditure and the like.
15
In a
responsibility statement for the CEO, which was signed by Mr. Davidson on 20
March 2015, it notes, inter alia, that the position is responsible for the health and
safety in all areas of their control and is responsible to:
16
11
Ex B1, pg. 9
12
Ex B1
13
Ex B12(26)
14
Ex C8(10), pg. 11
15
Ex C8(10), pg. 11
16
Ex C7(580)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 11 of 274

• Assist the business to develop and implement the Work Health and
Safety Plan and actively support the Plan to meet the safety objectives;
• Ensure that managers under their delegation are aware of the work health
and safety responsibilities;
• Ensure that relevant personnel perform risk assessments and implement
controls in accordance with an relevant Regulations, Australian
Standards and Codes of Practice;
• Establish an annual review of the Safety Management System to ensure
it reflects the current legislation and supports the needs of the company;
• Regularly assess (at least every year), via internal auditing, how
effectively operations comply with the required health and safety
standards; and
• Participate in and support safety inspections – shall conduct at least one
safety inspection of the Business per year.
36. The Operations Department, which is one of the largest within the Park, has a
number of subsets, including Aquatics, Attractions, Entertainment, Costume,
Security, Guest Services, Reception, Cleaning and Gardening.
17
The Operations
Department is responsible for the ‘smooth running of the park throughout the
day’ and encompasses the Ride Operators, supervisors, relief supervisors and
instructors.
18
At the time of the tragic incident, Mr. Troy Margetts was the
Operations Manager at Dreamworld. He had held this role since 2014, having
commenced employment with Dreamworld in 1990.
19
He was required to report
directly to Mr. Davidson.
37. Mr. Andrew Fyfe was the Attractions and Entertainment Manager at Dreamworld,
which was a subset of the Operations Department. He reported to the Operations
Manager, having held this position for the past 10 years.
20
Mr. Fyfe was
responsible for the daily operations of White Water World slide attendants,
Dreamworld Ride Operators and the Attractions Supervisory team, as well as the
entertainment staff and Laundry and uniform operations.
21
38. Within the Operations Department, Ms. Nichola Horton was the Operations
Systems Administrator, having worked at Dreamworld in various roles since
2002.
22
This role, which commenced in 2016, reported directly to Mr. Margetts,
and was responsible for examining systems in place across operations through
audits to determine what improvements could be made.
23
As part of this role, Ms.
Horton was involved in amending and writing Ride Operator procedures for
various rides within Dreamworld and ensuring these were placed onto Liferay, a
new electronic document library.
24
She also had carriage of accounts for
Operations, which included ordering for the Operations Department.
25
Ms.
17
Ex B12(26), pg. 5
18
Ex B12(26), pg. 5
19
Ex B3C(50), pg. 6 & 7
20
Ex B3A(17), [7]; Ex C8(6), pg. 5
21
Ex B3A(17), [8]; Ex C8(6), pg. 5
22
T25-4, lines 40-47
23
Ex B3C(25), [2]; Ex C7(24)
24
T25-8, lines 17-40
25
Ex B3C(25), [2]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 12 of 274

Horton also performed the role of Duty Manager at Dreamworld, which involved
responding to guest complaints, any ride related emergencies, or any major
events.
39. At the time of the incident, the Attractions Supervisors, who reported to Mr. Fyfe,
included Ms. Jennie Knight, Mr. Jason Johns, Ms. Tracey McGraw and Ms.
Sarah Cotter.
26
The responsibilities of the Supervisors were to ‘ensure the safe
and efficient daily operations of the Attractions Department through effective
management of people resources and operational efficiencies…’ which included
supervising the activities of attractions staff on a daily basis, attendance at daily
operational calls, Code 6’s and breakdowns on rides.
27
A Code 6 is the code
used when a ride has ceased operation due to a technical fault. Each of the
Supervisors had been Ride Operators previously and progressed to the position
of Supervisor.
40. Relief Supervisors within the Attractions and Entertainment Department are
responsible for supervising park operations, which includes supervising the
Operators out on the rides, being called out to breakdowns, being out in the park
to ensure that the operation runs smoothly and assisting to manage guest
issues.
28
41. According to the Attractions and Aquatics Induction Handbook, Supervisors in
the Operations Department were responsible for the day to day operation of the
park, which included daily supervision of all team members, liaising with other
Departments as necessary, attending emergency situations, hazard and incident
reporting, assessing team member’s performance and assisting with guest
enquiries.
29
They were also expected to work with management and various
team members to execute new ideas and initiatives.
42. Meetings were held weekly with Mr. Margetts, Mr. Fyfe and the Supervisors
within the Operations Department. Financial results were discussed, as were any
relevant findings from recent Executive Meetings, with Managers providing an
update as to any issues associated with their area.
30
Whilst ride down times and
safety were not generally discussed during these meetings, any prolonged delay,
unscheduled maintenance or ride shutdowns were canvassed.
31
43. The Engineering and Technical (E&T) Department within Dreamworld is
‘responsible for the servicing and maintenance of all of our rides and
attractions’
32
and is required to attend a ride in the event of a breakdown during
daily operations. Personnel in this Department include multiple technical
specialties, including electricians and mechanical fitters and turners. At the time
of the incident, Mr. Christopher Deaves was the General Manager of
Engineering. Whilst he had no tertiary engineering qualifications, he held an
Advanced Diploma in Mechanical Engineering, as well as a Diploma of Business,
Health and Safety and trade qualifications.
33
Mr. Scott Ritchie (Electrical), Mr.
Mark Watkins and Mr. Wayne Cox were all Supervisors within the Department.
26
Ex B3A(11), [2]; Ex C8(6), pg. 5
27
Ex C7(19), pg. 1 & 2; Ex C8(6), pg. 6
28
Ex C6(46), [13]
29
Ex B12(26), pg. 7
30
Ex B3C(50), pg. 19
31
Ex B3C(50), pg. 19 & 20
32
Ex B12(26), pg. 5; T5-19
33
Ex B3C(46), pg. 5 & 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 13 of 274

44. Long-term former employee, Mr. Bob Tan, who resigned from Dreamworld in
January 2016, commenced working at the Park in 1987 as the Assistant
Maintenance Controller. He subsequently performed a number of roles, including
the Projects Manager (1992), Technical and Services Director (1995),
Maintenance Controller (2003), General Manager of Engineering (2009), before
taking on the role of Director of Special Projects within the Engineering
Department (2014) when Mr. Deaves was promoted to the General Manager of
Engineering.
34
Mr. Tan reported directly to the CEO. During his tenure at
Dreamworld, he became a qualified engineer, however, was not RPEQ certified.
45. At the time of the incident, the Safety Department at Dreamworld was
responsible for assisting with safety compliance at the Park, and to continually
improve culture/business practice in conjunction with other Departments.
35
Mr.
Mark Thompson was the Safety Manager at the time having commenced in the
position in March 2016.
36
He was responsible for delivering training on general
safety matters at induction, park-wide safety matters, responding to issues raised
through the incident system and implementing control measures for these
hazards and investigating suspected safety breaches, as well as oversight of the
First Aid Clinic.
37
Mr. Thompson reported to Mr. Angus Hutchings, who was the
Group Safety Manager for Ardent Leisure.
38
Mr. Hutchings had held this position
since 2010, and was responsible for providing advisory services with respect to
safety and strategic planning to all of the Ardent Leisure business groups,
including Dreamworld.
39
From 2004 until 2010, Mr. Hutchings held the position
of Dreamworld Safety Manager.
40
In both roles, he was required to report to the
CEO. Mr. Hutchings had prior experience working for the Safety Regulator, OIR,
however, had not previously been involved in implementing or devising safety
systems.
41
46. Within Dreamworld there were also a number of subset groups and teams, which
met at various intervals to discuss different matters. From the records provided,
the most pertinent groups relevant to the decision making within the Park seem
to be as follows:
(i) The Leadership Team, which consisted of General Managers of the
various Departments within the Park, including Mr. Margetts, Mr.
Thompson, Mr. Tan and Mr. Deaves.
42
A wide range of issues were
discussed during these meetings, including safety, financials, guest
service issues, rides and upcoming events.
43
The CEO would sometimes
attend these meetings if needed.
(ii) The Executive Safety Committee consisted of the CEO and General
Managers of the Departments, which at the time of the incident relevantly
seems to have included Mr. Craig Davidson, Mr. Deaves, Mr. Hutchings
and Mr. Margetts.
44
Topics discussed at these meetings included ride
34
Ex B3C(54), pg. 20; Ex F12(540)
35
Ex C6(51), [40]
36
Ex C6(51), [3]
37
Ex C6(51), [3]
38
Ex C6(51), [7] & [8]
39
Ex C8(10), pg. 5 & 6
40
Ex C8(10), pg. 8
41
T21-28 & 29
42
Ex C8(6), pg. 19; Ex C8(10), pg. 14-17
43
Ex C8(10), pg. 18
44
Ex C8(6), pg. 19; Ex C6(51), [33]; Ex C8(4), pg. 9
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 14 of 274

modifications.
45
(iii) The Engineering Management Team, which consisted of the General
Manager of Engineering and Supervisors, as well as Mr. Thompson, as
the Safety Manager. Weekly meetings were conducted,
46
with issues
associated with rides, including down-times, being discussed.
47
47. Further specific details as to the Safety and E&T Departments at Dreamworld
and their respective responsibilities and staffing, commence at page 78.
THUNDER RIVER RAPIDS RIDE (TRRR)
48. The TRRR commenced operation in December 1986, as part of the rustically
themed Gold Rush Country section of the Theme Park. It was manufactured in-
house at Dreamworld between 1985 and 1986, and was based upon a 1979
Intamin Amusement Ride called ‘Rapids Ride’.
48
Information as to the original
construction and subsequent modifications to the TRRR, as provided by Ardent
Leisure and OIR, are minimal. A summary of the information provided as to the
various modifications and alterations made to the ride over its 30 year
commission, are outlined further below commencing at page 25.
49. The TRRR was designed by consultant engineers. Mr. Len Shaw, the
Engineering Services Manager for Dreamworld, oversaw the construction. The
engineering drawings were provided at the time to Workplace Health and Safety
(as it then was) and approved by the Chief Inspector of Machinery for the Division
of Occupational Safety.
50. On 14 August 1987, the design of the TRRR was approved by the Chief Inspector
of Machinery in principle, subject to safety devices and guarding being found to
be to the requisite satisfaction of the District Inspector of Machinery.
49
Supporting
documentation to the design approval indicates that the ride was certified at that
time by a Consulting Engineer attesting to the safe structural integrity of the
design, and that it was compliant with the Australian Standards.
50
51. The TRRR was designed as a family orientated, aquatic based amusement ride,
which consisted of a raft that seated six occupants. Riders entered a long
partially indoor queue with a number of switchbacks, along with an express line
for the Ride Express pass holders. Upon reaching the front of the queue, riders
were guided onto a circular raft by one of two TRRR Ride Operators, before
being dispatched from the loading area. The ride then proceeded to be propelled
by a natural flow of water through the man-made river’s watercourse, which
includes calm and turbulent rapids, with rafts reaching speeds of up to 45 kph.
51
52. The raft travelled a watercourse (rapids) through various troughs and tunnels,
which was approximately 450 m long.
52
A wooden conveyor transported the rafts
at the end of the ride to the unload area. The duration of the ride, until the
commencement of the conveyor, was approximately three minutes and 16
45
Ex C5(51), [36]
46
Ex C6(51), [30]; Ex B3C(53), pg. 11
47
Ex B3C(53), pg. 11 & 12
48
Ex B1, pg. 10
49
Ex F9C(3)(a), [9]; Ex F9C(3)(b), pg. 1
50
Ex F9C(3)(b), pg. 3
51
Ex B1, pg. 10
52
Ex F9A(1), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 15 of 274
seconds
53
with a 35 second delay between each raft. It took approximately 42
seconds for a raft to travel on the conveyor and arrive at the unloading area.
54
The approximate total ride time for the TRRR was 4 minutes and 10 seconds.
55
53. Riders could get wet during the course of the ride, which ended when the raft
was elevated and transported by a conveyor towards the unloading area, which
is adjacent to where patrons are loaded onto the ride.
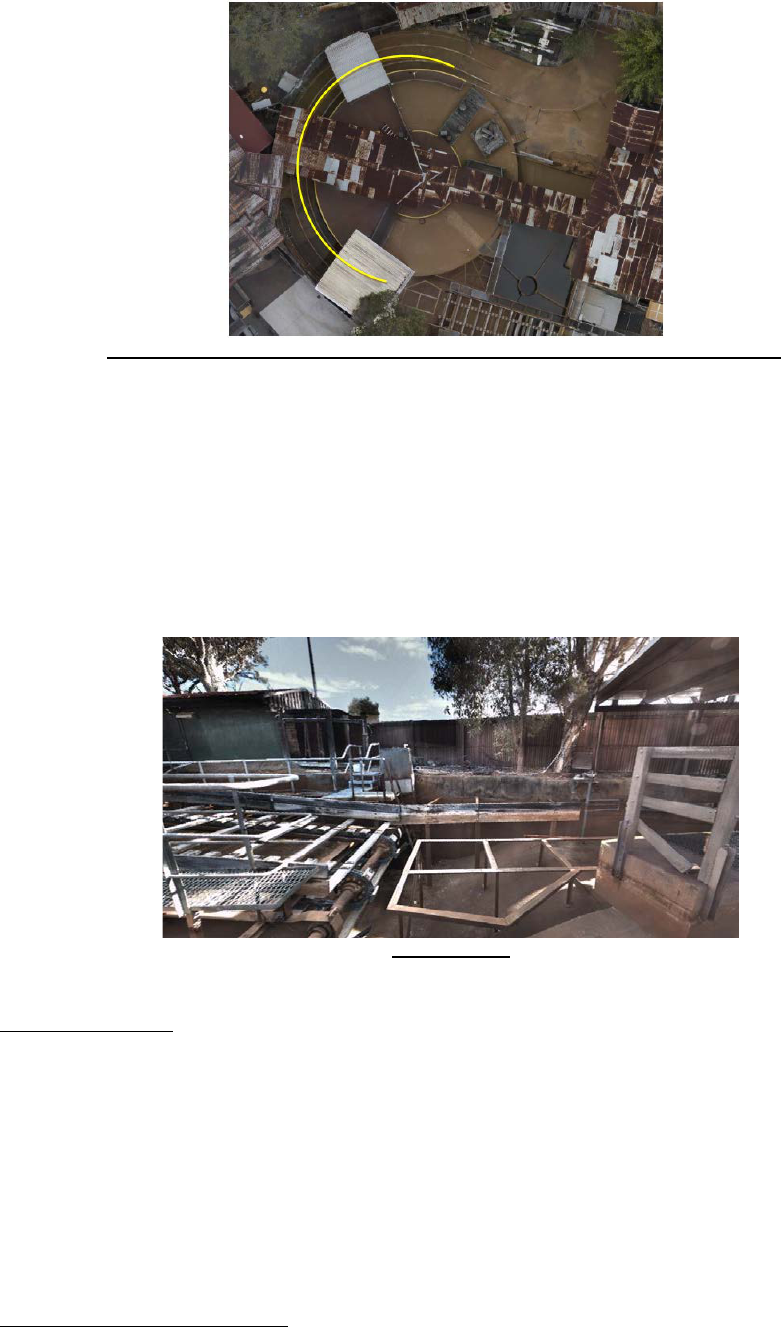
54. Below is an aerial view of the ride, with the path travelled by each raft through
the watercourse highlighted in yellow.
FIGURE: Ex F9A(1), pg. 4
Configuration of the TRRR
Forensic Crash Unit Investigation
55. As part of the QPS investigation, the mechanical and technical aspects of the
TRRR, its operation and the tragic incident were analysed by Senior Constable
Steven Cornish from the FCU at Coomera. This analysis included detailed
consideration of the technical operation of the ride and its components in their
entirety, relevant supporting documentation as to the ride and its history, as well
as the mechanism and timeline of the incident. Extensive on-site testing of each
component of the ride was carried out, in addition to various attempts to
reconstruct the tragic incident.
56. Senior Constable Cornish’s findings were detailed in a supporting coronial report,
with the various testing and other diagrams and exhibits annexed.
56
57. The findings reached by Senior Constable Cornish were accepted and reinforced
by expert evidence provided by way of a conclave during the inquest hearing,
and have formed the basis for the details as to the configuration of the TRRR,
the timeline of the incident, and the cause.
53
Ex B2, pg. 6
54
Ex B2, pg. 6
55
Ex B1, pg. 10
56
Ex B2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 16 of 274

Configuration of the TRRR at the Time of the Incident
58. There were a number of major components of the TRRR, which whilst operating
individually, also played an integral and interdependent role within the overall
successful function of the ride.
57
The central components of the ride consisted of
a trough, water pumps, conveyor system, rafts, pneumatic gates, operating
control system and raft support rails.
FIGURE EX. F9A(1), PG. 7: OVERVIEW OF TRRR WITH LOCATION OF LOADING &
UNLOADING AREA, PUMPS, CONVEYOR & RAILS
Operating Control System
59. The main operating control panel was located at the designated loading area of
the ride.
58
It had the capability of operating all of the independent components of
the ride, and was the only panel to have this access. The CCTV from five
cameras located around the ride were displayed on a monitor within a partitioned
wooden area. The position of this panel allowed the Ride Operator to oversee
the trough area as the rafts departed, as well as the conveyor system and unload
area.
MAIN CONTROL PANEL AS IT APPEARED OCT 2016 - EX B2, PG. 30
57
Ex B2, pg. 6
58
Ex B2, pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 17 of 274
60. There is an approximate distance of 12 metres between the Main Ride Operator
and the Unload Operator.
59
Due to the distance from the conveyor and unload
area, as well as the wooden structure of the control unit and exit walkway fencing,
the line of sight of the end of the conveyor by the Ride Operator stationed at this
panel was somewhat obstructed.
60
There was no electronic communication
between the two Operators.
Trough
61. The trough was the channeling system, which the water flows through over a
distance of 410 metres, transporting the rafts and occupants.
61
It was generally
constructed of concrete with a depth of 1.3 metres and a width measuring
between three to five metres around the course of the ride.
62
62. Along the length of the trough, there were a series of turns, barriers and floor
mounted wooden logs. These elements were designed to create a turbulent flow
for the water, and to simulate a rafting experience. There were also a number of
tunnels, one of which had animations and attractions related to the ride and
operated by motion sensors.
63
63. Through the load and unload area of the ride there were outer metal guide rails
and wooden barge planks on the trough, which were designed to assist with the
loading and unloading of guests from the rafts.
64
Raft Supporting Rails
64. Mounted throughout the trough system in the load and unload areas of the ride
were steel raft support rails, which were primarily intended to prevent the rafts
from heeling (tipping) or flipping whilst occupants were embarking or
disembarking.
65
The rails also prevented the rafts from dropping to the bottom of
the trough in the event that the water level reduced or completely dissipated.
65. The steel railings were a dual system constructed of 100 mm wide right angle
steel, spaced 1450 mm apart (outer to outer) and bolted to the concrete floor of
the trough.
66
Within the level area of the trough between the load and unload
areas, the railings were positioned a minimum of 700mm above ground level and
remained level for the complete length of the construction.
67
59
Ex B2, pg. 65
60
Ex B2, pg. 9 & 65
61
Ex B2, pg. 11
62
Ex B2, pg. 11
63
Ex B2, pg. 11
64
Ex B2, pg. 11
65
Ex B2, pg. 12
66
Ex B2, pg. 13
67
Ex B2, pg. 13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 18 of 274
DEPICTS THE RAILING SYSTEM THROUGH ENTRY/EXIT AREA - EX B2, PG. 12
66. Additionally, there were a series of support railings in the trough prior to the
beginning of the conveyor (bottom), which were installed in 2015.
68
67. In the area of the incident at the end of the conveyor (top), there was no variation
in the level, with the support rails having been adapted to suit the sloping nature
of the flooring leading back to the area beneath the conveyor, known as the ‘pit’.
69
This area is where the water for the ride was gravity drained back into the storage
reservoir.
EX B2, PG. 14
Conveyor System
68. The conveyor on the TRRR was a mechanical device, which was chain driven
by an electric motor. The conveyor belt was constructed of a series of wooden
planks of two variations in size and evenly spaced along the belt.
70
The conveyor
was located towards the end of the ride, and was used to carry rafts from the end
of the trough system up to the unloading area.
69. The drive axle and two cogs were fixed to the western end of the conveyor where
the electric motor was attached. There was a dual chain system, which the
68
Ex B2, pg. 13
69
Ex B2, pg. 14
70
Ex B2. Pg. 16
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 19 of 274
planks were attached to, that was pulled along from the drive axle.
71
The
conveyor was driven by its own dedicated, power source and control system,
which was not linked to any other of the ride’s components.
70. The main control system for the conveyor was located at the Main Control Panel,
with a further control box, primarily used for maintenance purposes, located next
to the conveyor away from public access.
72
At the Operator control panel, there
was a start and stop button, as well as a reset button, which could be used to
restart the conveyor in the event that it was stopped under the Emergency Stop
procedures.
73
Upon depressing the start button, it became illuminated to show it
was operating whilst the red button flashed. The red button initiates the slow shut
down of the conveyor. There was no Emergency stop for the conveyor available
at the Main Control Panel.
74
71. During testing of the conveyor and Main Control Panel, Investigators found that
depressing the stop button for the conveyor was sufficient to initiate a slow stop.
75
A slow stop of the conveyor took 8 seconds for the conveyor to come to a
complete stop.
76
Activation of the E-Stops were found to stop the conveyor in
two seconds.
77
72. Given the location of the incident and mechanism involved, extensive
examination of the conveyor was undertaken by Senior Constable Cornish and
other officers, which included intricate manual measurements.
78
Video
recordings of the conveyor’s movements also assisted to calculate speeds, as
well as the interaction with the rafts, supporting railings and water flow.
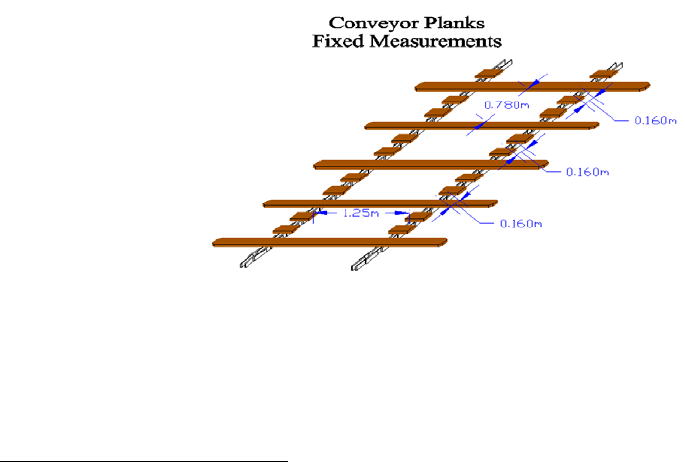
79
73. The measurements of the conveyor planks, including the spacing and
configuration, are as follows:
80
74. The speed of the conveyor was found to be 2.7 kph.
81
75. An open air gap was found between the end of the conveyor closest to the unload
station and the beginning of the raft supporting rails. This interface area, which
was significant during the incident as it was into this gap that Raft 5 was pulled
down once inverted, was extensively examined and measured. The gap of the
71
Ex B2. Pg. 16
72
Ex B2. Pg. 16
73
Ex B2, pg. 37
74
Ex B2, pg. 37
75
Ex B2, pg. 37
76
Ex B2, pg. 54; T2-43 & 44
77
Ex B2, pg. 82
78
Ex B2. Pg. 16
79
Ex B2. Pg. 16
80
Ex B2. Pg. 17
81
Ex B2, pg. 20
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 20 of 274
interface between the conveyor’s long planks at their furthest point, and the
leading edge of the support rail was found to be 430 mm, with a 760 mm gap
between the leading edge of the support rails and the drive axle (when
exposed).
82
DEPICTS SIDE PROFILE OF INTERFACE, Ex. B2, pg. 21
76. Further details as to the modifications made to the conveyor over the duration of
the ride’s 30 year commission commence at page 25.
Water Pumps
77. There were two Danfoss VLT Aqua VLT 8502 Drives, which operated the two
induction motors (water pumps) utilised by the ride.
83
The drives were installed
in 2006.
84
The pumps were referred to as the North and South pumps due to
their positioning. The pumps were located under the conveyor belt, in a separate
confined enclosure.
78. The controls for both the pumps (stop and start) were located at the Main Control
Panel by way of separate buttons. A display on the panel also showed the amps
for the respective pumps. This was a predetermined figure, which took into
account the condition of the pump and the operating hertz of the motor in the
main electrical room.
85
For the TRRR pumps, the reading was to be below 500
amp, and was generally between 430-460 amps.
86
The control panel had no
mechanism to allow for a variation of the power of the pump, which would
subsequently vary the water flow. The variation in the amp usage was
determined by the water level in the reservoir. The lower the water level, the
higher the amp output to maintain the constant flow through the outlet.
87
79. The amp display, red and green lights, were the only visible aspect on the panel,
which showed that the pump was functioning.
88
Each pump functioned
independently of the other, and could be started and stopped separately.
89
An
emergency stop at the panel also deactivated the North pump only.
90
There was
82
Ex B2, pg. 20
83
Ex B2, pg. 23; Ex G2, [24]
84
Ex G2
85
Ex B2, pg. 35
86
Ex B2, pg. 36
87
Ex B2, pg. 35
88
Ex B2, pg. 35
89
Ex B2, pg. 23
90
Ex B2, pg. 35
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 21 of 274
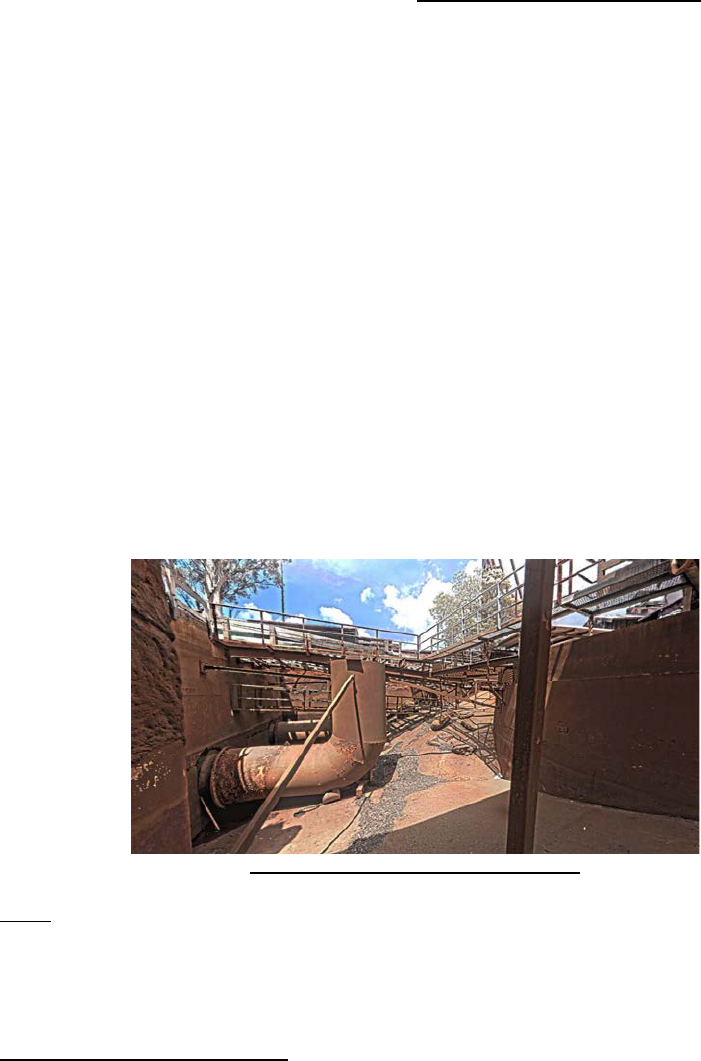
no emergency stop for the South pump, or one that stopped both pumps
simultaneously.
91
80. The North and South pumps were gravity fed from the storage reservoir, before
being pumped out through the two outlets positioned under the conveyor belt.
The pumps had the ability to pump up to 4000 litres per second.
92
This large
water flow created the initial current around the load and unload areas, before it
naturally flowed down through the trough system around the ride. The two outlets
were 1.6m in diameter and approximately 3 metres from the bottom of the pit.
93
They were also utilised in a reverse flow manner when water was being drained
from the ride area, which caused the water level to drop quickly and
considerably.
94
81. Under the instruction of Electrical General Manager, Scott Ritchie, Senior
Constable Cornish was shown the start-up procedures for the pumps. It was
observed that the North pump was activated first, and took approximately 7
minutes to get to operating capacity and its full ampere.
95
Once this was
achieved, the South pump was then activated and the same process followed.
Once the amp reading had stabilised and the pumps’ respective green lights
were at a solid illumination, the pumps were deemed to be operating at full
capacity. A final visual check was then to be undertaken by the Ride Operator of
the water level in the trough.
96
The same process could then be utilised to
manually shut down the pumps, pressing the red button to stop each pump.
97
A
key start and shut down process is stipulated in the Operators Procedure
Manual, which involves the use of a key start, which commences the auto
sequence.
98
PUMP OUTLETS IN PIT, EX. B2, PG. 15
Rafts
82. The rafts consisted of a fibreglass constructed tub, inserted into a large custom
built rubber tube, known as a floatation collar. The floatation collar was internally
separated into eight air chambers, which could hold a maximum of 2 PSI.
99
Each
91
Ex B2, pg. 35
92
Ex B2, pg. 24
93
Ex B2, pg. 86
94
Ex B2, pg. 86
95
Ex B2, pg. 36
96
Ex B2, pg. 36
97
Ex B2, pg. 36
98
Ex B2, pg. 36
99
Ex B2, pg. 25
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 22 of 274

raft had six allocated seats. They were inspected on a daily basis by E&T staff,
and often drained each morning as they would take on water during the day.
83. Neither the intended lifespan of the rafts or floatation collars in use at the time of
the incident nor how long they had in fact been in use by this date is known.
84. It should be noted that Raft 6, which was the stationary raft involved in the tragic
incident, had various notes recorded in recent daily checklists (6, 11, 15 & 20
October) with respect to air pressure in the floatation collar.
100
85. On 31 October 2016, all rafts in service on the TRRR were weighed. It was found
by Senior Constable Cornish that there was a variation of up to 100kgs between
all of the rafts.
101
Possible reasons offered for this variation were the rafts being
unable to be completely drained due to blockages in internal construction, an
amount of water soaking into the fibreglass, ropes or other materials within the
raft, or water within the collar.
102
Pneumatic Gates
86. A series of pneumatic gates, referred to as ‘jacks’ were positioned within the
loading and unloading zones. There were a series of two jacks at each of the
load and unloading areas. The primary function of the jacks was to restrict the
flow of the rafts through the trough system.
103
When operated, the jack protruded
into the canal stopping the raft from traveling further forward.
87. The primary operating system for the jacks was located at the main operating
panel. At the loading area, the jacks were used to hold the raft in place to allow
patrons safe access. There was a timing alarm integrated into the dispatch jack’s
release, which was designed to ensure that there was a safe gap between each
of the rafts leaving the area and commencing the water course. The timing was
approximately 35 seconds.
104
The Ride Operator at the Main Control Panel was
able to control the loading and dispatch jacks, as well as the final unload jack.
88. On the Main Control Panel, the load button operated the two jacks at the loading
area. Depressing the button caused both gates to open, moving the loaded raft
to the dispatch jack, whilst an empty raft moved forward to be loaded with further
patrons. Once the time delay alarm had sounded, the Ride Operator could
depress the load 2 button on the control panel, which then released the raft onto
the water course. The load and load 2 buttons were operated completely
independently of each other.
105
100
Ex B2, pg. 27
101
Ex B2, pg. 28
102
Ex B2, pg. 28
103
Ex B2, pg. 29
104
Ex B2, pg. 29
105
Ex B2, pg. 30
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 23 of 274
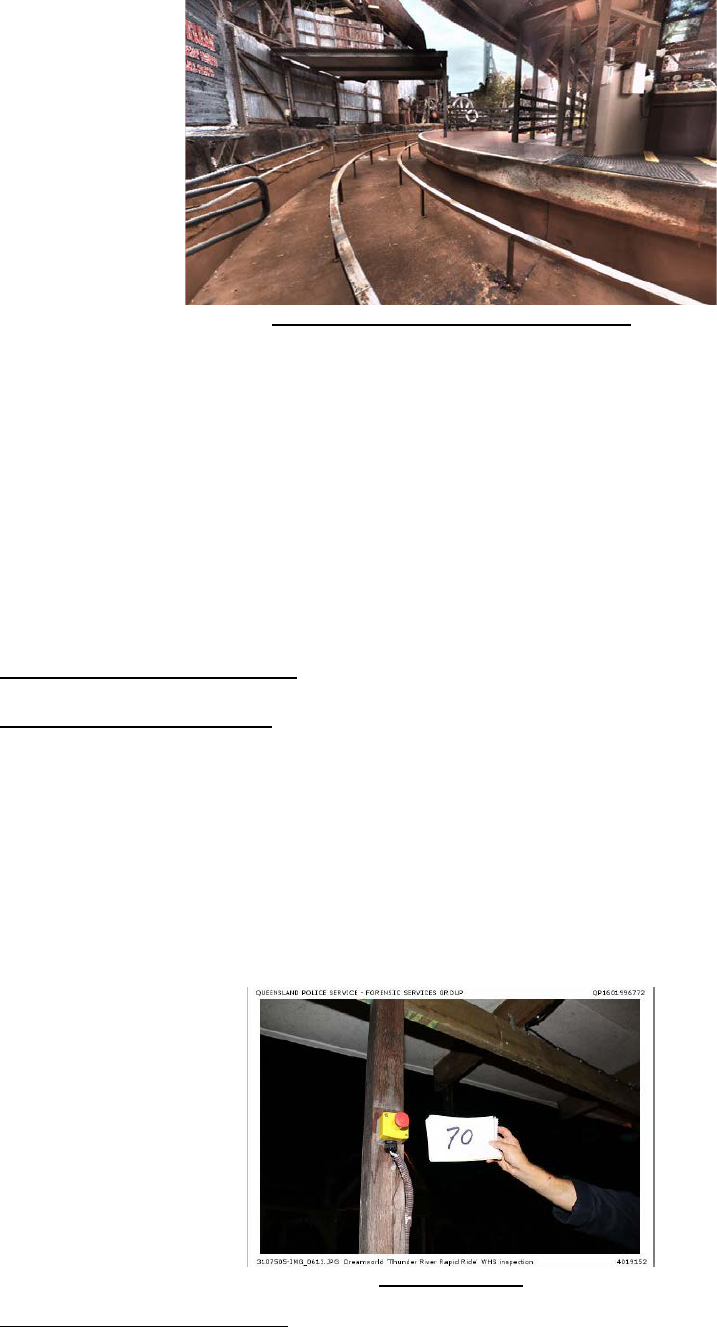
DEPICTS LOADING JACKS, Ex. B2, pg. 30
89. Within the unload area, there were two jacks with operating buttons on poles.
The first was used to stop and secure the rafts, which allowed the patrons to
disembark safely. The second jack was closer to the conveyor, and was
designed to prevent any approaching rafts from colliding with the stationary raft
in the unload area.
106
The jack near the conveyor was installed in 2004, following
an incident where an approaching raft collided with another in the unload area,
causing a patron to fall into the watercourse.
107
90. Further details as to the modifications made to the ride over its 30 year
commission and previous incidents are detailed below.
Safety Features of the TRRR
Emergency Stops (E-Stops)
91. There are a series of Emergency Stops, ‘E-Stops’, that were installed to activate
a near instantaneous stop of the conveyor.
108
They were located at the unload
area, the conveyor control panel box, and a lanyard emergency stop, which was
positioned either side of the conveyor.
92. The E-stop at the unload area was the only mechanism, which could stop the
conveyor, that was accessible by an employee or member of the public. It was
housed in a yellow box with a red button in the centre.
Ex. B4 (5), pg. 25
106
Ex B2, pg. 31
107
Ex B2, pg. 31
108
Ex B2, pg. 38
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 24 of 274
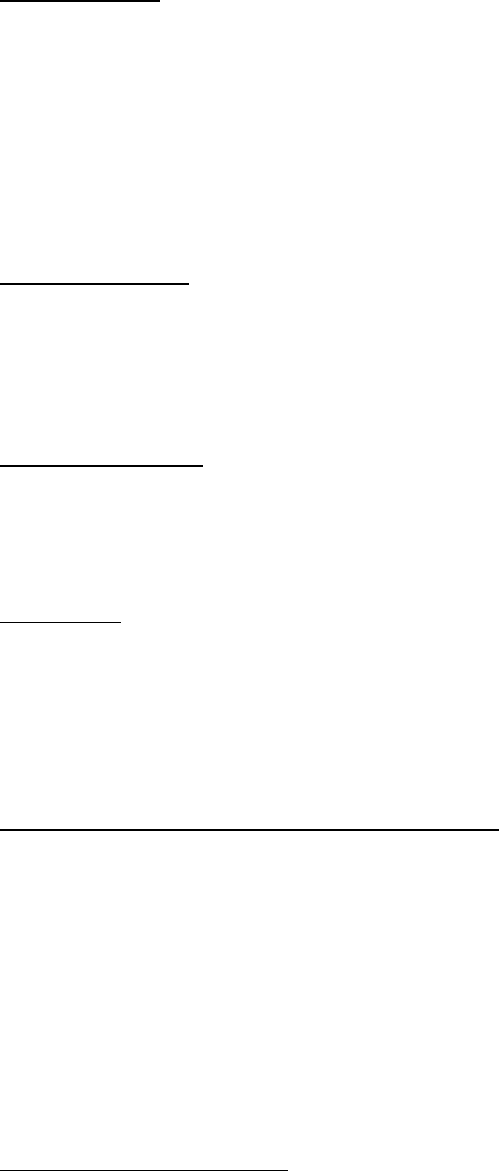
93. Testing by Investigators confirmed that there was not a single control button
which would initiate a complete shutdown of all of the ride’s mechanism.
109
Raft Safety Stop
94. Infra-red switches were positioned at the beginning of the conveyor (bottom),
which identified when a raft was stationary at that point for a period of at least 15
seconds. If this occurred, an audible alarm sounded, the conveyor stopped and
the release jacks were closed to prevent further rafts from entering the trough
system.
110
95. Further details as to these upgrades to the conveyor, which took place in 2016,
are set out below.
Chain Break Safety
96. A second series of sensors were located at the beginning of the conveyor, which
were designed to monitor the conveyor chain cadence at a certain rate. If the
sensor was not tripped for a period of five seconds there, it triggered a shutdown
of the conveyor as it assumed that there was a break in the chain.
111
Anti-Roll Back Gates
97. A set of four small gates were mounted to the incline component of the conveyor,
and were designed to stop rafts from sliding backwards along the conveyor
planks whilst traveling up the conveyor.
112
Water levels
98. Ride Operators were required to monitor water levels within the trough of the
ride. There was no formal water marker present in the trough of the load and
unload area.
113
Rather, Operators were required to measure the water level by
reference to a scum mark on the wall of the trough, which was made from years
of the ride operating.
114
History & Modifications to the TRRR Since 1986
99. The TRRR opened on 11 December 1986, and at the time of the incident, had
been operating for almost 30 years. During the course of its commission, the
Ride had undergone a number of modifications to various components, although
largely operated as it was intended to when first opened. A number of the major
components of the ride were original, with only slight improvements or
modifications having been made.
100. Documentation provided by Ardent Leisure relating to the history of the TRRR,
including the modifications made and any associated issues, which arose on the
ride, are scant at best. There is limited information as to the reasons for some of
the alterations, when they were carried out, and if any formal type of risk or
109
Ex B2, pg. 83
110
Ex B2, pg. 39
111
Ex B2, pg. 40
112
Ex B2, pg. 41
113
Ex B2, pg. 74
114
Ex C7(18)(a), pg. 27
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 25 of 274
hazard assessment was undertaken prior to or following the modifications being
made.
101. In more recent times, records suggest that ride modifications were discussed at
a number of different management meetings, including the Executive Safety
Committee Meetings, however, it seems proposals may have been verbally
discussed with the CEO, with capital expenditure approvals submitted through a
more formal process.
115
102. Overall, from the documentation provided, it appears that the modifications made
to the TRRR include:
• Removal of the conveyor slats (1989-1990 est.);
116
• Removal of the turntable (1990-1991 est.);
117
• Changes to the Operator Controls (1991-2016);
118
• Pump discharge pipes repositioned (1999-2000 est.);
119
• Pump motors replacement (2012);
120
• Mesh and rails at conveyor foot (2016);
121
• Pump motor drives replacement (unknown);
• Rails at conveyor head (unknown); and
• Removal of the rubber patches of the raft plug bases (unknown).
103. Below is a summary of some of the relevant modifications made to the TRRR
based on the limited records available.
Issues with the Conveyor and Removal of Slats
104. At the time of the tragic incident, it was evident that at some point in the history
of the ride, every 2
nd
and 3
rd
conveyor slat had been removed. Whilst it is not
clear when this modification was carried out, records suggest the following
timeline:
(I) 25 January 1988
122
– Rapid Ride Tail Shaft Failure
At 1:50 pm on 6 January 1988, the tail end of the TRRR conveyor started
to tear the timber slats off the conveyor chain.
123
An inspection found that
the tail shaft had fractured at a point in line with a locating bush on the
northern side of the idler sprocket. The break was clean and
‘unquestionably due to fatigue’ with similar damage found on the other
side of the sprocket. It was thought that this was due to a design fault.
This break caused the conveyor to destroy itself at the tail end on the
supporting steel, smashing 25 timber slats and badly distorting both chain
sections, tearing chain attachments off the links and completely
destroying bearing seals.
124
115
Ex B3C(54), pg. 10
116
Ex B12(16); Ex B4(1), 40
117
Ex C4(5), pg. 858-860
118
Ex B12(1)
119
Ex C4(5), pg. 444-445
120
Ex C4(5), pg. 444-449
121
Ex C4(5), pg. 447-449
122
Ex C9(165) – it appears that the reference to 1987 is an error, as 1988 is referred to throughout the memorandum
123
Ex C9(165)
124
Ex C9(165)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 26 of 274

It was noted that it was fortunate that a raft was not on the conveyor at
the time of the incident.
Repairs required to be carried out included the fitting of a new shaft, new
seals and new timber slats. The chain was able to be repaired.
(II) 16 January 1989 – Rapid Ride (timber slat removal suggestion)
In a memorandum directed to Mr. Garth Bell from Mr. Len Shaw,
Engineering Services Manager, it was reported that on 15 January 1989,
damage occurred to 3 slats on the TRRR conveyor.
125
This seems to
have been a recurring issue. On this occasion, it was surmised that the
issue may have been happening at the head of the conveyor due to water
flow from the southern pump, which was lifting the return side at an angle
sufficient for a slat to drop off the return guide track.
126
It was thought that
the slat would then run under the track until it reached the pump house
wall before it jammed and then broke as it tried to pass underneath.
It was suggested at this time that every alternate timber slat should be
removed in order to achieve the following:
- Reduce the overall weight of the system.
- Reduce the floatation effect of the timber.
- Reduce the number of things which can ‘get caught’.
It was suggested that a trial period of a section of the conveyor should be
conducted to ensure other issues weren’t created by this modification.
It was noted that something had to be done as ‘this chain is the subject
of continuous repair section by section. The working environment for a
steel chain is the worst possible imaginable.’
Mr. Shaw noted that ‘there is no way I can guarantee a trouble free run
on the ride when there is no control by us as to what the water does’.
105. According to Mr. Bob Wood, who commenced working at Dreamworld in
November 1988 as a mechanical fitter, the TRRR initially had full length planks
on the conveyor.
127
He recalls that the weight of the conveyor was causing the
conveyor chain to wear, which resulted in links having to be removed to shorten
it.
128
He was aware that a decision was made to remove every second plank
gradually from the conveyor to reduce the weight and the load being placed on
the chain.
129
To the best of his recollection, Mr. Wood thought this may have
taken place in the early 1990s.
130
The weight placed on the chain, however,
continued to be a regular issue despite this modification.
131
125
Ex B12(16)
126
Ex B12(16)
127
Ex B17(3), [8]
128
Ex B17(3), [8]
129
Ex B17(3), [9]
130
T28-12, lines 1-23
131
Ex B17(3), [9]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 27 of 274
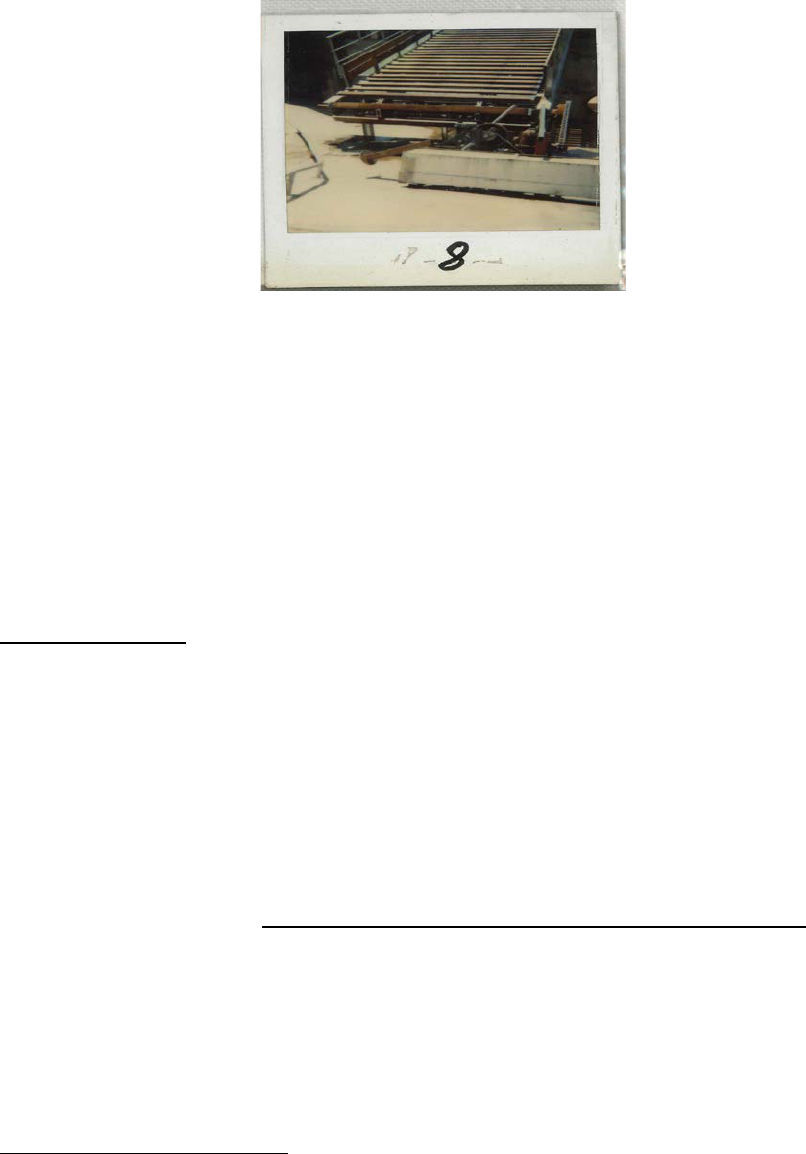
106. The below photograph depicts the conveyor as it was initially constructed in
1985.
132
107. Mr. Wood stated during the inquest that by the time he left employment with
Dreamworld in 2012, every 2
nd
and 3
rd
slat had been removed from the
conveyor.
133
108. According to Mr. Tan, who was employed in various roles within the Engineering
Department, including as the Manager since 1987, the removal of the wooden
slats on the conveyor took place between 1988 and 1990 because it was
frequently tripping.
134
The boards were removed to reduce the weight the
conveyor motors were required to drive, and to improve the chain ‘release’ from
the head sprocket.
135
Turntable Removal
109. Originally, the TRRR had a timber turntable at the end of the conveyor near the
unload area, which moved the rafts from the conveyor onto an arm of the
turntable that would then move the raft to a stationary position at the unload
area.
136
It was a large device, which spanned the end of the conveyor all the way
around the load and unload areas, whilst an arm of the turntable would ramp off
allowing the raft to float into the watercourse.
137
There were no steel supporting
rails near the conveyor or unload area at the time it was in use.
138
110. In a memorandum from Mr. Len Shaw, Engineering Services Manager, to Mr.
Wes Hepburn titled, Memorandum 13 August 1987 – Rapid Ride Turntable, it
was noted that there had been reoccurring issues associated with the turntable
at the TRRR.
139
Since December 1987, the total cost of requisitioned material
and services to maintain the whole of the ride operationally was $22,956.98, with
over 1000 man hours needed. The turntable component of those costs was
$5670, and about 300 man hours. The main issue seemed to be with the rolling
wheels, which shed the tyre, bearings in the rolling and thrust wheel collapsing.
To replace these failings was labour intensive and costly.
132
Ex B17(1)(a), pg. 2, photograph 8
133
T28-14, lines 17-25
134
Ex B3C(54), pg. 6
135
Ex B3C(54), pg. 6
136
Ex B17(3), [13]
137
Ex B17(3), [13]
138
Ex B17(1), [12]
139
Ex C9(167)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 28 of 274
111. It was submitted that air operated jack stands should be installed in lieu of the
turntable for the load and unload areas, with a controlled dispatch to pass rafts
at timed intervals. It was estimated that the cost of this system would be $7000.
112. In a memorandum from Mr. Len Shaw to Mr. Garth Bell titled, Memorandum 20
February 1990 – Rapid Ride Turntable, improvements to the way rafts were
loaded and unloaded at the TRRR were outlined.
140
By February 1990, the
issues were said to be urgent with rectification work needing to be carried out as
soon as possible. The support track for the turntable was reportedly
disintegrating fast, with further wheels needed and the cost of labour and
maintenance growing daily. The table was also unable to be driven properly
when wet. Further, the ride was unable to be operated with less than two people,
and in quiet times, the rafts had to be kept moving as there was nowhere to hold
an empty raft. The maintenance cost of the current system was $25,000 per
year.
113. An air operated holding and control system was costed to replace the current
turntable system. This would allow the rafts to be home when the activity of the
ride was zero. The cost of the modification was thought to be less than $5000. It
was expected that the new system would be installed before the Easter Holidays.
114. Evidence from employees at the time suggests that Mr. John Angilley was
involved in the removal of the turntable and the subsequent redesign of the load
and unload areas.
141
Whilst it is not entirely clear when this significant change
was undertaken, evidence suggests that it may have been in the 1990s.
142
According to Mr. Tan, the modification took place between 1988 and 1990, and
was done as the drive was slipping during wet weather, the bearings were
constantly failing due to its submerged operation, and the inadequate fixings of
the guide tracks required frequent attention and repairs.
143
115. Following the removal of the turntable, it appears that the support railings were
installed in the trough near the unload area at the end of the conveyor.
144
It
seems from the outset, the railings were bolted and welded to the trough, and
were required to be checked every day as part of the daily inspections.
145
During
the inquest, Mr. Angilley stated, to the best of his recollection, the steel support
railings were initially placed as close as possible to the end of the conveyor
limiting the gap, however, he was unable to recall the distance with any
certainty.
146
Pumps
116. In a memorandum from Mr. Len Shaw, Maintenance Manager, to Mr. Wes
Hepburn dated 23 November 1987, titled, Memorandum 23 November 1987 –
Rapid Ride Pumps, issues were raised with the ‘imbalance of loading’ on the
TRRR pumps.
147
This seems to have been a recurring issue, at least since 18
November 1987, following which daily tests had been carried out to try and
determine the cause.
140
Ex C9(168)
141
Ex B17(3), [11]
142
Ex B17(3), [15]; T28-34 & 35
143
Ex B3C(54), pg. 8
144
T28-33, lines 5-30
145
Ex B17(3), [15]
146
T28-34, lines 25-40; T28-39, lines 20-40
147
Ex C4(5), pg. 856
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 29 of 274
117. On 22 January, both pumps had to be stopped and started again in a short period
of time. On the first occasion, the No. 2 pump shut down by electrical overload.
This pump was able to restart a short time later. After a few minutes it was noted
that the electrical load on the No. 1 pump was very heavy, and the pump was
restarted. It was suspected that a ‘whirlpool’ at the suction point may be the
cause of the issue, which could be rectified if modifications were made to the
pump well.
148
118. Further similar tests were to be conducted over the next few days with differing
time lapses. If the findings supported the suspected cause, it was proposed that
steps be taken to improve the installation, ‘along with the proposal to modify the
conveyor within the next few weeks’.
149
Operation Control Panel Modifications
119. From a memorandum directed to Mr. Bob Tan, Mr. Steve Romer and Mr. John
Angilley from Mr. Greg Handley on 26 June 1998, titled, Memorandum 26 June
1998 – Operator panel upgrade, it seems that the main Operator controls at the
TRRR were upgraded, and appeared as was found by Investigators at the time
of the incident
150
This allowed the panel to be operated by way of a start key,
with indicators and switches pertaining to the North and South Pump, motor
current, conveyor, cave lights, air pressure and the automatic sequence of the
ride.
151
120. It was noted that the emergency stop was to be positioned separately to the main
panel, but in close reach to the Operator.
152
The location was to be selected by
Operations. The activation of the emergency stop would commence the following
steps - (1) shut down the North Pump only, (2) Stop the conveyor, but allow the
Operator to restart the conveyor at any time; and (3) Close the emergency
gate.
153
Raft Collar Quote
121. Documentation shows that in September 2015, a quote was sourced from
Dynamic Attractions as to three new floatation collars with a modified lashing
strap for the rafts at the TRRR.
154
Dynamic Attractions offer a wide range of
engineering, design and building solutions for the amusement industry.
155
122. In June 2016, a further quote was prepared by Dynamic Attractions for ‘River
Rapids Replacement Boats for Dreamworld’.
156
This proposal states that
Dreamworld had requested a quote for 12 replacement fibreglass boats for the
TRRR. They were to be identical to those currently in use, so as to ‘maintain the
look of the fleet and allow Dreamworld to continue to use all of the same parts
and attachments’.
157
Per boat, it was estimated that the cost would be
148
Ex C4(5), pg. 857
149
Ex C4(5), pg. 857
150
Ex B12(1)
151
Ex B12(1), pg. 1 -3
152
Ex B12(1), pg. 3
153
Ex B12(1), pg. 3
154
Ex B15(3)
155
Ex B15(4), pg. 4
156
Ex B15(4)
157
Ex B15(4), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 30 of 274
$12,125.
158
123. From the documentation provided and evidence given during the inquest, it is
not clear as to the reason this quote was sourced, and why it was not actioned.
General Feasible Improvements
124. A document dated the 11 October 2004, titled, ‘Thunder River Rapids Ride’
159
shows clearly that the following feasible improvements to the ride were being
considered at that time:
1) Consider and analyse the impact if E-Stop is changed to stop
both pumps instead of the current 1 pump.
2) Install a second E-Stop switch at Unload area.
3) Institute timer permitted despatch to both despatch stations.
4) Fabricate and install an additional ‘Raft Hold’ device at
location prior to the current unload location. Investigate:
a. Alarm if second gate occupied
b. Then followed by Conveyor Slow down
c. Then followed by Pumps stopping
5) Overhead Handrails with strap grips (similar to types for
bus/train standing passengers)
6) Design a device to power rotate raft at the current Unload
station – rollers at far end, and a powered conveyor on
platform side c/w self-homing feature.
125. It is not clear who authored this memorandum or the reason it was drafted. It is
evident from the configuration and state of the ride at the time of the tragic
incident that only some of the improvements were considered and had been
implemented in the 12 years since.
Changes to the Unload Area
126. Photographs within other records held by Dreamworld demonstrate the
difference following upgrades to the unload area of the TRRR.
160
A photograph
dated 14 May 2005 suggests that a wooden platform used to jut from the
unloading area back towards the conveyor. A further photograph dated 25
February 2006 shows a permanent concrete structure where the timber boards
used to be utilised.
161
Raft Track
127. In accordance with a Memorandum dated 25 January 1988 titled, ‘Rapid Ride
Loading Dock Raft Track’, on 12 January 1988, the load and unload dock raft
158
Ex B15(4), pg. 6
159
Ex B15(7)
160
Ex B12(1), pg. 11-13
161
Ex B12(1), pg. 13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 31 of 274

control arm track fractured, which resulted in 10 metres of track being
destroyed.
162
It was suspected that the support arm suffered a collapsed bearing.
The track was rebuilt overnight and normal operations commenced on 13
January 1988. The faulty bearing and wheel were replaced.
Conveyor Chain Break and Raft Slip Monitoring
128. In August 2015, following a risk assessment conducted by the Safety Department
in July 2015 (outlined further at page 76 onwards), a scope of work for the
upgrades to the Conveyor Chain Break and Raft Slip were prepared.
163
These
upgrades were intended to take place at the bottom of the conveyor (beginning
of the incline). It does not appear that Mr. Deaves or any member of the E&T
Department were directly involved in the risk assessment conducted, although
some consultation on-site did take place following the process.
164
It does not
appear that discussions as to the risks associated with rafts slipping or colliding
at the top of the conveyor near the unload platform were ever conducted.
165
129. According to Mr. Ritchie, in early 2015, Mr. Deaves highlighted the need to
upgrade the conveyor system for the TRRR, during the course of an Engineering
Management Team meeting.
166
Mr. Ritchie was not aware of any previously
identified hazards or concerns at the top of the conveyor, nor had he been tasked
to review the safety mechanisms in that area.
167
It was discussed during this
meeting that the upgrade would consist of a replacement of the conveyor chain,
the design of an anti-rollback system and an upgrade to the control system,
which included a chain break alarm and a safety Programmable Logic Controller
(PLC).
168
130. Mr. Ritchie subsequently prepared a scope of work for the project, which was
intended to deal with control systems for the conveyor only, and included the
following upgrades:
- Installation of sensors to monitor the movement of the
conveyor system to detect a ‘chain break’, and to ‘detect the
presence of a raft at the bottom of the conveyor’.
169
The Safety
PLC to be used was intended to control the stopping and
starting of the conveyor, monitor for Chain Break of the
conveyor, monitor the position of rafts at the bottom of the
conveyor, and interlock with the main pumping system.
170
It
was noted that the PLC should also be adaptable to ‘control
and monitor the pumping systems along with the arrival and
dispatch gates (stage 2)’.
171
- The existing lanyard emergency stop devices were to be
adapted along with the existing local control panels to fit with
the new control system.
162
Ex C4(5), pg. 571
163
Ex B12(10) & (11)
164
Ex B3C(46), pg. 35 - 37
165
Ex B3C(46), pg. 46 & 47
166
Ex B3A(18), [94] & [95]
167
Ex C6(27), [60]
168
Ex B3A(18), [96]
169
Ex B12(11), pg. 1
170
Ex B12(11), pg. 1
171
Ex B12(11), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 32 of 274
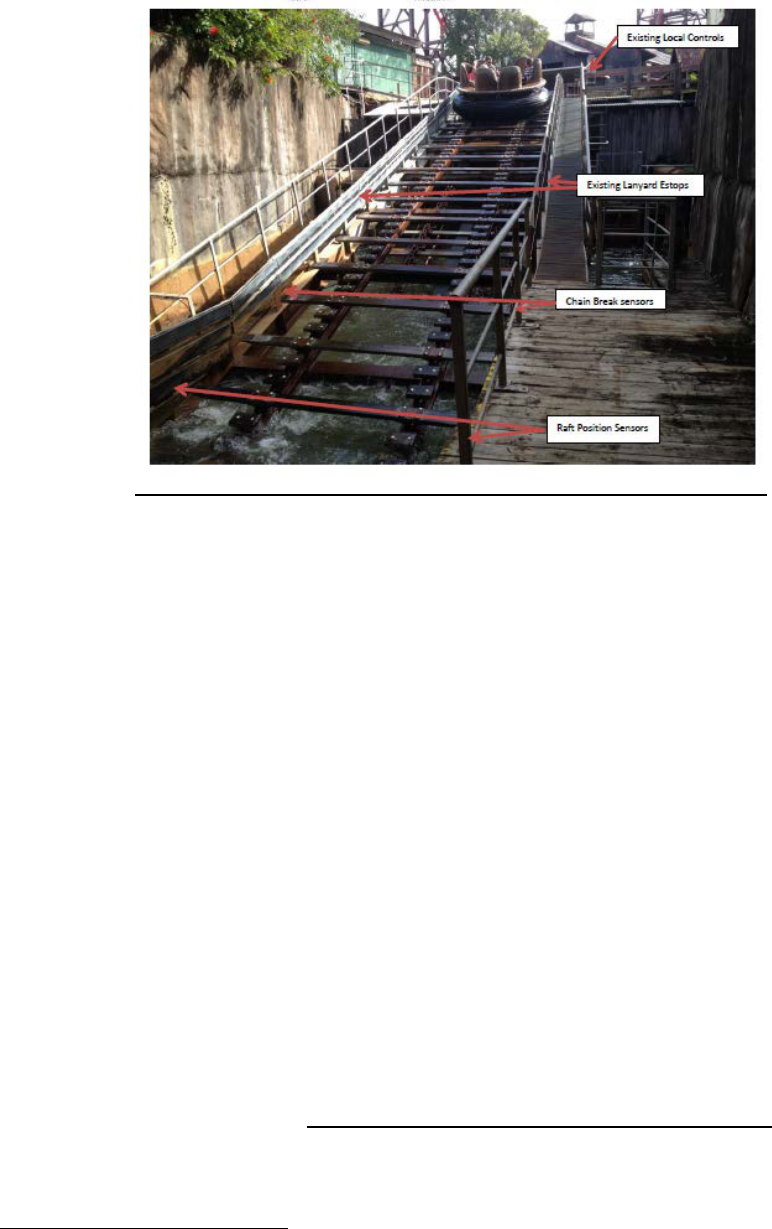
TRRR CONVEYOR CONTROLS UPGRADE OVERVIEW - EX B12 (11), PG. 2
131. It was also proposed that the scope of work be expanded to include an upgrade
of the Main Control Panel, as it had been ‘adapted and added to over many years
and are in a poor state’.
172
Mr. Ritchie clarified that he was referring to the
organisation of the wiring on the Main Control Panel as it was difficult to follow
and untidy.
173
The hardware was older and there was no colour coding,
numbering, labelling or features that would be expected for new wiring that
readily identifies the systems that each wire operates.
174
Furthermore, there
were no ‘as built’ electrical drawings, as well as different electrical components
that had different voltages in the same system.
175
Mr. Ritchie noted that these
aspects made reviewing the electrical components of the Main Control Panel
‘slow and time consuming’.
176
He did not consider, however, that the state of the
control panel adversely affected the safety or operation of the ride.
177
132. This upgrade was intended to include the following:
178
- The addition of a 7-inch Proface Touch Screen which would
monitor all alarms, monitor the water level and monitor the
pump loads; and
- Upgrade the controls of all arrival and exit gates.
133. It was estimated that the additional cost for this further component to the
upgrade, which would ‘future proof this system for years to come’ was
$10,000.
179
Mr. Ritchie was of the view that this increase to the scope of work
would allow for the necessary infrastructure to make the ride capable of future
automation projects, which may be considered, and would also improve the state
172
Ex B12(10)
173
Ex C6(28), [13]
174
Ex C6(28), [13]
175
Ex C6(28), [13]
176
Ex C6(28), [14]
177
Ex C6(28), [15]
178
Ex B12(10)
179
Ex B12(10); Ex C6(28), [29]-[31]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 33 of 274

of the wiring at the Main Control Panel, which would enable faster electrical fault
finding in the future.
180
134. In relation to the monitoring of the water level at the TRRR, Mr. Ritchie was of
the view that water level sensors could be installed, which would monitor the
operating efficiency of the pumps.
181
He was aware that the pumps for the TRRR
accounted for approximately 30% of Dreamworld’s overall electricity bill, and
such monitors may allow for the performance of the pumps to be adjusted to
increase or decrease the operating capacity, thereby leading to a significant cost
saving.
182
135. This memorandum was sent to Mr. Deaves by Mr. Ritchie via email.
183
Subsequent discussions were had whereby Mr. Deaves advised that whilst he
supported the additional work proposed, it could not proceed at this stage, with
the focus to remain on the upgrades to the bottom of the conveyor.
184
Mr. Ritchie
understood that the potential hazard identified at the bottom of the conveyor
needed to be rectified as a priority.
185
He did not consider that a delay to the
second stage of the project would have a negative impact on guests’ or
Operator’s safety.
186
136. Quotes were subsequently sought from Products for Industry (PFI) and Sage
Automation.
187
Ultimately, PFI was engaged to carry out the upgrades to the
TRRR, which included the following:
188
- Design the electrical integration of the PLC to perform the
following functions:
• Conveyor start/stop Operating including jogging
and override controls
• Chain Break Detection
• Raft Slip Detection
• Monitoring of the Lanyard Emergency stops
• Monitoring of the emergency stop at the local
control panel
- Replace the Existing Local Control panel
- Run new cabling to the local control panel and the ride
control station
- Install the Raft position spot 10 safety beam at the bottom of
the incline conveyor
- Install the Chain Break spot 10 Safety Beam further up the
incline to monitor the wooden cleats on the chain
180
Ex C6(28), [20]
181
Ex C6(28), [23] & [24]
182
Ex C6(28), [25]
183
Ex C6(28), [32]
184
Ex C6(28), [37] & [38]
185
Ex C6(28), [49]
186
Ex C6(28), [49]
187
Ex F1(13), pg. 1; Ex B16D(6)
188
Ex B12(9)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 34 of 274

- Supply all required electrical hardware and software
- Replace the existing local control panel with new panel &
controls and incorporate a new safety reset button
- Build and install a new Safety PLC Panel to install in the
main electrical control room
- New Safety PLC panel to incorporate redundant safety
contactors
- Also incorporate to interrupt the drive enable signal to stop
the drive before isolating safety contactors
- Program and Commission the Safety PLC
- Perform Safety Validation of the system and documentation
137. The purpose of these upgrades was to ensure that if a raft was stationary at the
base of the ride, it was detected and it would shut the conveyor drive down.
189
Detection of a break in the conveyor chain was also designed as part of the
upgrade, which by way of a sensor would shut down the conveyor motor.
190
The
plate and wiring of the local motor Control Panel was also replaced, with an
upgraded E-Stop installed at the unload area, which immediately stopped the
conveyor.
191
The controls for the conveyor at the Main Control Panel were also
rewired as part of the upgrade.
192
138. With respect to the function of the E-Stop, Mr. Ritchie consulted with Systems
Administrator, Ms. Horton, as to whether it should stop one of the pumps or the
conveyor.
193
It was determined that given the ability of the unload Operator to
see the conveyor and any associated issues, it would be best if the E-Stop only
allowed for a hard stop of the conveyor, with control of the pumps retained by
the Operator at the Main Control Panel.
194
139. PFI was not asked to install a water level monitor on the TRRR.
195
It was noted
that there was a request in the scope of works to include a pump interlock in
Stage 2 of the upgrade, however, there was no date stipulated as to when this
would commence.
196
Mr. Ritchie notes that these upgrades were discussed
during the site visit conducted by PFI in August 2015, however, were not to be
implemented until after the first upgrade had been successfully implemented.
197
189
Ex C4(12), [21]
190
Ex C4(12), [22]
191
Ex C4(12), [24]
192
Ex C4(12), [25]
193
Ex C6(28), [168] – [170]
194
Ex C6(28), [170]
195
Ex B3C(43), [13]
196
Ex B3C(43), [15]
197
Ex B3A(18), [101]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 35 of 274
140. The conveyor upgrades were commenced on 8 February 2016, and completed
within a week.
198
In March 2016, PFI was requested to return to site and make
the following modifications to the system:
199
• Raft stop timer to be extended by 15 seconds at the bottom of the
conveyor;
• Installation of an audible alarm on the Operator’s Panel if the conveyor
failed;
• Syncing the emergency dispatch gate with the audible alarm if the
conveyor stopped to automatically shut the dispatch gates to prevent the
further dispatch of rafts;
• Ride enable key must be in to start the conveyor; and
• Location of chain break sensors lowered by 20 mm.
141. Changes to the relevant management documents relating to the TRRR following
the above modifications were completed by Mr. Ritchie and Mr. John Lossie at
the request of Mr. Deaves.
200
These documents included technical drawings of
the work completed, changes and updates to the operating procedures, changes
to the service and maintenance procedures and task sheets, as well as details
as to the training to be undertaken by the Operator.
201
Two additional checks
were added to the daily and weekly maintenance checklists for the TRRR
following the modifications.
202
142. A completion memorandum was subsequently completed by Mr. Ritchie, which
was provided to E&T staff only, which explained the changes to the conveyor
control system.
203
On-site training was also provided to E&T staff by Mr. Ritchie
demonstrating the changes made as detailed in the completion memorandum. It
is unclear if any records were retained detailing who undertook this training and
were provided with the memorandum.
204
143. During the inquest, Engineer, Mr. Matthew Sullivan from PFI, gave evidence that
some of the spare safety inputs available following the conveyor upgrade could
have been used for a safe water level monitoring system.
205
PFI Modifications to the Log Ride in 2013
144. PFI had previously been engaged by Mr. Deaves to undertake upgrades to the
Log Ride in October 2013, which included the installation of a water level monitor
by way of two probes sending an electric signal to the PLC that registered the
level.
206
It was noted that the water monitoring was an ‘important feature’ of the
Log Ride as it was crucial to stopping the boats as they came off the conveyor.
207
198
Ex C4(12), [28]
199
Ex B3C(38), [47] & [48]; Ex F1(4)
200
Ex B3A(18), [112] & [114]
201
Ex B3A(18), [112]
202
Ex B3C(53), pg. 21 & 22; Ex E(242)
203
Ex C6(28), [172]
204
Ex C6(28), [173]
205
T16-27, lines 3-35
206
Ex B3C(43), [8] & [9]; Ex C4(12), [10]; Ex B3C(46), pg. 49
207
Ex B3C(43), [10]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 36 of 274
Mr. Deaves claims that these upgrades came about after he reviewed the ride
controls to consider having one Operator instead of two.
208
He was made aware
of concerns as to a raft coming over the top of the conveyor and colliding with
another at 70 kmph, and thought that a control system would be necessary to
prevent this from occurring.
209
He subsequently approached PFI to have it
designed. Mr. Deaves describes the manner in which this upgrade came about
as ‘ad hoc’ and in passing, rather than by way of a formal meeting or identified
risk, which needed to be rectified.
210
145. The scope of work also included monitoring the movements of the boats at the
top and bottom of the slide, which was to avoid collisions by way of block
controls.
211
The purpose of these controls was to ensure that only one boat
entered an area at any given time by way of a sensor at the start and exit point
of a designated area.
212
On the Log Ride, this included a block control at the top
of the slide and another at the bottom, which was designed to prevent a boat
being at the base and another coming towards it and resulting in a collision.
213
146. The cost of all of the modifications to the Log Ride, which in addition to the above
also included manual reset buttons and overrides, was $16,000.
214
Other Suggested Modifications to the TRRR
147. Records provided by Ardent Leisure during the course of the coronial
investigation suggest that further modifications were considered for the TRRR.
Unfortunately, these documents were provided without any context or further
records explaining the content or reasoning as to why modifications were
examined, nor the decision not to proceed. For completeness, and to highlight
the proposed changes, details as to the modifications are outlined below.
Automated Raft Rotation System
148. Minutes from the Executive Safety Committee Meetings held in February 2004,
suggest that consideration was given to a redesign and costing of an automated
raft rotation system, which was to be included in the 2005 budget.
215
It appears
that Mr. Tan and Mr. Angilley were responsible for this project. Unfortunately,
whilst this project is subsequently mentioned in minutes from a further meeting
in September 2004, it is not clear why this project did not proceed. In the minutes
from the September meeting, it states that ‘issue to be reviewed Feb’ 05.
Meantime operator training techniques to be used’.
216
Whilst the issue remains
an agenda item for the November 2004 meeting, the notation states, ‘design and
costing required for an automated raft rotation system. Work in progress in light
of recent events’.
217
It is not clear what the context of this notation was, and why
the project did not eventuate.
208
Ex B3C(46), pg. 50
209
Ex B3C(46), pg. 50 & 51
210
Ex B3C(46), pg. 50 & 51
211
Ex C4(12), [6]
212
Ex C4(12), [6]
213
Ex C4(12), [6]
214
Ex C4(12), [11]
215
Ex C9(82)
216
Ex C9(86)
217
Ex C9(88)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 37 of 274

Single Button Shutdown
149. According to Ms. Horton, she made a suggestion that a single stop button be
installed on the TRRR, as opposed to the four button shutdown sequence, which
needed to be undertaken by the Ride Operator at the Main Control Panel.
218
Whilst this proposal wasn’t made due to any safety concerns, Ms. Horton thought
this would make the process simpler for Ride Operators.
219
150. On 6 May 2016, an email was sent from Mr. Jason Johns on behalf of the
‘Dreamworld Attractions Supervisors’ to Mr. Lossie and Mr. Fyfe, which raised
the possibility of the four step emergency shutdown procedure for the TRRR
being changed to one step.
220
The four steps taken to shut down the ride were
as follows:
I. Press Emergency Gate Button;
II. Press Conveyor Stop;
III. Press Emergency Stop; and then
IV. Press Rapid Ride alarm button.
151. On the same day, Mr. Lossie replied stating that he would ‘look into what would
be required for this to be a one push button’.
221
152. According to Mr. Johns, this request was made at the behest of Mr. Fyfe, who
asked that he explore the possibility of simplifying the shutdown process.
222
153. Prior to the tragic incident, this simplification of the shutdown process had not
been implemented on the TRRR. At the inquest, Mr. Johns confirmed that he
had not received any further correspondence about the issue, however, he
acknowledged that it was not actioned.
223
Sourcing Further Wood for Conveyor in 2016
154. An email from Mr. Naumann to Gooding Timber dated 30 March 2016, suggests
that pricing was sought for 70 lengths of F14 Hardwood timber.
224
A
representative from Gooding Timber subsequently queried whether the wood
was being used for inside or outside, as this would be relevant to determining
the most suitable product.
155. When questioned as to how and why this quote was sourced during the inquest,
Mr. Naumann stated that he thought it may have been based on his assessment
of what was required and also previous ordering history.
225
He ‘wasn’t sure’
whether it would be pivotal to advise the supplier that the wood was being used
for a water based amusement ride.
226
218
Ex B3C(27), [8] & [9]
219
Ex B3C(27), [12]
220
Ex F12(853), pg. 2
221
Ex F12(853), pg. 1
222
T15-77, lines 5-25
223
T15-78, lines 27-45
224
Ex E(76)
225
T11-49, lines 1-15
226
T11-49, lines 15-20
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 38 of 274

156. In an update email sent by Mr. Naumann to Mr. Watkins and Mr. Cox dated 6
May 2016, he noted that ‘we have started alternating the planks on installation –
new then, good condition old’.
227
When asked for the rationale as to this
approach to replacing the planks, Mr. Naumann was unable to recall the
reasoning.
228
He did state, however, that to the best of his recollection, conveyor
slats with ‘excessive bowing’ were replaced during the 2016 annual shutdown of
the TRRR.
229
TRAINING & OPERATOR PROCEDURES
157. For each of the rides at Dreamworld, specific Operating Procedure Manuals were
drafted by the Operations Department, with final approval provided by Mr.
Margetts. Memorandums were also used to update the Operating Procedures
for each ride. These were displayed on a memorandum board.
230
Ride Operators
were then retrained on the change in procedure, which was noted on a roster
kept with the Supervisors.
231
158. For each of the attractions at Dreamworld, ride specific training was provided in-
house to new Ride Operators.
232
This was undertaken by Senior Ride Instructors
(level 4), who were experienced Ride Operators that had been trained in each
level of ride operation.
233
It does not appear that they were required to hold any
formal training qualifications or undertake any external course, which would be
recognised outside of the Theme Park. That being the case, evidence suggests
that internal courses were offered for Instructing Operators, such as the ‘Train
the Trainer’, which was conducted at Dreamworld in mid-2016 for all of the
Instructing Operators.
234
This course was conducted one day a week for three
hours over a 10 week period.
235
159. Senior Ride Instructors were required to provide instruction to Ride Operators
safely and efficiently, whilst also mentoring and training staff on an as required
basis.
236
They were also expected to identify and report methods for continuous
improvement within the Department and business, as well as any hazards or
incidents as identified.
237
One of the key responsibilities of an instructor was to
maintain Dreamworld’s high standards of practice and safety by ensuring ‘that
your trainee is aware of these safety commitments and they are appropriately
trained in all safety matters’.
238
160. Instructors were required to have one to two years’ exemplary performance in
ride operation.
239
However, evidence provided by various staff during the
investigation and inquest suggested that there was no enforced set timeframe
as to when a Ride Operator could progress to becoming an Instructing Operator.
For example, Ms. Amy Crisp progressed to a training position within a year of
commencing her employment as a Ride Operator with Dreamworld, although she
227
Ex E(91)
228
T11-49, lines 20-32
229
T11-79, lines 5-30
230
Ex B3A(21), pg. 20
231
Ex B3A(21), pg. 21
232
Ex B3A(11), [4]
233
Ex B3A(14), pg. 3
234
Ex C6(46), [20]
235
Ex C6(46), [20]
236
Ex B12(3), pg. 1
237
Ex B12(3), pg. 2
238
Ex B12(4), pg. 10
239
Ex B12(3), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 39 of 274

noted that it normally took staff longer to achieve this.
240
161. Practically, before a Ride Operator could become an Instructing Operator, they
were required to watch other training sessions provided to staff, and would then
be observed on at least three different training sessions they provided to new
Ride Operators.
241
Once the trainer is deemed to be competent by senior staff,
they are allowed to train Ride Operators without supervision.
242
162. If an Instructor discovers an issue with a procedure or a correction, which needs
to be made, there is a suggestion form that can be completed and provided to a
Supervisor to be actioned.
243
163. Instructors were also involved in the auditing of staff, to ensure Ride Operators
were still competent and to identify whether any further training may be
required.
244
This generally involved computer based and practical on-site
observation of the Ride Operator.
245
164. At the time of the incident, it was estimated that there were eight Instructing
Operators, six of whom were competent to train all staff on all rides. The Log
Ride and TRRR were the last rides that were taught to Ride Operators and
Instructors, due to the ‘higher responsibility’.
246
165. The manner in which this training was provided by the Instructing Operator was
largely based on how and what the Instructor had been shown when they were
a Ride Operator, and comprised of on-site practical training whilst the ride was
in operation with the Instructor, with a run through of the procedures specified in
the applicable operating procedure manual discussed and demonstrated before
the ride opened.
247
There was no checklist provided to the Instructor as to topics
to be covered during a training session for the ride, rather only a Training
Register, which was signed off at the end of the session.
248
The Operating
Procedure Manual for a ride was intended to outline the processes to be followed
when operating the ride and responding to different scenarios that may arise,
including emergencies specific to that attraction. The duration of the training
largely depended on the type and complexity of the ride. Trainers were required
to make an assessment of the trainee to determine if they were comfortable
operating the ride.
249
166. When training a staff member in the operation of a ride, it was a requirement of
Dreamworld policy that a ‘Training Register’ sheet be completed in full.
250
This
form states the day and time the employee was trained in a particular role on a
ride, and was only to be signed by the trainee if ‘they are confident that they know
and understand the procedure’.
251
The instructor is also only to sign the form if
they are ‘confident that the operator knows and understands the procedure and
is able to operate the ride confidently’.
252
In the Instructor Handbook developed
240
Ex B3A(14), pg. 5
241
Ex B3A(14), pg. 4
242
Ex B3A(14), pg. 4
243
Ex B12(4), pg. 6
244
Ex B3A(14), pg. 6
245
Ex B3A(14), pg. 9
246
Ex B3A(14), pg. 7
247
Ex B3F(3), [5]
248
Ex B3A(14), pg. 22 & 23
249
Ex B3A(14), pg. 9
250
Ex B12(4), pg. 5
251
Ex B12(4), pg. 5
252
Ex B12(4), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 40 of 274

by Dreamworld, there is advice provided to Instructors as to the different adult
learning styles and modalities.
253
167. The different levels of Operators on a ride indicate the different levels of training
and familiarity and seniority in relation to rides. There are requirements as to
what level a Ride Operator must be to work on particular rides, with some simple
rides only requiring a level 1 Operator.
168. Any change in procedure for a ride, requires that the Ride Operators be briefly
re-trained on the new procedure (usually within 15 minutes), which would be
recorded in a Training Register.
254
TRRR Position Responsibilities and Training
169. It was well-known that the Tower of Terror, Log Ride and TRRR were the most
complex rides to operate within the Theme Park, as the Ride Operators had the
most responsibility. Accordingly, a Level 3 (No. 1) Operator was necessary to
control the ride.
255
Like the Log Ride, the TRRR was said to have a number of
manual elements to its operation as opposed to automated controls, which made
the ride more difficult to operate.
256
The panel for the ride was described by Relief
Supervisor, and experienced Ride Operator, Ms. Cotter as being a ‘very complex
panel’.
257
170. At the TRRR, there were three possible Operator positions, with a maximum of
four staff manning the ride on a given day. The number of staff required to
operate the ride was dependent on the number of rafts in circulation, and the
expected volume of guests.
171. The staffing positions and configuration, which are detailed in the Operator
Procedure Manual for the ride, were as follows:
258
253
Ex B12(4), pg. 7-9
254
Ex C7(541); Ex B3A(11), [69]
255
Ex B3A(21), pg. 12; T6-95, lines 30-40
256
Ex B3A(21), pg. 12 & 13; T6-96, lines 1-5
257
T6-96, lines 5
258
Ex D4(102), pg. 4, sections 3.3.1 Operator Procedure Manual – Load Operator & Ex D4(103), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 41 of 274
2 staff present (operator and load operator)
(i) 1 at main control panel (load)
(ii) 1 at unload
3 staff present (operator, load and deckhand)
(i) 1 at main control panel (load)
(ii) 1 at unload
(iii) Deckhand at dispatch and roving queue line and assisting with
ride express
4 staff present (operator, load and deckhands)
(i) 1 at main control panel (load)
(ii) 1 at unload
(iii) Deckhand 1 at dispatch
(iv) Deckhand 2 roving queue line and assisting with Ride Express
172. The responsibilities for each position were outlined in role specific Operator
Procedure Manuals. The duration of the training provided for each position is
dependent on the level of responsibility. Primary responsibility for the operation
of the ride remained with the Level 3 Operator (No. 1), who also had a
supervisory responsibility over the Level 2 and Level 1 Operators.
259
173. Ms. Horton was responsible for drafting updates to the Operator Procedure
Manual for the TRRR, which came into effect in June 2016.
260
The reason for
the updates to the procedure was to reflect recent engineering changes to the
conveyor operating system, which prevented rafts from rolling back on the
conveyor.
261
All Operators were subsequently trained in the draft and
implemented changes to the Operator Procedure Manual.
262
At inquest, Ms.
Horton stated that whilst she considered the entire contents of the Procedure
Manual, she wasn’t aware of any associated memorandums that may be
applicable, as these had not been saved on the document management system,
Liferay.
263
The Safety Department was not involved in the drafting of any
operating procedures.
264
174. In order to demonstrate the time-frame in which the Operators for the TRRR had
to perform their respective functions and tasks, the following table demonstrates
the cycle times for the ride, as was documented within the operating procedures
maintained at the ride:
265
AVERAGE CYCLE TIMES
Cycles per hour
Guests per hour
Minutes per cycle
Non Holiday
83.4
458
0.72
Holiday
113
626
0.5
259
Ex B3A(2), pg. 5; Ex D4(102), pg. 4
260
Ex B3C(25), [3]; Ex B3C(26), [3]
261
Ex B3C(25), [3]
262
Ex B3C(26), [7]
263
T25-21, lines 5-35
264
T25-24, lines 40-48
265
Ex F19(1), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 42 of 274

175. The roles and responsibilities of each of the Operator positions at the ride are
outlined below.
Ride Operator Level 1 (No. 3) Deckhand
176. The Operations Procedure Manual (Rapid Ride Deckhand Operation) states that
the Deckhand will be positioned at the dispatch control panel and queue line, to
ensure all guests’ belts are secured, and to press and hold the dispatch jack
button until the raft has left the jacks.
177. As part of the Operator Procedure Manual, there was also a Rapid Ride Operator
Training component.
266
This document seems to apply to the training of the
Deckhand position at the TRRR. Section 3.2 of the procedure requires that the
training session should be a minimum of 1.5 hours, with 3.2.2 stipulating that
Instructing Operators and Attractions Supervisors ‘must never leave any person
to operate any equipment unless fully competent. If any doubt exists as to the
trainee’s level of competence, the Instructor is to extend the duration of the
training session.’
267
Sections 3.4 of the Procedure requires that the operating
procedures as outlined in the manual be explained, as well as ‘all of the
emergency and operational/Code 6 procedures’ (3.4.6).
268
The assessment is to
ensure that the trainee knows and understands each of the points covered in the
training session and once satisfied, the instructor is to assess the trainee’s
competency through at least two ride cycles before signing the Attractions
Training Register.
178. The Operating Procedure Manual for the Deckhand position is five pages in
length.
269
The relevant portions for the purpose of this coronial investigation are
as follows:
3.1.6 No 1 operator will ensure deckhand/s are aware of the
following:
(i) How to shut down the ride as per 3.4.4
(ii) Location of telephones to call for assistance and the Emergency
telephone number (222)
(i) How to advise guests of delay
(ii) Location of all emergency equipment, Emergency exits, and
Evacuation Zones
(iii) Number of rafts in circuit
3.2 Start Up
3.2.1 No.1 Operator is responsible for the startup of the ride
3.2.2 Check with No. 1 Operator for any specific operating instructions
for the day
266
Ex C6(47), pg. 9
267
Ex C6(47), pg. 10
268
Ex C6(47), pg. 10
269
Ex D16(6), pg. 1-5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 43 of 274
3.4 Operating Problems
3.4.1 Any operating problems must be reported immediately to the
No. 1 Operator. No raft should be dispatched if it has the
potential for risk to either:
(i) Guest/Staff safety or wellbeing
(ii) Ride operating conditions
(iii) Damage to ride equipment
3.4.3 No. 1 Operator initiate shut down
Advise the No.1 Operator immediately if any of the following problems
arise. No.1 Operator will ensure the rapid ride is shut down in the event
of any of the following
(i) Loss of power to one or both pumps
(ii) Loss of power to the conveyor
(iii) Conveyor chain break
(iv) Raft stall bottom of conveyor
(v) Raft jam
(vi) Raft slips on the conveyor
(vii) Load/unload jacks jam closed
(viii) Any situation where there is a risk of serious injury to guests or
Staff
(ix) Any situation where there is risk of damage to ride equipment
3.4.4 Shut Down Operation
No. 1 Operator and or a Supervisor may direct Deckhand to shut down
the ride in an emergency. Proceed to:
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press Emergency stop
(iv) Remove dispatch isolator key
(v) Call control via 325 stating the nature of your call
(vi) Await further instructions from a Supervisor
3.5 Periodic Checks
3.5.1 Monitor raft air pressure and condition of tubes. Report any
faults or problems to No. 1 Operator.
3.5.2 Monitor water level. Report any faults or problems to No. 1
Operator
3.5.3 Monitor the operation of all jacks. Report any faults or problems
to No. 1 Operator
3.5.4 Monitor the queue lines for guests under the age of 2 years and
Ride Express queue line
3.5.5 Monitor the ride for unusual sounds or smells during normal
operation. Report any faults or changes to No. 1 Operator
3.5.6 Ensure that the ride and the queue line areas are kept clean and
tidy at all times
179. Although the responsibilities of the Deckhand are limited and the training
relatively short, it appears from the requirements of the procedure that the
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 44 of 274

employee is required to be conversant with their responsibilities in respect of the
above competencies.
180. None of the prescribed procedures for this position give the Deckhand the
authority to take action in an emergency situation, without the direction of the No.
1 Operator.
Ride Operator Level 2 (No. 2) Load Operation
181. The training for a No. 2 Operator on any given ride generally involved training
on-site for between 1 ½ to 2 hours, which was consistent across the Theme
Park.
270
However, if an Instructing Operator was of the view a trainee required
additional time to complete the training to the requisite level, this could be
requested.
271
182. According to the ‘Attractions Training Register’ for the No. 2 Operator position at
the TRRR, Parts 3.1-3.8 of the Operator Procedure Manual were required to be
canvassed during training.
272
These sections of the Manual cover the following
topics:
• 3.1 – Opening
• 3.2 – Start up
• 3.3 – Operating
• 3.4 - Operating Problems
• 3.5 – Periodic Checks
• 3.6 – Emergency
• 3.7 – Closing
• 3.8 – Spiels
• Lock-out tag-out
183. The Operating Procedure Manual for the No. 2 load Operator position is 16
pages in length.
273
The relevant portions of the Manual for the purpose of this
coronial investigation are as follows:
3.1.7 Operator will ensure load operator is aware of the following
(i) How to shut down the ride in the event of an Emergency where
the No. 1 Operator is incapacitated (shut down procedure)
(ii) Location of the telephones to call for assistance and the
Emergency telephone number (222)
(iii) How to advise guests of a delay
(iv) Location of all Emergency equipment, Emergency exits, and
evacuation zones
(v) Number of rafts in circuit
3.2 Start Up
3.2.1 No. 1 Operator is responsible for the start up of the ride
3.2.2 Check with No. 1 Operator for any specific operating instructions
for the day
270
Ex B3A(21), pg. 11; Ex C7(541); Ex B3A(2), pg. 4
271
Ex B3A(14), pg. 16
272
Ex C7(541), pg. 6
273
Ex D4(102)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 45 of 274
3.2.3 Assist No. 1 Operator in dispatching rafts for test run
3.2.4 Open the Queue at the prescribed opening time
3.3.1 Staff positioning
…
NOTE: The No. 1 Operator is responsible for the operation of the ride
including the actions of load operator and deckhand/s. The Operator
will be vigilant of operators and ensure all staff rotate positioning (where
possible).
3.3.7 Load Operation (positioned main control panel)
3.3.8 Advise guests to remain behind yellow line until directed to enter
NOTE: Operators must ensure rafts are positioned correctly for
guests to enter/exit safely. Operators may press jack buttons to
turn rafts for correct positioning as necessary. Under no
circumstances are guests permitted to climb over seats to
load/unload.
3.3.9 Advise guests load spiel as per section 3.8.1. Ensure guests are
advised to take care when boarding the raft as the floor may be
slippery and request back/rear seats be filled first
3.3.10 Ensure guests load the raft one at a time
3.3.11 Fill every raft where possible utilising guest from the single/pairs
and Ride Express queue lines
3.3.12 Ensure belt extensions are given to adults accompanying
children if required
NOTE: Ensure the raft is balanced evenly
3.3.13 Ensure loose belongings are stored in the centre of the raft
3.3.14 Advise guests of belt instructions spiel as per 3.8.2
3.3.15 Check all belts are secured correctly
NOTE: A raft must not be dispatched until all belts are secured…
3.3.16 Advise guests of dispatch spiel as per section 3.8.3…
3.3.17 Press ‘load’ jack button on the main control panel (bar)
3.3.18 Hold ‘load’ jack button until the raft has left the jacks
NOTE: to ensure adequate raft spacing, the ‘dispatch’ jack has
an automatic minimum 35 sec delay. ‘Load 2’ button will
illuminate once raft is ready for dispatch. Rafts are unable to be
dispatch until the ‘Load 2’ button (dispatch) illuminates and an
audible alarm sounds.
3.3.19 Press and hold ‘Load 2’ button (dispatch) on the main control
panel until the raft has left the jacks
NOTE: Jacks will automatically close once raft passes dispatch
jack
NOTE: Minimum three rafts must be kept within sight of the No.
1 operator at all times. This is the area between conveyor and
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 46 of 274
dispatch area.
3.3.20 Load Operators must ensure they are watching camera.
Cameras must be checked prior to each raft being sent and in
any lag time between rafts being sent. Load Operators must be
vigilant of raft movements, conveyor operation and ensure no
obstructions exists. If in doubt of operating conditions, stop
dispatching. Contact a Supervisor via Control stating ‘Rapids –
Operational’ and await further operating instructions.
3.3.21 Unload operation (positioned unload control panel)
3.3.22 Advise guests to remain seated with belts secured until the raft
completely stops at the unload area (exit)
3.3.23 Once the raft stops at arrival jack, press ‘arrival jack’ button. This
will move the raft to the unload
3.3.24 Monitor the raft as it moves through, again advise guests to
remain seated with belts secured until the raft completely stops
at the unload area (exit)
NOTE: Operators must ensure rafts are positioned correctly for
guests to enter/exit safely. Operators may press jack buttons to
turn rafts for correct positioning as necessary. Under no
circumstances are guests permitted to climb over seats to
load/unload
3.3.25 Advise guests of unload spiel as per section 3.8.4
3.3.26 Farewell all guests as they exit
3.3.27 Visually check no rubbish or loose items are left in the raft.
Remove as necessary
3.3.28 Press ‘unload’ jack button. This will move the raft to the load
area.
3.3.29 Hold ‘unload’ jack button until the raft has left the jacks
3.3.30 Repeat sections 3.3.2 to 3.3.30 for daily operation
3.4 Operating Problems
3.4.1 Any operating problem must be reported immediately to the No.
1 Operator. No raft should be dispatched if it has the potential
for risk to either:
(i) Guest/Staff safety or well being
(ii) Ride operating conditions
(iv) Damage to ride equipment
3.4.2 Operator Initiate Shut Down
Advise the Operator immediately if any of the following problems arise.
Operator will ensure the rapid ride is shut down in the event of any of
the following:
(i) Loss of power to one or both pumps
(ii) Loss of power to the conveyor
(iii) Conveyor chain break
(iv) Raft stall bottom of conveyor
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 47 of 274
(v) Raft jam
(vi) Raft slips on the conveyor
(vii) Load/unload jacks jam closed
(viii) Any situation where this is a risk of serious injury to Guests or
Staff
(ix) Any situation where there is risk of damage to ride equipment
3.4.3 Shut Down Operation
No. 1 Operator and or a Supervisor may direct load operator to shut
down the ride. Proceed to:
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press Emergency stop
(iv) Remove dispatch isolator key
(v) No. 1 Operator will give direction to load operator attend the
bottom of the conveyor and talk with guests until Engineering
and Supervisors attend
(vi) If a deckhand is present No.1 Operator will give direction to
attend to the queue line and apologise to the guests as per 3.8.5
(vii) Await further instructions from a Supervisor
NOTE: persons in water and or Raft capsized. Follow
emergency procedure sections 3.6.2
3.4.4 Two (2) Rafts Dispatched Together
(i) Press emergency gate button
(ii) Stop dispatching
(iii) Advise the No. 1 Operator
(iv) Monitor raft movements via video camera
(v) Await further instructions from No. 1 Operator and/or Supervisor
3.4.5 Loss of Air Pressure (Low air alarm)
(i) Advise the No. 1 Operator
(ii) Stop dispatching
(iii) Await further instructions from the No. 1 Operator
3.4.6 Motor over Current
NOTE: Audible and visual alarm will activate when current is
over 500 amps
(i) Advise the No. 1 Operator
(ii) Stop dispatching
(iii) Await further instructions from the No. 1 operator
3.4.7 Video Monitor Failure
(i) Advise the No. 1 Operator
(ii) Stop Dispatching
(iii) Await further instructions from the No. 1 operator
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 48 of 274
3.4.8 Raft stall bottom of conveyor
NOTE: conveyor will automatically stop in the event of a raft
stalling at the bottom of the conveyor. An audible alarm will be
heard from the panel and conveyor reset button will illuminate
(i) Advise the No. 1 Operator
(ii) Stop dispatching
(iii) Await further instructions from the No. 1 Operator
NOTE: Operators are not permitted to restart the conveyor. This
must be done by Engineering and/or Supervisors
3.4.9 Conveyor chain break
NOTE: Conveyor will automatically stop in the event of a chain
break. An audible alarm will be heard from the panel and
conveyor reseat button will illuminate
(i) Advise the No. 1 Operator
(ii) Stop dispatching
(iii) Await further instructions from the No. 1 operator
NOTE: Operators are not permitted to restart the conveyor. This
must be done by Engineering and/or Supervisors
3.5 Periodic Checks
3.5.1 Monitor raft movements, conveyor operation and ensure nothing
is obstructing the video monitor images. If in doubt of operating
conditions, stop dispatching and advise the No. 1 operator
3.5.2 Monitor cameras and load/unload platforms for persons in water
and or raft capsized. Follow procedure 3.6.2
3.5.3 Monitor rafts loading onto the conveyor and/or conveyor failure.
Advise the No. 1 Operator if an operating problem arises
3.5.4 Monitor raft air pressure and condition of tubes. Report any
faults or problems to No. 1 operator
3.5.5 Monitor water level. Report any faults or problems to the No. 1
operator
3.5.6 Monitor the operation of all jacks. Report any faults or problems
to No. 1 operator
3.5.7 Monitor North and South pump amps. If a pump readout is
above 500 amps advise the No. 1 operator
3.5.8 Monitor the queue line for guests under the age of 2 years
3.5.9 Monitor the ride for unusual sounds or smells during normal
operation. Report any faults or changes to the No. 1 Operator
3.5.10 Monitor the control panel. Report any faults or changes to the
No. 1 operator
3.5.11 Ensure that the ride and the queue line areas are kept clean and
tidy at all times
3.5.12 Monitor all riders during a cycle via the video monitor system.
Report any concerns to the No. 1 operator
3.5.13 Ensure video monitor displays all camera images at all times.
Report any faults or changes to the Operator
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 49 of 274
3.5.14 Monitor weather conditions. A Supervisor and/or the No. 1
Operator may advise to dispatch less frequently
3.5.15 Monitor ride express queue line and incorporate loading guests
in daily operation
3.6 Emergency
3.6.1 In the event of serious injury to a guest or staff member contact
the Emergency Station
Via telephone
(i) Contact the Emergency Station via telephone ‘222’
NOTE: Remain calm, speak slowly and clearly
(ii) State ‘who you are, where you are and the nature of the
emergency’
(iii) Ensure that you are the last to hang up the telephone
(iv) Await for the arrival of the ‘Emergency Response Team’
(v) If possible, control any bystanders and/or assist where possible
(vi) Retain any witnesses if possible
(vii) Advise the guests in the queue line of the delay
(viii) Complete all reports
Via two way
(i) Ensure the two way is turned ‘on’ and transmitting on channel
‘one’. Ensure that the two way volume is on high.
…
3.6.2 Persons in water and or Raft Capsized
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press emergency stop
(iv) Remove dispatch isolator key
(v) Press rapid ride alarm button
(vi) Contact the emergency station as per section 3.6.1
NOTE: the dispatch isolator key must be retained by the No. 1
operator at all times when the operator is away from the
operator’s panel
(vii) Throw a life buoy to the person (if possible)
(viii) No. 1 operator will give direction to attend the bottom of the
conveyor throw life buoy
NOTE: Ensure the dispatch isolator is given to the No. 1
Operator before leaving the area
(ix) If a deckhand is present, Operator will direct them to attend the
yellow gate, near the Car park B entry, to throw life buoy
(x) Await further instructions from a Supervisor
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 50 of 274

3.6.3 If the No. 1 Operator is injured or incapacitated load operator
will:
(i) Press emergency gate button
(ii) Press conveyor stop
(iii) Press emergency stop
(iv) Contact the emergency station as per section 3.6.1
(v) Stay at the control panel, await further instructions from a
Supervisor
NOTE: if a deckhand is present, give direction to proceed to the
conveyor to talk with guests and apologise for delay as per 3.8.5
184. Essentially, once the TRRR is operational, the No. 2 Operator has the same
tasks and periodic checks as the No. 1 Operator. Both are expected to swap
positions from the unload area and the Main Control Panel at regular intervals.
The No. 1 Operator, however, retains overall responsibility for the operation of
the ride. Unless the No. 1 Operator is incapacitated, or in certain specific
circumstances, such as a person is in the water or a raft is capsized, it is clear
that the No. 2 Operator does not have authority to complete certain tasks, such
as responding to operational issues and shutting down the ride, except at the
direction of the No. 1 Operator.
185. The training provided to staff for the No. 2 Operator role involves both verbal and
visual instruction on each of the requisite areas whilst at the ride. The trainee is
required to read through the Operations Procedure Manual, and any
memorandums or addendum to the procedure, which are maintained in a folder
at the ride. At the completion of the training, both the trainer and trainee complete
and sign the Attractions Training Register.
Ride Operator Level 3 (No. 1)
186. The No. 1 Operator for the TRRR held primary responsibility for the operation of
the ride, as well as supervisory duty for the No. 2 and No. 3 Operators.
187. Unlike the other positions for the ride, the training for the No. 1 Operator at the
TRRR, consisted of a full day (8 hours approximately), which was carried out
onsite with an Instructor whilst the ride was in operation.
274
This training was
described by Mr. Nemeth as ‘onsite training and they’re showing you step-by-
step what to do and then you have to demonstrate that you can operate the ride
in front of the instructor’.
275
The Instructor takes the trainee through the operating
procedure manual whilst onsite.
276
The following day, the Instructor also
observed the No. 1 Operator to open and close the ride.
188. The discrepancy of the training provided to the No. 1 and No.2 Operator is said
to reflect the greater responsibility placed on the No. 1 Operator, who is
responsible for the operation of the ride, and has some supervisory capacity over
the No. 2 Operator.
277
This was generally understood by staff trained in both
274
Ex B3A(2), pg. 5
275
Ex B3A(2), pg. 5
276
Ex C7(18)(a), pg. 43
277
Ex B3A(21), pg. 15 & 16
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 51 of 274

positions of the ride.
278
189. The Operations Procedure Manual for the ‘Rapid Ride Operator’ consisted of 18
pages.
279
It largely mirrors that of the No. 2 Operator with respect to the load and
unloading of guests, however, primary control for the operation of the ride rests
with the No. 1 Operator, including decisions as to operational issues and the
actions of the No. 2 and 3 Operators.
280
190. Relevant further portions of the Operating Procedure Manual for the No. 1
Operator are as follows:
3.4 Operating Problems
3.4.1 Any operating problem must be reported immediately to
your Supervisor if it has the potential for risk to either:
(i) Guest/Staff safety or well being
(ii) Ride operating condition
(iii) Damage to ride equipment
3.4.2 Operator Initiate Shut Down
The Rapid ride must be shut down if any of the following occur as
directed by a Supervisor
(i) Loss of power to one or both pumps
(ii) Loss of power to the conveyor
(iii) Conveyor chain break
(iv) Raft stall bottom of conveyor
(v) Raft jam
(vi) Raft slips on the conveyor
(vii) Load/unload jacks jam closed
(viii) Any situation where this is a risk of serious injury to Guests or
Staff
(ix) Any situation where there is risk of damage to ride equipment
3.4.3 Shut Down Operation
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press Emergency stop
(iv) Remove dispatch isolator key
(v) Contact control on 325 stating ‘Rapid Ride – Code 6’ and advise
why shutdown was initiated e.g. loss of power to conveyor
(vi) Direct Load operator to attend the bottom of the conveyor
(vii) If a deckhand is present direct them to attend the queue line and
advise guests of delay as per 3.8.5
(viii) Count how many rafts are retrieved (from conveyor to dispatch
control panel area)
(ix) Await further instructions from a Supervisor
(x) Advise guests of an operational delay as per section 3.8.5
278
Ex B3A(12), pg. 10
279
Ex D4(103)
280
Ex D4(103), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 52 of 274
(xi) Record downtime
NOTE: In the event of persons in water and or Raft capsized
follow emergency procedure sections 3.6.2
NOTE: Number of rafts in circuit is vital information for shutdown
procedure. Supervisors will contact operators to determine
exactly how many rafts are left in circuit to retrieve
3.4.4 Two (2) Rafts Dispatched Together
(i) Press emergency gate button
(ii) Stop dispatching
(iii) Contact a Supervisor via Control stating ‘Rapid Ride –
Operational’
(iv) Monitor raft movements via video camera
(v) Await further instructions from Supervisor
3.4.5 Loss of Air Pressure (Low air alarm)
(i) Stop dispatching
(ii) Contact a Supervisor via control stating ‘Rapid Ride – Code 6’
(iii) Press Emergency Gate Button
(iv) Remove dispatch isolator key
NOTE: The dispatch isolator key must be retained by the
operator at all times when the operator is away from the
operator’s panel
(v) Tie the front raft to the deck railing at the end of the dispatch
control panel area
(vi) Insert dispatch isolator key
(vii) Retrieve all rafts in circuit
(viii) Unload guests (only if safe to do so)
(ix) Switch off one pump by pressing red pump stop button (north or
south)
(x) Advise guests of an operational delay as per section 3.8.5
(xi) Await further instructions from a Supervisor
(xii) Record downtime
3.4.6 Motor over Current
NOTE: Audible and visual alarm will activate when current is
over 500 amps
(i) Stop dispatching
(ii) Contact a Supervisor via control stating ‘Rapids – Operation
ASAP’
(iii) Retrieve all rafts in circuit
(iv) Remove dispatch isolator key
(v) Advise guests of an operational delay as per section 3.8.5
(vi) Await further instructions from a Supervisor
(vii) Record downtime
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 53 of 274

3.4.7 Video Monitor Failure
(i) Stop Dispatching
(ii) Contact a Supervisor via Control stating ‘Rapids – Operational
ASAP’
(iii) Retrieve all rafts in circuit
(iv) Remove dispatch isolator key
(v) Advise guests of an operational delay as per section 3.8.5
(vi) Await further instructions from a Supervisor
(vii) Record downtime
NOTE: The Emergency stop button located on the pole at
the unload station will stop one pump and the conveyor
when pressed
3.4.8 Raft stall bottom of conveyor
NOTE: conveyor will automatically stop in the event of a raft
stalling at the bottom of the conveyor. An audible alarm will be
heard from the panel and conveyor reset button will illuminate
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press Emergency Stop
(iv) Remove dispatch isolator key
(v) Contact Control on 325 stating ‘Rapid Ride – Code 6’
(vi) Direct Load Operator to attend the bottom of the conveyor
(vii) If a Deckhand is present direct them to attend the queue line
and advise guests of delay as per 3.8.5
NOTE: Operators are not permitted to restart the conveyor. This
must be done by Engineering and/or Supervisors
3.4.9 Conveyor chain break
NOTE: Conveyor will automatically stop in the event of a chain
break. An audible alarm will be heard from the panel and
conveyor reseat button will illuminate
(i) Press Emergency Gate Button
(ii) Press Conveyor stop
(iii) Press Emergency Stop
(iv) Remove dispatch isolator key
(v) Contact Control on 325 stating ‘Rapid Ride – Code 6’
(vi) Direct Load Operator to attend the bottom of the conveyor
(vii) If a Deckhand is present direct them to attend the queue line
and advise guests of delay as per 3.8.5
NOTE: Operators are not permitted to restart the conveyor. This
must be done by Engineering and/or Supervisor
191. In relation to the Periodic checks, which are set out at 3.7 of the No. 1 Operator
Procedure Manual, the requirements mirror those of the No. 2 Operator. The only
addition is section 3.5.13, which requires the No. 1 Operator to ‘monitor all
operator movements, ensure staff rotate operating positions throughout the day
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 54 of 274

(where possible).’
281
192. In relation to the required response to Emergencies, which is set out in section
3.6 of the Manual, the same process as that of the No. 2 Operator is followed,
however, the No. 1 Operator is also required to count how many rafts are
retrieved and record the down-time for the ride.
282
193. Each of the Ride Operators, who had been trained on the ride, noted that a
requirement of each of the roles was to watch the water level.
283
This was done
by looking at an informal ‘scum’ mark around the trough of the ride, as well as
the buoyancy of the rafts at the load and unload station, and whether they were
sitting on the rails.
194. It seems to be the consensus amongst Ride Operators, that the TRRR was one
of the most stressful rides to operate because of the difficulty and demands on
the Operators, which included monitoring of the pumps, CCTV, air pressure of
the gates and queue lines.
284
Generally, it appears that more experienced Ride
Operators would be rostered to run the ride.
285
Memorandums for the TRRR
195. In addition to the Operator Procedure Manual for each position of the TRRR,
memorandums were issued by the Supervisory Team to inform Ride Operators
of changes to procedure, draw attention to an issue that had arisen on the ride,
or to clarify roles and responsibilities. It became apparent during the inquest
hearing that there were no records maintained, and therefore no way to ascertain
with any certainty, who had authored a particular memorandum and what the
reason or purpose was for such a document to be created. According to Mr. Fyfe,
who was responsible for the Supervisory Team that authored the document,
each memorandum was supposed to be provided to him for final approval.
286
Unfortunately, in practice, it appears that he had no direct knowledge of who
wrote each memorandum, the specific reason it was created, and whether a
process of consultation between the Supervisors had been undertaken prior to a
memorandum being published.
287
He would occasionally author some
memorandums himself.
288
196. According to Mr. Fyfe, memorandums were generally issued if there had been a
change of ride operation, which could follow from advice provided by the E&T
Department as there were equipment or mechanical changes to a ride, or from
the Operations Department.
289
197. A copy of an issued memorandum was kept with the Operating Procedure at the
ride, and also where staff first attended in the morning on the memo board.
290
If
it was deemed a significant memorandum (although there was no clear guideline
on how this was determined) staff were required to sign off that they had read it
281
Ex D4(103), pg. 14
282
Ex D4(103), pg. 16
283
Ex B3F(3), [10]
284
T2-93, lines 7-27; T4-90, lines 6-35
285
T4-90, lines 23-35
286
Ex C8(6), pg. 11
287
Ex C8(6), pg. 8
288
Ex C8(6), pg. 8
289
Ex C8(6), pg. 9
290
Ex B3A(14), pg. 48; Ex C8(3), pg. 17
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 55 of 274

before they are able to operate a ride.
291
198. The relevant memorandums that had been issued and were in effect for the
TRRR at the time of the tragic incident, are detailed below.
12 February 2016
199. A ‘priority urgent’ memorandum was issued by the Supervisory team to all
Operators and Load Operators for the TRR, titled ‘TRR New buttons’.
292
The
memorandum stated that:
When doing your morning checks, the conveyor control
panel has changed. We must now check the e-stop is out
and the three switches below the e-stop are in Auto,
Forward and Run.
The Rapid Ride panel has been now fitted with a new Blue
Button (conveyor reset) this is for engineering only.
Two new sensors have been fitted at the bottom and half
way up the conveyor. In the event of a raft slipping or
becoming stuck at the bottom of the conveyor for more than
10 seconds, the conveyor will automatically stop and the
blue ‘conveyor reset’ button will flash. In the event of this
happening normal shut down procedure must be followed.
Also we have a new e-stop on the unload platform, this
will stop the conveyor. Operators and load operators
CAN press this ONLY in the event of an emergency, as
the emergency shut down procedure must follow.
Any further questions please see the supervisory team.
200. In relation to the memorandum dated 12 February 2016, this was issued by the
Attractions Supervisory Team as a collective document, which was primarily
prepared by Ms. Crisp and Ms. Tracey McGraw.
293
This memorandum was said
to have been issued following modifications made to the ride, including the
installation of sensors on the conveyor and a new E-Stop at the unload area,
however, the Operating Procedures were yet to be updated.
294
201. The term ‘emergency’ was not defined in the document. Each of the Supervisors
who provided evidence during the inquest gave somewhat different definitions of
what an ‘emergency’ may have meant.
295
There was clearly no universally
understood meaning of “emergency” that would have been easily understood by
Ride Operators stationed at the TRRR.
202. The wording of this memorandum is confusing, poorly defined, unclear and at its
highest, ambiguous and couched generally in negative terms. It is a significant
oversight that the term ‘emergency’, which is highlighted in the document in
connection with the use of the E-Stop, is not defined with examples provided. It
291
Ex B3A(14), pg. 48
292
Ex B15(18)
293
Ex C6(46), [168] & [169]
294
Ex C6(46), [169]; Ex C8(3), pg. 15
295
Ex C8(3), pg. 18 & 19
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 56 of 274
is entirely reasonable and foreseeable that Ride Operators and Supervisors
would have differing views as to what circumstances this direction may apply in,
which became evident during the evidence provided at the inquest. This is so
especially for newly trained or inexperienced Operators
29 May 2016
203. A further ‘priority urgent’ memorandum was issued to all Rapid Ride Operators
and Load Operators by the Supervisory Team, which was titled, Monitoring
conveyor movements’.
296
This memorandum provides that:
To All Thunder River Rapids Operator and Load
Operators. Please ensure you are remaining vigilant
when monitoring conveyor movements. This includes
any obstructions that may interfere with rafts such as
bent or broken brackets.
If you identify an issue of this nature, Operators are to
bring all rafts home and call for an ‘Operational ASAP’
via control on 325 and wait further instructions from a
supervisor.
204. According to Supervisor, Ms. Jennie Knight this memorandum was issued
following a clip coming off the conveyor, which was subsequently replaced.
297
Ride Operators were requested to be mindful in case another incident occurred.
18
October 2016
205. A further ‘priority urgent’ memorandum, also couched in negative terms, was
issued to Rapid Ride Operators and Load Operators by the Supervisory Team,
which was titled, ‘Unload E-Stop’.
298
This memorandum stated:
All Thunder River Rapids operators and Load operators,
The E-Stop situated at unload platform must only be
pressed in the event the main control panel cannot be
reached when there is potential or immediate risk either:
(emphasis added)
(i) Guest/Staff safety or well being
(ii) Ride operating conditions
(iii) Damage to ride equipment
Activating this will cause the rides conveyor to stop.
206. According to Ms. Knight, whilst she did not specifically draft this memorandum,
she is aware through consultation that it was created as there was a
misunderstanding amongst Ride Operators as to whether the E-Stop at the
unload area stopped the conveyor and one pump or just the conveyor.
299
296
Ex B12(20); Ex B12(7)
297
Ex C8(3), pg. 21
298
Ex B12(19)
299
Ex C8(3), pg. 22
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 57 of 274

207. It is significant that, despite being the Attractions and Entertainment Manager,
whom the Supervisors answered to, Mr. Fyfe had no knowledge of the
memorandums issued in relation to the TRRR, and was unable to advise who
had authored the documents or the reasons each of them were issued.
300
He
acknowledged during the inquest that the wording of this memorandum was
ambiguous, especially for a first day Operator.
301
208. When this memorandum is read in conjunction with sections 3.1.7 and 3.6.3 of
the Operating Procedure Manual, it is clear that the direction to the No. 2
Operator is that the E-Stop is only to be pressed in the event that the No. 1
Operator is incapacitated, and under no other circumstances. Mr. Fyfe agreed
with this interpretation during the inquest.
302
It is very clear from the Operating
Procedure Manual that the No. 1 Operator is responsible for the operation of the
ride, which includes the command of Code 6 situations, where they are not
incapacitated.
Pre-ride Checks on the TRRR
209. Under usual conditions, when the No. 1 Operator arrived at the TRRR to open
for the day, they attended the Main Control Panel to carry out the pre-start
checklist.
303
This checklist required that the Operator check the following:
304
a. Engineering have signed the checklist signaling that they had completed
the necessary checks of the ride;
b. That ‘Area Open’ has signed;
c. Check that the Rapids Alarm has been tested;
d. That the access area is clear;
e. Fire-Extinguisher is charged and tamper seal is in place;
f. The First Aid kit is stocked; and
g. That Ride Express equipment is present.
210. The Pre-Operational service sheets, which are to be completed daily by staff
from the E&T Department, reflect the service checks conducted on rides.
305
Each
item listed on the sheet needs to be considered and inspected by the allocated
staff, and is specific to each ride. Each component of the ride to be inspected is
initialed by the staff members responsible.
306
If an issue is identified with a ride
during these checks, depending on the complexity, it will often be escalated to
an E&T Supervisor to determine whether it needs to be fixed immediately or at a
later time.
307
To ensure the service sheets are being completed, an audit is
conducted by supervisors every Tuesday.
308
The TRRR requires the check of
300
Ex C8(6), pg. 9 – 13
301
T19-47, lines 10-20
302
T19-48, lines 1-25
303
Ex B3A(11), [16]
304
Ex B3A(11), [16]
305
Ex B3A(15), [24]
306
Ex B3A(15), [24] & [25]
307
Ex B3A(15), [26]
308
Ex B3A(15), [29]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 58 of 274

around 40-50 items each day.
309
In addition, since early 2016, there are weekly
checks conducted of the sensors installed at the bottom of the conveyor.
310
211. The Ride Operator is then required to sign the checklist to signify that the above
had been completed. If there is an issue with any of these actions, an Operator
is required to call a Supervisor for them to rectify the issue.
311
If the checklist is
missing a signature from the E&T Department, the ride will not be opened to the
public.
312
212. As part of the start-up, the Ride Operator is also required to do the following:
313
• Check that three switches are in the correct position, and that the
Emergency Stop on the control panel is not activated.
314
• Turn the control panel on with a key;
• Place the isolator key in the control panel;
• Press the jack reset button to activate the jacks;
• Commence the automatic-sequence start-up for the water pumps, which
takes approximately 7 minutes for the South Pump to automatically start;
and
• Dispatch an empty raft as a test-run before guests are allowed to board the
ride.
213. At the TRRR, a folder with various documentation was maintained. From an E&T
perspective, this folder contained two weeks’ worth of daily checklists.
315
Down-
time sheets recording when a ride has been out of operation (e.g. shutdown
following a breakdown) are stapled to the back of the sheet. The down-times for
each ride are subsequently entered into a computer spreadsheet by a
Supervisor, with older sheets being removed each Sunday and replaced with a
new sheet.
316
214. Decisions as to when rides are closed due to operational issues or following a
breakdown was a matter for E&T Department Supervisors.
317
E&T staff are the
only ones permitted to restart a ride. Once they restart the ride, the Operator
does not go through the start-up checklist again.
318
Emergency Scenario Training
215. Whilst emergency response drills have previously been carried out at
Dreamworld for the Buzzsaw ride and a Tiger escape,
319
no practical scenario
training for emergency situations were ever implemented for the TRRR. This is
309
Ex B3A(15), [30]
310
Ex B3A(15), [31]
311
Ex B3A(11), [18]
312
Ex B3A(11), [20]
313
Ex B3A(11), [27]
314
Ex B3A(11), [24]
315
Ex B3A(11), [70]
316
Ex B3A(11), [70]
317
Ex B3A(11), [58]
318
Ex B3A(11), [67]
319
Ex B3C(12), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 59 of 274
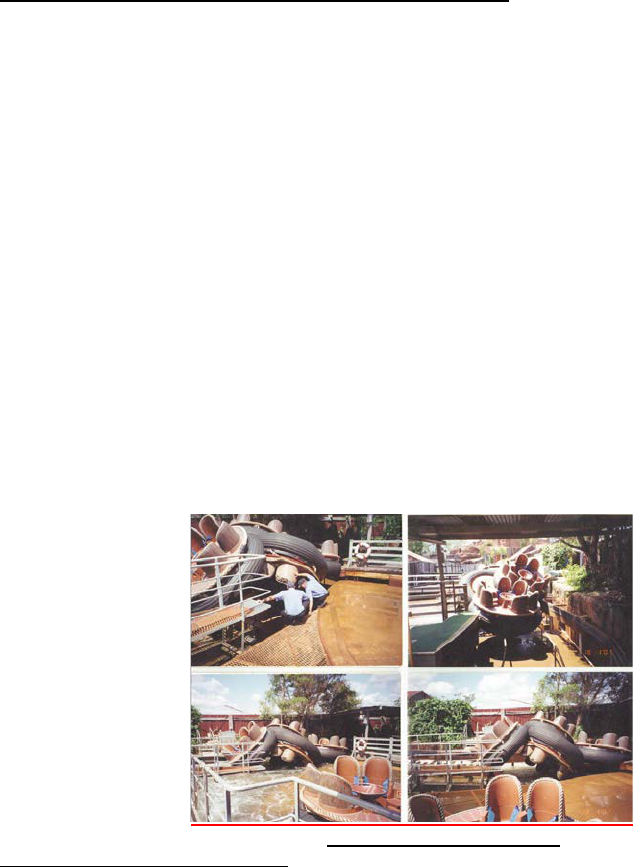
despite recommendations made following previous incidents that this should
take place.
320
216. It was noted by Ride Operators of the TRRR that whilst responses to emergency
situations, which may arise on the ride, were outlined in the Operator Procedure
Manuals, no practical scenario training was provided to equip Operators with the
means to respond to various operating problems.
321
PAST INCIDENTS ON THE TRRR
217. Documentation provided by Ardent Leisure over the course of the coronial
investigation, and also produced during the inquest hearing, confirmed that there
had been a number of previous incidents on the TRRR over the course of its 30
year commission. A summary of the most relevant incidents is detailed below.
18 January 2001 – H101/0019 – Property Damage
322
218. On 18
th
January 2001, Ms. Melinda Lynd was rostered to perform the role of No.
1 Ride Operator on the TRRR. She commenced the start-up procedure at
approximately 9:17 am, releasing all of the rafts to run a full cycle, prior to
opening the ride to guests.
323
She was the only Operator present at the time. At
around 9:30 am, Mr. Joe Stenning, who was rostered on as the No. 2 Operator
for the TRRR that day, arrived and opened the queue line for guests. Whilst the
empty rafts were travelling the water course, guests had commenced lining up.
As Ms. Lynd began speaking to guests in line, two rafts became stationary at the
unload area, with a further three traveling down the conveyor, having completed
a full cycle of the ride.
324
This was noticed by both Ms. Lynd and Mr. Stenning,
however, no attempt was made by Ms. Lynd to release the stranded rafts. As the
three additional rafts came off the conveyor, they collided with the stationary
rafts, causing one to flip. Having seen the rafts flip, an operational Code 6 was
called, at which time Ms. Lynd called 222 and tried to describe the incident, which
was not clear. She then hit the emergency jack button and stopped the
conveyor.
325
The rafts were unable to be freed. Senior Attractions staff arrived at
the TRRR shortly thereafter, and guests were cleared from the area. The
following photographs of the aftermath of the incident depict the scene.
2001 INCIDENT - Ex. B10(1)
320
Ex B3A(3), pg. 13; Ex B3A(12), pg. 30
321
T4-56, lines 15-30
322
Ex B10(2)
323
Ex B10(2), pg. 1
324
Ex B10(2), pg. 1
325
Ex B10(2), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 60 of 274

219. Ms. Lynd commenced employment with Dreamworld in the late 1990s, and had
been a Ride Operator for around five years prior to the incident.
326
She recalls
being trained as an Assistant Operator on the TRRR on her first day working at
Dreamworld. It was a few years before she was trained as the No. 1 Operator.
327
220. In relation to the incident, Ms. Lynd recalls in her statement that she was very
upset by what had happened, and did not believe there was anything that she
could have done to prevent it from occurring.
328
221. Mr. Stenning had been working at Dreamworld since 1999 as an Attractions staff
member, which included the operation of some of the simpler rides.
329
He recalls
being trained as a Deckhand and at the unload station of the TRRR, however,
never manned the control panel or was taught to shut down the ride.
330
222. Mr. Stenning recalls that following the incident, he was taken away from the area
separately to Ms. Lynd, and was not able to speak about the incident whilst the
investigation was pending.
331
He believes that he may have participated in a
debrief discussion following the event.
332
Incident Report
223. An investigation into the cause of the incident was conducted and a report
compiled (‘the Report’). It was found that, ‘the push of the conveyor caused a
compaction effect, resulting in the rafts being caught at the unload area and one
raft flipping. It is then believed that the unload button may have been depressed
releasing a raft, but the second raft with the push of the additional rafts behind
had got caught on the edge of the platform’.
333
224. The incident was identified as a ‘dangerous event’, following which OIR were
called. Having explained the sequence of events verbally, it was determined that
no formal notification was required. The Report notes that ‘the response team
including TBS, RB, BT, SH & AN identified the incident as a dangerous event
and at 10:08 am AN contacted the Workplace Health & Safety – South Coast
Division and was put through the Dave Mazzer, District Manager Workplace
Health & Safety (Southport). The sequence of events was explained by mobile
phone. Dave responded that he was confident with DW’s own internal
investigation process and requested that a file be kept that a courtesy call was
made to the Division. No formal notification was required.’
334
225. The contributing factors with respect to the actions of the Operator, were found
to be as follows:
335
• Distraction from guests – attention was diverted from operating ride.
• Second employee stuck – there should have been two Operators start
the ride at 9:15 am.
326
Ex B3F(1), [2]
327
Ex B3F(1), [6] & [7]
328
Ex B3F(1), [11]
329
Ex B3F(3), [2]
330
T9-6, lines 15-47
331
Ex B3F(3), [18] & [19]
332
T9-13, lines 38-40
333
Ex B10(2), pg. 1
334
Ex B10(2), pg. 2
335
Ex B(10)(2), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 61 of 274

• Employee panicking – Operator responded inappropriately. Lack of
confidence to make own decision in an emergency situation (when it
was noted that she is the more Senior Operator).
• Communication – employee did not relay details of events satisfactorily
to Control or Supervisors.
226. The final outcome of the incident was determined to be that there had had been
a failure to adhere to the start-up procedure, and the Operator had not followed
the correct emergency response procedure.
336
As part of the investigation into
the incident, the Report notes that a review of the operational procedures of the
TRRR was conducted, and that the possibility of the same event occurring whilst
guests were on the rafts was held to be ‘nil’.
337
This conclusion was based on
the following reasoning (assuming the correct operating procedures were being
followed):
338
o There would have been two people operating the ride;
o No loaded rafts are to be dispatched without the second Operator being
present, which would eliminate the rafts banking up at the unload area.
The Deckhand has control of the unload of guests and the flow of rafts
through to the unload area;
o The dispatch time between the rafts would have been greater, giving the
Deckhand and No. 1 Operator more time to react to the situation; and
o The Deckhand would have seen the situation as it was evolving and
been able to react in a more timely fashion and/or followed correct
emergency procedures.
227. A review of the training procedures for the TRRR and Ms. Lynd’s records were
also undertaken as part of the investigation. It was noted in the Report that she
had been trained by Mr. David Wilkinson, a Relief Supervisor (who was an
accredited trainer, and staff member for 12 years), and subsequently audited by
Mr. Garren Cox, who was an Attractions Supervisor and Training Coordinator.
339
228. It was further acknowledged that there had been a breakdown in the
communication process and notification by way of the two-way broadcast. That
was because the incident was not called in as a ‘Code 222-Grey’ but rather
dubbed ‘operational’.
229. During the inquest, Mr. Stenning stated that he was not made aware of the
findings of the investigation report following the incident.
340
336
Ex B10(2), pg.2
337
Ex B10(2), pg.2
338
Ex B10(2), pg.2
339
Ex B10(2), pg.2
340
T9-16, lines 10-15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 62 of 274
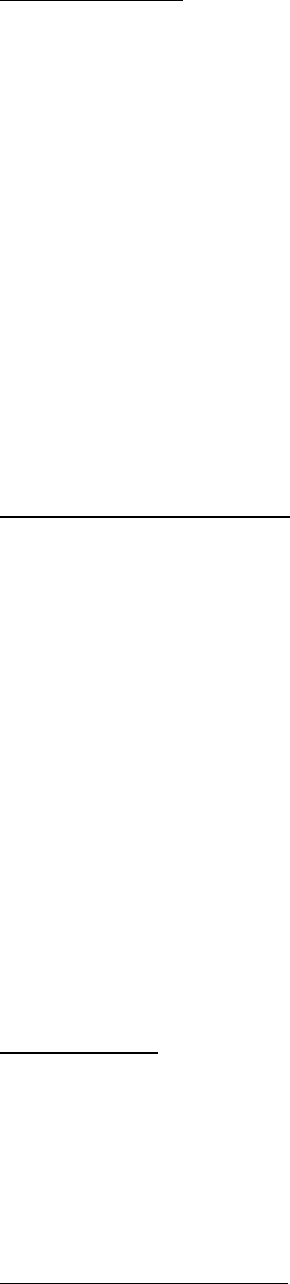
Recommendations
230. The following recommendations were made following this incident:
341
• Emergency Response Scenario Training for all Ride Operators in the
various Code 222’s in order to improve confidence when involved in an
emergency situation.
• Communication – a review of determining notification of broadcast from
Code 222 phone calls.
• Human Resources to be involved in disciplinary action in regard to incorrect
operation of ride.
• Amend procedure so that both Operator and the deckhand should be
present to start ride (opening and operating procedures) on all occasions.
231. Following the incident, Ms. Lynd was moved into a position working in the Food
and Beverage division of Dreamworld, however, resigned shortly thereafter.
342
Comments About the Incident
232. From the extensive documentary exhibits provided by Ardent Leisure, and the
evidence given during the course of the inquest, it does not appear that the
investigation into this particular incident extended to consider the design of the
ride, although subsequent modifications were made to the unload platform.
233. I am satisfied that a thorough engineering hazard or risk assessment of the ride
was not conducted as a result of this incident. Engineering staff, who were
employed at the time, were not consulted as to whether any modifications
needed to be made to the ride to ensure a similar incident did not reoccur.
234. Despite the recommendations of this incident, no practice scenario-based
training for emergency situations was ever provided for the TRRR, or any other
ride at Dreamworld prior to the subject tragedy. It is unknown why this
recommendation was never implemented. A thorough review of this incident
would have presented a timely and graphic reminder to all safety staff as to what,
potentially, could have occurred once a raft blocked the passage of following
rafts coming down the conveyor. It is fortunate there were no passengers in the
rafts at the time.
7 October 2004
343
235. At around 3:05 pm on 7 October 2004, a raft on the TRRR entered the unload
station and patrons started to disembark. As the final passenger was leaving the
raft with the assistance of an Operator, another raft entered the unloading dock
and made contact with the stationary raft. The passenger lost her balance and
fell into the water, passing under the raft. A fellow passenger and the Ride
Operator entered the water to provide assistance and retrieve the guest. No
injuries aside from subsequent neck pain were sustained by the passenger.
344
341
Ex B(10)(2), pg. 3
342
Ex B3F (1), [12]
343
Ex B10(3)
344
Ex B10(3), pg. 2 & 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 63 of 274
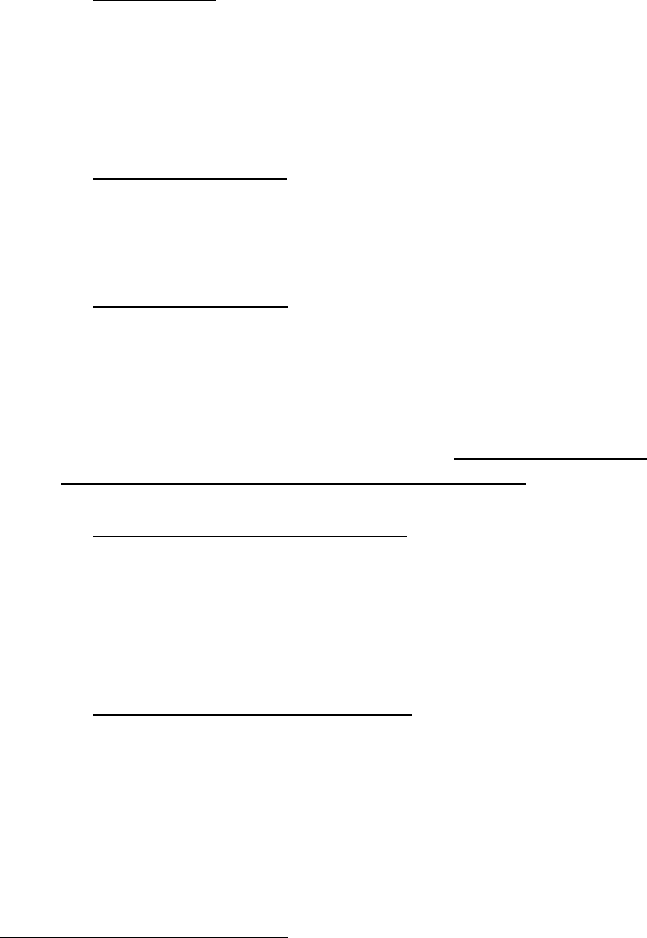
236. OIR were notified of the incident via telephone on 7 October 2004.
345
No statutory
notices were issued under the condition that the incident was internally
investigated by Dreamworld, and engineering controls to prevent the incident
from re-occurring were considered.
346
237. It appears that the incident was investigated by Dreamworld, with a report
subsequently prepared.
347
The contributing factors to the incident were identified
as follows:
• Raft spacing – during normal ride operation, the rafts are released from the
loading dock at uniform intervals, which is designed to prevent contact
between the rafts allowing patrons sufficient time to disembark. However,
extra time taken for passengers to disembark from a raft or a difference in
the speed at which the rafts travel, can cause the rafts to ‘queue up’ and
make contact at the unloading area.
348
• Engineering control – the Report noted that ‘at the time of the incident,
administrative procedures and engineering controls were employed to
prevent rafts contacting. However, the ride could be improved by
implementing further engineering controls…’
349
• Operational factors – the efficiency and time required to disembark
passengers from the raft at the end of the ride is related to the experience of
the Operator. Video footage of the incident suggests that the Ride Operator
assisting guests to disembark, who was relatively new, may have ‘struggled’
to be meeting the unloading demands.
350
238. A number of short-term and long-term corrective actions were identified to
‘more adequately control the risk of raft collision’.
351
These actions included:
• Installation of emergency stops: It was noted that an additional emergency
stop button had been installed in the un-loading dock, which shuts down one
of the two main pumps circulating water through the ride. Further
investigation was to be ‘directed towards ‘double pump’ E stopping’, which
was intended to immediately shut down both pumps to ‘rapidly dissipate the
water’.
352
• Fewer rafts circulating the ride: It was noted in the Report that a ‘timer
permitted dispatch is scheduled for installation by late 2004’, which would
release rafts at the loading dock at predetermined intervals.
353
Following the
incident, the rafts used in circulation for the ride was decreased from 12 to
eight. A standing order was then put in place, which limited the maximum
number of rafts in circulation to eight. It was noted that ‘This will remain
current until the completion of improvements to the ride and further
assessments indicate a higher number can be safely operated’.
354
345
Ex B10(3), pg. 3
346
Ex B10(3), pg. 3
347
Ex B10(3)
348
Ex B10(3), pg. 3
349
Ex B10(3), pg. 3
350
Ex B10(3), pg. 3
351
Ex B10(3), pg. 4
352
Ex B10(3), pg. 4
353
Ex B10(3), pg. 4
354
Ex B10(3), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 64 of 274
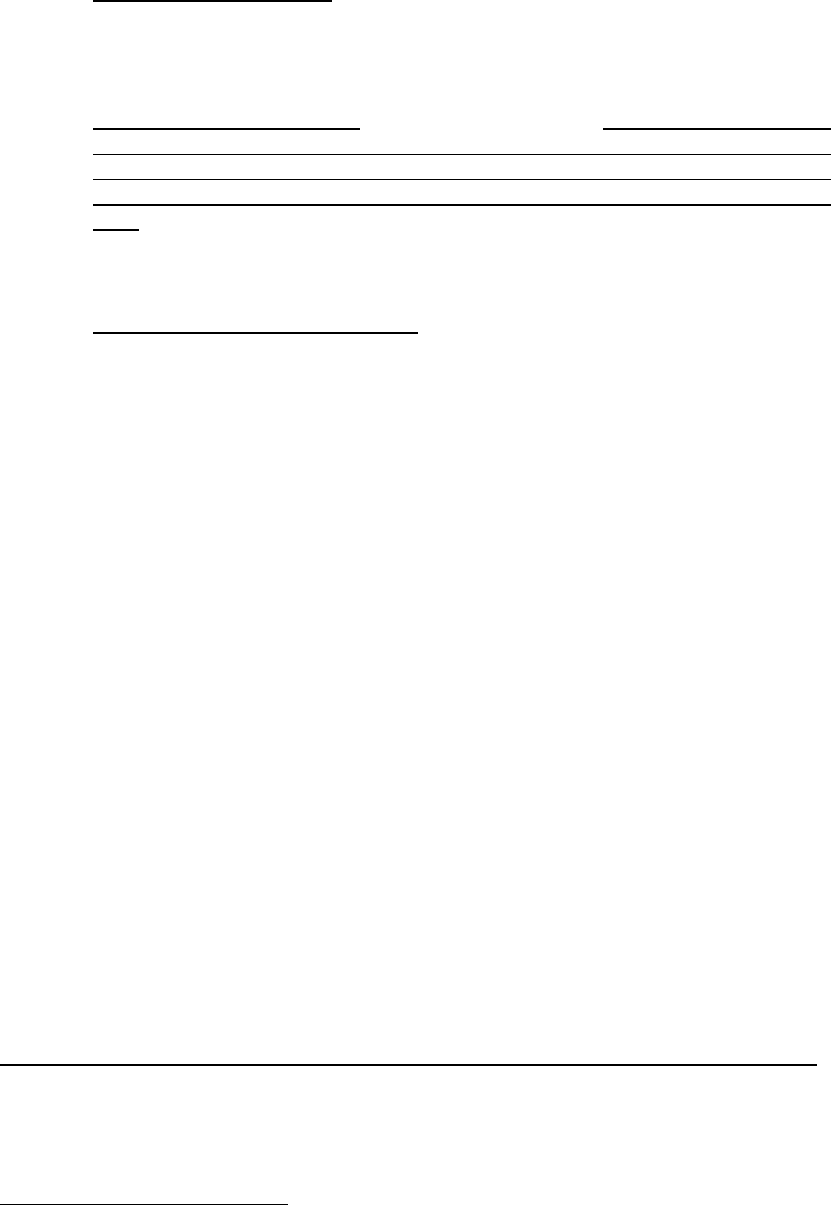
• Additional raft hold gate: A further holding gate was to be positioned before
the unloading dock, to ensure that a raft approaching the unload area would
not make contact with another raft. This gate was subsequently installed at
some time before 21 October 2004.
355
• Conveyor speed controller: The Report noted that ‘some investigation has
already been undertaken into the possible installation of a conveyor belt
speed controller. This controller (operated by the unload attendant) would
lower the speed of the conveyor belt should rafts begin to queue in the unload
dock. At this time, the speed controller is not considered necessary. However
if collision potential is still unsatisfactory following installation of the timer and
holding gate, further investigation into the speed controller will take place.’
356
• Power assisted raft positioners: the Report stated that ‘the process of
correctly positioning the raft in the unloading dock is planned to be automated
via the use of a mechanical raft positioner. The positioner will no longer
require the operator to manually manoevre the raft with their arms and
legs.’
357
The intention of this corrective action was to reduce the Operator’s
‘manual task exposure’. According to the Report, this system was in the
‘design stage’ and intended to be installed during major refurbishments of the
ride in 2005.
239. In addition, operational issues were identified following the incident. Whilst the
Report noted that ‘all staff required to operate the Rapids Ride undertake
comprehensive training in all facets of the ride’s operation and emergency
procedures’, a number of changes were subsequently made to the training
regime.
358
These changes included, refresher training to be provided to
Operators, an update of the procedures manual, as well as the expansion of the
auditing checklists to include an assessment of the rafts queuing in the unload
dock.
359
It was intended, according to the Report, for the operating procedures
manual to be updated to include the engineering controls once installed.
240. It was also recommended, following the investigation into this incident, that
Senior Ride Operators may be required to monitor the ability of the unload
attendant to ‘cope’ with the unloading demands, so that those who were thought
to be struggling could be provided with additional training and mentoring.
360
241. The Report acknowledged that at the time of the incident, administrative controls
were the primary means of avoiding raft collision at the unload area. The
corrective actions suggested were intended to more adequately control the risk
of future raft collisions.
361
Further Consideration and Implementation of the Recommendations by Dreamworld
242. Following the incident, consideration was given to increasing the number of rafts
in circulation at the TRRR from 10 to 11 with a three person operation.
362
The
purpose and findings of the investigation were detailed in a Report (‘the Report’).
355
Ex B10(3), pg. 6, See Appendix 2
356
Ex B10(3), pg. 4
357
Ex B10(3), pg. 5
358
Ex B10(3), pg. 5
359
Ex B10(3), pg. 5
360
Ex B10(3), pg. 5
361
Ex B10(3), pg. 5
362
Ex C4(5), pg. 541
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 65 of 274

The Report was intended to exclude the model where only two Operators were
present, as a maximum of nine rafts would continue to be used.
243. Since the incident in October, an additional holding gate had been installed at
the unload area, as well as an automated timer for the dispatch of rafts to ensure
they were dispatched with a minimum time lag of 30 seconds.
363
The Report
noted that ‘the combination of these controls ensures that the rafts are sufficiently
separated and at no time can a raft being unloaded ever be contacted by a
following raft.’
364
Following the implementation of these engineering controls, the
number of rafts in operation was increased to nine for two Operators and 10 for
three.
244. The intention of having an extra raft in use was to ensure there was an additional
raft available at the load area to minimise the time guests have to wait to load a
raft, which was thought to positively increase capacity.
365
245. An assessment was conducted of the further increase in the number of rafts. As
detailed in the Report, it was found that:
366
• A complete circuit of the TRRR from the timed release gate to the holding
gate was around 245 seconds. Therefore, if a raft is released by the timed
gate every 30 seconds, the maximum number of rafts that can be in circuit
between the timed gate and the first unload gate is nine.
• Due to the number of rafts that would be operational, it would require
efficient running of the ride, in order to prevent an accumulation of rafts at
the load area.
• If an accumulation of rafts was to occur, four could be in place between the
load and unload dock before any issue arose.
246. The limitations of the assessment as to the increase in the number of rafts was
stated in the Report to be that it was based on sighting eight rafts in operation
with both two and three Operators. It was recommended that a trial of 11 rafts
should be undertaken before final approval was made.
367
247. Ultimately, the final recommendations made were:
368
• To mitigate risk, only experienced staff should operate the TRRR when 11
rafts are in operation.
• Trials should be undertaken outside of standard operating hours to ensure
no other risks are identified and to ensure timings are accurate.
• Implementation should be monitored and reviewed to ensure the operation
of 11 rafts is sustainable.
• Two rafts must be taken out of circuit and stored appropriately in the holding
area if the operation of the attraction is reduced to two Operators.
363
Ex C4(5), pg. 541
364
Ex C4(5), pg. 541
365
Ex C4(5), pg. 541
366
Ex C4(5), pg. 541
367
Ex C4(5), pg. 541
368
Ex C4(5), pg. 541 & 542
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 66 of 274

Comments about the Incident
248. It is unclear from the Report, further documentary material and the evidence
provided during the inquest, as to whether any Engineering input was sought for
the purpose of the investigation and/or Report. On balance, it appears that those
in the E&T Department did not consider the risks associated with the ride
following this incident.
249. It is clear given the configuration of the TRRR at the time of the tragic incident in
2016, not all of the recommendations, particularly the further engineering
controls, had been implemented. It is unclear based on the records available as
to why this course was taken.
28 August 2005
250. On 28 August 2005, the Unload Ride Operator observed an extended gap
between the rafts arriving at the unload dock. He observed on the conveyor that
three rafts were traveling on the belt together. The Ride Load Operator
immediately closed the emergency jack to prevent further rafts from being
dispatched, and all guests were returned and able to disembark safely.
369
251. Supervisors from the Engineering and Operations Departments were called to
attend the incident. It was found that the first raft had taken on water, and was
removed from circulation. This may have contributed to the incident by making it
more difficult for the raft to transition onto the conveyor belt and a lower stance
when on the water.
370
252. The investigation Report (‘the Report’) prepared following the incident noted that
there were limitations to the coverage provided by the current CCTV monitoring
system at the TRRR, which was only a single camera located beneath the Mine
Ride. The Report noted that, ‘this location may be inappropriate and thus
compromise the ability of the load operator monitor the belt effectively’.
371
253. The following recommendations and corrective actions were undertaken as a
result of the incident:
(iv) Short-term
• Extensive testing was carried out to determine the cause of the water
leak in the initial raft. A more comprehensive system for dewatering the
rafts was subsequently developed, which was to occur four times a
week (rather than three). Records of this dewatering activity were also
introduced.
372
• In order to assist Ride Operators to monitor the conveyor belt,
consideration was to be given to a second CCTV screen positioned at
the unload station. The intention of the screen was to ‘solely display the
conveyor belt and enable the unload operator to monitor raft spacing
more effectively and consistently. Furthermore, this would also be
369
Ex B10(4), pg. 1
370
Ex B10(4), pg. 1
371
Ex B10(4), pg. 1
372
Ex B10(4), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 67 of 274
advantageous to the load operator, who must perform numerous tasks
simultaneously – many of which are cognitively draining.’
373
• A warning was also issued to all Attractions Supervisors and TRRR
Ride Operators, which emphasised the need for Operators to monitor
raft gaps and CCTV coverage of the conveyor belt prior to dispatching
rafts. Operators were also advised that the Load Operator’s screen had
been re-configured to ‘enlarge the view of the conveyor belt camera.
This will enable more effective monitoring of raft transition onto the
conveyor belt’.
374
(v) Long-term
• It was noted that the TRRR’s safety would also benefit from Attractions
Supervisors continuing to carry out visual assessments of the Ride
Operators, in particular, focusing on the required periodic checks.
375
• Raft floatation indicators were also being investigated by the
Engineering Department in order to ‘assist operators in identifying
possible water infiltration during operation’.
376
26 February 2008
254. On 26 February 2008 at around 11:10 am, Ride Operators experienced issues
with the raft dispatch sensor, which prevented rafts from being dispatched
consistently.
377
A Supervisor was contacted and advised of the problem. An E&T
employee attended the TRRR and repaired the sensor. By this time, three rafts
had banked up at the dispatch area and were resting on the emergency jack.
Whilst three empty rafts were cleared by being released, there was concern that
there may have been inadequate spacing. A further four rafts were released, one
with patrons on board. Two of the rafts initially dispatched became jammed at
the jungle section of the TRRR, which caused the other four rafts to stop,
including the one containing guests. The emergency procedure was activated
and the guests were evacuated without incident.
255. Following an investigation of the incident, the factors found to have contributed
were:
• Breach of operational procedure: the Investigation Report (‘the Report’)
noted that whilst the operating procedures for the TRRR are ‘clear and un-
ambiguous’, there was a clear breach of the requirement to monitor rafts
via the CCTV and to heed the spacing stipulations.
378
The breach of the
procedure was considered to be the major contributing factor towards the
incident. The Operator admitted to being aware of the procedure and the
safety implications of having rafts dispatched at incorrect intervals, saying
that ‘rafts could jam or flip under these circumstances’.
379
373
Ex B10(4), pg. 1
374
Ex B10(4), pg. 2
375
Ex B10(4), pg. 2
376
Ex B10(4), pg. 2
377
Ex B15(17), pg. 2
378
Ex B15(17), pg. 2
379
Ex B15(17), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 68 of 274
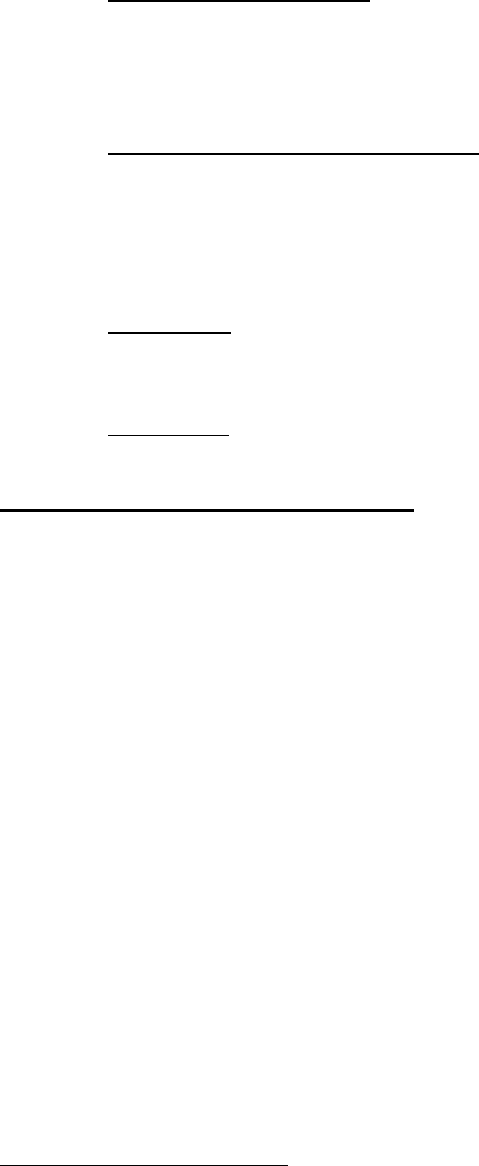
• Release of rafts procedure: Whilst not considered to be a major contributing
factor towards the incident, the release by the engineer of the rafts banked
up at the emergency jack without appropriate spacing intervals due to the
technical nature of the jack, was identified as an issue, which could be
further investigated.
380
• Ride control status during Code 6: Whilst not found to be a major
contributing factor to the incident, the ‘change-over’ of control of the ride
between Engineering and Attractions staff was identified as a potential
issue.
381
256. Ultimately, the following recommendations were made:
• Engineering: Investigate whether the electrical/mechanical systems
controlling the emergency jack can be modified so as to release one raft at
a time.
382
• Procedural: Further definition to be provided as to when Ride Operators
hand over control of the ride to engineering staff, and vice-versa.
383
6 November 2014 – ‘The BUSS Incident’
257. On 6 November 2014 at around 12:30 pm, Mr. Stephen Buss was the No. 1 Ride
Operator at the TRRR. He claims that he heard the backup compressor shut
down, without the sounding of a low air alarm.
384
Around 10 minutes later, he
claims that a low air alarm sounded and he stopped the dispatching of rafts,
before roping and securing the 1
st
raft. The water level was observed to drop
following the sounding of the alarm.
385
Mr. Buss subsequently retrieved six of the
nine rafts in circulation. He admitted that he had mistakenly turned a single pump
off during the incident. Due to the lower water level, a raft had stopped at the
unload area shortly off the end of the conveyor and was stuck on the rails, with
another approaching on the conveyor. Upon noticing this, Mr. Buss claims that
he turned the conveyor off to avoid a collision.
386
Video footage of the incident,
however, shows that the conveyor was only stopped after the rafts came into
contact with one another with the tubes bumping as the conveyor continued to
move.
387
This accords with the No. 2 Operator’s recollection of the incident.
388
Mr. Buss then manually restarted the pump he had turned off, retrieving the 7
th
and 8
th
rafts. He was notified by the gift stop that the 9
th
raft had drifted in to the
reservoir, at which time he commenced a Code 6. Accounts suggest this
occurred at around 12:32 pm.
389
When Mr. Buss observed the 9
th
raft at the
bottom of the conveyor, he decided to restart the ride in an attempt to retrieve
the raft.
380
Ex B15(17), pg. 3
381
Ex B15(17), pg. 3
382
Ex B15(17), pg. 3
383
Ex B15(17), pg. 3
384
Ex C8(21), pg. 67
385
Ex C8(21), pg. 81
386
Ex C8(21), pg. 67
387
Ex C8(15), see RAPIDS06111402, at 03:08:32 onwards
388
Ex C8(21), pg. 81
389
Ex C8(21), pg. 75
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 69 of 274

258. Supervisors and E&T staff arrived at the TRRR shortly after the Code 6 was
called in relation to the incident. Mr. Buss, however, continued to operate the
TRRR for the remaining part of that day.
390
259. An investigation into the incident, which was deemed a ‘serious breach of safety’,
was subsequently commenced.
391
In addition to viewing CCTV footage of the
incident, staff were interviewed and a number of meetings were held with Mr.
Buss.
392
It was alleged that he had failed to follow the correct procedure for a
‘Loss of Air Pressure Alarm (Low Air Alarm)’ at the TRRR, and had subsequently
restarted equipment without authorisation or direction, which had resulted in
creating a significant risk to guest safety.
393
260. Ultimately, Dreamworld found the following in relation to the incident:
394
• Surveillance footage confirmed that Mr. Buss did not follow the correct
procedure for a ‘Low Air Alarm’, and had shut down a pump at the TRRR
without verifying the location of all rafts in operation in the ride circuit. This
led to a situation where a raft containing patrons ‘bottomed out’ at the top
of the conveyor due to a lack of water supply, and an additional raft
containing guests has then collided with it. This raft continued to be
pushed by the conveyor until the conveyor was shut down. In shutting
down the pump, footage confirmed that this resulted in a change of
direction for the water at the bottom of the conveyor, which forced a raft
with guests on board into the reservoir, where they floated unattended for
a period of more than two minutes.
395
• Mr. Buss confirmed that he had manually restarted the pump he had shut
down, which was not in line with the procedure for a ‘Loss of Air Pressure
Alarm’ or the ‘Operator Initiate Shut Down’ procedures. This action was
completed without authorisation or direction, and created a significant risk
to guest safety.
396
• After freeing the two rafts at the top of the conveyor by manually restarting
the shut-down pump, the No. 2 Operator advised Mr. Buss that there
were guests stuck at the entrance of the reservoir. At this time, he
escalated the incident from an ‘Operational’ to a ‘Code 6’, however, did
not follow the procedure to initiate an Operator Shut Down as per the
operating procedure of the TRRR. He also did not raise the ‘Rapid Ride
Alarm’. Instead, Mr. Buss restarted the conveyor to capture another raft
that was visible in his monitor at the bottom of the conveyor. He then
called off the ‘Code 6’ claiming that all the rafts had been homed. It was
noted that, ‘This raft, left sitting at the bottom of the conveyor was at
serious risk of flipping due to the increased pressure from the re-started
pump’.
397
261. Mr. Buss’ conduct was held to constitute a serious breach of safety and the
390
T12-98, lines 1-15
391
Ex C8(21), pg. 53
392
Ex C8(21), pg. 53 onwards
393
Ex C8(21), pg. 53
394
Ex C8(21), pg. 53
395
Ex C8(21), pg. 53
396
Ex C8(21), pg. 53
397
Ex C8(21), pg. 55
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 70 of 274
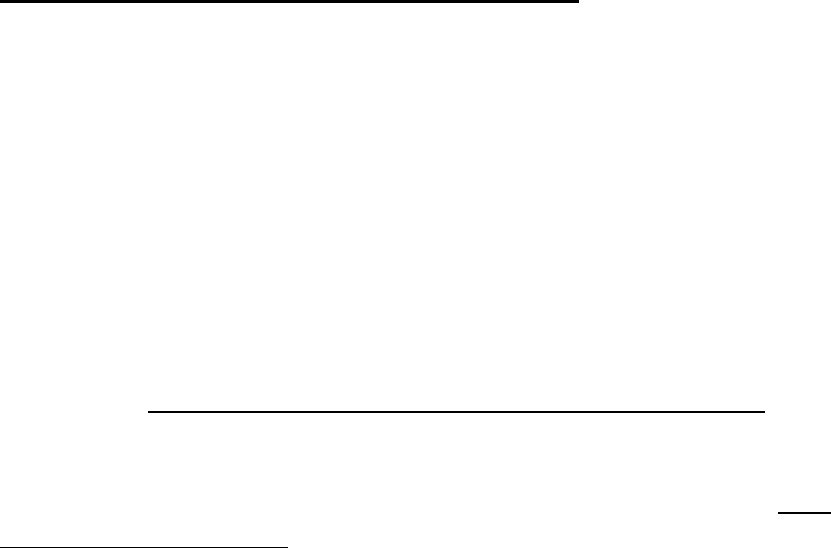
Dreamworld Code of Conduct, ‘Expectations of all Team Members’.
398
He was
asked to show cause as to why his employment should not be ceased due to his
conduct and concerns in relation to his ability to operate rides in a safe manner.
He failed to do so and was terminated.
262. Mr. Buss was first employed with Dreamworld in 2006. At the time of the incident,
he was an experienced Level 3 (No. 1) Operator for all of the rides at the Theme
Park.
399
From the various records provided, it appears that Mr. Buss was first
trained as a Ride Operator on the TRRR in April 2008.
400
During the inquest, he
claimed that he had been rostered on to operate the TRRR around once a week
and was very familiar with the ride.
401
He had also previously been involved in
Code 6s at the TRRR with various causes, including a pump failure and low
pressure alarm.
402
Mr. Buss, despite being one of the most senior Ride Operators
at the park at the time, was not offered any retraining prior to his dismissal.
403
263. Despite his extensive experience, Mr. Buss described the operation of the TRRR
as more difficult than other rides as there were a lot of tasks to undertake
simultaneously.
404
264. It does not appear that following Mr. Buss’ termination, his actions from a safety
perspective were discussed or redressed by way of training with other Ride
Operators.
405
13 November 2014 - Bob Tan Email to Leadership Team
265. On 13 November 2014, following the incident involving Mr. Buss, Mr. Bob Tan,
General Manager of Special Projects, sent an email to the Dreamworld
Leadership Team titled, ‘Re: Ride incidents of relevance’.
406
The email highlights
some ‘peak relevant incidents’ on similar rides, following a discussion at the
meeting that day concerning breaches/deviations in procedures.
266. The first incident occurred in Texas in 2013, when a woman fell from a Giant
roller coaster. It was thought that she may have been of too large a size to be
secured by the restraint bar. Mr. Tan noted that, ‘Actual cause still unconfirmed,
but an innocent guest dies because a safety process was deficient…’
407
267. The second incident highlighted the incident involving Ms. Lynd in 2001, with
pictures of the flipped rafts attached. Mr. Tan noted, ‘This occurred on the rapid
ride several years ago, and fortunately there was no injury except for property
damage. I shudder when I think if there had been guests on the rafts…’
408
268. The Head of the Engineering Department, Mr. Christopher Deaves, responded
to Mr. Tan’s email inquiring as to how the incident on the TRRR had occurred,
as he had never ‘seen or heard’ of the event.
409
Mr. Tan responded stating, ‘scary
398
Ex C8(21), pg. 55
399
Ex F2B(1)(a), pg. 3 & 4
400
Ex C8(21), pg. 589-605
401
T12-81, lines 35-45
402
Ex F2B(1)(a), pg. 25
403
Ex F2B(1)(a), pg. 35; T12-94, lines 10-20
404
T12-84, lines 30-47
405
T5-8, lines 35-45
406
Ex C8(26)(c), pg. 1
407
Ex C8(26)(c), pg. 1
408
Ex C8(26)(c), pg. 1
409
Ex C8(26)(c), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 71 of 274
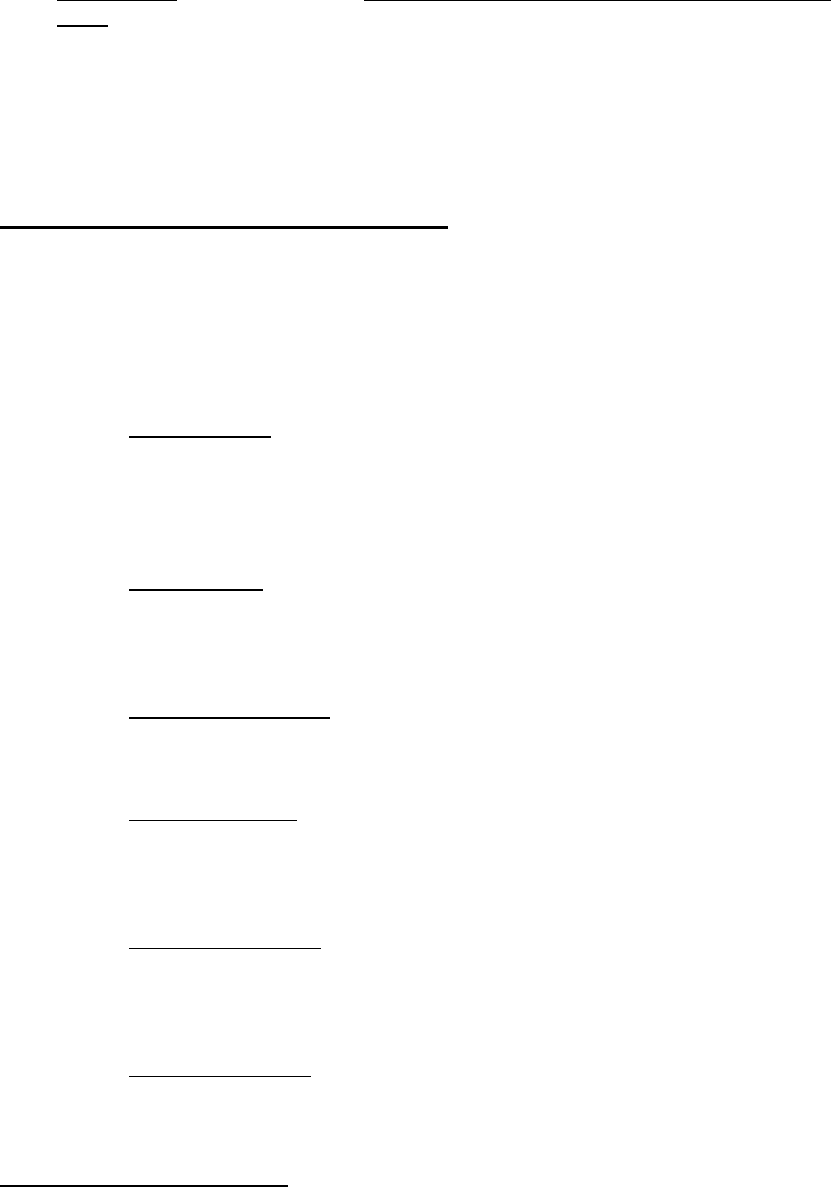
photos huh?’
410
He also noted, ‘Allowing rafts to bank up against a raft at unload
dock’.
411
269. Mr. Deaves subsequently asked whether the risks highlighted (presumably from
the Texas incident) were ongoing from seat belts being undone on rides.
412
In
response, Mr. Tan relevantly stated that, ‘No, 2 senior long service
operators/instructors breeching procedures: Rapid Ride – Shut off a
pump/restarted again. Also stopped conveyor, all against procedure...’
413
Further Incidents Recorded in Log Reports
270. A number of other less significant incidents and issues, which occurred on the
TRRR, were identified in Log Reports provided as part of the documentary
material supplied by Ardent Leisure.
271. A summary of some of the more pertinent incidents and issues are as follows:
• 27 June 2010: A power dip caused the South Pump at the ride to shut
down. The alarm was sounded by the Operators. Two rafts floated into
the reservoir where they were retrieved by engineering staff. A third raft
stalled between the conveyor and the unload station, and guests were
unable to be safely unloaded until both pumps could be restarted.
414
• 30
June 2010: Report that a guest fell into the water whilst helping another
guest out of the raft. Other rafts have pushed through the stopping jack
and contacted stationary raft. Guest landed between the metal guard
rails. Operations and Attractions in attendance.
415
• 16 September 2011: Reported that guest was on the ride when the raft
was climbing the conveyor and has slipped down and contacted another
raft at the bottom of the conveyor.
416
• 13 October 2012: An incident occurred when three rafts jammed together
in the trough next to the sand filter. The trough was inspected and the
water level was checked, and it appeared to be an issue with the dispatch
of the rafts.
417
• 23 December 2013: Staff member was working at the unload dock of the
ride, when they slipped and fell into the water on the up current side of
the raft. Employee had started to be dragged under the raft, and was
grabbed by the guest. Rapids ride alarm was hit and the ride stopped.
418
• 29 February 2016: The alarm was set off when the conveyor ceased to
work. There were approximately five rafts stopped at the bottom of the
conveyor. Engineers, attractions supervisors, first aid and security
attended the incident. There were no reported injuries as a result.
410
Ex C8(26)(c), pg. 12
411
Ex C8(26)(c), pg. 14
412
Ex C8(26)(c), pg. 10
413
Ex C8(26)(c), pg. 10
414
Ex E(369)
415
Ex E(511)
416
Ex E(508); Ex E(514)
417
Ex E(281); E(350)
418
Ex E(550)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 72 of 274

Approximately 28 guests were involved.
419
• 15 June 2016: Under “issues” on the Engineering Supervisors Sheet, it
was noted that the Rapid Ride South Pump had a bearing failure and
there was monitoring of southern pump temperatures.
420
• 22 June 2016: The TRRR was under service from 10 am until 11:30 am
due to issues with the South Pump Flange (Code 237).
421
DREAMWORLD SAFETY DEPARTMENT
272. The purpose of the Dreamworld Safety Department was to assist with safety
compliance and continually improve culture/business practice in conjunction with
other Departments.
422
At the time of the tragic incident, the team consisted of
four Safety Officers, two of whom were experienced paramedics, Mr. John Clark
and Ms. Allyson Sutcliffe, a First Aid Officer, Mr. Benjamin Hicks and Ms.
Rebecca Ramsey, a Registered Nurse.
423
Ms. Ramsey describes her
responsibilities on a daily basis as checking the risk management system,
Figtree to see what incidents had occurred around the park in order to determine
what further investigations needed to be undertaken, which included risk
assessments.
424
273. Mr. Mark Thompson was the Safety Manager (Dreamworld), and Mr. Angus
Hutchings was the Group Safety Manager for Ardent Leisure. Mr. Hutchings and
Mr. Davidson were responsible for ensuring that Senior Committee and Board of
Director members were kept abreast of safety related issues at Dreamworld.
425
274. Mr. Hutchings, as the Group Safety Manager for Ardent Leisure, had a number
of broad responsibilities across various businesses, which included Dreamworld.
He was required to provide support and assistance to Ardent Safety Managers
as to a range of safety and risk issues at strategic and operational levels, as well
as monitor group wide OHS performance and coordinate various audits,
inspections and safety initiatives throughout the group.
426
275. As the Safety Manager, Mr. Thompson describes his role as ‘one of consultancy
and advisory response’ whereby he did not have decision making powers.
427
His
responsibilities included the following:
428
• Deliver training on general safety matters at induction, including basic
hazard identification information;
429
• Deliver training on park-wide matters such as lock-out, tag out
procedures or chemical training;
• Respond to management or employee issues that were raised through
419
Ex E(369)
420
Ex E(57)
421
Ex E(49)
422
Ex C6(51), [40]
423
Ex C5(23)(c), pg. 5
424
Ex C5(23)(c), pg. 5
425
Ex C6(51), [58] & [60]
426
Ex C8(23)(a)
427
Ex C6(51), [28]
428
Ex C6(51), [3]
429
T6-15, lines 40-48
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 73 of 274

the Figtree system and implement control measures for hazards through
the process;
• Attend meetings of Senior Leadership Team, the Safety Executive, Park
Operations Meetings and Engineers Supervisors;
• Investigate workers compensation claims;
• Investigate suspected safety breaches or operating procedures for
Human Resources or the relevant Departments;
• Order PPE;
• Oversee management of the First Aid Clinic; and
• Preparation of various reports.
276. Mr. Thompson did not conduct regular safety audits or inspections at
Dreamworld.
430
He states that he thought these were organised by Mr. Hutchings
with external auditors or carried out by Health and Safety Representatives (also
known as safety ambassadors).
431
Whilst Mr. Thompson did not conduct any
holistic risk assessments of rides having the view that the E&T Department were
responsible for such matters, he did note during the inquest that individual
components of rides were assessed from time to time, such as the cleanliness
of the water in use for the cannons located on the walkway near the TRRR.
432
There were no safety audits conducted, according to Mr. Thompson, as to the
human components of the ride systems at Dreamworld.
433
277. It is significant to note that Mr. Thompson, as the Safety Manager of Dreamworld,
was not aware of the recommendations made by any external auditors
commissioned by Dreamworld to conduct assessments in relation to safety of
the rides and attractions, and did not have a copy of the reports commissioned.
434
Decisions as to the implementation of external auditor recommendations were
made by Mr. Hutchings, Mr. Deaves and Mr. Tan before his departure.
435
278. According to Mr. Thompson, the Safety Team at Dreamworld was not structured
to operate effectively.
436
He describes his role as having a large amount of
responsibility, which made it difficult for him to complete the reactive work
required, let alone any proactive safety management.
437
He notes that on a daily
basis, members of the Safety Team would be ‘pulled away’ to conduct ride
assessments for guests arriving at the Park or other tasks, which left the group
short staffed. This meant Mr. Thompson was personally required to compensate
and carry out the tasks of his delegates.
438
This was an ongoing issue he claims
he raised directly with Mr. Hutchings.
439
Furthermore, the members of the Safety
Team were primarily first aid officers, rather than experienced safety officers.
440
430
Ex C6(51), [13]
431
Ex C6(51), [13]; T6-20, lines 34-45
432
Ex C6(51), [14]; T6-21, lines 25-45
433
T6-22, lines 30-50
434
Ex C6(51), [51] – [53]
435
Ex C6(51), [16]
436
Ex C6(51), [71]
437
T6-24, lines 24-35; T6-37, lines 1-10
438
T6-24, lines 25-48
439
T6-24, lines 35-45
440
T6-24, lines 40-48
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 74 of 274

Mr. Thompson described the safety systems in place at Dreamworld at the time
of his commencement as ‘quite immature’.
441
279. In terms of issues associated with rides or operating procedures, Mr. Thompson
stated during the inquest that whilst he would have assisted had any issues been
raised with him, he does not recall this ever taking place in relation to the
TRRR.
442
Figtree Reporting System
280. Figtree is an electronic database that was utilised by Dreamworld at the time of
the tragic incident to record any injuries, hazards or incidents that occurred
throughout the Theme Park.
443
Corrective action taken was then noted in the
system.
444
Mr. Thompson described the system as ‘reactive management’.
445
281. During the inquest, Mr. Hutchings stated that he wanted to introduce a risk
register across the business, which would record all of the risks within each
department, the perceived level of risk and also ways to control and reduce the
risk.
446
He stated that he received some ‘pushback’ for this idea.
447
Mr. Hutchings
noted that at the time, the document control systems in place at Dreamworld
were ‘quite poor’, and he was concerned that there may have been a range of
risk management activities occurring, which weren’t being recorded in any kind
of formal register.
448
He was advised over a number of years that the funding
wasn’t available for such a register.
449
In 2009, a new risk management system
was introduced to Dreamworld, however, Mr. Hutchings noted that the system
was not used as widely as he would have hoped as it was not sufficiently user
friendly.
450
282. Mr. Hutchings acknowledged that within Dreamworld there was segmentation of
knowledge between the Departments, which caused him concern as there was
a perception and tendency that issues within Dreamworld were someone else’s
responsibility.
451
This tendency was not deliberate, but rather a
misunderstanding as to each Department’s responsibility.
452
TRRR Risk Assessments
283. From the sparse and haphazard records provided by Ardent Leisure, it appears
that various ‘risk assessments’ were conducted on different aspects of the rides
by members of the Safety, Operations and Attractions Departments.
453
The
template documents used for these assessments had a risk matrix, which were
pre-designed and broadly applied for all of the investigations conducted.
454
The
catalyst for such assessments seem to be issues raised by Ride Operators or
441
T6-35, 36, lines 1-11
442
T6-27, lines 17-40
443
Ex C5(23)(c), pg. 6
444
Ex B3C(50), pg. 13
445
T6-16, lines 28
446
T21-16, lines 40-47
447
T21-16, lines 35-47
448
T21-17, lines 25-40
449
T21-17, lines 32-40
450
T21-18, lines 1-40
451
T21-33, lines 23-50; T21-34, lines 1-5
452
T21-34, lines 9-18
453
Ex C8(3), pg. 5 & 6
454
Ex C5(23)(c), pg. 19; Ex C5(23)(d)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 75 of 274
other staff about corrective actions or work that needed to be undertaken.
455
284. Whilst the scope of these risk assessments varied somewhat, it is clear from the
material provided that a documented engineering risk assessment of the ride,
adequately considering the hazards posed by different components or the ride
as a whole, was never conducted. This is particularly troubling having regard to
the previous incidents already documented.
285. Based upon the documentation, a summary of the ‘risk assessments’ conducted
on the TRRR is outlined below. Given the limited and poor record keeping and
databases maintained in relation to such assessments, it is not possible to
determine if any further undocumented assessments were conducted, and what
changes if any were subsequently made.
286. On 9 July 2015, Mr. Deaves, Mr. Alex Navarro, Mr. Shane Green and Ms.
Anneke Triebels conducted a ‘risk assessment’ of various aspects of the TRRR,
including breakage of the conveyor chain and the depth of the watercourse.
456
It
is not clear what the catalyst was for this risk assessment. Ms. Horton does recall
two instances were rafts had slid down the conveyor, whilst on the mechanism.
457
287. The issues considered and findings reached in the Risk Assessment Form are
as follows:
Task/Topic/Issue
Description of
Hazard
Description of
potential hazard
Current control
measure
L
C
R
Comment
Components on the
conveyor chain
have been
identified as posing
a risk of breakage
due to thinning of
metal components
Conveyor
chain breakage
Chain breakage will
lead to an derailing of
conveyor, potentially
causing:
-
Rafts potential to
slide
backwards/colliding
creating a backlog
-
High potential for
debris (chain
components as well
as t
imber palings)
to congest
conveyor area as
well as pump
components
- Potential for raft to
flip
Alarm/Code 6
activation
1
3
1
1
4
4
4
4
4
12
4
4
Suggested control
mechanism:
Sensor mechanism
fitted toward the
bottom
of the
conveyor will
identify breakage
or derailing of
chain.
Roll back gates to
be fitted to prevent
rafts from sliding
backwards down
conveyor.
Additional sensor
fitted to identify
stationary rafts in
pool immediately
prior to conveyor
will identify flip risk.
Depth of
watercourse
immediately prior to
conveyor load
Approx. 2m
pool – non
compliant with
AS
Depth could potentially
result in raft being
flipped in this space
Alarm/Code 6
activation
1
4
4
Platforms and rails
to be added to
reduce depth/risk
of flipping.
455
T14-34, lines 7-20
456
Ex B12(8)
457
Ex B3C(26), [11]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 76 of 274
288. The chart shows how the Likelihood (L), Consequence (C) and overall qualitative
risk (R) was rated by the evaluation team. The R measurement of four for most
of the potential hazards cited suggested that they were a ‘low risk’. The risk of
rafts sliding backwards and colliding was found to be 12, which is in the ‘high
risk’ rating and required management’s attention.
458
289. A further Risk Assessment was conducted on 19 October 2015, in relation to the
sufficiency of the CCTV monitoring at the TRRR, which consisted of one small
monitor broken up into nine screens.
459
It was thought that a further screen would
allow the Ride Operator at the Main Control Panel to have better visibility of the
ride in order to evaluate the risks in the ‘ride envelope’.
460
It is significant to note
that one of the reasons for the need to be able to evaluate the risk of the ride
was increased ride breakdowns in recent months.
461
290. Ms. Ramsay and Mr. Jason Johns subsequently attended the TRRR for the
purpose of conducting a ‘risk assessment’ of the issue, which consisted of
examining the monitors and speaking to the Ride Operators on shift to ascertain
their thoughts on whether the change would be of assistance.
462
The risk
assessment was subsequently sent to Mr. Fyfe, and a work order generated.
463
An extra larger screen was installed at the ride as a result.
464
291. The Risk Assessment Form, and findings reached, are as follows:
465
Task/Topic/Issue
Description of
Hazard
Description of
potential hazard
Current control
measure
L
C
R
Comment
Monitor –
surveillance of ride
area
Monitor split
into 9 screens
(5 in use, 4 not)
making the size
of the screens
in use too small
to evaluate
risks in ride
area
Inability to see risks
in the ride area –
Has the potential to
miss persons in the
water/ride area
1 x monitor split in
to 9 small screens
3
3
9
Additional monitor
available if needed.
Increased ride
breakdowns in
previous months
Inability to see
potential
danger to
guests
Injury to guest,
guests in restricted
area, guest in water
1 x monitor split in
to 9 small screens
3
3
9
292. Whist a score of nine on the risk analysis matrix was found to be a ‘moderate
risk’, it was noted in the risk assessment that Attractions Supervisors had the
ability to source another monitor if required, and could increase the size to make
it easier for Operators to see guests in rafts, guests that have the potential to fall
in the water, guests in restricted areas and another potential danger that arises
during the operation of the ride. It was specifically recognised that, ‘As we are
unable to lose one camera, the recommendation is to have one monitor with 4
split screens and an additional monitor with 1 big screen to monitor rafts as they
458
Ex B12(8), pg. 2
459
Ex C5(23)(c), pg. 13; Ex C5(23)(d)
460
Ex C5(23)(d)
461
Ex C5(23)(d)
462
Ex C5(23)(c), pg. 14
463
Ex C5(23)(c), pg. 15
464
Ex C5(23)(c), pg. 15
465
Ex C5(23)(d)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 77 of 274

approach the conveyor area. This is the area that is high risk if there is a
breakdown on the ride’.
466
ENGINEERING & TECHNICAL (E&T) DEPARTMENT
293. At the time of the incident, Mr. Christopher Deaves was the General Manager of
the E&T Department, whom consisted of around 40 staff members, 25 of which
worked on amusement rides at the Park.
467
He was not a qualified engineer,
although he had an Advanced Diploma in Mechanical Engineering as well as
trade qualifications in metal fabrication.
468
He commenced employment with
Dreamworld in April 2012.
294. As the General Manager of Engineering, Mr. Deaves describes his
responsibilities as including asset management through repairs and
maintenance, which includes amusement rides as well as other varied business
facilities.
469
He previously worked at Village Roadshow for 12 years as the
Engineering Coordinator, where he had oversight of the Engineering Department
for Sea World, Movie World, Wet ‘n’ Wild, Paradise Country and Australia
Outback Spectacular.
470
When Mr. Deaves was first recruited by Dreamworld,
he reported to Mr. Bob Tan, who was the General Manager of Engineering and
Special Projects. The position Mr. Deaves occupied had reportedly been vacant
for some time.
471
Mr. Tan left Dreamworld in January 2016.
472
He is presently the
Vice President of Technical Developments at PT Trans Studio in Indonesia.
473
295. Upon commencing at Dreamworld, Mr. Deaves found that the records and
document control, including for the rides, safety systems, maintenance and
training of staff, were significantly lacking, with the limited information available
difficult to navigate for the purpose of retrieval, cataloguing and distribution.
474
Compared to the document control architecture in place at Village Roadshow,
Mr. Deaves described that at Dreamworld as needing to evolve, with the first step
being to ensure that the right information was available.
475
He notes that he was
focused on addressing the asset management system, which was to interface
with the safety management system, of which MEX was a large component.
476
However, without a formal document and control system in place, he notes that,
‘most of the platforms to manage safety of all asset management were failing
because the information always wasn’t available and it wasn’t available to
everybody who needed it’.
477
The sourcing and storage of information was also
difficult, as it was not easy to locate and therefore hard to determine whether the
requisite up to date information as to ride, maintenance and staffing had been
maintained.
478
Mr. Deaves commenced by trying to gather information and
records to create an asset register so as to determine whether each of the rides
were compliant with various specifications and the requisite Australian
Standards.
479
Once all of the information had been collated and it was
466
Ex C5(23)(d)
467
Ex B3C(46), pg. 10 & 11
468
Ex B3C(46), pg. 6
469
Ex B3C(46), pg. 6
470
Ex B3C(46), pg. 7
471
Ex B3C(46), pg. 8 & 9
472
Ex B3C(54), pg. 3
473
T29-3, lines 24-32
474
Ex B3C(46), pg. 12 & 51
475
Ex B3C(46), pg. 13
476
T22-36, lines 3-18
477
Ex B3C(46), pg. 14
478
Ex B3C(46), pg. 55
479
Ex B3C(46), pg. 55
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 78 of 274

determined to be adequate, he intended to develop systems to ensure this
document control continued, which was still taking place at the time of the tragic
incident.
480
According to Mr. Deaves, this was an ‘enormous process’, which he
estimated would take at least two years.
481
296. Mr. Scott Ritchie was the Engineering Supervisor (Electrical), with Mr. Mark
Watkins and Mr. Wayne Cox performing the role of Engineering Supervisors
(Mechanical). Mr. Ritchie is a qualified electrician, having commenced in the role
of Electrical Supervisor in 2013.
482
Mr. Watkins and Mr. Cox are both qualified
fitters and turners, with a wealth of experience.
297. Engineering Supervisors were required to manage teams of E&T staff and co-
ordinate and supervise daily work, as well as plan maintenance to be undertaken
within the Park.
483
All of the Engineering Supervisors reported to Mr. Deaves.
298. Within the E&T Department there were qualified electricians, fitters and turners,
mechanics, boilermakers, welders, trades assistants and apprentices.
484
The
electrical team, which consisted of a number of electricians, including Mr. Jacob
Wilson, Mr. Quentin Dennis, Mr. Mark Palmer, Mr. Daniel Thompson, Mr.
Francois De Villiers and Mr. John Lossie were specifically managed by Mr.
Ritchie.
485
Their responsibilities on any given day included the following:
486
• Performing prescheduled maintenance of equipment around the park on
any electrical components (which includes pumps, motors and anything
electrical); and
• At times, undertaking the role of electrical ‘Park Technician’ and attending
breakdowns of any electrical components of rides. This includes
attending rides to resolve any issues, as well as carrying out general
electrical repairs for items, such as air conditioners, power points, lighting
and switches.
299. Within the E&T Team, daily pre-start meetings with all staff allocated on shift that
day were generally held, conducted by the Supervisor rostered that day.
487
Topics discussed during these meetings included who was allocated to which
ride, nominations of the Park Technicians for the day, procedures and any faults
that had been experienced on rides the previous day.
488
Weekly safety meetings
were also conducted, and generally took place on a Wednesday for all staff.
489
300. Informal ‘Take 5’ or ‘Toolbox’ meetings were also conducted, which typically
occurred at least once a month to discuss specific work related issues and safety
topics.
490
These sessions were conducted by the Engineering Supervisors or Mr.
Deaves, with the information discussed being placed on the Notice Board for all
employees to read. Formal training was also provided in relation to specific safety
issues and procedures, such as chemical training, low voltage rescues or lock-
480
Ex B3C(46), pg. 57 & 58
481
Ex B3C(46), pg. 58; T22-88, lines 10-47
482
Ex B3A(18), [5] & [6]
483
Ex B3A(18), [9] & [10]
484
Ex B3C(6), [4]
485
Ex B3C(12), pg. 2; Ex B3C(38), [12]
486
Ex B3C(12), pg. 2; Ex B3C(38), [13]
487
Ex B3C(38), [22]; Ex C5(29)(a), pg. 7
488
Ex C5(29)(a), pg. 7
489
Ex B3C(13), [20]
490
Ex B3C(38), [19]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 79 of 274

out procedures.
491
301. Two Park Technicians were rostered each day from the E&T Department, who
were responsible for attending each of the ride breakdowns.
492
They were
required to attempt to diagnose the issue and rectify it if possible. Other specialty
staff were also able to be called to assist with the issue, if necessary. The
response was time-based, so extra support would be provided if a fault could not
be rectified in a certain time.
493
Whilst it was intended that one of the Park
Technicians be from the electrical specialty and the other mechanical, it was
sometimes the case that, due to staff constraints, both of the nominated Park
Technicians were mechanical staff.
494
Safety Issues Identified by E&T Staff
302. According to Mr. Wilson, an electrician, staff were encouraged to communicate
any safety issues with a Supervisor at any time, which could be informing a direct
line Supervisor or another of the E&T Department supervisors.
495
If any concerns
were held by a member of the E&T Department as to the safety of a ride, this
was to be escalated to an Engineering Supervisor to consider having it shut
down. This decision rested with the Supervisor.
496
Mr. Lossie shared this view,
stating that all employees had the authority to express safety concerns about a
ride to an E&T Supervisor or Mr. Deaves.
497
Mr. Cox reiterated this was the case,
and that he would make a determination as to the further action necessary.
498
303. Down-time reports for rides were clipped up on the whiteboard in the Engineering
workshop for all staff to consider.
499
304. It does not appear that ‘risk assessments’ of rides within the park were carried
out by members of the E&T Department prior to the incident.
500
Evidence
provided by staff within the Department suggests that the team were delegated
to develop and implement controls for a potential hazard, once this had been
brought to the attention of the E&T Department.
501
According to Mr. Deaves, he
recalls participating in a few ride risk assessments in relation to components of
rides at the request of other Departments, however, describes them as ‘very ad
hoc’.
502
He was unaware if there was any documentation to reflect that such an
assessment had taken place.
503
Mr. Murphy, the maintenance manager, notes
that whilst no one had the specific task of conducting risk assessments on rides
or specific components, it was expected that if a staff member identified a
problem they would report it.
504
305. It does not appear from the records available, and the accounts of senior staff,
that a full risk assessment of the TRRR was ever undertaken internally by
491
Ex B3C(38), [20]
492
Ex B3C(11), [24]
493
Ex B3C(11), [24]
494
T9-29, lines 23-35
495
Ex B3C(12), pg. 4
496
Ex B3C(12), pg. 4
497
Ex B3C(38), [25] & [26]
498
Ex B3C(7), pg. 15
499
Ex B3C(12), pg. 4
500
Ex C5(29)(a), pg. 15; Ex B3C(7), pg. 10; Ex B3C(53), pg. 9
501
Ex C6(27), [58]
502
Ex B3C(46), pg. 29 & 30
503
Ex B3C(46), pg. 31
504
T11-14, lines 35-45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 80 of 274
Dreamworld.
505
Mr. Deaves states that to his knowledge, there had not been any
‘formal assessment’ of the load and unload area of the TRRR.
506
Whilst the ride
was inspected daily by E&T staff, there was no regular assessment process to
proactively determine whether hazards existed on rides, including the TRRR.
507
Rather, issues would only be considered reactively, when an incident
occurred.
508
Furthermore, staff within the E&T Department were not aware of any
previous risk assessments that may have been carried out on the TRRR.
509
306. Mr. Deaves describes the Operations Department as owning the device or ride,
and the E&T Department as the maintainers.
510
Training for E&T Department Staff
307. Staff have stated that for new members of the E&T Department one on one
learning sessions were provided, until a staff member was assessed as
competent for a particular ride.
511
Each person deemed competent to maintain a
ride, would be noted in the log book located at the ride.
308. Staff from the E&T Department have previously participated in some training and
drills for emergency response and management, which include tiger escapes
and simulated emergency response drills for the Buzzsaw ride.
512
309. Electrical staff also participate in role specific training from time to time, including
low voltage rescues, and CPR and First Aid courses (which are undertaken
annually).
513
New procedures for rides, such as lock-out tag-out training is also
completed, the most recent prior to the incident being in early 2016.
514
Role of Junior Engineer
310. In September 2014, Mr. Gen Cruz was employed as a junior engineer to work
within the E&T Department at Dreamworld reporting to Mr. Deaves.
515
He had
an engineering degree, which he obtained in 2013.
516
311. According to Mr. Deaves, Mr. Cruz was recruited for two main purposes, one of
which was to consider the efficiency of the utilities, such as water, gas and
electricity within the Park. The second was to gather current information and data
as to rides, maintenance and training.
517
He was not employed to undertake risk
assessments of the rides, and it was recognised that he did not have the
necessary skills to do so.
518
It appears that Mr. Cruz was required to consider
and audit the records pertaining to each ride, referred to as ‘data mining
compliance’, which he commenced with the Class 5 thrill rides.
519
This involved
identifying gaps in the information retained by Dreamworld with respect to the
505
Ex B3C(46), pg. 75
506
T22-35, lines 23-30
507
T22-44, lines 7-22; 22-47, lines 1-10
508
T22-47, lines 18-48
509
Ex B3C(7), pg. 10
510
Ex B3C(46), pg. 30
511
Ex B3C(13), [19]
512
Ex B3C(12), pg. 3
513
Ex B3C(12), pg. 3
514
Ex B3C(12), pg. 3
515
Ex B3C(53), pg. 5
516
Ex B3C(53), pg. 6
517
Ex B3C(46), pg. 73
518
Ex B3C(46), pg. 73
519
Ex B3C(46), pg. 88
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 81 of 274
rides.
520
312. Mr. Cruz described his responsibilities as a project relating to ‘ride auditing’, by
considering existing maintenance programs within Dreamworld for each of the
rides, and ensuring that they harmonised with the national audit tool and were
up to date with the manufacturers’ specifications, standards and regulations.
521
He was also considering the power and water usage around the Park. Mr. Cruz
states that in order to perform his role, he considered AS-3533 Part 3, which
relates to in-service inspections, for which he was mentored directly by Mr.
Deaves.
522
He subsequently developed checklists, which he went through for
each of the rides, in consultation with Mr. Deaves.
523
313. With respect to the TRRR, prior to the tragic incident, Mr. Cruz had not conducted
a risk assessment of the ride, nor considered the maintenance program.
524
He
does not recall ever sighting a documented risk assessment relating to the
TRRR.
525
According to Mr. Deaves, Mr. Cruz was only a few months away from
considering the TRRR as part of his audit.
526
The difficulty associated with
locating the information pertaining to the ride was that it wasn’t in a central
location, but rather detailed in paper-based records, and also on individual’s
computers and hard drives.
527
314. During the inquest, Mr. Cruz stated that he had been instructed to prioritise the
nine Big Thrill Rides (Class 5 rides), with the TRRR toward the end of the list of
rides to audit as it was a Class 2 ride.
528
The decision on how rides were
prioritised rested with Mr. Deaves.
529
Mr. Deaves explained during the inquest,
that Class 5 rides had more complex systems controlling them, and as such, the
inspection criteria under the Australian Standards would be higher.
530
315. Mr. Cruz confirmed during the inquest that he did not conduct any engineering
risk assessments of any of the rides at Dreamworld prior to the tragic incident.
531
Mr. Deaves stated during the inquest that following the mining of information
being undertaken by Mr. Cruz for each ride, the next step was ‘hazard
discovery’.
532
This process had not commenced at the time of the tragic incident.
316. Following the tragic incident, Mr. Cruz’s role changed ‘dramatically’ whereby he
is now more involved in the corrective actions imposed by external auditors.
533
Mr. Bob Tan’s Role
317. Mr. Tan was the longest serving staff member of the E&T Department, ceasing
employment with Dreamworld around 10 months before the tragic incident. He
commenced working at the Theme Park in September 1987, initially as an
520
11-105, lines 1-18
521
Ex B3C(53), pg. 6 - 8
522
T11-93, lines 5-35
523
T11-93, lines 40-47
524
Ex B3C(53), pg. 8; T11-94, lines 37-45
525
Ex B3C(53), pg. 8 & 9
526
Ex B3C(46), pg. 96
527
T22-37, lines 32-45
528
T11-94, lines 40-50
529
T11-96, lines 37-40
530
T22-37, lines 10-35
531
T11-101, lines 1-5
532
T23-100, lines 1-20
533
Ex B3C(53), pg. 7
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 82 of 274

Assistant Maintenance Controller.
534
He held a Diploma in Mechanical
Engineering awarded by Singapore Polytechnic in 1976, and whilst employed by
Dreamworld, he obtained First Class Honours in Mechanical Engineering from
QUT in 1992, and a Post Graduate Diploma from QUT in Project Management
in 1994.
535
He became the Technical and Services Director at Dreamworld in
1996, before being moved to Special Projects briefly in 2004.
536
He was
appointed as the General Manager of Engineering in 2007, before becoming the
General Manager of Special Projects in 2014.
537
318. In 2005, Mr. Tan was given the responsibility of project managing the
development of White Water World, as well as the introduction of the new ride,
the FlowRider, at Dreamworld.
538
During this time, given the scope of the project,
the role of the General Manager of Engineering was filled by Mr. Tony
Hawkins.
539
By 2007, Mr. Tan had returned to being the General Manager of
Engineering for Dreamworld, however, in addition, he retained the responsibility
of implementing new rides at the Theme Park.
540
319. As the Engineering Manager at Dreamworld over a number of years, which
included between 2007 to 2013, Mr. Tan’s responsibilities, per the position
description prepared, appear to have included the following:
541
• Oversee the maintenance of all rides, plant, equipment, property and
operating assets; define and review preventative maintenance schedules
to optimise efficiency, safety and best practice methods.
• Establish engineering methods, policies and procedures and oversee
their implementation to give effect to safety policy.
• Direct the regular review of plant and equipment to ensure it meets safety,
efficiency and quality requirements and report on other options available
to achieve objectives.
• Implement approved safety-related actions as determined by Safety
Executive Committee, QEST and audits.
• Establish the systems for and oversee the keeping of maintenance
records.
• Ensure activities related to the engineering and technical function comply
with relevant Acts, legal demands and ethical standards.
320. As the Engineering Manager, Mr. Tan had the authority to:
542
• Take actions and issue inspections that may be reasonably required to
assure safety of any ride, equipment or asset;
534
Ex B3C(54), pg. 3
535
Ex B3C(54), pg. 3
536
Ex J1
537
Ex B3C(54), pg. 6; Ex J1
538
T29-8, lines 2-18; Ex J1
539
T29-8, lines 5-20
540
T29-8, lines 22-30; Ex J1
541
Ex C7(20), pg. 2
542
Ex C7(20), pg. 3; T29-55, lines 35-45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 83 of 274

• Sign off on expenditure up to the delegated amount; and
• Represent the company to statutory body officials in regard to technical
matters.
321. Whilst Mr. Tan held a number of different positions during his almost 30 year
tenure with Dreamworld, given his expertise and experience, it is clear that he
was consistently involved in the engineering aspects and decisions made at the
Theme Park. Whilst he primarily reported directly to the CEO, at different times,
he also had various staff reporting to him, including the Engineering Manager.
543
322. Mr. Tan claims that in relation to decisions as to the conduct of ‘safety audits’ of
amusement ride, directives were given by the Board to the CEO, who in turn
allocated such matters to the Safety Manager and Mr. Tan to implement.
544
Records in relation to these audits were maintained by the Safety Department.
545
323. During the inquest, Mr. Tan stated that he and the E&T Department were
responsible for conducting assessments of amusement rides at Dreamworld to
the AS-3533.
546
He claims this was done by way of the daily inspections and ‘our
regime of periodic inspections on equipment’, including the annual shutdowns.
547
He clarified that this did not involve considering the design of the ride, pursuant
to AS3533.1, but rather the maintenance requirements in Part 2 and 3.
548
324. Mr. Tan left Dreamworld in January 2016 in order to accept a role in Dubai.
Following his departure, Mr. Tan’s hard drive was retained by the Theme Park,
as it contained a number of significant historical and current records relating to
the engineering aspects and history of the rides, including drawings, manuals,
incident reports, design registration documentation, as well as electrical,
mechanical and structural drawings and documentation.
549
It appears that the
contents of this hard drive was gradually integrated into the broader system held
by Dreamworld, however, was only accessible by E&T staff.
550
325. During the inquest, Mr. Tan acknowledged that given his long tenure at
Dreamworld and the roles he performed, he had extensive knowledge of the
engineering aspects of the Theme Park.
551
Nonetheless, he was unable to say
where information as to a safety audit conducted on a ride or decisions made to
alter or modify devices were documented and retained.
552
Mr. Tan did state,
however, that up until 2000, records were maintained manually before the
process of recording electronically was commenced.
553
E&T Department Knowledge of the Design, Modifications and Incidents on the
TRRR
326. From the accounts provided during the course of the investigation and inquest
hearing, it is evident that only a scant amount of knowledge was held by those
543
Ex B3C(54), pg. 4
544
Ex B3C(54), pg. 4
545
Ex B3C(54), pg. 5
546
T29-27, lines 25-47
547
T29-27, lines 30-40
548
T29-27, lines 33-40
549
T12-54, 55, lines 1-25 & T12-55
550
T12-54, lines 40-48
551
T29-9, lines 5-15
552
T29-18, lines 1-17
553
T29-22, lines 17-45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 84 of 274

in management positions at Dreamworld, including Mr. Deaves, as the General
Manager of Engineering, as to the design, modifications and past notable
incidents on the TRRR.
554
327. Mr. Deaves was unaware as to when any of the changes to the TRRR, such as
the removal of the turntable or the conveyor slats, had been undertaken, or the
reasons why such alterations were made.
555
Mr. Deaves noted that to his
knowledge, there had not been any ‘formal assessment’ of the load and unload
area of the TRRR.
556
Whilst the ride was inspected daily by E&T staff, there was
no regular assessment process to proactively determine whether hazards
existed on rides, including the TRRR.
557
Rather, issues would only be considered
reactively, when an incident occurred.
558
328. It was recognised by Mr. Deaves that there were no records kept, which were
easily accessible or centrally located, whereby staff responsible for the safety of
the rides, both from an operations and engineering perspective, could examine
and consider previous issues associated with a device. This absence of effective
and complete record keeping essentially precluded any staff from being in a
position to be able to appropriately and adequately assess and manage the risks,
which may be present on rides, particularly those like the TRRR, which was 30
years of age. It is significant that the General Manager of Engineering at
Dreamworld had no knowledge of past incidents involving rafts coming together
on the TRRR. It is arguable that this lack of knowledge essentially prevented him,
and anyone else, from assessing or determining risks associated with the TRRR
from an engineering perspective.
329. Furthermore, it became clear during examination at the inquest that Mr. Deaves
had a very limited knowledge of the operation of the ride and the various
components. Whilst his role may have involved a heavy administrative and
coordination component, the fact that there was no one employed at Dreamworld
who was dedicated or qualified to undertake full risk assessments of the rides,
including the TRRR, from an engineering and hazard perspective, is of significant
concern.
559
330. Mr. Deaves acknowledged during the inquest that given the previous incidents,
which had occurred on the TRRR, a root cause analysis should have been
conducted, to determine whether engineering upgrades or modifications needed
to be made to the TRRR to ensure that contact between rafts didn’t happen
again.
560
331. Whilst Mr. Tan, given the duration of his tenure and involvement, was expected
to have retained personal knowledge of these modifications, when he left
Dreamworld in 2016, records as to the alterations made and reasoning were
scant and difficult to locate.
332. In relation to the TRRR, Mr. Tan claims that he had no direct knowledge of the
design of the ride as it was already in operation when he commenced
554
Ex B3C(46), pg. 92; Ex C8(6), pg. 18; T19-48 & 49; T23-4 - 9
555
Ex B3C(46), pg. 92 & 93
556
T22-35, lines 23-30
557
T22-44, lines 7-22; 22-47, lines 1-10
558
T22-47, lines 18-48
559
T23-9, lines 40-45
560
T23-5 & 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 85 of 274

employment with the Theme Park.
561
He was aware of issues associated with
the rotating table initially in place on the ride, and the conveyor motor power
capacity.
562
The modifications subsequently made to address these issues were
to rectify the bearings and track, as well as reducing the load on the conveyor by
removing the number of slats.
563
Mr. Tan claims that whilst he was aware that
there were no manufacturer’s specifications and recommendations as the ride
was built in house, the maintenance schedule and strategy for the ride was
developed prior to his commencement at Dreamworld.
564
He acknowledged that
he was involved in the additions and changes made to the TRRR up until the
time he resigned from Dreamworld.
565
He further stated that whilst there was no
formal process for considering holistically the component parts and maintenance
suggestions for the ride, this was done.
566
333. In relation to the ‘nip point’ between the end of the conveyor and steel support
rails on the TRRR, Mr. Tan stated during the inquest that he never identified this
as an issue from an engineering perspective.
567
334. According to Mr. Tan, engineering controls were considered for the TRRR to stop
the conveyor in the event of a pump failure, however, a safer system could not
be identified.
568
Mr. Tan noted, ‘simply stopping the conveyor if a pump failed
had the potential to create new hazards and risks’.
569
335. Mr. Tan was unable to recall whether consideration had been given to the
installation of an interlock system shutting down the conveyor automatically in
the event that a raft was stranded on the support rails positioned near the unload
area, shortly after the end of the conveyor for a period of time, or from a reduced
water level.
570
RIDE MAINTENANCE AT DREAMWORLD
336. For each ride, including the TRRR, daily, weekly, monthly and yearly checks by
various Departments within Dreamworld were conducted. The E&T Department
were responsible for carrying out these tasks at the direction of Mr. Deaves and
the Supervisors.
337. Mr. Stephen Murphy was the Maintenance Team Leader at Dreamworld at the
time of the tragic incident, a position he had held for 2 ½ years.
571
He is a qualified
fitter and turner.
572
338. Mr. Grant Naumann, a qualified fitter and turner, was the Maintenance Planner
at Dreamworld, having held this position since 2007.
573
He reported to Mr.
Deaves.
574
A position description relating to Mr. Naumann’s role describes the
purpose of the position was, ‘to provide leadership, training and management of
561
Ex B3C(54), pg. 5 & 6
562
Ex B3C(54), pg. 6
563
Ex B3C(54), pg. 6
564
T29-11 & 12
565
T29-12, lines 7-24
566
T29-12, lines 28-40
567
T29-16, lines 35-48
568
Ex B3C(54), pg. 13
569
Ex B3C(54), pg. 13
570
Ex B3C(54), pg. 14
571
Ex B3C(13), [7]
572
Ex B3C(13), [12]
573
Ex B3C(14), [5]
574
Ex B3C(15), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 86 of 274

outlined reports within the technical services department and ensure all
procedures are adhered to in accordance with the business.’
575
He was
responsible for the servicing and maintenance of equipment and all buildings at
Dreamworld to the prescribed standards to ensure their safe and efficient
operation.
576
This responsibility included the annual maintenance of all major
rides from an administrative perspective, for which he was required to supervise
the process, organize and direct staff.
577
According to Mr. Naumann, the
prescribed standards applicable to his role related to the requirements of the
Original Equipment Manufacturer, AS-3533 and any regulatory requirements, for
which he was not provided with any specific training.
578
339. Mr. Naumann states that he was hired by Dreamworld to assist with the
implementation of the computerised maintenance management software, known
as MEX, which included the scheduling of works on rides through work orders.
579
340. The MEX system allowed for preventative maintenance to be scheduled for a
ride, which was manually controlled by Mr. Naumann, who was also responsible
for generating the associated work orders.
580
Whilst he was aware of the
Breakdown Policy for rides, he was not notified of any breakdowns on rides.
581
341. According to Mr. Naumann, work orders for maintenance and changes to rides
could be generated by the Safety Department or Mr. Deaves as the head of the
E&T Department, following the identification of an issue, or based on
recommendations made by JAK and other external auditors.
582
A MEX ops is the
avenue available for members of other departments, such as Food and
Beverages or Attractions, to request certain maintenance work be undertaken.
583
Such requests could be declined if capital expenditure was needed, which would
require a supervisor to obtain the relevant permissions or for a necessary risk
assessment to be carried out.
584
To the best of Mr. Naumann’s knowledge, risk
assessments of the rides were carried out by the Safety Team at Dreamworld
and not the E&T Department.
585
342. In terms of records retained in relation to maintenance at Dreamworld, whilst log
books were not maintained, daily work orders and spreadsheets were kept for
each ride, with annual maintenance information recorded on a spreadsheet
listing the tasks to be performed and those who had actioned it.
586
Mr. Naumann
stated during the inquest that he was only ‘vaguely’ aware of where the various
maintenance tasks lists for the TRRR, as an in-house custom built ride, were
generated.
587
343. Mr. Deaves claims that whilst budgetary constraints at Dreamworld may have
impacted on requests to rectify negotiable components of the Park, such as
presentation like paint work, upgrades or changes to safety systems and the
575
Ex C7(21)
576
Ex C7(21)
577
Ex B3C(14), [6] & [10]
578
T11-40, lines 25-47
579
Ex B3C(15), pg. 4
580
Ex B3C(15), pg. 5; Ex B3C(15), pg. 8
581
Ex B3C(15), pg. 9
582
Ex B3C(15), pg. 17; see Procedure Ex D7(847)
583
Ex C5(28)(a), pg. 17
584
Ex C5(28)(a), pg. 17
585
Ex B3C(8), pg. 11
586
Ex C5(28)(a), pg. 14
587
T11-75, lines 14-41
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 87 of 274
maintenance of the rides were not delayed or refused due to cost.
588
Daily Inspection
344. Checklists were developed for each ride listing the items that needed to be
examined and inspected by maintenance and engineering staff on a daily
basis.
589
The time taken to carry out and complete the requirements of each
checklist differed. It was estimated that the daily service and inspection of the
TRRR was around 35 minutes to 60 minutes for two staff.
590
345. For the TRRR, staff were required to check a number of points on the ride
including:
591
• Operators Report - carrying out any repairs listed
• Operation: remove ride inhibitors and E-stop lanyard function
• Conveyor: Various including chains, planks and bolts, chain-break sensor
• Raft Gates: Various including pivot bushes and pins, gate operation
• Rafts: Various including tubes check for damage, tube inflation, seating
plug, seat belt security and integrity, drain rafts.
• Pumps: Spider bearings and glands
• Waterway: Various including barriers, logs and water top-up
• Animation: Tunnel lights and animation operational
• Camera: Check operation 5 off
• Filter: back wash filter under Mine raft
• Rafts in use: Number of rafts in use circled
346. Each of these components, once checked, was required to be initialled by the
competent person. These daily checks were conducted by members of the E&T
Department, however, an electrician (members of this group) was generally not
involved unless an electrical issue was identified by the technicians undertaking
the checks.
592
On average, it took a team of two staff from the E&T Department
40-45 minutes to complete the requisite checks daily.
593
347. It was noted by members of the E&T Department that the conveyor planks were
checked regularly and replaced if there was any sign of damage or they were
deemed to be in poor condition.
594
588
Ex B3C(46), pg. 17 & 18
589
Ex B12(2) – example of daily pre-service inspection of the TRRR 12
th
October 2016
590
Ex F16C(10) – estimated provided to JAKS in 2004; Ex B12(2) – notation of total man hours taken
591
Ex B12(2)
592
Ex B3C(12), pg. 3
593
Ex B3C(6), [13]
594
Ex B3C(11), [33]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 88 of 274
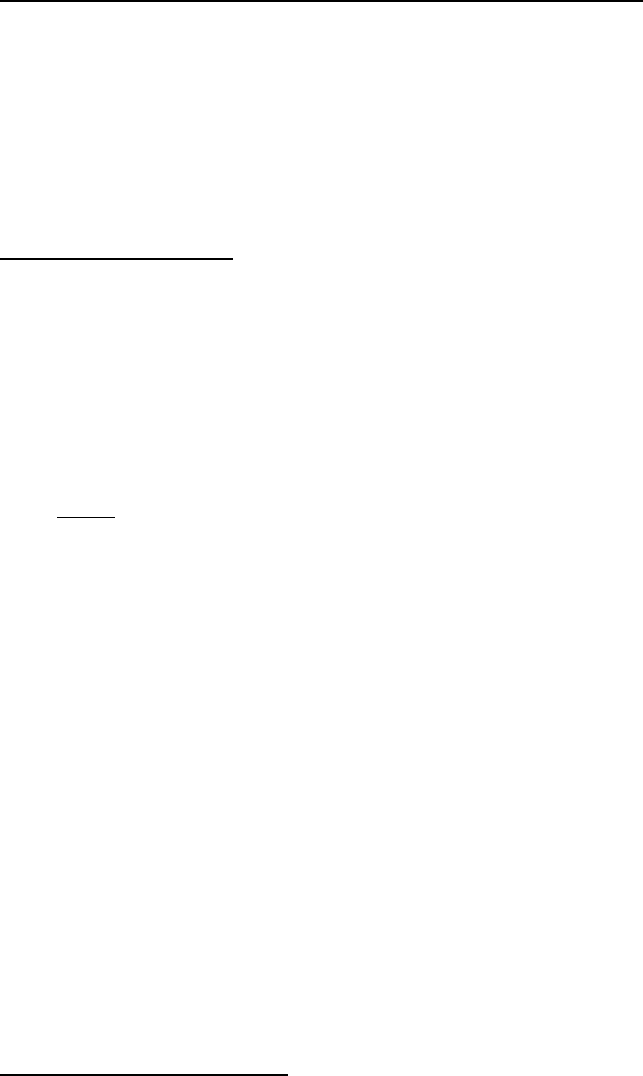
348. In the event that an issue with a ride was identified during the daily inspections,
E&T staff were required to escalate it to the shift Supervisor for a determination
to be made as to whether a maintenance work order needed to be generated for
rectification.
595
The urgency by which corrective action needed to be undertaken
would determine the priority placed on the work order.
596
Daily Operator Pre Start Up and Post Operation Shutdown Sheets
349. At each ride, a daily record of checks by Operations and E&T staff is maintained.
These are designed to ensure the ‘safe daily operation of rides and correct
closure at the end of the day’.
597
Before a ride is able to be opened for the day,
these inspection sheets, which also record the completion of the E&T
Department inspections, in addition to the pre-operation check by the ride
attendants, have to be completed.
598
Prior to an Operator leaving the ride at the
end of the day, the post shutdown checks need to be completed.
599
Breakdown Procedure
350. A formal Breakdown Procedure (‘the Procedure’) was in place at Dreamworld,
which outlined ‘the procedure to be followed when a major ride or piece of
equipment is out of service or reduced capacity due to equipment fault or
failure'.
600
This document was authored by Mr. Deaves.
601
351. The TRRR was a ‘major ride’ within the meaning of the definitions in Part 4 of
the Procedure.
352. Part 5 of the Procedure provided:
• The first response to a breakdown call is to ascertain if there is any
immediate danger to persons or equipment. If so, isolate the danger. If you
are unsure how to do this safely, call a Supervisor BEFORE proceeding.
• If there is no immediate danger attempt to ascertain the fault with the
equipment. If the fault is clearly evident and the repair can be effected within
15 minutes, carry out the repair and report to the Supervisor at the next
available opportunity.
• If there is a repeat of the fault within the next 24 hours do not attempt to
rectify the fault until the Engineering Supervisor has been notified and given
authority to rectify the problem.
• If the equipment is likely to be inoperable for more than 15 minutes the
Engineering Supervisor must be called.
• For any equipment that is inoperable for more than 1 (one) hour or is
required to operate at reduced capacity, the Engineering Manager must be
notified. If a repair or alteration is required to be performed on any control
circuitry or on any other part or component of a piece of essential safety
595
Ex B3C(15), pg. 19
596
Ex B3C(15), pg. 19
597
Ex B12(26), pg. 19
598
Ex B12(15); Ex B12(26), pg. 19
599
Ex B12(26), pg. 19
600
Ex B3A(19), pg. 53 & 54
601
Ex B3C(46), pg. 81
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 89 of 274

equipment. The Engineering Supervisor must be notified and an
independent functional safety test should be carried out before the
equipment is permitted to return to service. The Engineering Manager will
report to the General Manager accordingly.
• If the cause of an issue can’t be positively identified the Supervisor is to be
called and all parties must be satisfied there are no problems operating the
equipment.
• At no time will any safety control systems be compromised to allow for
equipment availability. Any discussion on acceptable criteria under this
procedure must include the involvement of the Engineering Supervisor or
the Engineering Manager. The Engineering Manager will report to the
General Manager accordingly.
• Should a fault or failure occur to a critical component the Engineering
Supervisor and/or the Engineering Manager MUST be consulted to
ascertain if further checks are to be carried out.
• This procedure MUST be followed even when the fault is clearly diagnosed
and seems to be of an insignificant nature. Examples of equipment
requiring reporting would be: harnesses, brakes, zone and speed control
systems.
• During any absences by the Engineering Manager or General Manager, a
delegation of authority will remain in effect until either returns to work.
• If a device is to operate at reduced capacity or with a known non critical
maintenance issue an action plan must be put in place from the person
giving authority to continue operating.
353. Mr. Deaves stated that it was his intention for the Procedure to reflect that if there
was a reoccurrence of a fault within a day (24 hour period), then it was to be
escalated to a Supervisor.
602
354. There was some discrepancy in how this Procedure applied to ride breakdowns
across the Park and when rides would be shut down. According to electrician,
Mr. Dennis, his understanding was that if there were two breakdowns on a ride
in one day, then the Supervisor was to be advised, and could decide whether the
ride remained open.
603
He states that some staff believed that it was three
breakdowns in one day.
604
Mr. Gordon was of the view that, based upon a verbal
direction given by Supervisor, Mr. Wayne Cox during an early morning meeting,
a fault had to occur three times before it was escalated to a Supervisor.
605
Mr.
Cox described the Procedure as follows, ‘we have a policy that if there are three
faults with a ride within the same day, then we close the ride down to source and
rectify the problem.’
606
Mr. Cruz also shared this view based upon a discussion
during a meeting in October 2015, whereby it was stated that the escalation of a
fault to a Supervisor was to occur after the third occasion.
607
602
Ex B3C(46), pg. 81
603
Ex B3C(44), pg. 16 & 17
604
Ex B3C(44), pg. 17
605
Ex C5(29)(a), pg. 13 & 14; T10-80, lines 30-46; T10-83, lines 4-15
606
Ex B3C(6), [16]
607
Ex B3C(53), pg. 13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 90 of 274
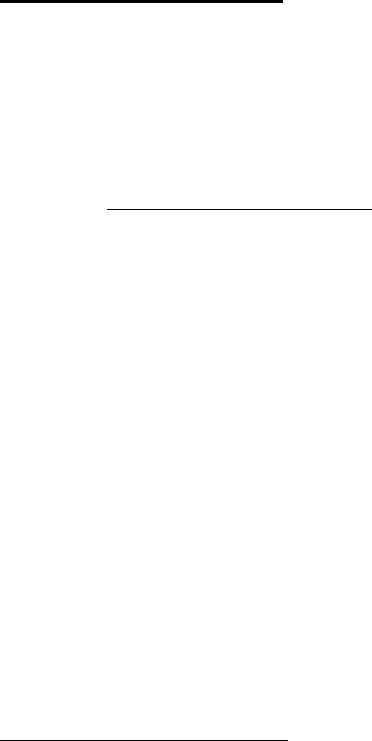
355. From the various accounts provided by members of the E&T Department, there
was clearly some confusion as to how this policy was to be applied, and whether
a fault needed to occur two or three times before it was escalated to a Supervisor
to consider whether the ride needed to be shut down for safety issues.
608
Whilst
the written Procedure was kept in the workshop, it seems that a verbal direction
may have been given, which suggested that the same fault needed to occur three
times before it was necessary to escalate it to a Supervisor.
609
Regardless of
whether this was the case or not, it was evident that there was a lot of confusion
amongst experienced members of the E&T Department as to what the applicable
policy was in relation to ride breakdowns. It appears that some members of the
E&T Department had not seen the formal written Procedure for some time prior
to the incident, and were relying on verbal accounts.
610
356. Furthermore, in relation to ascertaining what may constitute ‘immediate danger’
for a particular ride, including the TRRR, there was no specific training provided
to staff nor any guidance outlined in the Procedure.
611
During the inquest,
evidence was given that staff were not provided with training as to any particular
risks or dangers, which might be present for a ride, or any particular component
of a ride.
612
Park Technician Procedure
357. Dreamworld also had in place a Park Technicians Procedure,
613
which was a
formalised document required to be followed by an E&T staff member nominated
for the role on a particular day. The reference document listed as part of this
procedure was the ‘Breakdown Policy’, which it can be assumed was intended
to be a reference to the ‘Breakdown Procedure’.
358. The Park Technician Procedure stipulates the following:
• On any day during park operating hours there will be at least two
people/staff assigned to the role of Park Technician. One should be
Electrical and the other Mechanical.
• Unless committed to a higher priority both technicians should attend a
call and stay with the rectifications work until complete or otherwise
directed.
• If multiple requests are received simultaneously, the Park Technicians
should contact their Supervisor for assistance.
• Should the situation be, that the first call can be safely completed by 1
(one) technician, they may separate to attend another call.
• Park Technicians should have their breaks at different times to the
majority of engineering staff to allow for responsibility hand over during
their breaks.
608
Ex C5(29)(a), pg. 13 & 14; Ex B3C(8), pg. 8 & 9; T5-27
609
Ex C5(29)(a), pg. 14
610
T5-27, lines 35-47
611
T7-61, lines 25-45
612
T7-61, lines 33-45
613
Ex B3A (19), pg. 56 & 57
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 91 of 274

• When called to a breakdown, the Breakdown Procedure MUST be
followed.
• If the Park Technicians do not have sufficient experience or training in the
area of need, they are to call their Supervisor for further support BEFORE
undertaking any rectification work.
• Generally, it would be expected that a Park Technician with lesser
experience would be coupled with an experienced Park Technician, to
assist with locations, company policies and procedures, and the decision
making process.
• Two way code will be mechanical 5 and calls will be taken directly by the
technician.
• Where practical, there should be a brief meeting between the Park
Technicians and a senior staff member before the start of each operation
shift.
• Topics covered during meetings should include:
Any special events for the day/night
Any rides not operating or on annual shutdown
Reported incidents
Staffing – which staff are available/unavailable.
359. A printed copy of this Procedure was available in the E&T Department workshop.
According to some staff, Supervisors often reminded them of the policy
requirements during pre-start meetings.
614
360. Evidence from staff suggests that this policy was introduced a few years prior to
the incident when the Park Technician role was established. When the policy
was first introduced, E&T staff were trained in the policy.
615
It is not clear from
the recollection of staff whether refresher training was ever provided to E&T staff,
either by way of targeted training or during ‘Take 5’ meetings.
616
361. Any repairs or rectification of issues carried out by E&T staff were recorded in
the Ride Logs, which were located in a folder at each ride.
617
The Park
Technicians are required to fill out the ‘Down Time’ sheet in the Ride Log folder
setting out what the issue was, what was done to resolve the issue, and the
length of time the ride was not operating. The Down Time sheets were collated
each day by the Attractions Supervisors who put the information contained in
these documents into a report, which was emailed daily to Mr. Margetts, Mr. Fyfe
and the E&T Team. The Down Time report is also given to the Park Technicians
each morning, as well as were placed on the whiteboard in the Engineering
workshop.
618
614
Ex B3C(12), pg. 4
615
Ex B3C(38), [29]
616
Ex B3C(38), [29]
617
Ex B3C(38), [31]
618
Ex B3C(38), [32] & [33]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 92 of 274

TRRR YEARLY PREVENTATIVE MAINTENANCE INSPECTION
362. For each ride at Dreamworld, annual preventative maintenance inspections are
conducted, which involve the shutdown of the attraction for a requisite duration,
and various tasks to be completed and examined, which are stipulated on a ride
specific checklist.
619
363. In relation to the TRRR, the annual preventative maintenance inspection, which
involved around eight E&T Departmental staff, included examination and
servicing of the following components of the ride:
• Southern and northern pump, which included electrical connections at
the motor;
• Pump area for the removal of waste material;
• Screens, which include inspection for integrity, security and corrosion;
• Trough area, which includes a visual inspection of trough joints, as well
as the trough gates and logs etc. for security;
• Holding gates 1-6, which includes the operation and integrity of control
valves, airlines and pivot points;
• Tunnel, where the integrity and security of concrete ceiling was to be
inspected; and
• Conveyor, which included the motor (megger test and record results),
Gearbox (for leaks and replace oil), drive train (sprockets for excessive
wear).
364. Any repairs or upgrades to a component of the ride, including replacement parts
and inspections, were to be carried out during this shutdown.
620
All task
performed were documented on a spreadsheet, with the work carried out signed
off by staff.
621
This sheet was retained electronically and as a hard copy.
365. In relation to the TRRR, annual maintenance required that the ride be shut down
for around three to four weeks.
622
Shutdown June 2016
366. Mr. Naumann supervised the TRRR annual maintenance in 2016.
623
He notes
that the shutdown maintenance undertaken was routine, aside from replacement
of the conveyor chain, which involved the removal of planks attached to the
chain, so that it could be replaced, as well as some old planks replaced with
new.
624
He notes that the conveyor had a mixture of new and old planks.
619
Ex B12(12)
620
Ex B3C(14), [11]
621
Ex B3C(14), [11]
622
Ex B3C(14), [9] & [10]
623
Ex B3C(14), [12]
624
Ex B3C(14), [12]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 93 of 274
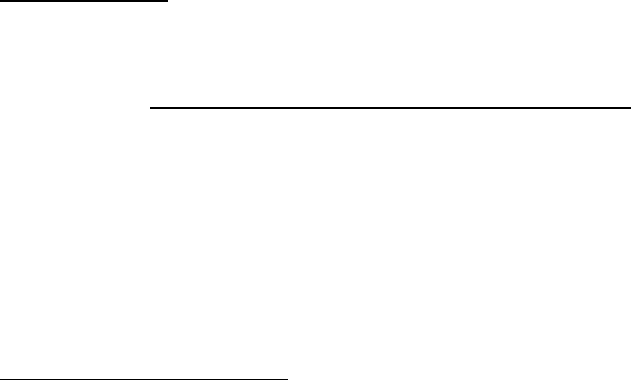
367. During these shut downs, external contractors would sometimes be engaged to
attend the ride to service various components, including the Danfoss Variable
Speed Drives (VSD’s).
625
The most recent occasion that this had occurred was
during the shutdown on 15 June 2016, during which the following areas were
canvassed:
626
• Back up of all drive parameters to LCP
• Check heat sink cooling fan operation
• Visual checks for ‘hotspots’, corrosion and vermin ingress
• Check all Line input and motor connections
• Check earthing and cable screening
• Replace filters where fitted
• Check internal fuses
• Check PCB plugs are correctly fitted and secure
• Remove dust and any other contamination
• Checks DC bus
• Check input & output Voltages & Currents
• Save all settings and other info
368. It should be noted that on this occasion, due to a breakdown of the south pump
on the TRRR, both VSD’s could not be test run.
627
The south pump was down
for maintenance that day. Accordingly, the ‘Check input & output Voltages &
Currents’ component of the schedule could not be completed.
628
RECENT BREAKDOWNS OF THE TRRR
369. On the days shortly prior to the tragic incident, maintenance and down time
records for the TRRR confirm that the ride had experienced a number of
breakdowns, which were primarily related to an ‘earth fault’ recorded on the drive
of the South Pump. The relevant circumstances of each of these breakdowns
are outlined below.
19
October 2016
370. The Down Time Report for the TRRR commencing the week of 17 October 2016,
shows that the ride broke down on 19 October 2016 at 11:20 am with the cause
cited as ‘South pump tripped out – alarm earth fault’.
629
A reset test was
conducted, and the ride returned to operation at 11:57 am.
371. Electrician, Mr. Jacob Wilson attended the Main Control Panel and requested
backup from other members of the E&T Department, due to the nature of the
ride.
630
Team Leader, Mr. Dave Foster, Mr. Michael Stead and Mr. Mark Gordon
subsequently attended the ride to assist.
631
372. Mr. Wilson was advised by Ms. Sarah Cotter, Attractions Supervisor, that the
pump had ceased to operate by itself, and the ride had been shut down.
632
Mr.
Quentin Dennis attended the ride in support of Mr. Wilson, and went to the
625
Ex B3A(22), [4]
626
Ex B3A(22), [5]
627
Ex B3A(22), [6]
628
Ex B3A(22), [6]
629
Ex B15(16), pg. 3
630
Ex B3C(12), pg. 5
631
Ex B3C(9), [11]
632
Ex B3C(12), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 94 of 274
Control Room, where the switchboard and drives are located, to try and
determine the cause of the issue.
633
He advised Mr. Wilson over the two-way
radio that the South Pump display window showed an error, ‘Earth Fault – Alarm
14’.
634
It was decided that the ride should be evacuated, as the error required
further investigation.
635
Mr. Wilson advised the other E&T staff who had attended
to assist with the evacuation of guests.
373. Once guests were evacuated from the ride, Mr. Wilson handed control of the
Main Control Panel to E&T mechanical team member, Mr. Michael Stead and
went to the Control Room to assist Mr. Dennis.
636
Mr. Wilson took a photograph
of the error message on the south pump drive, before attempting to reset the
drive. Despite pressing the reset button on the drive, the fault did not clear.
637
Mr. Wilson contacted Mr. Scott Ritchie, Engineering Supervisor (Electrical), and
advised him of the earth fault.
638
374. Mr. Dennis subsequently tried to fix the error by turning the isolator switch on the
front of the drive to remove power to see if it would reset. When power was
restored, the earth fault had cleared.
639
The south pump was then restarted from
the main Operator control panel, and worked without issue.
640
All the rafts were
moved into the home position at the dispatch area. Mr. Wilson advised Mr.
Ritchie as to the process undertaken.
641
375. On this occasion, Mr. Ritchie was notified and made the decision to have the
‘drive guys’ from Applied Electro attend to examine the cause of the fault. A
request was subsequently made on 22 October 2016 for Mr. Michael Takac, an
Electrician with Applied Electro, to attend the TRRR for a service call for the
VLT.
642
Mr. Ritchie stated that, ‘we have experienced an earth fault on two
separate occasions and cannot fault the motor. We are back up and running now,
however the sooner you are able to get to the site, the better.’
643
He was
scheduled to attend site on 27 October 2016.
644
22 October 2016
376. At 11:05 am on 22 October 2016, a breakdown occurred at the TRRR, which
was attributed to a ‘South Pump earth fault’. This required the ride to be shut
down between 11:05 am and 11:56 am. Mr. Wilson attended this breakdown with
Mr. Mark Watkins.
645
He went to the Control Room, with Mr. Watkins stationed
at the Main Control Panel.
646
He was advised that the south pump had ceased
to operate by itself, however, would not be able to be restarted immediately as
there were ducklings in the area that would need to be removed beforehand.
647
Guests were subsequently evacuated from the ride.
633
Ex B3C(12), pg. 6
634
Ex B3C(12), pg. 6
635
Ex B3C(12), pg. 6
636
Ex B3C(12), pg. 7
637
Ex B3C(12), pg. 7
638
Ex B3A(18), [29]
639
Ex B3C(12), pg. 7
640
Ex B3C(12), pg. 8
641
Ex B3C(12), pg. 8; Ex B3A(18), [29]
642
Ex F12(40)
643
Ibid.
644
Ex B3A(22), [8]; Ex F12(40)
645
T17-11, lines 13-35
646
Ex B3C(12), pg. 9
647
Ex B3C(12), pg. 9
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 95 of 274
377. Mr. Wilson noticed that the South Pump drive had the same fault as had occurred
on 19 October 2016, which he photographed. He called Mr. Ritchie over the two-
way radio, who subsequently attended the Control Room.
648
Mr. Wilson
performed the same reset as Mr. Dennis had on the previous occasion, which
cleared the earth fault.
649
Mr. Ritchie made a comment that he was unsure if the
cooling fans were working, however, this was not a significant concern, which
would warrant the ride being shut down.
650
The south pump was then reset at
the Main Control Panel, and the rafts were returned to the dispatch area.
378. Mr. Ritchie advised Mr. Wilson that he would get ‘the drive guys’ out to look at
the fault.
651
Mr. Wilson offered to megger the motors (conduct an insulation
resistance test), however, Mr. Ritchie stated that this was not necessary.
652
379. Mr. Ritchie subsequently notified Mr. Deaves that day of the fault.
653
According
to Mr. Ritchie he told Mr. Deaves that he believed that there was an intermittent
earth fault with the drive on the South Pump, and given it was the second
occurrence in four days, he intended to request that external drive specialists
attend to further investigate.
654
Mr. Deaves agreed that this was an appropriate
course. According to Mr. Ritchie, the TRRR was ‘the most popular ride in the
Park’ and he was concerned to ensure it was operating properly.
655
He further
states that whilst he was motivated to have the drive specialist attend to
investigate the fault, this was to avoid any further operational down-time not
because he had any concern as to any risk posed from further faults.
656
380. Mr. Ritchie subsequently sent an email to Mr. David Butler at Applied Electro,
the authorised service agent for the Danfoss drives in use, requesting that they
attend site to investigate the recurring issue.
657
Arrangements to have the drives
looked at by external contractors was communicated by way of email to the E&T
Supervisors by Mr. Ritchie that evening.
658
23 October 2016
381. At 10:45 am on 23 October 2016, the TRRR broke down once again due to
‘South pump – tripped north pump earth fault’.
659
A reset test was conducted,
and the ride was returned to operation at 11:02 am. E&T team members, Mr.
Stephen Murphy, Mr. Quentin Dennis and Mr. Frank De Villiers attended the
Code 6 on this occasion, with Mr. Dennis and Mr. De Villiers resetting the drive
in the control room, allowing the pumps to be restarted.
660
It is not clear from the
evidence provided whether an E&T Supervisor was notified of this breakdown.
382. According to Mr. Dennis, he was unaware of the fault the previous day, and had
not been advised by Supervisors at the morning ‘tool-box’ talk.
661
648
Ex B3C(12), pg. 9; Ex B3A(18), [32] & [33]
649
Ex B3C(12), pg. 9
650
Ex B3C(12), pg. 9
651
Ex B3C(12), pg. 10
652
Ex B3C(12), pg. 10
653
Ex B3A(18), [39] & [40]
654
Ex B3A(18), [40]
655
Ex B3A(18), [40]
656
Ex B3A(18), [41]
657
Ex B3A(18), [46]
658
Ex B3C(7), pg. 24-29
659
Ex B15(16), pg. 3
660
Ex B3C(13), [25] & [26]
661
Ex B3C(44), pg. 18
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 96 of 274
383. The following day, Mr. Ritchie was made aware of the fault by way of an
‘Operations Report’, which briefly outlines any issues with rides the previous day,
and is sent via email to all Operations Management Team members and
Maintenance Supervisors.
662
Day of the Incident – 25 October 2016
384. Specific details as to the break downs that were experienced on the day of the
tragic incident are outlined further under the heading, Timeline of Events on 25
th
October 2016.
385. By way of a brief summary, the Down Time Report for the TRRR on 25
th
October
2016,
663
shows that the ride broke down at 11:50 am and 1:09 pm. On both
occasions, the reasons stated for the down time was, ‘South pump dropped
out earth Fault’. The action taken by E&T staff that day was recorded as
evacuating the guests and resetting the drive, following which the ride
restarted.
664
386. Arrangements had been made by Mr. Ritchie for Applied Electro to attend site to
inspect the drives on Thursday, 27 October 2016.
665
387. These records confirm that in the seven days prior to the fatal incident, there
were five breakdowns of the TRRR, which were attributed to a failure of the south
pump due to an ‘Earth fault’. On each occasion, the drive was reset without any
diagnosis of the cause or further investigation being conducted.
TIMELINE OF EVENTS ON 25 OCTOBER 2016
388. On 25 October 2016, the TRRR was operating with nine rafts in circulation and
two Ride Operators.
666
This is the maximum number of rafts able to be utilised
with a two person Operator model. Under this model, there is a No. 1 Operator
and No. 2 operator, who have different responsibilities for the manning and
command of the ride. The No. 1 Operator is responsible for the operation of the
TRRR, as well as the actions of the Load Operator (No. 2 operator). At all times,
one operator is positioned at the Main Control Panel with the other at the unload
station. It is standard practice that the Operators switch roles at regular intervals,
however, the responsibility for the ride remains that of the No. 1 Ride Operator,
no matter where they are positioned.
389. At the time of the incident, Mr. Peter Nemeth (38 years of age) was performing
the No. 1 Operator role, with Ms. Courtney Rhianne Williams (21 years of age)
as the No. 2 Operator. Mr. Nemeth was an experienced Ride Operator having
worked at Dreamworld for four years prior to the incident.
667
He had worked on
the TRRR over the previous two years, initially as a No. 2 Operator for the first
six months, and then as a No. 1 Operator.
668
Training records confirm that he
was trained as a No. 2 Operator for the TRRR on 21 August 2015, which took
one hour and 45 minutes.
669
He estimates that within the last year, he had
662
Ex B3A(18), [43]
663
Ex B15(1)
664
Ex B15(1)
665
Ex B3A(18), [49]
666
Ex B1, pg. 13
667
Ex B3A(1), [1]
668
Ex B3A(1), [5]
669
Ex C7(498)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 97 of 274

operated the TRRR on 50 occasions.
670
390. Due to his experience and tenure, Mr. Nemeth was also a safety representative
for Ride Operators, and engaged in safety audits of rides, which included the
TRRR, identifying any issues of concern to be rectified.
671
These audits were
subsequently submitted to supervisors and the Safety Department for their
consideration and action.
672
Mr. Nemeth was not provided with any specific
training in order to conduct audits, except by the prior representative.
673
He
participated in monthly meetings with the Safety Department and group
inspections were conducted of different departments around the park.
674
391. Whilst Ms. Williams had worked as a Ride Operator in both a part-time and full-
time capacity at Dreamworld since July 2015,
675
the 25 October 2016 was the
first day she was trained as the No. 2 Operator for the TRRR.
676
She had
previously been trained as a Deckhand on the TRRR in December 2015.
677
392. Ms. Amy Crisp and Ms. Sarah Cotter were the Relief Supervisors for the Ride
Operators assigned that day.
678
Ms. Crisp was also performing the role of
Instructing Operator and Induction Presenter.
679
As Supervisors, they were
responsible for the general running of the park and attending all reported park
problems, including ride operational issues, which were notified by the Security
Control room.
680
Ms. Crisp commenced employment with Dreamworld as a Ride
Operator in March 2011, and was employed as an Instructing Operator on a full-
time basis since April 2012.
681
Prior to 25 October 2016, she had trained
approximately 30 to 40 people in the varied roles at the TRRR, a majority of
which were at the Level 2 or 1 roles.
682
393. Mr. Wayne Cox was the E&T Supervisor rostered that day. Mr. Gordon and Mr.
Matthew Robertson were the nominated Park Technicians. At the pre-work
briefing that morning, Mr. Cox advised staff that if a ride had the same fault three
times, on the third occasion then it needed to be escalated to a supervisor to
investigate further.
683
394. Having considered the witness statements, documentation and evidence
provided during the inquest, the timeline of critical events leading up to the tragic
incident on 25 October 2016, are as follows.
8:00 am: An E&T Pre-Service Inspection on TRRR
395. At 8:00 am, Park Technician, Mr. Robertson, who was a Park Technician for the
day, and Mechanical Tradesperson, Mr. Kamlesh Prasad carried out the E&T
Pre-service Inspection on the TRRR.
684
The requisite checklist was completed,
670
Ex B3A(3), pg. 10
671
T2-96, lines 35-46; T2-98, lines 20-45
672
T2-96, lines 35-47
673
T2-97, lines 7-15
674
T2-97, lines 10-15
675
Ex C8(16), [7]
676
Ex B3A(4), [10]
677
Ex C8(16), [10]
678
Ex B3A(11), [3]; Ex B3A(14), pg. 14
679
Ex C6(46), [10]
680
Ex B3A(20), [14]
681
Ex C6(46), [15]
682
Ex C6(46), [31] & [32]
683
Ex B3C(9), [16]
684
Ex B3A(16), [14-20]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 98 of 274

which requires specific components of the ride to be inspected on a daily basis,
including components of the north and south pumps, gates, draining of the rafts
and raft tube inflation.
685
There were no issues with the checks conducted on
that morning, and the service sheet was initialled as required.
686
9:25 am: Courtney Williams commenced training
396. Having been advised that morning by the rostering coordinator that she was to
be trained on ‘Rapids Load’ at the TRRR, Ms. Williams attended the
administration block at 9:25 am, where she met Ms. Crisp, who was scheduled
to train her at the TRRR in the Number 2 Operator position.
687
Training was
commenced in transit to the ride. According to Ms. Williams, Ms. Crisp spoke to
her about the evacuation points and how to manoeuvre the rafts with her feet.
688
397. Upon arriving at the ride, Ms. Crisp showed Ms. Williams the first Emergency
Evacuation point for the TRRR, which is near the guest line up. A walk through
of the ride was conducted, where components were pointed out relevant to the
role.
689
Ms. Crisp highlighted the steel support beams around the ride, including
those at the unload station, and advised her that the rafts would rest on these if
the water drained out of the ride following a malfunction.
690
According to Ms.
Crisp, whilst near the conveyor, she spoke to Ms. Williams about Code 6
situations on the ride, comparing it to the responsibilities of the Deckhand at the
Log Ride, which would require her as the No. 2 Operator to attend the bottom of
the conveyor and speak to guests.
691
The operation of the jacks at the unload
area were also explained to Ms. Williams, as was the second emergency
evacuation point near the guest line up.
692
Ms. Williams stated during the inquest
that Ms. Crisp did not explain to her about the water level dropping and rafts
resting on the supporting rails, however, she was generally aware that the water
level needed to be monitored.
693
398. Ms. Crisp then took Ms. Williams to the main Operator panel, where certain
buttons were demonstrated, including the gate reset button (for a Code 6) and
emergency stop button above the panel.
694
The release of the rafts and the
holding gate were also explained and shown.
695
Ms. Crisp claimed in a response
provided to OIR that she advised Ms. Williams that she could not dispatch two
rafts together as the timer would prevent this from occurring. She claims that she
explained to Ms. Williams that if two rafts were sent together, they could bump
into one another resulting in a potential capsize.
696
Ms. Crisp also claims that she
discussed the amp readings for the pump with Ms. Williams, as well as the need
for her to stop operating if the reading was over 500, and have her No. 1 Operator
attend so the operational issue could be dealt with.
697
685
Ex B3A(15), [35]; Ex B3A(16), [14], [15], [17] & [39]
686
Ex B3A(15), [35]; Ex B3A(16), [18]
687
Ex B3A(4), [14]
688
Ex B3A(4), [16]; Ex B3A(14), pg. 14
689
Ex B3A(4), [17]-[19]
690
Ex B3A(4), [19]; Ex B3A(14), pg. 20
691
Ex B3A(14), pg. 20 & 21; Ex C6(46), [35]-[38]
692
Ex B3A(4), [19]-[21]
693
T2-72, lines 30-47 & T2-74, lines 30-45
694
Ex B3A(4), [24] & [25]; Ex C6(46), [84]-[90]
695
Ex B3A(4), [24]
696
Ex C6(46), [41]
697
Ex C6(46), [52]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 99 of 274

399. Although during her interview with the Police, Ms. Crisp seemed to acknowledge
that she did not show Ms. Williams the start-up and shut down of the ride,
698
in
her statement subsequently provided to OIR, she claimed that she ‘showed
Courtney how to shut down the conveyor as part of the emergency shut-down
procedures.’
699
She claims that she explained how to shut down the ride at the
Main Control Panel, and also how to shut down the conveyor at the unload
station.
700
Ms. Williams acknowledged during her interview with OIR and at the
inquest that she had been shown four buttons as part of circular motion to shut
down the ride on the main panel, which included two emergency stops.
701
However, Ms. Williams disagrees that she was shown the shutdown for the
conveyor as part of the emergency shutdown procedure to be followed at the
Main Control Panel.
702
She was simply shown the buttons to press during the
procedure, and was not aware mechanically what those buttons did.
703
400. Ms. Williams was also shown the unload area, where the respective yellow poles
with buttons, which open the gates in the area, were explained.
704
401. Ms. Williams’s induction training went for approximately 15-20 minutes, until the
No.1 Operator rostered that morning, Mr. Tim Williams arrived to open the ride.
705
Training records indicate that he had been trained as the No. 2 Operator for the
TRRR on 26 September 2014.
706
He was not trained in the No. 1 Operator role
until 5 October 2016 by Ms. Cotter.
707
9:50 am: Operator start-up checks conducted
402. Upon arrival, No. 1 Operator, Mr. Williams carried out the ‘Operator Pre Start-up
Checks’, noting that Engineering Staff had signed the checklist.
708
He stated that
during these checks, the amps for the South Pump fluctuated and at one point
exceeded 500 amps, however, a visual alarm on the panel did not activate, which
should occur.
709
He spoke to Ms. Crisp about the issue, and also sought advice
from Relief Supervisor, Ms. Cotter.
710
Whilst speaking to Ms. Cotter, Mr. Williams
noticed that the south pump amps dropped back down to 420, which was in line
with the north pump.
711
Ms. Cotter contacted Mr. Francois De Villiers, who
attended the TRRR and inspected the control panel. Mr. Williams was advised
to keep an eye on the fault and to call E&T Department staff if the fault reoccurred
or any further problems arose.
712
403. Ms. Williams stayed with Mr. Williams whilst he turned the ride on, however, was
also observing Ms. Crisp as she demonstrated how to run the queue line.
713
Ms.
Williams recalls that she returned to the unload area and watched as the pumps
began to operate. Ms. Crisp demonstrated how to stand at the unload area to
698
Ex B3A(14), pg. 44
699
Ex C6(46), [68]
700
Ex C6(46), [68]
701
T3-70 & 71, lines 1-15
702
T3-72, lines 1-10
703
T2-72, lines 20-30
704
Ex B3A(4), [27] & [28]
705
Ex B3A(4), [29]; Ex B3A(11), [14]
706
Ex C7(533)
707
Ex C7(530)
708
Ex B3A(11), [15] & [16]
709
Ex B3A(11), [28] & [29]; T4-46, lines 5-35
710
Ex B3A(11), [30]-[32]; Ex B3A(14), pg. 43
711
Ex B3A(11), [32]
712
Ex B3A(11), [35]
713
Ex B3A(4), [30]; Ex B3A(14), pg. 35
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 100 of 274

ensure the conveyor was being monitored, and which buttons on the poles
needed to be pressed at certain times.
714
Ms. Crisp demonstrated the first
practice run, allowing Ms. Williams to undertake the second.
715
Ms. Crisp had to
correct Ms. Williams to ensure her body was facing the conveyor and to prevent
her from straining whilst guiding the raft into position.
716
She states that she
impressed upon Ms. Williams the importance of not having her back to the
conveyor at the unload area.
717
Ms. Williams undertook approximately two to
three test runs before guests were traveling on the ride.
718
10:05 am: TRRR opens to the public
404. The ride was opened to the public by the operators. Mr. Williams was stationed
at the Main Control Panel loading guests onto the ride, with Ms. Williams (still
being trained by Ms. Crisp) at the unload area, and performing the role of
unloading guests.
719
Ms. Crisp performed the first few unloads of guests, whilst
Ms. Williams watched, before seeing whether she was comfortable to undertake
the next round.
720
Ms. Williams continued to perform the unloading of guests
under Ms. Crisp’s watch and guidance.
721
405. Ms. Crisp states that she advised Ms. Williams as to the water level, and referred
her to the markings on the wall. She stated, ‘As long as the rafts are bobbling
around you know that your water level is enough. As soon as they’re not moving
or as soon as you notice that level there drop that’s how you know your water
level is right’.
722
406. According to Ms. Williams, whilst she was at the Main Control Panel with Ms.
Crisp, the yellow case enclosing the E-Stop button at the unload area was
pointed out from a distance, which at the time had Mr. Williams drink bottle on
it.
723
According to Ms. Williams, Ms. Crisp stated that this was the E-Stop button
for the unload side, and words to the effect of ‘but don’t worry about it, no one
ever uses it’.
724
According to Ms. Crisp, she pointed out the E-Stop button, and
advised Ms. Williams that it would stop the conveyor and a pump.
725
She claims
that she also stated that ‘the only situation you’d use that in is, say you were
unloading and Tim fell in, he obviously can’t shut down the ride on himself, you
can hit that to start the process rolling.’
726
In her subsequent statement to OIR,
Ms. Crisp states that she told Ms. Williams that she could press the E-Stop if she
was at the unload area and there was an emergency and the ride needed to be
stopped to ‘get the shutdown started’, however, she needed to alert the No. 1
Operator.
727
She claims that she specifically mentioned the scenario of someone
standing on the conveyor or a raft slipping down in the context of explaining what
an emergency situation may be.
728
714
Ex B3A(4), [32]
715
Ex B3A(4), [33]
716
Ex B3A(4), [34]; Ex B3A(14), pg. 38
717
Ex B3A(14), pg. 38 & 41
718
Ex B3A(4), [37]
719
Ex B3A(11), [36]
720
Ex B3A(4), [38]-[41]
721
Ex B3A(4), [41]
722
Ex B3A(14), pg. 41
723
Ex C8(16), [77]; Ex B3A(14), pg. 47
724
Ex C8(16), [77]
725
Ex B3A(14), pg. 47
726
Ex B3A(14), pg. 47
727
Ex C6(46), [95] & [96]
728
Ex C6(46), [96]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 101 of 274

407. At inquest, Ms. Williams stated that Ms. Crisp did not tell her that the E-Stop
button at the unload area stopped the conveyor.
729
She claims that this would
have been important information for her to be told.
730
10:30 am: Operator positions swapped
408. Mr. Williams swapped positions with Ms. Williams (who was still accompanied by
Ms. Crisp), so that she could be trained at the Main Control Panel in the loading
area.
731
Ms. Williams describes Ms. Crisp as loading the first couple of sets of
guests onto rafts to allow her to observe.
732
In between guests boarding the rafts,
Ms. Crisp is said to have taken Ms. Williams to the control panel to demonstrate,
which buttons to press and not to press.
733
Ms. Williams subsequently performed
the loading of guests onto the rafts under Ms. Crisp’s guidance and instruction
as to each step to be undertaken.
734
11:15 am: Ms. Williams completed training
409. Ms. Williams was deemed to have completed her training as the No. 2 Operator
at the TRRR by Ms. Crisp, and both signed the requisite training documents.
735
Ms. Williams recalls that at this time, she read through documents in the folder
kept at the ride, including the Operator Procedure Manual and memorandums.
736
According to Ms. Crisp, she pointed out the memorandum relating to the E-
Stop.
737
This training was also considered to be a concurrent retraining of the
Deckhand role (No. 3) at the TRRR.
738
410. Ms. Crisp then left the TRRR with Ms. Williams’ manning the Main Control Panel.
The total time Ms. Williams was provided with training in the No.2 Operator role
at the TRRR was 1 ½ hours.
11:30 am: Operator change
411. At this time, Ms. Chloe Brix arrived at the TRRR to relieve Ms. Williams at the
Main Control Panel, whilst Mr. Williams remained at the unload platform.
739
Ms.
Brix was a Senior Ride Operator, who commenced working at Dreamworld in
December 2011.
740
She was first trained as the No. 2 Operator on the TRRR in
2013
741
, and in the No. 1 Operator position on 17 September 2015.
742
She recalls
that prior to attending the TRRR, she had spoken to Ms. Crisp, who advised her
that Ms. Williams had been trained in the No. 2 Operator position that morning,
and was performing well.
743
She requested that Ms. Brix check to see whether
Ms. Williams had any questions when she attended the ride.
744
729
T2-72, lines 7-25
730
T2-76, lines 35-40
731
Ex B3A(4), [42]; Ex B3A(11), [37]
732
Ex B3A(4), [42]
733
Ex B3A(4), [43]
734
Ex B3A(4), [44]
735
Ex B3A(4), [47] & [48]; Ex B3A(14), pg. 51
736
Ex B3A(5), pg. 8
737
Ex B3A(14), pg. 49
738
Ex C6(46), [81] & [82]
739
Ex B3A(11), [39]; Ex B3A(12), pg. 22
740
Ex B3A(12), pg. 5
741
Ex C7(542)
742
Ex C7(389)
743
T4-101, lines 5-30
744
T4-101, lines 10-30
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 102 of 274

11:50 am: 1
st
pump breakdown – South pump failed - Code 6
412. Whilst Ms. Brix was at the Main Control Panel performing the No. 2 Operator
position, she noticed that the water level had dropped. She called to Mr. Williams
at the unload area. At this time, a raft had just exited the conveyor and entered
the first jack area. Mr. Williams asked Ms. Brix to wait whilst he managed the raft
and passengers.
745
He then noticed that the raft did not move when he pressed
the first jack button as it was sitting on the rails, and soon realised that the south
pump was off.
746
After telling the patrons in the raft to stay seated, he attended
the Main Control Panel and commenced the shutdown procedure for the ride,
which included closing the emergency jack, turning off the conveyor and pressing
the emergency stop for one pump.
747
Mr. Williams then called Control to report
a Code 6.
748
Ms. Brix attended the bottom of the conveyor to tell the passengers
about the issue and to ask them to remain seated.
749
413. Mr. Mark Gordon and Mr. Robertson attended the ride to inspect the issue.
750
Mr. Robertson attempted to reset the south pump at the Main Control Panel,
however, this was not successful.
751
He subsequently contacted the Electrical
Department to request assistance.
752
Electrician, Mr. Frank De Villiers attended
the control room where the pump drives are located.
753
He noticed that the drive
for the South Pump had tripped and there was an alarm on it, which read ‘Alarm
14 Earth Fault’.
754
He contacted Mr. Robertson at the Main Control Panel to
advise him that he was going to try and reset the drive by pressing the reset
button on the keypad where the fault was displayed.
755
This did not work, so Mr.
De Villiers decided to turn the south drive off. After allowing the drive to power
down, he turned it back on, and this cleared the fault.
756
He then requested that
Mr. Robertson attempt to reset the pumps once again at the Main Control Panel,
which was successful.
414. Mr. Robertson requested that Mr. De Villiers show himself and Mr. Gordon how
to re-set the south pump, should the fault occur again, which he did by
demonstrating the main switch (large lever) in the control room, which powered
the pump motor.
757
During the inquest, Mr. Robertson claimed that he made such
a request as the Electrical team were ‘distracted that day’ by other electrical
issues within the Park that needed to be resolved.
758
Accordingly, the timeframe
taken to evacuate guests had been prolonged awaiting electrical assistance,
which had caused some upset. Mr. Robertson thought that if he could reset the
pump himself, this would speed up any subsequent attendances.
759
415. Ms. Cotter and Ms. Crisp also attended the ride and made sure that the required
switches at the Main Control Panel were turned off and the ride was locked
745
Ex B3A(11), [41]
746
Ex B3A(11), [42] & [43]; Ex C7(18)(a), pg. 32; T-4-48
747
Ex B3A(11), [40], [44] & [45]
748
Ex B3A(11), [46]
749
Ex B3A(11), [47]
750
Ex B3A(16), [24]; Ex B3C(9), [24] & [25]
751
Ex B3A(16), [24]
752
Ex B3A(16), [24]
753
Ex B3A(16), [24]; Ex B3C(35), [24] & [25]
754
Ex B3C(35), [25]
755
Ex B3C(35), [26]
756
Ex B3C(35), [27]
757
Ex B3A(16), [24]
758
T5-33, lines 3-30
759
T5-33, lines 3-30
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 103 of 274
out.
760
Whilst the Engineering and Electrical staff were attempting to rectify the
issue, a decision was made to evacuate the guests from the ride as some were
getting impatient with rafts stranded at various places around the watercourse.
761
416. Once the pumps were reset and the ride restarted successfully, Ms. Cotter
handed control of the ride back to Mr. Williams.
762
417. At a later time that day, Mr. Williams, whilst manning the Giant Drop, recalls
hearing Ms. Cotter speaking to the E&T staff, whereby it was stated that if there
was another failure of the pump, the ride would be closed for the day.
763
According to Ms. Cotter the issue with the south pump had been ‘happening
frequently over the last week’ following which the water level drops
‘dramatically’.
764
The consequence of this has been that the north pump ceases
to operate, which causes the ride to lose almost all of the water.
765
418. Mr. De Villiers subsequently had a conversation with Mr. Ritchie later that day
about the pump tripping, where he states that it was decided that the South Motor
would be megger(ed) on the following day before Dreamworld opened to the
public.
766
According to Mr. Ritchie, he spoke to Mr. De Villiers briefly about what
may have been causing the issue and formed the belief that it was an intermittent
fault in the drive and not with the motor.
767
He advised Mr. De Villiers that the
drive specialists were attending to inspect the issue on Thursday.
12:21 pm: TRRR reopened to the public
419. The TRRR was reopened to the public, with Ms. Williams returning from her
lunch break, relieving Mr. Williams. He did not return to the TRRR that day.
768
420. Ms. Williams recalls that Mr. Williams explained that there had been an increase
in the amps reading for the pumps whilst she was on lunch and the ride had to
be shut down.
769
1:09 pm: 2
nd
pump breakdown – South pump failed – Code 6
421. Whilst Ms. Williams was stationed at the Main Control Panel, Ms. Brix, who was
at the unload station, approached her and advised that the south pump light was
flashing, which means that one of the two pumps had faulted.
770
As the No. 1
Operator, Ms. Brix instructed Ms. Williams to stand at the end of the conveyor
whilst she undertook the shutdown procedure.
771
During her field interview, Ms.
Brix stated that Ms. Williams was not allowed to shut down the ride even though
she was stationed at the Main Control Panel at the time, as she remained the
No. 2 Operator for the ride.
772
Ms. Williams recalls that during the time the ride
shut down, the water level had dropped and completely drained out of the pool,
760
Ex B3A(20), [26]-[28]; Ex B3A(20), [32] & [33]
761
Ex B3A(11), [53]; Ex C7(18)(a), pg. 36; Ex B3A(20), [42]-[45]
762
Ex B3A(20), [46] & [47]; Ex B3A(16), [25]
763
Ex B3A(11), [58]; Ex C7(18)(a), pg. 45; T4-50
764
Ex B3A(20), [31]
765
Ex B3A(20), [31]
766
Ex B3C(35), [31]
767
Ex B3A(18), [25] & [26]
768
Ex B3A(11), [54] & [56]
769
Ex B3A(4), [50] & [51]
770
Ex B3A(4), [54]; Ex B3A(12), pg. 24 & 25
771
Ex B3A(4), [55]
772
Ex B3A(12), pg. 28
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 104 of 274
which left the rafts resting on the support railings.
773
422. Mr. Gordon and Mr. Robertson attended the TRRR once again.
774
Whilst Mr.
Robertson went to the Main Control Panel, Mr. Gordon attended the control room
and reset the pump drive for the south pump motor, as was demonstrated by Mr.
De Villiers.
775
Mr. Robertson subsequently successfully reset the south pump at
the control panel.
776
They assisted to return rafts to the dispatch area, before
evacuating guests.
423. Ms. Cotter also attended to ensure that the ride was operating correctly, before
handing back control of the ride to Ms. Brix.
777
Ms. Cotter recalls saying to Mr.
Robertson, ‘What are we doing about this pump problem. This is ridiculous’.
778
He is said to have advised her that ‘It’s our procedure that the alarm has to occur
three times before the ride is shut down. If another one happens we will close
the ride for the day. The ride is fine now to run.’
779
It does not appear that the
second fault of the south pump was escalated to an E&T Department
Supervisor.
780
1:25 pm: TRRR was reopened to the public
424. The ride was reopened to the public with Ms. Brix stationed at the Main Control
Panel and Ms. Williams at the unload station.
781
Shortly thereafter, Mr. Peter
Nemeth arrived at the TRRR to relieve Ms. Brix as the No. 1 Operator for the
afternoon. He was stationed at the Main Control Panel, with Ms. Williams
remaining at the unload area.
782
425. As Mr. Nemeth arrived at the TRRR, Ms. Cotter told him that there had been
water level issues earlier in the day, as the water pump had stopped on two
occasions.
783
He was aware that there were two pumps that serviced the ride,
which in the event one failed, the water level of the ride dropped dramatically.
784
In such circumstances, the ride needed to be shut down.
785
Ms. Cotter advised
Mr. Nemeth that if there was a further issue, the ride would have to be closed.
786
2:00 pm: Raft 6 loaded and released
426. Raft 6 carrying Mr. Stephen Anthorpe, Ms. Bree Dedini, Arlen Anthorpe (one year
of age), Chase Anthorpe (4 years of age), Ms. Michelle Farah and Dakota Marks
(4 years of age), was released onto the water course by Mr. Nemeth.
427. Ms. Williams states that at around this time, she had intended to swap positions
with Mr. Nemeth, who was still at the Main Control Panel.
787
She unsuccessfully
attempted to get his attention, as she did not see a raft coming down the
conveyor. When she turned around, she observed a raft coming down the
773
Ex B3A(4), [55]
774
Ex B3A(16), [28]
775
Ex B3A(16), [28]; Ex B3C(9), [35]
776
Ex B3A(16), [28]
777
Ex B3A(20), [52]-[68]
778
Ex B3A(20), [66]
779
Ex B3A(20), [67]; T5-35, 36, lines 1-25
780
Ex B3C(6), [16]
781
Ex B3A(4), [58]
782
Ex B3A(4), [6]
783
Ex B3A(1), [7]; Ex B3A(21), pg. 33 & 34; T2-58, lines 5-25
784
Ex B3A(1), [7]
785
Ex B3A(2), pg. 25
786
Ex B3A(1), [7]; T2-58, lines 20-25
787
Ex B3A(4), [61]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 105 of 274
conveyor, which she brought into the unloading area to allow the patrons to
disembark.
788
2:01 pm: Raft 5 loaded and released
428. Raft 5 carrying Ms. Goodchild, Ebony Turner, Mr. Dorsett, Ms. Low, Keiran Low
and Mr. Araghi was loaded and released into the watercourse by Mr. Nemeth.
429. Between 2:01:28 pm and 2:03:35 pm, Raft 6 can be seen on CCTV footage
provided by five cameras situated around the watercourse, traveling the ride
without incident. At this time, the raft is picked up by the conveyor. Similarly,
between 2:02:12 pm and 2:03:53 pm, Raft 5 can be seen traveling the
watercourse without incident.
2:03:50 pm: CCTV captures south pump stopping
430. Camera 14, which is positioned on a southern maintenance shed and provided
a view over the south pump inlet and the descending end of the conveyor,
captured the south pump ceasing to work, with water visibly flowing back into the
pump outlet.
2:03:53 pm: Raft 6 descends the conveyor belt
2:04:10 pm: Raft 6 becomes stranded on the support rails
431. Camera 14 of the CCTV footages captures Raft 6 descending the conveyor
before becoming stranded on the support rails near the unload station. Ms.
Williams claims that upon seeing this, she pressed the green button on the first
pole in the unload area to try and open the first gate, however, this did not
assist.
789
Knowing that she needed to notify the No. 1 Operator who was in
control of the ride, she claims that she turned towards the main control booth and
tried to get Mr. Nemeth’s attention, as she was aware that this was a Code 6
situation.
790
She states that at the time, he had his back to her and was loading
people into a raft. Ms. Williams turned back to the guests in the stranded raft and
advised them that there would be a short delay.
791
A photograph of the guests
being loaded into the raft where Mr. Nemeth was stationed was time stamped as
2:04 pm. It is evident from the photograph that the water level in the watercourse
is significantly reduced at this time.
792
432. According to Mr. Nemeth, as he was viewing the loading area where guests were
boarding the rafts, he noticed that the water level was going down dramatically,
and he could see the support railings, which were normally under water.
793
He
notes that ‘it only takes a few seconds for the water level to go down enough for
the rafts to sit on the rails’, following which the rafts cannot be moved.
794
At the
time, Mr. Nemeth recalls that one raft was ready to be released onto the
watercourse, with a further behind it that had been loaded with guests. At the
unload area, he noticed that there were two rafts waiting to be unloaded, one of
which had come off the conveyor and was sitting on the supporting railings, as
788
Ex B3A(4), [64]
789
Ex B3A(4), [65]; Ex C8 (16), [94]; T4-5, 6 & 7
790
Ex B3A(4), [65]; T4-5-7
791
Ex B3A(4), [65]
792
Ex B1, pg. 18
793
Ex B3A(1), [10]; Ex B3A(2), pg. 39; T2-59, lines 5-17
794
Ex B3A(1), [10]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 106 of 274
the water level had reduced.
795
433. According to Mr. Nemeth, he told the guests he had loaded into the raft that they
would need to disembark as the ride could not operate.
796
He assisted the guests
to exit the raft.
797
Mr. Nemeth acknowledges that this was a Code 6 situation,
and he would need to shut down the ride and notify his Supervisor and the
Control Room.
798
434. According to guests on the raft Mr. Nemeth was loading, it took around 40
seconds for all of the guests to be seated.
799
A photograph of the group was
taken, however, the raft did not move. One of the occupants recalls seeing Mr.
Nemeth turn to the control panel, which was about a metre away, for around 10
seconds, before advising them that they needed to disembark.
800
It was thought
that he may have been using a two-way radio at this time.
801
Mr. Nemeth is said
to have mentioned that the water level was too low, and an engineer would need
to come and reset the ride.
802
2:04:22 pm: Raft 5 is picked up by the conveyor
435. Camera 9 at this time captures Raft 5 being picked up by the conveyor. During
Mr. Nemeth’s field interview, he stated that at this time he had realised that Raft
6 was stranded on the support rails at the unload area, however, didn’t see
another raft on the conveyor.
803
He did, however, see that the conveyor was still
operating. Mr. Nemeth claims he commenced the procedure for a Code 6,
however, could not recall if he had called first or commenced the ride
shutdown.
804
2:04:50 pm: Raft 5 begins to descend the conveyor
436. Camera 14 captured Raft 5 as it began to descend the conveyor towards where
Raft 6 was stranded on the metal support railings. Mr. Nemeth stated that Raft 5
appeared on the conveyor all of a sudden and he could see that it was getting
close to Raft 6. He claims that he pressed the red conveyor stop button a few
times (maybe two or three times) in a panic, however, the conveyor did not
stop.
805
During his first field interview, Mr. Nemeth initially claims that when he
first saw Raft 5 it was just ‘over the top’ of the conveyor.
806
He then demonstrates
where the raft was at the time, and claims that it was ‘not far away from the end
of the conveyor’.
807
During the inquest, Mr. Nemeth clarified that there was
between 5 to 10 metres between the rafts when he first saw Raft 5 on the
conveyor.
808
795
Ex B3A(1), [10]
796
Ex B3A(3), pg. 23
797
Ex B3A(3), pg. 28
798
Ex B3A(3), pg. 24 & 25
799
Ex B3B(7), [11] & [12]
800
Ex B3B(7), [13]-[15]
801
Ex B3B(7), [15]
802
Ex B3B(9), [16] & [17]
803
Ex B3A(2), pg. 41 & 42
804
Ex B3A(2), pg. 41
805
Ex B3A(1), [11]; Ex B3A(2), pg. 42 & 43; T2-60, lines 14-20
806
Ex B3A(2), pg. 44; T2-6-, lines 1-15
807
Ex B3A(2), pg. 46
808
T2-60, lines 5-13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 107 of 274
437. According to Mr. Nemeth, the collision then occurred, which is when it ‘became
really serious’, and he used the phone to call 222, which is an emergency call.
809
He claims after he hung up the telephone, he then pushed an audible alarm,
which is intended to advise all of the departments in the Theme Park to attend a
ride urgently.
810
438. Ms. Williams claims that whilst she had her back to the conveyor attempting to
communicate with Mr. Nemeth about the situation, she saw that his ‘facial
expressions just completely dropped’.
811
She turned around and saw that a raft
was traveling down the conveyor, and would collide with the raft stranded on the
metal support rails.
812
She claims that she didn’t move from the unload area, as
she wasn’t sure if it was a Code 6 and Mr. Nemeth wanted her to attend the deck
at the bottom of the conveyor, as she had previously done during the Code 6
earlier that day.
813
In a later statement, Ms. Williams further states that she saw
Mr. Nemeth was looking over in her direction at the time, and she had assumed
that he was counting the rafts so that he could inform control when he called, as
is required of the No. 1 Operator.
814
Mr. Nemeth acknowledges in a field interview
with OIR that he made eye contact with Ms. Williams before he saw the raft was
approaching the other stranded on the railings.
815
To the best of his recollection,
he believes that he had tried to stop the conveyor before he made eye contact
with Ms. Williams.
816
During the inquest, Mr. Nemeth acknowledged that whilst
he was looking at Ms. Williams prior to the collision, he never directed or told her
to activate the E-Stop at the unload platform.
817
2:05:03 pm: Raft 5 first contact with Raft 6
439. Camera 14 captured Raft 5 as it first collides with Raft 6 at the end of the
conveyor near the unload platform.
2:05:06 pm: Raft 5 and Raft 6 pivot upwards
440. Camera 14 captures Raft 5 as it continues to be propelled forward by the moving
conveyor belt, causing both rafts to pivot upwards.
2:05:07 pm: Raft 5 aligned with the conveyor head and support rails
441. Raft 5 can be seen on the CCTV to continue into a vertical position with Raft 6
seen to fall back into a horizontal position resting on the rails. Raft 5 is then
shaken violently, as the conveyor belt continues to rotate.
442. Ms. Williams claims that during this time, Mr. Nemeth appeared to have an empty
expression, and he was just staring.
818
She ran to the conveyor to assist.
819
2:05:11 pm: Ms. Goodchild is seen to fall from the bottom left hand side of
Raft 5
809
Ex B3A(2), pg. 43
810
Ex B3A(2), pg. 43
811
Ex B3A(4), [68]
812
Ex B3A(4), [70]
813
Ex B3A(4), [70]; Ex C8(16), [89]
814
Ex C8(16), [86]
815
Ex B3A(3), pg. 29 & 30
816
Ex B3A(3), pg. 30 & 31
817
T3-56, lines 37-47 & T3-57, lines 1-26
818
Ex B3A(4), [73]
819
Ex B3A(4), [75] & [76]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 108 of 274

2:05:13 pm: Mr. Dorsett is seen to fall from the top of Raft 5
2:05:14 pm: The conveyor is seen on the CCTV to start to slow down speed
2:04:22 pm: The conveyor is seen on the CCTV to cease movement
2:05:27 pm: Ebony Turner is observed to climb out of Raft 5 onto a concrete
platform
2:05:35 pm: Kieran Low is observed to climb out of Raft 5 onto an employee
walkway
Immediate Response to the Tragic Incident
443. While the recollection provided by Mr. Nemeth is somewhat conflicting, it appears
that immediately following the collision of the rafts, he remained at the Main
Control Panel and rang ‘222’ speaking to Security Officer, Mr. Nigel Irwin. Mr.
Irwin was the sole staff member rostered to work in the control room that day.
His general responsibility was communications throughout the park by way of
three different hard wired radios and monitoring CCTV footage.
820
444. Mr. Nemeth advised Mr. Irwin that there was a ‘Code 222 Blue’ at the TRRR, and
that there was a raft on the conveyor.
821
Mr. Irwin initiated this call over the two-
way radio, however, upgraded the incident to a ‘Code 222 Grey’ once he had
viewed the CCTV footage, and noticed that a raft was in a vertical position.
822
This Code alerts all responding staff that there is machinery involved in the
medical emergency and ride shut down.
823
Mr. Irwin noted that the River Rapid
alarm had not sounded, which is meant to occur over every two way radio in the
Park when the pumps fail.
824
This is a manual alarm at the control panel at the
TRRR, which is activated by the Ride Operator.
825
445. Ms. Williams, along with occupants of Raft 6 and other patrons in the vicinity of
the incident, immediately helped to evacuate uninjured guests from the area. Ms.
Williams crossed the conveyor to assist Kieran, who was seated next to the
upturned raft, to usher him away from the scene.
826
Mr. Danny Haber, who was
queuing up for the ride, assisted Kieran to cross the conveyor belt so that he
could be removed from the area.
827
446. Mr. Steven Anthorpe, who was in Raft 6 with his family, secured his children and
immediately entered the watercourse via the conveyor to try and assist Ms.
Goodchild.
828
He saw that there was a female and male trapped in the raft.
829
Other patrons in the area provided him with assistance, including Mr. Haber. Mr.
Anthorpe immediately commenced CPR on Ms. Goodchild, and was joined soon
thereafter by Dreamworld First Aid Officers, including Mr. John Clark.
830
Attempts
were made to remove Ms. Goodchild from the watercourse using a nearby
820
Ex B3A(13), [14] & [15]
821
Ex B3A(13), [24]
822
Ex B3A(13), [29] & [30]
823
T12-61, lines 30-40
824
T12-62, lines 8-20
825
T12-62, lines 23-30
826
Ex B3A(4), [77] & [78]
827
Ex B3B(1), [xxi]
828
Ex B3A(9), [15]-[19]
829
Ex B3A(9), [19]
830
Ex B3C(34)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 109 of 274

garden hose, however, these were unsuccessful.
831
As the water receded, Ms.
Goodchild was dragged onto a hard flat surface, so that further resuscitation
efforts could be carried out.
832
By this time, she had ceased breathing. Chest
compressions were commenced, and Mr. Clark was provided with his first
response bag.
833
Further life saving measures, including mouth to mouth
resuscitation, were carried out prior to Queensland Ambulance Service (QAS)
arrival at the scene.
834
447. At 2:09 pm, other Dreamworld employees from all over the Park arrived on the
scene and attempted to assist with the evacuation area and also securing the
rafts to the conveyor.
448. A number of calls were made immediately to emergency services, the first being
at 2:10 pm by Mr. Irwin.
835
The QAS contacted QPS at 2:16 pm, who arrived on
the scene within six minutes. At 2:17 pm, a QAS call taker provided instructions
regarding the treatment of patients. It is clear from this phone conversation that
only two patients, Ms. Goodchild and Mr. Dorsett had been located at this time.
449. A short time after QAS arrived on the scene, Mr. Irwin was contacted by Mr.
Margetts via the two way radio.
836
He requested that Mr. Irwin switch to Channel
six, which is used solely by senior management. He asked questions as to how
many people were in the raft. Mr. Irwin viewed the CCTV footage and
subsequently advised Mr. Margetts that there were six people in the raft,
however, two children had appeared to have exited the raft safely.
837
450. The first responding QAS officers arrived at the scene at 2:22 pm. Following this
time, a further 9 QAS officers attended the scene to provide medical assistance
to all of the patients involved in the tragic incident. QAS officers conducted rapid
assessments of Ms. Low and Mr. Dorsett, who were trapped in the mechanism
of the conveyor. Life extinct was declared shortly thereafter for Ms. Low at 2:25
pm and Mr. Dorsett at 2:27 pm. Mr. Araghi, who was still receiving CPR at the
time, was also subject to a rapid discontinuation assessment, and subsequently
declared life extinct at 2:33 pm. During this time, Ms. Goodchild continued to
receive CPR, however, despite extensive resuscitation measures, she was
unable to be revived, and life extinct was declared at 2:45 pm.
451. The actions of patrons and some Dreamworld staff immediately following the
event, in what was extremely traumatic and difficult circumstances, was truly
remarkable and should be commended.
Further Evidence from Ms. Williams
452. During the course of the coronial investigation, Ms. Williams provided a number
of statements and participated in a walkthrough of the scene with OIR
investigators. In addition, Ms. Williams gave evidence during the proceedings
over the course of two days.
831
Ex B3C(34), [37]
832
Ex B3C(34), [38]; Ex B3B(1), [xxiii]
833
Ex B3C(34), [43]
834
Ex B3C(34), [44] & [45]
835
Ex B3A(13), [38]-[46]
836
Ex B3A(13), [53]
837
Ex B3A(13), [54]-[58]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 110 of 274
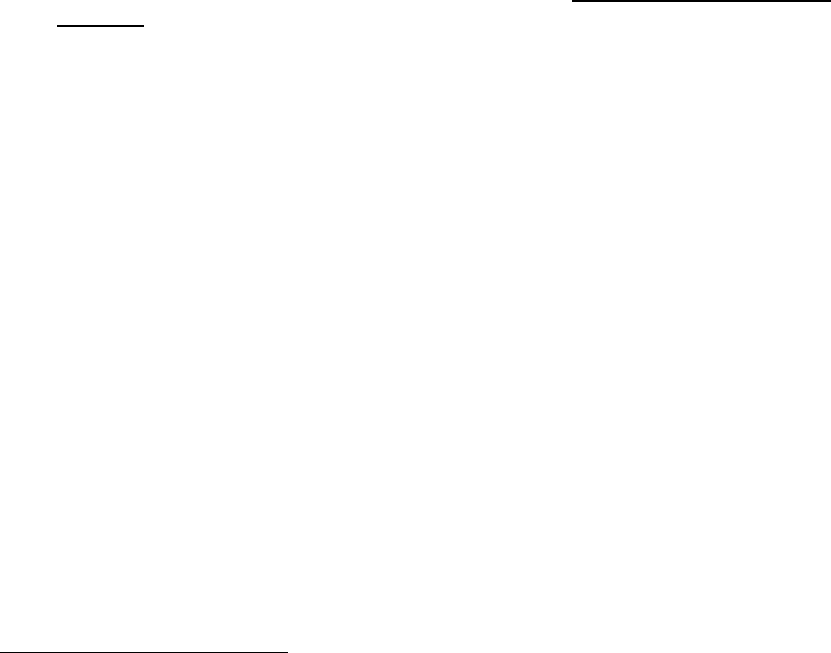
453. Ms. Williams claims that she was provided with training in respect of some
hazards related to the ride, which included monitoring patron’s movements in
rafts by way of the CCTV, and how to progress a raft with her foot whilst in the
load and unload bays.
838
She was also advised about the water pumps green
light on the control panel and the amp readings, as the ride would stop if either
pump failed.
839
Ms. Williams was also made aware of a drop in water in the event
that one of the pumps failed, however, thought the ride would stop
automatically.
840
She knew that there were no water level indicators on the ride,
and Operators were required to keep an eye on the water itself.
841
In terms of
considering the written components of the 18 page Operator Procedure Manual,
Ms. Williams stated during the inquest that whilst she was given the opportunity
to consider the content at the end of her training session, it was only ‘briefly’ and
she was required to digest and comprehend the sections herself.
842
454. As the No. 2 Operator for the TRRR, Ms. Williams was of the understanding that
it was No. 1 Operator’s responsibility to take control of any Code 6 issues on the
ride, and her role would be to attend the deck under the bridge immediately prior
to the conveyor belt.
843
Whilst she was shown some details as to the shutdown
controls, it was her understanding that if she was ‘comfortable and confident
doing so’, then she could undertake the four button shutdown.
844
Given she had
not been trained in the No. 1 Operator position, and had only received training
for the No. 2 Operator responsibilities that morning, she was understandably not
‘100 % comfortable with being the one to shut-down the ride’.
845
455. In support of Ms. Williams understanding as to the role of the No. 2 Operator in
a Code 6 situation, Ms. Crisp stated during her field interview that in relation to
shut down procedures and reasons this may occur, it was for the No. 1 Operator
to know, which is what she advised Ms. Williams.
846
Furthermore, Ms. Crisp
noted that whist showing Ms. Williams the Main Control Panel she ‘was a bit
overwhelmed’ as she knew she was going to have to start moving the rafts, so
they stayed at the unload area until she was comfortable.
847
In relation to the
Operator Procedure Manual for the No. 1 Operator, Ms. Williams stated during
the inquest that whilst she had skimmed this manual present at the ride, she
didn’t take much notice of it as she was being trained in the No. 2 Operator role
only.
848
456. It was Ms. Williams’ understanding that as the No. 1 Operator, Mr. Nemeth would
shut down the ride, and she would be required to attend the deck near the
conveyor.
849
457. In relation to the E-Stop button, Ms. Williams stated that ‘in the heat of the
moment’ she did not consider pressing the button, for the following reasons:
850
a. It was her first day in the No. 2 Operator role at the ride and there ‘was
838
Ex C8(16), [20] & [21]
839
Ex C8(16), [27]
840
Ex C8(16), [27] & [28]
841
Ex C8(16), [29]
842
T4-41, lines 5-38
843
Ex C8(16), [36]
844
Ex C8(16), [43]
845
Ex C8(16), [43]
846
Ex B3A(14), pg. 34
847
Ex B3A(14), pg. 36
848
T3-67, lines 40-48
849
Ex C8(16), [88]
850
Ex C8(16), [103]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 111 of 274

lots to be thinking about all at once’;
b. When the incident occurred, and the raft had tipped, she was focused on
the events that were unfolding in front of her;
c. It was her understanding that at all times the No. 1 Operator was in
control of the Main Control Panel. Had she been directed to press the E-
Stop she would have pressed it.
d. Given Ms. Crisp’s comments to her about the E-Stop, it seemed that the
button was less important than the controls at the Main Control Panel;
and
e. Whilst she had a general understanding that E-Stop buttons for different
theme-park rides stopped the ride, she was not aware that the E-Stop at
the TRRR stopped the conveyor, or another aspect of the ride.
458. Ms. Williams noted that she received no training as to what to do if a raft came
down the conveyor when a Code 6 occurred.
851
Further Evidence of Mr. Nemeth
459. Mr. Nemeth was aware that the No. 1 Operator for the TRRR was ‘responsible
for the ride’, which included a supervisory role over the No. 2 Operator.
852
He
received training in the No. 1 Operator position around a 1 ½ years before the
incident, by Ms. Crisp.
853
This training involved a full day operating the ride whilst
being simultaneously trained, as well as opening and closing the ride with the
trainer the following day.
854
He recalls that the Operating Procedure Manual was
used during the training, as he was taken through each step and then able to
read it in its entirety at the conclusion of the training session.
855
Whilst various
hazards, such as the pumps or conveyor stopping, were brought to his attention,
the prospects of rafts colliding were not canvassed.
856
460. At inquest, Mr. Nemeth noted that he had found it difficult to communicate with
the unload Operator whilst at the Main Control Panel, however, had never raised
this issue with the Supervisors.
857
461. In relation to the E-Stop at the unload area, Mr. Nemeth stated during his field
interview that he was aware that it could stop the conveyor, however, was of the
understanding following training that ‘it should only be used if the – if the
emergency stop is not accessible on the control panel’.
858
During a field
interview, Mr. Nemeth was asked about the various memorandums relating to
the TRRR, particularly that of the 18 October 2016 relating to the E-Stop. It was
his understanding that this memorandum was to inform staff as to the use of the
E-Stop, which was to be pressed in an emergency if that Main Control Panel
could not be accessed.
859
851
Ex C8(16), [111]
852
Ex B3A(2), pg. 5; Ex B3A(3), pg. 18
853
Ex B3A(3), pg. 6
854
Ex B3A(3), pg. 6
855
Ex B3A(3), pg. 7 & 8
856
Ex B3A(3), pg. 9
857
T2-92, lines 29-41
858
Ex B3A(2), pg. 8
859
Ex B3A(3), pg. 15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 112 of 274
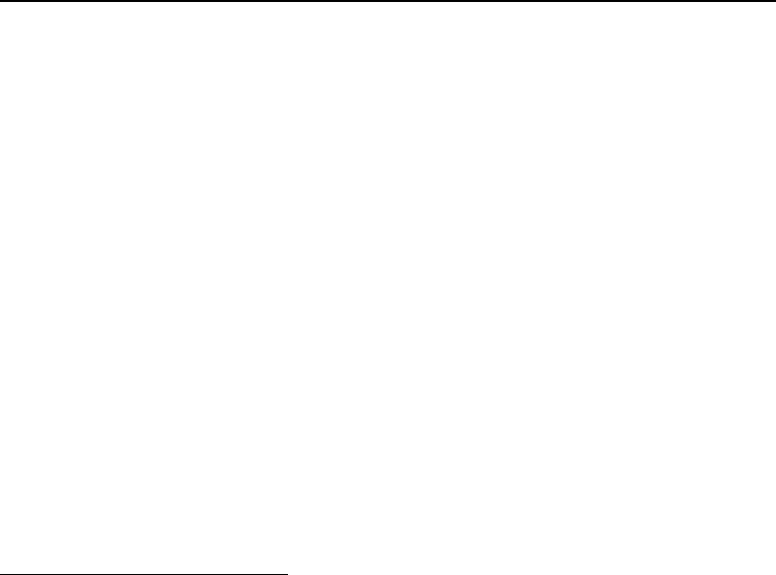
462. With respect to the water level, Mr. Nemeth noted that there were no official
markers around the trough of the ride, rather Operators used the discoloration
marker around the edge to gauge whether the water level had dropped, and may
be too low.
860
463. During training, various Code 6 scenarios were considered, including one or both
pumps stopping.
861
It was his understanding that a Code 6 applied to
circumstances when the ride was not fully operational and unsafe to operate.
862
464. In relation to the pump breaking down, Mr. Nemeth stated that he was aware that
there had been an issue with the south pump turning off, which had been
happening over a number of days.
863
This seemed to be common knowledge
amongst Ride Operators.
864
465. Mr. Nemeth was not aware of the Breakdown Procedure, which was applicable
to staff in the E&T Department as to ride closures.
865
466. Mr. Nemeth stated that he had pressed the conveyor stop button several times
on previous occasions whilst operating the ride, and had never had an issue with
it working before.
866
He stated during the inquest that he had previously been in
situations on the TRRR where the rafts had been resting on the rails due to a
drop in the water level, and on these occasions, he had turned to the Main
Control Panel, and carried out the shutdown procedure per the Operators
Procedure Manual.
867
Discussion with QPS, OIR & Dreamworld Management on 25 October 2016
467. Commencing at 5:27 pm on 25 October 2016, shortly following the tragic
incident, a number of recorded discussions took place on-site at Dreamworld
with the following participants:
• Senior Constable Paul Joyce – QPS, Forensic Crash Unit
• Mr. Michael Chan – OIR, Chief Safety Engineer
• Mr. Ian Stewart – OIR, Principal Inspector
• Mr. Craig Davidson – CEO, Dreamworld
• Mr. Chris Deaves – General Manager, Engineering, Dreamworld
• Mr. Clinton Ford – Pitt and Sherry Consulting Engineers, Consulting
Engineer
• Mr. Angus Hutchings – Safety Manager, Ardent Leisure
• Mr. Mark Thompson – Safety Manager, Dreamworld
• Mr. Troy Margetts – General Manager of Operations, Dreamworld
• Mr. Scott Ritchie – Engineering Supervisor, Dreamworld
• Mr. Damien Hegarty – Kaden Borros Legal, Representing Ardent Leisure
468. A general discussion was had as to what was known about the incident at the
time, the mechanism and operation of the ride, as well as further information that
needed to be provided by Dreamworld for the purpose of the OIR and QPS
860
Ex B3A(2), pg. 19
861
Ex B3A(2), pg. 20
862
Ex B3A(2), pg. 21
863
Ex B3A(2), pg. 36
864
Ex B3A(11), [73]
865
Ex B3A(2), pg. 38
866
Ex B3A(2), pg. 52 & 53
867
T2-59, lines 25-35
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 113 of 274

investigation into the circumstances of the tragedy.
469. Relevantly, during the conversation the following comments were made:
• Mr. Deaves noted that there was a ‘pinch point’ at the conveyor.
868
• Mr. Deaves confirmed that the focus of the improvements to the ride have
been at the start of the conveyor where there had been a bank up of rafts
prior to the conveyor.
869
He claimed that this was based on ‘historical
knowledge’.
870
• Mr. Ritchie advised investigators of the PLC switches at the beginning of
the conveyor, and explained that they had been installed to ‘stop the raft
tip’ if a pump stopped operating causing the water level to drop, it was
recognised that there was the potential to catch on the conveyor and get
tipped upwards.
871
• Mr. Deaves claimed that there was review of the ride and testing was
conducted. He recalls discussing the consequences of a pump failure,
and what the best course of action would be in response to this, such as
stopping the conveyor or the pumps. During these discussions, it seemed
to have been accepted that the top of the conveyor, where the incident
happened, was ‘ok’ as there was no historical knowledge of any
problems.
872
TECHNICAL CAUSE & CIRCUMSTANCES OF THE INCIDENT
470. Based upon the investigation, analysis and testing conducted on-site by Senior
Constable Cornish, as well as consideration of supplementary documentary and
physical exhibits, the technical timeline of the raft and conveyor movements
shortly before and during the tragic incident, are as follows:
873
I. At 2:03:50, the south pump can be seen to stop operating as water is
rapidly flowing back into the pump outlet.
874
II. Raft 6 is observed to exit the conveyor system at 2:04:05 initially moving
freely into the trough. At 2:04:10, it is then seen to become stranded on
the raft supporting rails at the interface area due to the sudden drop in
the water flow.
875
III. As the conveyor continues to operate, at 2:04:22, Raft 5 approached the
start of the conveyor before beginning to commence traveling the incline.
At this time, Raft 6 had been stationary at the interface at the end of the
conveyor for 12 seconds.
876
IV. Raft 5 can be seen approaching the downside of the conveyor at 2:04:50.
868
Ex B3G(38)(f), pg. 1
869
Ex B3G(38)(f), pg. 4
870
Ex B3G(38)(g), pg. 6
871
Ex B3G(38)(g), pg. 6
872
Ex B3G(38)(g), pg. 7
873
Ex B2, pg. 42-54
874
Ex B2, pg. 43
875
Ex B2, pg. 44
876
Ex B2, pg. 44
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 114 of 274

It is now apparent that Raft 6 is seated directly on top of the support rails
with insufficient water height in the area to allow the raft to flow
forward.
877
V. After Raft 6 has been stationary for 53 seconds, at 2:05:03, Raft 5
reaches the end of the conveyor and is released into the unloading zone.
Contact between the two rafts first occurs at 2:05:03.
878
VI. As the conveyor continues to operate, the rafts subsequently make
contact three times. On each occasion, both rafts appear to move slightly
forward, with Raft 5 bumping into Raft 6 causing it to move along the
support rails before it comes into contact with the cross beam of the
support rails. CCTV footage confirms that the conveyor is still in
operation at this time, as the planks can be seen to be moving
underneath Raft 5.
879
VII. Following the third impact between the two rafts, contact is then
maintained as they pivot upwards at the central contact point (2:05:06).
This is because the force of the conveyor, an amount of compression
between the contact point of each tube, the long plank and cross beam
create a hinge point. The rear of Raft 6 and front of Raft 5 have then
become slightly raised.
880
VIII. At 2:05:07, the rafts appear to become inverted at an approximately 90
degree angle. At this time, Raft 5 has become entrapped between the
moving conveyor and the fixed leading edge of the support rails.
881
IX. Raft 5 has continued to invert, whilst Raft 6 has dropped back into a level
position on the support rails. Raft 5 was inverted for 7 seconds before
the conveyor began to slow, before coming to a complete stop a further
8 seconds later. During this time, 22 planks (eight long and 14 sets of
short planks) have passed through the area, which is in contact with
tubing and fibreglass construction of the raft.
882
X. As Raft 5 became fully inverted, the conveyor continued to operate,
causing the raft to shake violently, as each pass of the planks, long or
short, damaged the raft ripping pieces of fibreglass from the tub
construction. During this time, Raft 5 was pulled down within the interface
void between the conveyor and supporting rails. At 2:05:11, Ms.
Goodchild can be seen to be shaken from the raft. At 2:05:13, Mr. Dorsett
also falls from the raft and into the moving conveyor drive axle and cog
area. The conveyor can be seen to begin to slow at 2:05:14, coming to
a final stop at 2:05:22.
883
XI. The force and position of the raft has ‘pulled’ Raft 5 down between the
conveyor and the support rails to a distance of approximately 45
centimetres. It was during this time that one of the air chambers of Raft
5 has become torn and deflated. The final resting position of Raft 5 is
877
Ibid.
878
Ibid.
879
Ex B2, pg. 45
880
Ex B2, pg. 46
881
Ex B2, pg. 47
882
Ex B2, pg. 47 & 48
883
Ex B2, pg. 53
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 115 of 274
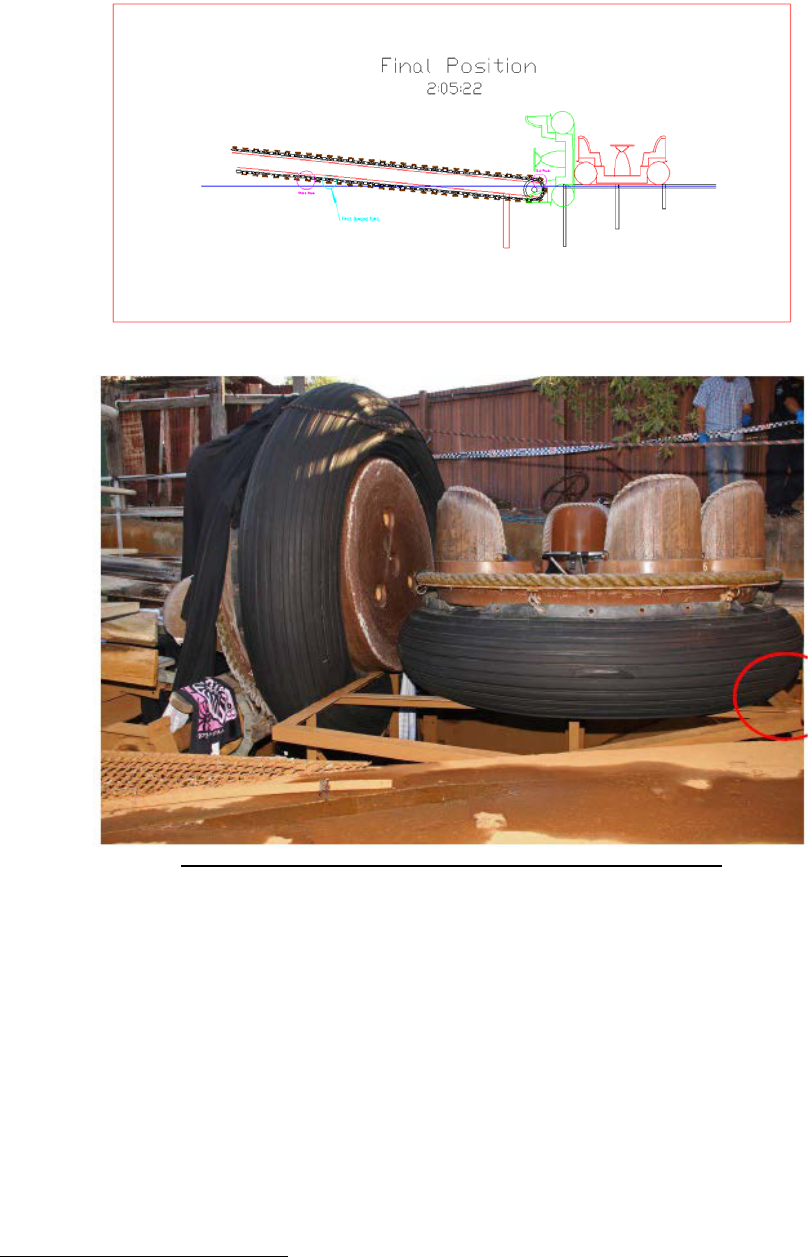
depicted below.
884
FINAL RESTING POSITION OF RAFT 5 & RAFT 6 - Ex B2, pg. 51
471. It is evident that it only took one minute and 17 seconds from the time the south
pump failed until Raft 5 became inverted.
885
472. Investigators have established that within the first 15 seconds of a pump failure
on the TRRR, approximately (200mm) of water height was drained.
886
As Raft 6
entered the unload area, there was insufficient water flow for it to proceed
forward over the support rails once it exited the conveyor. This occurred within
20 seconds of the pump failure.
887
473. Further testing conducted by Investigators following the incident confirmed that
when one pump was not operational there was a difference in water level of
884
Ex B2, pg. 50
885
Ex B2, pg. 54
886
Ex B2, pg. 77
887
Ex B2, pg. 53
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 116 of 274
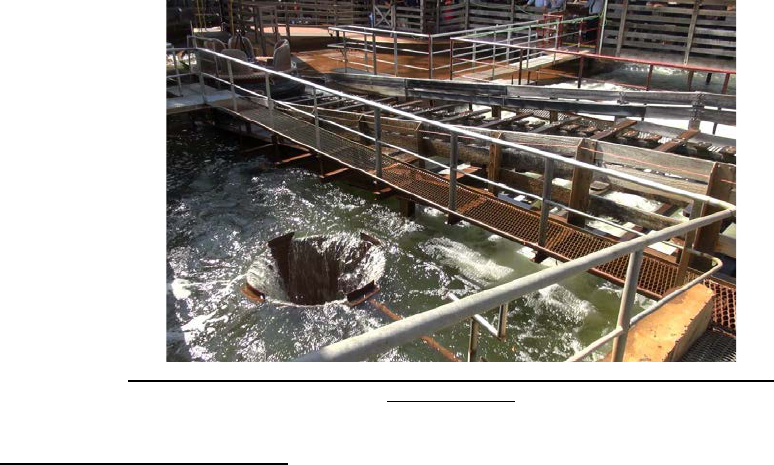
approximately (400mm), which occurred over approximately one minute.
888
When only one pump was in operation, it was found that there was insufficient
water flow over the support rails in the unload area to allow rafts to pass over
them. Within a minute, the rails can be seen to be exposed above the water.
474. Raft 6 was stationary for 53 seconds prior to coming into contact with Raft 5.
889
It took four seconds for Raft 5 to become inverted, and to commence to shake
violently whilst the conveyor continued to operate at its normal speed.
475. Given the violent nature of Raft 5 being pulled into the mechanism, Ms.
Goodchild and Mr. Dorsett were released from their Velcro strap seatbelts and
tragically fell between the moving conveyor planks, drive axle and cog
mechanism. Ms. Low and Mr. Araghi, who were positioned at the rear of the raft,
were subsequently caught within the moving mechanism of the conveyor belt
during the period of inversion, and were pulled into the plank and cog mechanism
as it continued to operate.
890
476. Raft 5 sustained significant damage to three of the six seats at the back of the
raft where Ms. Goodchild, Mr. Araghi and Ms. Low were seated. There was no
contact damage sustained to Raft 6.
891
477. Testing of the E-Stops at the TRRR by investigators following the tragic incident,
in the presence of Dreamworld staff, confirmed that none of the E-stop’s had
been activated at any time during the course of the incident.
892
CCTV footage of
the incident also confirms this finding.
478. Testing also revealed that the opening of the pump outlets within the pit area
under the conveyor were at a level lower than that of the raft support rails.
893
Due
to this design aspect of the ride, and the large volume of water that is extracted
during the reverse flow, the water drops below the level of the rails quickly.
894
DEPICTS NORTH PUMP OPERATING WITH BACKFLOW & EXPOSED RAILS
- Ex. B2, pg. 87
888
Ex B2, pg. 76
889
Ex B2, pg. 53
890
Ex B2, pg. 51
891
Ex B2, pg. 66
892
Ex B2, pg. 38
893
Ex B2, pg. 86
894
Ex B2, pg. 86
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 117 of 274

Plank Damage and Observations
479. Investigators determined that during the course of the incident, eight large planks
and 15 pairs of small planks were damaged.
895
The type of damage observed
ranged from small chips of timber being removed to small planks being split into
two.
480. During examination of the planks on the conveyor, Senior Constable Cornish
noted that there were some large planks that had a degree of concave and
convex bowing along the centre.
896
Video review of the CCTV footage suggests
that the two ‘pivot’ planks passing under Raft 5 have a degree of convex
bowing.
897
Testing was attempted to replicate whether these planks could cause
an inversion, however, this was unsuccessful.
898
Reconstruction of the Incident
481. A series of tests were conducted by Investigators with loaded and unloaded rafts
in an attempt to reconstruct and replicate the incident. Whilst different set ups
were utilised during the testing, with the rafts positioned and held by different
methods, one test involved the holding of a raft in place in an attempt to replicate
the positioning of Raft 6 whilst in a stationary position. The failure of the south
pump was then emulated prior to the collision with a secondary raft. Whilst the
raft inversion was not able to be replicated, the testing did reveal the following:
• Variations in the behaviour of the planks with the centre convex aspect
were highlighted. Planks that bowed outwards were found to make
considerably more contact with the floatation collar of the raft, gripping
into wear strips and compressing the collar.
899
During the inquest, Senior
Constable Cornish noted that whilst the bowing of the planks could be a
variable in the incident, he was unable to say with any certainty whether
they played a part.
900
• The presence of the cross beam at the support rails near the unload area
was found to restrict forward motion of the raft during the course of one
test, and when this occurred, there was a ‘severe’ grab by a long plank
at the rear of the raft on the wear strip of the collar.
901
• The resistive nature between the rafts floatation collars and the exposed
support rail was evident during testing.
902
482. No inversion or pivoting of the rafts occurred during testing. Investigators opined
that this may have been as a result of alterations in the positioning of the rafts
during testing as opposed to the actual incident.
903
Nonetheless, during testing,
the resistive nature between the rafts floatation collar and the exposed support
rails was evident, as was the prospect of a large movement of the second raft by
the first, which would force it along the support rails to the area of the cross
895
Ex B2, pg. 62
896
Ex B2, pg. 62
897
Ex B2, pg. 62
898
Ex B2, pg. 62
899
Ex B2, pg. 89
900
T2-39, lines 10-30
901
Ex B2, pg. 89
902
Ex B2, pg. 90
903
Ex B2, pg. 91
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 118 of 274

beam.
904
483. It was observed during testing that whilst the conveyor continued to move,
combined with the convex planks and 0.78 m gap between the long planks, this
created an open area for the floatation collar to slightly drop within, which makes
it easier for the plank to make substantial contact with the wear strips.
905
484. At inquest, Senior Constable Cornish stated that at the time of the reconstruction
he did not have unrestricted access to a copy of the CCTV for the purpose of the
positioning of the rafts.
906
FCU Investigation Findings as to Causation
485. Having considered the Operator controls, design and mechanical function of the
components of the ride, as well as the Operator procedures and safety features,
Senior Constable Cornish reached the following conclusions as to the causes
and circumstances of the incident:
907
I. The primary cause of the event was due to the failing of the south pump,
which in turn led to a sudden drop in water level. It was proven during
testing that a raft was unable to complete the circuit when only one pump
was in operation. Water level monitoring for the ride was undertaken
through visual observations by the Operator, using existing structures of
discoloration of the trough walls. There was no automated safety system
to monitor the water level and provide any audible or visual alert should
the level fall below a safe operating level.
908
II. Monitoring the operation of the pumps was also through operator
observation by way of the ride water level, a small digital ampere reading
and the sighting of pump activation lights on the control panel. This
monitoring is in addition to the other responsibilities of the Operators,
which include the safe loading of patrons into rafts. Given the normal
sounds of the environment when the ride was in operation, it was noted
that there was no discernible change in environmental noise when one
pump failed, and only one remained in operation.
909
There was no
audible alarm or visual warning associated with the failure of either one
of the pumps, combined with a full ride shutdown.
III. The two major components of the ride were the water pumps and
conveyor, which were controlled independently of each other.
Accordingly, when one of these components failed or malfunctioned, the
other continued to operate. This was a factor during the incident, as the
CCTV confirms that when the south pump broke down, the conveyor
continued to operate at full speed, collecting Raft 5 and transporting it
towards the unload area where the incident transpired.
910
There is no
automated electronic system recognizing the failure of one component
which automatically ceases the operation of the other system.
911
904
Ex B2, pg. 90
905
Ex B2, pg. 92
906
T2-23, lines 2-5
907
Ex B2, pg. 9-7
908
Ex B2, pg. 97; T1-86, lines 10-30
909
Ex B2, pg. 97
910
Ex B2, pg. 97 & 98
911
Ex B2, pg. 98
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 119 of 274

IV. Raft 5 became entrapped within the gap of the conveyor and the raft
support rails.
912
The intent of the raft support rails was to prevent the raft
from dropping to the bottom of the trough and to reduce excessive
heeling should the raft become unstable. Senior Constable Cornish
noted that it could not be determined if the closure of the gap would have
prevented or increased any loss of life, given there was no automated
shutdown systems in place. Consideration should have been given to
the potential risk of the gap exposure and prevention of injury.
913
V. The height of the pump outlets was below that of the support rails. As
such, during a pump stoppage and subsequent reverse backflow, the
water level rapidly reduced below the rails given water will find its lowest
point with the least amount of resistance.
914
Whilst the north pump was
still operating leading up to the incident, it was visually noticeable that
the majority of this water predominantly flowed back into the south inlet.
Senior Constable Cornish noted that had the height of the inlets been
above the support rails this may have slowed the water extraction and
ensured that sufficient water and/or current was available for a greater
amount of movement of Raft 6 upon its exit of the conveyor.
915
VI. Within the unload area there was an Emergency Stop button easily
accessible by the unload Operator, or a member of the public. It was
established that this button was not utilised during the incident.
916
VII. The visual inspection of the Main Control Panel area revealed that there
was an obscured view of the conveyor, particularly the area where the
tragic incident occurred.
917
Further, the CCTV monitors positioned at the
Main Operator control panel did not have any available view of the
unload area or end of the conveyor. Senior Constable Cornish noted
that, in his opinion, had the view of the conveyor/support rail interface
area been unobstructed and the CCTV positioned in a more easily visible
position with more views available, the identification of the incident may
have been prompter.
918
VIII. ‘Raft Safety Stops’ were installed at the beginning of the conveyor, which
detected a stationary raft and shutdown the conveyor. Had the same
sensor mechanism be in place at the end of the conveyor, it would have
acted as a secondary stoppage device, in conjunction with the
automated pump and conveyor shutdown as was also recently proposed
to be installed.
919
IX. Examination of the main operating panel revealed that there was no
Emergency Stop for the conveyor, only a standard stop button, which
took 8-9 seconds to stop the operation. The implementation of an
Emergency Stop for the conveyor, or a full ride Emergency Stop, which
would have reduced the shutdown protocols.
920
912
Ex B2, pg. 98
913
Ex B2, pg. 98
914
Ex B2, pg. 98
915
Ex B2, pg. 98
916
Ex B2, pg. 98
917
Ex B2, pg. 99
918
Ex B2, pg. 99
919
Ex B2, pg. 99
920
Ex B2, pg. 99
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 120 of 274

X. Throughout the testing procedures and review of the CCTV footage, it
became evident that once the first raft became stationary atop the
support rails there was no other mechanism, other than water current, to
enable it to flow/move through to the unload area.
921
XI. The occupants were restrained in the raft by a large Velcro strap. There
is no variation in the strap depending on the patron’s age, gender or size,
nor is there any vertical adjustment of the belts.
922
The locking
mechanism was through the adhesiveness of the Velcro itself, with no
secondary system. Had an alternate system, inclusive of a three or five
point harness or a ride bar, as a secondary locking system to supplement
the Velcro, this may have reduced the injuries to those killed, particularly
Mr. Dorsett.
923
XII. Senior Constable Cornish expressed the view that the Operators had a
substantial amount of tasks and functions to perform, in a short
timeframe, whilst also conducting continued operational requirements.
He opines that the lack of automated safety systems, audible alarms,
CCTV range and situational awareness training were contributing factors
in this incident.
924
486. In summary, Senior Constable Cornish found that:
…it was not one single event that caused the fatal incident
that occurred on Tuesday the 25
th
of October 2016, but a
series of preventable safety features, operating procedures
and engineering design faults all occurring together within a
short period of time…
In my opinion based on the information I have been
supplied, the introduction of a simple water level alarm or
other warning device(s), automated shutdown facilities or a
change in operation procedures would have completely
prevented this incident from occurring. Notwithstanding
these modifications could have been introduced with
independent evaluation and consultation from similar
facilities worldwide. Acknowledging that the ride has been
functioning for approximately 30 years, it must be known that
advances in safety requirements and technology should be
an integral part of any amusement ride and their
maintenance and renovation programs.
925
487. During the inquest, Senior Constable Cornish described the TRRR as ‘severely’
lacking in any type of automation, which is readily available.
926
He described the
event as ‘twofold’ having occurred due to the design of the interface between the
conveyor and support railings, as well as the lack of safety mechanism for the
electrical system.
927
921
Ex B2, pg. 99
922
Ex B2, pg. 100
923
Ex B2, pg. 100
924
Ex B2, pg. 100
925
Ex B, lines 2, pg. 101
926
T1-86, lines 26 & 27
927
T1-86, lines 15-21
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 121 of 274

EARTH FAULT AND PUMP DRIVES EXAMINATION
488. Between 25 October and 2 November 2016, several electrical tests were
conducted on the Danfoss Variable Speed Drives (VSD’s) following the tragic
incident in order to establish a probable cause of the noted Code 14 ‘Earth Fault’.
History of VSDs at Dreamworld
489. A VSD is an electronic device, which is connected to electrical mains power and,
depending upon the control system used, regulates the electric motor speed via
electrical power cables from the output terminals of the drive.
928
The VSD works
as follows:
929
The electric motor converts electrical energy provided by the
drive into mechanical energy in the shaft of the electric
motor, which is mechanically connected to the water pump
and therefore turns the water pump, which then draws water
from the inlet pipe through the pump with the outlet of the
pump into the watercourse of the ride.
The water flow and subsequent height of the water in the
watercourse depends on the pump’s output flow, which is
governed by the motor speed. The motor speed is
determined by the power (voltage and frequency) output of
the drive which is set by an operator or a control system.
…
The VFDs adjust the speed of electric motors by varying the
output (frequency and voltage) of the electrical supply to the
electric motor.
490. The design operating life of the VSD’s was 10 years, with the estimated average
operating time per unit being 6,000 hours/year.
930
According to Danfoss, under
normal operating conditions and load profiles, the VSD’s are maintenance free
throughout its designed lifetime, other than cleaning of fan filters etc.
931
491. Prior to the tragic incident, Danfoss had been contacted in February 2012 by
Dreamworld regarding the number of faults and repairs required of the two VSD’s
since installation. Faulty parts were sent back to the factory for further analysis
and the complaint was answered by Danfoss.
932
A service history for the North
and South Pump drives show that service jobs were performed in 2008, 2009
and 2012.
933
In 2015, Danfoss Drives Help Desk were contacted by Dreamworld
in relation to Earth Fault trips, which had been experienced on the South Drive.
934
Assistance was provided to the technician onsite as to an assessment of the
drive and it was suggested that an external wiring problem be explored, motor
low insulation resistance and for a new control card and ribbon cables to be
replace and tested to see whether the Earth Faults continued. Danfoss’ records
928
Ex G2, [18]
929
Ex G2, [19] – [22]
930
Ex G2, [43]
931
Ex G2, [44]
932
Ex G2, [41]
933
Ex G2, [56]
934
Ex G2, [71]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 122 of 274

suggest that AES swapped control cards with the North Drive when diagnosing
the Earth Faults of the South Drive.
935
492. According to Danfoss’ records, Dreamworld had been advised that spares for the
current drives were becoming limited and therefore, given the drives’ age and
operating hours, they should start to budget for replacement drives if they
required ‘reliable operation’.
936
In 2015, Danfoss sales partner, Electronic Power
Solutions, requested a quotation for replacement drives, which was provided to
Dreamworld.
937
Testing on drives post incident
493. On 25 October 2016, Mr. Takac, an Electrical Services Technician with Applied
Electro Systems Pty Ltd, attended Dreamworld to retrieve the ‘fault logs’ from the
Danfoss VSDs.
938
From 2009 until June 2017, Applied Electro Systems Pty Ltd
were contracted with Danfoss as an authorised service partner.
939
Records
confirm that Applied Electro attended Dreamworld on a number of occasions
during this time to carry out annual maintenance of the VSD’s and when
requested to service the drives, including on the following dates:
940
• June 2012 – Onsite commissioning of the VLT;
941
and
• August 2013 – commission drive with new motor.
942
494. In 2015, Mr. Takac made a call to Danfoss Drives Help Desk to seek guidance
as to ‘earth fault trips experienced on the south drive’.
943
A help desk engineer
provided assistance with the assessment of the drive. It was suggested that
checks be undertaken to determine whether external wiring problems, motor low
insulation resistance and to replace/test a new control card and ribbon cables be
undertaken, to see if the Earth Faults trips continued.
944
New control cards were
purchased and exchanged in the drives.
945
495. In June 2016, Mr. Takac, on behalf of Applied Electro, attended Dreamworld to
conduct maintenance of the VSD’s at the TRRR. However, he was unable to do
so as the south pump had broken down and was not in operation.
946
During the
inquest, Mr. Takac confirmed that the requisite checks that needed to be carried
out on the VSD’s, including input and output voltage and currents, could not be
performed when one of the pumps was not in operation.
947
935
Ex G2, [71]
936
Ex G2, [46]
937
Ex G2, [47]
938
Ex B3A(22)
939
Ex G2, [49]
940
T16-73
941
Ex G2(19)
942
Ex G2(22)
943
Ex G2, [71]
944
Ibid.
945
T16-76, lines 15-45
946
T16-74, lines 17-45
947
T16-74, lines 25-45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 123 of 274

496. The logs taken following the tragic incident revealed that the ‘South VSD’
recorded eight trips, the first two of which were ‘heat seek temperature too high’
faults and the remaining six were ‘Earth Faults’.
948
Mr. Takac was of the view
that three faults appeared to have been recorded within a short time period.
949
He expressed the view that the various faults could have been caused by a
number of reasons both internal and external to the VSD.
950
497. According to the Danfoss Manual for the VSD, in relation to an Earth Fault it
states, ‘There is a discharge from the output phases to ground, either in the cable
between the frequency converter and the motor or in the motor itself. Turn off the
frequency converter and remove the earth fault’.
951
498. The first series of testing was carried out by Mr. Christopher Sandry, Senior
Electrical Safety Inspector, OIR, who attended the scene on the day of the
incident and on a number of occasions following. He was present for a number
of walkthroughs and information downloads from the drives during the course of
the days he attended site.
952
499. Relevantly, on 28 October 2016, Mr. Sandry was requested by OIR to perform
an insulation resistance test on the South pump motor. He determined that both
the North and South pump motors needed to be tested in order to compare
results.
953
He isolated the supply to the South and North pump motor drives by
turning off the pump circuit breakers in the switch-room, which was confirmed in
accordance with ESO procedure. He then disconnected each pump motor supply
cable from their respective drive units. The insulation resistance test between
each pump motor cable and earth revealed a reading of OL, which indicates that
the resistance value is higher than the instrument can register.
954
The minimum
value of insulation resistance to be deemed compliant by AS/NZS 3000:2007,
the wiring rules, is 1 mega ohm.
955
As such, the pump motors were deemed to
have passed.
956
On completion of the testing, Mr. Sandry reconnected all pump
motor cables to their respective drive units.
500. Based upon the insulation resistance testing conducted, Mr. Sandy formed the
view that the cause of the South Pump failure was the result of an intermittent
fault in the pump drive unit.
957
501. On 2 November 2016, representatives from Danfoss Pacific, including Mr. Mike
Smits, Danfoss Pacific Director and Mr. Eduardo Gie, the Technical and
Engineering Manager of Danfoss Drives, Danfoss (Australia) attended
Dreamworld to examine the Danfoss VLT AQUA VLT 8502 Drives in use on the
TRRR, which ran the North and South water pumps at the TRRR.
958
These drives
had been in use at the ride since 2005. This was at the request of OIR for the
purpose of visually inspecting the mechanical and electrical installation of the
Danfoss drives, and to perform static and dynamic test procedures in line with
948
Ex B3A(22), [34]
949
Ex B3A(22), [36]
950
Ex B3A(22), [37]
951
Ex B3A(22), [35]
952
Ex B4(6)
953
Ex B4 (6), [38]
954
Ex B4 (6), [42] & [43]
955
Ex B4 (6), [43]
956
Ex B4 (6), [52]
957
Ex B4 (6), [52]
958
Ex B15(15), pg. 2; pg. 4; Ex G2, [73]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 124 of 274
the applicable service manuals.
959
Unfortunately, as the water pumps could not
be run due to the water being drained, the dynamic testing could not be carried
out.
502. Given the age of the two drives (approximately 10-11 years old) it was
challenging to extract data from the units.
960
503. The data that was obtained from the drive disclosed no recent Fault Trips on the
North Drive, however, the South Drive recorded six recent Earth Faults, Trip
Locked (Error Code 14).
961
The last three of these six fault alarms occurred within
two hours.
962
An Earth Fault (Error Code 14) is described as follows,
‘…a discharge from the output phases to earth, either in the
cable between the frequency converter and the motor or in the
motor itself. The drive relies on three current transducers to
measure the output currents drawn by the motor, and when
the addition of the three output currents are above 48% of
nominal current of the VLT 8502 (658A) for 10 µsec it results
on a Trip Locked Fault. A Trip Locked Fault is only cleared by
cycling the main power supply and then a Local Reset to the
frequency converter. As per drive’s settings the reset function
(Par. 400) was set to infinite and the auto restart time (par.
401) to 10 sec. Meaning that drive, during a Trip Locked
condition, would have been ready to start the motor 10
seconds after cycling the mains supply, without the need to
apply local reset.’
963
504. In a statement provided by Mr. Gie for the purpose of the coronial investigation,
he noted that an Earth Fault is usually caused by conditions external to the drive
and nothing was observed during the site visit, which would indicate that the
faults were caused by an internal drive component.
964
The static test procedures
conducted by Danfoss show that the main drives’ components were within the
range at time of measurement, except the fans mounted on the enclosure door.
As such, the root cause of the earth faults leading up to the tragic incident could
not be determined.
965
505. Ultimately, a cause as to the Earth Fault could not be determined.
Recommended Course of Action in Response to an Earth Fault
506. According to Danfoss, their recommended course of action to ascertain the root
cause of an Earth (Ground) Fault Alarm #14 is as follows:
966
(a) Disconnect the mains supply to the VLT 8000;
(b) Remove the motor cables from the drive end;
959
Ex B15(15), pg. 4
960
Ex B15(15), pg. 2
961
Ex B15(15), pg. 2
962
Ex B15(15), pg. 8
963
Ex B15(15), pg. 8
964
Ex G2, [78]-[82]
965
Ex G2, [78]-[81]
966
Ex G2, [103]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 125 of 274
(c) Measure the insulation resistance of the motor winding and earth,
including the motor cables, with a test voltage > 500 V;
a. A low resistance measurement would mean a faulty motor,
damage cable insulation, or presence of moisture in the
motor cable and/or motor windings.
b. A high resistance value, in other words reading open, will
require further investigation.
(d) Power up the drive without the motor cable connected, start the
drive and read the motor current from the display. Any offset current
reading .2A on the VLT’s display without motor connected suggests
the need for the re-calibration of the current sensor offset by doing
an Automatic Motor Adaptation (AMA) procedure, select ‘RUN
LIMITED AMA’ option in para 1-07.
(e) If the Alarm 14 keeps re-occurring after doing the AMA procedure,
now with motor connected to the drive, there is either a large offset
in the current sensors outputs, problem with the control card,
problem with the +/-15 volts power supply on the power card that
supplies the sensor circuit, a bad connection between the control
card and sensors, etc. In this scenario a service call should be
arranged to identify the faulty component within the drive.
507. It was noted that sometimes intermittent earth fault alarms, which occur more
often over time, can be attributed to slow motor insulation resistance
degradation.
967
508. During the inquest, Mr. Takac was asked what his advice would be if he had
been informed that there had been an Earth Fault over a number of days, and
then in quick succession on the same day. He stated that he would recommend
that the client ‘obviously, stop the machine and not use it and investigate deeper
what that earth fault is’.
968
Mr. Takac noted that a recurrent issue like that
requires ‘a lot more thorough testing’.
969
Mr. Ritchie’s Assessment of the Fault Prior to the Tragic Incident
509. Prior to the incident, it was Mr. Ritchie’s assessment that the earth fault was no
more than an inconvenient and intermittent issue, which did not pose any risk to
guest or Ride Operator’s safety.
970
During the inquest, he acknowledged that he
had consciously made a decision that the ‘intermittent fault’ would not be a
danger, as long as the operating procedures were followed.
971
510. At the time of the incident, Mr. Ritchie states that as the fault was happening ‘so
intermittently (four times in six days to my knowledge) and because I had already
contacted the experts to come and have a look at the situation, I did not consider
that it was necessary to shut the ride down or take any further steps as there was
no risk to staff or guests’.
972
967
Ex G2, [104]
968
T16-78, lines 40-48
969
T16-79, lines 9-20
970
Ex B3A(18), [53]
971
T17-83, lines 10-30
972
Ex B3A(18), [54]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 126 of 274

511. During the inquest, Mr. Ritchie gave evidence that it was his firm view that the
‘Alarm 14’ error was caused by an internal fault in the drive, rather than the
motors.
973
When challenged with the definition of the alarm as contained in the
operating manual for the drive, which stated that ‘there is a discharge from the
output phases to ground either in the cable between the frequency converter and
the motor or in the motor itself’,
974
Mr. Ritchie disagreed.
975
He was of the view
that an Earth Fault could not be intermittent.
976
However, he was unable to
explain, given his diagnosis, why during the QPS testing of the ride, which
involved some 200 starts and stops, the drives didn’t fail.
977
He based his opinion
on ’42 years’ experience as an industrial electrician.
978
HISTORY OF EXTERNAL SAFETY AUDITS AT DREAMWORLD
JAK Leisure Company Audits
512. In a scope of work prepared by Chief Executive Officer, Mr. Tony Braxton-Smith
in January 2003, it appears that the need for a safety audit at Dreamworld was
introduced, ‘for internal purposes to provide an overall assessment as to the
appropriateness of internal maintenance and engineering procedures and the
safety of operations.’
979
The assessment was intended to ‘identify any issues that
may impact on continued safe operation and to provide a prioritised list of specific
items for management attention’.
980
Accordingly, it was thought that a detailed
evaluation would need to be conducted of all amusement rides, attractions, as
well as associated buildings and structures, with the support and assistance of
maintenance and operations personnel.
513. The Consultant engaged would be required, as part of the evaluation, to review
the documentation, interview personnel and make physical inspections of the
rides and attractions, with any further expert testing required to then be
suggested.
981
A documented report was to be provided summarising the
assessment, findings and recommendations, with indications as to priority.
982
514. In terms of assessing the rides and attractions, Dreamworld required that the
Consultant engaged to carry out the safety audit consider the following in relation
to each ride:
983
• Queue lines, walkways, platforms, stairs, ramps and related structures
• Safety systems
• Passenger carrying vehicles
• Passenger restraint systems
• Lighting
• Guards, barriers, fencing and enclosure area
• Track systems
• Structural and support components
973
T18-37, lines 40-50
974
Ex G2(28), pg. 178
975
T18-37, lines 25-50
976
T18-37, lines 45-50
977
T18-40, lines 2-35
978
T18-40, lines 33-38
979
Ex F16B(23), pg. 1
980
Ex F16B(23), pg. 1
981
Ex F16B(23), pg. 1
982
Ex F16B(23), pg. 1
983
Ex F16B(23), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 127 of 274
• Drive systems
• Safety and instructional signage
• Ride area maintenance condition
• Safety related equipment
• Storage areas
515. In addition, the Consultant was also required to evaluate and assess ride
operations and maintenance procedures, and comment on the following specific
elements:
984
• Ride inspection and maintenance procedures
• Daily ride opening, operation and closing procedures and compliance
with manufacturers requirements
• Training procedures and Operator certification
• Comparison of written procedures and actual application of same
• Review of maintenance documents and procedures
• Review of preventative maintenance procedures and records
• Review of annual service procedures and records
• Review of incident reporting criteria
• Safety and efficiency of ride operations
516. It appears that JAK Leisure Company were ultimately engaged for this purpose.
JAK were billed as an internationally recognised auditor, who specialised in
Theme Park rides and attractions.
985
517. Documentation provided by Ardent Leisure confirms that JAK Leisure Company,
which were based in the United States, were engaged at various intervals over
a number of years to undertake an ‘independent safety audit’ of Dreamworld to
provide an ‘overall assessment as to the appropriateness of internal
maintenance and engineering procedures and the safety operations’.
986
In the
final reports provided of these assessments, which were titled, ‘Loss prevention
Survey’ of the amusement rides and attractions at the park, the scope of work
commissioned appears to be,
‘visual safety evaluations of all rides and associated buildings
and guest waiting areas directly associated with each ride,
including overall assessment of the condition of the ride and
evaluation of the maintenance being performed’.
Evaluation of the rides operation and any general issues that
are noted regarding the ride.
Visual safety evaluation of associated ride and attraction
maintenance support facilities including mechanical inspection,
housekeeping and documentation.
987
984
Ex F16B(23), pg. 2
985
Ex F16H(116), pg. 1
986
Ex F16B(17)
987
Ex F16B(1), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 128 of 274

518. The method and assessments conducted for the purpose of these inspections,
included the following:
988
• Personnel spent 12 days on-site observing and accessing the
procedures and conditions of the park.
• Various management staff in the Engineering and Operations
department were interviewed. In addition, mechanical and electrical
technicians and Ride Operators were interviewed and observed in the
function of their work.
• Procedures applicable to the Engineering and Operations Departments
were considered before staff were observed to evaluate compliance.
• Manufacturer’s manuals were considered to determine compliance.
• Compliance with Daily checklists by engineering and operations
personnel were observed to determine compliance with procedures, as
well as manufacturers and industry standards.
• JAK personnel walked each queue area, including stairs, ramps to note
the condition. Safety signage was also observed and considered.
• All passenger carrying vehicles and restraint systems were examined.
• Track systems, ride structure, drive systems and storage areas (where
applicable to the rides) were also examined.
• General Ride maintenance and condition were accessed on each ride
and attraction.
• Safety equipment, including fire extinguishers, water rescue equipment
and general life safety equipment and procedures were accessed.
• Operations training procedures, certification process and effectiveness
were reviewed and confirmed.
• Reviewed preventative maintenance records and accident reporting.
• Evaluated Fire Safety systems in buildings, structural safety where
applicable, and general condition of buildings.
• Reviewed organisational charts in both engineering and operations,
and job descriptions of personnel in the Engineering Department.
519. Whilst it’s not clear from the varied and somewhat sparse records available, it
appears that inspections were carried out by JAK Leisure Company in the
following years:
• 2003;
• 2004;
• 2006;
988
Ex F16B(1), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 129 of 274
• 2008-9;
• 2012; and
• 2013
520. Mr. Dennis Gilbert, who was the President of JAK Leisure Company, during their
engagement with Dreamworld, had previously held various positions within
different International Amusement Parks, including Chief Operations Officer and
General Manager.
989
In terms of engineering and mechanical matters, it does not
appear as though he had any formal qualifications.
521. Mr. Kevin Hehn, who reportedly accompanied Mr. Gilbert during some of the
inspections conducted at Dreamworld, was a certified Amusement Ride
Inspector and maintenance technician, who had previously held positions as a
Loss Control Specialist, ride mechanic and mechanical supervisor at various
United States Theme Parks.
990
522. Mr. Tan was responsible for assisting and coordinating JAK’s audits, with support
from the Operations and Safety Managers.
991
The reports provided by JAK
following the audits were considered by the managers of the Engineering,
Operational and Safety Departments.
992
523. A summary of the findings of each of these Surveys, in relation to the TRRR, are
outlined below.
May 2003 – Inspection
993
524. From the final report provided by JAK, it appears that assessments of each of
the rides at Dreamworld were conducted by Mr. Dennis Gilbert and Mr. Kevin
Hehn, ‘two qualified and experienced inspectors’
994
, between 1
st
to 14
th
May
2003.
525. With respect to the TRRR, the following issues were highlighted in Chapter 15 of
the Final Report:
995
I. DWORLD 03-15-01: It was noted that the E-Stop button on the Operator’s
control panel does not disable the conveyor when depressed. It was
recommended that the system be adapted to ensure positive emergency
stop to include all moving components to ensure full stop.
996
II. DWORLD 03-15-02: The permanently mounted evacuation ladders poses
as a blunt impact or possible entanglement hazard and should be removed
or elevated higher.
997
III. DWORLD 03-15-03: Loose anchor nuts on the guide rail bracket base,
located near the crocodile element, which were recommended to be
tightened.
998
989
Ex F16B(4)
990
Ex F16B(6)
991
Ex B3C(54), pg. 15
992
Ex B3C(54), pg. 16
993
Ex F16B(1)-(6)
994
Ex F16B(17), pg. 2
995
Ex F16B(3)
996
Ex F16B(3), pg. 2
997
Ex F16B(3), pg. 3
998
Ex F16B(3), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 130 of 274
IV. DWORLD 03-15-04: Heavy corrosion noted beneath the station platform
should be cleaned, evaluated and corrected.
999
V. DWORLD 03-15-05: Recommend the placement of additional signage
within the rafts stating the need to keep arms and legs within the raft at all
times to ensure that all riders see decals.
1000
VI. DWORLD 03-15-06: The location of the high voltage equipment for the
main pumps in relation to the electrical panels could pose itself as a serious
electrical hazard, should the adjacent retaining wall be breached by water.
It was recommended that this issue be considered by a qualified electrical
engineer.
1001
VII. DWORLD 03-15-07: Recommend installing a removable guide rail across
the opening of the reservoir gate/dam at raft level to prevent the possibilities
of blunt impact.
1002
VIII. DWORLD 03-15-08: Recommend that all control buttons be permanently
labelled.
IX. DWORLD 03-15-09: The monitor at the Operator position had been
removed. As this was the only means of observing the lower conveyor area,
it was recommended that the monitor be replaced immediately and that the
ride not be operated without this monitor in place or an Operator in place at
a positon to observe the lower area.
1003
X. DWORLD 03-15-10: Recommend that the areas that are step off, such as
the unload area, be highlighted to bring attention to the change in
elevation.
1004
XI. DWORLD 03-15-11: Noted emergency stop on conveyor. Recommend all
emergency stops be accented with the red colour.
1005
XII. DWORLD 03-15-12: The life ring at the base of the conveyor was noted to
not have AS certification stamp and is not recognised as a life saving
device. IT was recommended that all life rings and life jackets be AS
certified and dated. These should then be put on a review plan to ensure
that they are checked every year for current dates.
1006
XIII. DWORLD 03-15-13: Recommended proper safety signage of the Chlorine
storage behind the TRRR.
1007
XIV. DWORLD 03-15-14: Recommended that the Ride be pumped down on a
more frequent basis that annually to allow a visual inspection of the weir
logs, rail anchors and conveyor hardware, which are normally covered by
water.
1008
999
Ex F16B(3), pg. 5
1000
Ex F16B(3), pg. 6
1001
Ex F16B(3), pg. 7
1002
Ex F16B(3), pg. 8
1003
Ex F16B(3), pg. 10
1004
Ex F16B(3), pg. 11
1005
Ex F16B(3), pg. 12
1006
Ex F16B(3), pg. 13
1007
Ex F16B(3), pg. 14
1008
Ex F16B(3), pg. 15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 131 of 274

526. Whilst documentation in relation to the TRRR was requested by JAK,
1009
it is not
clear, from the records available, what information may have been provided for
the purpose of the audit.
1010
527. Upon completion of the final report, JAK presented the findings and
recommendations to the Safety Executive Committee.
1011
528. Following receipt of the report, it appears that an internal review by Dreamworld
was to be undertaken to determine the priorities for each recommendation.
1012
This included a number of meetings, which were held between an
Implementation Team that consisted of representatives from the Safety,
Operations and Engineering Departments, who were required to consider and
progress the recommendations made.
1013
According to Mr. Hutchings, this
Implementation Team were responsible for categorizing the recommendations
based on the risk posed, and the subsequent timeframe for which it needed to
be executed.
1014
He noted that whilst the aim was to implement all of the
recommendations, there were occasions when a decision was made not to do
so, which would be recorded.
1015
According to Mr. Hutchings, there was no
financial expenditure barrier to implementing the recommendations made by
JAK.
1016
529. Decisions as to the recommendations to be actioned and the timeframes were
transferred into an Excel spreadsheet, which was updated when the status of
items changed.
1017
The progress of implementing the recommendations was to
be reviewed by Dreamworld’s Safety Executive Committee on a quarterly basis,
with monthly reviews undertaken by Departments.
1018
Each Department
Manager was responsible for the final inspection and sign off on each item.
1019
November 2004 – Inspection
530. Documentation provided suggests that further inspections were carried out by
JAK between 2 and 11 November 2004.
1020
However, a letter dated 3 September
2004, addressed to Mr. Bob Tan, who was the General Manager of the E&T
Department at Dreamworld at the time, suggests that an alternative had been
sought to the ‘full independent safety audit proposal’ initially provided by JAK.
The alternate proposal was for a ‘follow-up audit to review the progress from the
previous visit’.
1021
The extent of this ‘follow-up’ audit is outlined as follows:
1022
• On-site audit and review of all items that were noted in the previous safety
audit conducted by JAK in May 2003;
1009
Ex F16B(16)
1010
Ex F16B(15)
1011
Ex C8(10), pg. 49
1012
Ex F16H(116), pg. 1
1013
Ex C8(10), pg. 42 -47
1014
Ex C8(10), pg. 44 - 47
1015
Ex C8(10), pg. 44
1016
Ex C8(10), pg. 55 & 56
1017
Ex F16H(116), pg. 2
1018
Ex F16H(116), pg. 2
1019
Ex F16H(116), pg. 2
1020
Ex F16C(3), pg. 1
1021
Ex F16C(11), pg. 1
1022
Ex F16C(11), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 132 of 274
• Documentation and comment on progress made at Dreamworld on those
items noted in the previous safety audit; and
• Documentation on items outstanding from previous report.
531. It was proposed that the inspection was to be conducted with one qualified
inspector, and an electronic report prepared with photographs and ‘the
appropriate code and standards comments’, which was then to be presented to
management at the conclusion.
1023
The cost of the report was quoted as being
$9,500 ($US). At the conclusion of the correspondence, it was stated that:
It is the recommendation from JAK Leisure Company to all of
our clients that consideration be given to the advantage of
having our inspectors conduct a full independent safety audit
on an annual basis. With the full audit, repeat items from
previous reports are noted, as well as, all attractions and
facilities are inspected for operational and maintenance safety
issues.’
1024
532. The findings in relation to the TRRR were outlined in Chapter 15 of the final
report.
1025
Helpfully, this report considered the recommendations made in 2003,
and confirmed whether the recommended changes had been implemented. The
findings were as follows:
I. DWORLD 04-15-01: E-Stop at the control panel now able to disable the
conveyor as well.
1026
II. DWORLD 04-15-02: Management assessed that the rafts do not hit the
area where the evacuation ladder was placed. Action was marked as
incomplete.
1027
III. DWORLD 04-15-03: This item was marked as corrected and ongoing.
1028
IV. DWORLD 04-15-04: In terms of the heavy corrosion observed bellow the
station platform, this action item was marked as on going. It was further
noted that given the age of the ride, the corrosion hidden by the themed
elements may be ‘severe’. As such, plans should be made to evaluate these
areas for possible failure. This item was marked as ‘ongoing’.
1029
V. DWORLD 04-15-05: The additional signage had not been placed in the
rafts. The item was marked as ‘incomplete’.
1030
VI. DWORLD 04-15-06: RCD protection was added to the high voltage
equipment, and as such, the item was marked as complete.
1031
VII. DWORLD 04-15-07: The flow of water was evaluated by management and
it was determined that reservoir gating, which may create back draft of
1023
Ex F16C(11), pg. 1
1024
Ex F16C(11), pg. 1
1025
Ex F16C(2)
1026
Ex F16C(2), pg. 2
1027
Ex F16C(2), pg. 3
1028
Ex F16C(2), pg. 4
1029
Ex F16C(2), pg. 5
1030
Ex F16C(2), pg. 6
1031
Ex F16C(2), pg. 7
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 133 of 274
water and could cause issues with rafts. The item was marked as
closed.
1032
VIII. DWORLD 04-15-08: In terms of the labelling of all control buttons, it was
noted that progress had been made. As such, the item was marked as
partially completed.
1033
IX. DWORLD 04-15-09: The video monitor had been replaced and upgraded.
The action item was marked as compete.
1034
X. DWORLD 04-15-10: Areas of elevation highlighted. Item marked as
complete.
1035
XI. DWORLD 04-15-11: All emergency stops accented with red colour. Item
marked as complete.
1036
XII. DWORLD 04-15-12: In relation to the life ring at the base of the conveyor,
the Australian Standard was researched by Dreamworld staff and it was
found that there was none applicable. As such, no action was deemed to
be required.
1037
XIII. DWORLD 04-15-13: In relation to the chlorine storage behind the raft ride,
it was noted that the water conditions had been improved. The
recommendation in terms of the need for additional signage was to
stand.
1038
XIV. DWORLD 04-15-14: It was noted that the TRRR was pumped down two
times a year to examine the condition of the trough. Item was therefore
marked as complete.
1039
533. In addition to the above, JAK also recommended that evacuation procedures be
re-evaluated on rides where more ‘specific evacuation procedures’ are called for,
which included the TRRR.
1040
The Dreamworld Board response to this
recommendation was that ‘specific ride evacuation procedures are in place for
these rides…’
1041
534. A document titled, ‘Information for JAK’, which was dated 4 November 2004,
appears to outline the planned improvements to be carried out for various rides.
In relation to the TRRR, the following actions were listed:
1042
• Dual unload gates;
• Raft rotate feature;
• Timed dispatcher;
• Handgrips;
• E/Stop – 2 pumps?
1032
Ex F16C(2), pg. 8
1033
Ex F16C(2), pg. 9
1034
Ex F16C(2), pg. 10
1035
Ex F16C(2), pg. 11
1036
Ex F16C(2), pg. 12
1037
Ex F16C(2), pg. 13
1038
Ex F16C(2), pg. 14
1039
Ex F16C(2), pg. 15
1040
Ex F16C(6), pg. 4
1041
Ex F16C(6), pg. 4
1042
Ex F16C(9)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 134 of 274
• Conveyor stop?
535. It seems these were the actions Dreamworld intended to take or were
considering carrying out in relation to this ride. No further information was
provided as to why these actions had been included, and whether they were
actioned.
536. A spreadsheet listing all of the audit items and recommended actions as
suggested by JAK in relation to each ride, was maintained by Dreamworld, with
the status of each item updated at various intervals.
1043
A spreadsheet from 24
April 2006, suggests that all of the outstanding action items for the TRRR, as
listed above, had been completed except for the rebuilding of the timber load and
unload stations, which was in progress at the time.
1044
July 2006 – Inspections
537. Prior to a safety audit being conducted at Dreamworld in 2006, it appears that
quotes were sought from JAK and David Randall and Associates (DRA).
538. On 25 January 2006, a quote was provided to Mr. Bob Tan by DRA in relation to
Safety audits of Dreamworld, which would be ‘looking at compliance to both
AS3533 and the current Workplace Health & Safety Legislation’.
1045
DRA, at that
time, conducted audits for Warner Village Theme Parks, and had developed a
checklist from AS3533 requirements, which covered the following elements:
1046
• Maintenance schedules compared to the manufacturer’s requirements
and AS3533;
• Operations manuals compared with the manufacturer’s requirements;
• Attendance at the daily inspections to ensure standardisation of
procedures and training of staff;
• Observation of Operators to ensure compliance with operation
procedures;
• An inspection of the ride to identify any areas of statute non-compliance,
i.e. guarding, structural integrity etc; and
• Riding on the device to ensure clearance zones are observed, etc.
539. From previous experience at Warner Village Theme Parks, DRA suggested that
it would take three days to thoroughly audit the large rides, with the smaller rides
(such as the children’s train) taking up to a day to complete.
1047
The proposed
completed report by DRA was to include an executive summary, the results of
the audit and an action plan to remedy areas of non-compliance ranked
according to their risk. The risk assessment method utilised had been adopted
from AS4360.
1043
Example is Ex F16C(14) & Ex F16C(20)
1044
Ex F16C(30)
1045
Ex F16D(13), pg. 1
1046
Ex F16D(13), pg. 1
1047
Ex F16D(13), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 135 of 274
540. A scope of work was provided by JAK canvassing largely the same areas as was
the case in 2003. Ultimately, a decision was made to once again engage JAK.
Documentation provided suggests that further inspections were carried out at
Dreamworld between 12 and 26 July 2006.
1048
On this occasion, a full
independent safety audit of the Park was commissioned, which included an
‘overall assessment of ride equipment, appropriateness of internal maintenance
and engineering procedures, as well as, the safety of operations’.
1049
In addition,
emphasis was to be placed on the electrical area of the Park with a Professional
Electrical Engineer attending as one of the qualified inspectors. It is important to
note that in the scope of work provided by JAK, whilst it explicitly included ‘visual
loss prevention and safety evaluation of all Amusement rides’, as well as a ‘visual
safety evaluation of associated ride and attraction maintenance support
facilities’, and ‘visual evaluation of ride operations and maintenance procedures
as related to safety and operational standards’, the applicable Australian
Standards (especially AS3533) are not cited, nor is any specific clarification
provided as to what standard (if any) such an evaluation was to be conducted.
1050
541. With respect to the TRRR, the following issues were highlighted in Chapter 15 of
the Final Report:
1051
I. DWORLD 06-15-01: Recommended that all access to boarding the ride by
guests have accessible safety requirement signs.
1052
II. DWORLD 06-15-02: Recommended that all objects, such as fans, theme
pieces, lighting that could fall on guest pathways be secured with a safety
cable to ensure single point failure will not allow to land on or swing into
guests.
1053
III. DWORLD 06-15-03: Recommend the placement of additional signage
within the rafts stating the need to keep arms and legs within the raft at all
times to ensure that all riders see decals. It was noted that this was a repeat
recommendation.
1054
IV. DWORLD 06-15-04: Control panel noted all buttons and indicator lights are
properly labelled on day of audit.
1055
V. DWORLD 06-15-05: Noted that the cameras in station area are not secured
by secondary point. Recommended that all overhead objects be secured to
prevent single point failure that could result in fall onto guests or
employees.
1056
VI. DWORLD 06-15-06: Noted actuator button not labelled. Recommend that
all Operator buttons be clearly labelled.
1057
1048
Ex F16D(8)
1049
Ex F16D(15)
1050
Ex F16D(14)
1051
Ex F16D(12)
1052
Ex F16D(12), pg. 2
1053
Ex F16D(12), pg. 4
1054
Ex F16D(12), pg. 5
1055
Ex F16D(12), pg. 6
1056
Ex F16D(12), pg. 7
1057
Ex F16D(12), pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 136 of 274
VII. DWORLD 06-15-07: Recommend that the area under the lift hill be cleaned
out and a handrail be replaced on the far side of the work area under the
lift as it was severely corroded.
1058
VIII. DWORLD 06-15-08: Recommend tightening the connector at the bottom of
the motor unit. The current connector shown was loose at the time of
inspection.
1059
IX. DWORLD 06-15-09: Recommend opened electrical box and wiring be
repaired or removed to prevent electrical shock.
1060
X. DWORLD 06-15-10: Recommend the steel box tube located at the top of
the lift hill in the access walk be secured to ensure it does not move out into
the lift hill, or is loose to fall onto the feet of employees using the
walkway.
1061
XI. DWORLD 06-15-11: Recommend the Park have a certified diver available
onsite to allow for immediate maintenance and inspection of the underwater
items on the water attractions.
1062
XII. DWORLD 06-15-12: Recommend installation of pipe supports for the PVC
pipe under the pedestrian bridge over the rapids ride.
1063
XIII. DWORLD 06-15-13: Recommend removal of all old bridge bolts from
pedestrian bridge of the ride.
1064
XIV. DWORLD 06-15-14: Recommend regular review of the pedestrian bridge
plank bolts to make sure they are installed and holding the planks in position
properly. The bolts should be galvanised or stainless.
1065
XV. DWORLD 06-15-15: Conveyor – Recommend the UHMW plastic be
chamfered at the end to reduce the chance for catching the lift chain boards
while sliding on the plastic.
1066
XVI. DWORLD 06-15-16: Conveyor - Recommend reduction in the amount of
grease being used on the lift hill bearings.
1067
XVII. DWORLD 06-15-17: Recommend the access gate to the lift hill of the ride
be installed with a latch of some nature which cannot be opened by a
standard guest.
1068
XVIII. DWORLD 06-15-18: Recommend installation of a diagonal support behind
the guide-way column in the rapids trough. The current column is loose at
1058
Ex F16D(12), pg. 9
1059
Ex F16D(12), pg. 10
1060
Ex F16D(12), pg. 11
1061
Ex F16D(12), pg. 12
1062
Ex F16D(12), pg. 13
1063
Ex F16D(12), pg. 14
1064
Ex F16D(12), pg. 15
1065
Ex F16D(12), pg. 16
1066
Ex F16D(12), pg. 17
1067
Ex F16D(12), pg. 18
1068
Ex F16D(12), pg. 19
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 137 of 274
the anchor bolts and should be braced to reduce movement on impact from
a raft at this location.
1069
XIX. DWORLD 06-15-19: Recommend the light attached to the bridge just past
the load station be secured using through bolts and a backing plate rather
than lag screws.
1070
XX. DWORLD 06-15-20: Recommend review of the anchor bolts for the weir in
the water channel to be sure they are secure and tight to the channel
bottom.
1071
XXI. DWORLD 06-15-21: Recommend review of the old column supporting the
old Sky Link deck above the ride, as it has a large amount of corrosion.
1072
XXII. DWORLD 06-15-22: Recommend repairs to the rock work at the entry to
the tunnel on the right side.
1073
XXIII. DWORLD 06-15-23: Recommend review of the interior rock work in the
tunnel of the ride as it has many cracks. A regular review of the condition
should be made and a determination made what the useful life of the rock
work is according to the installation.
1074
XXIV. DWORLD 06-15-24: Recommend ALL logs and branches found within the
tunnel area of the ride be secured to the deck so they cannot enter the
trough of the ride.
1075
XXV. DWORLD 06-15-25: Recommend all old posts and stands along the trough
sides be removed.
1076
XXVI. DWORLD 06-15-26: Recommend review of the air exhaust coming out in
the tunnel passing under the mine ride.
1077
XXVII. DWORLD 06-15-27: Recommend review of the corrosion on the columns
supporting the tunnel roof and the mine ride, located adjacent to the rapids
trough.
1078
XXVIII. DWORLD 06-15-28: Recommend review of these open bulb type fixtures
in areas above the guest ride.
1079
XXIX. DWORLD 06-15-29: Recommend installation of or painting of the depth at
the edge of the dock.
1080
1069
Ex F16D(12), pg. 20
1070
Ex F16D(12), pg. 21
1071
Ex F16D(12), pg. 22
1072
Ex F16D(12), pg. 23
1073
Ex F16D(12), pg. 24
1074
Ex F16D(12), pg. 25
1075
Ex F16D(12), pg. 26
1076
Ex F16D(12), pg. 27
1077
Ex F16D(12), pg. 28
1078
Ex F16D(12), pg. 29
1079
Ex F16D(12), pg. 30
1080
Ex F16D(12), pg. 31
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 138 of 274

XXX. DWORLD 06-15-30: Noted sharp edge of roof below head height on the
non-station side of the trough. Suggest that this be marked or removed to
ensure no impact to the head of employees.
1081
XXXI. DWORLD 06-15-31: Noted appropriate signs and response equipment to
deal with chlorine storage area. Suggest measured introduction of chlorine
into the Rapid Ride based on size and dosage necessary to maintain proper
levels.
1082
September 2009 – Inspections
542. From 21 to 30 September 2009, Ocean Embassy (Formerly JAK Leisure
Company) conducted safety audits of the rides and attractions at
Dreamworld.
1083
During this audit, personnel spent 12 days on-site, observing
and accessing the procedures and conditions of the Park, as well as interviewing
various staff at different levels.
1084
543. Records suggest that the scope of work of the audit conducted in 2009 were
intended to be a ‘follow-up’ and not a full independent safety audit.
1085
As such,
the audit consisted of conducting visual loss prevention and safety evaluations
of all amusement rides, attractions, associated buildings and facilities, review of
the audit items carried out in July 2006, as well as a full safety audit of a number
of rides, which included the TRRR.
1086
The specific issues cited for the TRRR
were, ‘manual handling issues with raft arrivals and handling; operational system
in supervisor and operator competency training methodologies’.
1087
544. A fee of $26,200 (US$) was payable for this work and the provision of the final
report.
1088
545. With respect to the TRRR, the following issues were highlighted in Chapter 15 of
the Final Report:
1089
I. DWORLD 09-15-01: Verbiage on the official safety notice at the ride is
repeated in the theme signs, which is acceptable if all official notices are in
standard format on the red background signs and placed to ensure guests
have access to read them prior to boarding.
1090
II. DWORLD 09-15-02: Recommend that all objects such as fans, theme
pieces, lighting that could fall on guest pathways be secured with a safety
cable to ensure a single point failure will not allow it to land on or swing into
guests.
1091
1081
Ex F16D(12), pg. 32
1082
Ex F16D(12), pg. 33
1083
Ex F16E(5)
1084
Ex F16E(5), pg. 2
1085
Ex F16E(114), pg. 1
1086
Ex F16E(110), pg. 1 & 2
1087
Ex F16E(110), pg. 1 & 2
1088
Ex F16E(109), pg. 3
1089
Ex F16E(7)
1090
Ex F16E(7), pg. 2
1091
Ex F16E(7), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 139 of 274
III. DWORLD 09-15-03: It was noted that the buttons and indicators on the
control panel at the main Operator’s booth were properly labelled on the
day of the audit.
1092
IV. DWORLD 09-15-04: The ‘emergency shutdown’ procedure posted at
ride. During an emergency, it was recommended that a simpler
automatic process should be considered. Recommend that the safety
system be updated to ensure correct steps are taken by a single
emergency button, which will ensure the appropriate timing and
sequence.
1093
V. DWORLD 09-15-05: Noted that cabinets at the panel area are in disarray
and cluttered.
1094
VI. DWORLD 09-15-06: Recommended immediate discontinued use of fan in
queue area as it is rusted and corroded.
1095
VII. DWORLD 09-15-07: Monitor at the Operator panel does not appear to be
an outdoor, mountable monitor, and should be replaced or at least secured
to prevent falling.
1096
VIII. DWORLD 09-15-08: Recommended all overhead objects, including
cameras, be secured to prevent single point failure.
1097
IX. DWORLD 09-15-09: Noted that there was damaged and inconsistent
application of safety decals on all ten rafts in the station. Recommend all
decals be replaced and ongoing program to ensure proper decals are in
place.
1098
X. DWORLD 09-15-09(2): Noted non-skid finishes on entry to following boats
has worn beyond its useful life on a number of rafts. Recommend a non-
skid be applied to essential areas of loading.
1099
XI. DWORLD 09-15-10: A number of rafts were seen to have Velcro seat belts
worn beyond useful life.
1100
XII. DWORLD 09-15-11: Recommended program instituted to check all life ring
units and other such preservers around the bodies of water in the Park on
a regular basis to ensure they are appropriate for planned use of rescue.
Recommend research be undertaken to ensure compliance to Australian
Standard of water safety.
1101
XIII. DWORLD 09-15-12: Recommend review of the corrosion on the gates in
the upper pump pool.
1102
1092
Ex F16E(7), pg. 4
1093
Ex F16E(7), pg. 5
1094
Ex F16E(7), pg. 6
1095
Ex F16E(7), pg. 7
1096
Ex F16E(7), pg. 8
1097
Ex F16E(7), pg. 9
1098
Ex F16E(7), pg. 10
1099
Ex F16E(7), pg. 11
1100
Ex F16E(7), pg. 12
1101
Ex F16E(7), pg. 13
1102
Ex F16E(7), pg. 14
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 140 of 274
XIV. DWORLD 09-15-13: Recommend installation of retaining clips on the grate
at the end of the walkway above the pump pool and conveyor to hold gate
section in place.
1103
XV. DWORLD 09-15-14: Recommend replacing the boot material around the
slide boot on the lift hill emergency stop box.
1104
XVI. DWORLD 09-15-15: Recommend review of the corrosion in the service
area by the pump motors.
1105
XVII. DWORLD 09-15-16: Recommend replacing the wooden members of the
roof under the lift hill chain during the chain change out. The wood has
significant rot and should be replaced as soon as budget allows.
1106
XVIII. DWORLD 09-15-17: Recommend the heat tape used on the motors be
installed permanently or that a switch box be installed to control the
operation and protect against shock.
1107
XIX. DWORLD 09-15-18: Recommend the mount bolts for the motors are
Ultrasound tested to verify condition on a regular basis if not currently
done.
1108
XX. DWORLD 09-15-19: Recommend review of the underside of the main
bridge crossing over the ride. The bridge was scheduled for replacement in
a year or so.
1109
XXI. DWORLD 09-15-20: Recommend installation of safety cables to prevent
the single point mount or attachment from breaking – lighting.
1110
XXII. DWORLD 09-15-21: Recommend the landscape hanging into the ride be
monitored by the landscapers and trimmed as necessary.
1111
XXIII. DWORLD 09-15-22: Recommend installation of a board at the lower third
board level in order to keep boats from getting caught under the upper two
boards – in cave.
1112
XXIV. DWORLD 09-15-23: Recommend using shorter tire pieces to keep them
better attached to the wood supports.
1113
XXV. DWORLD 09-15-24: recommend the chlorine response kits are checked on
a regular schedule and the paperwork is checked for readability.
1114
XXVI. DWORLD 09-15-25: Recommend review of the boat maintenance area and
how it is utilised for the work process on the boats during normal operation.
1103
Ex F16E(7), pg. 15
1104
Ex F16E(7), pg. 16
1105
Ex F16E(7), pg. 17
1106
Ex F16E(7), pg. 18
1107
Ex F16E(7), pg. 19
1108
Ex F16E(7), pg. 20
1109
Ex F16E(7), pg. 21
1110
Ex F16E(7), pg. 22
1111
Ex F16E(7), pg. 23
1112
Ex F16E(7), pg. 24
1113
Ex F16E(7), pg. 25
1114
Ex F16E(7), pg. 26
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 141 of 274
It was suggested that a lift unit or rail system could be installed to assist in
the movement of the boats within the area.
1115
546. Further supplementary comments were provided by the auditors, which were
detailed in a separate report.
1116
In relation to the TRRR, the following was
recommended:
1117
• Noted that the manual handling and turning of units as they enter the
unload area on a relatively unstable waterway presents operational and
safety issues in preventing guests or staff from stumbling or falling. It
was noted during the audit that unload Operators were handling the
rafts in a consistent manner in accordance with procedures.
• Suggestions to solve the instability of the units were:
o A rotating system commonly used on other raft rides to allow
continued movement of units and to provide a stable surface for
units to rest upon during the load and unload process.
o Queuing of boats in the load/unload area and loading/unloading
in mass and then dispatching with spacing. This would require
a belt system to be speedy and steady enough to handle.
o Indexing the units on a stable surface – suggested to be the
safest option.
• It was recommended in report that control system be reviewed and
consideration be given to updating, especially in relation to the
emergency shut down procedure.
March 2013 – Inspections
547. From 17 February until 2 March 2013, Ocean Embassy conducted safety audits
of the rides and attractions at Dreamworld.
1118
The scope of work intended to be
the subject of these full safety audits where outlined by Mr. Bob Tan in a
document dated 4 June 2012, and largely consist of those previously provided
by JAK.
1119
It appears that three companies were approached to provide a quote
on the proposed scope of work, however, only two responded.
1120
Ultimately,
Ocean Embassy was selected to conduct the audits. The cost for this service
was $30,200 (US$).
1121
548. With respect to the TRRR, the following issues were highlighted in Chapter 15 of
the Final Report:
1122
I. DWORLD 13-15-01: Recommended evaluation of allowing Bats within the
tunnel of ride. Also, review of concrete ceiling inside the ride.
1123
1115
Ex F16E(7), pg. 27
1116
Ex F16E(1)
1117
Ex F16E(1), pg. 7
1118
Ex F16F(20), pg. 1
1119
Ex F16F(9)
1120
Ex F16G(14)
1121
Ex F16G(16)
1122
Ex G16F(18), pg. 244 onwards
1123
Ex G16F(18), pg. 245
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 142 of 274
II. DWORLD 13-15-02: Recommend bolts on weir log be changed or secured
so it will not be sticking up and result in impact with boat tube.
1124
III. DWORLD 13-15-03: Recommend general clean-up in the pump pit area of
the ride.
1125
IV. DWORLD 13-15-04: Recommend fire extinguishers be placed in
compliance with the Dreamworld requirement for inspection every 6
months.
1126
V. DWORLD 13-15-05: Recommend the themed wood and items on the
loading deck of the ride to be repaired, changed out and removed.
1127
VI. DWORLD 13-15-06: Recommend labelling of the gate and E-stop buttons
of the ride, located at the far end of the boat dispatch fence. Ride control
buttons should be labelled and identified as to action and/or function.
1128
VII. DWORLD 13-15-07: Recommend repainting of the EXIT and ‘arrow’ on the
walkway from the ride to better identify the exit pathway and direction.
1129
VIII. DWORLD 13-15-08: Suggest removal of chlorine kit at the back of the
TRRR.
1130
IX. DWORLD 13-15-09: Noted roof deterioration with pieces of roof falling off.
Recommend review of queue structure and roof for repair.
1131
X. DWORLD 13-15-10: Noted emergency light failed the power test.
Recommend review of all emergency lights in queue and review of testing
method and frequency.
1132
XI. DWORLD 13-15-11: Noted rusted and corroded fan in queue area.
Recommended discontinued use of fans in this condition.
1133
XII. DWORLD 13-15-12: Noted cameras in station do not have safety cable to
prevent single point failure.
1134
XIII. DWORLD 13-15-13: Noted ‘emergency shutdown’ procedure posted at
the ride. Recommended that during an emergency, a simpler
automatic process should be considered. Recommend that the safety
system be updated to ensure correct steps are taken by a single
emergency button, which will ensure the appropriate timing and
sequence.
1135
1124
Ex G16F(18), pg. 246
1125
Ex G16F(18), pg. 247 & 248
1126
Ex G16F(18), pg. 249
1127
Ex G16F(18), pg. 250
1128
Ex G16F(18), pg. 251
1129
Ex G16F(18), pg. 252
1130
Ex G16F(18), pg. 253
1131
Ex G16F(18), pg. 254
1132
Ex G16F(18), pg. 255
1133
Ex G16F(18), pg. 256 & 257
1134
Ex G16F(18), pg. 258 & 259
1135
Ex G16F(18), pg. 260
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 143 of 274
XIV. DWORLD 13-15-14: Noted Operator panel – the labelling was ‘worn
and difficult’ to read, Recommend replacement of faded labels.
1136
XV. DWORLD 13-15-15: Expired registration is posted at ride and should be
removed - not required.
1137
XVI. DWORLD 13-15-16: Poor housekeeping in control panel area.
Recommended that it be kept in good order and better practices be
enforced.
1138
XVII. DWORLD 13-15-17: Noted damaged and inconsistent application of safety
decals on rafts. Recommend all decals be reviewed and replaced as
necessary. Further recommended that there be an ongoing program to
ensure proper decals are in place.
1139
XVIII. DWORLD 13-15-18: Recommended program instituted to check all life ring
units and other such preservers around the bodies of water in the Park on
a regular basis to ensure they are appropriate for planned use of rescue.
Recommend a reaching hook be placed near such bodies of water and that
an inspection program be implemented on all water-safety equipment with
proper tags and records.
1140
XIX. DWORLD 13-15-19: Safety cable to be installed for overhead speaker at
front of ride.
1141
549. A spreadsheet was maintained recording each of the recommendations made
by JAK/Ocean Embassy and Dreamworld’s response, including whether the task
had been completed or whether the risk was acceptable and no further action
needed to be taken.
1142
The recommendation suggesting a simpler automatic
shutdown process for the TRRR was recorded as ‘risk acceptable’.
1143
Comments about JAK / Ocean Embassy Safety Audits
550. The safety audits conducted by JAK Leisure Company/Ocean Embassy, whilst
seemingly thorough, were largely focused on the aesthetic issues associated
with rides and attractions at Dreamworld, rather than a proper safety assessment
against the applicable Australian Standards (AS-3533). This limitation was
known and recognised by Dreamworld in supporting documentation provided
during the course of the inquest hearing, whereby it was noted that,
An external audit is performed every 3 years by JAK. Reviewing
the value of this audit. Much time is being spent on aesthetics
per the external audit when more pressing issues need to be
addressed. The difficulty with JAK audit is they are based
internationally and are not aware of the Australian Standards
which are usually different to international standards. Is there
an Australian body that does a similar audit/review? Based
1136
Ex G16F(18), pg. 261
1137
Ex G16F(18), pg. 262
1138
Ex G16F(18), pg. 263
1139
Ex G16F(18), pg. 264
1140
Ex G16F(18), pg. 265 & 266
1141
Ex G16F(18), pg. 267
1142
Ex D6(129)
1143
Ex D6(129)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 144 of 274

on price, being coming for 8 years. There are Australian
companies that do the same thing.
1144
551. During the inquest, Mr. Hutchings acknowledged the concern held in relation to
the fact that the audits by JAK were not being conducted to the Australian
Standards.
1145
552. The reoccurring nature of the recommendations made by JAK, particularly given
the cost of the reports, was also raised by Dreamworld staff in the E&T
Department following the 2013 audit.
1146
It was noted that:
1147
Issues
An analysis of each JAK survey identifies common issues and
recurring recommendations for each ride. So much so, the
survey report from 2013 is substantially similar to that of
previous surveys. Given that each JAK review costs circa $60K,
it is debatable whether a future JAK survey (scheduled for
2016) represents ongoing value for money. This issue has
generated discussion amongst the Dreamworld Safety and
Engineering Departments as to what other options are available
to improve safety outcomes and ensure value for money.
Most preferred option
Whilst various options are available, the most preferred option
would involve a twofold approach focussing on improving
existing systems as well as an external auditor subjecting the
rides/systems to an Australian Standard 3533 audit.
…
AS3533 Audit – as of 2012, the new nationalised safety
legislation requires all amusement devices to be inspected and
accredited against AS3533. Whilst this could be done with in-
house expertise, the preference is to utilise independent
expertise. (JAK are not able to undertake specific AS3533
audit, as they predominantly reference American and European
standards). However, a variety of local or international auditors
could perform this task…
553. Unfortunately, despite repeated attempts during the course of the coronial
investigation to contact and obtain information from Mr. Gilbert and JAK Leisure
Company/Ocean Embassy, no response was ever received. It is not entirely
clear, therefore, the actual extent of JAK’s involvement with Dreamworld, the
scope of the brief or the intended limitations of the advice provided. This is further
exacerbated by the limited and ad hoc nature of the documentary records
retained, a significant number of which were only provided whilst Court was
sitting, rather than beforehand.
554. That being the case, given the qualifications of Mr. Gilbert and Mr. Hehn, which
were known prior to engagement with the company, as well as the superficial
1144
Ex F16H(7), pg. 1
1145
T21-49, lines 5-35
1146
Ex F16H(115)
1147
Ex F16H(115), pg. 1 & 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 145 of 274
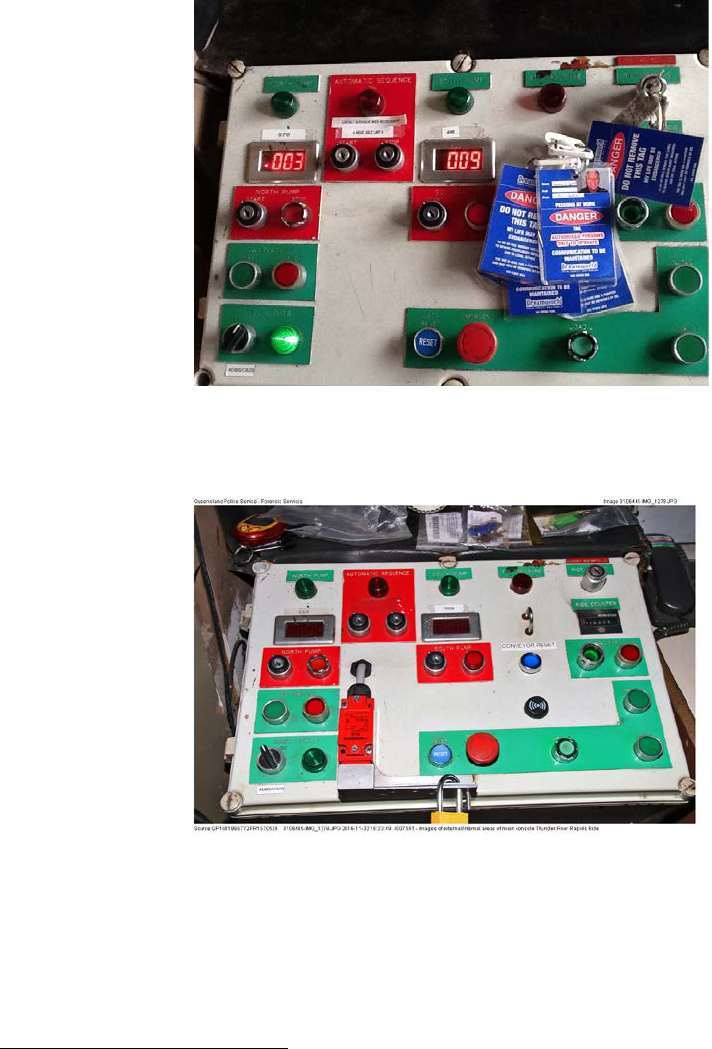
nature of the audits conducted, as was recognised by Dreamworld, it seems
obvious that the safety advice provided was not intended to be a substitute for a
thorough hazard assessment of the amusement rides, as was stipulated
pursuant to the Standards.
555. Furthermore, some of the recommendations made by JAK, which may have
pertained to safety, such as the labelling of the Main Control Panel buttons and
the E-Stop at the unload area, which were raised in previous years, were not
actioned by Dreamworld. In 2013, the Main Control Panel at the loading area
when considered by JAK appeared as below:
1148
556. The Main Control Panel on the date of the incident, appeared as follows:
1149
557. Mr. Naumann, the Maintenance Planner for Dreamworld at the time of the
incident, acknowledged during his interview with OIR, that the recommendations
made by JAK, particularly as to the labelling of the control panel and E-Stop at
the unload area at the TRRR, should have been actioned during the annual
shutdown of the ride, however, were not carried out.
1150
He could not offer an
1148
Ex F16F(19), pg. 261
1149
Ex B6(6)(g)(ii), pg. 50
1150
Ex B3C(15), pg. 18
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 146 of 274

explanation as to why this hadn’t occurred.
558. The E-Stop at the unload area at the time of the tragic incident, appeared as
below:
1151
559. Despite the recommendations made by the external auditor that the ride control
buttons, including the E-Stop, should be labelled and the action identified, in a
response provided to OIR by Ardent during the course of their investigation into
the circumstances of this tragic incident, they maintain that ‘the emergency stop
button at the unload platform of the TRRR was clearly marked on 25 October
2016’.
1152
This is clearly not the case.
DRA Safety Management Audits
560. In 2013, DRA Safety Specialists were first engaged by Ardent Leisure through
Mr. Hutchings, to conduct audits of the Work Health and Safety Management
Systems (WHSMS) in place in all of its businesses, including Dreamworld,
having regard to the National Self Insurance WHS Audit tool (based on AS
4801).
1153
The Managing Director of DRA, Mr. David Randall, who is a certified
practicing engineer and a globally certified OHS auditor, states that these audits
involved a ‘systematic examination of the WHSMS against defined criteria in the
1151
Ex C4(5), pg. 316
1152
Ex C6(7), [66]
1153
Ex C4(16), pg. 1; Ex C5(35)(a), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 147 of 274

National Self Insurance WHS Audit Tool, to review its effectiveness in managing
health and safety in the workplace and ensure it achieves the organisation’s
policies and objectives in that regard’, which is done by looking at the procedures
and processes set up to manage an overall health and safety program.
1154
This
auditing process is different to that of a workplace inspection to detect specific
deficiencies, failures or hazards in particular processes or areas.
561. Whilst DRA were also engaged by Dreamworld to consider two specific instances
on rides involving the Cyclone Rollercoaster and the Log Ride, they were not
involved in the inspection of any specific ride from a safety or operational
perspective.
1155
Mr. Randall confirmed that the TRRR was not specifically
inspected or part of the audits conducted.
1156
562. Following DRA’s first WHSMS audit in 2013, annual audits were scheduled and
performed in February 2014 and July 2015 for the purpose of determining
whether the WHSMS had been properly implemented and maintained, and to
monitor the process of the implementation of recommendations made.
1157
Subsequent consultancy visits were also undertaken to further assist with
implementation in October 2014, November 2014, January 2015, April 2015,
December 2015, April 2016 and August 2016.
563. According to Mr. Randall, the safety management system at Dreamworld was
below industry standards when compared to Village Roadshow Parks, however,
was above others.
1158
He describes Village Roadshow’s safety management
system and the recording for the maintenance of their rides as ‘strong’, and he
intended to try and assist Dreamworld to achieve a similar standard.
1159
During
the inquest, Mr. Randall stated that after his audit at Dreamworld, he identified
the need for a ‘very strong safety maintenance system’ to be put in place, as well
as a ‘good maintenance engineer’ to establish the systems required.
1160
564. Following on from Mr. Randall’s recommendations, it appears that Mr. Deaves
was promoted to General Manager of Engineering, with Mr. Tan being moved to
Special Projects. In relation to Mr. Tan, Mr. Randall stated during the inquest
that, ‘he is a very capable engineer, but the systems that I desire and require for
me to be able to certify a ride weren’t there.’
1161
February 2013 Audit
565. The first audit conducted by DRA at Dreamworld took place over four days in
February 2013.
1162
It involved a desktop audit of Dreamworld’s WHSMS, along
with a review of Departments, including Operations and Maintenance, which
included an evaluation of checklists, worker competencies, risk management
documentation for particular rides, as well as a pre-start inspection of the newest
ride, the Buzz Saw.
1163
1154
Ex C4(16), pg. 1
1155
Ex C4(16), pg. 2
1156
Ex C5(35)(a), pg. 16
1157
Ex C4(16), pg. 1
1158
Ex C5(35)(a), pg. 13
1159
Ex C5(35)(a), pg. 14
1160
T24-6, lines 20-30
1161
T24-6, lines 37-47
1162
Ex C4(16), pg. 1
1163
Ex C4(16), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 148 of 274
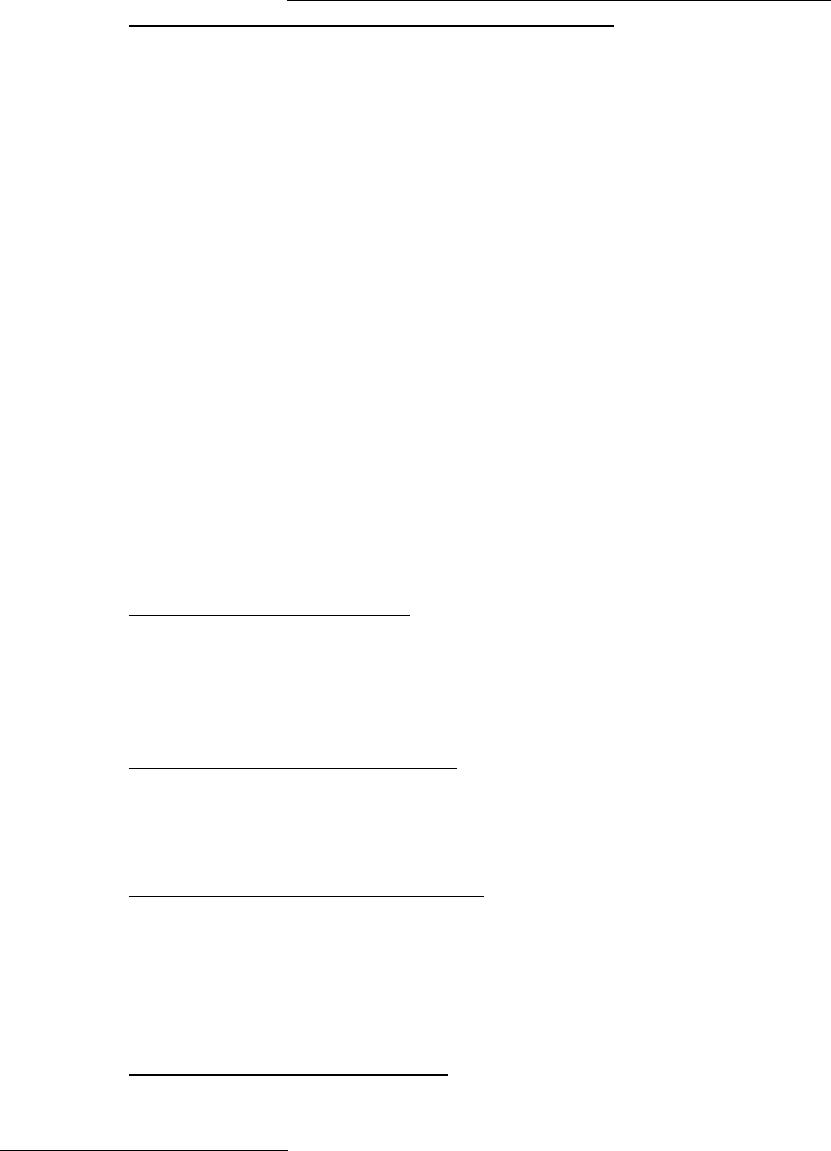
566. The Executive Summary of the findings highlight the following matters:
1164
• The safety management system was originally located on Lotus Notes,
which was no longer supported and had limited access throughout the
Park. The documents had recently been transferred into a common drive
whilst they were being reviewed and updated to current legislative
requirements. In essence, there was no documented Safety
Management System in operation within the Park.
1165
• The rides and attractions were being well maintained with competent
staff, however, there was no documentary evidence to support this
process.
• The Safety Unit was noted to be very operational in that most of the day
was involved in hands-on activities from conducting inspections to
providing training, with little available time for strategic development of
the Safety Management System.
• The implementation of Figtree, as a platform for risk management, was
praised as an excellent platform for managing the risks within the Park
incident reporting. However, managers were required to finalise incidents
open for their departments to ensure it reflected the current status of the
Park.
• It was noted that emergency procedures were well managed, with staff
participating in evacuation drills, attending training annually with
procedures reviewed regularly.
567. The areas for improvement were listed as follows:
1166
• Safety Management System: The SMS has not been reviewed for a long
period of time and is currently not compliant with the Harmonised
Legislation. Procedures do not clearly identify the reference against
which the document seeks compliance nor does it clearly define
responsibilities for the implementation of that procedure.
• Document Management System: There is no document management
system to manage version control, develop approval work flows etc. The
current process is to use a common drive for storing the data in Word and
Adobe Acrobat, which is inaccessible to most staff.
• Ride and Attraction Documentation: Although the rides and attractions
appear to be well inspected and maintained, there is no evidence that the
inspections comply with the manufacturer’s requirements or AS3533,
there has been no formal risk management process applied to the rides
and competencies of staff to inspect and maintain the rides has not been
demonstrated etc.
• Engineering Training Records: There is little to no evidence of
department induction, work at height, confined space training,
competency to operate high risk plant and equipment and records of
1164
Ex F(8)(1), pg. 3
1165
Ex F(8)(1), pg. 3
1166
Ex F(8)(1), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 149 of 274
licenses etc. With the appointment of the new Engineering Manager and
administration staff member, the program is being resurrected and will
require significant resources to bring it back to compliant levels.
• Lock-out Tag-out Procedure (LOTO): The blue tag system allows
maintenance staff to work on equipment while it is operational without a
competent person at the control panel. All rides and attractions must have
the controls locked out to prevent the inadvertent starting of that
equipment while persons are in the ride envelope which will require a
complete review of the LOTO procedure and some modification to Ride
Operator consoles.
• Job descriptions/KPI’s: Significant review of job descriptions will be
required to ensure that the essential and desirable skills of that role have
been clearly identified, and the quantifiable safety responsibilities where
applicable are detailed for the role. Performance evaluation reviews are
ad hoc and safety key performance indicators are in their infancy for
General Managers. Hence, there is no clear understanding of who is
responsible for certain safety activities and no measure of performance
to those activities.
• Consultation: This is in regards to the purchasing of new attractions, the
purchasing of plant and chemicals within departments whereby there is
no formal process to ensure stakeholder involvement.
• Electrical compliance: Compliance with the Electrical Safety Regulation
2002 is being readdressed with safety switches being performance tested
after a five year absence from testing, and electrical equipment in
Maintenance Workshops scheduled for testing and tagging after not
having been tested since 2011.
568. In summary, the audit of the Safety Management System at Dreamworld
received a final score of 41.7%, which was low and predominantly due to the lack
of an up-to-date, easily accessible document controlled Safety Management
System that sets the framework for compliance to the legislative
requirements.
1167
A score of 75% is seen as fully compliant with such
requirements. At inquest, Mr. Randall noted that a compliance mark about 75%
was required under the audit tool for self-insurance.
1168
569. In relation to the comment made in the Executive Summary as to the fact that
there was no evidence that the rides complied with AS-3533 and no formal risk
management process applied to the rides, Mr. Randall told OIR investigators that
the reason he had included this was that it had become evident after the first
audit that there were no records for the amusement rides to be able to
demonstrate compliance with the manufacturer’s requirements or AS3533.
1169
In
July 2015, Mr. Randall recommended that a junior engineer be appointed to
complete a full ride audit every two months, which could be verified by an
external specialists.
1170
1167
Ex F(8)(1), pg. 5
1168
T24-15, lines 1-10
1169
Ex C5(35)(b), pg. 18
1170
Ex C5(35)(b), pg. 18
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 150 of 274
2014 Audit
570. Between 24 and 28 February 2014, DRA attended Dreamworld to conduct a
Management Systems Audit, using the National Self Insurers Audit Tool V2.1.
1171
The audit was conducted in conjunction with the Safety Department, and
included interviews with various Departmental Managers and Supervisors.
571. The following comments were made in the Executive Summary as to the findings
of the audit:
• The current Safety Management System was out of date, fragmented and
requiring significant resources to bring it up to current legislative
standards. The previous year had been spent developing a platform to
house and manage the Safety Management System documents along
with the purchase of a product, which can be used as a guide in the
development of the procedures. It was noted that significant resources
will be required to update and review all the policies and procedures and
transfer them into the Oracle Document Management System.
572. The strengths identified during the audit were listed as follows:
• Training;
• Electrical - Significant work had been undertaken by the Engineering
Department, and electrical tagging and testing had been systemised,
although non-compliances were identified within the Audit;
• Contractor Management – Significant work had been undertaken to
ensure all contractors engaged onsite have been inducted and have
provided details of their relevant insurance policies and safe work
methods before commencing work;
• Incident/Hazard Reporting – Figtree usage is improving across all
departments, which is now providing useful data for quarterly reports;
• Consultation – Significant work had been undertaken to improve
consultation across the Park with regard to the introduction of new
equipment, attractions and procedures. Change management
documentation is in the process of implementation;
• Job Descriptions/KPI’s – A review of job descriptions indicated that
essential and desirable skills of the role have been clearly identified, and
management staff now have a safety KPI linked to their pay.
573. The areas for improvement were similar to that stated in the 2013 audit, and
included the following:
1172
• Safety Management System – Safety Direct is now available in Oracle
and includes a safety management plan for its effective implementation.
Significant work will be required to implement the SMS, which will require
the Executive Leadership Team to determine which procedures have
1171
Ex F(8)(2), pg. 3
1172
Ex F(8)(2), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 151 of 274
priority for implementation.
• Rides and Attraction Documentation – Although significant work had
been undertaken by the Engineering Manager to collate all the
documentation for rides in an electronic format and make it available for
staff, the following issues were still found to have existed:
1173
Inspection checklists for each ride have not been formally
compared to the manufacturers requirements, and during
the audit, where differences have been noted there is no
evidence to support the change in inspection.
Standard operating procedures for daily and weekly
inspections have not yet been developed and hence there
is no consistency in the inspections performed by
maintenance staff.
There are limited records of competency assessments of
engineering staff to perform the daily and weekly
inspections, and what does exist is an assessment against
an inspection sheet rather than a standard operating
procedure.
The existing lock-out tag-out system still relies on an
administrative control i.e. tag, to prevent the operation of
a ride whilst a maintainer is in the ride envelope.
• Corporate Risk Management – Consideration of generating a corporate
register which records all issues raised through internal and external
audits. A single register will enable management to prioritise the risks and
allocate resources accordingly.
• Training Plan/Records – A majority of the training was undertaken within
departments and training records held at this level. There is no electronic
Learning Management System which would enable the recording of
training against each individual.
• Hazardous Chemical Management – Without purchasing controls on
chemicals, chemical registers are out-of-date which places the
organisation at risk.
• Lock-out Tag-out: This system needed to be revised as a matter of priority
to ensure that it achieves the single aim of ensuring staff entering the ride
envelope cannot be struck by a ride.
574. In summary, the audit on this occasion had a final score of 46.1%, which was
noted to only be a ‘marginal improvement’ on that achieved in 2013.
1174
It was
suggested that the recommendations of this report be placed into a Corporate
Risk Register, prioritised and allocated to Managers for implementation,
following which significant improvements will be made.
1175
1173
Ex F(8)(2), pg. 4
1174
Ex F(8)(2), pg. 6
1175
Ex F(8)(2), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 152 of 274

575. Mr. Randall claims that the 46.1% score obtained on this occasion following the
audit surprised him as he had expected a far greater improvement in the 12
months with the implementation of the recommendations made in 2013.
1176
It
was his understanding that this limited improvement was due to resources within
the Safety Department at Dreamworld.
1177
Mr. Randall expressed concern to the
Board as to the lack of improvement, following which additional staff were
added.
1178
Consultancy Visits 2014
576. In late 2014, DRA conducted their first consultancy visit at Dreamworld whereby
document management systems and document control structures were
discussed with Management before a meeting held with the Safety Executive
Committee.
1179
It was determined that the executive team would determine a
suitable document management system for the storage of all Dreamworld
documentation, and the Safety Department would be in charge of managing the
updating of the procedures.
2015 Audit
577. On 13 and 14 July 2015, Mr. Randall from DRA conducted a Safety Management
Systems Audit on Dreamworld, using the National Self Insurers Audit Tool. Given
the limited timeframe, the audit focused on those criteria that did not gain a score
of 3.0 in the last audit conducted in February 2014.
1180
578. It was noted in the Executive Summary that significant improvements had been
made with the implementation of the Safety Direct Management System, Liferay,
a new LMS and the expansion of MEX ops.
1181
These introductions would allow
for significant improvements in the automation of the safety management
functions over the next 12 months to two years. Furthermore, a restructure of the
Safety Unit at Dreamworld has enhanced services provided to the Departments.
The Engineering Department had also made significant inroads into upskilling
their staff and ensuring that training records were available for the inspection of
rides. Full risk management reviews of the major attractions had also been
commenced.
579. In addition to the strengths listed in the 2014 audit, the following further positives
were also noted:
1182
• Safety Management System – now readily available online to all staff.
• Risk Management – Quarterly inspections of departments, the
development of corrective action registers for each department along with
the development of a static risk register for each department has
improved the risk management practices across the property.
• First aid management – is now approaching best practice with excellent
facilities, highly trained staff and a comprehensive First Aid Procedures
1176
Ex C5(35)(b), pg. 14
1177
Ex C5(35)(b), pg. 15
1178
Ex C5(35)(b), pg. 15
1179
Ex F(8)(4); Ex F(8)(8); Ex F(8)(11)
1180
Ex F(8)(3), pg. 2
1181
Ex F(8)(3), pg. 2
1182
Ex F(8)(3), pg. 2 & 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 153 of 274
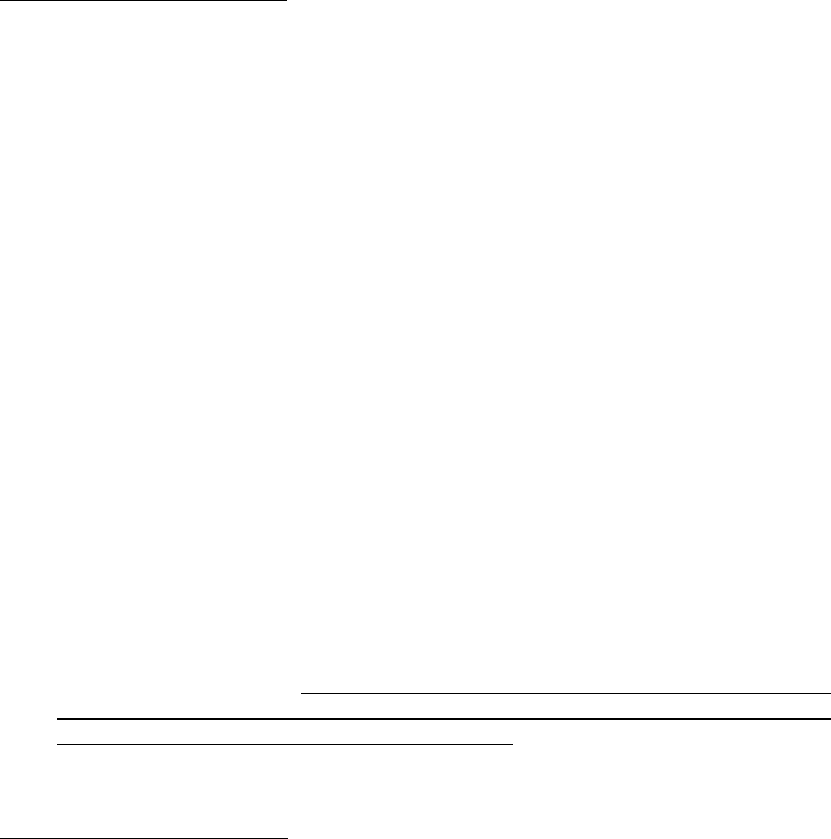
Manual.
580. The areas for improvement largely mirrored that of the 2014 audit with the
removal of the Safety Management System and Ride documentation. The
additional area of concern was Emergency Management, which it was noted
were out-of-date and did not accurately reflect the procedures undertaken within
the Park for emergency situations.
1183
581. In summary, the audit in 2015, yielded a final score of 61.6%, which was a
significant improvement from the previous year.
1184
It was noted that with the
imminent implementation of LMS, Liferay and the enhancement of MEX ops,
significant automation of the safety functions could be achieved making the SMS
resilient to change in staff. Furthermore, with Departmental Managers having
clearly defined responsibilities, which are documented in the annual Safety Plan,
safety will become a standard part of business rather than an ‘add on’.
1185
Consultancy Visit - April 2015
582. In April 2015, a further consultancy visit took place whereby the status of the
recommendations from the audit conducted in January 2015 was reviewed with
the continuous improvements within the Engineering Department and contract
management noted.
1186
Further action in relation to the Emergency Procedures
for rides were identified, which primarily involved the development of suitable
picture based procedures to deal with all emergencies.
583. In relation to the Engineering Department, the following was noted:
1187
• A review of work undertaken by the engineer on the documentation for
the Wipeout and Buzz Saw clearly showed that significant work had been
completed to ensure the rides could be inspected systematically to best
practice standards based on manufacturers, Australian standards, ride
bulletins and experience. This process was to continue with all high risk
thrill rides being completed as a matter of priority, with one ride being
completed per month.
• On the daily and weekly inspection sheets, the types of lubricants to be
used for greasing to be included, as well as the tools required to complete
the inspection.
• Supervisors to ensure all maintenance staff have completed the
competency to operate the rides, as daily and weekly inspection
procedures are developed.
584. DRA recommended that ‘management consider engaging an external consultant
to manage the AS3533 compliance issue associated with the introduction of new
rides as part of the design registration process’.
1188
585. In terms of change management, DRA recommended that consideration be
1183
Ex F(8)(3), pg. 2
1184
Ex F(8)(3), pg. 2
1185
Ex F(8)(3), pg. 2
1186
Ex F(8)(5)
1187
Ex F(8)(5), pg. 5 & 6
1188
Ex F(8)(5), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 154 of 274

given to rotating Ride Operators during a shift, to ensure they remain vigilant
when undertaking their functions.
1189
Consultancy Visit - December 2015
586. In December 2015, a further consultancy visit took place where the progress of
the implementation of the recommendations from April and July 2015 were
considered.
1190
587. In terms of actions undertaken, the report highlighted the following:
1191
• Picture based emergency procedures had been developed for the five
major rides by the Engineering Department.
• A lubricant register for each ride had been developed.
• A change management form in Safety Direct was available for use by
staff.
• All corrective actions identified in the Safety Management System Audit
conducted in July 2015 have been included in a corrective action register.
• Engineering were continuing to make progress with improving the
documentation and systems of work related to ride operation and
maintenance, with items that remained un-actioned detailed in an action
plan.
588. In addition to a range of recommendations made about issues such as
Hazardous Chemical Management, Emergency Procedures, Contractor
Management and the Safety Management Plan, DRA also outlined the
requirements of annual ride inspections per the OIR Regulations.
1192
The
requirements of Form 8 and ss. 266 and 267 of the Act were explained. It was
recommended that the following take place:
1193
• Consider re-assigning the task of annual registration to the Engineering
Department given they are deemed the person in control of the plant.
• Ensure an annual statement is obtained from either an external RPEQ
Engineer or an internal competent staff member to state that the ride is
safe for operation, the completed National Audit Tool for Amusement
Devices would be sufficient to satisfy this requirement.
Consultancy Visit - April 2016
589. In April 2016, a further consultancy visit took place whereby a review of the
progress of previous recommendations from prior consultancy visits and audits
were considered.
1194
1189
Ex F(8)(5), pg. 6
1190
Ex F(8)(9)
1191
Ex F(8)(9), pg. 4
1192
Ex F(8)(9), pg. 8
1193
Ex F(8)(9), pg. 8 & 9
1194
Ex F(8)(6)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 155 of 274

590. The report prepared noted the following items of significance:
• Work had been ongoing in updating emergency procedures and ensuring
Warden’s boxes in each of the zones were fitted with suitable equipment.
• The annual inspection requirements for each of the attractions will now
be completed by an external provider.
591. It was noted that ‘given the transition in the Safety Managers role, it is
understandable that many of the issues raised in the December report are yet to
be formally addressed.’
1195
Furthermore, the corrective action register was said
to have listed all of the recommendations from previous audits, however, should
be extended to include all from external/internal reports to ensure that there is a
current log of risks available for review.
1196
592. Relevant issues considered with further recommendations made were identified
as follows:
1197
• The corrective action register in Safety Direct to be used as the major tool
for monitoring the implementation of the recommendations for those
elements in the audit that were identified as below a score of 3.0.
• Locate resources within each department to ensure the requirements of
the chemical management system are implemented prior to the
November audit.
• In relation to emergency procedures, conduct a desk-top and other drills
of key emergency procedures prior to the November audit with evidence
of the drill outcomes available.
• The need for a comprehensive training needs analysis for each
department, as this was one of the major non-conformances in all of the
previous audits.
593. In April 2016, DRA were also requested to conduct a review of the Log Ride
incident where a male patron was injured falling from the ride.
1198
The purpose
of the review was to provide a further opinion as to the investigation process and
findings to date, to compliment that already undertaken internally and by the
Regulator, in order to ensure the safe reopening of the ride.
594. In addition to the further controls recommended for the ride, which included extra
CCTV cameras and automatic audio safety warnings at critical points on the ride,
DRA suggested that a ‘full documented risk assessment of the ride be
conducted’, which was intended to provide evidence of Dreamworld’s primary
duty of care, that both the current and proposed risk control measures are
reasonable and have a timeframe for implementation which is reflective of the
risk posed.
1199
1195
Ex F(8)(6), pg. 4
1196
Ex F(8)(6), pg. 4
1197
Ex F(8)(6), pg. 4 & 5
1198
Ex F(8)(15)
1199
Ex F(8)(15), pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 156 of 274
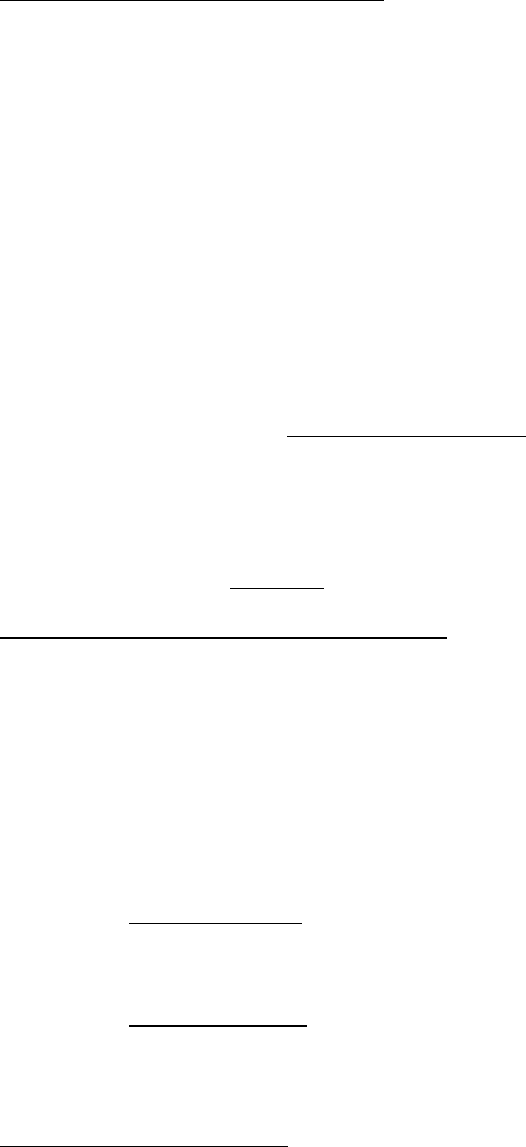
Dreamworld’s Response to DRA Audits
595. Following each audit and consultancy visit, a final report was produced by DRA,
which would outline the findings made and recommendations.
1200
Mr. Randall
presented his findings for each of the DRA reports to the Ardent Leisure Board
by way of an Ardent Safety Committee meeting.
1201
To assist in the ongoing
implementation of the recommendations following the audits, a Risk Register and
Action Log was developed in December 2014, which was to be maintained by
Dreamworld Safety staff.
1202
596. It appears that the Safety Department were the custodian of the DRA audit
reports. The recommendations, however, were shared with various
Departmental Managers, including the Operations Department, so that corrective
actions could be addressed.
1203
597. According to Mr. Hutchings, Mr. Davidson was aware of the DRA findings and
recommendations.
1204
He notes that not all of the recommendations made were
implemented as it was ‘purely a constraint issue’.
1205
Regardless, it is clear that
with the improved auditing scores, gradual improvements were being made by
Dreamworld.
598. During the inquest, Mr. Randall stated that, ‘I firmly believe had we gone through
that process and had another, you know, three months, that some of these issues
that have caused this event would have been identified and rectified’.
1206
Dreamworld Safety Auditing Strategy FY15
1207
599. In May 2014, Mr. Deaves in consultation with Mr. Hutchings drafted a
Dreamworld Safety Auditing Strategy for 2015.
1208
This document notes that the
annual DRA audits, which is described as providing a comparison between the
safety management systems as against the national self-assessment audit tool,
have highlighted the absence of a formalised document control system.
1209
Whilst some improvements were noted in the 2013 and 2014, in order to improve
the scores of the audits, it was proposed that the following strategies be
implemented:
1210
• Auditing strategy: It was proposed that the money spend on auditing
($14,000) be used to engage DRA as a consultant to assist in completing
the work required, as identified by previous audits.
• Document control: It was noted that the Ardent IT Department had been
working on a group wide document control solution for some years.
Recently, a small module was made available to the Dreamworld Safety
Department in order to deposit and manage Park wide safety policies and
procedures. In order for the system to be complete, it was noted that a
1200
Ex C4(16), pg. 2
1201
Ex C8(10), pg. 66; Ex C4(16), pg. 2
1202
Ex C4(16), pg. 2
1203
Ex B3C(50), pg. 44 & 45
1204
Ex C8(10), pg. 60
1205
Ex C8(10), pg. 60
1206
T24-69, lines 5-15
1207
Ex B3C(46), pg. 102
1208
Ex C8(26)(b); Ex B3C(46), pg. 102 & 103
1209
Ex B3C(46), pg. 102
1210
Ex B3C(46), pg. 102
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 157 of 274

module was required for each major Department.
• Engineering: Whilst it was noted that the preventative maintenance,
inspection and training regimes had evolved over the operating life of the
Ardent Theme Park Division, there was no formal evidence of compliance
with the current system. As such, it was suggested that the following
points for compliance be reviewed:
o OEM Inspection and servicing requirements, including safety
alerts and service bulletins.
o Applicable Australian Standards compliance.
o Queensland Regulation compliance assessed against the
National audit tool.
o Consolidation of historic information from JAK, DRA and internal
audits. It was noted that this review would likely ‘detail a large
amount of recommendations that are currently not performed or
partially performed’.
1211
It was recommended that a junior
engineer be recruited to undertake the following tasks:
1212
- Review each device and consolidate the information in
the document control centre for retrieval by all relevant
staff.
- Assess the relevance of each task, negotiate with OEM
on variations.
- Manage change documentation.
- Develop training plans and assessment tools based on
the final service requirements.
600. Upon completion of the proposed review, it was further submitted that the
process and inspection regime be independently verified for compliance, as this
would provide a ‘base line for any engineer’s inspection to work from which is
not an annual requirement of the Queensland regulation’.
1213
601. It appears that in April 2014, steps were taken to have the above proposal
discussed between Mr. Deaves, Mr. Hutchings and Mr. Davidson.
1214
According
to Mr. Deaves, this meeting took place whereby resourcing to assist Engineering
in carrying out further audits on amusement rides was discussed following the
identification of gaps in the safety systems management.
1215
This proposal was
agreed to and further administrative support, as well as junior engineer, Mr. Cruz
were subsequently hired to undertake the tasks as listed.
1216
1211
Ex B3C(46), pg. 102
1212
Ex B3C(46), pg. 103
1213
Ex B3C(46), pg. 103
1214
Ex B3C(46), pg. 104
1215
Ex C8(5), pg. 6 & 7
1216
Ex C8(5), pg. 7 -14
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 158 of 274

CHANGES AT DREAMWORLD FOLLOWING THE INCIDENT
602. Material provided by Ardent Leisure during the inquest proceeding notes that a
number of significant changes were made at Dreamworld following the tragic
incident. The need for such changes to be made were expressed by Mr.
Hutchings during an Ardent Leisure Board meeting, which took place on 7
December 2016, where he ‘expressed his desire to replace human behavioural
controls with engineering or monitored solutions’.
1217
He further highlighted his
intention to improve hazard identification and associated documentation. Below
is a summary of the review, auditing and changes implemented since this tragic
incident.
603. Shortly following the incident, Pitt & Sherry Operations Pty Ltd, an Australian
Engineering firm with expertise in amusement devices and moving plant, were
engaged by Ardent Leisure to inspect and assess the Amusement Devices and
relevant associated components at Dreamworld and WhiteWater World.
1218
The
scope of the work was to:
1219
• Conduct a general safety review, utilising a team of engineers (Structural,
Mechanical and Electrical and Control) including providing signoffs as
part of a 3-Tier Review; and
• Conduct Annual Inspections on all Amusement Devices.
604. Following the above inspections, Pitt & Sherry issued an Annual Inspection
Certification Letter for those devices found to comply with s.241 of the
Regulations and AS3533.3. Corrective actions identified were outlined in reports
provided for each ride.
605. In addition, Leisure Technical Consultants (LTC) were also engaged by Ardent
Leisure to conduct its own Functional Tests and Peer Review of Pitt & Sherry’s
findings. These findings were outlined in detailed reports, which contained 160
recommendations and observations as to Corrective Actions.
1220
LTC found that
the inspections conducted by Pitt & Sherry had been to a high standard.
1221
606. The Engineering Department worked closely with Pitt & Sherry and LTC to
facilitate their inspection of rides at the Park, and to complete remedial works on
the matters identified by the Consultants.
1222
607. In 2017, Pitt & Sherry were engaged by Ardent Leisure to conduct additional
inspections and audits at Dreamworld and WhiteWater World to assess the work
conducted in response to the Corrective Actions, as implemented by Dreamworld
Technical Services.
1223
608. In 2018, Ardent Leisure engaged Chapalex Pty Ltd, a company specializing in
the integration of safety and risk management principles and practices into
existing operational frameworks, to assist in gaining ‘an understanding of the
current status of work health and safety operating systems, policies and practices
1217
Ex C8(23)(f), pg. 1
1218
Ex F4(1)
1219
Ex F4(1), pg. 4
1220
Ex F4(1), pg. 20
1221
Ex F4(4), pg. 7
1222
Ex F11, [17]
1223
Ex F4(1), pg. 26
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 159 of 274
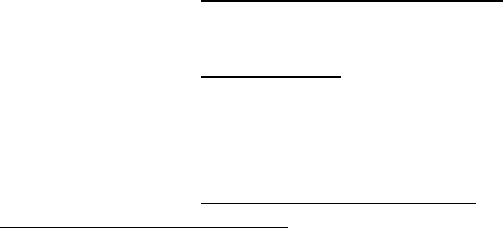
at Dreamworld and WhiteWater World’.
1224
Chapalex agreed to allow the
Director, Mr. Phil Tanner, to undertake the role of Director of Safety at
Dreamworld, WhiteWater World and Skypoint from 1 July 2018.
1225
Mr. Tanner
was responsible for identifying opportunities to enhance the Park’s existing WHS
practices.
1226
609. Whilst not exhaustive, other pertinent changes made throughout the Theme Park
following the incident, include the following:
• Dreamworld staff were required to review applicable operating
procedures for rides and attractions at the Park, in consultation with Pitt
& Sherry to ensure that any modifications arising out of the reviews
undertaken were incorporated into the Operating Procedures.
1227
• Refresher training was provided to Ride Operators before the rides at the
Park were reopened to the public.
1228
• SP Solutions, external consultants with expertise in assisting companies
identify, assess and control risks, were engaged to conduct workshops
with Dreamworld staff and assist them in conducting risk assessments on
rides at the Park.
1229
.
• A Memorandum Creation Procedure was introduced in the Operations
Department, which requires consultation with the Attractions and
Entertainment Manager, as well as a final sign off by either the Attractions
Manager or General Manager of Park Operations, before it is
disseminated to staff.
1230
According to Mr. Fyfe, following the incident,
there is now a focus on ‘risk assessment’ and widespread consultation
when creating memorandums.
1231
• The configuration and members of the Safety Department were
significantly changed to include an Engineering Safety Advisor, Safety
Training Advisor, Environment Advisor and a Senior Safety Advisor.
1232
• A number of safety initiatives were also introduced at the Park, including:
o Emergency management plans - sets out the Park-wide response
to various emergency situations, including for particular rides.
1233
o Scenario drills – a program was developed to be conducted on
rides at the Park in consultation with Pitt & Sherry.
1234
Engagement was also commenced with the Queensland Fire and
Emergency Services, QPS and OIR.
o Park-wide Evacuation Drills – introduced to provide training to
1224
Ex F11, [4] & [6]
1225
Ex F11, [1]
1226
Ex F11, [7]
1227
Ex F11, [17]
1228
Ibid.
1229
Ibid.
1230
Ex C8(6), pg. 16 & 17
1231
Ex C8(6), pg. 29
1232
Ex C6(51), [39]
1233
Ex F11, [20]
1234
Ex F11, [26]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 160 of 274

staff as to how to proactively respond to emergency situations.
1235
o Incident Controller – a revised incident controller structure was
implemented to provide situational leadership.
1236
o Park-wide audio system – enable more effective coordination of
evacuation and personnel management during an emergency.
1237
• A review of the health care able to be provided by the Park Health Facility
was undertaken with necessary improvements actioned to achieve best
practice.
1238
• An analysis was undertaken as to the scoping and resourcing
requirements of establishing an in-house Park training academy to
canvas the operation of the Parks, with accredited training programs
recognised Australia wide.
1239
• A review was undertaken of the Ride Induction Training Program
provided to new employees with improvements made.
1240
• Implementation of new data management and IT Systems at the Park,
which includes a new safety management system that consolidates
previous systems into one single platform to control safety risks. A new
document management system was also introduced, which efficiently
and effectively tracks, manages and stores documents across all
Departments.
1241
610. Ardent Leisure have also developed a hazard and operability study (HAZOP)
model for identifying and evaluating issues, which may present to staff, guests
and rides at the Park. This risk assessment tool is intended to be the basis for
any changes to the Regulatory regime in place in Queensland in response to this
incident.
AMUSEMENT PARK REGULATION IN QUEENSLAND
611. The responsibilities of the Regulator for Amusement Park rides in Queensland is
identified in the Work Health and Safety Act 2011 (WHS Act) and Work Health
and Safety Regulation 2011(the Regulations), which commenced on 1 January
2012.
1242
The implementation of this legislation gave effect to the national
framework of model work, health and safety laws under the agreement of the
Inter-Governmental Agreement for Regulatory and Operational Reform in
Occupational Health and Safety.
1243
OIR are also responsible for administering
the Electrical Safety Act 2001 and the Electrical Safety Regulation 2013 in
conjunction with the Electrical Safety Office (ESO).
1244
1235
Ex F11, [32] – [36]
1236
Ex F11, [37] – [39]
1237
Ex F11, [40] – [45]
1238
Ex F11, [48] & [49]
1239
Ex F11, [51] – [58]
1240
Ex F11, [59] – [61]
1241
Ex F11, [69] – [78]
1242
Ex F2A(3)
1243
Ex F2A(3) [2]
1244
Ex F2A(3) [3]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 161 of 274
612. In administering this legislation, OIR is responsible for ‘monitoring and enforcing
the primary objectives of the WHS Act and ES Act to protect workers and other
persons from harm to their health, safety and welfare through the elimination and
minimisation of risk arising from work or from particular types of substance and
plant’.
1245
Brief History of WHS Legislation - Past Decade
613. In 2011, the Workplace Health and Safety Act 1995 and the Workplace Health
and Safety Regulation 2008 was repealed. The previous regulatory regime
included a number of requirements relevant to amusement park rides in
Queensland, such as general requirements for registrable plant and registrable
plant design.
1246
614. Plant design registration has been a feature of WHS legislation in Queensland
for many years. It was intended to be a mechanism to ensure that the design of
an item of plant had a verification statement confirming that it meet the technical
standards and engineering principles appropriate for the plant.
1247
615. In 2011, a nationally recognised set of model occupational health and safety laws
were made to harmonise the different Australian jurisdictions. This model was
adopted in Queensland in 2011, and commenced on 1 January 2012.
616. When Queensland adopted the model WHS laws in January 2012, it delayed the
commencement of the five yearly renewal cycle for registration of items of plant
and preserved the existing annual registration cycle due to operational and
systems considerations. This is further explored below.
2011 WHS Act – Regulator Responsibilities
617. The WHS Act imposes a range of duties on persons and owners of plant
(amusement devices), which are relevant to the design, maintenance and
provision of safe plant. In discharging these responsibilities, OIR, as the
Regulator of Amusement Parks, have three distinct functions:
1248
• Administrative;
• Compliance monitoring and engagement; and
• Enforcement and sanctions.
Administrative Functions as of October 2016
618. The statutory regime administered under OIR includes requirements for plant
registration and plant design registration, with certain classes of amusement
devices requiring registration design and item registration. This has been a
feature of the legislation in Queensland for many years, and was intended to
check that the design of an item of plant had a complied with the published
technical standards and engineering principles applicable to the plant.
1245
Ex F2A(3) [4]
1246
Ex F2A(3) [49] & [50]
1247
Ex F9C(1)(a), [9]
1248
Ex F2A(3) [6]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 162 of 274

Plant Design Registration
619. Pursuant to s.259 of the Regulations, registration for plant design for a device is
a one-off process, unless the design is altered or modified.
1249
Plant design
registration requirements are generally consistent across all Australian
jurisdictions.
620. There are currently 15 types of plant requiring design registration, which includes
items such as amusement devices, cranes, lifts and pressure equipment. In
particular, design registration for amusement devices is covered by s.2.1 of
AS3533 – Amusement Rides and Devices.
621. The registration process consists of verification through several steps:
1250
• Initial application consisting of design plans, technical standards and the
assessment carried out by an independent competent person (a
registered professional Engineer).
• Verification by the OIR Engineering Unit, which may include additional
requests for information to address discrepancies.
• Should the Engineering unit remain concerned, an audit against the
design and application is undertaken to ensure requirements are met.
• Design registration is only certified if the plants design satisfies this
process and registration fees are paid.
622. Under the Regulations, the design verifier must be a competent person and must
not have been involved in the production of the design or engaged by the design
company at the time it was developed. A competent person for design
verification, under s.252 of the Regulations, means a person who has the skills,
qualifications, competence and experience to design the plant or verify the
design. For Queensland, this means a suitably qualified and experienced RPEQ.
623. Items of plant requiring design registration under s.243 the Regulations are
coordinated by the OIR Engineering Services Unit. When Theme Park Operators
are planning to install new amusement devices, OIR’s Chief Safety Engineer will
provide input to ensure health and safety legislation and Australian Standard
requirements are met.
1251
624. The OIR Engineering Services Unit provides advice and strategic leadership on
plant-related safety matters under the WHS legislation, as administered by OIR.
This includes providing engineering support to the OIR investigation team when
the incidents they are investigating involve the operation of plant, which include
amusement devices.
1252
Plant Registration Renewal
625. Separate to the design registration of a piece of plant, items of plant are then
required to have their registration renewed annually. The OIR Licensing and
1249
Ex F9C(1)(a), [11]
1250
Ex F2A(3) [16]
1251
Ex F2A(3) [14] – [15]
1252
Ex C4(8), [3]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 163 of 274
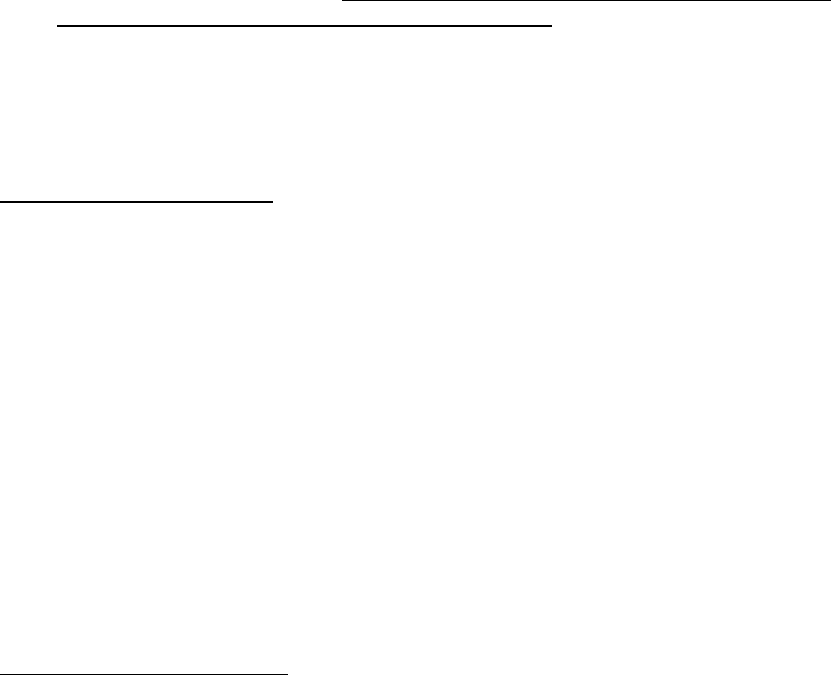
Advisory Services unit co-ordinates the items of plant requiring registration under
s.246 of the Regulations. The registration involves a yearly application for plant
registration, either lodged online or via a hardcopy using the requisite application
form.
1253
A processing fee is applicable, following which a certificate of
registration is provided.
626. For registration renewal of plant, the Regulator is not required to inspect the plant
or verify any element of its safety as part of the process. Accordingly, the
requirement to register items of plant is ‘an administrative transaction between
the person with management or control of the plant (e.g. the plant owner) and
the regulator’.
1254
The duty to inspect the plant rests with the plant owner and the
registered professional engineer.
627. The registration of plant items provides OIR with a database, which records all
of the location and owner details of plant items in the event that this information
needs to be accessed following a safety concern.
1255
628. For operational and OIR reasons, at the time of the national harmonisation in the
work health and safety laws in 2012, Queensland did not move to the five yearly
renewal cycle for plant registration provided under the model WHS laws.
1256
It
seems that the primary reason for the delay in Queensland moving to the five
year renewal period was the ‘significant upgrade it would require to the Office of
Industrial Relation’s information technology system’.
1257
629. Current plant item registration requirements continue to differ amongst the States
with annual registration renewal required in Queensland and NSW, with five year
renewal for Tasmania, South Australia, Northern Territory, the ACT and the
Commonwealth.
1258
Safety Regulations for Plant
630. The regulation of plant safety, which is separate to the requirements for plant
design and item registration, has significantly changed in Queensland over the
past decade.
631. Prior to the implementation of the national model WHS laws, there were general
workplace health and safety obligations in the Workplace Health and Safety Act
1995 (repealed) on persons conducting business or undertaking; designers,
manufacturers and suppliers of plant; erectors and installers of plant; owners of
plant and persons in control of fixtures, fittings of plant in workplace areas.
1259
Generally, the obligations included providing and maintaining safe plant,
ensuring the safe design of plant and to ensure the plant is maintained in a
condition that ensures the plant is safe. The supporting Workplace Health and
Safety Regulation 2008 (repealed) was limited to control of high risk plant by
way of registration of plant items and plant designs based on the list of plant in
the National Standard for Plant. No other specific safety regulations for plant
existed at the time.
1260
1253
Ex F2A(3) [8]
1254
Ex F9C(1)(a), [23]
1255
Ex F9C(1)(a), [24]
1256
Ex F2A(3) [9]
1257
Ex F9C(1)(a), [18]
1258
Ex F9C(1)(a), [22]
1259
Ex F9C(1)(a), [26]
1260
Ex F9C(1)(a), [28]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 164 of 274

632. Practical advice on managing risks were provided in the former Plant Code for
Practice, which included guidance on inspection programs, frequency and
documentation.
1261
The former Code stated that plant should be serviced and
maintained in accordance with the manufacturer’s specifications if applicable,
and if not, in accordance with other proven and tested procedures.
633. The introduction of the national model WHS laws in Queensland in January 2012,
provided more comprehensive regulatory provisions specifically related to the
registration and maintenance of plant, including amusement devices.
634. The provisions relating to plant safety in the Regulations are contained within
ss.204-213, and generally relate to the control of risks, proper use of plant,
guarding, emergency stops and maintenance and inspection of plant.
635. Relevantly, ss. 210, 211 and 213 of the Regulations specifically state:
210 Operational controls
(1) The person with management or control of plant at a
workplace must ensure that any operator’s controls are –
(a) identified on the plant so as to indicate their nature
and function and direction of operation; and
(b) located so as to be readily and conveniently
operated by each person using the plant; and
(c) located or guarded to prevent unintentional
activation; and
(d) able to be locked into the ‘off’ position to enable
the disconnection of all motive power
Maximum penalty – 60 penalty units.
…
211 Emergency stops
(1) If plant at a workplace is designed to be operated or
attended by more than one person and more than one
emergency stop control is fitted, the person with
management or control of plant at the workplace must
ensure that the multiple emergency stop controls are of
the ‘stop and lock-off’ type so that the plant cannot be
restarted after an emergency stop control is reset.
Maximum penalty – 60 penalty units.
(2) If the design of plant at a workplace includes an
emergency stop control, the person with management or
control of the plant at the workplace must ensure that –
(a) the stop control is prominent, clearly and durably
marked and immediately accessible to each
operator of the plant; and
(b) any handle, bar or push button associated with
the stop control is coloured red; and
(c) the stop control cannot be adversely affected by
electrical or electronic circuit malfunction.
Maximum penalty – 60 penalty units.
213 Maintenance and inspection of plant
(1) The person with management or control of plant at a
workplace must ensure that the maintenance, inspection
and, if necessary testing of the plant is carried out by a
1261
Ex F9C(1)(a), [29]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 165 of 274

competent person.
Maximum penalty – 36 penalty units.
(2) The maintenance, inspection and testing must be carried
out –
(a) in accordance with the manufacturer’s
recommendations, if any; or
(b) if there are no manufacturer’s recommendations,
in accordance with the recommendations of a
competent person; or
(c) in relation to inspection, if it is not reasonably
practicable to comply with paragraph (a) or (b),
annually.
636. A ‘competent person’ for the purpose of s.213 of the Regulations is defined in
Schedule 19 as, ‘a person who has acquired through training, qualification or
experience the knowledge and skills to carry out the task’.
637. In relation to the control measures for amusement devices, ss.238-241 of the
Regulations are applicable.
638. Relevantly, ss. 238, 240 and 241 of the Regulations provide:
238 Operation of amusement devices
(1) The person with management or control of an amusement
device at a workplace must ensure that the amusement
device is operated only by a person who has been
provided with instruction and training in the proper
operation of the device.
Maximum penalty – 60 penalty units.
(2) The person with management or control of an amusement
device at a workplace must ensure that –
(a) the amusement device is checked before it is
operated on each day on which it is to be
operated; and
(b) The amusement device is operated without
passengers before it is operated with passengers
on each day on which the amusement device is to
be operated; and
(c) the daily checks and operation of the amusement
device without passengers are properly and
accurately recorded in a log book for the
amusement device.
Maximum penalty – 36 penalty units.
240 Maintenance, inspection and testing of amusement
device
(1) The person with management or control of an amusement
device at a workplace must ensure that the maintenance,
inspection and, if necessary, testing of the amusement
device is carried out –
(a) by a competent person; and
(b) in accordance with –
(i) the recommendations of the designer or
manufacturer or designer and manufacturer; or
(ii) if a maintenance manual for the amusement
device has been prepared by a competent
person, the requirements of the maintenance
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 166 of 274
manual.
Maximum penalty – 60 penalty units.
(2) A person is not a competent person to carry out a detailed
inspection of an amusement device that includes an
electrical installation unless the person is qualified, or is
assisted by a person who is qualified, to inspect electrical
installations.
241 Annual inspection of amusement device
(1) The person with management or control of an amusement
device at a workplace must ensure that a detailed
inspection of the device is carried out at least once every
12 months by a competent person.
Maximum penalty – 60 penalty units.
(2) An inspection must include the following –
(a) A check of information about the operational history of the
amusement device since the last detailed inspection;
(b) A check of the log book for the amusement device;
(c) A check that maintenance and inspections have been
undertaken under section 240;
(d) A check that any required tests have been carried out, and
that appropriate records have been maintained;
(e) A detailed inspection of the amusement device to ensure
compliance with the Act and this regulation (including a
specific inspection of the critical components of the
amusement device).
(3) The regulator may extend the date for an inspection by up to
35 days if an inspection is scheduled to coincide with the same
event each year.
(4) If the date is extended under subsection (3), the new date is
the date from which future annual inspections of the
amusement device are determined.
(5) In this section –
Competent person means a person who –
(a) In the case of an inflatable device (continuously blown)
with a platform height less than 9m- has acquired through
training, qualification or experience the knowledge and
skills to inspect the plant; or
(b) In the case of any other amusement device –
(i) Has the skills, qualifications, competence and
experience to inspect the amusement device; and
(ii) Is registered under a law that provides for the
registration of professional engineers; or
(c) Is determined by the regulator to be competent person.
(6) The regulator may, on the application of a person, make a
decision in relation to the person for the purposes of
subsection (5), definition competent person, paragraph (c) if
the regulator considers that exceptional circumstances exist.
(7) An annual inspection under an equivalent provision of a
corresponding WHS law is taken to be an annual inspection
for the purposes of this section.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 167 of 274

639. The current Regulation requires that the inspection of an amusement device
pursuant to s.240 is to be carried out by a registered professional engineer with
the appropriate skills, qualifications, competency and experience.
1262
This is a
reflection of the consensus reached during the development of the national
model WHS laws, that a competent person to inspect plant should have
academic or vocational qualifications in a relevant engineering discipline and
knowledge of technical standards.
1263
At the time, Engineers Australia
recommended that a professional engineer should be the person who is
competent to inspect plant due to the complexity and high risk nature of the
plant.
1264
Compliance Monitoring and Engagement
640. Mr. Michael Chan is the Director and Chief Safety Engineer, Engineering Unit for
OIR, a position he has held since 2004.
1265
He is a Chartered Professional
Engineer with more than 40 years’ industry experience.
1266
He is a Registered
Professional Engineer with the Board of Professional Engineers Australia. Mr.
Chan is also a member of Engineers Australia at the fellow grade and is an
Honorary Fellow of the Safety Institute of Australia.
641. As the Chief Safety Engineer, Mr. Chan is responsible for the design registration
of high risk plant and also provides technical advice to the plant item registration
function.
1267
He manages the Engineering Unit at OIR, which consists of six
Engineers.
1268
642. Recorded as assessments or advisories within the OIR case management
system (CISr), OIR undertakes compliance monitoring and engagement both
proactively and reactively.
1269
Assessments are conducted as workplace visits
by inspectors to assess compliance with the relevant legislation, and may be
planned proactively or as a response to a complaint or incident.
643. An advisory generally represents engagement activities undertaken to advise,
inform and consult with the industry.
1270
This may include planned advisory
interventions, industry forums or individual interactions between inspectors and
workplaces.
644. Since 2002, OIR have conducted 8702 assessments pertaining to Theme Parks
or amusement devices.
1271
Assessments have, on a yearly basis, increased from
547 to 697 a year (pre and post 25 October 2016).
645. A majority of these assessments were recorded as ‘proactive’ meaning that they
were not linked to an event. Before 25 October 2016, OIR proactively inspected
4074 general amusement devices, and 2779 regional shows, school fete and
festivals.
1272
‘Reactive’ assessments, which are linked to an event or complaint
prior to 25 October 2016, were carried out on 46 general amusement devices,
1262
Ex F9C(1)(a), [35]
1263
Ex F9C(1)(a), [36]
1264
Ex F9C(1)(a), [36]
1265
Ex F9C(3)(a), [1]
1266
Ex F2A(4)(5), [2]
1267
Ex F2A(4)(5), [4]
1268
Ex F9C(3)(a), [5]
1269
Ex F2A(3) [22]
1270
Ex F2A(3) [25]
1271
Ex F2A(4), pg. 1
1272
Ex F2A(4), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 168 of 274
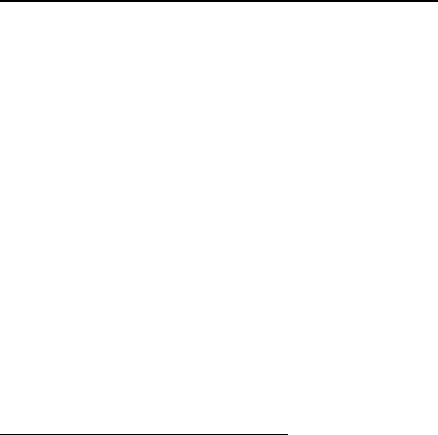
and 43 regional shows, school fete and festivals.
646. In relation to Theme Parks, 111 proactive inspections were carried out at
Dreamworld prior to 25 October 2016, with 20 reactive inspections recorded.
1273
Following the tragic incident, 134 proactive inspections were conducted at
Dreamworld, with 10 reactive inspections being carried out. Prior to 25 October
2016, 101 proactive assessments had been carried out at Movie World, with 18
reactive assessments.
1274
647. OIR have also carried out 4,830 activities pertaining to Theme Parks or
amusement devices since 2002.
1275
A majority of these (74%) were site visits
largely at regional shows, school fetes and festivals. Mr. Chan gave evidence
that a total of 128 amusement device incidents were reported in Australia from
2000 to September 2018. The analysis of data showed over 96% of those
incidents related to mobile rides; 4% related to fixed rides at Theme Parks.
648. With respect to statutory notices issued to Theme Parks or amusement devices
since 2002 up until the tragic incident, Dreamworld received 34 notices, the
highest for all of the Theme Parks, and the Ekka.
1276
Movie World and Wet N Wild
for the same period, received no notices. Following the 25 October 2016, 17
notices were served on Dreamworld, with Movie World receiving two and Wet N
Wild receiving one.
1277
649. During the inquest, Mr. Chan acknowledged that the Regulatory framework in
place at the time of the incident in relation to amusement devices effectively
expected Theme Parks to have developed and implemented safety management
systems, including maintenance, operation, training and emergency control, with
the qualified engineering and other staff to action it.
1278
Industry Guidance & Engagement Activity
650. The OIR Chief Safety Engineer and Engineering Unit members meet with the
major amusement device stakeholders (including Theme Park Operators)
approximately twice a year, or as much as may be required due to emerging
issues.
1279
An example would be a meeting which took place with staff at Movie
World in 2015, following an incident involving critical bolt failures on the Green
Lantern Ride.
1280
651. As the Chief Engineer of OIR, Mr. Chan facilitated the development of the
National Audit Tool for Amusement Devices in 2005.
1281
This Tool was intended
to enhance the consistency and transparency of audit procedures for
amusement devices, and covers all facets of maintenance and operation of
amusement devices.
1282
Mr. Chan has also provided national training sessions
on the application of the Audit Tool in Melbourne and Tasmania for WHS
Inspectors from all Australian WHS regulators. The Tool has since been adopted
1273
Ex F2A(4), pg. 1
1274
Ex F2A(4), pg. 1
1275
Ex F2A(4), pg. 2
1276
Ex F2A(4), pg. 4
1277
Ex F2A(4), pg. 4
1278
T27-14, lines 15-35
1279
Ex F2A(3) [27]
1280
Ex F2A(3) [29]
1281
Ex F9C(3)(a), [23(a)]
1282
Ex F9C(3)(a), [23(a)]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 169 of 274
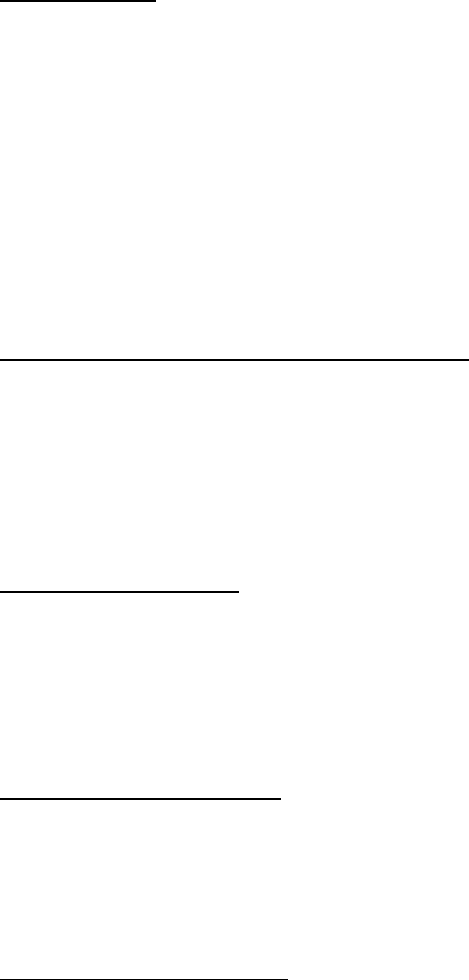
by industry and all WHS Regulators around Australia.
1283
652. Mr. Chan facilitated the development of a register as a database to record
serious incidents involving amusement devices and enforcement notices issued
by every Australian WHS Regulator on amusement devices.
1284
Since 2005,
Queensland has been the custodian of the register, which is shared with all WHS
Regulators in Australia. The data is collated and analysed annually and shared
with industry stakeholders as performance graphs.
1285
AALARA Forum
653. Since 2003, OIR have been associated with the Australian Amusement, Leisure
and Recreation Association Inc. (AALARA).
1286
As the peak national body
representing the amusement, leisure and recreation industry of Australia,
AALARA is responsible for safety, operations and management.
654. At the annual conference convened by AALARA, a regulators and stakeholders
forum chaired by OIR, to discuss safety issues affecting the amusement device
industry is conducted (e.g. the development and implementation of the National
Audit Tool for Amusement Devices). OIR works closely with AALARA to identify
safety concerns and also publishes OIR information sheets (i.e. new regulations)
and alerts (relating to amusement devices safety) on their magazines.
1287
Annual Amusement Device Stakeholders Forum
655. Commencing in 2003, OIR hosts an Annual Amusement Device Forum, which
includes Theme Park representatives, industry engineers and Interstate
Regulators.
1288
The information presented canvas various topics, including
recent safety incidents and issues with amusement devices, as well as learning
the outcomes resulting from OIR audits of amusement rides, revision of the
Australian Standards and design registration requirements.
Functional Safety Forum
656. On 9 August 2016, OIR held a Functional Safety Forum, which included Theme
Park representatives, functional safety engineers and Interstate Regulators.
1289
The forum focused on the validation procedures for safety controls systems of
plant (i.e. what the validation process includes, engineering qualifications
required, and the OIR auditing process).
Published Guidance Material
657. The following Safety Alerts have been published by OIR as a consequence of a
number of incidents involving amusements rides:
1290
• 2009 Safety Alert – Risk of being hit by moving parts of an aerial
amusement ride;
1283
Ex F9C(3)(a), [23(b)]
1284
Ex F9C(3)(a), [23(c)]
1285
Ex F9C(3)(a), [23(d)]
1286
Ex F2A(3) [30]
1287
Ex F2A(3) [32]
1288
Ex F2A(3) [33]
1289
Ex F2A(3) [34]
1290
Ex F2A(3) [35]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 170 of 274
• 2010 Safety Alert – Inflatable water balls;
• 2013 Safety Alert – Safety of amusement rides;
• 2015 Safety Alert – Re-design of rider restraint systems on amusement
devices; and
• 2015 Safety Alert – Setting up and dismantling of amusement rides.
658. Post the tragic incident, OIR have published a number of Safety and Incident
Alerts, including:
1291
• 2017 Incident Alert – Child injured after jumping castle became airborne;
• 2017 Safety Alert – Uncontrolled starting of amusement device; and
• 2018 Safety Alert – Inflatable water balls – electrical equipment near
water.
659. Provided by Safe Work Australia as information for the public, nine packages of
national guidance material to support the WHS Act 2011 and the WHS
Regulations 2011 were published on the OIR website. Of the nine packages, one
was the relevant Amusement Devices General Guide.
1292
660. For guidance on complying with obligations under the WHS Act, industry
participants may refer to the ‘Managing risks of plant in the workplace – Code of
Practice 2013’. The Code was established under s.274 of the WHS Act and may
be used in proceedings as evidence of whether or not a duty or obligation under
the Act has been complied with.
1293
The Code provides advice on the safe use of
plant and references technical standards that provide guidance on the design,
manufacture and use of certain types of plant.
1294
For amusement devices the
Code references Australian Standard AS3533.1 – 2009: Amusement Rides and
Devices for design, manufacture and use.
Enforcement & Sanctions
661. OIR enforces compliance with obligations owed under statutory regime
consistent with guidance published in the Safe Work Australia National
Compliance and Enforcement Policy.
662. Enforcement responses include the issuance of statutory notices requiring
contraventions be remedied, unsafe activities prohibited and unsafe equipment
not be used. In addition, enforcement may involve monetary fines, prosecution
of offenders through the judicial system, and revocation or alteration of licenses
issued by the regulator.
Compliance Notices
663. OIR introduced an Enforcement Note in March 2012. This instructed inspectors
1291
Ex F2A(3) [36]
1292
Ex F2A(3) [37]
1293
Ex F2A(3) [38]
1294
Ex F2A(3) [38]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 171 of 274

on the use of prohibition notices under s.195 of the Act, when resolving
contraventions relating to plant without design registration.
1295
This Note was
subsequently withdrawn in December 2015, and appropriate instructions were
issued to Inspectors supported by training in the use of the s.191 Act.
Investigations
664. Records suggest that there have been 68 comprehensive investigations
undertaken by OIR at the Theme Parks.
1296
Prosecutions
665. In 2016, a prosecution was commenced by OIR against one of the major Theme
Parks for failing to adequately assess the hazard of metal fatigue, which resulted
in one patron sustaining a minor laceration to the forehead.
1297
The company
received a penalty of $25,000, with the ride being subsequently dismantled and
removed from service.
666. In 2017, the prosecution of two matters relating to amusement rides were
decided:
1298
• The first matter involved an inflatable jumping castle, which was
dislodged. A penalty of $15,000 was imposed.
• The other matter involved a worker who was fatally injured when
dismantling an amusement ride. The company received a penalty of
$80,000.
667. From June 2011 until the fatal incident in October 2016, OIR had undertook nine
investigations involving amusement devices at shows and school fetes. As of
October 2016, eight had been finalised with one matter before the court (this has
since been finalised).
1299
668. OIR reports that seven matters were successfully prosecuted with penalties
ranging from $500 to $40,000 and four of the seven penalties were in excess of
$25,000.
1300
These prosecutions involved fracture and head injuries where the
rider was ejected from the amusement device, and in one case, a worker
sustained crush injuries when trapped by moving machinery.
Regulatory Focus on Mobile Amusement Rides
669. Prior to the tragic incident at Dreamworld in 2016, OIR’s efforts to monitor
compliance for amusement devices had been focused on amusement devices at
major agricultural shows, local carnivals and school fetes.
1301
This was due to
the mobile nature of the amusement devices at these events, in addition to their
frequent erection and dismantling. Furthermore, due to the transient nature of
the operations, it was reported to be difficult to regulate without significant
1295
Ex F2A(3) [41]
1296
Ex F2A(3) [42] & Annexure 4
1297
Ex F2A(3) [44]
1298
Ex F2A(3) [45]
1299
Ex F2A(3) [46]
1300
Ex F2A(3) [47]
1301
Ex F2A(3) [59]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 172 of 274
resource allocation.
1302
Previous Notifications Made to OIR in Relation to the TRRR by Dreamworld
670. OIR records clearly show that since the approval of the design of the TRRR on
14 August 1987, there have been no notifications made by Dreamworld as to
the ride being altered or modified as part of the design registration process.
1303
CLASS 2 RIDES INSPECTION & REGISTRATION
671. From 1999, all data records relating to plant item registration were stored by OIR
electronically in the Plant Admin System.
1304
Records relating to the TRRR since
this time confirm that the requisite renewal applications were submitted up until
2015.
1305
672. In 2015, OIR undertook a review of the processes that supported plant item
registration, as plant and financial records were identified as requiring a
significant cleanse.
1306
After the due date for the registration renewals of 31
January, there were a number of business processes to be completed before the
list of plant owners with outstanding registration renewals could be compiled.
Approximately, 2,400 renewal applications are made each year via hard copy
application forms, rather than electronically. These forms are manually entered
into the system via an online portal by a third party contractor.
1307
In February,
invoices for registration fees are issued for those with unpaid renewal
applications received between 1 December and 30 January.
673. Records suggest that in 2016, approximately 5,400 renewal forms were sent out,
which covered 30,000 pieces of plant in Queensland.
1308
Dreamworld’s Compliance with the Requirement for Renewal of Plant
Registration
674. Following the introduction of the harmonised legislation in 2012, particularly
s.241 of the Regulations, it does not appear that there was a conclusion reached
amongst Dreamworld’s management as to how compliance for the renewal of
plant registration would be achieved.
1309
Legal representatives for Ardent Leisure
advised OIR during the audit process undertaken as a result of this tragic incident
that the following ‘system’ approach was adopted to the requirement for a
‘competent person’ by Dreamworld, which encompassed the following:
1310
• Our Chief RPE Bob Tan who oversaw the system (a veteran Amusement
Park RPE of 28 years’ experience).
• Maintenance and inspection regimes based around:
o OEM recommendations
1302
Ex F2A(3) [60]
1303
Ex F9C(3)(a), [9]
1304
Ex F9C(2)(a), [3]
1305
Ex F9C(2)(a), [8]
1306
Ex F9C(2)(a), [90]
1307
Ex F9C(2)(a), [92]
1308
T27-60, lines 30-35
1309
T29-63 & 64
1310
Ex F9C(8)(6)(b), pg. 44 & 45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 173 of 274

o Trend analysis
o Industry advice
o Regulatory bulletins and documents
• A tiered approach to on-site engineering personnel undertaking
inspections (e.g. qualified trades, Team Leaders, Supervisors and Senior
Managers – all of whom are trained and assessed as competent to
undertake maintenance tasks, including annual maintenance
inspections).
• Periodic inspections intervals based on modern and more current
condition monitoring equipment for acute failure detection.
• Use of local and international audit professionals to audit all facets of:
o Management policy
o Compliance with local laws, standards, industry bulletins etc.
o Document control
o Training and competence
o Accuracy of inspections
o Change management policy
o Ride operation
o Technical integrity
• This systematic approach assists with:
o Compliance with the national regulators auditors tool
o Compliance with OEM inspections
o Fitness for purpose on all repairs/inspections
o An auditable system of non-routine defects
675. Whilst Mr. Tan was never RPEQ certified, there seems to have been an
assumption made within Dreamworld that his ‘expertise’ was sufficient to certify
the rides for annual registration renewal.
1311
In relation to the required annual
inspection of the amusement devices pursuant to the Regulation, Mr. Tan was
aware that this had to be done by a ‘competent person’, however, this did not
mean an RPEQ.
1312
After the changes to the Regulations were made in 2012,
Mr. Tan stated that despite conversations with Mr. Deaves, there was no
conclusion reached within Dreamworld as to how the annual inspections
conducted would comply with the new requirements.
1313
Accordingly, the same
process was followed through the annual and periodic inspections of the
amusement devices at Dreamworld by members of the E&T Department.
1314
He
stated during the inquest that it was not his responsibility to action the annual
renewal applications for plant registration, as this was a matter for the Safety
Department.
1315
Rather, Mr. Tan was involved in the initial registration, as this
was a more rigorous process, including close communication and coordination
with the manufacturer.
1316
1311
T22-79, lines 1-15
1312
T29-59, lines 3-36
1313
T29-64, lines 8-34
1314
T29-60 & 61
1315
T29-62, lines 18-25; 30-37; T29-86 & 87
1316
T29-62, lines 18-25
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 174 of 274

2016 Dreamworld Plant Registration
676. On 16 December 2015, plant registration renewal forms for the 2016 registration
period were sent to Ardent by a third-party processing provider.
1317
Payment for
registration of 25 amusement devices were made by Ardent on 25 February
2016, however, no completed registration applications were received.
677. On 29 July 2016, OIR sent correspondence to Dreamworld reminding them of
the requirement to renew registrable plant by a competent person, per the
requirements of the Regulation.
1318
It was noted that the application for renewal
of the amusement devices was incomplete, and all of the amusement devices at
Dreamworld were unregistered.
1319
A 28 day period from the date of the letter to
complete the registration renewal process was provided.
1320
678. On 11 August 2016, OIR Chief Engineer, Mr. Chan, with OIR Principal Advisor,
Mr. Terry O’Sullivan from the Engineering Unit, met with Mr. Deaves and Mr.
Hutchings to discuss plant item registration requirements under the Regulation
for amusement devices at Dreamworld.
1321
The purpose of the meeting was to
discuss ss.240 and 241, in particular the requirement of a competent person to
conduct annual inspections on registrable amusement devices. According to Mr.
Chan, Mr. Deaves and Mr. Hutchings explained that whilst Dreamworld had
implemented comprehensive maintenance, inspection and testing regimes on all
amusement rides at the Park, they had not engaged a registered professional
engineer to conduct annual inspections pursuant to the requirements of s.241 of
the Regulations.
1322
As such, Dreamworld were not able to register their
amusement devices.
679. Mr. Deaves and Mr. Hutchings proposed that Dreamworld be exempt from
needing to engage a registered professional engineer under s. 241(5)(b) of the
Regulation, and in lieu OIR accept that an effective ‘in house maintenance and
inspection system’ had been implemented.
1323
Mr. Chan claims that he advised
them that such a proposal was not acceptable pursuant to the Regulations, and
that the annual inspection must be performed by a suitably qualified and
experienced person and not by a ‘in-house maintenance, inspection and testing
system’.
1324
680. On behalf of Dreamworld, Mr. Thompson subsequently sent a letter to OIR via
email on 16 August 2016, stating the following:
1325
At the time of renewal, Dreamworld was of the belief that
compliance with s241 of the Regulations (2011) had been
achieved. Our continuous maintenance programme utilises in-
house professional Engineers and a range of external
professional Engineers to undertake the required annual
inspections. It was felt that this combination of engineering
expertise was sufficient to meet the definition of “competent
1317
Ex F2A(3) [10]
1318
Ex B12(17)
1319
Ex F2A(3) [11]
1320
Ex F2A(3) [11]
1321
Ex F2A(4)(5), [5]
1322
Ex F2A(4)(5), [7]
1323
Ex F2A(4)(5), [9]
1324
Ex F2A(4)(5), [10]
1325
Ex B12(17), pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 175 of 274

person”.
Since this time, we have held in-depth discussions with OIR
Chief Engineer Michael Chan regarding the definition of
“competent person”. In particular, our current combination of
Engineers lacks the registered professional engineers (RPE)
certification and hence does not meet the definition of
competent person.
We acknowledge this technical non-compliance and have been
working quickly to identify an appropriate RPE who can
undertake the necessary inspections and sign-off. Our RPE can
commence the inspections in early September and have them
concluded by the end of September (there are some 35
amusement devices in the Dreamworld fleet).
Accordingly, we would respectfully ask for an extension of time
to undertaken these assessments in order to comply as quickly
as possible with s.241. In the meantime, our continuous
maintenance programme provides many layers of safety
inspection to ensure the on-going safety of all patrons.
…
681. During the inquest, Mr. Thompson claimed that he had been provided with the
initial correspondence from OIR by Mr. Deaves. There was some subsequent
discussion between himself, Mr. Deaves and Mr. Hutchings as to which
Department within Dreamworld was actually responsible for ensuring the plant
remained registered.
1326
In relation to the letter that was sent to OIR under Mr.
Thompson’s hand requesting an extension, he claims that Mr. Hutchings had in
fact drafted that letter following discussions about the registration requirements
with Mr. Deaves.
1327
682. Following receipt of the request for an extension, Mr. Chan discussed the matter
with Ms. Johanna Sutherland from the Licensing and Advisory Service Unit,
OIR.
1328
He recommended that the extension be granted on the basis that ‘on
my knowledge of Dreamworld’s maintenance, inspection and testing regime and
that a delay of a few months for a professional engineer to progressively conduct
annual inspections will not introduce significant risks to Dreamworld’s continued
operation’.
1329
During the inquest, Mr. Chan clarified that whilst he did not have
detailed knowledge of the maintenance of individual rides at Dreamworld, he had
previously had discussions with Mr. Deaves, with whom he had a long standing
professional relationship, about the existence of their inspection and testing
program, and this was the basis of his recommendation.
1330
683. Dreamworld were subsequently granted an extension until 30 September 2016,
to inspect and assess their plant items for the purpose of the registration
renewal.
1331
684. On 29 September 2016, a further email was sent by Mr. Thompson to Mr. Chan
1326
T6-45, lines 23-35
1327
T6-46 & 47
1328
Ex F2A(4)(5), [13]
1329
Ex F2A(4)(5), [14]
1330
T27-21, 22 lines 1-12
1331
Ex B12(17), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 176 of 274

advising that whilst Dreamworld had been able to engage someone to inspect
the smaller rides, they had struggled to find a “competent person” to inspect the
‘Big 9 rides’.
1332
A further extension until 1 December 2016, for compliance with
s.241 of the Regulation was requested. It was noted in the correspondence that
the TRRR had been inspected by this date by a “competent person”.
1333
Mr. Chan
recommended that the further extension sought by Dreamworld be granted on
the basis that it would allow the Park to continue its business with some of the
‘unregistered’ amusement devices in operation whilst others ceased for the
engineer to conduct the required inspections.
1334
685. In August 2016, Mechanical Registered Professional Engineer (RPEQ), Mr. Tom
Polley from Tom Polley - Machinery Inspection Services, was engaged by Mr.
Deaves to carry out Class 2 Annual Inspections on rides at Dreamworld,
including the TRRR.
1335
Initial correspondence sent to Mr. Polley from Mr.
Deaves states the following:
1336
…
Our business has been having discussions with WPH&S about
the competent person and accountabilities under the regulation
for annual inspections.
The preferred model for us would be to make the business as
an entity accountable for the auditing of the appropriate
professionals required to ensure safe operation of equipment.
As you know the Queensland regulation is written and at this
time does not allow for this option. In order to maintain plant
registration we are required to have our rides inspected before
the end of September. Is this a service you could provide for us
in the time frame available.
Attached is a list of equipment. Many of the rides are small and
our documentation is good….
686. Mr. Polley, who has experience in the amusement ride industry since 1992,
agreed to conduct inspections for the Class 2 rides on 12 September 2016,
charging a rate of $1200 per day.
1337
He indicated that he would need to inspect
the ride and view documentation. Mr. Polley was subsequently provided with
plant registration numbers for some of the rides by way of a spreadsheet.
1338
He
did not request to see, and was not shown, the current Certificate of Registration
for each item of plant he was asked to inspect.
1339
687. Mr. Polley states that he requested from Mr. Deaves and Mr. Cruz maintenance
documentation of all the Class 2 Rides for the past 12 months, in order to assist
him in completing his inspections and subsequent reports.
1340
He claims that
during conversations as to these documents, he was advised that Dreamworld
had been focusing on getting their maintenance documentation up to an
1332
Ex B12(17), pg. 4
1333
Ex B12(17), pg. 2 & 3
1334
Ex F2A(4)(5), [15] & [16]
1335
Ex B3A(23), [5]; Ex F9C(8)(9)(c), pg. 1
1336
Ex F9C(8)(9)(c), pg. 1
1337
Ex F9C(8)(9)(d), pg. 1
1338
Ex F9C(8)(9)(g), [3]
1339
Ex F9C(8)(9)(g), [8] & [9]
1340
Ex B3A(23), [7]; Ex F9C(8)(9)(g), [6]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 177 of 274
acceptable level for the Class 5 rides, which are the bigger thrill rides.
1341
As
such, he was told that there was no maintenance documentation available.
1342
He subsequently requested from Mr. Cruz records as to the annual inspections
conducted previously.
1343
688. In relation to the TRRR, Mr. Polley claims that he did not receive any completed
maintenance documentation or log books, rather he was provided with a blank
Daily and Annual Inspection Schedule via email.
1344
Mr. Polley was advised that
there had been no issue with the TRRR for the past 12 months, and that there
was no current maintenance documentation due to the effort being put into the
Class 5 rides.
1345
689. According to Mr. Cruz, Mr. Polley was provided with the ‘entire maintenance
program’, for each of the rides he was asked to inspect.
1346
At inquest, Mr. Cruz
clarified this to mean a copy of the preventative maintenance checklists for the
daily, weekly and monthly inspections, leading up to the annual shutdown.
1347
He does not recall providing Mr. Polley with maintenance records, including
down-time reports.
1348
At Mr. Deaves request, Mr. Cruz accompanied Mr. Polley
around each of the rides as he carried out his inspections and outlined the daily
inspection checks undertaken for each ride.
1349
690. In relation to the TRRR, Mr. Cruz gave evidence that the only information he
provided Mr. Polley was the preventative maintenance checklists.
1350
691. On 29 September 2016, Mr. Polley attended Dreamworld and conducted a visual
inspection of the TRRR, which was limited to the mechanical and structural
aspects of the ride, and did not include the electrical or operational systems.
1351
692. Despite being the Ardent Group Safety Manager, Mr. Hutchings had no
involvement with engaging Mr. Polley.
1352
Certificate Issued for TRRR
693. An Annual Mechanical and Structural Inspection Certificate/Report 39/16 (the
Certificate) was subsequently issued by Mr. Polley for the TRRR, which was
dated 17 October 2016.
1353
This certificate states that no faults were found with
the following:
• Operational history since the last detailed inspection;
• Log book; and
• Inspection, including accessible critical components.
1341
Ex B3A(23), [8]
1342
Ex F9C(8)(9)(g), [6]
1343
Ex F9C(8)(9)(g), [6]
1344
Ex B3A(23), [9]
1345
Ex B3A(23), [10]
1346
Ex B3C(53), pg. 25 & 26
1347
T11-102, lines 37-45
1348
Ex B3C(53), pg. 26 & 27
1349
Ex B3C(53), pg. 27; T11-102, lines 20-45
1350
T11-102, lines 40-45
1351
Ex B3A(23), [11]
1352
Ex C8(10), pg. 26
1353
Ex F9C(8)(9)(h)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 178 of 274
694. The following recommendation and faults were found with the TRRR:
1354
• Recommendation 1: Anti Roll Back Gate – Consideration should
be given to introducing a scheduled inspection in the Daily Pre-
Service Inspection for the anti-roll back gates as the top gate
remained open when it should have automatically closed.
• Fault Found 1: Anti-Roll Back Gate – The top gate automatically
closing mechanism is not working and must be repaired.
695. The Certificate notes that:
1355
Statement
A visual inspection of the device (including a specific inspection
of visible mechanical and structural critical components) has
been completed. This inspection did not include an electrical
inspection.
In my opinion, this device was mechanically and structurally
safe to use at the time of inspection provided the above
Recommendation is appropriately considered and the above
Fault Found is repaired.
696. Mr. Polley claims that despite a lack of maintenance documentation, he was able
to conduct a visual mechanical and structural inspection of the TRRR, based on
‘my observations of issues like oil leaks, wear, cracking, and signs of corrosion,
together with assertions given to me by park maintenance personnel that there
had been no mechanical or structural issues with the ride in the past 12
months’.
1356
Draft Report for all Class 2 Rides
697. On 24 October 2016, Mr. Polley sent via email, a draft report to Mr. Deaves and
Mr. Cruz with general findings following the annual inspections carried out of all
of the Class 2 devices.
1357
698. The draft report outlines generally the applicable OIR legislative framework for
amusement device registration. The following limitations of Mr. Polley’s annual
mechanical and structural inspections are stated as follows:
1358
• Visually inspecting accessible mechanical and structural
components and accessible critical components of
individual devices in the presence of Dreamworld
technical staff for:
o Cleanliness including fluid leaks;
o Wear;
o Cracking;
1354
Ex F9C(8)(9)(h), pg. 2
1355
Ex F9C(8)(9)(h), pg. 2
1356
Ex B3A(23), [15]
1357
Ex F9C(8)(9)(i), pg. 7
1358
Ex F9C(8)(9)(i), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 179 of 274
o Signs of corrosion; and
o Signs of buckling, permanent deformation, paint
cracking, paint flaking or other indications of
stress beyond the yield point.
• Perusing a selection of computerised and hard copy
maintenance records for individual devices.
• Visually observing electrical issues, however, my annual
inspection did not include a detailed electrical inspection.
Of note, a detailed electrical inspection should be carried
out by a qualified electrical person.
Of note, my annual inspection did not extend to:
• Assessing the competence of technical and operational
staff to run the devices;
• A full audit of pressure equipment against the design
registration and plant registration requirements of
Schedule 5 of Work Health and Safety Regulation 2011,
nor did it extend to a full audit against the inspection
requirements of AS 3788-2006, Pressure equipment-In-
Service equipment; and
• An assessment of bolting hardware and bolting
techniques used in critical bolted connections.
699. In relation to General Findings of the Annual Inspections, Mr. Polley noted that a
daily inspection schedule was available for most devices, with a yearly inspection
schedule available for some.
1359
Furthermore, processes were in place and had
commenced for reviewing and updating current inspection schedules for the
Class 2 devices, as had been done on the higher class rides.
1360
700. Mr. Polley noted a number of Recommendations in his Draft Report, including
the following:
1361
• Inspection schedules: The organisation should continue, on a risk
assessment basis, reviewing all inspection schedules. All devices
should have a daily and annual inspection schedule and an analysis
should be undertaken to determine the need for any weekly,
monthly, three monthly and six monthly scheduled inspections or
any other special inspections not based on calendar parameters.
1359
Ex F9C(8)(9)(i), pg. 4
1360
Ex F9C(8)(9)(i), pg. 4
1361
Ex F9C(8)(9)(i), pg. 4 & 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 180 of 274
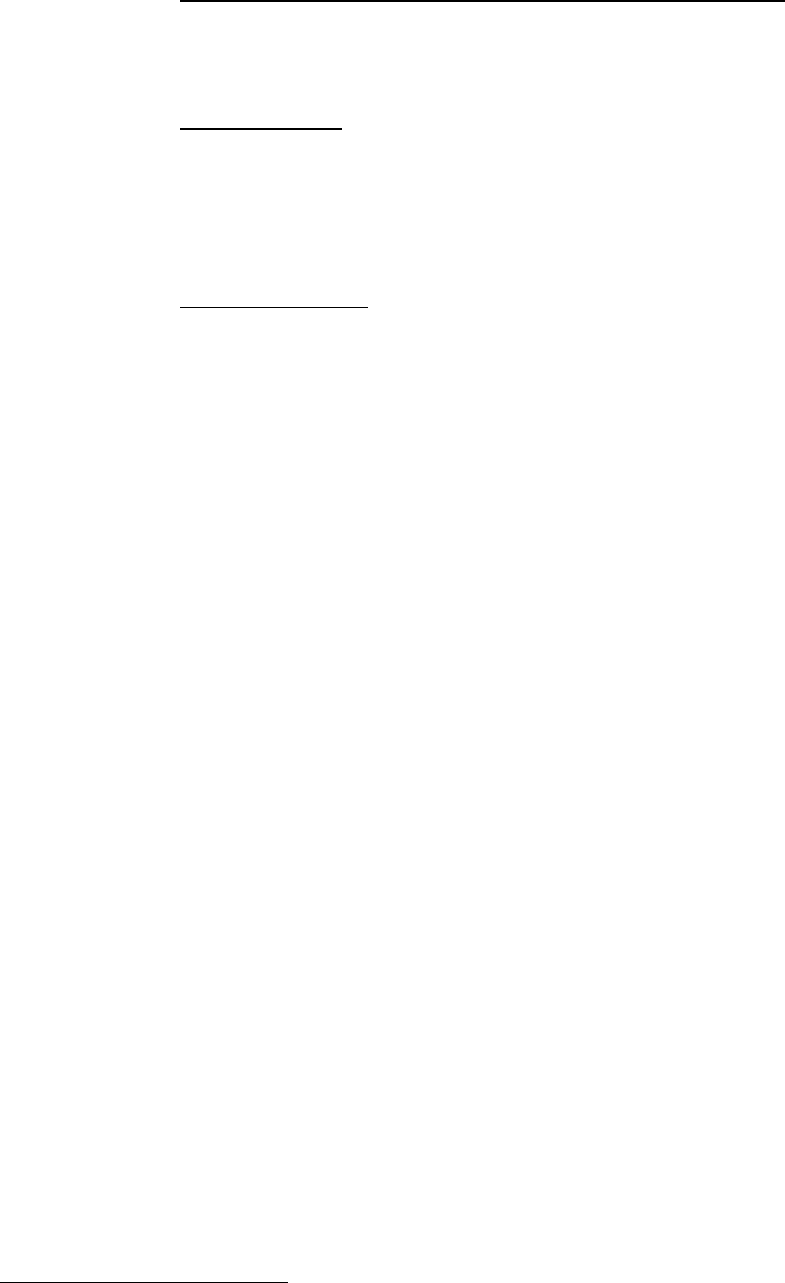
• Documentation following Servicing, Repair and Maintenance: The
organisation should introduce a formal procedure for checking all
documentation is in order prior to returning a device back to normal
use following servicing, repair or maintenance.
• Class of Device: As part of the review of all inspection schedules,
the organisation should establish the current Class 2 for the rides
inspected is correct in accordance with the Classification
requirements of Australian Standard AS-3533.1. The organisation
should also record the parameters used to establish the class of
ride.
• Dead Man controls: On a risk assessment basis, each device should
be assessed on the need for Operator dead man controls and if
required, modifications should be introduced on a priority basis as
determined by the risk assessment. Appropriate testing
requirements should also be introduced as required.
701. In conclusion, Mr. Polley stated that:
1362
In my opinion the organisation will have an acceptable
maintenance regime in place once it satisfactorily addresses
the Recommendations above including the upgrade and
implementation of all inspection schedules for the Class 2
devices.
702. Individual certificates were subsequently provided for each of the Class 2 Rides.
703. At the time of the incident, Dreamworld had engaged Pitt & Sherry, a Specialist
International Engineering company, to carry out inspections on the major thrill
rides.
1363
Representatives from the company were on-site inspecting other rides
the day of the tragic incident.
704. Records from OIR confirm that the registration process for all of the amusement
devices were completed by 24 January 2017.
1364
OIR INSPECTOR AUDITS OF DREAMWORLD PRIOR TO THE INCIDENT
705. Between 2002 and 25 October 2016, the Regulator conducted a number of
compliance activities for Dreamworld and WhiteWater World, which consisted
of:
1365
• 38 investigations (interventions with duty holders in response to a
notifiable incident, complaint or request for assistance);
• 111 assessments (interventions with duty holders to monitor compliance
and record enforcement actions, and in response to a notifiable incident);
• 36 notices (records of the issue of statutory notices to duty holders); and
1362
Ex F9C(8)(9)(i), pg. 5
1363
Ex B3C(53), pg. 28
1364
Ex F2A(3) [13]
1365
Ex F17(a), pg. 1-3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 181 of 274
• 10 advisories (records of inspector interactions with duty holders where
there is no anticipation of any compliance action being taken).
706. Principal Inspector Ian Baker, who has been employed by OIR for over 26 years
and involved in the inspection of high risk plant at Amusement Parks since 1990,
notes that he has always had a productive and professional relationship with
Dreamworld.
1366
He notes that in his experience, the safety practitioners and
Engineering Management at the Park have always been receptive to advice and
suggestions made by OIR in relation to any safety matter. He has undertaken
numerous site visits to Dreamworld, which were both reactive and proactive,
estimating that on average he has attended site approximately once a month.
1367
Prior to 2014, Mr. Baker recalls that when he attended site, he used to have
extensive contact with Mr. Tan.
1368
The last time he attended site for an OIR audit
was 3 March 2016.
1369
707. During the inquest, Mr. Baker stated that he had never seen the Operator
Procedures nor any documentation in relation to repairs and alterations of the
TRRR.
1370
He had also not inspected the conveyor of the TRRR during a safety
audit at Dreamworld.
1371
When shown photographs of the trough of the ride,
including the end of the conveyor and steel support railings at the unload area,
Mr. Baker acknowledged that there was a ‘nip point’ and that he would have been
‘concerned’ had he observed the area in this manner.
1372
He noted that when
OIR Inspectors were attending site to carry out a safety audit, they weren’t
closely examining the construction and integrity of the amusement device unless
a specific complaint had been received.
1373
Furthermore, there was no
concentrated effort to determine whether a piece of plant had been modified or
altered without notification made to the Regulator.
1374
708. In relation to the actions taken specifically for the TRRR by the Regulator prior
to the incident, the following was noted:
1375
• 18 November 2003: Two assessments were undertaken as part of a
major audit program coordinated by Inspector Ian Baker, for which the
TRRR was considered by three inspectors.
Notebook recordings of the findings made for these assessments state
that this was a large plant audit for which the Theme Park was viewed
during a walk around.
1376
The TRRR was physically inspected, as was
documentation pertaining to the ride. It was noted that ‘no breach of the
WH&S Act could be identified’.
1377
• 12 October 2014: A Hazard Specific Workplace Assessment was
conducted by Inspector Ian Baker (35774) which was in response to an
un-notified incident on 7 October 2004, where rafts collided in the
1366
Ex C4(10), [6] & [7]
1367
Ex C4(10), [9] & [10]
1368
Ex C4(10), [12]
1369
Ex C4(10), [16]
1370
T28-55, lines 25-47
1371
T28-49, lines 32-47
1372
T28-50, lines 5-25
1373
T28-51, lines 38-45
1374
T28-52, lines 25-35
1375
Ex F17(a), pg. 3
1376
Ex F17(a), pg. 12
1377
Ex F17(a), pg. 12
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 182 of 274

unloading area and a female guest fell into the water as she was
disembarking from the raft.
The site visit took 1 ½ hours. Notebook recordings of the findings of
investigators state that, ‘assessment re safe load & unload procedures.
E-Stop fitted at debarkation point. CCTV to monitor point. Electronic stop
& release system is being upgraded. 2
nd
gate option currently being
investigated’.
1378
709. Records provided by Ardent Leisure confirm the OIR safety inspections
conducted in 2003.
1379
Prior to the audit of Dreamworld, meetings were
conducted with Inspectors from OIR in order to establish the parameters of the
pending audit.
710. Commencing on 18 November 2003, 24 inspectors from OIR attended
Dreamworld to conduct the safety audit. This lasted four days, with each group
of Inspectors being accompanied by a Dreamworld team member, Mr. Bob Tan,
Mr. John Angilley, Mr. Steve Corrie and Mr. Russell Reed.
1380
I note in the
submissions from the OIR, referring to their document relating to that inspection,
there is a reference to electrical GPO’s needing to check inside the pump area
of the Rapids ride. The OIR goes on to mention that at the time of the inspection,
“the support rails were placed as close as possible to the end of the conveyor;
thereby limiting the gap and potential to identify any nip point which may have
been evident at the time.” I do not accept this submission. The OIR concede in
their submission that Inspector Baker “had not personally looked at the TRRR as
a safety audit or for safety aspects of it. On all occasions that Mr. Baker went to
Dreamworld, he did not see the TRRR not operating and the water drained from
the system.”
711. I find this admission alarming. Especially when considered against the evidence
of the independent engineers, and indeed the findings of the inspectors from OIR
who attended the scene after the accident, who all agree that the placement of
the support rails in proximity to the end of the conveyor created an obvious nip
point, as did the spacing between the rails of the conveyor, in contravention of
the Australian Standards, and an extreme danger to the passengers in the rafts.
712. I find that had the TRRR been inspected, in its design, condition and layout at
the time of the fatal incident, by a properly qualified engineer this serious and
highly dangerous situation would have been prevented and the ride closed.
Especially against a background of constant breakdown of the water pumping
system in place causing regular and frequent drops in the water level, a situation
well known to the owners and Operators of the ride as well as inspectors from
the OIR.
713. The OIR were also involved with the amusement industry in assisting and
consulting extensively with industry stakeholder groups to enhance safety of
amusement rides. The Engineering Unit has, over the last 14 years consulted
with industry, Engineers Australia and has been responsible for establishing the
National Work Health and Safety (WHS) Regulators Group.
1378
Ex F17(a), pg. 11
1379
Ex F16B(28), pg. 1
1380
Ex F16B(28), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 183 of 274
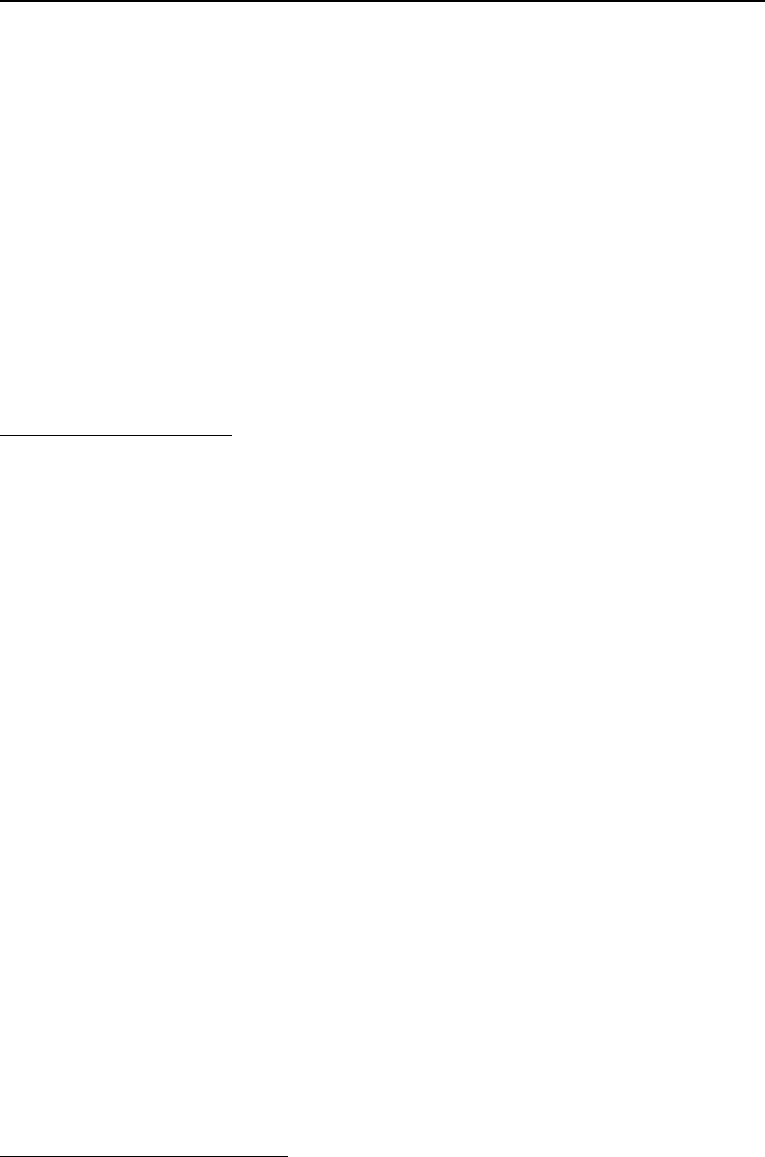
OIR TECHNICAL ADVICE ABOUT THE INCIDENT
Technical Advice - Principal OIR Adviser (Mechanical), Mr. David Flatman
714. Principal Workplace Health & Safety Adviser (Mechanical), Engineering Service
Unit, Mr. David Flatman provided a detailed report in relation to this incident for
the purpose of providing advice to the Legal Unit of OIR.
1381
He attended site on
a number of occasions, and provided an opinion as to what the contributing
factors and likely causes of the incident may have been, as well as the safety
issues associated with the maintenance and inspections of the ride. Only
relevant technical information as to the incident and cause is detailed below.
715. Mr. Flatman, who is now the Chief Advisor for Engineering Services, Specialised
Health and Safety Services with OIR, had almost 10 years’ experience as a
Principal Inspector at the time of the tragedy.
1382
In this role, he provided technical
support to the inspectorate, legal and prosecutions units within OIR, as well as
external advice to stakeholders in relation to plant safety. He held engineering
roles prior to his employment with OIR.
Inspections and Testing
716. Mr. Flatman attended the scene on a number of occasions and was involved in
the re-enactment testing undertaken.
1383
Relevantly, he noted the following:
• The ride appeared to be in generally poor condition, with significant
corrosion evident throughout the steel components of the ride and
concrete degradation in two of the tunnels.
1384
• Testing in an attempt to reconstruct the incident demonstrated that the
rails near the unload area were approximately 300 mm below the water
surface during operation.
1385
It also showed that the conveyor can cause
a raft to bounce when it is pushed back into the conveyor and the
conveyor turned off.
1386
• The tests also showed that the water level dropped by approximately 400
mm in 40 seconds when the south pump is turned off. The operating
water level was 2.26 m, which dropped to 1.83 m when only the North
pump was operating.
1387
717. Mr. Flatman’s findings as to the sequence and likely cause of the incident largely
accord with that of Senior Constable Cornish. In summary, he finds that the
incident was primarily due to the second raft being forcefully driven towards and
colliding with the stationary leading raft while the leading raft’s forward movement
was obstructed on the rails.
1388
The leading raft was grounded on the rails near
the unloading area as a result of the southern pump failing and causing the water
level to drop below the rails. It is likely that the leading raft was obstructed by the
cross brace between the rails in the vicinity of the unloading area. The second
1381
Ex F9A(1)
1382
Ex F19(11)
1383
Ex F9A(1), pg. 8
1384
Ex F9A(1), pg. 8
1385
Ex F9A(1), pg. 11
1386
Ex F9A(1), pg. 12
1387
Ex C4(4), pg. 248-250
1388
Ex F9A(1), pg. 12
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 184 of 274
raft was then driven into the stationary leading raft by positively engaging with
the slats on the conveyor. This resulted in both rafts rising up at their point of
contact. The motion of the conveyor caused the rear of the second raft to be
drawn down into the gap between the rails and the conveyor fatally injuring four
passengers.
1389
718. In terms of the contributing factors to the incident, Mr. Flatman identified the
following:
• Stationary raft – listed as a significant contributing factor, given the
collision would not have occurred had this raft not been grounded on the
rails near the unload platform.
1390
• Gap at the end of the conveyor – the geometry of the gap between the
head of the conveyor and the steel rails was sufficiently large enough to
allow the second raft to be drawn in by the motion of the conveyor.
Measurements by Mr. Flatman indicate that the gap between the rails
and the conveyor shaft were 760 mm, with the gap from the rails to the
wooden slats was 390 to 460 mm.
1391
Given the measurements of the rafts and the tube diameter, it was found
that the tube could easily fit into the gap if it was pushed back. The gap
at the head of the conveyor between the slats and the rails is small
enough to allow the slats on the conveyor to bite onto the tube and draw
it into the gap.
• Missing slats – measurements taken by Mr. Flatman of the gap created
by the missing slats on the conveyor were 770 mm, with the width of the
gap between the small wooden pads on the conveyor being 1255 mm.
This created a void large enough to allow the 1650 mm diameter of the
raft plug to drop down and positively engage with the slats on the
conveyor.
1392
Mr. Flatman notes that ‘when a raft was positioned on the conveyor in
such a way that resulted in the slat being located under the middle of the
plug, the resulting seesaw effect could cause the rear of the plug to tip
downwards into the void and positively engage with the adjacent slats on
the conveyor. In addition with the conveyor running the missing slats
created alternating large and small gaps that could bite into a raft tube
and increase the likelihood of a raft being drawn in the gap at the head of
the conveyor. The missing slats is considered to be a significant
contributing factor to the incident’.
1393
• Bowed slats – Some of the slats on the conveyor were observed to be
bowed upwards approximately halfway along their length by
approximately the thickness of the slats (50 mm). This increased the bite
on the tube and may also have caused the slat to bow further outwards
when loaded against the tube of a stationary raft, increasing the tendency
for the tube to be drawn into the gap between the conveyor and the
1389
Ex F9A(1), pg. 13
1390
Ex F9A(1), pg. 13
1391
Ex F9A(1), pg. 13
1392
Ex F9A(1), pg. 14
1393
Ex F9A(1), pg. 14 & 15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 185 of 274
rails.
1394
• Gap between rails – the distance measured by Mr. Flatman of the rails in
the vicinity of the unload platform was 1250 mm, which is similar to that
between the small wooden pads on the conveyor.
1395
The distance
between the cross rails was 1270 mm. This created a void large enough
for the plug in the leading raft to protrude into and positively engage with
the cross brace preventing it from moving along the rails. The likelihood
of this occurring is increased if the raft was misaligned towards one side
on the rails, so as to prevent the plug from being supported by both the
rails. This can be worsened if the rails were located towards one side of
the channel rather than in the centre. Measurements taken during
inspections show that the rails in the vicinity of the second cross brace
were located off centre towards the northern side of the channel.
1396
• Low air pressure – Mr. Flatman theorizes that the low air pressure in the
tubes may have contributed to the incident by reducing the support
provided by the tube and allowing the plug to protrude below the slats or
rails and into the voids. It could have also contributed to the incident by
allowing the tube to deform and be drawn into the gap between the
conveyor and the rails.
1397
• Low water level – Mr. Flatman found that the low water level was a
significant contributing factor to this incident, as it caused the leading raft
to become grounded on the rails.
1398
• Pump failure – CCTV confirm that the incident was initiated by the south
pump failure that caused the water level to drop below the rails and
resulted in the leading raft being grounded on the rails. Testing confirmed
that when one pump stopped, the water level dropped below the rails in
approximately 40 seconds.
1399
• Seat belts - Mr. Flatman notes that the seatbelts in place, which were
made of Velcro, were unable to restrain the passenger when the raft was
tilted upwards and shaken during the incident. Had the seatbelt been
secured with a positive locking mechanism, such as a buckle, it may have
prevented the person falling into the conveyor.
1400
• Operator procedures – it is noted that the procedures, which require the
unload Operator to contact the Main Operator before activating the
emergency stop, prevented the conveyor from being stopped prior to the
rafts colliding, which may have limited the severity of the incident.
1401
• Operator tasks – had the main Operator not been distracted by the task
of explaining and removing passengers from the load area, he may have
activated the emergency stop in time to prevent the incident. In addition,
Mr. Flatman notes that it is difficult for a busy Operator to identify the low
1394
Ex F9A(1), pg. 15
1395
Ex F9A(1), pg. 15
1396
Ex F9A(1), pg. 14-17
1397
Ex F9A(1), pg. 17 & 18
1398
Ex F9A(1), pg. 19
1399
Ex F9A(1), pg. 19
1400
Ex F9A(1), pg. 20
1401
Ex F9A(1), pg. 20
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 186 of 274
water level in the space of 35 seconds between rafts when they rely solely
on a visual check of the water level.
1402
• Operator experience and training – one of the Operator’s had only been
trained on the day of the incident. It is unclear whether the unload
Operator had been trained in the use of the E-Stop and detection of the
low water level.
1403
• Ride Layout – It is likely that the layout of the loading and unloading
platforms resulted in the load Operator at the loading platform facing
away from the Unload Operator while he was talking to guests. Had he
not been distracted by this task, and the orientation of the loading
platform was such that he could clearly see the Unload Operator and
conveyor, he may have activated the emergency stop in time to prevent
the incident. Mr. Flatman is of the view that had there been an additional
Operator or deck hand available at the time of the incident, they may have
been able to attend to guests and allow the Load Operator to focus solely
on the operation of the ride. This may have allowed him to identify the
potential collision and activate the emergency stop in time to prevent the
incident or respond to the unload Operator’s attempts to gain his
attention.
1404
Mr Flatman notes, however, that these are administrative controls, which
are not the best way to prevent incidents and should only be utilised after
more reliable control measures, such as engineering controls, are
considered.
• Control markings – The controls at the unload platform, including the
emergency stop control, were not labelled. This lack of marking would
have made it harder for an unfamiliar Operator to locate it in the case of
an emergency.
1405
719. In Mr. Flatman’s opinion, the three most significant contributing factors to
the incident were:
I. Stationary rafts on the rails;
II. Missing slats on the conveyor; and
III. Operator training
Control Measures
720. Mr. Flatman also briefly considered various control measures, which could have
been implemented to avoid the incident.
1406
Specifically, he cited the following
measures:
1407
• Conveyor modifications: the missing slats on the conveyor could have
been replaced, which would have reduced the likelihood of a raft being
1402
Ex F9A(1), pg. 21
1403
Ex F9A(1), pg. 23
1404
Ex F9A(1), pg. 21 & 22
1405
Ex F9A(1), pg. 22
1406
Ex F9A(1), pg. 24
1407
Ex F9A(1), pg. 24 & 25
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 187 of 274
forcefully driven into another by positively engaging with the slats, and
reduce the possibility of the slats biting into the tube and drawing a raft
down into the gap at the end of the conveyor.
• Stationary raft monitoring: Installation of a stationary raft monitoring
system at the head of the conveyor similar to that at the foot of the
conveyor. The stationary raft monitoring system could be integrated with
the ride control system so that it could automatically stop the conveyor,
pumps and close the jacks to prevent additional rafts from being
dispatched in the event a raft becomes stuck near the head of the
conveyor for any reason.
• Operators: Improve Operator training by explaining the position and
operation of the emergency stop controls. Increase the period of time a
new Operator spends with an experienced Operator when learning to
operate a ride. Emergency drills could be conducted to ensure the
competency of Operators in such a situation. Mr. Flatman notes s. 36 of
the Work Health and Safety Regulation 2011, which requires that the
other control measures, such as engineering controls, should be
implemented first, with the residual risk then controlled by administrative
controls.
• Modifications to rails: The rails could have been modified by adding an
additional rail midway between the existing rails. A centre rail would
reduce the depth the plug could protrude below the top surface of the
rails and most likely prevent it from positively engaging with the cross
brace.
Ride Modifications
721. The TRRR had undergone a number of significant modifications since its initial
construction and design registration in 1987, registration number E1624. The
TRRR was initially listed as a Class 2 amusement device.
722. There were no records of the modifications included in the design registration
documents held by OIR.
1408
It is therefore unknown if the modifications were
designed by a competent person in accordance with relevant technical
standards, or if the design of the modifications were verified by a third party
RPEQ. In accordance with s.244 of the Work Health and Safety Regulation 2011,
the alterations to design registered plant must also be registered when they may
affect health and safety. Whilst a number of the alterations were likely to have
occurred before 2011, similar provisions were in place at the time.
723. Mr. Flatman is of the view that the removal of the slats on the conveyor was a
major contributing factor to the incident.
1409
Markings on the channel floor in the
vicinity of the unload area near the head of the conveyor indicate that the rails
may have been altered. Details as to these modifications are unknown. It is
possible that the markings may be left over from the turn table system that was
previously removed from the ride. He is of the view that the removal of the
conveyor slats was a significant modification to the ride, and the regulator should
have been notified.
1408
Ex F9A(1), pg. 25
1409
Ex F9A(1), pg. 26
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 188 of 274
Previous Incidents on TRRR
724. Mr. Flatman considered the previous incidents that had occurred on the TRRR.
In relation to the incident that occurred in 2001 involving Ms. Lynd, he notes that
no engineering controls were implemented to prevent this incident from re-
occurring, which did not involve the water level dropping.
1410
He notes that
modification of the control system to detect a stationary raft between the unload
area and the head of the conveyor would have been preferable. Clearly, there
was little learning from previous incidents.
725. Mr. Flatman notes that despite the 4 incidents involving the TRRR taking place
in the vicinity of the unload area near the head of the conveyor, upgrades were
carried out to the beginning of the conveyor in 2016. He expresses the view that
the greater risk was clearly at the head of the conveyor near the unload area.
1411
Maintenance and Inspections
726. The information available to Mr. Flatman suggests that there was periodical and
routine maintenance performed on the ride.
1412
This consisted of daily, weekly,
monthly inspections, as well as annual shutdowns. In addition, maintenance was
performed during ride breakdowns to return the ride into operation.
727. Mr. Flatman refers to AS-3533.2 Amusement Rides and Devices, Part 2:
Operation and Maintenance which requires that rides undergo major inspections.
This is a requirement in addition to the annual inspections. It is likely that the
annual shut downs did cover some of the requirements for a major inspection.
1413
728. During the inspections of the ride carried out by OIR, the following faults were
identified:
1414
• Missing slats from the conveyor;
• Excessive corrosion;
• Crumbling concrete;
• No guarding at the foot of the conveyor, rail system and pump outlets;
• No water back flow prevention;
• Water running over electrical components; and
• Unidentified controls including emergency stop controls
729. The inspections carried out by OIR showed that the maintenance performed on
the TRRR was insufficient to prevent significant corrosion occurring or water
running over the electrical components in the pump enclosure.
1415
The
maintenance activities appeared to ensure that the ride remained in operation
1410
Ex F9A(1), pg. 27
1411
Ex F9A(1), pg. 27 & 28
1412
Ex F9A(1), pg. 26
1413
Ex F9A(1), pg. 27
1414
Ex F9A(1), pg. 27
1415
Ex F9A(1), pg. 26
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 189 of 274
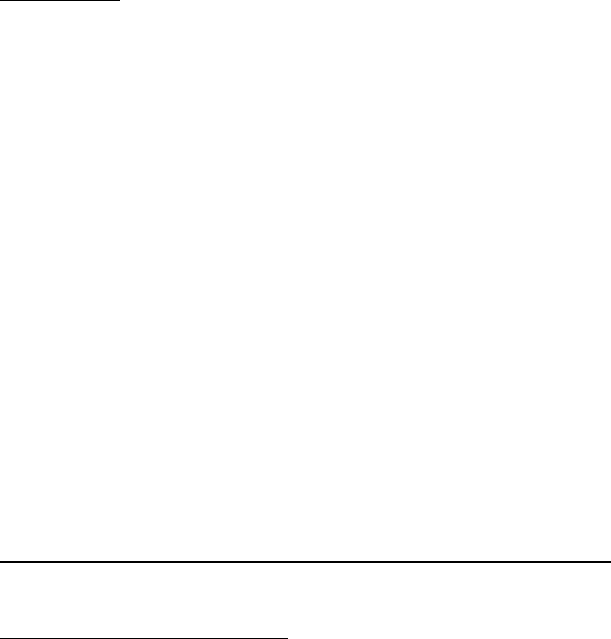
rather than keeping it in good condition. Mr. Flatman is of the opinion that more
should have been done to prevent and rectify the excessive corrosion and to
ensure that the pump motors and electrical components were kept as dry as
possible. He is of the opinion that due to the faults identified, the ride was unsafe
to operate and a more rigorous maintenance regime should have been
implemented.
1416
730. In considering the inspection conducted by Machinery Inspection Services (Tom
Polley) in September 2016, Mr. Flatman notes that ‘a visual inspection carried
out of visible parts only of the TRRR is not a detailed visual examination and is
likely to lack sufficient detail to accurately form the opinion that the ride is
mechanically and structurally safe to use for the next annual period when many
structural components on the ride are submerged in water’ (pg. 24, 25).
731. Mr. Flatman is of the view that the faults identified by Mr. Polley that is the
presence of corrosion and the critical bolted connections on the ride, were not
contributing factors to the incident.
732. A number of the issues raised in previous risk assessment audits of the TRRR
were present at the time of the incident, particularly the lack of control
identification labelling, corrosion and the emergency stop procedure. Mr.
Flatman notes that this clearly shows that the issues have been ongoing and
have not been adequately addressed.
1417
Conclusions
733. By way of summary, in Mr. Flatman’s opinion, the most likely cause of the
incident was due to the second raft being forcefully driven by the conveyor
towards and colliding with the leading raft, while the leading raft’s forward
movement was obstructed against a cross brace on the rails.
1418
The space
caused by the missing slats on the conveyor allowed the raft to enter the gap at
the conveyor head and rails. The motion of the conveyor drew the rear of the
second raft and three passengers into the gap. The conveyor continued to run
for approximately 19 seconds during this time, with the raft shaking vigorously
and the fourth passenger fell from his seat into the gap.
734. The incident was initiated by a sudden drop in water level as a result of the south
pump stopping, due to a fault. In Mr. Flatman’s opinion, monitoring the water
level may have prevented the incident.
1419
735. Mr. Flatman notes that despite previous incidents on the TRRR, at the time of
the tragic event, there was a heavy reliance on administrative controls, rather
than engineering control measures, to manage the evident risks and ensure the
safety of the ride, which is unacceptable.
1420
He notes that there was little
learning from previous incidents on the ride.
1421
Technical Advice - OIR Principal Inspector, Mr. Ian Stewart
736. Mr. Stewart, Principal Inspector with OIR, was requested to attend and assist
1416
Ex F9A(1), pg. 26 & 27
1417
Ex F9A(1), pg. 27
1418
Ex F9A(1), pg. 34
1419
Ex F9A(1), pg. 35
1420
Ex F9A(1), pg. 35 - 37
1421
Ex F9A(1), pg. 37
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 190 of 274

with the OIR investigation into this tragic incident. He has extensive practical
industry experience and as an investigator considering health and safety issues,
with formal trade qualifications and experience, a certificate in Competency
Engineer – Inspection of Machinery, and a graduate diploma in Occupational
Health and Safety.
1422
737. Mr. Stewart attended the scene on a number of occasions in October and
November 2016, and considered various relevant documentation associated
with the ride. As a result, he prepared a memorandum of his findings in relation
to the causal factors of this fatal incident.
1423
The relevant findings of this report
are outlined below.
Issue 1 - Reliance on Administrative Control in Emergency Situations
738. Mr. Stewart noted that the safe operation of the TRRR primarily relied upon
administrative controls, which are outlined in the operating procedures
developed for the ride.
1424
These controls require the Operators to have an
understanding and ability to observe and respond to situations, including
emergencies, as and when they arise, including:
• The controls used to operate the ride.
• Ensuring adequate water level.
• Preventing raft collisions.
• Monitor guest’s behaviour to ensure they stay in the rafts when
required.
• Loading and unloading guest’s onto and off the rafts.
• A section of the ride traverses and is monitored solely by the operator
at the Main Control Panel observing CCTV monitors, in conjunction with
other tasks.
• Maintaining order and sorting guest’s waiting to ride and those exiting
the ride.
739. In relation to the tasks being performed by the Level 2 and 3 Operators prior to
the fatal incident, which may have contributed to the delay in becoming aware of
the developing emergency situation, Mr. Stewart notes that:
1425
• Tests runs of the ride following the incident demonstrated that it was
difficult to identify that the south pump had stopped solely by observing
any change in noise levels. The north pump continuing to operate
generates sufficient noise levels as a possible indicator to Operators that
a pump had tripped.
• The Ride Operators rotate positions between the ‘Load’ and ‘Unload’
stations periodically while the TRRR is in operation.
1422
Ex F19(1)(b)
1423
Ex F19(1)
1424
Ex F19(1), pg. 4
1425
Ex F19(1), pg. 5 & 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 191 of 274
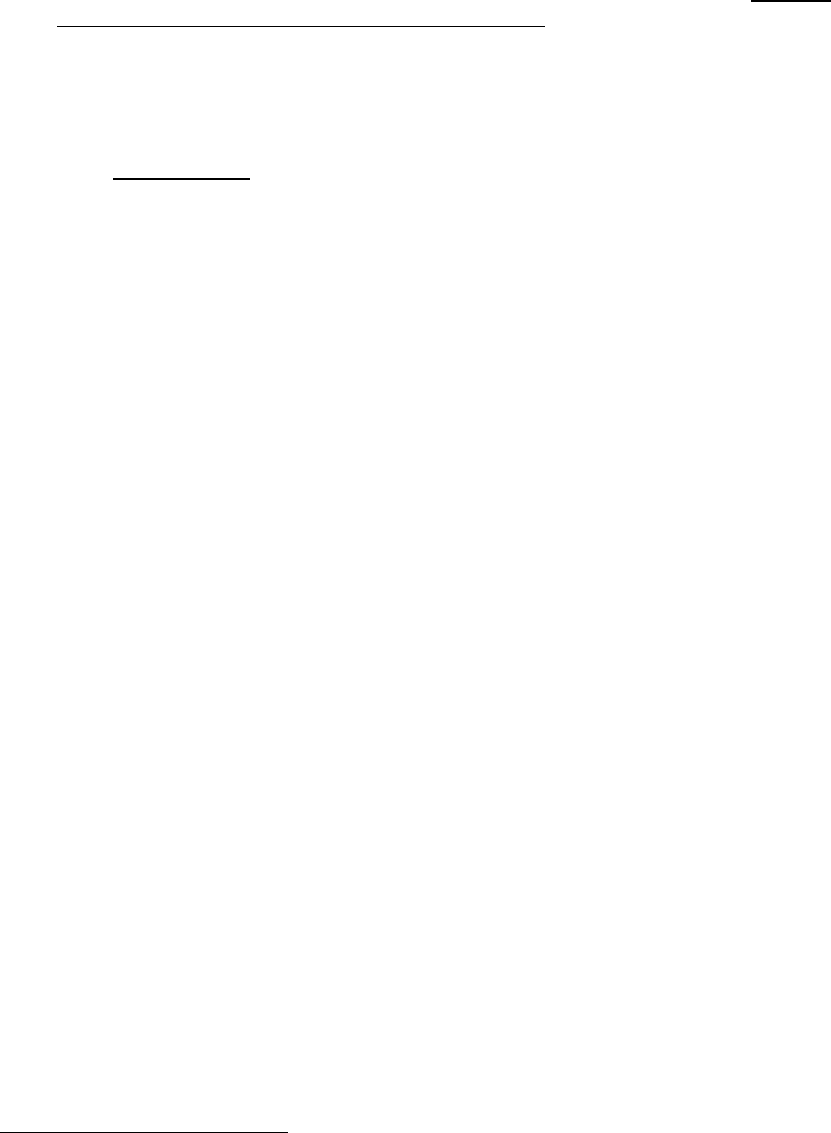
740. Having considered the functions required of the Level 3 Operator whilst manning
the TRRR, Mr. Stewart notes that a majority would have had Mr. Nemeth facing
away from the Main Control Panel and the unload area where Ms. Williams was
located.
1426
741. The applicable Australian standards (AS-3533 series & AS/NZS 4024), provide
guidance as to ‘Operator Information Handling Limitations’. AS/NZS
4024.1901:2014 – Safety of Machinery Part 1901, and describe situations and
tasks that may impact negatively on the Operator’s ability to respond effectively
in emergency situations, where the number and/or complexity of concurrent
tasks is excessive. At Appendix A ‘Application Guide’ of this Standard, the
following guidance is provided:
1427
A.2 Attention
In many situations, e.g. those involving a human operator in a
human-machine system, the person can be viewed as a single
channel processor with capacity to process information from no
more than a few sources at a time.
Attention is normally confined to two main sources, the internal
world i.e. thoughts and sensations from the body, and the
external world. Since attention can be described as a limited
resource, there may be competition among attentional
resources. For example, an operator who is occupied with
thoughts or decision making may suffer attentional deficits
regarding events happening in the outside world. A
consequence of the design of human-machine systems is that
it is essential not to overload the attentional resources of the
operator.
742. Mr. Stewart identified a number of tasks performed administratively by the TRRR
Operators to control ‘high risk’ situations, which he is of the view should have
been controlled and/or minimised by appropriate ‘engineering controls’,
namely:
1428
• Monitoring and prevention of rafts colliding in the unloading area; and
• Water level monitoring.
743. Additionally, the following components of the ride were in Mr. Stewart’s opinion,
deficient at the time of the incident, and are likely to have limited the Operators
ability to respond effectively to prevent this tragic incident from occurring:
1429
• Ride operating controls.
• Marking of controls.
• Ride operating procedures.
• Testing of emergency procedures, including how often the testing
should be done.
1426
Ex F19(1), pg. 7
1427
Ex F19(1), pg. 9
1428
Ex F19(1), pg. 11
1429
Ex F19(1), pg. 11
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 192 of 274

744. Mr. Stewart outlines details of the past incidents from 2001-2014, which had
occurred on the TRRR. He questions why, given the circumstances of some of
these incidents, particularly that involving Stephen Buss, as to why a risk
assessment process resulting in the installation of suitable engineering controls,
was not carried out.
1430
Mr. Stewart notes that the design of an amusement
device should include features (higher order controls, such as engineering
controls) to protect guest’s, Operators and equipment when a failure occurs. In
Mr. Stewart’s view, these earlier incidents on the TRRR, therefore, should have
alerted Dreamworld to the fact that the current administrative controls were not
effective in preventing incidents involving serious risks, such as rafts colliding in
the unload area.
1431
Mr. Stewart considered what a risk assessment of the TRRR
could have considered, based on the applicable legislation and regulations,
noting that any such reassessment or review should have thoroughly reassessed
the methods of control of the risk with a focus on implementing appropriate higher
order controls, such as engineering controls.
1432
745. In Mr. Stewart’s opinion, the previous incidents on the TRRR on 18 January
2001, 7 October 2004 and 2 November 2014 where rafts collided in the unloading
area, should have caused Dreamworld to thoroughly assess the control of the
risk by installing suitable engineering controls.
1433
He notes that engineering
controls are preferred over administrative controls as outlined in WHS Regulation
36, and s.4 of the OIR, How to manage work health and safety risks – Code of
practice 2011.
Issue 2: Limitations of the Ride Emergency Controls, Systems and Procedures
Provided for the Operator to Respond to Emergencies
746. Mr. Stewart notes that the prevention of the fatal incident was solely reliant on
the Ride Operators observing and responding to:
(a) Rafts colliding in the unloading area; and
(b) Water level drop.
747. In this regard, Mr. Stewart raises concern as to the limitations of the ride controls
and procedures as are required to be used by the Operator.
1434
He notes that
controls should be marked such that the Operators can easily identify the control,
the equipment involved and task the control performs.
1435
This becomes
particularly important in an emergency situation when Operators may panic
and/or hesitate in deliberating a course of action.
748. Section 210 of the WHS Regulation specifically requires the marking of
operational and emergency stop controls. Mr. Stewart notes that the control
panel at the main load section on the TRRR does not comply with WHS
Regulation as the controls are not clearly marked.
1436
749. Section 211 of the WHS Regulation pertains to Emergency Stops. Mr. Stewart
notes that the conveyor emergency stop located at the unload area is an
1430
Ex F19(1), pg. 11
1431
Ex F19(1), pg. 14
1432
Ex F19(1), pg. 20
1433
Ex F19(1), pg. 18
1434
Ex F19(1), pg. 21
1435
Ex F19(1), pg. 23
1436
Ex F19(1), pg. 24
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 193 of 274
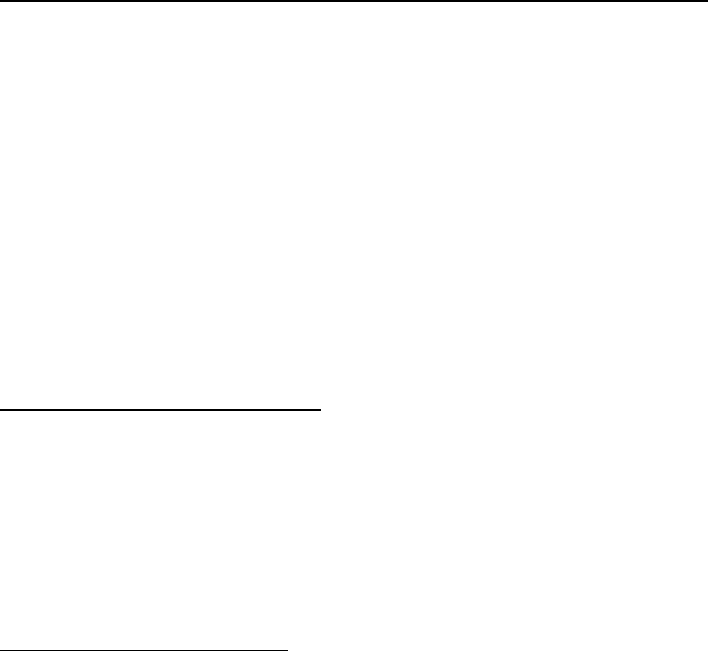
essential control as it is the only way for this to take place, and should have been
clearly marked ‘Conveyor Emergency Stop’. He opines that this may have
prompted the Unload Operator to activate this stop, had she been trained
accordingly.
1437
750. In relation to the Operator Procedure in effect, Mr. Stewart notes that in his view,
there was an inordinate amount of material and information to absorb in a short
time, and also to become competent in. He is of the view that a longer period of
supervised training would have been appropriate.
1438
However, he finds that
irrespective of the sophistication in the training provided, the risks associated
with rafts colliding and/or the water level drop are significant, such that
administrative controls, including Operator monitoring and controlling them is not
an appropriate control measure.
1439
751. Mr. Stewart also notes that regardless of the sophistication of plant, equipment
and means of controlling emergency situations, it is common practice within the
Amusement Park industry to perform periodic emergency drills.
1440
No
emergency drills were conducted for the TRRR. He is of the view that these drills
may have assisted in preventing the incident, however, could not have been used
in lieu of appropriate engineering controls to minimise the ‘high risk’ issues
associated with the ride.
1441
Issue 3 - Monitoring and Prevent of Rafts Colliding in the Unloading Area
752. In Mr. Stewart’s view, rafts impacting each other in the unloading area, is the
primary risk to the health and safety of patron’s riding the TRRR, specifically
referring to the previous 2001 incident.
1442
He notes that when the conveyor
continues to operate after this occurs, the following raft could then be driven by
the conveyor into the stationary raft where there is a risk of serious injury or death
due to crushing, entrapment and/or drowning. In Mr. Stewart’s opinion, these
previous incidents should have caused Dreamworld to assess and control the
risk prior to the fatal incident.
1443
753. Reference is made to the previous engagement of suitable persons to install
appropriate controls to minimise a similar risk at the beginning of the conveyor.
Accordingly, suitable technical standards, appropriate monitoring equipment and
competent persons were known to Dreamworld prior to the fatal incident.
1444
Issue 4 – Water Level Monitoring
754. Mr. Stewart notes the layout of the TRRR, specifically the use of the water
pumps, which ensure that an artificial stream is provided so that the rafts can
float. Hazardous situations may be created when one or both pumps fail. In
particular, when one pump fails, the water, which normally covers the raft catch
rails located at the unload area, drops, which doesn’t allow sufficient buoyancy
for the rafts to float, and as such, they rest on the rails. Occurrences where the
pumps have tripped causing a subsequent loss of water were not uncommon on
1437
Ex F19(1), pg. 25
1438
Ex F19(1), pg. 30
1439
Ex F19(1), pg. 30 - 32
1440
Ex F19(1), pg. 32
1441
Ex F19(1), pg. 32
1442
Ex F19(1), pg. 34 & 35
1443
Ex F19(1), pg. 34
1444
Ex F19(1), pg. 35
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 194 of 274
the TRRR. However, in the week prior to the incident, the pumps had tripped
more frequently.
755. Mr. Stewart notes that water level monitoring equipment, which was capable of
stopping the conveyor when the water level dropped, would have cost around
$2000 - $3000 if it had been included in the earlier upgrade work.
1445
He further
highlights that consideration had been given to having this type of monitoring
implemented by Dreamworld in 2016, demonstrating that this risk had been
identified earlier, and was known.
Issue 5 – Gap at the End of the Conveyor at the Unloading Area
756. The width of the gap at the unloading end of the conveyor on the TRRR is
sufficient to allow a raft to be drawn into it, creating the risk of death or serious
injury associated with entanglement or entrapment of persons on the raft.
1446
757. It does not appear that any risk assessments were conducted by Dreamworld in
relation to this gap, which may be somewhat hidden during the normal operation
of the ride by the water.
1447
Mr. Stewart expresses the view that this hazard would
not have been obvious to the casual observer, and therefore, detailed research
and observation would have been required to identify and control the hazard.
1448
758. In relation to the standards applicable to conveyors, Mr. Stewart specifically
refers to AS/NZS 4024.1201:2014 Safety of Machinery Part 1201: General
Principles for Design – Risk Assessment and Risk Reduction, which provides
examples of hazards, hazardous situations and hazardous events. Moving
elements with the potential to draw in, as was the case for the conveyor on the
TRRR, is specifically cited.
1449
759. AS/NZS 4024.3610:2015 Safety of Machinery Part 3610: Conveyors – General
Requirements, at point 1.5.21, defines a ‘nip point’, which is:
The point at which a moving conveyor element meets a fixed or moving
element, so that it is possible to nip, pinch, squeeze, entangle or entrap parts
of the human body.
760. Relevantly, at Point 2.13.2 – Hazardous Situations and Parts Requiring
Safeguards of this guidelines, it further states that:
1.13.2.1 General
Safeguards shall be designed to prevent –
(a) Persons reaching into the danger zone or other body
parts becoming caught or entangled;
(b) Conveyed materials accidentally falling or being projected into
persons;
(c) The hazard from the failure of a component;
(d) Contact with a danger point (i.e. nip or shear points) on
the conveyor.
1445
Ex F19(1), pg. 42
1446
Ex F19(1), pg. 44
1447
Ex F19(1), pg. 44
1448
Ex F19(1), pg. 44
1449
Ex F19(1), pg. 45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 195 of 274
1.13.2.2 Shear points and nip points
All accessible shear and nip points which create a risk to health or
safety shall be safeguarded in accordance with this Standard or
the AS 4.24.1 series, except for belt conveyor applications in
accordance with AS/NZS 4.24.3611
NOTES
…
2. Shear and nip points are created where the gap between
any moving part of the conveyor and any fixed equipment is
greater than 5 mm and less than 120 mm.
1.13.2.3 Rotating parts
All exposed rotating shafts or other parts shall be guarded, unless
the design risk assessment indicates there is no unacceptable risk
to health or safety.
All exposed projections, gaps, shafts couplings, collars or similar
shall be guarded.
761. At AS/NZS 4.24.3612:2015 Safety of Machinery Part 3612: Conveyors – Chain
conveyors and unit handling conveyors, it notes that:
TABLE 2.1 – TYPICAL HAZARDS ASSOCIATED WITH CHAIN CONVEYORS
AND UNIT HANDLING CONVEYORS
ENERGY
SOURCE/HAZARDS
DESCRIPTION
Mechanical Hazards
Crushing and shearing
hazards
Hazards may occur where parts can move against or past one another or
against fixed parts or past one another or past other fixed parts so that persons
or parts of their bodies can be crushed or sheared.
Entanglement hazards
Hazards may occur where projecting sharp edges, teeth, wedges, screws,
lubricating nipples, shafts, shaft ends or the like move so that persons, parts of
their bodies or their clothing can be caught and carried along.
Drawing-in hazards
(nip points)
Hazards may occur where parts move so that a constriction is formed in which
persons, parts of their bodies or their clothing can be drawn in.
Examples of drawing in points or nip points are as follows:
(a) Between the traction or carrying elements or attached pushers and
fixed parts of the conveyor or of the surrounding.
(b) At the traction or carrying elements in the area of direction changing
points.
(c) Between the traction or carrying elements and supporting rollers.
(d) At contact points of pushers on slide ways.
(e) At transfer points of conveyors as well as at chutes, roller and gravity
tables.
762. Accordingly, Mr. Stewart notes that the gap on the conveyor on the TRRR varies
from 500 mm to around 1 metre at the unloading end of the conveyor.
1450
As this
is greater than 120 mm, this technical standard does not consider it a hazard.
However, he noted the following:
1451
• AS/NZS 4024.3610:2015 primarily considers the movement of product
1450
Ex F19(1), pg. 46
1451
Ex F19(1), pg. 47
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 196 of 274

and materials and not persons.
• A risk assessment should have been conducted following the
modification/s that appears to have created this gap.
763. In addition to the risk posed by the gap at the end of the conveyor and the unload
area rails, the following further hazards were also observed:
1452
• Gaps between the slats in the conveyor system were excessive, such
that a person may fall and/or get out of the raft due to skylarking and
panic, and could fall through the conveyor resulting in injury or death due
to crushing, shearing and/or drowning.
• Lack of maintenance and excessive corrosion negatively impacting on
structural integrity and impacting on patron and worker safety.
764. In terms of the risks associated with the conveyor, Mr. Stewart notes that
reinstating the slats and extending the raft catch rails would have minimised the
risk of a raft or person’s whole body falling through the gap, however, a sufficient
gap may have remained that there would still be a risk to body parts, such as
arms and legs.
1453
Had an appropriate SIL 3 rated engineering control been
installed to monitor and control the risks associated with raft collision and
maintain correct water level, this would have removed the threat posed.
1454
765. Mr. Stewart is of the view that there was information readily available to
Dreamworld to identify the potential hazard created by the large gap at the end
of the conveyor.
1455
PROHIBITION NOTICE – ARDENT LEISURE
766. On 8 November 2016, following the tragic incident, a Prohibition Notice (‘the
Notice’) was issued to Ardent Leisure by Principal Inspector, Mr. Ian Stewart,
pursuant to s. 195 of the Workplace Health and Safety Act 2011.
1456
This Notice
precluded the operation of the TRRR until a serious risk to health and safety
emanating from an immediate exposure to a hazard associated with a person
being entangled in moving conveyors or submerged obstacles was rectified. The
basis for the view held by Mr. Stewart was listed as follows:
• The width of the gap between the end of the conveyor and the steel catch
platform, which is sufficient to allow a raft to be drawn into it creating a
risk of death or serious injury.
• Insufficient controls are in place to prevent a raft from entering the
unloading station whilst another raft remains in the area between the end
of the conveyor and unloading deck. This creates a serious risk of death
or serious injury associated with entanglement or entrapment.
• Where a person falls from a raft there is limited access for effective
emergency response.
1452
Ex F19(1), pg. 47
1453
Ex F19(1), pg. 49
1454
Ex F19(1), pg. 49
1455
Ex F19(1), pg. 49
1456
Ex F19(1), pg. 59 & 60
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 197 of 274

767. The Notice states that in its current state, the TRRR was not able to be put back
into service at any time, and poses an imminent risk to person’s health and safety
from exposure to the hazards cited above.
REGULATORY RESPONSE FOLLOWING THE INCIDENT
2016 Audit Campaign
768. Commencing on 29 October 2016 and concluding on 2 December 2016, a
compliance and audit program of Queensland’s six largest Theme Parks,
including Dreamworld, was undertaken by OIR.
1457
The audit team consisted of
a Director, Operations Manager, Engineers, and a number of Senior and
Principal Work Health and Safety and Electrical Safety Inspectors. Assistance
was also provided by other jurisdictions, with Engineers and Work Health and
Safety Inspectors from WorkSafe Victoria and SafeWork South Australia.
1458
769. OIR described this audit as ‘comprehensive’, and included over 90 audits
conducted using the National Audit Tool for Amusement Devices, which involved
a desktop review of the ride followed by on-site testing and verification.
1459
Specifically, Inspectors reviewed the documentation for each ride in relation to
plant and design registration, maintenance and operating manuals, instruction
and training of Operators, annual inspections by competent persons, repairs and
alterations, critical components and associated non-destructive testing,
emergency plans, asbestos, noise and electrical hazards and risks.
1460
The site
verification process involved Inspectors observing the operation of the ride,
talking to the Ride Operators and other relevant persons, and assessing the
actual operation of the ride against the systems outlined in the documentation
provided.
1461
In addition, engineers were also engaged to review the current risk
assessment documentation for each ride and provide support to Inspectors
through technical assistance during the site verification.
1462
770. The OIR Public Swimming Pool Checklist was used for those Theme Parks,
which operated water based rides. Key elements, which were addressed in the
audit tool, included: administration, general supervision, first aid, facility design,
water features and technical operation.
1463
771. As a consequence of the audit, 96 Individual Assessments were completed, 14
Improvement Notices and three Prohibition Notices, which related to amusement
ride the Buzzsaw at Dreamworld, were issued.
1464
772. Twenty-four audits were conducted for Dreamworld, with a focus on the ‘Big 9
Thrill Rides’. Eight notices were issued in total.
1465
773. In a Theme Park Report 2016, OIR outlined the findings of the audits conducted.
Relevantly, the following recommendations were made:
1466
1457
Ex F2A(3) [64]
1458
Ex F2A(20), pg. 1
1459
Ex F2A(20), pg. 1
1460
Ex F2(2), pg. 99
1461
Ex F2(2), pg. 99
1462
Ex F2(2), pg. 99
1463
Ex F2A(3) [65]
1464
Ex F2A(3) [66]
1465
Ex F2A(20), pg. 2
1466
Ex F2A(20), pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 198 of 274

• OIR to review and comment as necessary on the reports prepared by
external engineers Pitt & Sherry on all amusement rides at Dreamworld.
• Facilitate a forum with stakeholders in the amusement ride industry to
discuss current legislative requirements, policy decisions, audit tools and
relevant issues in the first half of 2017.
• Conduct proactive audits on fixed amusement rides by 30 June 2017, to
ensure compliance with relevant Work Health and Safety Laws.
• Conduct annual inspections of fixed amusement rides each year
following the initial six monthly audits listed above.
• Conduct proactive audits to ensure that all plant at major Theme Parks is
registered as required.
2017 Audit Campaign
774. A second major compliance program was undertaken between 12 October 2017
and 17 November 2017, involving the six major Theme Parks.
1467
The process
of assessment for this audit was broadened to include a review of the overall
safety management system and hazard specific systems of each person
conducting a business or undertaking.
1468
Existing assessment tools, such as
WHS Regulators National Audit Tool for Amusement Devices, were modified for
use at Theme Parks and incorporated input from five OIR specialist units.
Furthermore, industry stakeholders, including AALARA and the Australian
Workers Union, as well as business owners, were consulted for the purpose of
the audit program and advised of the process and tools to be used.
1469
775. As a result, 102 Individual Assessments were completed, 16 Improvement
Notices and three Electrical Safety Notices were issued during the campaign.
1470
The major non-compliance issues identified were those relating to annual
inspections of registered plant. Other issues that were identified include the
following:
1471
• Falls from height;
• Fuel dispensing in close proximity to electrical equipment;
• Electrical installations and maintenance; and
• The ‘test and tag’ procedure for specified electrical equipment on rides.
776. An additional 22 issues were identified by inspectors during the audits and were
immediately rectified therefore not attracting a non-compliance notice.
1472
777. A number of audit tools were used for the purposes of the campaign,
including:
1473
• Theme Park Systems Assessment;
1467
Ex F2A(3) [68]
1468
Ex F2A(26), pg. 2
1469
Ex F2A(26), pg. 2
1470
Ex F2A(3) [69]
1471
Ex F2A(3) [69]
1472
Ex F2A(3) [70]
1473
Ex F2A(3) [73]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 199 of 274

• Hazard management systems assessment;
• Onsite verification;
• Waterslide inspection guidance and checklist; and
• Theme Park audit survey.
778. OIR note that they, ‘will continue to support the major Theme Parks to enable
improved safety outcomes for workers and the general public. Businesses are
also encouraged to work together to improve safety within their industry. OIR
have increased the level of enforcement activities on the Theme Park industry
by verifying effectiveness of training for operation of amusement rides, including
emergency procedures; and conducting random auditing of the design of new or
modified amusement rides’.
1474
779. A Draft Project Closure Report was prepared by OIR detailing the findings of the
2017 audit report.
1475
Best Practice Review of OIR
780. The Best Practice Review (BPR) was commissioned by the Queensland
Government following this tragic incident and another fatality at an Eagle Farm
worksite in October 2016. This tragedy raised particular concern as to the
regulation of safety matters in Queensland.
781. Relevantly, the BPR and its recommendations considered:
1476
• The appropriateness of OIR’s Compliance and Enforcement Policy;
• The effectiveness of OIR’s compliance regime, enforcement activities
and dispute resolution processes;
• OIR’s effectiveness in relation to providing compliance information and
promoting work health and safety awareness and education;
• The appropriateness and effectiveness of the administration of public
safety matters by OIR; and
• Any further measures that can be taken to discourage unsafe work
practices, including the introduction of a new offence of gross negligence
causing death as well as increasing existing penalties for work-related
deaths and serious injuries.
782. The general findings of the BPR recognised that there was an ongoing need for
OIR to improve the human capital, systems and processes in place, particularly
in relation to the inspectorate, investigations and prosecutions.
1477
A re-balance
of priorities in favour of ‘hard’ compliance work, as opposed to capacity building
areas, with a view to increasing ground visibilities and activity of the inspectorate
was recognised as necessary.
1478
783. Overall, the BPR made 58 recommendations, with the following three relating to
1474
Ex F2A(3) [71] & [72]
1475
Ex F2A(26)
1476
Ex F2(1), [4]; Ex F2(2), pg. 18
1477
Ex F2(2), pg. 8
1478
Ex F2(2), pg. 9
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 200 of 274
public safety, specifically requiring the introduction of regulatory amendments to
improve amusement device safety:
1479
• Recommendation 41: The WHS Regulation 2011 be amended to require
that:
Mandatory major inspections of amusement devices, by
competent persons, are conducted;
Competent persons are nominated to operate specified
amusement devices, and
Details of statutory notices are recorded in the amusement
device log book and made available to the competent
person inspecting the amusement device.
• Recommendation 42: OIR in consultation with relevant stakeholders,
determine the level of competency required for the inspection of specified
types of amusement devices, and the level of competency required for
the operation of specified amusement devices (including the potential
need for formal licensing arrangements to apply in respect of certain
categories of device), and that the WHS Regulation 2011 be amended
accordingly.
• Recommendation 43: The WHS Regulation be amended to require, for
Operators of amusement devices, a similar regulatory approach to that
taken for Operators of facilities which use, generate, handle or store
hazardous materials. That is, for Operators and facilities whose
amusement devices collectively present a high risk, require preparation
of a safety case (which includes a WHS System) and application of a
licensing regime. For Operators and facilities whose amusement devices
collectively present a medium risk, require preparation of a WHS
management system and application for a lower level licensing regime.
784. It was noted in the BPR that for older amusement devices poor mechanical
integrity and a lack of modern safety control measures were a concern.
1480
Although annual inspections are mandated under the WHS Regulation, this
requirement falls short of a ‘major inspection’, which should include the
examination of all critical components of the device, as well as a check of the
effective and safe operation of the ride by a competent person with formal
engineering qualifications and experience.
1481
OIR indicated that they were in
discussions with the engineer’s professional body (Engineers Australia) to re-
activate the National Engineers Register for in-service inspection of amusement
devices. A proposal is also to be made to the Board of Professional Engineers,
Queensland to set up a similar register.
1482
785. It was recognised that the level of risk to the public from amusement devices is
comparable to that of facilities, which use, generate, handle or store hazardous
materials.
1483
Accordingly, it was acknowledged that a similar regulatory
approach may be necessary for Operators of amusement devices where the
1479
Ex F2(2), pg. 14 & 15
1480
Ex F2(2), pg. 100
1481
Ex F2(2), pg. 100
1482
Ex F2(2), pg. 100
1483
Ex F2(2), pg. 101
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 201 of 274
collective risk for those devices exceeds certain thresholds.
1484
786. In August 2017, the Queensland Government considered the recommendations
of the BPR and supported the recommendations made regarding amusement
devices.
1485
OIR has consulted with a range of peak bodies and individuals
following the release of the BPR.
787. On 31 August 2017, two meetings were held with show circuit representatives
and the major Theme Parks to discuss the BPR recommendations in relation to
amusement devices. The Honourable Grace Grace MP, who was the Minister
for Employment and Industrial Relations, Minister for Racing and Minister for
Multicultural Affairs at that time, attended part of the meeting with the Theme
Park representatives.
1486
788. Following these meetings, the Amusement Device Working Group of industry
stakeholders was established and met on 27 September 2017 to discuss the
BPR recommendations.
1487
789. A draft of proposed regulatory amendments was developed by the Office of the
Queensland Parliamentary Counsel during early 2018. On 11 May 2018, the
Amusement Device Working Group met to discuss the proposed amendments
to the WHS Regulation.
1488
790. I accept that the recommendations of the BPR have been accepted and are
being put in place. Once in place, the OIR should conduct a further audit to
determine all recommendations are in operation and are achieving the best
results possible.
OIR Plant Inspectors (Amusement Devices) Subgroup
791. The effectiveness of the compliance campaigns on amusement devices has
been improved through the implementation of regular training updates for OIR
inspectors conducting the audits.
1489
In June 2017, a subset of the OIR Plant
Network Group was established. The Amusement Device Inspectors function to
provide specialist support to the audit programs for both fixed and mobile
amusement devices. These specialists possess a high level of understanding of
the plants, as well as knowledge of the National Audit Tool for Amusement
Devices and the AS3533 series of standards.
1490
792. The members of the amusement device sub-group are provided with the relevant
training and experience sharing opportunities by the OIR Engineering Unit.
1491
This sub-group act as a repository of amusement device-related information,
audit issues or operational procedures to be shared with other inspectors (who
may at stages be auditing amusement devices).
1492
The sub-group members
support the mentoring and training of inspectors for amusement device auditing,
and meetings are held prior to the commencement of audits at Theme Parks or
1484
Ex F2(2), pg. 102
1485
Ex F2(1), [9]
1486
Ex F2(1), [11]
1487
Ex F2(1), [12]
1488
Ex F2(1), [14]
1489
Ex F2A(3) [78] & [79]
1490
Ex F2A(3) [79]
1491
Ex F2A(3) [80]
1492
Ex F2A(3) [80]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 202 of 274

regional shows.
1493
Plant Item Registration Working Group
793. Convened in November 2016, the Plant Item Registration Working Group aimed
to examine the current administrative, system and compliance activities
undertaken throughout the plant registration life cycle.
1494
The working group
considered the following:
1495
• The feasibility of compliance audits for registered plant for high risk plant
owners, e.g. those registrable plant items with additional specific
regulatory requirements; and
• Constraints of the existing plant system and possible enhancements to
ensure the plant registration life cycle is administered effectively.
794. As a result of the working group, a number of system enhancement and process
improvements were made, namely:
1496
• Improvements to invoicing and journaling functions to reduce manual
intervention required for reconciliations;
• Inclusion of audit trail and notes functionality to better maintain
information on customer transactions; and
• Changes to field functionality to make the system data easier to interpret
for internal staff.
795. Although the administrative registration scheme for plant does not replace or
relieve a duty holder of the regulatory requirements regarding plant use,
maintenance and inspection data gathered through the registration process can
be used to assist compliance of high risk plant, including amusement devices.
1497
796. OIR has initiated a two phase audit program for plant item registration:
1498
• Phase 1: physical inspection of items of plant that are not re-registered in
the new registration period, to ensure that unregistered plant are not in
operation. These audits are carried out by the regional inspectorate
supported by the engineering unit. Statutory notices are to be issued if an
unregistered plant is found to be in operation.
• Phase 2: desktop audit of registered plant items to confirm the required
design registration, maintenance and inspection records are available
and are compliant with the Regulation.
797. Upon implementation, 70 plant item registrations per year will be randomly
selected for desktop audit, until the introduction of the new Regulation is in force
and a safe case system implemented.
1499
1493
Ex F2A(3) [81]
1494
Ex F2A(3) [82]
1495
Ex F2A(3) [82]
1496
Ex F9C(2)(a), [98]
1497
Ex F2A(3) [83]
1498
Ex F9C(2)(a), [100] – [102]
1499
Ex F9C(2)(a), [103]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 203 of 274
Amusement Devices Stakeholders and Regulators Forum
798. OIR held an amusement devices stakeholders’ forum in Brisbane during
February 2017. Subsequently, in May 2017, OIR chaired the Amusement
Devices Stakeholders and Regulators Forum, as a part of the annual conference
organised by AALARA.
1500
PROPOSED REGULATORY AMENDMENTS
799. Following the tragic incident, a number of changes were made to the WHS Act
and the Regulations.
800. In December 2016, ss. 2, 272A and 279A of the Regulations were amended to
retain the existing annual plant item registration and renewal arrangements until
1 January 2019. This amendment was made through the Work Health and Safety
and Other Legislation Amendment Regulation (No.1) 2016 (SL No. 229 of 2016),
which was made by Governor in Council on 7 December 2016, and notified on
the Queensland legislation website on 9 December 2016.
1501
801. At the time of the amendments, the removal of plant registration was being
considered as part of the Council of Australian Governments (COAG) review of
model WHS laws. Maintaining the annual registration for two further years
(through the amendment to the Regulation) was intended to minimise the
disruption for businesses until the Government considered the recommendations
arising from the COAG review.
1502
The effect of this amendment was that owners
of registrable plant, including certain amusement devices, were required to
continue renewing registration annually.
Draft Further Amendments to the Regulations
802. Following the BPR, further proposed amendments to the Regulations were
drafted to reflect the recommendations made, namely:
• The introduction of major inspections of amusement devices;
• That competent persons be nominated to operate specified amusement
devices and details of statutory notices are recorded in amusement
device logbooks; and
• A requirement for Theme Parks to prepare a safety case and the
application of a licensing regime.
803. The first consultation draft of the new Regulatory provisions were circulated to
stakeholders on the Amusement Device Working Group on 2 August 2018.
Following on from feedback provided by the Group, a further amended draft was
prepared in November 2018.
804. By way of an overview as to the proposed changes to the regulatory environment
should the Regulation amendments be enacted, the amusement devices at
Major Amusement Parks,
1503
as defined in the Regulation, would still need to be
1500
Ex F2A(3) [84]
1501
Ex F2A(3) [54]
1502
Ex F2A(3) [55]
1503
Ex F19(13), Chapter 9A, s.608A
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 204 of 274

registered/renewed until such time as a license is granted to the Park. On
granting the license, it is proposed that the amusement device would be covered
by a safety case prepared by the Park, and therefore the device would not need
to be registered separately. The systems for inspection, maintenance and testing
of amusement devices at Major Amusement Parks would be audited by the
Regulator as part of monitoring compliance with the proposed Major Amusement
Park license and safety case system. Registration for amusement devices at
workplaces other than licensed Major Amusement Parks would remain the same.
Major Amusement Parks and the Proposed Safety Case Licensing System
805. Through the introduction of Part 9A.3 of the draft amendments to the
Regulations, it was proposed that a safety case and license regime be
established for Major Amusement Parks, requiring a comprehensive and
integrated approach for managing safety at the Parks.
806. The Major Amusement Parks
1504
which would fall within this regime are:
• Aussie World;
• Dreamworld and WhiteWater World;
• Sea World;
• Warner Bros. Movie World; and
• Wet ‘n’ Wild.
807. From a declared date, a Major Amusement Park will have:
• Six months to provide the Regulator with a safety case outline.
1505
This
outline is required to include a written plan for preparing a safety case
about the amusement devices at the Park, including key steps and
timelines, methods and resources to be used, details as consultation with
workers, draft emergency plan and how the case will address annual and
major inspections, maintenance and testing of devices, instruction and
training to Operators, log books and how the effectiveness of the safety
case will be monitored.
1506
• Two years to provide the Regulator with a safety case and apply for a
Major Amusement Park license. A Park can continue to operate
amusement devices during this period. The license will be for the
operation of the amusement devices at the Park.
1507
808. As part of the proposed safety case regime, Major Amusement Parks will be
required to prepare a written presentation addressing the following:
1508
• Identify potential hazards and incidents involving amusement devices at
the Park;
• Carry out a safety assessment for amusement devices at the Park;
• Implement control measures designed to eliminate or minimise the risk
1504
Ex F19(13), s.608A
1505
Ex F19(13), Chapter 9A, Division 2
1506
Ex F9C(1)(d), pg. 6; Ex F19(13) – s.608G
1507
Ex F19(13), s.608Q
1508
Ex F19(13), s.608H-P, 608R
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 205 of 274
of an incident occurring;
• Prepare an emergency plan and implement it if an incident involving an
amusement device occurs;
• Implement a safety management system for amusement devices at the
Park; and
• Consult with workers, for example, in relation to the emergency plan,
safety management system and preparing and reviewing the safety case.
809. A safety management system is a comprehensive and integrated system for
managing all aspects of risk control in relation to potential amusement device
incidents at the Park. It is intended to be the primary way in which it is ensured
that incidents do not expose the people to serious risk to their health or safety.
1509
810. It is proposed that once licensed, a Major Amusement Park will not be required
to register its amusement devices as the Regulator will be aware of relevant
information about the devices through the safety case. A license will be granted
for a period of up to five years, and conditions can be imposed by the Regulator
on the license.
1510
811. Sections 608N, 608O and Schedule 18C of the proposed amendments specify
matters which are required to be covered in the emergency plan and safety
management system for amusement devices.
812. Major Amusement Parks will still be required to comply with specific regulatory
requirements regarding amusement devices, for example, in relation to annual
inspections, major inspections, Operator competency and log books.
1511
Mandatory Major Inspections of Amusement Devices
813. Through the introduction of s.241A and associated provisions, major inspections
of amusement devices would be required to be conducted by, or under the
supervision of, a competent person, who has the necessary skills.
1512
A
competent person for amusement devices aside from inflatable devices, would
be a registered engineer.
814. Such inspections, which are in addition to the existing legislative inspection and
testing requirements already in place, are intended to ensure that a
comprehensive check and test of the amusement device is carried out through
an examination of the critical components of the device, as well as checking the
safe operation of the device.
815. Major inspections would be required to be carried out every 10 years unless
otherwise specified by the manufacturer of the device or a competent person,
who previously inspected the device.
1513
The responsibility of ensuring such an
inspection was carried out would rest with the person who had management or
control of the device. By way of a transition, the next major inspection for a
1509
Ex F9C(1)(d), pg. 7
1510
Ex F19(13), s.608ZL
1511
Ex F19(13), s.227
1512
Ex F19(13)
1513
Ex F19(13), s.241A(2)(c)
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 206 of 274
current amusement device would depend on the age of the device and whether
it has already undergone a major inspection. For amusement devices that are
over 10 years old and have not previously undergone a major inspection, the
next major inspection must be carried out within 2 years of the new Regulation
coming into effect.
1514
816. Requirements to maintain log books (ss.242, 242A) are also to be introduced,
which specify the details to be recorded.
Operators of Amusement Devices
817. Under the proposed amendments, persons with management or control of an
amusement device would be required to ensure that the device is only operated
by a competent person.
1515
A ‘competent person’ is defined as a person who has
acquired through training, qualification and experience the skills to carry out the
task. The effect of this provision is that an Operator, after being provided with
proper instruction and training in operating the device, would also have to be
assessed and determined as competent to operate the device. A record of the
worker having completed the necessary instruction is required to be included in
the log book for the device.
818. The intent of these provisions is to recognise that different amusement devices
require varying levels of knowledge and skill to operate the ride.
1516
Amusement Device Log Books
819. Pursuant to ss.242 and 242A of the proposed amendments, additional
information would need to be recorded in the log book for an amusement device,
including:
• The competency of the Operator of the device;
• The person who stores, installs, assembles, constructs, commissions,
decommissions or dismantles the device being a competent person;
• Details about major inspections, including the name of the competent
person who carried out the inspection, the date of the inspection, results
of the inspection and recommendations of the competent person, and
any components repaired or replaced during, or as a result of, the
inspection;
• Details about major inspections, including the name of the competent
person who carried out the inspection, results of the inspection and
recommendations made, and any components repaired or replaced
during or as a result of the inspection; and
• Relevant enforcement notices given for the device.
820. The log book is required to be available for inspection by a competent person
carrying out a major inspection of the amusement device or an entity that has
control or management of an event where the device is being operated.
1514
Ex F19(13), ss.789 & 790
1515
Ex F19(13), s.238 & Schedule 19
1516
Ex F9C(1)(d), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 207 of 274

Purpose of the New Proposed Safety Case Regime
821. OIR maintain that the proposed safety case and licensing regime for Major
Amusement Parks will involve an ongoing relationship between the Regulator
and the Theme Park industry. It will require Major Amusement Parks to regularly
review and update their safety case to ensure that safety is being systematically
managed at the workplace. As safety cases are reviewed, updated and
resubmitted to the Regulator for renewal of license application, OIR will have an
ongoing role in working with the Major Amusement Parks, auditing compliance
and performing the Regulator’s function.
1517
822. During the inquest, Mr. Bradley Bick, Executive Director of WHS Engagement
and Policy Services, OIR stated that the safety case regime was intended to
ensure that there has been a systematic and comprehensive risk assessment
undertaken on each of the rides at the Theme Park by the Operator, and that
there is an overlaying safety management system in place, which verifies that
the necessary controls are present and effective.
1518
With respect to major
inspections, Mr. Bick stated that ‘there would be ongoing checks to make sure
that operators were actually complying with that new regulatory requirement'.
1519
823. Practically, whilst the implementation of the process for auditing, assessing and
administrating the safety cases for Major Amusement Parks is still being
determined by OIR, Mr. Bick stated that it is anticipated that upon a safety case
being submitted, Mr. Chan and the Engineering Unit at OIR would be responsible
for conducting the requisite assessment.
1520
Three additional positions within the
Engineering Unit, which will possess engineering qualifications and be trained to
undertake the requisite assessments under the new Regulations, are to be
funded to facilitate this process.
1521
It is not envisaged that third party
assessments of the safety cases will be undertaken at this stage.
1522
824. At inquest, Mr. Chan acknowledged that the new safety case regime would
involve the active auditing by the Engineering Unit within OIR of Theme Parks to
ensure the proposed management maintenance programs and other areas
detailed in the safety case were actually effective following implementation and
had been suitably verified by a qualified external specialist as required.
1523
825. In addition to the amended Regulations, OIR are also developing a Code of
Practice for the industry in consultation with relevant stakeholders, including the
Amusement Device Working Group, which will set a minimum standard for the
operation of amusement devices.
1524
826. On 21 March 2019, the aforementioned amendments to the Regulations as
stipulated in the Work Health and Safety (Amendment Devices – Public Safety)
were approved by the Governor in Council and commenced on 1 May 2019.
1517
Ex F2(1), [17]-[19]
1518
T30-10, lines 26-45
1519
T30-5, lines 12-20
1520
T30-9, lines 3-13; 30-11, lines 5-15
1521
T30-15, lines 30-45
1522
T30-11, lines 12-40
1523
T27-16, lines 15-45
1524
T30-12, lines 35-48; 30-13, lines 1-15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 208 of 274

INDUSTRY RESPONSE & INFORMATION
827. For the purpose of the coronial inquiry, various pertinent industry groups were
invited to provide comment as to the incident and issues associated with the
Regulation of Amusement devices in Australia and worldwide. Whilst most
refused to provide any formal comment, below is a summary of the responses
received.
Submission by the Safety Institute of Australia
828. On 1 August 2018, Mr. Patrick Murphy, the Chair of the Safety Institute of
Australia (SIA) provided a submission as to issues associated with the
management, maintenance, safety risk assessment and training associated with
fixed amusement rides, such as those found at Dreamworld, as well as the
Regulatory environment.
1525
829. The key issues identified by the SIA in relation to the aforementioned matters
were as follows:
1526
(a) Issues pertaining to the adequacies of annual and longer term
inspections and audits, and engineers signing off on the safety design
of amusement rides, particularly in relation to the competencies of
those professionals having to certify the safety of the ride. Safety
covers all structural, mechanical and electrical/electronic aspects of
the ride, and impacts on the effective life of the ride.
(b) Issues pertaining to the management of modifications to the
manufacturer’s specifications, during or following installation to
ensure compliance with local Standards or legislation. Such
modifications have to be approved by a competent person consistent
with the requirements in item (a).
(c) The role of Australian standards in a situation where rides are
generally developed and manufactured overseas to overseas
standards, in particular Europe and the USA.
(d) Issues pertaining to the adequacy of maintenance of the structural,
mechanical and electrical/electronic aspects of the ride in terms of
compliance with manufacturers’ and construction design
specifications. Routine maintenance and environment has an impact
on the effective life of the ride.
(e) Issues pertaining to the training and competency assessment of ride
supervisors, operators and maintainers. This will include the
adequacy of standard operating procedures relating to opening or
closing a ride, normal operation and emergencies.
830. Generally, the SIA raised some concern as to the definition of a ‘competent
person’ within the meaning of the Regulations and Australian Standards, as well
as insufficient quality control on the application of the relevant definitions.
1527
It
was noted that there was no formal mechanism to assess the competence of
1525
Ex G3(1), pg. 1
1526
Ex G3(1), pg. 3 & 4
1527
Ex G3(1), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 209 of 274

those engineers who elect to practice in Amusement Rides and Device-in-
Service. Accordingly, an RPEQ could be deemed a competent person and sign
off on the issues.
1528
Whilst s.241 (5)(b) defines a competent person, SIA noted
that without a ‘clear understanding’ of how the Regulator decides on who is a
competent person, the potential for confusion exists and could result in the
inappropriate sign-offs on the operation and safety of amusement rides.
1529
831. SIA also cited the current lack of competent professional engineers with
experience in amusement rides, as well as a lack of process to try and ensure
these numbers grow so as to ensure the necessary expertise is sustained.
1530
It
was noted, however, that IEAust was convening a panel to examine the required
competency standards for the amusement ride category.
832. SIA submitted that the Regulator should undertake spot checks of the annual
inspections, particularly of high risk rides, to check the appropriateness and
consistency of the sign-off, and whether the inspecting engineer/auditor(s) has
an appropriate holistic plant design and operating verification process.
1531
It was
also submitted that the Regulator require the inclusion of maintenance plans as
part of the registration of amusement rides, particularly for high risk rides.
833. With respect to the Australian Standards, SIA was of the view that Standards
Australia and the Regulators should consult to harmonise their requirements for
design verification a large number of amusement rides in use in Australia are
internationally manufactured.
1532
834. With respect to the maintenance of rides, SIA noted that those older than 10
years will generally not have been designed to the current safety standards. In
these circumstances, it is submitted that a competent person should be required
to ensure that the risk management record for the ride identifies each of the risks,
implemented controls and the residual risk to ensure that safety is maintained,
so far as is reasonably practicable.
1533
835. In relation to training of Ride Operators, SIA is of the view that in order for staff
to maintain competency in operating a ride, they should be tested in emergency
and evacuation procedures every six months, and Operators of high-risk rides
should be routinely tested through simulations of emergencies.
1534
836. The critical recommendations made by SIA are as follows:
1535
I. The definition of a competent person in relation to amusement rides
needs to be clarified to reflect the unique characteristics of amusement
rides and their multi-disciplinary scope. This should be a joint activity
between IEAust and the Regulators.
II. IEAust needs to consider planning for succession to the current small
group of RPEs competent to assess amusement rides to ensure
continuity and safety of rides.
1528
Ex G3(1), pg. 4
1529
Ex G3(1), pg. 5
1530
Ex G3(1), pg. 5
1531
Ex G3(1), pg. 5
1532
Ex G3(1), pg. 6
1533
Ex G3(1), pg. 7
1534
Ex G3(1), pg. 7 & 8
1535
Ex G3(1), pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 210 of 274

III. The Regulators should audit the quality of sign-offs of ride designs,
modifications and maintenance plans, and the adequacy of training and
assessment of amusement ride supervisors, Operators and maintainers.
This particularly applies for older rides.
IV. For staff to maintain competency, they should be tested in emergency
and evacuation procedures every six months, and Operators of high risk
rides should be routinely tested through simulations of emergencies
when the public is not on the ride.
V. The relevance of design aspects of A3533.1 is questioned, given that
rides used in Theme Parks are manufactured in the EU or USA to
standards pertaining in those countries. AS3533.2 and AS3533.3 still
have an essential role.
OIR Response to SIA Submission
837. OIR were asked to consider the submission made by SIA and respond to the
recommendations made and issues raised.
838. A response was subsequently provided by Mr. Bradley Bick, the Executive
Director, WHS Policy and Engagement Services in the OIR.
839. OIR’s response to the key issues identified by the SIA are as follows:
1536
a) The lack of a formal mechanism to assess the competence of those engineers
who elect to practice as ‘competent persons’ to approve the design of an
amusement ride, conduct compliance checks, risk assess or perform and
develop maintenance procedures and programs.
I. The OIR does not have a role in assessing or regulating the
competence of engineers in their capacity as professional engineers
registered under the PE Act. This is administered by the Board of
Professional Engineers of Queensland (BPEQ). There is a formal
assessment regime used to assess engineers’ competencies
against minimum requirements for engineers to gain registration as
professional engineers in Queensland.
1537
b) How does the Regulator determine who is a ‘competent person’, pursuant to
s.241 (5)(b) of the Regulation.
I. Pursuant to the Regulation (s.241 (5)(b)(ii) & (i)) for amusement
devices that must be inspected by an RPEQ, the person must also
have acquired through training, qualification or experience the
knowledge and skills to inspect the device. The Regulator does not
have a legislated role to determine who meets the criteria under this
section, as the knowledge and skill required will depend heavily on
the particular type of device being inspected and its critical
components.
1538
1536
Ex F9C(1)(b), pg. 1
1537
Ex F9C(1)(b), pg. 1
1538
Ex F9C(1)(b), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 211 of 274

c) The need for a holistic approach to be taken in certifying a ride as safe pursuant
to the WHS Act 2011, which may necessitate the involvement of multiple
person/s to ensure that all technical competencies associated with components
of a ride are considered.
I. More than one competent person may be required to inspect the
device, for example, a mechanical engineer and an electrical
engineer may be required. The OIR understands it is routine for
inspecting engineers to call upon people with specialist skills to
assist when conducting annual inspections on amusement devices
under s.241. The inspecting engineer maintains overall
responsibility for the inspection of the amusement device including
the work carried out by the assisting specialists.
1539
II. During the inquest, Mr. Chan agreed that there needed to be a
holistic signing off with respect to amusement devices.
1540
He
acknowledged that as a mechanical engineer, he would not have
the requisite training to consider all of the components of a ride, and
may need to engage other external experts, such as non-destructive
testing specialists or control systems, to consider certain elements
and mechanisms.
1541
It would be likely that such specialists would
need to be engaged externally.
d) The suggestion that the Regulator should undertake spot checks of the annual
inspections, particularly of the high risk rides, to check the appropriateness and
consistency of the sign-off, and whether the inspecting Engineer/auditors has
an appropriate holistic plant design and operating verification process.
I. Audits of the major Theme Parks were undertaken by OIR in 2016,
2017 and 2018. These audits included checks that the annual
inspection had been carried out by a competent person as required
under s.241 of the WHS Regulation. The audits were conducted in
accordance with the National Audit Tool for Amusement Devices by
a multi-disciplinary team from OIR.
1542
II. As part of implementing the recommendations about amusement
devices made by the Best Practice Review of Workplace Health and
Safety Queensland, a consultation draft of the proposed regulation
was prepared. Annual inspections of amusement devices are an
element of the safety case system proposed and Major Amusement
Parks would be audited annually by the Regulator to check
compliance.
1543
Mr. Chan acknowledged during the inquest, that this
tragic incident had highlighted the need for the Regulator to do more
to ensure compliance, with the development of Regulations
requiring such action to be taken.
1544
III. For amusement devices generally, the Regulator is also proposing
that as part of the 2019 plant item registration renewal process,
amusement device owners will be required to provide the name and
1539
Ex F9C(1)(b), pg. 2
1540
T27-12, lines 29-40
1541
T27-12, lines 5-30
1542
Ex F9C(1)(b), pg. 2
1543
Ex F9C(1)(b), pg. 2
1544
T27-14, lines 1-15
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 212 of 274

details of the competent person who has undertaken the annual
inspection of the device and the date of inspection. This information
will enable the Regulator to confirm the person is registered as a
professional engineer in Queensland.
1545
IV. In addition, OIR has commenced recruitment for an additional 33
workplace health and safety inspectors, with three being placed as
amusement device inspectors with engineering qualifications to
assist in the regulation of the Theme Parks and amusement
devices.
1546
e) The suggestion that the Regulator require the inclusion of maintenance plans
as part of the registration of amusement rides, particularly for high risk rides.
I. The proposed safety case and license regime for Major Amusement
Parks will require detailed information on how amusement devices
will be maintained, inspected and tested. This information would
need to be provided to the Regulator in the license application.
Matters such as the maintenance of amusement devices would be
audited annually by the regulator. Accordingly, OIR is of the view
that the proposed approach addresses the outcome of SIA’s
suggestion.
1547
f) Each of the critical recommendations as listed in [826]:
I. OIR will continue to consult with Engineers Australia and the BPEQ
about the development of regulatory proposals in relation to
amusement devices. The OIR acknowledges that the different
definitions used for the term ‘competent person’ under the WHS
Regulation are not always easily distinguished by persons not
familiar with the legislation.
1548
II. The OIR acknowledges concern in the industry as to the availability
of registered engineers to inspect amusement devices. Consultation
will continue with industry stakeholders, Engineers Australia and
BPEQ about this matter, and broader factors influencing the
decisions of engineers to work in the amusement device field.
1549
III. Every application for design registration is checked by the OIR to
ensure that the relevant technical standards have been applied for
the particular type of plant and that the design has been verified by
a competent person. Independent audits are conducted by the
Regulator on the design of high-risk amusement devices to verify
the quality of the sign-offs on new and modified designs by external
professional engineers. Necessary action will be taken if there is
evidence that the engineer who conducted the design verification is
not fully competent. This process of checking and auditing applies
to modification of an existing design for the purpose of re-
registration.
1550
1545
Ex F9C(1)(b), pg. 2
1546
Ex F9C(1)(b), pg. 3
1547
Ex F9C(1)(b), pg. 3
1548
Ex F9C(1)(b), pg. 3
1549
Ex F9C(1)(b), pg. 3
1550
Ex F9C(1)(b), pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 213 of 274

IV. OIR supports a rigorous approach to ensure that amusement device
operators are competent and maintain their competencies with
regular opportunities to practice emergency and evacuation
procedures. The draft Regulation changes will insert a provision to
require that the person with management or control of an
amusement device is to ensure that the device is only operated by
a person who is a ‘competent person’. An amendment will also be
made to mandate the instruction and training requirements for
amusement device Operators, which will be outlined in the safety
case to be provided by the Major Amusement Parks.
1551
Risk control
measures will also be required to be implemented by Major
Amusement Parks to minimise the magnitude and severity of an
incident to people at the Park.
1552
V. The OIR has been actively participating in international efforts to
‘harmonise’ the requirements of relevant design standards on
amusement devices from Europe, America and Australia.
Harmonisation will ensure that critical safety requirements are
similar across the standards.
1553
VILLAGE ROAD SHOW SAFETY SYSTEMS
840. During the course of the coronial investigation, information was sought as to
Safety Management System in place at the various Village Road Show Theme
Parks throughout Australia.
1554
Details as to the training and ride operation of the
Wild West Falls Adventure Ride at Warner Brothers Movie World on the Gold
Coast was also sought.
1555
841. Executive Safety Manager, Mr. John Donaldson, who has held this position with
Village Road Show for the past 17 years, subsequently provided a number of
statements detailing the various safety systems and practices in place at Village
Road Show.
842. For the maintenance, inspection and testing of amusement devices at Sea
World, Movie World and Wet ‘n’ Wild, the following processes are in place:
• Requirements of the manufacturer are reviewed and added to the
maintenance schedule program (Maximo). This program, which has been
in use for the past 20 years, contains a database of all maintenance
checklists, inspection reports and any documentation received by any
inspections undertaken throughout the year.
1556
• Any advice received back from a manufacturer in relation to a ride or
process is recorded and actioned through the record of change of
management/maintenance process.
• Annually, an audit schedule is tabled with the Corporate Governance
Committee, which states that an independent ride engineering audit
1551
Ex F9C(1)(b), pg. 5
1552
Ex F9C(1)(b), pg. 5
1553
Ex F9C(1)(b), pg. 5 & 6
1554
Ex F2A(4)(2)(e)
1555
Ex C4(18)
1556
Ex F2A(4)(2)(e), [6]
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 214 of 274

commences in October.
1557
Upon completion of an amusement ride audit,
Village Road Show is issued with a certificate from an external engineer
to verify a record of the annual inspection, which is utilised for renewal of
plant registration. The competent persons engaged by Village Road
Show to carry out inspections on the amusement devices are DRA Safety
Specialists, Tom Polley and Tim Gibney, all of whom are qualified RPEQ
engineers.
1558
A yearly rotating schedule is used for the engineers
utilised.
• Figtree is a risk management database also utilised by Village Road
Show, which records all of the hazards, risks and actions identified for the
Theme Parks.
1559
Actions are assigned to managers to rectify issues,
which are escalated if not completed.
843. Since 2011, Village Roadshow have been utilising external engineers to review
their rides and provide independent advice and reports.
1560
Mr. Donaldson notes
that some of the Engineers have been engaged by Village Road Show for around
20 years to undertake AS3533 audits.
1561
These external audits are in addition
to internal audits, which are conducted by safety advisors within Village Road
Show who are required to undertake checks throughout the year on the various
attractions.
1562
844. At inquest, Mr. Donaldson elaborated on the training regime and maintenance
scheduling program in place at the various Village Roadshow Theme Parks. For
the past 20 years, a system has been in place to house the records in relation to
each of the rides, maintenance checklists, inspection reports, and including all
regular inspections undertaken on the ride (such as daily, weekly, monthly and
yearly).
1563
Updates and safety bulletins issued by the manufacturer of rides or
Regulator are housed in this database as well.
845. Information was also provided as to the attractions training procedures (‘the
Procedures’) in place at Movie World for the Wild West Falls Adventure Ride.
1564
Relevantly, the Procedures state the following:
1565
• A structured and methodical approach to Operational training is
contained within the Attractions Training Framework.
• The Operational department maintain a close relationship with the
Technical Services Department regarding attraction matters and ensure
that Manufacturer bulletins and/or procedure manual updates are
implemented and adhered to.
• All Attractions are rated annually by the Park Supervisors and Trainers
for the purpose of ranking the most appropriate progression of team
members. Team members are assigned an Easy or Moderate Attraction
at the start of their employment based on their comprehension and
1557
Ex F2A(4)(2)(e), [7]
1558
Ex F2A(4)(2)(e), [8]
1559
T28-96, lines 23-40
1560
Ex F2A(4)(2)(e), [9]
1561
Ex F2A(4)(2)(e), [10]
1562
T28-96, lines 1-10
1563
T28-94, lines 5-25
1564
Ex C4(19); Ex F2A(4)(2)(e)
1565
Ex C4(19), pg. 1
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 215 of 274

aptitude shown at Attractions Essential training, and depending on
Attraction availability with Scheduled Closures. Once trained on one or
two Attractions, team members will not progress to their next Attraction
until assessed as ready by their Supervisory and Trainer team.
1566
• Individual Attraction training is provided, which includes an overview of
the ride by way of a PowerPoint presentation, a specific training plan for
the ride to be followed by the trainer, as well as a procedure manual
issued to the trainee for the specific Attraction being learnt. It is noted that
these manuals are reviewed and updated annually as a minimum, more
frequently as procedural and/or manufacturer changes occur. Every
training day is to follow a similar pattern, which includes all elements of
the Procedure Manual, practical time at each position and an evacuation
walk through for each position.
1567
If simple changes are to be made,
these are communicated in the form of Toolbox Talks delivered by the
Ride Supervisor in the morning and signed by all operating team
members on the day.
1568
• At the end of each Training Day, a team member must have
demonstrated their competency in each required line of the Competency
Checklist and completed a Written Test achieving more than 80%.
1569
• Each Attraction has a dedicated daily Supervisor who oversees the
Attraction and provides feedback and support to each Attraction
Attendant. This feedback and coaching is detailed on the daily Attraction
Transfer Sheet, which is recorded in each individual team members
Discipline Dossier.
1570
• All team members must also undergo an individual Attraction Training
written test every six months and score more than 80%.
• Team members conduct weekly Attraction evacuation drills, scheduled
for a particular day at each Attraction and is logged on an Evacuation
Record sheet.
1571
• Team members are subject to random Assessment at Attractions using
the iAuditor app.
• A mentor program was in place called HERO (Helping, Encouraging and
Respecting Others), which identifies key team members who are role
models to other employees. HERO team members are rostered on to
buddy training on training days.
1572
• Operations Trainers were progressing through key modules of a Cert IV
in Training and Assessment.
1573
1566
Ex C4(19), pg. 4
1567
Ex C4(19), pg. 6
1568
Ex C4(19), pg. 8
1569
Ex C4(19), pg. 7
1570
Ex C4(19), pg. 7
1571
Ex C4(19), pg. 7
1572
Ex C4(19), pg. 8
1573
Ex C4(19), pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 216 of 274
EXPERT EVIDENCE
Engineering Expert Advice
846. During the course of the coronial investigation, expert engineering advice was
sought in relation to the incident and various aspects associated with the TRRR.
Separate advices were provided by the following experts:
I. Dr Frank Grigg, Forensic Engineering Consultant;
II. George Rutherford, Technical Director of Projects etc. Pty Ltd; and
III. Dr Duncan Gilmore, Gilmore Engineers.
847. At inquest, evidence from the engineering experts was heard by way of a
conclave.
848. A summary of the individual expert reports received, as well as the joint expert
advice and evidence provided during the inquest, are outlined below.
Report on the Design of the Conveyor System by Dr Frank W. Grigg, Forensic
Engineering Consulting Pty Ltd
849. On 3 November 2016, as part of the OIR investigation into this incident, Dr Frank
Grigg was requested to consider the construction of the conveyor and provide
expert comment on a number of matters including, whether it was suitable for its
application as of 2016, the modifications made and the shutdown process that
was in place when the water level dropped.
1574
In addition to considering various
internal Dreamworld documentation as well as CCTV of the incident, he also
attended the scene on two occasions with OIR investigators.
1575
850. In order to assess the suitability of the conveyor design, Dr Grigg noted that it
was necessary to determine, as best as possible, the interaction of the conveyor
with the rafts during the incident.
1576
CCTV footage of the event was utilised,
along with survey data and measurements taken by Bennett and Bennett, in
order to estimate the raft positions and likely interactions during critical
events.
1577
It was noted that:
• Immediately after the first contact of the rafts, as Raft 6 was pushed
forward by Raft 5, it would be expected, based on the properties of the
inflated tubes as well as the observations during subsequent OIR testing,
that there would be some compression of the tubes as a result of the
forces between them.
1578
• Given the continued movement of the conveyor, the contact geometry
and the compression of the tubes during contact at this stage of the
incident (first contact), it would be expected that:
o The lower quadrant of the front of Raft 5’s tube would have
pushed against the upper quadrant of the rear of Raft 6’s tube -
1574
Ex B4(1), pg. 4
1575
Ex B4(1), pg. 1
1576
Ex B4(1), pg. 11
1577
Ex B4(1), pg. 11
1578
Ex B4(1), pg. 13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 217 of 274

locally compressing and distorting the tube segment contact.
1579
o The front of Raft 5 plug would have tended to pitch upwards
because the compression of its tube at the front would have acted
as a ‘jack’ against the surfaces beneath it and because the
geometry of the tube contact would have tended to cause the front
of the raft to ‘ride up’ on the rear of the leading raft. Notably, a lot
of the rafts weight at the time would have been borne by the
conveyor. As such, the dominant direction of force transferred
from Raft 5 to Raft 6 would have been in the horizontal
direction.
1580
o The rear of Raft 6 would have tended to pitch upwards because
of the compression of its tube at the rear by Raft 5, which would
have acted as a ‘jack’ against the support frames surfaces.
1581
851. Dr Grigg noted that ‘the amount of upward pitch experienced by each raft plug at
the contact end would depend significantly on the inflation pressures of the
deformed tube segments and the magnitude of the contact forces between
them’.
1582
Given Raft 5’s tendency to pitch upwards, it would be expected that
the rear edge of Raft 5 would pitch downwards, and as such, become ‘more
exposed to contact with the front edges of the full width slats on the
conveyor’.
1583
This would have been similar for Raft 6, which would have caused
it to pitch downwards and be more exposed to contact with the edges of the
support frame.
1584
852. Dr Grigg further noted from the CCTV footage, that at 2:05:04 pm, Raft 6 can be
seen to be providing sufficient resistance to the forward motion of Raft 5 to cause
it to slip on the moving conveyor slats.
1585
The conveyor then ‘engaged’ with the
raft substantively, during which time it was thought that a full width slat was likely
positioned immediately behind the rear of Raft 5.
1586
853. Dr Grigg found that the following characteristics of the conveyor and the support
frame, contributed to the incident:
1587
• The distance between the full width slats was excessive, which led to –
o Increased probability of the plug pitching down aft and engaging
more substantively with the slats and being driven forward
forcefully. An increase in the number of full width slats would have
reduced the probability of this occurring and may have made it
more likely that the raft would have slipped on the top of the
conveyor.
1588
o Provided a significant gap between the conveyor head end and
the support frame, which increased the probability of the raft
1579
Ex B4(1), pg. 13
1580
Ex B4(1), pg. 14
1581
Ex B4(1), pg. 14
1582
Ex B4(1), pg. 14
1583
Ex B4(1), pg. 14
1584
Ex B4(1), pg. 14
1585
Ex B4(1), pg. 14
1586
Ex B4(1), pg. 14 & 15
1587
Ex B4(1), pg. 16
1588
Ex B4(1), pg. 17
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 218 of 274

falling into and becoming caught in the gap. Additional full width
slats would have reduced the size of the gap between the
conveyor head end and support frame, which would have likely
reduced the engagement of the raft in the gap.
1589
o Increased the severity at which the raft shook once it had fallen
into the gap. If additional full width slats had been in place, this
would have changed the size of the gap thus lessening the size
of the compressive force imposed on the raft tube and plus, which
would have resulted in less severe shaking.
1590
• Upwardly bowed full width slats on the conveyor increased the probability
of the conveyor engaging the raft and moving it forward forcefully.
• The distance between the support frame cross members was excessive.
Dr Grigg noted that the distance between the first and second cross
members was about 1450mm, with the second and third being 1270 mm.
The distance between the support frame rails was 1450 mm. Accordingly,
there was limited support to a raft plug, increasing the probability of the
front edge of a downwardly pitched raft plug engaging with the third cross
member.
1591
A central longitudinal member could have prevented the
bottom of Raft 6’s plug from engaging the cross member of the frame.
• The distance between the conveyor head end and the support frame was
excessive.
854. Dr Grigg found that:
The design of the conveyor, most notably the fitting of a full
width slat to every 6
th
link (every 3
rd
outer link), gave rise to the
risk of positive engagement between the slats and the bottoms
of the plugs of the rafts as well as the tubes, so as to produce
the force necessary to cause the raft being discharged from the
conveyor to tilt upwards when it hit the rear of the raft that was
stranded on the support frame as a result of the water level
dropping. It also resulted in the violent shaking of raft #5 after it
had been titled up and caught between the conveyor and the
support frame.
1592
855. Dr Grigg noted that an automatic shutdown of the conveyor in the event that one
of the pumps failed would have prevented the incident from occurring.
1593
Furthermore, had a means of detecting a stranded raft in the unload area been
installed, which stopped the conveyor, the tragic incident would have been
prevented, as had been the experienced in 2001.
1594
In relation to the incident in
2001, Dr Grigg concluded that this ‘provided clear operational experience of what
could occur in the event that the movement of a raft became blocked after being
discharged from the conveyor, even without pump failure and water level
dropping’.
1595
1589
Ex B4(1), pg. 17
1590
Ex B4(1), pg. 17
1591
Ex B4(1), pg. 17
1592
Ex B4(1), pg. 18
1593
Ex B4(1), pg. 17
1594
Ex B4(1), pg. 18
1595
Ex B4(1), pg. 18
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 219 of 274

Safety Related Control Systems, Summary Report 170326GRa, Expert Report by
George Rutherford, 26 March 2017
856. Mr. George Rutherford, Technical Director from Projects etc Pty. Ltd was
requested by OIR to attend Dreamworld immediately following the incident to
assist with their investigation. Various site visits were subsequently undertaken,
including observation of the re-enactment attempts carried out by QPS.
1596
857. Mr. Rutherford is a qualified engineer and has various workplace health and
safety competency training. For 25 years, he has been involved in Safety/ EMC
Assessments and Testing for a wide range of Products, Plants (Machinery) and
Systems against International and National Regulations and Standards.
1597
858. Despite multiple requests, documentation relating to the TRRR, namely circuit
diagrams, critical components lists, risk assessments were not provided to Mr.
Rutherford by Dreamworld. He raised significant concern should these ‘basic’
documents not exist as they would ‘likely lead to unsafe maintenance practices
by Dreamworld Staff and perhaps inadequately safety design in rides’.
1598
It is
of note that documents of this nature were unable to be sourced by Ardent
Leisure, and as such, have never been produced.
859. Mr. Rutherford reached the following conclusions as a result of assessing the
circumstances of the incident:
1599
• The incident appears to have occurred due to the sudden lowering of the
water level at the upper area of the ride. This resulted in the grounding of
a raft at the exit side of the Conveyor, which was subsequently struck by
the raft carrying Ms. Goodchild, Mr. Dorsett, Ms. Low and Mr. Araghi, as
it was forced off the conveyor.
1600
• The lowering of the water level is likely to have been caused by the south
water pump stopping. Such a stoppage may have gone unnoticed and
was possibly masked by the noise of the North Pump, which was still
operating. Mr. Rutherford noted that he did not observe any difference in
noise level when the south pump was started/stopped, nor was there a
significant change in water turbulence.
1601
• The lowering of the water level to a ‘dangerous state’, which could cause
a raft to ground once the south pump had stopped, would have happened
‘very quickly’, and in Mr. Rutherford’s opinion, far too quickly for a busy
Ride Operator to take any appropriate action, ‘even if it was clear to the
operator what action they were meant to take’.
1602
He is of the view that
the lowering of the water level should have been detected
automatically.
1596
Ex B4(3), pg. 3
1597
Ex C2(1)(a)
1598
Ex B4(3), pg. 4
1599
Ex B4(3), pg. 4
1600
Ex B4(3), pg. 4
1601
Ex B4(3), pg. 4
1602
Ex B4(3), pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 220 of 274
• The result of the raft collision was worsened by the air gap between the
end of the conveyor and the metal structure (support rails) in the
unloading/loading areas.
1603
The reasons for the large gap needed to be
determined, particularly as this may have occurred inadvertently over
time with the replacement of corroded parts, as opposed to by a
deliberate design.
1604
• The ride operation procedure appeared to be ‘vague’, with the
Dreamworld technicians observed by Mr. Rutherford not to have been
completely confident as to what components of the ride were stopped by
the Emergency stop button at the Main Operator control panel.
1605
• The modification carried out on the conveyor in early 2016 (installation of
SIL 3), was confirmed to have been able to achieve the necessary level
of safety.
1606
860. In Mr. Rutherford’s opinion, the primary cause of the tragic incident was ‘the
lack of a suitable safety rated water level detective system interfaced to the
upgraded conveyor system – such a safety system could easily have been
provided and at a minimal cost’.
1607
He further states that the incident occurred
as a result of a series of unfortunate events and timings, the absence of which
had allowed the ride to operate for many years without incident. He opines that
‘I feel lessons should be learnt from this unfortunate incident particularly the
importance of a correct initial risk assessment/regular updating of that risk
assessment and the need for correctly assessed/rated safety circuitry’.
1608
861. Further, whilst unrelated to the incident, Mr Rutherford highlighted the following
issues associated with his observations of the TRRR:
1609
• The interlocked lockout facility on the Main Operator control panel had
NO level of safety designed into it and could have ‘foreseeably failed
dangerously (and undetected) in a single fault condition and would then
not provide any protection against start-up of the ride’.
1610
• The emergency stop located above the Operator panel that stops the
water pumps has NO level of safety designed into it, and only stops the
north pump. It could foreseeably fail dangerously (and undetected) in a
single fault condition and would then not provide any emergency stopping
of the pump.
1611
• Upon opening the Operator panel, a ‘rat’s nest of wiring’ was found, with
some dangling disconnected wires with uninsulated ends. Mr. Rutherford
was of the view that ‘such a poor level of installation could lead to
dangerous malfunctions of the ride including unexpected start-ups and
even unexpected launching of rafts during loading.’
1612
1603
Ex B4(3), pg. 5
1604
Ex B4(3), pg. 5
1605
Ex B4(3), pg. 5
1606
Ex B4(3), pg. 5
1607
Ex B4(3), pg. 6
1608
Ex B4(3), pg. 7
1609
Ex B4(3), pg. 5
1610
Ex B4(3), pg. 6
1611
Ex B4(3), pg. 6
1612
Ex B4(3), pg. 6
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 221 of 274

• From the CCTV footage, it is clear that when the south pump stopped, a
massive and fast backflow of water went into the outlet for which there
was no guarding. If a patron had fallen into the water at such a time, there
was a high likelihood that they would have been drawn into the pump
outlet. Such a hazard could have been identified in a risk assessment of
the ride, with appropriate countermeasures put in place.
1613
862. On 7 July 2017, a further supplementary report was provided by Mr. Rutherford
in relation to the feasibility of a water level detection system being added to the
TRRR safety control system at the same time that the Conveyor Safety Control
System was upgraded in 2016.
1614
863. In relation to the above, Mr. Rutherford noted the following:
1615
• Based on circuit diagrams provided by the new system installer company,
there remained some spare capacity for additional safety sensors/safety
outputs on the ABB Pluto D45 system. These inputs could have been
used had a system to detect water level been installed in the load/unload
area of the TRRR.
1616
• A detection of the sudden lowering of the water level could have been
achieved by a simple arrangement of suitable float switches in a ‘baffled
area’ within the load/unload area. Otherwise, more sophisticated water
level switches could have been made available on the controller by
reconfiguring some of the inputs.
1617
• In either case, a SIL 3 rating for the water level detection system would
have easily been achievable. This would have brought the conveyor to a
safe stop as soon as the water level had fallen to a critical level, thereby
likely avoiding the collision of the rafts which resulted in the fatalities.
1618
864. Mr. Rutherford estimated that the cost of such a water level detection system
being supplied and interfaced with the safety controller already installed,
including dual diverse water level sensors, cabling installation, programming and
testing/validation, would have been around $2000-$3000, had it been carried out
at the same time as the other modifications in February 2016. Mr. Rutherford
confirmed his view that the ‘primary cause of the tragic incident was the lack of
a suitable safety rated water level detection system interfaced to the upgraded
Conveyor system’.
1619
Report by Dr Duncan Gilmore, Managing Director and President of Gilmore
Engineers Pty Ltd
865. For the purpose of the coronial investigation, an independent expert engineering
review and assessment of the TRRR and incident was sought from Consultant
Engineer, Dr Duncan B Gilmore, Director and President of Gilmore Engineers.
An expert advice was subsequently provided.
1620
1613
Ex B4(3), pg. 7
1614
Ex B4(4)
1615
Ex B4(4), pg. 4
1616
Ex B4(4), pg. 5
1617
Ex B4(4), pg. 5
1618
Ex B4(4), pg. 5
1619
Ex B4(4), pg. 6
1620
Ex I
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 222 of 274

866. Dr Gilmore was briefed with a selection of the relevant documentary, expert and
visual exhibits contained within the inquest brief, deemed necessary to provide
an expert opinion as to the questions posed. A schedule of this material was
settled and provided to all of the parties for comment. No objection or submission
to include further material was advised by any of the parties prior to the inquest
hearing.
867. A summary of the general comments made as to the ride and incident, as well
as advice as to the specific questions posed, are outlined below.
General comments as to the TRRR, past incidents and risk assessments
868. Having considered the design of the ride, Dr Gilmore notes that the ride is clearly
dependent on an adequate water level. When this drops, the rafts settle on the
steel supporting rails and cannot travel through the watercourse, which includes
at the end of the conveyor discharge point. This means that rafts can collide
before a raft has cleared the conveyor.
1621
869. Dr Gilmore states that the behaviour of rafts in low water was not understood as
there was no engineering controls on the water level; when it fell only
administrative controls were in place. There was no critical water level for which
the water should not fall below nor an acceptable time for the water level to be
below normal.
1622
870. Dr Gilmore noted that the presence of the unexplained, arbitrary and
unnecessary horizontal 430 mm gap between the end of the conveyor and the
steel support frames in the unload area allowed the raft that flipped to be jammed
within the space. He opines that had this gap not been present, the dynamics of
the incident may have been different, and the raft may have risen up vertically
but not wedged.
1623
This would have been driven by the large slat gap and the
presence of a raft in the unload area. It all originates, however, from a low water
level and low water flow.
871. Dr Gilmore recognised that this particular incident was a ‘high risk, low probability
incident, similar to an aircraft losing engine power or having to ditch in water’.
1624
This type of fault had seemingly not been experienced previously, although pump
failure was not a new occurrence on the ride.
872. Dr Gilmore notes that the probable cause of the incident suggests that there has
been a lack of ‘design mind’ behind the ride, which has been ‘configured to
perform an action without an overall design philosophy’.
1625
The ride had been
extensively modified over the past 30 years, with the original rotating platforms
removed, underwater supporting steelwork frames added, conveyor slats
removed, as well as many other features.
873. In Dr Gilmore’s opinion, the root cause of the incident was a combination of
events, namely an equipment failure (pump), leading to a water level drop, and
a subsequent lack of timely recognition by staff of the importance of this event
combined with shutdown action.
1626
He notes that the incident happened quickly
1621
Ex I, pg. 18
1622
Ex I, pg. 18
1623
Ex I, pg. 18
1624
Ex I, pg. 18
1625
Ex I, pg. 19
1626
Ex I, pg. 18
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 223 of 274

and required the Operators to react quickly to stop the conveyor, amongst the
other tasks of loading and unloading guests. The best remedy, in his opinion,
would have been the installation of engineering controls to monitor the water
level and quickly shut down the conveyor belt should the pump fail.
874. Dr Gilmore further states that the ‘design’ of the ride should have been put
through a rigorous risk assessment process initially when commissioned, and
each time any modification was made, exploring all of the possible operating
scenarios for the ride. The purpose of this would have been to uncover hidden
low probability operating scenarios which may pose a risk to patrons.
1627
875. In relation to Mr. Polley’s assessment of the TRRR 27 days prior to the incident,
Dr Gilmore notes that this was a ‘cursory inspection’ and not a risk assessment
of the design and analysis of the operation of the ride for which a design fault or
the like may be identified.
1628
It seems it was assumed that the ride was safe and
will continue to be operated safely and appropriately.
876. In relation to the JAK audits, Dr Gilmore notes that whilst the level of risk
assessment conducted is somewhat unknown, given no design modifications
were recommended in any of the years they were engaged, it can be confidently
concluded that a full risk assessment of the design and operation was not
conducted.
1629
Dr Gilmore did note that a number of recommendations made by
JAK, particularly in relation to the labelling of buttons, were not carried out by
Dreamworld.
1630
Dr Gilmore notes that pictures of the ride taken at the time of
the incident demonstrates that the buttons at the Main Operator control panel
remained unlabelled.
877. In 2013, JAK recommended that an ‘Emergency shutdown’ procedure be posted
on the wall of the ride and that a simpler process be considered, such as a
singular emergency button. This recommendation was not actioned by
Dreamworld, with the risk being deemed as ‘acceptable’.
1631
878. Having considered a wealth of records provided by Ardent Leisure for the
purpose of the coronial inquiry as to the history of the TRRR, Dr Gilmore
concluded that there was no evidence a thorough risk assessment and
questioning/analysis/review/testing of the design of the TRRR was ever
conducted.
1632
Dr Gilmore stated that:
Based on the ability of the failure of one pump in 2016 to lower
water levels to critical and unsafe values at the unloading zone,
without being safeguarded by an engineering control, an ability
which seemingly has been in place for the 30 year life of the
ride, it is my opinion that a risk assessment of the ramifications
of the design methodology of the ride was never conducted
initially in 1985/1986 during design and construction, and has
not been conducted thoroughly since that time.
1633
1627
Ex I, pg. 20 & 21
1628
Ex I, pg. 6
1629
Ex I, pg. 7
1630
Ex I, pg. 7
1631
Ex I, pg. 7 & 8
1632
Ex I, pg. 8
1633
Ex I, pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 224 of 274

879. With respect to the previous incidents on the TRRR, in particular that which
occurred in 2001, Dr Gilmore noted that:
1634
• No engineering controls were implemented subsequently to prevent such
an impact, and administrative action was instructed.
• The incident in 2001, in Dr Gilmore’s opinion, should have been sufficient
to instigate installation of engineering controls and an investigation of
what caused the rafts to tilt vertically and bunch up at the conveyor exit.
• This experience was first hand at Dreamworld and was available for
implementation immediately and further testing as desired. It was a lost
opportunity not to have followed through and subsequently modified the
design of the TRRR, making it safer for patrons and potentially avoiding
the October 2016 incident.
Specific Issues to be considered
880. Dr Gilmore was requested to consider the following specific issues, the answers
of which are outlined below:
I. Whether the initial construction of the TRRR was compliant with the
requisite Australian Standards in place at the time (as can best be
determined from the material available)? Particular comment is
requested in relation to the appropriateness of the design of the
conveyor slope.
1635
The TRRR was most likely generally compliant with Australian
Standards in place in 1986.
There is no information available as to whether a risk
assessment was conducted by a designer in 1986.
II. Whether the modifications made to the TRRR were in breach of the
requisite Australian Standards particularly those applicable to the
construction of the conveyor and the installation of guiding rail?
1636
The modifications made to the ride, including the removal of the
conveyor slats, removal of the turntable and installation of
supporting steelwork in the water, represent major alterations to
the physical construction of the ride and should have been
configured by a designer or ‘competent person’ with tertiary
engineering qualifications and experience (AS-3533.1-2009 and
AS-3533.2-2009).
In addition, such modifications should have been subject of a
detailed and exhaustive risk assessment investigation, and
should have also been registered with OIR.
1634
Ex I, pg. 10
1635
Ex I, pg. 21
1636
Ex I, pg. 22
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 225 of 274

III. Whether the TRRR, as it was on 25 October 2016, complied with the
requisite Australian Standards in place at the time?
1637
Australian Standards cannot stipulate guidelines for the
construction and maintenance of every type of component which
might be required in an amusement ride. The Standards allow
for individuality by delegating responsibility to a ‘designer’ or
‘competent person’ with tertiary qualifications in engineering and
experience.
Current AS-3533.1-2009 and AS3533.2-2009 both require the
regular risk assessment of the design and any modifications by
a person nominated as the ‘designer’ by the proprietor, or an
appointed suitable ‘competent person’. With respect to the
TRRR, there was no evidence that a thorough risk assessment
and analysis/review/testing of the design of the TRRR was ever
conducted or attempted.
The design and construction of the TRRR did not comply with
the requirements of the Australian Standards in place at the
time.
IV. What risks did the design and construction of the TRRR, including the
various modifications made, pose to patrons?
1638
Given the TRRR operated successfully and injury/fatality free for
approximately 30 years indicates that for the majority of its
lifetime, the design and construction of the ride posed little risk
to patrons. However, as built at the time of the tragic incident, it
is Dr Gilmore’s opinion that the design and construction of the
TRRR in the conveyor/unload zone posed a significant risk to
the health and safety of patrons. The risks include:
o Electrical faults of unknown origin existed in the power
circuit.
o If one pump failed, the water level on which proper
operation of the ride relied dropped dramatically.
o Two-thirds of the conveyor had been removed, which
created a gap into which the rafts might lodge between
the slats and be pushed forcefully by the conveyor,
rather than allow the slats to slip and slide uneventfully
beneath the raft.
o If the water dropped in the unload zone, a raft would
drop and rest on supporting steelwork in the trough,
which prevents a raft from moving forward and away
from the exit region of the conveyor.
1637
Ex I, pg. 22 & 23
1638
Ex I, pg. 23 & 24
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 226 of 274

o When a raft is pushed along forcefully by the conveyor
and came into contact with a stationary raft on the
supporting steelwork in the unload zone, the rear raft
was caused to ride up and over the raft ahead, flipping
it vertically. Once flipped and tilted the raft was drawn
into the gap created between the end of the conveyor
and supporting steel work. Dr Gilmore is of the view that
the gap should never have been present. Had it been
minimal, the raft may have flipped, but the outcome for
the occupants may have been different, although a risk
of bodily crushing injuries remained. Dr Gilmore noted
that ‘being tilted and under threat of being spilled onto
a moving slat conveyor is however a catastrophic event
and one which should have been guarded against
under any circumstances’.
1639
o The seat belts were only ever intended to brace
passengers against inadvertently falling into the water,
with the seats not designed to be in any way protective
for a tipping event.
o The Main Control Panel had no emergency stop button,
which could stop the conveyor.
V. What engineering measures could have been implemented to prevent
a similar incident from happening?
1640
The following engineering measures could have been
implemented:
o Promptly investigate and control electrical faults
occurring in the pump circuit.
o Install a control function to shut down the conveyor if a
pump fails or the water level drops to a critical level
where rafts do not float in the unload area.
o Install a heightened water intake mouth on the pumps
to maintain water level at a satisfactory level if one
pump failed.
o Size the pumps so that the water level can be
maintained on one pump alone.
o Remove supporting steelwork from the unload/load
area trough.
o Install other means of ensuring stable and slow raft
movement in the unload/load areas if required.
o Install proximity sensors in the rafts so that if they
become overly close in the unload zone, the conveyor
1639
Ex I, pg. 24
1640
Ex I, pg. 24 & 25
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 227 of 274

is stopped.
o Reinstall all conveyor slats to ensure that the conveyor
will slip underneath the rafts and not forcefully engage
with their base.
o Install an emergency conveyor stop button at both the
main and unload control panels.
o Consider protective seat structures and seats which will
protect patrons from injury if the raft is tipped.
VI. Were the previous risk assessments and maintenance of the TRRR
undertaken internally by Dreamworld, and those commissioned by
external providers namely DRA, JAKS and Mr. Tom Polley, sufficient to
identify risks associated with the TRRR?
1641
Risk assessments were not commissioned from external
providers DRA, JAKS or Mr. Tom Polley.
JAKS conducted a visual inspection of the ride with respect to
safety and compliance, rather than a risk assessment. Given no
design modifications were recommended in any of the years, Dr
Gilmore confidently concludes that a full risk assessment of the
design and operation was not conducted.
Mr. Polley’s inspection was cursory and not a risk assessment
of the design with analysis and demonstration of the operation
of the ride.
Maintenance conducted by Dreamworld can only be inferred
from the pre-service inspections.
There is no evidence that a thorough risk assessment and
questioning/analysis/review/testing of the design of the
TRRR has ever been conducted.
VII. Please consider the content of the safety bulletin from OD Hopkins
(ODHA 00-1) issued in March 2000 and provide comment on the
content and how it may have applied to this tragic event?
1642
The relevant items from the Bulletin were (1) the need to
immediately activate an emergency stop on a ride if a raft gets
jammed or hung up any way; (2) critical to maintain water levels;
and (3) aviator type seat belts, with Velcro belts also acceptable.
All the items recommended, following incidents on raft rides
carrying guests turned over during the course of the ride, were
nominally enacted by Dreamworld, including an emergency stop
button (which was not readily accessible to the Operator in
charge), the awareness of staff that the water level needed to
be maintained, and Velcro seat belts were in use.
1641
Ex I, pg. 25
1642
Ex I, pg. 26
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 228 of 274

VIII. In light of the tragedy of this incident are there any changes that could
be made to the Australian Standards or present regulatory system for
amusement rides in Queensland which may prevent a similar incident
from happening in the future?
1643
Current WHS Regulations and Australian Standards as are in
place are adequate.
Changes are required to the tightening of the checking and
enforcement process i.e. full risk assessments and inspections
are actually conducted and fully reported, recommended
engineering, administrative and protective equipment controls
are properly implemented together with documentation of the
history and maintenance. This could be performed by having the
requirements independently certified annually by an RPEQ in a
similar manner to the annual inspections for mechanical and
structural adequacy, together with random spot checks of
documentation by WHS Queensland.
Evidence suggests that prior to 2016, the system of ensuring
compliance of amusement rides with Australian Standards and
WHS Regulations had been unsuccessful at Dreamworld.
IX. In your opinion are there any other issues arising from this tragic event,
which need to be considered and addressed in order to ensure a similar
incident that can occur in the future? If so what measures need to be
undertaken?
1644
Dr Gilmore recommended the following measures:
o Initiate a formal document and control systems for each
ride. Appoint a ‘designer’ or ‘competent person’ for
every ride, registered with WHS Queensland, with
tertiary qualifications in engineering and experience.
o An external party (RPEQ) to be used to conduct
independent risk assessments.
o Specify that a full risk assessment on the whole ride be
conducted at least every 5 years or each time new
hardware/electrical modifications or
additions/subtractions are performed.
o Spot checks by OIR to ensure proper conduct and
thoroughness.
o Regulations should make it clear the onus placed on the
RPEQ when conducting an annual inspection or a risk
assessment.
o The operation of the ride should be visually observed
during a risk assessment.
1643
Ex I, pg. 27
1644
Ex I, pg. 28 & 29
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 229 of 274

o Look for probability failures – the excuse that the ride
has been trouble free for 30 years is not an acceptable
excuse. History shows that low probability coincidences
often turn out to be the cause of a major unexpected
incident.
o Observe how the machine handles adverse events.
o Consult Theme Park records internally and
internationally.
o Look at design records.
o New designs should be documented to reveal the
design methodology, what was considered, safety
considerations, log and register with WHS Queensland
to keep centrally.
o Testing must be carried out and be comprehensive.
ENGINEERING EXPERT CONCLAVE
881. The expert engineering evidence in relation to this incident was heard
concurrently during the inquest by way of a conclave. Accordingly, Dr Frank
Grigg, Dr Duncan Gilmore and Mr. George Rutherford gave evidence as a panel,
and a joint expert advice was tendered.
1645
Joint Engineering Expert Advice
882. Following the provision of further short answer written responses by each of the
experts,
1646
and a teleconference with Counsel Assisting, a joint advice opinion
was provided by Dr Grigg, Dr Gilmore and Mr. Rutherford. It was acknowledged
that given the differing areas of engineering expertise, the opinions expressed
by Mr. Rutherford in answer to the questions posed were limited to Risk
Assessment Concepts, Safety Related Control Circuit Concepts and Electrical
Safety Concepts. Statements made, which were not specifically attributed to Dr
Grigg or Dr Gilmore, were intended to be read as opinions shared, given their
area of practice and expertise.
883. Relevant excerpts from this advice, as well as the evidence provided during the
inquest proceeding, is summarised below.
(1) Whether the initial construction of the Thunder River Rapids Ride was compliant
with the requisite Australian Standards in place at the time?
Standard in place at the time of construction
884. It was agreed amongst the experts that there was no key applicable Australian
Standard (AS) in place at the time the TRRR was commissioned in 1985/1986.
The first edition of the AS-3533: Amusement Rides and Devices was published
in 1988. Section 1.3.20 relates to Amusement Rides and Devices, including ‘Raft
1645
Ex I5
1646
Ex I2-4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 230 of 274
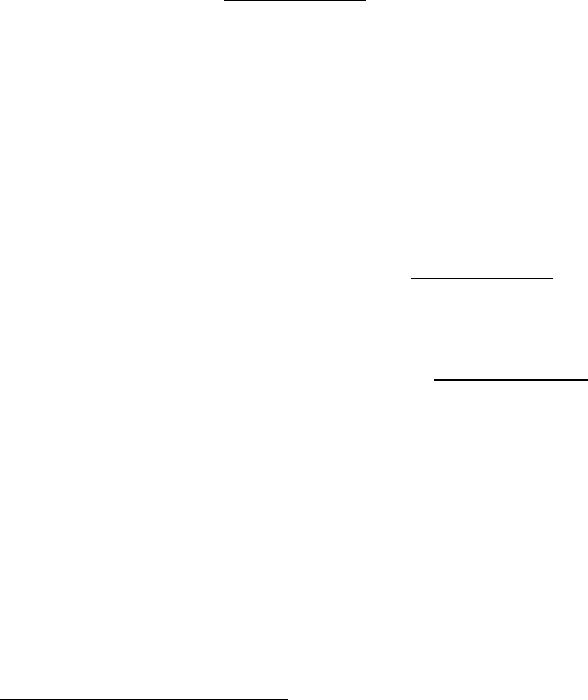
Rides’ like the TRRR.
1647
Accordingly, the ride was required to satisfy the District
Inspector, OIR that it complied with other safety standards, which it appears to
have done based on the material available in relation to the initial design and
registration.
1648
885. Mr. Rutherford is of the view that no similar standards (which are now current for
the area of Safety Related Control Circuits) existed at the time of the initial
construction of the TRRR. However, traditional ‘electro-mechanical’ type
interlocking & non-safety controllers (of a lesser level of reliability compared to
equivalent systems used today) were already in existence, and may well have
been applied.
1649
He further notes that with respect to electrical safety
requirements, which were in place at the time, such as the National Wiring Rules,
would have likely resulted in adequate electrical safety had it been installed to a
professional standard. Mr. Rutherford is of the view that the Safety Related
Control Systems and Electrical Safety of the TRRR were probably in line with
standard practices at the time of initial construction, however, have become non-
compliant with current practices over time.
1650
AS-3533 - 1988
886. Upon release of AS-3533-1988, the view shared by the experts was that best
practice would have been to ensure the TRRR complied with the Standards,
although no action was mandated.
1651
887. At inquest, Dr Grigg further explained that ‘best practice’ in this instance would
have been to take all precautions suggested in the Standard, even if they weren’t
mandatory, with a common sense consideration of the risks present for the ride
and rectification by way of engineering solutions where possible.
1652
Dr Gilmore
further noted that ‘best practice’ would be to take the most updated advice given
in relation to safety, per the Standards.
1653
888. With respect to the requirements of AS-3533-1988, the following were noted in
relation to the TRRR:
1654
i. It appears on the documentation available that the TRRR would
have complied with the AS-3533-1988 design requirements for
Rafts (s. 4.4.10) and Flumes (s. 4.4.10.2) when the ride was first
opened. However, Dr Gilmore noted s.4.4.10(b), which stipulated
that the depth of the water in the flume shall be the minimum
necessary to maintain floatation of the raft when fully loaded, does
not appear to have been adhered to. The water course on the TRRR
was substantially deeper than that necessary for floatation and
increased the risk of drowning. Dr Grigg notes, however, that the
water depth near the head end of the conveyor may have been
greater than that in other parts of the ride due to the horizontal
discharge of the original pump.
1647
Ex I5, pg. 1
1648
Ex I5, pg. 1; T30-20, lines 1-30
1649
Ex I5, pg. 1 & 2
1650
Ex I5, pg. 1 & 2
1651
Ex I5, pg. 2
1652
T30-20, lines 28-45
1653
T30-21, lines 1-5
1654
Ex I5, pg. 2
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 231 of 274
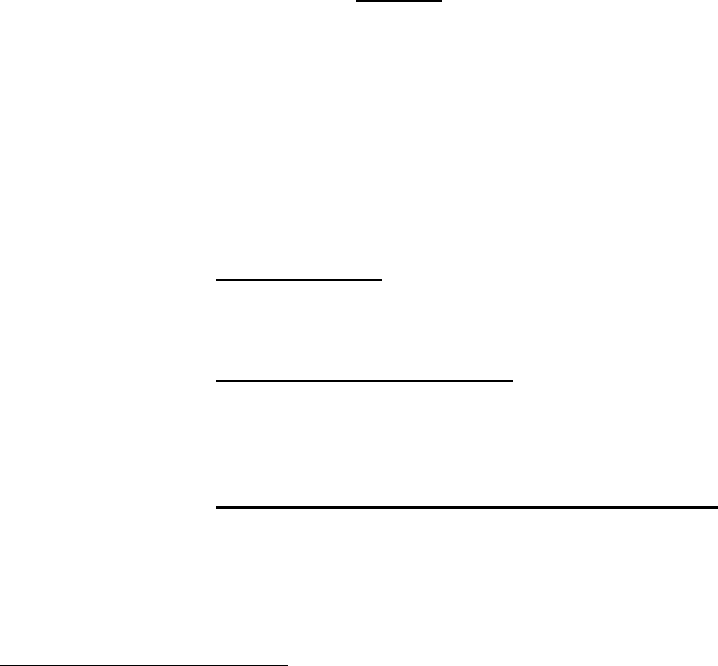
ii. It is unknown whether the TRRR would have complied with AS
section 7: Maintenance and Inspection, particularly those pertaining
to Logbook (s. 7.5), Section 9: Information provided by the
manufacturer, and Section 10: Marking. At inquest, the experts
agreed that it was unclear as to compliance in this regard due to the
lack of documentation available, kept or retained in relation to the
TRRR.
1655
iii. Given the loading and unloading components of the ride design
when first commissioned involved a turntable, which was removed
at some time before 1998, it cannot be determined whether the
original installation would have provided unrestricted views of all
embarkation and disembarkation stations, as was required by
Section 3.13: Controls Stations.
iv. Having considered the control arrangements found in place after the
tragic incident, it appears that the Operator at the Main Control
Panel may not have had safe control of all functions in an
emergency, per s.3.13(c), which includes the absence of an
emergency stop button for the conveyor. Additionally the “Conveyor
Stop” and “Emergency Stop” (which only Stopped the North Pump)
and likely all other “safety functions” (e.g. Raft Release etc) were
not designed/implemented as “safety related features” but were of
low reliability and subject to failure in the case of a single fault
occurring.
v. No edition of the AS-3533 applicable to Design and Construction
(1988 or subsequent) deals directly with the design, construction of,
or modifications to a conveyor.
(2) Whether the modifications made to the TRRR were in breach of the requisite
Australian Standards, particularly those applicable to the construction of the conveyor
and the installation of the guiding rail?
889. The experts found that the known mechanical modifications to the TRRR, which
are relevant to the incident, were as follows:
1656
i. Conveyor slats: Whilst it seems that every second slat of the
conveyor was removed in 1989/90, it is unclear when the
removal of every third slat took place.
ii. Removal of the Turntable: It appears that the turntable
passenger loading and unloading device was removed in the
early 1990’s, with the support rails in the unload area being
installed at the same time.
iii. Addition of raft support rails in the unload area: Whilst the
specific date of the installation of the support rails downstream
from the conveyor is unknown, it seems that these may have
been put in place at the time of the removal of the turntable. It
was noted, however, that the rails in place at the time of the
incident were younger than expected, and therefore may have
1655
T30-21, lines 5-38
1656
Ex I5, pg. 2 & 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 232 of 274
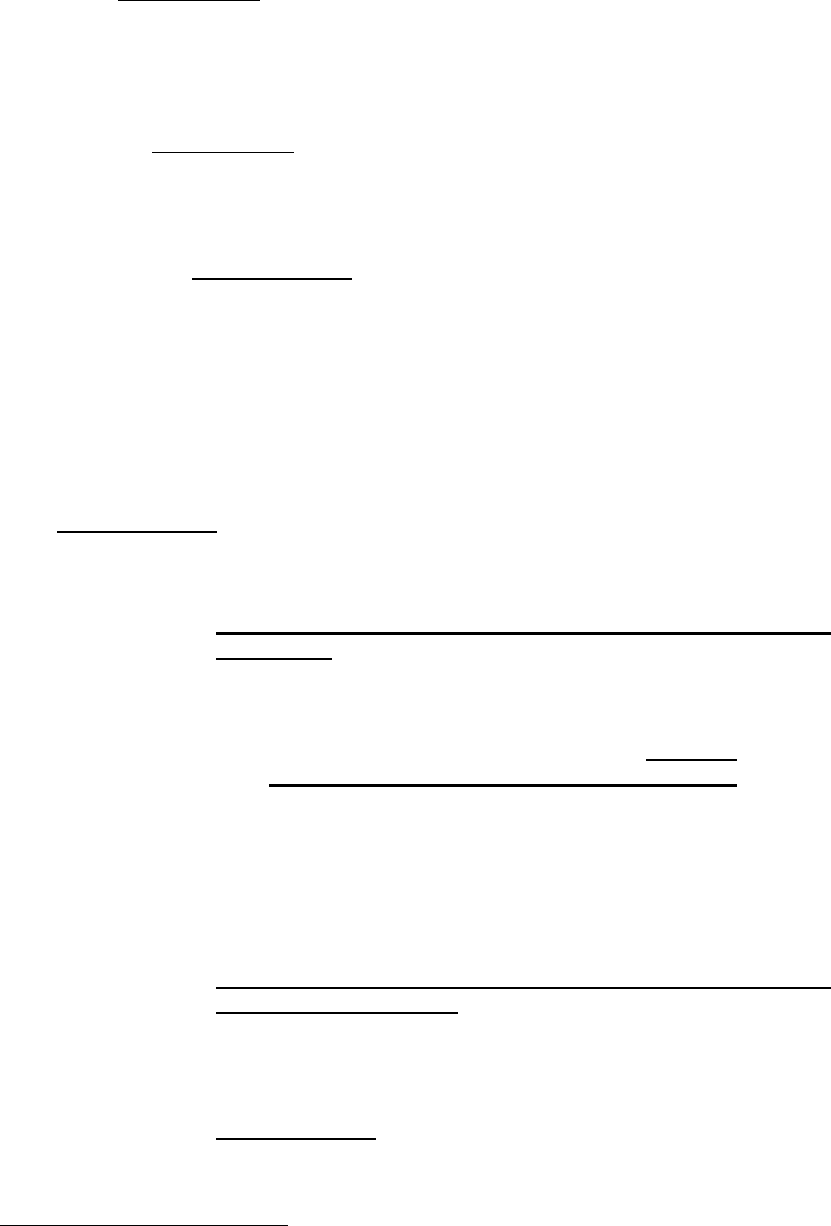
been replaced and/or moved since the original installation.
890. It appears probable that the majority of the modifications were made to the TRRR
when AS-3533-1988 was in place.
1657
Accordingly, reference to modifications
was made in Appendix H: Statutory Approval, Section H4 – Modification and
Alterations, which states that modifications, which may cause increased stresses
or ‘otherwise affect safety’, are deemed to make the unit a new model and new
approval may be required.
891. In 1997, AS-3533-1988 was expanded to include Hazard Identification, risk
assessment and risk control measures (s.2.2). Accordingly, if the modifications
to the TRRR were made before the introduction of the 1997 Standard, there was
no strict requirement for a reassessment of the safety of the TRRR, unless further
modifications made were considered to constitute a redesign, pursuant to the
application of AS-3533.1-1997.
1658
892. The experts were of the view that in modifying the original design of the conveyor
(removal of the slats) and the installation of the support railing at the unload area,
a “designer” should have consulted with a documented risk assessment of the
hazards envisaged to be introduced or altered undertaken. These alterations
would have amounted to a new design, and should have been re-registered with
the Regulator. Notification of these modifications should have been made to the
Regulator.
1659
893. AS-3533.2-1997 described the requirements for the operation, maintenance and
inspection of fixed amusement rides and should have been considered in relation
to the TRRR. Specifically,
i. Section 5 – Maintenance, Replacement, Repair and
Inspection – specifically, s.5.1, which includes:
….
Following major maintenance and repair, and at
random intervals on other occasions, a hazard
identification and risk assessment procedure
should be completed to ensure new hazards are
not present, and residual risks identified by the
designer or manufacturer are not increased.
NOTE: A typical hazard identification and risk
assessment procedure is given in Appendix F.
ii. Appendix F – Hazard Identification, Risk Assessment and
Risk Control Process – This Appendix explicitly details
Mechanical Hazards for consideration as part of the hazard
identification and risk assessment process, which includes
those involving crushing, shearing and entanglement.
AS-3533.2-2009 provides almost identical guidance as that
provided in Section 5.1 of 1997 Standard, with more substantial
guidance provided for in Appendix F, and reference directly to
1657
Ex I5, pg. 3
1658
Ex I5, pg. 3
1659
Ex I5, pg. 3
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 233 of 274
AS 4360-1995 – Risk Management.
894. It was agreed by the experts that AS 3522.2-1997, s.5.1 should have triggered a
mechanical hazard identification and risk assessment of the TRRR on a number
of occasions during the operating period after the 1997 edition of the Standard
was in place.
1660
If a hazard identification and risk assessment procedure, as per
the recommendation of Section 5.1, had been completed following the
implementation of any of the relevant modifications, it is most probable that some
safety issues associated with at least the removal of the full width conveyor slats
and the installation of the support rails, would have been identified.
1661
895. At inquest, it was agreed that s.5.1 essentially reflected what was ‘best practice’
for amusement device owners at the time in relation to the process to be
undertaken should any modifications be made to the ride.
1662
896. Given the TRRR 1991 Operator Procedure Manual identified the events ‘loss of
power to one or both pumps’ and ‘person in the water’ as ‘emergency situations’,
consideration should have been given to mechanical hazards associated with
these situations in any hazard identification and risk assessment, regardless of
the requirements of the Australian Standards or Regulations.
1663
Such an
assessment would have considered the underwater risks to a “person in the
water”, of which some of the obvious include:
A. The excessive gap between the full width conveyor slats
posed a significant risk of injury to any person who fell
onto the conveyor whilst it was in operation;
B. The area between the head of the conveyor and the
support rails posed a significant mechanical hazard;
C. The clearance between a moving raft and the support
rails was a shear/pinch point; and
D. The support rails could have been considered an
entrapment hazard.
ii. If the event of ‘loss of power to one or both pumps’ had been
risk assessed, it should have indicated that when the water level
dropped:
A. The ride would have been operating outside of its design
envelope and there was at best a significant risk of
property damage or at worst a significant risk of injury to
patrons.
897. Given the unclear history for the various changes (both electrical and
mechanical) that have occurred over the years since the initial installation of the
TRRR, it appears that most of the ride has been modified in an undocumented
way with little or no consideration being given to the effect of safety via a detailed
and formal risk assessment process. As such, hazards were never identified by
1660
Ex I5, pg. 4
1661
Ex I5, pg. 4
1662
T30-21, 22 lines 1-20
1663
Ex I5, pg. 4
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 234 of 274
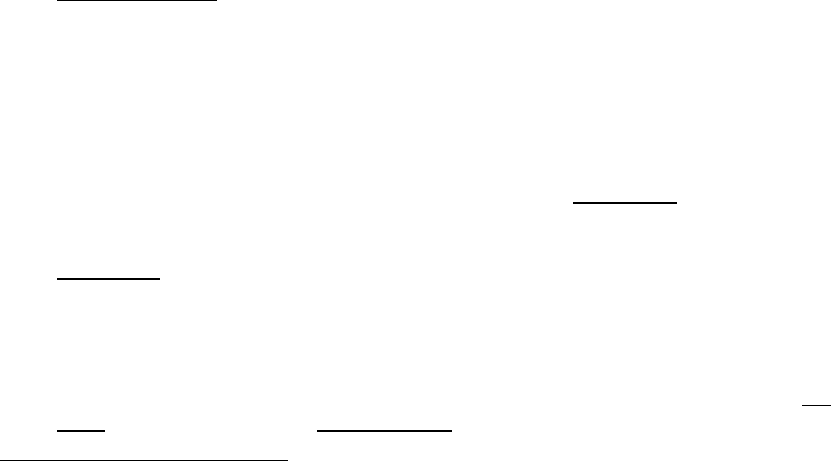
a designer with a risk assessment being undertaken.
1664
898. In relation to the importance of risk assessments for amusement rides, during
the inquest, Dr Grigg noted that:
1665
…the important thing about doing a risk assessment is to try
and think about the possibilities of what could happen under
virtually all circumstances, and to take appropriate action to
minimise those risks. In some cases, it mightn’t be possible
to completely eliminate a risk.
But you’ve got to be aware of what the risk is and you may
need – if you can’t come up with an engineering solution, it
may be that you’ve got to rely on some sort of administrative
control by putting – having people telling patrons what
they’ve got to do and what they’ve got to look out for, or
something…
But nevertheless you’ve got to identify that the risks exist.
899. All of the experts concurred that the previous incidents on the TRRR, particularly
in 2001 and 2014, should have alerted Dreamworld to the hazards present on
the ride.
1666
These incidents should have prompted a thorough risk and hazard
assessment of the ride, including the design, looking beyond the circumstances
of the incident. In accordance with the hierarchy of controls, elimination of the
risk, plant and engineering controls should have been considered as solutions to
identified hazards before administrative controls.
1667
(3) Whether the TRRR, as it was on 25 October 2016, complied with the requisite
Australian Standards in place at the time?
900. AS-3533.2-1997 and subsequent editions describe the recommendation in
section 5.1 for hazard identification and risk assessment (including mechanical
hazards) to be performed at reasonable intervals, and the requirement of the
involvement of ‘competent persons’ in these tasks. It also describes other
maintenance, replacement, repair and inspection activities. The documentation
available in relation to the TRRR clearly shows that whilst a number of audits
and ‘risk assessments’ were performed on aspects of the ride, the identification
and assessment of mechanical hazards was rarely considered and when it was,
it was not considered to the extent recommended by AS-3533.2.
1668
901. It is clear that the maintenance documentation, including logbook records (s.5.5
AS-3533.2) did not comply with the Standard, and because of this, relevant
information regarding modifications and alterations were not communicated to or
assessed by competent persons.
1669
902. There were no directly relevant safety designs applicable to the conveyor at the
time of the incident of concern. Mr. Rutherford further noted that although the AS
1755 (now superseded by AS/NZS 4024 Parts 36XX), which covers conveyors,
1664
Ex I5, pg. 4
1665
T30-23, lines 2-25
1666
Ex I5, pg. 4; T30-35, lines 8-47
1667
Ex I5, pg. 4
1668
Ex I5, pg. 5
1669
Ex I5, pg. 5
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 235 of 274

states that conveyors specifically designed to carry people are not covered by
these Standards, any Risk Assessment carried out under the AS/NZS 4024
(Safety of Machinery) should have identified the pinch/draw-in/shear hazards at
the end of the conveyor.
903. Mr. Rutherford notes that other than the modifications made to the Conveyor
Control System by PFI, other parts of the TRRR Safety Related Control System,
including existing controls for the ‘Prevention of Start-Up’, ‘Water Pump
Emergency Stop’, ‘Conveyor start/stop’ and possibly other “safety features” (e.g.
Raft Release etc) at the Main Operator Panel were not in compliance with the
Standards for Safety Related Control Circuits at the time of the incident.
Additionally, the state of the electrical wiring within the Main Operator control
panel and apparent lack of documented electrical circuit diagrams and critical
components list could have impacted on the safety of the ride during any
maintenance and modifications being performed.
1670
(4) What risks did the design and construction of the TRRR, including the various
modifications made, pose to patrons?
904. It was recognised by the experts that the TRRR had operated successfully and
injury/fatality free for almost 30 years. As such, for a majority of its lifetime it
seems that the general design and construction of the ride may have posed little
risk to patrons. However, at the time of the fatal incident, the design and
construction of the conveyor and unload area posed a significant risk to the
health and safety of patrons.
1671
Specific hazards associated with the design and operation of the TRRR:
905. As it was at the time of the incident on 25 October 2016, the experts agreed that
the design and construction of the TRRR in the conveyor/unload zone posed a
significant risk to the health and safety of patrons.
1672
906. The following specific hazards associated with the design and operation of the
ride were identified:
1673
i. The wide spacing of the slats of the conveyor would have
created a much greater risk of injury to a person who had
fallen into the water in the vicinity of the conveyor or had
otherwise interacted with the conveyor whilst it was
operating. This spacing of slats also gave rise to the risk that
the plug of a raft would engage on a slat causing the raft to
be pushed forward positively, rather than simply slipping and
sliding uneventfully beneath the raft, in the event of the
forward movement of the raft being obstructed.
ii. The gap between the slats at the head end of the conveyor
and the steel support frame was much larger than
necessary. This gave rise to the flotation collar of raft
number 5 being able to fit into the gap when the raft tilted;
and this resulted in the occupants of the rear seats of the raft
1670
Ex I5, pg. 5
1671
Ex I5, pg. 5
1672
Ex I5, pg. 5
1673
Ex I5, pg. 5-7
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 236 of 274
being struck by the slats of the conveyor. Had the gap been
minimal, the raft may have flipped and the occupants jostled,
but the outcome may have been somewhat different. Being
tilted and under threat of being spilled onto the moving slat
conveyor is a catastrophic event and one which should have
been guarded against under any circumstances. Falling
towards the slat conveyor which is powering onwards can
only lead to body crushing injuries.
iii. The head end of the conveyor being unguarded would have
created a high risk of injury to a person who had fallen into
the water in the vicinity of the conveyor or otherwise
interacted with the conveyor whilst it was operating.
iv. The installation of the steel support frame and rails would
have created a much greater risk of injury to a person who
had fallen into the water by creating pinch/shear points with
the raft movements and also increasing the probability of
entanglement and drowning. However, it is recognised that
the frame probably assisted in stabilising the rafts at the load
and unload stations as well as being of assistance when
inspecting the undersides of the rafts.
v. Electrical faults of unknown origin existed in the pump power
circuit. These occurred randomly.
vi. If one pump failed, the water level on which proper operation
of the ride relied dropped dramatically and quickly at both
the unloading and loading stations.
vii. If the water level dropped in the unload zone, a raft in that
zone would drop and rest on steel support frame, which had
been installed in the trough. This undoubtedly allowed
patrons to disembark safely if the water level was low, but it
stopped the raft moving forwards and away from the exit
region of the conveyor, creating a blockage.
viii. From the information provided, it is unable to be determined
whether the removal of the turntable at the unload area of
the TRRR increased the risk of exposing patrons to
mechanical hazards. Information available suggests that the
operation of the turntable may have reduced the Operator
workload, and lessened the risk of rafts jamming or colliding
in the unload area. However, without more detailed
information as to the construction of the turntable, the
comparative level of risk cannot be adequately determined.
ix. It appears that the seat belts were only ever intended to
brace passengers against inadvertently falling into the water
as the raft travelled around the waterway on rough waves.
The seats were not designed to be in anyway protective for
a tipping event i.e. they were not steel reinforced so that they
might protect their occupants and cause the conveyor to stall
rather than crush both the seats and patrons.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 237 of 274
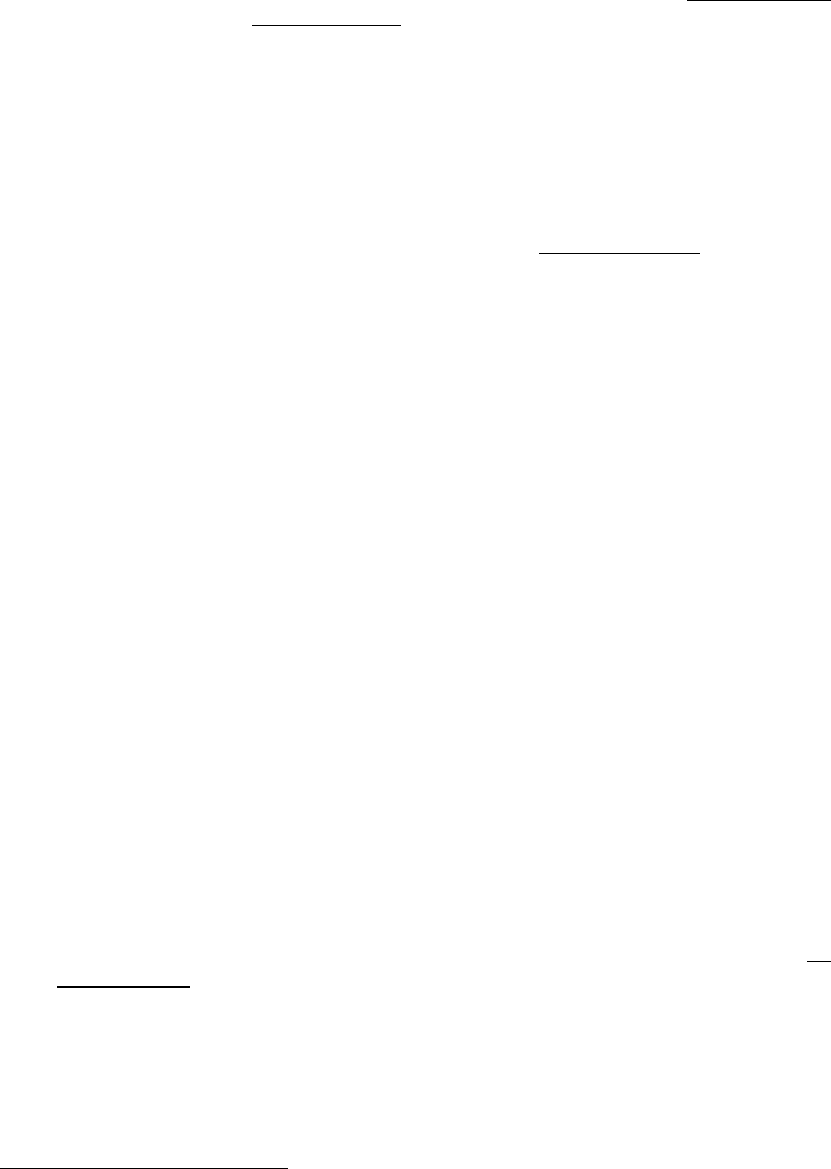
x. The Main Control Panel had no emergency stop button,
which would stop the conveyor immediately.
xi. Mr. Rutherford notes that parts of the TRRR Safety Related
Control System, including existing controls for ‘Prevention of
Start-Up’, ‘Water Pump Emergency Stop’, ‘Conveyor
start/stop’ at the Main Operator Panel were not in
compliance with the Standards for ‘Safety Related Control
Circuits’ at the time of the incident. They were not designed
to have any particular level of safety reliability and could
have malfunctioned in the case of a single foreseeable fault
condition. The “Conveyor Stop” function at the Main Control
Panel was not designed as a “safety stop”. It is designated
as a Category 2 Stop under AS/IEC 60204-1, which could
fail to stop the conveyor in a single fault condition.
907. It was noted by Dr Gilmore during the inquest that none of the other comparable
international rides had a similarly configured conveyor to the TRRR. Rather, the
slats were closer together preventing a person from falling through into the water
or mechanism.
1674
Dr Grigg notes that it is unknown why the gap in this area is
so big, and he suspects that it was done without anyone considering the
implications.
1675
908. Dr Grigg and Dr Gilmore both agreed during the inquest that any competent
person conducting a risk and hazard assessment of the ride would have easily
identified a risk associated with the slat spacing, as well as the other aspects of
the formation of the ride as outlined above.
1676
All of the experts strongly rejected
any suggestion that their conclusions in this regard as to the obvious nature of
the hazards on the ride were influenced by ‘hindsight biased’ or knowledge of
the tragic incident.
1677
909. Mr. Rutherford highlighted during the inquest that the changes and modifications
made to the TRRR over its 30 years in commission not being documented was
a ‘major issue’.
1678
(5) The cause of the incident on the TRRR
910. In general terms, the experts were of the view that the incident occurred as a
result of an equipment failure (south pump), leading to a water level drop,
following which the conveyor was not stopped.
1679
911. The experts agreed that the following sequence of events transpired on 25
October 2016:
i. Drop in the water level due to failure of the southern pump.
ii. Continued operation of the conveyor.
iii. Contact between the Raft (#5) and the lead raft (#6).
1674
T30-25, 26, lines 1-35
1675
T30-31, lines 20-30
1676
T30-31, lines 1-45
1677
T30-144-147
1678
T30-68, lines 2-5
1679
Ex I5, pg. 7
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 238 of 274

iv. Forceful engagement of the Raft (#5) by the conveyor.
v. The lead raft (#6) snagged on support frame.
vi. Raft (#5) entered gap between conveyor and support frame.
912. It was the view of the experts that if any of the above events had been avoided,
the incident would not have occurred. It is considered that a change of any one
of the engineering measures identified in Question 6 would probably have
prevented the disastrous outcome. Significantly, whilst the water level drop
was a primary cause of this incident, there were multiple other hazards
evident on the ride, as outlined previously (conveyor slat removals, nip
point etc.), which could have caused other catastrophic incidents to occur
at any time.
1680
913. Dr Grigg also noted that Raft #6 was heavily loaded towards the front and very
lightly loaded at the rear. Raft #5 was heavily loaded at the rear. These
distributions may have contributed to the interactions that the lead raft (#6) had
with the support frame, and Raft #5 had with the conveyor. Differences in raft
passenger weight distribution may in part have explained why a similar incident
did not occur in 2014, when rafts came into contact at the same location.
1681
914. The experts also noted that a number of human factors associated with the
failure of the procedures to enable a rapid response to an emergency situation
also appeared to have contributed to the tragic outcome, including:
1682
i. Delay in action because of the procedural requirements of
Operators, including the multitasking required of the No. 1
Operator and the requirement of the No. 2 Operator to alert
the No. 1 Operator.
ii. Inadequate alarms to alert the No. 1 Operator.
iii. Multi-step shutdown procedure, which caused a delay in
isolating critical machinery (conveyor).
iv. The memorandum, dated 18 October 2016, requiring the
Unload Platform E-Stop only to be pressed if the Main Control
Panel cannot be reached.
v. Insufficient training of the Operators, especially in actions
required in an emergency situation.
vi. Inadequate recognition or downgrading of what constitutes an
emergency. In the June 2016 edition of the Operators
Procedure Manual, the only identified emergency event was
person in water and/or raft capsized.
915. Dr Gilmore noted that, in his opinion, the root cause of the incident was that a
combination of events occurred for which the outcome was uncertain and
unknown. Staff (operational and technical design and maintenance), as well as
1680
Ex I5, pg. 7; T30-41 & 42
1681
Ex I5, pg. 7 & 8
1682
Ex I5, pg. 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 239 of 274

auditors and annual inspectors had never been alerted or aware that this
combination of events could pose a threat. The ride design should have been
put through a rigorous Risk Assessment process initially when commissioned,
and each time any modification was made, exploring all possible operating
scenarios for the ride.
1683
916. Dr Gilmore further stated that the TRRR was internally manufactured, as
opposed to being purchased from an international manufacturer, the onus for
identifying necessary periodical safety upgrades, thoroughly analysing and
documenting the implications of any modifications to equipment, and conducting
risk management audits would rest totally with the owners of the TRRR.
1684
(6) What engineering measures could have been implemented to prevent a similar
incident from happening?
917. The experts were of the view that a number of engineering measures could have
been implemented to prevent a similar incident from occurring. Namely:
1685
(a) Installation of a control function to shut down the conveyor if a pump
fails or the water level drops to a critical level where rafts do not float
in the unload area. Mr. Rutherford noted that had there been an
appropriately safety rated, designed and installed automated
detection system for the water level as of the date of the incident,
which was suitably interfaced to the Conveyor Safety Control
System, the tragedy may have been avoided. Such water level
sensing systems are now common place on modern rides and can
be easily retrofitted in cases that their existence will enhance safety
on older rides. Other means of stopping the conveyor movement in
the event of a drop in water level, such as interfacing to the Pump
Operation circuits, could also have achieved a similar safe result.
(b) Size the two pumps so that the water level can be maintained on one
pump alone. Dr Grigg noted, however, that the two pumps installed
are very powerful, and it is considered likely that for power supply
reasons it was necessary to use two pumps so that their starting did
not occur simultaneously and thereby create a very substantial peak
load on the power supply. It is not apparent that one pump would be
more reliable than two.
(c) The E-stop for the conveyor at the unload station should have been
clearly labelled, and its function should have been duplicated at the
Operator’s control station so that in an emergency the conveyor
could be stopped as quickly as possible.
(d) A central longitudinal member in the steel support frame may have
moderated the degree of obstruction of the forward movement of raft
number 6, thereby reducing the risk of the lead raft snagging and the
rafts tipping up. Alternatively, removal of the supporting steelwork
from the unload/load area trough could be considered. However, it
was noted that the removal of this steelwork may have resulted in
undesirable instability of the rafts during unloading and loading.
1683
Ex I5, pg. 8
1684
Ex I5, pg. 8
1685
Ex I5, pg. 9
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 240 of 274
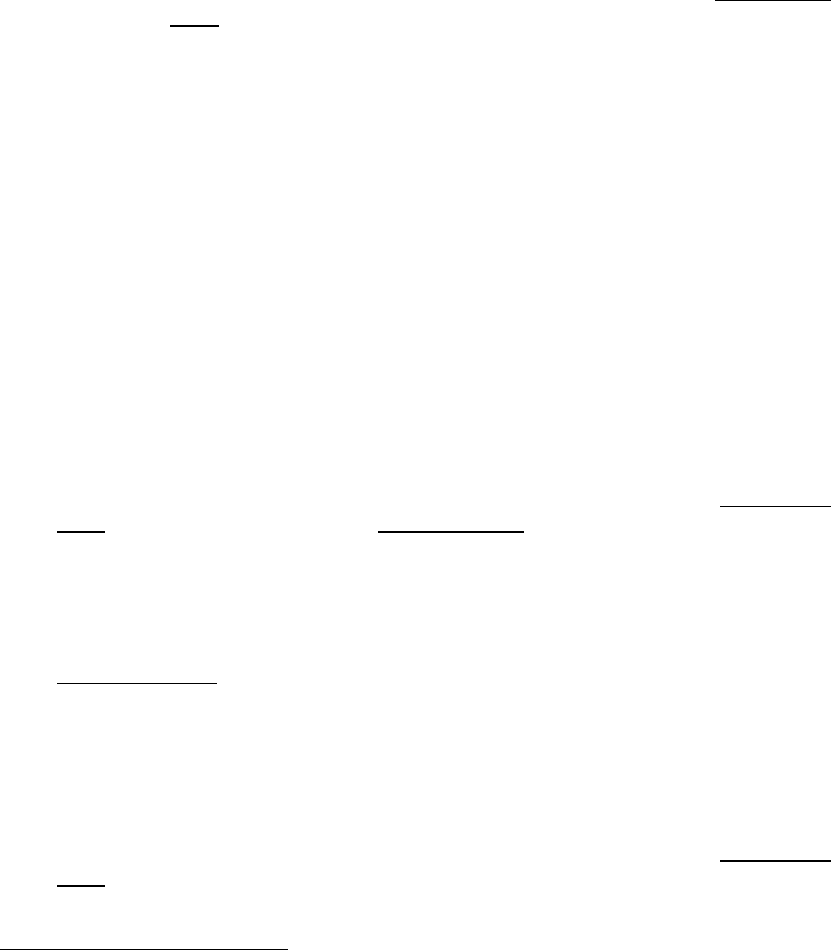
(e) Dr Gilmore suggests the installation of other means of ensuring
stable and slow raft movement in the unload/load areas if required,
to prevent rafts from becoming stationary in the unload area. Dr Grigg
questions the cost effectiveness of such an arrangement.
(f) The spacing of the slats on the conveyor should have been much
closer or an alternative conveyor design used.
(g) The gap between the slats at the head end of the conveyor and the
steel support frame should have been only sufficient for reliable
operation, and probably no more than about 100mm.
(h) Consider protective seat structures and seats, which will guard
patrons from injury if the raft is tipped. The seat belts must be quick
release, however, as the danger of drowning persists. AS3533.1 –
2009 section 2.8.10.4.1, specifically prescribes quick release fittings
only with no metallic buckles. Dr Grigg was of the view that properly
installed aircraft style lap seatbelt with a positive latching mechanism
should have been used instead of the Velcro belt.
(i) Install proximity sensors in the rafts so that if they become overly
close in the unload zone, the conveyor is stopped. Dr Grigg,
however, questions whether this would achieve the desired outcome.
(j) Promptly investigate and correct electrical faults occurring in the
pump control circuit.
(7) Were the previous risk assessments and maintenance of the TRRR undertaken
internally by Dreamworld, and those commissioned by external providers namely
DRA, JAKS and Mr. Tom Polley, sufficient to identify risks associated with the
TRRR?
918. The experts unanimously agreed that the response to this question was no.
1686
The risk assessments, maintenance and inspections of the TRRR described in
the brief were insufficient and did not meet the recommendation of AS-3533.2-
1997 (and later editions) or AS/NZS 4024. This was because Hazard
Identification and Risk Assessment Procedures (s. 5.1 and Appendix F) were
lacking. It is not clear who was nominated as the qualified ride ‘designer’ or
‘competent person’ with responsibility for the design overview and initiation of all
ongoing modifications.
919. AS-3533.2-1997 separately describes the requirement for Annual inspections (s.
5.4.2) and the recommendation for Hazard Identification and Risk Assessment
Procedures (s. 5.1 and Appendix F). There was no indication in the records
produced by Ardent Leisure of an ‘Annual Inspection’ as defined by the Standard
having been performed prior to 2016.
1687
920. The experts agreed that Mr. Polley’s inspection in 2016, would have met the
general requirements for an ‘annual inspection’ as described in AS-3533.2-
2009.
1688
However, his inspection was cursory in nature and not a risk
assessment of the design with analysis and demonstration of the operation of
1686
Ex I5, pg. 10
1687
Ex I5, pg. 10
1688
Ex I5, pg. 10
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 241 of 274
the ride, which was not required by the Standard.
921. On the material provided, which is scant, poorly recorded and entirely
inadequate, there does not appear to have been any risk assessments of the
operating procedures and the physical functioning of the TRRR and its controls
other than by JAK. However, the scope, level of risk assessment and audit tools
used by JAK are largely unknown, with no reference made to AS-3533.
1689
It
does appear that the audits consisted of visual inspections of the rides with
respect to safety and compliance. However, given that no design modifications
were recommended in any year (such as comments on water depth, pump
reliability, steel frames in the troughs, conveyor design, conveyor slat
design/replacement, seat belt reliability), it can be confidently stated that a full
risk assessment of the design and operation was not conducted by JAK. It was
noted that JAK appear to have been the only external assessors to have
considered the functioning of the controls, however, some of their
recommendations were not acted upon.
922. The focus of Mr. Polley and DRA appear to have been on the maintenance and
structural condition of the ride, and related management documentation, as dealt
with in AS-3533 Parts 2 and 3, rather than on the design aspects as to the rides
fitness for purpose and safety as a system when operating.
1690
923. Mr. Rutherford noted that a ‘visual’ inspection of the external areas only (e.g.
Main Operator control panel area) may indicate that an adequate set of safety
features are in place as the ‘Prevention of Start-Up’ interlock switch was an
approved switch intended for safety applications, and the Emergency Stop was
the required RED/YELLOW colour. However, this will not reveal that the internal
components used and interfaced to, as well as the configuration, provide an
actual safety level. This can only be determined by a person with adequate
knowledge of Safety Related Control Circuits, along with reference to up to date
Circuit Diagrams and detailed CCL (Critical Component List), neither of which
appear to be in existence for the TRRR at the time of the incident, other than in
the case of the PFI 2016 modification.
1691
(8) In light of the tragedy of this incident, are there any changes that could be made
to the Australian standards or present regulatory system for Amusement Rides in
Queensland, which may prevent a similar incident from happening in the future?
924. The suggested changes to the current regulatory system in Queensland to
ensure a similar incident doesn’t happen again, as recommended by the experts,
are outlined below. I accept that those recommendations should be adopted.
925. It was recommended that Annual Risk assessments of amusement devices
should be required to include detailed examination of the operation of the ride
during all modes of operation and possible emergency conditions.
1692
The
assessment should include all possible control system functions and variations
and it is likely that it would require assessment by both competent mechanical
and electrical engineers. At inquest, the importance of this detailed consideration
of the device was said to be necessary given the complexity of the machine.
1693
1689
Ex I5, pg. 10
1690
Ex I5, pg. 10
1691
Ibid.
1692
Ex I5, pg. 11
1693
T30-44, lines 2-38
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 242 of 274

926. Furthermore, the section in the Australian Standards applicable to waterborne
rides (including raft rides) needs to be reassessed to include some of the types
of safety requirements associated with roller coasters, including more thorough
considerations for lifts/elevators, collisions and passenger loading/unloading.
1694
927. The requirement for hazard identification and risk assessment in AS-3533.2
section 5.1 should also be made mandatory. Any modification or alteration to the
ride should require hazard identification and risk assessment to ensure that
changes made do not affect safe operation and use.
1695
928. Better direction to other relevant Australian Standards (e.g. the AS 4024 series)
should also be provided. A requirement that hazard identification and risk
assessment include consideration of failures that may affect safety.
929. Dr Gilmore is of the view that whilst the relevant Australian Standards and
Regulations in place in Queensland are adequate, a tightening of the checking
and enforcement process should take place, such as a requirement that full risk
assessments and inspections are actually conducted and fully reported. It is also
recommended that engineering, administrative and protective equipment
controls are properly implemented, together with documentation of the history
and maintenance.
1696
This could be performed by having the requirements
independently certified annually by an RPEQ (or several RPEQ’s), in a similar
manner to the annual inspections for mechanical and structural adequacy,
together with random spot checks of documentation by OIR. Mr. Rutherford
noted that any such RPEQ involved must be able to demonstrate adequate
knowledge and experience in the areas that they are reviewing.
1697
For example,
an Electrical RPEQ does not necessarily have adequate knowledge in the area
of Safety Related Control Circuits, as this is a specialist area.
930. At inquest, Dr Gilmore noted that whilst the Australian Standards have stipulated
hazard identification requirements since 1997, this was not being carried out in
relation to the TRRR, and unfortunately there were no regulatory checks to
ensure it was being done.
1698
931. Dr Grigg is of the view that seat belts with positive latching buckles, as found on
aircraft lap seatbelts, should be required. Their mounting points should be
located in the same position relative to the seat as that used in cars and
aircraft.
1699
932. Mr. Rutherford is of the view that there are adequate details and requirements in
the current applicable Australian Standards with respect to Safety Related
Control Systems and Electrical Safety, if these standards are followed correctly.
However, he cites a lack of enforcement by the Regulators as an issue to be
addressed.
1700
The enforcement by the Regulators in Australia varies on a State
by State basis. In Mr. Rutherford’s experience, OIR is currently the most pro-
active Regulator in Australia in relation to Machinery Safety compliance, and has
a culture of trying to educate not only the Amusement Ride Industry, but Industry
1694
Ibid.
1695
Ibid.
1696
Ex I5, pg. 11
1697
Ibid.
1698
T30-45, lines 1-17
1699
Ibid.
1700
Ibid.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 243 of 274
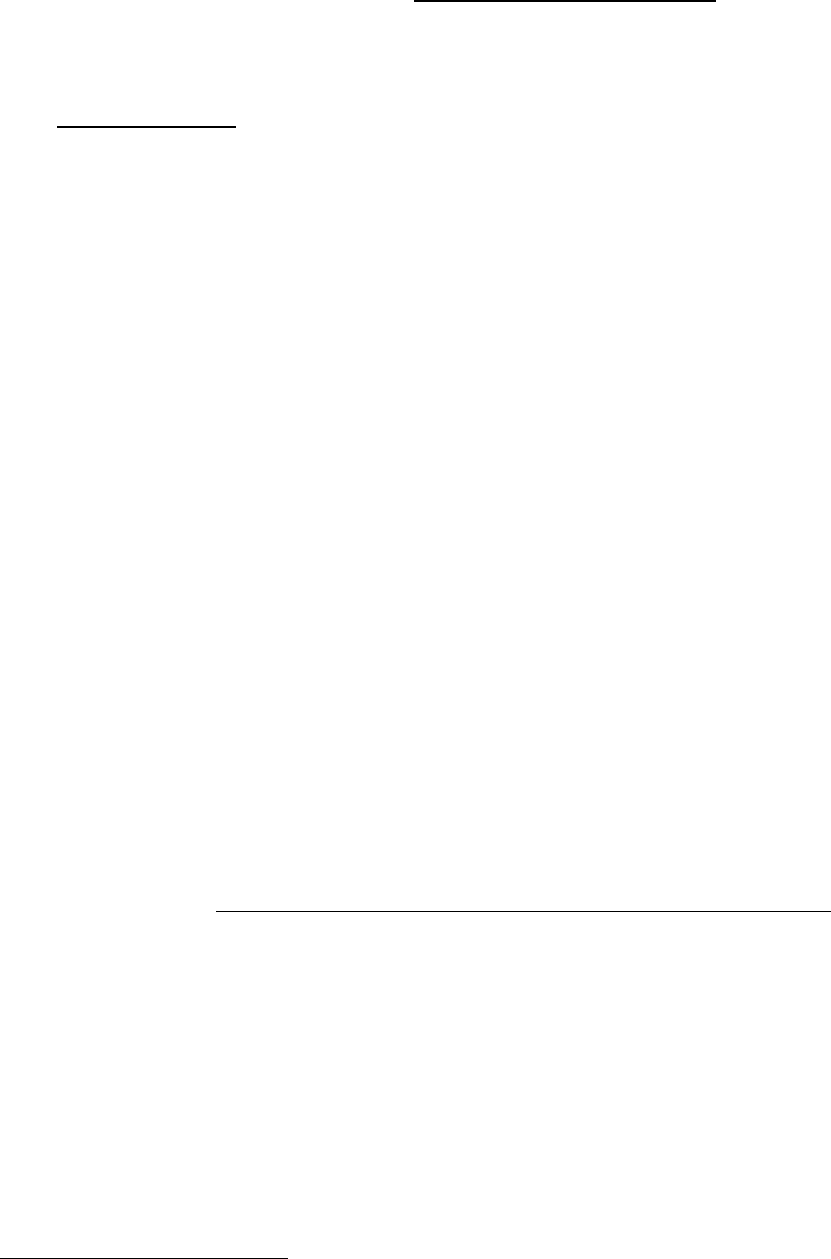
in general, as well as other State Regulators.
1701
One weakness in this approach
is the lack of detailed knowledge on Safety Related Control Circuits held by the
majority of OIR Inspectors. Mr. Rutherford is of the view that this must be
addressed, in conjunction with mandatory requirements for up to date circuit and
component documentation for all Plant safety features (not only Amusement
Rides). There must also be support provided by OIR for Inspectors to issue
Prohibition notices and the like on significant Plant.
1702
(9) In your opinion, are there any other safety issues arising from this tragic event,
which need to be considered and addressed in order to ensure a similar incident
does not occur in the future? If so, what measures need to be undertaken?
933. The experts all agreed that having considered the circumstances of this tragic
incident, the recognised absence of adequate documentation and engineering
controls destroys the assumption that the annual ride inspection was a sufficient
oversight mechanism (according to Regulations) for the public safety of the
ride.
1703
The initiation of a formal document and control system for each ride
should take place, which includes the appointment of a designer or competent
person for every ride, registered with OIR, with tertiary qualifications in
engineering and relevant experience.
934. Dr Gilmore recommended the use of an external party to be engaged to conduct
independent risk assessments. The independent party must be a Registered
Professional Engineer of Queensland (RPEQ). Dr Grigg questions the need for
an independent RPEQ for annual assessments if the competent person is
qualified.
935. It was further proposed that the Regulations should make clear the onus placed
on a competent person (who may be an RPEQ) when conducting an annual
inspection or a risk assessment, in order to provide support for time spent in
conducting such a task thoroughly. These assessments should include the
following:
1704
i. The operation of the ride must be visually observed, with the
‘what if’s’ asked and trial events conducted i.e. not a cursory
inspection or tour.
ii. Low probability failures need to be actively considered.
Suggestions that the ride has been trouble free for 30 years is
not an acceptable excuse. History demonstrates that low
probability coincidences often turn out to be the cause of a major
unexpected incident. Examples abound in aircraft, train, motor
vehicle, motor cycle and helicopter crashes, crane and elevating
work platform collapses, and fires.
iii. Observe how the machine handles adverse events. Run trial
days where pumps are shut down, water levels decreased (or
increased), rafts bottle neck, impact each other, to highlight
weaknesses and expose hidden features of the design.
1701
Ibid.
1702
Ibid.
1703
Ex I5, pg. 12
1704
Ex I5, pg. 12
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 244 of 274

iv. Consult Theme Park records internally and internationally.
v. Consider whether the machine was fool-proof, and if not what
engineering controls could be possibly utilised.
vi. Look at design records.
936. During cross examination at the inquest, when asked about predicting low
probability events, as this incident was characterised, Dr Grigg stated,
1705
Dr Grigg: I can agree that low probability events
can be difficult to predict, but I don’t
think for a minute that anyone doing a
risk assessment on that ride would
not observe things which could be
regarded as anything other than
hazards.
Mr. Hodgkinson: Well, I will come back to that, but do I
understand your evidence to be that
the proposition you agree with, in
relation to this ride, you draw some
additional matters about the
objectives foreseeability of the
hazards?
Dr Grigg: No, I think – it’s a low probability event
simply because it has operated for 30
years without anything happening. I
think that’s my interpretation of what
Dr Gilmore is referring to, and it’s a bit
like, you know, somebody crossing
the road: they’ve done it many times,
but there’s the risk that they’re going
to get knocked down by a car. It might
be a low probability event, but you
know that you – it’s a hazard and
you’ve got to do something about it if
you’re the individual crossing the
road. And in this case, the patrons
weren’t in a position to do that, but the
people running the ride should have
appreciated that there was a risk
there.
937. When he asked about the inability of investigators to re-enact the tragic incident,
Dr Gilmore stated:
1706
The outcome of the – the unfortunate deaths of people might
have been difficult to – to predict, but the – the coming
together of rafts was not difficult to predict, and in fact,
Dreamworld themselves had three – three prior incidents, in
1705
T30-56, lines 1-18
1706
T30-59, lines 15-25
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 245 of 274

’04, ’05 and ’14, in which rafts came together and bumped,
and they themselves shut down the conveyor because they
required the – they thought that the situation had become
undesirable and dangerous – and I think that’s as far as you
need go. If you identify a situation where two rafts come
together, that’s – that is a situation where you shut the
conveyor down, and whatever happens after that – that –
that may be more – more difficult to predict, but the – it can
go any way from there, but – and, in – in this incidence, it
went one particular way.
938. Dr Gilmore further stated:
1707
…I don’t think it’s actually relevant that the police were
unable to exactly replicate the – the exact incident because
the crux of - of the incident was that two rafts came together.
After that, what actually happened – we know what
happened – but it could’ve gone any one of many different
ways.
…
The fact that the – it turned upside down and people fell into
the conveyor, into the water, that’s one way but another
might’ve been people fell off the raft into the water. Who
knows – might’ve happened then.
..
It might’ve ended up happening but it may have ended up
another way.
939. It was also suggested that a requirement be introduced stipulating that a full risk
assessment (according to Australian Standards) on the whole ride be conducted
during commissioning, after major modifications and every 5 years.
1708
The
annual inspection is an ideal time to report any new modifications or
installations/equipment changes in the past year. The RPEQ, who performs the
mechanical/structural inspection, or another independent competent person
(preferably also an RPEQ), should be requested to include a review of written
documentation and the ride, illustrating any recent modifications within the past
year, including photographs, and present a recommendation as to whether a
fresh risk assessment should be conducted immediately. The Proprietor must
keep ongoing detailed written documentation of equipment maintenance and any
modifications, which can be made available for spot checks by OIR. It would be
expected that the RPEQ would be assisted by the designated competent person
during these assessments.
940. With respect to annual inspections, given the report need not be submitted for a
compliance check, it is recommended that spot checks by OIR be carried out to
ensure proper conduct and thoroughness.
1709
Annual inspections should also
include photos to identify if modifications have been made and if they have been
1707
T30-150, lines 23-40
1708
Ex I5, pg. 12
1709
Ex I5, pg. 13
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 246 of 274
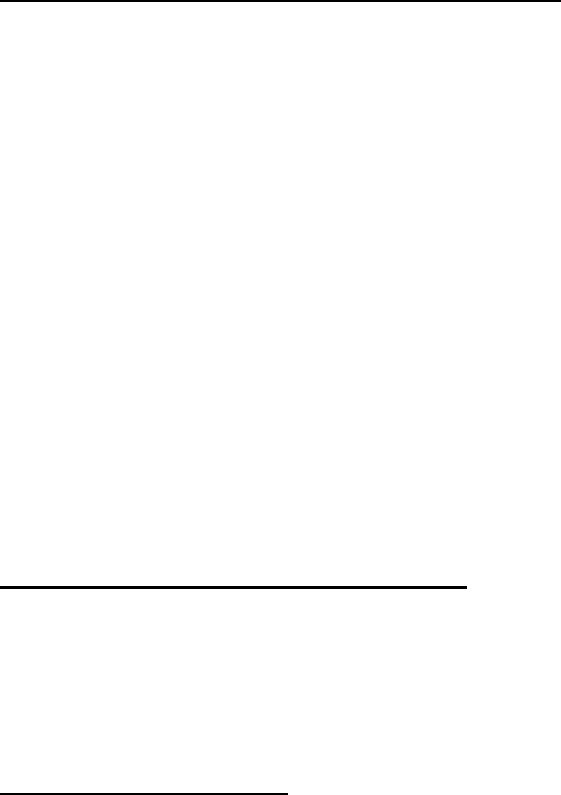
advised to WHS Queensland as required.
941. In relation to ‘new designs’, the experts suggested that these should be
documented to reveal the design methodology, what was considered, safety
considerations, with the log and register with OIR to be kept centrally.
1710
Further,
testing of a ride must be carried out, and be comprehensive. It is difficult to
nominate dynamic aspects which might be required for example to identify a
problem hidden for 30 years. This has to be overcome by inquisitiveness and
enthusiasm, which needs to be well documented.
942. Mr. Rutherford is of the view that OIR Inspectors (and any organisation or
individual involved in this area) need to be more aware and knowledgeable on
applicable Safety Related Control Systems and Electrical Safety. He also notes
that it is important that documented Electrical Circuitry, Critical Component Lists
etc. are updated as modifications occur. These are essential to the safe on-going
maintenance of Plant.
1711
Expert’s Response to the Proposed Draft Regulations
943. Having heard the evidence of Mr. Bick in relation to the new safety case regime
proposed in Queensland, the experts were asked to comment on the sufficiency
of the amendments and new scheme.
944. In response, the following comments of note were made by the experts:
(i) Dr Gilmore and Dr Grigg agreed that the new Regulations needed to
include a requirement that the owner of an amusement device
comply with the updated Australian Standards.
1712
(ii) Dr Gilmore endorsed the development of a Code of Practice for
amusement devices as has been suggested by OIR.
1713
(iii) Dr Gilmore endorsed the introduction of a safety system of
management and the enforcement of such a requirement by the
Regulator through active auditing and spot checks.
1714
(iv) Mr. Rutherford noted that it was important that the new Regulations
require the consideration of hidden components of an amusement
device to ensure a detailed review is conducted.
1715
Mr. Chan’s Response to the Expert Evidence
945. Mr. Chan agreed with the suggestion made by Dr Gilmore as to the extension of
the annual inspection requirements for the competent person engaged so as to
include a risk assessment, as detailed above at [925]. Whilst he acknowledged
that the current requirement for annual inspections does not expressly include a
risk assessment, the obligation of the Engineer conducting the inspection to
consider the hazards present would be beneficial.
1716
We would interpolate
1710
Ibid.
1711
Ibid.
1712
T30-23, lines 32-45
1713
T30-27, lines 28-38
1714
T30-45, lines 30-40; T30-46, lines 1-25
1715
T30-46, lines 27-48
1716
T31-3, lines 5-45
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 247 of 274
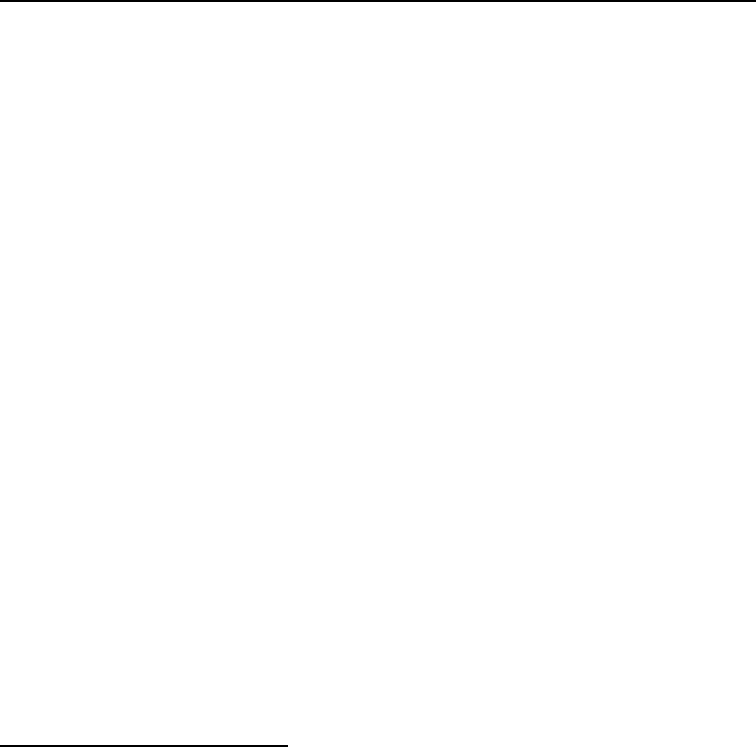
‘essential’.
946. With respect to the suggestion that a full risk assessment on the whole ride be
undertaken after all major modifications and every five years, Mr. Chan stated
that the proposed amendments to the Regulations included a requirement with
respect to major inspections of amusement devices, at timeframes suggested by
the manufacturer or a component, or 10 years.
1717
He questioned the validity of
stipulating a general 5 year arbitrary timeframe, when this may not accord with
the requirements of the manufacturer in relation to a particular component of the
device (i.e. a shorter or longer period may be necessary).
1718
947. Whilst Mr. Chan did not agree with a blanket requirement that amusement device
owners should follow ‘best practice’ by updating a ride when any change was
made to the applicable Australian Standard, he did agree that this would be
appropriate for changes made to the Standards applicable to the maintenance
and inspection of a device.
1719
I would agree that it becomes mandatory.
FURTHER EXPERT ADVICE
Human Factors Report on Fatal Incident, Professor Penelope Sanderson
948. During the course of the OIR investigation into the causes of this fatal incident,
a Human Factors Report was sourced from Professor Penelope Sanderson, a
Professor of Cognitive Engineering and Human Factors, School of Psychology,
University of Queensland.
1720
949. Professor Sanderson was requested to consider nine specific questions
concerning the cognitive and other factors impacting Ride Operators in various
situations with respect to the specific operation of the TRRR. The expert advice
provided is outlined below.
(1) Given the ride’s layout, controls and displays, what perceptual motor and
cognitive skills should Operators have developed to carry out the ride’s required
tasks across a range of normal conditions?
950. In relation to a two person operation of the TRRR, Professor Sanderson notes
that there are 22 signals to process and tasks to perform if Ride Express guests
and children are present, and 17 signals if this is not the case.
1721
In addition,
there are also around 21 background or periodic checks of the ride operation and
engineering status for the Load Operator to carry out. Accordingly, there are a
total of between 38 to 43 signals and checks that must be done.
1722
951. Based on calculations and analysis conducted by Professor Sanderson of the
TRRR cycle times, the following factors of a two person operation were noted:
1723
(a) The 17-22 signals to notice and tasks to perform have to be completed in
around 35 seconds during holiday periods and in around 43 seconds during
non-holiday periods.
1717
T31-5, lines 30-48
1718
T31-5, lines 30-47
1719
T31-6, 7, lines 1-25
1720
Ex C2(5)
1721
Ex C2(5), pg. 7
1722
Ex C2(5), pg. 7
1723
Ex C2(5), pg. 7 & 8
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 248 of 274

(b) For every one second of operation, therefore, an Operator should process
approximately one signal or perform one task.
(c) In addition, for every one second of operation, an Operator should complete
approximately one background or periodic check.
(d) This very high ratio of signals/tasks/checks to elapsed time would be difficult
to achieve fully, and difficult to sustain fully.
(e) Given the operational constraints of the ride, including timing and buffering
capacity, Operators are forced to prioritise activities that get rafts loaded and
dispatched. Accordingly, they would need to develop ways to manage
periodic and background checks either through incorporating them into
‘rituals’ where possible, performing them parallel to other activities,
performing them only when there is unoccupied time during load activities
or performing them less frequently then on every dispatch cycle.
(f) There was no explicit training for Operators on how to prioritize or manage
what could become an overload of activities.
952. Professor Sanderson noted that given the Load Operator’s primary task is to
settle guests into rafts and have them dispatched, which already requires 17-22
steps, it is unlikely that all the 21 background and periodic checks could be done
for each cycle.
1724
However, a failure to perform any one of those checks might
be a factor which could contribute to an incident.
953. Professor Sanderson states that the design of the Main Control Panel at the
TRRR does not translate the buffering capacity of the ride or the potential time
for the Operator to process signals, complete tasks and perform periodic and
background checks.
1725
That is, the design of the panel does not make the Load
Operator ‘smart’ about how best to use the time available in the system.
1726
In
addition, there are no cognitive aids provided in the form of readily visible
checklists of periodic and background checks, which need to be performed.
(2) Given the ride’s layout, controls and displays, what perceptual motor and
cognitive skills should operators have developed to carry out the ride’s required tasks
in different kinds of emergency situations?
954. Professor Sanderson noted that in the TRRR manual, there was ‘quite complex
mapping of anticipated emergencies and operational problems’ to the actions
that the Operator is expected to carry out.
1727
There are differences in the
expected response depending on the type of emergency or operational issue,
which includes whether the ride needed to be shut down or whether dispatch
should be suspended, as well as whether a supervisor needed to be advised or
not.
1728
Professor Sanderson noted that there was potential for Operators to be
made ‘smarter’ in their response to anticipated emergencies by better
information design and display, as well as better training and training evaluation
processes, such as emergency drills or simulations.
1729
1724
Ex C2(5), pg. 9
1725
Ex C2(5), pg. 10
1726
Ex C2(5), pg. 10
1727
Ex C2(5), pg. 12
1728
Ex C2(5), pg. 12
1729
Ex C2(5), pg. 12
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 249 of 274

955. In relation to classifiable emergencies, which are defined as a feasible
emergency situation that the Operators and/or engineers recognise, Operators
will need to be able to recognise the potential consequences of the emergency
and apply to appropriate procedure.
1730
In order for this to occur, a general
familiarity with the ride structure, functioning and risks will be necessary.
(3) Could operators be impaired from executing corrective action in an emergency
situation?
956. Professor Sanderson notes that any operator of a system can be impaired from
executing appropriate corrective action in an emergency situation, which can
arise from a variety of sources, including stress.
1731
Stressful situations can
narrow a person’s attentional focus, and may prevent them from processing
information, which seems peripherally less important.
1732
Several studies have
shown that people under stress may be able to carry out highly familiar and well-
practiced routines, however, will struggle carrying out novel or rarely used
processes.
1733
957. Professor Sanderson noted that from Mr. Nemeth’s account, the approach of
Raft 5 towards Raft 6, stranded on the support rails, was stressful and may have
narrowed his attentional focus so he did not fully process the information Ms.
Williams was asking him from the unload area.
1734
Furthermore, the stressful
events coupled with the poor user interface design of the Main Control Panel,
may have meant that Mr. Nemeth did not activate the conveyor stop button
effectively.
1735
958. In evidence during the inquest, Professor Sanderson stated that the stress
associated with responding to the emergency situation, which presented on the
day of the tragic incident, in addition to the regular Operator duties to be carried
out, would have made it difficult to work out exactly what to do in the situation,
particularly as there wasn’t a procedure for exactly that situation.
1736
(4) Could Operators’ normal tasks/duties impact on their ability to observe and
respond effectively to emergency situations in a timely manner?
959. Professor Sanderson notes that normal tasks and duties may delay or preclude
Operators from either noticing or being able to respond effectively to operational
problems or emergency situations, with the reverse also being the case.
1737
960. Having considered the activity sequence specified in the Operator Procedure
manual in the event of an operational problem requiring a shutdown, which has
up to 11 steps, Professor Sanderson found that this may make it difficult for
Operators to observe and respond to emergency situations, which occur in
addition to operational problems, such as retrieving rafts, focusing on operating
the Main Control Panel or observing guest behaviour.
1738
961. In relation to operating problems, which require a shutdown, as noted in the
1730
Ex C2(5), pg. 12
1731
Ex C2(5), pg. 15
1732
Ex C2(5), pg. 16
1733
Ex C2(5), pg. 16
1734
Ex C2(5), pg. 16 & 17
1735
Ex C2(5), pg. 17
1736
T31-19, lines 40-47
1737
Ex C2(5), pg. 18
1738
Ex C2(5), pg. 19
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 250 of 274
Operator Procedure Manual, Professor Sanderson noted the following:
• Loss of power to one or both pumps: This causes a drop in water level
over a short period, which may be noticed relatively quickly by an Operator
if they are loading a raft or manning the Main Operator control panel and
noticed the pump amps drop. However, if the Operator was communicating
with guests, these signals may be missed, thereby delaying the Operator’s
ability to observe and respond quickly to this operational problem.
1739
• Loss of power to the conveyor or chain break: Normal activities could
delay an Operator noticing that the conveyor wasn’t operational, thereby
delaying the response.
• Raft stall at the bottom of the conveyor: Unless the Operator was
viewing the CCTV at the Main Control Panel, other operational tasks would
delay their ability to observe this issue and respond accordingly.
1740
• Raft Jam: How quickly an Operator responds to such a situation largely
depends on where this happens around the watercourse and what the
normal duties and tasks the Operator is engaged in at the time.
1741
• Raft slips on conveyor: Whilst it was recognised that this failure was
lessened by the recent installation of the sensors and jacks at the beginning
of the conveyor, CCTV would be the only means such an event would be
noticed, and it would depend on what other tasks the Operators were
engaged in as to how quickly this issue was identified.
1742
962. Professor Sanderson noted that with the TRRR, ‘any situation where there is a
risk of serious injury to Guests or Staff’ depending on its nature, may not be
identified if the Operator is ‘facing away from visible evidence of it, if attempted
communication between operators does not succeed, or if ambient noise makes
it impossible to hear any evidence of it’.
1743
963. In addition to emergencies, Professor Sanderson was of the view that normal
tasks and duties of Operators would affect their ability to observe and respond
effectively to operating problems, which may not require a shutdown of the
ride.
1744
964. Two types of emergencies were identified in the Operator Procedure Manual for
the TRRR, namely; serious injury to a guest or staff member (3.6.1) and person
in water and/or raft capsized (3.6.2). Per the requirements of the manual, an
Operator needs to respond to an operational problem by interlacing three sets of
activities, namely:
1745
a. Normal duties/tasks relating to guest management and answering guest
questions, and performing background checks and periodic checks on
system status.
1739
Ex C2(5), pg. 19
1740
Ex C2(5), pg. 20
1741
Ex C2(5), pg. 20
1742
Ex C2(5), pg. 20
1743
Ex C2(5), pg. 20
1744
Ex C2(5), pg. 21
1745
Ex C2(5), pg. 22
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 251 of 274
b. Procedure associated with handling the operational problem.
c. Procedure associated with handling the emergency.
965. Professor Sanderson noted that when two or more activity sequences are
interlaced, the likelihood of any one of them may be resumed or completed at an
incorrect point is increased.
1746
Given the number of events to attend to in such
a situation, the time required to complete each may be greater than that available
to complete them in a safe manner.
1747
(5) What factors might prevent or limit effective communication between Operators at
the un-load and load stations?
966. Professor Sanderson noted that the following factors limited or prevented
effective communication between Operators at the load and unload stations of
the TRRR:
• Sight lines – there was 12 m between the two stations, with some structures
creating obstacles between the two. There was no radio or telephone
communication between the two points. Visual communication was the
main potential means of communicating, which was difficult when the
responsibilities of each Operator require them to have their back to one
another.
1748
• Noise: It was noted that ambient noise created by the functioning of the ride
could jeopardise the Operator’s ability to successfully attract the attention
of the other through vocal communication.
1749
Various noise was evident
from the operation of the ride and includes the sound of the dispatch alarm,
the conveyor, the rapids, guest conversations and other nearby attractions
(for example, the Buzzsaw).
• Reflections on the glass of the Load station workstation
967. Given the above ambient sounds present at the TRRR whilst it was in operation,
it would have made it difficult for the unload and Load Operators to attract each
other’s attention and to sustain a conversation, which would make it more
challenging to respond to an emergency.
1750
(6)(a) Did the training provided to Operators enable them (on the day) to respond
effectively to emergency situations in a safe and timely manner?
968. Professor Sanderson recognised that it was impossible to write procedures and
to train staff in all emergency situations. However, training is not a ‘reliable way
to compensate for poor design in the way the engineering constraints and
possibilities for operation action have been conveyed to the operator through the
user interface’.
1751
969. Having considered the circumstances of the incident on 25
October 2016, and
the response by both Mr. Nemeth and Ms. Williams in the context of the Operator
1746
Ex C2(5), pg. 23
1747
Ex C2(5), pg. 22
1748
Ex C2(5), pg. 24
1749
Ex C2(5), pg. 24 & 25
1750
Ex C2(5), pg. 26
1751
Ex C2(5), pg. 27
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 252 of 274

Procedural Manual and associated supplementary memorandums, Professor
Sanderson noted that:
1752
• The manual does not specify the timeframe by which a shutdown needs to
be performed in the event of a pump failure; and
• It is unclear what kind of training would be adequate to ensure reliably rapid
and highly accurate responding to the unanticipated emergency as
transpired during the tragic incident.
(6)(b) Would periodic and scenario-based emergency drills improve Operators’ ability
to respond to actual emergency situations?
970. Professor Sanderson noted that emergency drills provide an opportunity to
develop procedural knowledge, rather than a purely operative level of declarative
knowledge through simply reading procedures or hearing them described.
1753
Drills can help Operators reduce the impact of stressors on their performance
and provide experience at solving the problems presented under less stress than
in an actual emergency, which provides procedural knowledge. However, for an
Operator to obtain the ability to respond to different kinds of actual emergencies,
drills need to cover a range of emergencies, including anticipated emergencies,
classifiable emergencies and multiple-event emergencies.
971. Professor Sanderson notes that an important component in any kind of drill is
the after-action replay and the after-action debriefing.
1754
(7) Are user interface principles applicable to the design of each control board?
Could the design and layout of the control boards contribute to errors?
972. Professor Sanderson notes that user interface principles are applicable to the
design and layout of any device or system with which people interact. This is
especially so when the system is physically large or involves a hazard, in which
case ‘the user interface must bring relevant information to the operator, display
it in a way that the operator will understand, and provide appropriate controls
whose functioning the operator will understand’.
1755
973. Professor Sanderson found that from viewing the video walkthroughs, Operators
had different mental models of some system functioning and procedures, as well
as different ways of enacting procedures.
1756
Examples include:
• Order of performing the emergency sequence.
• Whether the E-Stop at the unload station stopped the conveyor or the
conveyor and the North pump.
• How long the operator should hold down the conveyor stop button on the
Main Control Panel for it to activate.
974. Professor Sanderson also noted that the Operator Procedures for the ride use
1752
Ex C2(5), pg. 29
1753
Ex C2(5), pg. 30
1754
Ex C2(5), pg. 31
1755
Ex C2(5), pg. 32
1756
Ex C2(5), pg. 32
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 253 of 274

text only, with no schematics, pictures or diagrams. The procedures therefore
are possibly not as effective as they could be for all learning styles.
1757
(8) Could individual, situational and environmental factors contribute to the way
Operators implemented procedures?
975. Professor Sanderson found that individual, situational and environmental factors
could contribute to the way Operator’s implemented procedures both in general
and around the time of the incident.
1758
In general, situational and environment
factors have a more systematic influence on how Operators implement
procedures.
976. It was noted that in relation to the TRRR, there was some differences, which
emerge as to the Operator Procedure manual descriptions of procedures and
how Operators implemented those procedures.
1759
977. In relation to the tragic incident, it is unclear whether and when the technical part
of the shutdown sequence of the ride was initiated at the Load station, and if
initiated, when it was completed. If the procedure was not completed in the 54
second interval between Raft 1 being grounded and Raft 2 colliding with it,
factors needed to be considered as to why this may occur with an experienced
Operator.
1760
It is possible that the sequence was interrupted by other tasks
necessary to perform, or there was sequence confusion.
1761
(9) Did the operators’ normal duties/tasks (and degree of training) have any impact
on their ability to observe and respond to the emergency situation?
978. Professor Sanderson was of the view that when the Operator’s execution of
normal Code 6 duties at the Load station is combined with the communications
difficulties and the unanticipated nature of the emergency, there is a strong case
that the combination of factors would have reduced the Operator’s ability to
observe and respond to the emergency.
1762
Expert Report by Principal Naval Architect, Mr. Mark Devereaux
979. At the request of OIR, Principal Naval Architect, Maritime Safety Queensland,
Mr. Mark Devereaux considered the floatation and stability characteristics of the
rafts used on the TRRR.
1763
980. Mr. Devereaux, having considered the CCTV footage, relevant photographs, the
physical rafts and other relevant brief material, as well as the design aspects of
the ride, he concluded that the floatation or buoyancy aspects of the design or
construction of the rafts were not significant contributing factors in the tragic
incident.
1764
Assuming the rafts are regularly drained of any trapped water and
the tube channels are kept inflated, he found that the rafts had adequate stability
for operation in the TRRR. Mr. Devereaux notes that if the raft tubes are kept
properly inflated, they have adequate stability for their intended purpose, ‘as it is
1757
Ex C2(5), pg. 34
1758
Ex C2(5), pg. 35
1759
Ex C2(5), pg. 36
1760
Ex C2(5), pg. 37
1761
Ex C2(5), pg. 39
1762
Ex C2(5), pg. 42
1763
Ex B4(2)
1764
Ex B4(2), pg. 11
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 254 of 274

the volume of the inflated tubes that provides the significant majority of the
buoyancy and stability of the rafts’.
1765
981. Having considered the tragic incident, Mr. Devereaux further noted that there
was a critical rate at which water needed to be pumped into the TRRR, to
maintain adequate height of the water above the steel supporting rails to allow
rafts to remain buoyant and not become stranded.
1766
Dreamworld Ride Velcro Seatbelt Test, APV Engineering & Testing Service, Mr.
Jose de Freitas
982. During the course of the OIR investigation, APV Engineering and Testing
Services were requested to conduct static testing as to the performance and
reliability of the Velcro Seatbelts in used on the TRRR at the time of the fatal
incident. A report outlining the findings of this testing was prepared by Test
Engineer, Mr. Jose de Freitas.
1767
983. The testing conducted found that the performance of the Velcro Seatbelts can
vary significantly, depending on various factors, which are often not apparent
and can be difficult to control.
1768
The belt strap overlap, condition and the applied
pressure during the belt strap engagement were found to be the three major
factors that affected the performance.
984. It was recommended that, for the purpose of the Dreamworld ride application
considered (TRRR), an industrial seatbelt in accordance with SAE J386, along
with an automatic lock retractor ought to have been used.
1769
1765
Ex B4(2), pg. 9
1766
Ex B4(2), pg. 11
1767
Ex F18
1768
Ex F18, pg. 38
1769
Ex F18, pg. 40
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 255 of 274

ANALYSIS OF THE CORONIAL ISSUES
The Findings required by s.45 of the Coroners Act 2003
985. In accordance with s.45 of the Coroners Act 2003 (‘the Act’), a Coroner who is
investigating a suspected death must, if possible, make certain findings.
986. On the basis of the evidence presented at the inquest, I make the following
findings pursuant to s.45:
a. The identities of the deceased persons are Kate Louise
Goodchild, Luke Johnathan Dorsett, Cindy Toni Low and
Roozbeh Araghi.
b. At around 2:05 pm on 25 October 2016, the deceased, whilst
traveling on Raft 5 of the Thunder River Rapids Ride at
Dreamworld Theme Park, collided with a raft stranded on the steel
support railings at the unload area shortly after exiting the
conveyor. This collision caused Raft 5 to be lifted and pulled
vertically into the mechanism of the conveyor. Two other
occupants of Raft 5 managed to escape, however, the deceased
were caught in the mechanism of the ride, and were either ejected
into the water beneath the conveyor or trapped in the raft.
c. The date of the death of all of the deceased persons was 25
October 2016.
d. The place of death for all of the deceased was the Dreamworld
Theme Park, 1 Dreamworld Parkway, Coomera on the Gold
Coast.
e. The cause of death for all of the deceased was as a result of the
combined effect of severe internal and external injuries as a result
of multiple compressive impacts.
987. Comments as to the specific issues identified and considered during the course
of the inquest hearing are outlined below. I find as follows:
Examination of the Thunder River Rapids Ride at the Dreamworld Theme Park,
including but not limited to, the construction, maintenance, safety measures,
staffing, history and modifications.
988. It is clear from the expert evidence that at the time of the incident, the design and
construction of the TRRR at the conveyor and unload area posed a significant
risk to the health and safety of patrons. The hazards associated with
configuration of the ride identified by the experts and investigators were
significant, and included the wide spacing of the slats of the conveyor, the nip
point at the head of the conveyor and the steel support railing, the effect of a
pump failure on the water level and the absence of the emergency stop button
for the conveyor at the Main Control Panel. Each of these obvious hazards posed
a risk to the safety of patrons on the ride, and would have been easily identifiable
to a competent person had one ever been commissioned to conduct a risk and
hazard assessment of the ride.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 256 of 274
989. The experts engaged for the purpose of this coronial inquest and by OIR to
investigate the cause and circumstances of the tragic incident reached their
opinions independently and were all in basic agreement as to the combination of
causes. They were highly qualified to do so, based on the evidence presented,
and were not influenced by so-called “hindsight bias” in reaching their
conclusions. There was ample evidence of the potential for disaster of this nature
occurring, based on the evidence before them, and had notice been taken of and
lessons learned from, the preceding incidents that were all of a very similar
nature, and of which there was ample photographic evidence and reports
prepared. It is indeed very fortunate, to quote Mr. Tan, that no lives were lost in
those earlier incidents.
990. Whilst it appears from the records provided that the initial design of the TRRR
was approved by the Chief Inspector of Machinery in 1987, there were multiple
significant modifications made to the ride prior to the incident in 2016. The
records available with respect to these modifications are scant and ad hoc, and
establish that for the duration of the rides commission, it was modified essentially
without a ‘designer’. It does not appear that anyone external or internal to
Dreamworld, including Mr. Tan, were ever formally charged with conducting a
holistic engineering risk and hazard assessment of the ride, despite the major
modifications and changes made during its tenure. The modifications made to
the ride, despite being significant, were also never reported to the Regulator. It
can be accepted, as was the evidence of the experts that these alterations would
have amounted to a new design and should have been registered by Dreamworld
with the Regulator. A failure to record modifications, a lack of ‘designer’ input and
a lack of reporting to the Regulator have contributed to the masking of the real
risk of the TRRR.
991. From the limited documentary information available, it appears that the
modifications made to the TRRR were somewhat random, seemingly in
response to specific acute issues, without any consideration given as to the other
risks or hazards that may be created as a result of the change. There was no
proper engineering oversight of the ride, changes made or consideration of past
incidents for which engineering solutions should have been implemented.
Accordingly, it can be accepted, as was found by the experts, that whilst there
were various occasions for which s.5.1 of the AS3522.2-1997 should have been
triggered, and a mechanical hazard identification and risk assessment of the ride
undertaken, this was never done. Unfortunately, there were clearly a number of
missed opportunities during which Dreamworld could and should have identified
the safety issues associated with the ride.
992. The maintenance tasks undertaken on the ride, whilst done so regularly and
diligently by the staff charged with such a responsibility, seem to have been
based upon historical checklists, which were rarely reviewed, despite the age of
the device or changes to the applicable Australian Standards, particularly 3533
Part 2 and 3.
993. The external auditing undertaken by JAK was not done so by way of reference
to the Australian Standard, and, as was acknowledged and known by
Dreamworld, focused on superficial aspects of the ride, rather than the
engineering, design and safety aspects. This shortcoming is blatantly obvious
from the reports provided by JAK, and was also raised by Mr. Randall once DRA
were engaged by Dreamworld in 2013. I am satisfied that Dreamworld knew of
this significant limitation with respect to the safety auditing being conducted on
its devices, however, failed to take any steps to rectify it.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 257 of 274
994. Previous incidents on the TRRR, particularly in 2001 and 2014, should have
alerted Dreamworld to the hazards present on the ride, particularly the collision
of rafts on the watercourse. These incidents should have prompted a thorough
risk and hazard assessment of the ride, including the design, looking beyond the
circumstances of the particular incident. In accordance with the hierarchy of
controls, plant and engineering measures should have been considered as
solutions to identified hazards. Whilst administrative controls are the lowest in
the hierarchy, they nonetheless may be sufficient to manage some risks.
However, for such a decision to be made, risks actually have to be identified and
properly qualified consideration given as to the best solution to manage that risk.
The risks and hazards posed by the TRRR, which have been highlighted by this
incident and the experts, were never identified by Dreamworld as such
assessments were never undertaken. A heavy and unreasonable reliance on
administrative controls to ensure the safety of patrons on the TRRR was clearly
not a reasoned decision following a proper risk assessment. Rather, it was simply
a continuation of processes and procedures that had always been followed,
during which there had not been a previous serious incident. This reliance by
Dreamworld on the operation history of the ride as to whether a risk or hazard
was present is clearly unsound and dangerous. The various high and low
probability hazards and risks associated with the ride, which have been
highlighted by the experts, were present and should have been identified by a
suitably qualified risk assessor.
995. Rafts coming together on the TRRR was a well-known risk, highlighted by the
incident in 2001 and again in 2004. During the investigation into the 2004
incident, it was acknowledged that various corrective actions could be
undertaken to ‘adequately control the risk of raft collision’, however, a number of
these suggestions, including a conveyor speed controller or raft positioners, were
not implemented by Dreamworld. The Report into this incident acknowledged
that at the time, the primary means of avoiding raft collision at the unload area
was through administrative controls by Ride Operators. Whilst some engineering
and automation modifications were made to the ride post this incident, it is clear
that this primary reliance continued. Clearly, the combination of these controls
at the TRRR was not sufficient to ensure that rafts were not able to come into
contact with one another near the unload area. The knowledge that rafts could
flip if they came together on the watercourse, particularly at the end of the
conveyor near the unload area, was recognised throughout the history of the
ride, including most recently in 2014. This risk and the peril posed to patrons of
rafts colliding and possibly flipping was further highlighted by Mr. Tan in his email
to the Leadership Team, where he outlined the events in 2001, stating, ‘I
shudder when I think if there had been guests on the rafts…’ Indeed this was
recognised during Ms. Crisp’s training of Ms. Williams where she claims she
made a point of highlighting that two rafts could not be dispatched together or
else there was a risk of capsize. Clearly, the risks associated with rafts colliding
was known to Dreamworld.
996. Whilst the exact scenario that occurred in this instance may not have been able
to be replicated during testing by Investigators, this is of limited relevance, and
does not render the identification of the risk present unpredictable without the
benefit of hindsight. The hazards and risks, which caused the rafts to collide at
various points on the ride, and in particular at the end of the conveyor, were
present and known, and should have been identified by someone qualified to
conduct a risk and hazard assessment. Unfortunately, Dreamworld never
engaged such a person and as such these risks were never mitigated.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 258 of 274
997. It was agreed by the experts, and became obvious during the inquest hearing,
that best practice for the TRRR was not followed by Dreamworld, particularly in
relation to compliance with introduced Australian Standards designed to ensure
the safety of devices. Whether these requirements are mandatory or not is
largely irrelevant. Those Standards are the minimum practice that is required. It
is the responsibility of those that own and operate high risk plant to ensure that
the most up to date safety standards, risks and requirements known to the
industry are considered and instituted if possible, to ensure the safety of staff
and patrons. This was certainly not the case in relation to the conduct of
Dreamworld as to the management, modification and maintenance of the TRRR.
Dr Gilmore stated during the expert conclave that should ‘best practice’ not be
followed with respect to safety standards, an owner would do so at their own
peril. Unfortunately, this failure by Dreamworld to adequately ensure the safety
of the ride and manage the obvious hazards and risks present was done so at
the peril of Ms. Goodchild, Mr. Dorsett, Ms. Low and Mr. Araghi.
998. Given the nature of fixed amusement devices, it is reasonable for the community
to expect that the owner and operator would ensure that there is no risk to the
safety of patrons. Owners should be risk averse, which includes considering and
identifying low probability failures for their devices, so that these risks can be
mitigated altogether. Whilst it is accepted that there is always an inherent risk to
safety given the nature of an amusement ride, it is expected, and is indeed
reasonable to do so, that all action has been taken by the owner to eliminate the
risks posed. That was not the case with respect to the TRRR. There is no
evidence that Dreamworld ever conducted a proper engineering risk assessment
of the ride in its 30 years of commission. The risks and hazards, which have now
been highlighted by the experts, were never identified and considered by
Dreamworld because such an assessment was never undertaken.
999. Dreamworld placed a great deal of reliance on Mr. Tan’s engineering ‘expertise’
to ensure the safety of the amusement devices at the Park. Mr. Tan was not an
RPEQ, which should have been known by Dreamworld, and was involved in a
number of Special Projects within the Park. Sole reliance on him to undertake
such an assessment on all of the devices at Dreamworld during his tenure was
dangerous, given the level of responsibility associated with such an undertaking
and his other responsibilities, including oversight of the E&T Department. Mr.
Tan was, until Mr. Cruz was employed shortly before the incident, the only
qualified engineer engaged by the Theme Park. It is obvious from the response
provided by Ardent Leisure to OIR when asked about compliance with s.241 of
the Regulations, that Mr. Tan’s experience was a central tenant of the safety
program in place at Dreamworld. For Australia’s largest Theme Park that
approach was irresponsibly and dangerously inadequate, particularly given the
lack of succession planning in place following Mr. Tan’s departure in January
2016.
1000. It is surprising, however, that Mr. Tan did not ever recognise the risk and hazards
present on the TRRR from a design perspective, despite being consulted on
various modifications made throughout its commission. Given his formal
qualifications, experience and knowledge of the device, this seems like a missed
opportunity, although it is accepted that Mr. Tan’s role did not extend to
considering the design of the ride.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 259 of 274
1001. In addition to Mr. Tan, it seems that Dreamworld placed significant reliance on
E&T staff and Ride Operators to identify risks and issues associated with rides.
Whilst there can be no suggestion that these staff did not perform the roles they
were given with dedication and in accordance with their training, it is
unfathomable that this serious and important task fell to staff, who did not have
the requisite qualifications or skillset to identify such hazards. Whilst the
information and feedback from staff, who work with and on rides, is always
valuable, it cannot and should not be the solitary means by which such hazards
and risks are identified.
1002. Irresponsibly, and consequently tragically, the Safety Department at Dreamworld
was not structured to operate effectively, with the safety systems in place at the
time of the incident correctly described as ‘immature’. Document management
was poor, with no formal risk register in place, members of the Department did
not conduct any holistic risk assessments of rides with the general view being
that the E&T Department were responsible for such matters. There were no
safety audits conducted as to the human components of the ride systems at
Dreamworld. Furthermore, members of the Safety Department were not involved
in the drafting of Operating Procedures for the amusement rides, a responsibility
left solely with the Operations Department. It seems clear that there was a
significant segmentation of knowledge between the Departments, which was
further exacerbated by a poor record and document management system,
making information difficult to obtain and access. It is important to note that
evidence suggests that members of the E&T Department were only involved in
developing and implementing controls for a potential hazard once it had been
brought to the Department’s attention.
1003. The resounding message of the General Managers responsible for the
Departments at Dreamworld was that, as such risks and hazards had never been
identified to them, they were unaware and therefore unable to take any action.
Given no steps were ever taken to properly identify these risks by qualified
people, it is unsurprising that such issues were not raised with management. This
general ignorance of proper safety and adequate assessments was a recurring
theme throughout Dreamworld in many of the Departments and reflects a
systemic failure to ensure the safety of patrons and staff by the use of a proper
safety management system, with the necessary engineering oversight of high
risk plant.
1004. From the accounts provided during the course of the investigation and inquest
hearing, it is evident that only a scant amount of knowledge was held by those
in management positions at Dreamworld, including Mr. Deaves, as the General
Manager of Engineering, as to the design, modifications and past notable
incidents on the TRRR.
1005. It can be concluded beyond doubt that in the 30 years prior to this tragedy,
Dreamworld failed to undertake, either internally or via an external auditor, a
holistic examination of the TRRR by a suitably qualified engineer, so as to ensure
its safe operation through the identification of the high and low probability risks
and hazards present.
1006. During the inquest, Maintenance Planner, Mr. Naumann agreed that there had
been a ‘total failure’ by everybody at Dreamworld to identify the safety issues in
respect of the TRRR, which he acknowledged was completely unsafe at the time
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 260 of 274

the tragic incident occurred.
1770
This failure is supported by the evidence
obtained and presented during the course of the coronial inquiry. Dreamworld
has a reputation as a modern and world-class Theme Park. However, the safety,
maintenance and operating systems in use to ensure guests safety were
rudimentary at best, with Departments operating in silos, an absence of risk
management and informal and ad hoc record keeping. The manner in which the
documentation was provided during the course of the coronial inquiry and inquest
further demonstrates the frighteningly unsophisticated ‘systems’ in place at
Dreamworld intended to ensure the safety of patrons and staff. It is surprising,
given the state of the safety management systems in place at Dreamworld that
a tragedy of this nature had not occurred before now. It was simply a matter of
time. That time came on 25 October 2016.
Records
1007. Records as to the design and manufacture of the TRRR are sparse. There is
limited context as to the creation of the ride, how certain components were
designed and commissioned, and the intended ongoing management and
maintenance. It is unfortunate that this poor recording keeping continued
throughout the 30 years of its commission, with respect to all aspects of the ride.
Whilst voluminous records and documents were produced by Ardent Leisure
following this tragic incident, and throughout the coronial investigation and
inquest, they were arbitrary in nature and lacked context and explanation. This
has made the task of piecing together the history of the ride, the modifications
made, and the repairs and maintenance conducted, incredibly difficult for all
parties. It becomes a more critical issue as a ride ages, because the demands
for maintenance, and even replacement, will increase.
1008. What is clear from the records produced, and the difficulties Ardent Leisure had
locating the requested information, is that the record keeping, document
management and interdepartmental communication at Dreamworld was dire. It
appears that the maintenance, inspection and repair action taken in relation to a
ride was reactionary to issues arbitrarily or accidentally identified, rather than a
proactive systematic approach following an independent, thorough assessment
of a ride.
1009. The records and document control in place at Dreamworld, including for the
rides, safety systems, maintenance and training of staff, was clearly significantly
lacking, with only limited information available. Whilst Mr. Cruz was in the
process of undertaking ‘data mining compliance’ with respect to the amusement
devices at the time of the incident, this was clearly a difficult process that
exposed the widespread lack of record keeping and document management that
had been in place at Dreamworld for the past 30 years.
1010. It was recognised by Mr. Deaves that there were no records kept, which were
easily accessible or centrally located, whereby staff responsible for the safety of
the rides, both from an operations and engineering perspective, could examine
and consider previous issues associated with a device. This absence of effective
and complete record keeping essentially precluded any staff from being in a
position to be able to appropriately and adequately assess and manage the risks,
which may be present, particularly for rides like the TRRR. It is significant that
the General Manager of Engineering had no knowledge of past incidents
involving rafts coming together on the TRRR. It is clear that this lack of
1770
T11-90, lines 25-47
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 261 of 274

knowledge essentially precluded him, and anyone else, from assessing or
determining risks associated with the TRRR from an engineering perspective,
which contributed to the environment in which such a tragic incident could
transpire. I find that shoddy record keeping was a significant contributor to this
incident.
The circumstances and cause of the fatal incident on the Thunder River Rapids Ride
at the Dreamworld Theme Park, which occurred on 25 October 2016.
Technical Circumstances
1011. The technical cause and sequence of the tragic incident has been expertly
considered and addressed in detail in the evidence as provided by the expert
engineers, Senior Constable Cornish and the OIR Inspectors. I am satisfied that
the incident occurred as previously outlined.
1012. It is clear that the primary cause of this tragic incident was the failure of the south
pump, leading to a sudden drop in water level, following which the conveyor was
not stopped. Dreamworld were aware that when one pump failed on the TRRR,
the ride was no longer able to operate, with the water level dropping dramatically
stranding the rafts on the steel support railings around the trough. Regardless,
there was no formal means by which to monitor the water level of the ride, or
audible alarm to advise one of the pumps had ceased to operate. Rather, a light
on the Main Control Panel or ampere reading was all that notified an Operator of
the pump failure, aside from the recognition that the water appeared to have
fallen below a historical scum mark in the trough. Despite the significance of the
water level to the safe operation of the ride, there was no automated safety
system in place to monitor the water level or provide any audible or visual alert
should it fall below a safe level.
1013. It was a second, major contributing factor of the incident that the conveyor
continued to operate in the event of a pump failure. It remains unknown, and
impossible to understand why, the two major components of the ride were
controlled independently of each other. It is also unknown as to why there was
such an arbitrary gap between the end of the conveyor and the steel support
railings, which created a nip point of sufficient size for Raft 5 to be pulled into
during the incident. When contact occurred between Raft 5 and the raft stranded
on the steel support railing, it became forcibly engaged by the conveyor, due to
the slat removal, entering that gap as it continued to impact the other raft, which
was snagged on the steel support railing. It was the view of the experts, and
which I accept, that had any one of the contributory factors been absent, the
incident, as it transpired, would not have occurred. That being the case, given
the multiple other hazards evident on the ride as was highlighted by the experts,
this would not have precluded another catastrophic incident from occurring in
another way.
1014. While the TRRR had operated fatality free for around 30 years, at the time of the
fatal incident, it is clear that the design and construction of the conveyor/unload
area posed a significant unidentified risk to the health and safety of patrons. A
properly documented history with appropriate risk assessments, in all likelihood,
would have identified and eliminated the serious risks.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 262 of 274
Lack of Automation
1015. During the inquest, Senior Constable Cornish described the TRRR as ‘severely’
lacking in any type of automation, which was readily available. This was clearly
accurate, and a sentiment shared by the engineering experts. It is unknown as
to why basic engineering controls, such as a water level monitor or an interlock
shutdown function for the conveyor in the event of a pump failure, was not
installed on the ride. It is clear from Mr. Rutherford’s evidence that a basic
automated detection system for the water level would have been inexpensive
and may have prevented the incident from occurring.
1016. The lack of a single emergency stop on the ride, which was capable of initiating
a complete shutdown of all of the mechanisms, was also inadequate. Whilst JAK
had recommended that a simpler automatic process be considered, and the
Operations Department had sought input from the E&T Department as to a one
button shutdown, it is unfortunate that no further action or follow up was
undertaken. It is not clear as to why such a recommendation was not actioned
and the risk deemed by Dreamworld to be ‘acceptable’. It seems this lack of an
emergency stop button for the conveyor at the Main Control Panel was contrary
to the Australian Standards.
Operators Account of the Incident
1017. It is apparent that at the time of the tragic incident, Mr. Nemeth held the role of
the No.1 Operator and was stationed at the Main Control Panel. He had primary
responsibility for the operation of the TRRR. Ms. Williams, as the No. 2 Operator,
was stationed at the unload area. There were no other Dreamworld employees
in the area at the time.
1018. From the CCTV footage, and Mr. Nemeth’s statement, it appears that it only took
around 20 seconds from when the water level started to drop following failure of
the south pump, before Raft 6 became stalled in the unload area on the steel
support rails. The water dropped dramatically causing the ride to be unable to
operate. A further 55 seconds passed, during which time Raft 5 travelled the
conveyor and impacted with Raft 6. Statements from the occupants of Raft 6, as
well as those, which were being loaded at the time of the incident by Mr. Nemeth,
provide contradictory accounts of the sequence of events during the critical
seconds before the tragic impact.
1019. It is evident from the CCTV footage that at the time of the incident, Mr. Nemeth
remained at the Main Control Panel. Having noticed that the water level had
dropped significantly, Mr. Nemeth advised the guests he had loaded that they
would need to disembark. It is not clear when he initiated the shutdown sequence
of the ride, particularly whether this was before or after the rafts collided and/or
he had contacted the control room. There is no way to ascertain with any
certainly as to whether he did and if so precisely when Mr. Nemeth may have
pressed the conveyor stop button. He claims he pressed it multiple times but
nothing happened. Testing following the incident by investigators found no issue
with the operation of that particular control button. From the CCTV footage, the
conveyor can be seen to commence a slow stop approximately 11 seconds after
the rafts have collided. It seems in all likelihood, given the events that followed,
that Mr. Nemeth may not have pressed the conveyor stop button until the rafts
had collided or moments beforehand.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 263 of 274

1020. During this time, Ms. Williams recalls, and can be seen on the CCTV footage, to
remain at the unload station. She did not press the E-Stop button at that platform
for a number of reasons, including the fact that the No. 1 Operator was not
incapacitated, and as such retained overall control of the ride, including the
shutdown procedure. She was also unaware that it stopped the conveyor.
1021. Given the traumatic events that were unfolding, and the multiple tasks being
performed by both Ride Operators, it is understandable that there are
discrepancies in the recollections provided by Mr. Nemeth and Ms. Williams as
to the exact sequence of events prior to the tragic incident. As Ms. Williams had
only been trained that morning, her recollection and knowledge of the Operating
Procedures for the ride are understandably limited, and based on what she could
remember from her 1 ½ hours training with Ms. Crisp.
1022. The stress associated with operating the TRRR, let alone responding to an
emergency situation, was highlighted by Professor Sanderson. It is clear that the
38 signals and checks to be undertaken by the Ride Operators was excessive,
particularly given the failure to carry out any one could potentially be a factor,
which would contribute to a serious incident. There was no training provided to
Ride Operators or Ride Instructors as to how tasks should be prioritised, with
further hindrance provided by the poor user interface design of the Main Control
Panel. The stress associated with responding to an emergency situation, which
presented on the day of the tragic incident, in addition to the regular Ride
Operator duties to be carried out, would have made it difficult to determine what
should be done and in what order.
1023. Whilst it has been suggested by other staff, including some Supervisors, that Ms.
Williams should have pressed the E-Stop button at the Unload platform in the
circumstances that transpired on that tragic day, this simply does not accord with
the training she was provided that morning, the clear requirements of the
Operating Procedure Manual for the No. 2 Operator, nor the plain reading of the
Memorandum issued on 18 October 2016. Mr. Nemeth was not incapacitated
nor did he direct her to activate the E-stop. Rather he was standing at the Main
Control Panel, and as the No. 1 Operator, had primary responsibility for the
operation of the ride, which included the shutdown in a Code 6 situation. In these
circumstances, the fact that Ms. Williams did not press the E-Stop button, which
was unlabelled, is unsurprising. In addition, I have already referred to the
negative wording of the memorandum produced regarding the pressing of the
stop button. Had this been a positive direction to the No. 2 Operator to press the
stop button in the circumstances, the tragedy may have been averted.
1024. It is clear that the safe operation of the TRRR primarily relied upon administrative
controls, which required the Ride Operators to have an understanding and ability
to observe and respond to situations, including emergencies, as and when they
arise, including monitoring the water level, load and unload guests onto and off
rafts and to monitor guests movements. This lack of engineering controls on a
ride of this nature is unjustifiable.
Operator Responsibilities
1025. The responsibilities and substantial tasks placed on the Ride Operators at the
TRRR, particularly the No.1 Operator who had primary responsibility for the
operation of the ride and a supervisory role over the No. 2 and 3 Operators, were
clearly unreasonable and excessive. The TRRR was commonly recognised as
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 264 of 274

one of the more complex rides to operate at Dreamworld, largely due to the
manual elements, monitoring requirements and lack of automated controls. The
Main Control Panel was complex, confusing and lacked the required labelling.
1026. Operating Procedures for the rides at Dreamworld were drafted by members of
the Operations Department, with minimal input from E&T Department staff or
Safety Department. They were supplemented by Memorandums, which were
drafted by unknown authors. Those prepared for the TRRR, particularly with
respect to the use of the E-Stop at the Unload area, were ambiguous and poorly
worded, with relevant terms often left undefined. The expectation that a Ride
Operator would be able to become familiar with a detailed Operating Procedure
and the supplementary material, which sometimes conflicted, is wrong and poor
practice.
Response to the South Pump ‘Earth Fault’
1027. In the seven days prior to the fatal incident, there were five breakdowns of the
TRRR, which were attributed to a failure of the south pump due to an ‘Earth fault’.
On each occasion, the drive was reset without any diagnosis of the cause or
further investigation being conducted. Whilst Mr. Ritchie concluded that such a
fault was no more than an inconvenient and intermittent issue, it seems clear that
steps should have been taken to investigate the cause of the fault before the ride
was allowed to continue to operate. The fact that the fault caused the pump to
fail, rendering the ride inoperable, should have been sufficient to shut down the
ride until a deeper investigation had been conducted. Mr. Ritchie’s logic as to the
risk posed to guests or Ride Operator’s safety by the fault is unsound, as was
the decision to allow the ride to continue to operate pending the inspection by
Applied Electro.
1028. From the various accounts provided by members of the E&T Department, there
was clearly confusion as to how the Breakdown Policy was to be applied, and
whether a fault needed to occur two or three times before the matter was
escalated to a Supervisor. This clearly played a part in the fatal incident, given it
was the third breakdown of the ride that day. Furthermore, in relation to
ascertaining what may constitute ‘immediate danger’ for a particular ride,
including the TRRR, there was no specific training provided to staff nor any
guidance outlined in the procedure. During the inquest, evidence was given that
E&T staff were not provided with training as to any particular risks or dangers,
which might be present for a ride, or any particular component of a ride.
1029. Upon any reading of the requirements of the Breakdown Procedure, it seems
evident that the practice of resetting the drive for the South Pump following an
‘Earth Fault’, given the nature of the component and the recurring breakdowns
over the previous seven days, two of which occurred in close proximity of the
same day, was in contravention of the Procedure. It does not appear that the
Procedure was adhered to 25 October 2016 at the TRRR. Mr. Ritchie in his
evidence agreed that there had been a significant breakdown of the procedure
leading up to the incident.
1030. The various elements and components of this tragic incident, clearly
demonstrate a systemic failure by Dreamworld, in relation to all aspects of safety,
to ensure that the amusement rides open to the public were safe, well maintained
and designed to minimise the risk they posed to patrons and the staff. It is
unimaginable for the life of the TRRR that a failure of a pump and the
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 265 of 274

consequential drop in water level created immediately a known potential risk to
patrons. Why safety action was not taken earlier that day I find very difficult to
understand.
Examination of the sufficiency of the training provided to staff in operating the
Thunder River Rapids Ride.
1031. The manner in which new Ride Operators were trained, that is by unqualified
Senior Ride Instructors, had been in place at Dreamworld for many years prior
to the tragic incident. The time taken to train a Ride Operator seemed to be
dependent on the level of complexity and responsibility associated with the ride,
and at most, extended to a day on-site training with follow up the next morning.
During this time, Ride Operators were expected to become sufficiently familiar
with a ride specific Operating Procedure Manual, which for the TRRR, spanned
some 18 pages. This level of training, as was highlighted by Professor
Sanderson, was clearly inadequate, and led to extensive and necessary ‘on the
job’ learnt behaviour as to how to operate the ride effectively.
1032. Whilst there is no suggestion that the Instructors charged with training new Ride
Operators did so without the necessary due diligence, they were limited by the
training they had been provided and the expectations placed on them with
respect to the in-house training. Whilst the training Ms. Williams undertook on
the morning of the tragic incident was clearly insufficient for the extensive tasks
and functions she was required to perform, this was not due to any particular
failing by Ms. Crisp. Rather, it was evidence of an inherent lack of proper training
and process in place at Dreamworld to ensure the training provided to new Ride
Operators and Instructors was suitable for the roles and responsibilities to be
undertaken.
1033. Those responsible for managing the ride, whilst following the process and
procedure in place, were largely not qualified to perform the work for which they
were charged. Furthermore, the processes and procedures in place at
Dreamworld seem to have been created by unknown persons, who it is safe to
assume, lacked the necessary expertise. It seems that the practice at
Dreamworld was simply to accept what had always been done in terms of policy
and procedure, and despite change to safety standards and practices happening
over time, only limited and largely reactionary consideration was ever given to
making changes, which includes to the training provided to staff.
1034. The Operating Procedures in place in relation to the TRRR, which were
supplemented by further memorandums, were extensive and confusing. An
example of this was the use of the E-stop at the unload area, for which it was
expressly stipulated that it was not be utilised unless in an emergency. There
was no indication as to what constituted an ‘emergency’, nor were staff
adequately trained or provided with sufficient authority and situational awareness
to use the button when necessary. Furthermore, there were no emergency drills
undertaken at the Theme Park, despite recurring recommendations from internal
and external audits that this be undertaken. Had this been done, it may have
reduced the stressors associated with responding to such traumatic events, and
made such a response more effective.
1035. Regardless of the training provided at Dreamworld, it would never have been
sufficient to overcome the poor design of the TRRR, the lack of automation and
engineering controls. The responsibilities on the Ride Operators to respond to
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 266 of 274

various different situations and emergencies, as well as general operational
duties, was clearly excessive and unsound.
Consideration of the regulatory environment and applicable standards by which
Amusement Park rides operate in Queensland and Australia, and whether
changes need to be made to ensure a similar incident does not happen in the
future.
1036. While I accept the OIR submissions that they did undertake onsite auditing and
that they were very pro-active with the industry generally concerning safety, the
onsite auditing by the Regulator of amusement devices at Theme Parks in
Queensland prior to this tragedy obviously did not pick up the dangerous state
of the TRRR as described by the independent engineering experts and the OIR
inspectors who came to the site after the tragedy. It is also evident from the basis
of the extensions granted to Dreamworld for compliance with the annual renewal
registration in 2016, that there was an unjustified trust held by the Regulator as
to the sufficiency of the safety and maintenance systems in place to ensure the
safe operation of the high-risk plant. Clearly, given the nature of this tragedy, and
the surrounding circumstances, including the lack of record management, the
absence of any meaningful hazard assessments or effective engineering
oversight of these devices, this was simply not the case. During the inquest, Mr.
Chan acknowledged that the Regulatory framework in place at the time of the
incident in relation to amusement devices effectively expected Theme Parks to
have developed and implemented safety management systems, including
maintenance, operation, training and emergency control, with the qualified
engineering and other staff to action it. This was not the case at Dreamworld,
and should have been recognised by the Regulator had proper oversight of the
industry been in place.
1037. In response to this finding, some of the parties raise the issue of “hindsight
bias”. I have previously rejected this argument. It ignores the Australian
Standard prohibiting the creation of pinch points. It ignores the history of four
previous incidents, extremely similar in nature. It ignores the well-known danger
presented by the numerous and regular pump failures. This danger was well
known to the Operators, with prescribed responses set out in the Operator’s
manuals.
1038. The experts cited by Ardent Leisure in support of the hindsight bias contention
do not qualify as experts and are not independent. Indeed no independent expert
engineering or other suitably qualified independent witnesses were called except
by the Coroner. Those cited by Ardent were not sufficiently trained nor were any
of them engaged to consider the design of the TRRR holistically. Modifications
were made without much thought to the design of the ride, or other hazards such
changes may create. Further, Mr. Tan, as the only engineer, had a number of
responsibilities within the Park, and was moved to different positions at different
times throughout his tenure with Dreamworld. These hazards were obvious, and
were not identified as no-one was ever charged with conducting an appropriate
hazard and risk assessment of the ride. The engagement of Mr. Cruz to
commence a desktop review of the rides, further supports this lack of
consideration and risk assessment of the rides.
1039. In terms of hindsight bias as to the hazards present in the ride, it is clear the while
the maintenance and operational staff, as well as OIR inspectors who attended
site over the years, may not have identified such hazards, this was not because
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 267 of 274
they were not ‘obvious’. The experts made it clear that such hazards would have
been obvious to someone suitably qualified, who was charged with conducting a
holistic risk and hazard assessment of the TRRR. It was not the responsibility,
nor should it have been, for any of these individuals to conduct such a hazard
and risk assessment of the ride. This should have been a separate process to
the daily maintenance and operation of the ride. Clearly, this was not the role of
external auditors JAK, as was recognised by Dreamworld. Had a proper risk and
hazard assessment been done, it is likely that such obvious hazards would have
been identified. This was established and reiterated by the experts called by the
Coroner.
1040. Submissions are made that there was a 30-year history of incident free operation
of the TRRR. This submission ignores the four previous similar incidents. It is
quite true no one was injured. This is more good luck than good management.
One only has to recall Mr. Tan’s email and the report concerning the 2001
incident, which said, in part, ‘the push of the conveyor caused a compaction
effect, resulting in the rafts being caught at the unload area and one raft
flipping’. Mr. Tan’s email several years later in 2014, concerning another similar
incident, contained a salutary warning: - ‘This occurred on the rapid ride
several years ago, and fortunately there was no injury except for property
damage. I shudder to think if there had been guests on the rafts’.
1041. It is concerning that despite the multiple compliance activities, including site
visits, undertaken by the Regulator at Dreamworld between 2002 and 2016, the
deficiencies identified as to the maintenance, inspection, risk assessments,
record keeping and engineering oversight of these devices, was not detected.
Furthermore, the risks and hazards associated with the TRRR, including the nip
point, were not identified by any of the Inspectors, who at times had cause to
inspect the ride. Whilst limitations as to the intended purpose of these inspections
and attendance at the Theme Park is acknowledged, this failing raises concern
as to the sufficiency of the qualifications and training provided to Inspectors
responsible for auditing amusement devices.
1042. For older devices, like the TRRR, there is a significant concern as to the poor
mechanical integrity of the device, with a lack of modern safety controls and
automation, placing a significant and unfair burden on Ride Operators to
compensate for these lack of basic safety measures. While newly manufactured
and constructed amusement devices are generally engineered to higher
standards with greater safety measures and safeguards built in, there is a need
to ensure that such devices meet international technical standards, as well as
those stipulated in Australia. It is essential that any difference in these standards
are recognised and steps taken to ensure any shortfalls with a device
manufactured internationally is managed.
1043. Although annual inspections of amusement devices is mandated by the
Regulation, it is not a ‘major inspection’ of the device, and the enforcement and
check of such an inspection has been seriously lacking in Queensland for some
time. As was recognised in the BPR, a ‘major inspection’ should be carried out
by a competent person who had formal engineering qualifications and
experience, and needed to include an examination of all critical components of
the amusement device, as well as the effective and safe operation. Such a
person needed to be qualified to make recommendations about the severity of
faults observed and the intervals at which inspections and repairs needed to be
undertaken for the particular device. This was simply not the case at
Dreamworld. Whilst each of the members of the E&T Department were
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 268 of 274

technically qualified and experienced to perform their roles, this did not extend
to effectively and properly inspecting, maintaining and risk assessing the
amusement devices they were attending. Whilst the evidence of each of these
staff members shows that they performed their roles to the best of their abilities,
it is clear that there was a broader systemic problem with the lack of qualified
oversight of the procedures and practices in place by management.
1044. The extensive auditing by OIR carried out following the tragic incident with
respect to the prescribed annual inspections, whilst proper, served to
demonstrate the absence of adequate prior compliance activity undertaken by
the Regulator. This commitment to in-depth auditing of amusement devices will
need to continue under any proposed changes to the regulatory framework. It is
essential that for the regulation of amusement device in Queensland to be
effective and for owners to remain compliant, regular, ongoing and adequate
auditing of all aspects of the safety systems in place at the Theme Park will need
to be undertaken by the Regulator.
1045. Concern has been raised by the experts and SIA as to the lack of competent
professional engineers with the necessary experience to effectively inspect
amusement devices. OIR has stated that consultation will continue with industry
stakeholders, Engineers Australia and BPEQ, as to ensure this issue is further
progressed. Such steps will be necessary to ensure the effective compliance of
the proposed safety case regime once it comes into effect.
1046. The move to self-regulation is fraught with danger. Self-interest and the drive to
contain costs leads to the issues, which arose with the internally unqualified
engineer, and the type of investigation undertaken by Mr. Polley. The Regulation
lacked diligence in these matters.
1047. I accept the OIR, through their BPR and Industry Review, have taken steps to
correct the short-comings revealed in the evidence as set out above, however, it
has been necessary to draw attention to those matters by way of explanation for
the cause of the tragedy. It is to emphasize there were multiple causes all of
which must be recognised and addressed to prevent such a tragedy occurring
again. I accept there has been a considerable effort put in by the OIR to address
these issues.
1048. The OIR draws my attention to the difficulties arising when requiring all
amusement devices to comply with Australian Standards. This difficulty is
brought about by the fact that most amusement devices are designed and
manufactured overseas, predominantly based on European standards. Of
course, this was not the case with the TRRR. While I accept the obvious
difficulties this may present, it could and should be overcome by initial and
regular inspections when the devices are installed and operating in Australia.
This will ensure that such rides comply with obvious standards, such as the
Australian Standard to prevent nip points, like the extreme danger to passengers
presented by the TRRR should the raft be tipped up or passengers fall out into
the conveyor mechanism as was the case under consideration.
Mr. Polley’s Conduct
1049. With respect to the inspections undertaken by Mr. Polley, and the subsequent
annual plant renewal certification provided for the TRRR and other amusement
devices at Dreamworld, it is concerning that this was done without the provision
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 269 of 274
of any documentation pertaining to the ride. That this limited the scope of Mr.
Polley’s engagement by Dreamworld is clear, and his failure to ensure that he
was furnished with documentation relevant to his assessment, which is cited in
the certificate issued, falls below the industry standards expected of an RPEQ,
particularly those charged with inspecting amusement devices.
Changes Made at Dreamworld Following the Incident
1050. Since the tragic incident, significant changes have been made at Dreamworld,
including the audit and inspection of the amusement devices by qualified
Engineering firms, consideration of WHS practices, reviews of operating
procedures, changes to the training regime with emergency drills being
introduced, as well as the introduction of a safety management system to control
safety risks. Whilst these steps are certainly positive, they serve to highlight,
particularly given the established safety management systems in place at Village
Roadshow, how rudimentary and deficient the safety management practices in
place at Dreamworld were prior to this tragedy. Such a culpable culture can exist
only when leadership from the Board down are careless in respect of safety. That
cannot be allowed.
What further actions and safety measures could be introduced to prevent a
similar future incident from occurring?
1051. Considering the circumstances of this tragic incident, it is clear that the
recognised absence of adequate documentation and engineering controls
challenged and contradicts any assumption that the annual ride inspections
carried out by Dreamworld were a sufficient oversight mechanism (according to
the Regulations) for the public safety of the ride.
1052. The transition to a safety case and licensing regime in Queensland, as detailed
in the new Regulations, if enforced and audited regularly by the Regulator, will
certainly be a more rigorous and hands-on regulatory approach to the Major
Amusement Park industry. The requirement for a safety management system
certainly appears to be a far more comprehensive and integrated approach to
ensuring the effective management and control of risks with respect to
amusement devices. It is undoubtedly a significant move away from the current
self-regulatory nature of the industry. Given the circumstances of this tragic
incident, it is without question that more direct oversight and regular auditing of
the maintenance and inspection of amusement devices within the Theme Park
industry is necessary. It was acknowledged by OIR that there needed to be a
more holistic sign off with respect to amusement devices in Queensland, which
will likely require the engagement by the RPEQ of other specialists. It is essential
that there is regulatory oversight of this process to ensure compliance and that
safety is being systematically managed by the Amusement Park. The proposed
changes to the required competencies, training and instruction of those charged
with operating amusement devices, as outlined in the draft Regulation, are
necessary to ensure the safe operation of such a device.
1053. As was proposed by SIA, for this regime to be effective, spot checks of the annual
and major inspections carried out by the competent person, particularly of high-
risk rides, will need to be undertaken regularly by OIR. This will ensure
consistency and sufficiency of the sign-off. It will be incumbent on the Regulator
to ensure, through auditing and enforcement, that the approach taken by the
RPEQ engaged by the owner of the high-risk plant to undertake such an
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 270 of 274

inspection, thoroughly considers the history, maintenance, safety and
performance of the ride prior to certification. Those responsible for auditing the
Theme Parks will need to have the requisite skills and knowledge to be able to
effectively assess the suitability and sufficiency of the maintenance, inspection
and safety programs in place. If there is no appropriate history, then the device
should not be allowed to operate.
1054. From the draft Regulations provided, which are now in effect, it appears that the
proposed safety case and license regime will require detailed information on how
amusement devices will be maintained, inspected and tested to be submitted to
OIR. Matters, such as the maintenance of amusement devices, would then be
audited annually by the Regulator. It is this auditing oversight that will be
necessary to ensure compliance by owners with the new regulatory framework.
Until this event, there was an abject failure of obligation in this part of the
Regulation.
1055. I note that Counsel for Ardent Leisure Limited raise objection to the scope of the
inquest and any finding I make regarding the system of training in place at
Dreamworld contributing to the incidents as inappropriate, wrong, and beyond
the scope of the inquest. They also raise the same criticism of any finding relating
to the lack of record keeping. This submission is interesting given the material
willingly supplied by Ardent Leisure as to other rides within the Theme Park,
supplemented by the extensive oral evidence volunteered by Ardent employees
under extensive cross examination by all Counsel, including those appearing for
Ardent Leisure. I reject this submission in so far as it is relevant as this evidence
is clearly “connected to” and “relates to” the matters under consideration in this
inquest. See Doomadgee v Clements [2006] 2 Qd R 352 per Muir J paras 30-33.
RECOMMENDATIONS IN ACCORDANCE WITH s.46
1056. Section 46 of the Act provides that a Coroner may comment on anything
connected with a death that relates to:
a. public health and safety,
b. the administration of justice, or
c. Ways to prevent deaths from happening in similar circumstances in the
future.
1057. Given the concerns raised in this matter and the evidence provided during this
inquest, I make the following recommendations:
I. OIR
(a) Changes be made to the current regulatory framework in Queensland
with respect to the inspection and licensing of Major Amusement Park
devices to ensure that a more structured and compliance focused
regime is implemented. Given the circumstances of this tragic
incident, it is crucial that consideration is given to the following, when
changes to the Regulation are considered:
• The requirement that owners of amusement devices utilise a
safety management system to effectively manage and control
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 271 of 274
risks with respect to amusement devices.
• An owner of an amusement device must comply with the
applicable updated Australian Standards.
• Annual risk assessments should be conducted by competent
person/s and involve the detailed consideration of the device,
including all possible control system functions and variations,
as well as a detailed examination of the operation of the ride
during all modes of operation and possible emergency
conditions.
• The competency of those charged with operating an
amusement device.
• The requirement of a major inspection or full risk assessment
of the device by a competent person (RPEQ) at stipulated
intervals, as suggested by the manufacturer or at a mandated
duration (5 – 10 years).
• Regulations should make it clear of the onus placed on the
RPEQ when conducting an annual inspection or a major risk
assessment, which should include:
i. The operation of the ride should be visually observed
during a risk assessment.
ii. Low probability failures need to be actively
considered.
iii. Observe how the machine handles adverse events.
Run trial days where pumps are shut down, water
levels decreased (or increased), rafts bottle neck,
impact each other, to highlight weaknesses and
expose hidden features of the design.
iv. Consult Theme Park records internally and
internationally.
v. Consider whether the machine was fool-proof, and if
not what engineering controls could be possibly
utilised.
vi. Look at design records.
• Regular auditing and oversight of such devices, as well as the
associated inspections and required safety systems in place
at the Major Amusement Park, must be conducted by the
Regulator.
Whilst the safety case regime introduced by the recent amendments
to the Regulations would appear to ensure this necessary regulatory
oversight by way of a more mandated approach to the maintenance
and inspection of amusement devices, it is essential that this be
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 272 of 274

monitored and maintained by way of regular and effective auditing.
Such auditing should be undertaken by suitably qualified and trained
OIR Inspectors. Major Amusement Parks in Queensland need to be
required to implement effective control measures with respect to the
devices in operation, and the Regulator must actively ensure this
takes place.
Strict adherence to the timeframes proposed by the safety case and
licensing regime in the draft Regulation should be maintained in order
to ensure the expedited introduction of a more intense regulatory
framework for Major Amusement Parks in Queensland and, most
importantly, patron’s safety.
(b) That OIR continue to develop a Code of Practice for the amusement
device industry in Queensland, which will establish a minimum
standard for the operation of amusement devices, in consultation with
the requisite industry stakeholders, including the Amusement Device
Working Group.
(c) That efforts to harmonise the requirements of the relevant design
standards, particularly the critical safety requirements on amusement
devices in Australia, Europe and America continue in consultation
with relevant industry stakeholders.
(d) Steps be taken to rectify the lack of detailed knowledge of Safety
Related Control Circuits held by the majority of OIR Inspectors.
II. Other agencies
(a) The Board of Engineers, in consultation with OIR and other industry
groups, to continue efforts to address the shortfall in suitably qualified
and experienced RPEQ’s with respect to the inspection of
amusement devices.
(b) That a reassessment of the Australian Standards applicable to
waterborne rides (including raft rides) be undertaken to include some
of the types of safety requirements associated with roller coasters,
including more thorough considerations for lifts/elevators, collisions
and passenger loading/unloading.
(c) Consideration as to whether the requirement for hazard identification
and risk assessment in AS-3533.2 section 5.1 should be made
mandatory. Furthermore, whether any modification or alteration to the
ride should require hazard identification and risk assessment to
ensure that changes made do not affect safe operation and use.
DISCRETION TO REFER IN ACCORDANCE WITH s.48 (4)
1058. Section 48 of the Act gives the Coroner discretion to refer information obtained
whilst investigating a death, to give the information to the appropriate prosecuting
authority, if the Coroner ‘reasonably suspects a person has committed an
offence’.
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 273 of 274
1059. A referral can also be made pursuant to s.48 as to a person’s professional
conduct to the relevant professional disciplinary body if the Coroner reasonably
believes the information might cause that body to inquire or take steps in relation
to the conduct.
Referral of Ardent Leisure Limited to the OIR
1060. It is reasonably suspected that Ardent Leisure may have committed an offence
under workplace law. Whilst various breaches of the WHS Act have previously
been considered by OIR with respect to this incident, the details of which have
been included in the inquest brief, given the significant further documentary
material provided during the course of the coronial inquiry, and produced at
inquest. I refer my Findings and the evidence gathered in the course of the
Inquest to OIR for further consideration as to these matters. Whether there is
sufficient evidence to proceed to prosecution is a matter for OIR.
Mr. Polley
1061. It is arguable that Mr. Polley’s conduct in issuing the subsequent annual plant
renewal certification for the TRRR and other amusement devices at Dreamworld,
without any documentation pertaining to the ride being supplied by the Park and
his failure to properly inspect the ride, was a failure, which falls below the industry
standards expected of an RPEQ, particularly those charged with inspecting
amusement devices. For this reason, I refer his conduct to the Board of
Professional Engineers of Queensland.
I close the inquest
James McDougall
Coroner
Southern Region
Findings of the inquest into the death of Kate Louise Goodchild
Luke Jonathan Dorsett, Cindy Toni Low & Roozbeh Araghi
Page 274 of 274
