DRINK
DRIVING
A road safety manual for
decision-makers and practitioners
Drink driving: a road safety manual for decision-makers and practitioners
A road safety manual for
decision-makers and practitioners
DRINK DRIVING

© International Federation of Red Cross and Red Crescent Societies 2022. All rights reserved. This publication or any part thereof may
not be reproduced, distributed, published, modified, cited, copied, translated into other languages or adapted without prior written
permission from the International Federation of Red Cross and Red Crescent Societies. All photos used in this document are copyright
of the IFRC unless otherwise indicated.
Module break photo source: Police MTTD, Accra.
Recommended citation:
Drink Driving: a road safety manual for decision-makers and practitioners, second edition. Global Road Safety Partnership, International
Federation of Red Cross and Red Crescent Societies, Geneva; 2022.
Design by Inis Communication
Preface v
Acknowledgements vii
Executive summary ix
Introduction 1
Why were these manuals developed? 1
Why were these manuals revised? 1
Safe System Approach 2
References 3
Module 1 Why must we address drink driving? 5
1.1 The context and magnitude of the drink driving problem worldwide 5
1.2 How is alcohol measured? 6
1.3 Effects of alcohol 7
1.4 Prevalence and economic impact 9
1.5 Risk factors for drink driving crash involvement 9
Module Summary 10
References Module 1 11
Module 2 Evidence-based interventions 15
2.1 Legislation 17
2.2 Licence Restrictions (Effective) 22
2.3 Offender Management 22
2.4 Public Education 24
2.5 Other effective legal measures 28
2.6 Engineering countermeasures 30
2.7 Post-crash response 30
Module Summary 31
References Module 2 32
Contents
iii
Module 3 Enforcing drink driving laws 37
3.1 Enforcement methods 39
3.2 Safely intercepting vehicles 44
3.3 A dedicated alcohol intervention unit 47
3.4 Penalties for drink driving offences 47
Module Summary 48
References Module 3 49
Module 4 Implementing evidence-based drink driving
interventions 51
4.1 Cycle of improvement 51
4.2 Pathways to change 52
4.3 Assessing the situation 53
4.4 Opportunities and challenges in implementing drink driving interventions 60
4.5 How to evaluate progress and use results for improvement 63
Module Summary 65
References Module 4 66
Appendix A. Suggested wording for draft drink driving
legislation 69
Section 1: Who must undergo a breath screening test 69
Section 2: Adult drink driving 69
Section 3: Zero alcohol for under 20 / novice drivers 70
Section 4: Drink or drug driving causing injury or death 70
iv

Preface
Road traic injuries are a major public health problem and a leading cause of death and injury around the
world. Each year approximately 1.3 million people die and millions more are injured or disabled as a result
of road crashes, mostly in low- and middle-income countries. As well as creating enormous social costs
for individuals, families and communities, road traic injuries place a heavy burden on health services
and economies. The cost to countries, many of which already struggle with economic development,
may be as much as 5% of their gross national product. As motorization increases, preventing road
traic crashes and the injuries they inflict will become an increasing social and economic challenge,
particularly in low-and middle-income countries. If the present trend continues, road traic injuries will
increase dramatically in most parts of the world over the next two decades, with the greatest impact
falling on the most vulnerable citizens.
Appropriate and targeted action is urgently needed. The World report on road traic injury prevention,
launched jointly in 2004 by the World Health Organization and the World Bank, identified improvements
in road safety management and specific actions that have led to dramatic decreases in road traic
deaths and injuries in industrialized countries active in road safety. The use of seat-belts, helmets and
child restraints, the report showed, has saved thousands of lives. The introduction of speed limits, the
creation of safer infrastructure, the enforcement of limits on blood alcohol concentration while driving,
and improvements in vehicle safety are all interventions that have been tested and repeatedly shown
to be eective.
The international community must continue to take the lead to encourage good practice in road safety
management and the implementation of the interventions identified in the previous paragraph in
other countries, in ways that are culturally appropriate. To speed up such eorts, the United Nations
General Assembly has passed a number of resolutions urging that greater attention and resources be
directed towards the global road safety crisis. These resolutions stress the importance of international
collaboration in the field of road safety. These resolutions also reairm the United Nations’ commitment
to this issue, encouraging Member States to implement the recommendations of the World report on
road traic injury prevention and commending collaborative road safety initiatives so far. In particular,
they encourage Member States to focus on addressing key risk factors and to establish lead agencies
and coordination mechanisms for road safety. These were further encouraged through the Moscow
Declaration (2009), Brasilia Declaration (2015) and the Stockholm Declaration (2020).
Preface v
To contribute to the implementation of these resolutions, the World Health Organization, the Global
Road Safety Partnership, the FIA Foundation, and the World Bank have collaborated to produce a
series of manuals aimed at policy-makers and practitioners. This manual on drink driving is one of
them. Initially published in 2007, it has been updated to include new evidence and case studies. Each
manual provides guidance to countries wishing to improve road safety and to implement the specific
road safety interventions outlined in the World report on road traic injury prevention.
They propose simple, cost-eective solutions that can save many lives and reduce the shocking burden
of road traic crashes around the world. We encourage all to use these manuals.
Etienne Krug
Director
Department of Social
Determinants of Health
World Health Organization
David Cli
Chief Executive Oicer
Global Road Safety
Partnership
Saul Billingsley
Executive Director
FIA Foundation
Nicolas Peltier
Global Director for
Transport Sector
Infrastructure
Practice Group
The World Bank
vi Drink driving: a road safety manual for decision-makers and practitioners

Acknowledgements
The World Health Organization (WHO) coordinated the production of this revised manual and
acknowledges, with thanks, all who contributed to its preparation. Particular thanks are due to the
people listed below.
Advisory Committee (1st edition): Saul Billingsley (FIA Foundation), Gayle Di Pietro (Global Road
Safety Partnership), Dipan Bose (World Bank).
Advisory Committee (2nd edition): Nhan Tran & Meleckidzedeck Khayesi (World Health
Organization), Margie Peden (The George Institute for Global Health), Dave Cli & Judy Fleiter (Global
Road Safety Partnership), Natalie Draisin (FIA Foundation), Alina Burlacu (World Bank).
Project coordinator (2nd edition): Meleckidzedeck Khayesi.
Writers (2nd edition): Judy Fleiter, Cristina Inclán-Valadez, Chika Sakashita, Dave Cli, Brett
Harman, Al Stewart, Margie Peden and Meleckidzedeck Khayesi.
Reviewers (2nd edition): Natalie Draisin, Barry Watson, Dante Rosado, and Marisela Ponce De
Leon Valdes.
Literature review (2nd edition): Martha Hijar, Cristina Inclán-Valadez.
Financial support: Financial support to update this manual was provided by Bloomberg
Philanthropies and the Global Road Safety Partnership.
Acknowledgements vii
viii Drink driving: a road safety manual for decision-makers and practitioners

Executive summary
Alcohol plays a cultural and social role in many societies. However, the harmful eects of alcohol
that are experienced in many aspects of daily life are undeniable. In the context of improving road
safety outcomes, the need to manage harmful levels of alcohol use remains a paramount challenge.
Eective campaigns to reverse the level of community acceptance of drink driving behaviour, coupled
with sustained and well-resourced enforcement of strong anti-drink driving laws, has seen significant
reductions in alcohol-related road crashes in many jurisdictions. However, more must be done.
This manual provides advice and examples that, if implemented accordingly, will reduce the prevalence
of drink driving and associated road trauma. The manual is aimed at policy-makers and road safety
practitioners and draws on experience from countries that have succeeded in achieving and sustaining
reductions in alcohol-related road trauma. It includes recommendations for developing and implementing
drink driving legislation and advice on how to monitor and evaluate progress. A particular focus is the
design and implementation of interventions that include legislation, enforcement and public education/
advocacy measures. Importantly, these interventions must work in concert to achieve optimal results.
In developing the material for this manual, the writers have drawn on case studies from around the
world to illustrate examples of “good practice”. This 2nd edition of the manual was produced in 2022 to
reflect changes in road safety data, evidence and good practices, particularly evidence from low- and
middle-income countries. Strategies that work in one country may not necessarily transfer eectively
to another. The manual attempts to reflect a range of international experiences but does not oer
prescriptive solutions. Rather, it is hoped that the manual acts as a catalyst for local initiatives and actions
to improve road safety. It provides information and evidence that stakeholders can use to generate their
own solutions and develop advocacy and awareness-raising tools and legislation to reduce alcohol-
related road trauma.
Executive summary ix


Introduction
Why were these manuals developed?
The World Health Organization (WHO), the World Bank, the FIA Foundation and the Global Road
Safety Partnership (GRSP) produced a series of good practice manuals, following the publication of
the World report on road traic injury prevention in 2004, which provide guidance on implementation
of interventions to address specific risk factors in road safety. The topics covered in the initial series
of manuals are: helmets (2006), drinking and driving (2007), speed management (2008), seat-belts
and child restraints (2009), data systems (2010), pedestrian safety (2013), road safety legislation (2013),
powered two- and three-wheeler safety (2017) and bicyclist safety (2020). In addition, WHO produced
a road safety technical package, Save LIVES (2017), which presents evidence on 22 evidence-based
interventions related to speed management, leadership, infrastructure, vehicles, enforcement and post-
crash care. These documents are available in multiple languages on the World Health Organization
website at https://www.who.int/violence_injury_prevention/publications/road_traic/en/.
Why were these manuals revised?
Since the series of manuals was first published, the scientific evidence base relating to various risk
factors and the eectiveness of interventions has continued expanding. Contemporary research has
refined our knowledge about specific risk factors, such as distracted driving, and vehicle impact speed
and risk of death for pedestrians. New issues and practices have arisen, such as a tropical helmet
standard and anti-lock braking system (ABS) for motorcycles. New and existing interventions have
been implemented and evaluated, with increasing application in low- and middle-income countries.
Research attention and policy response has also increasingly been applied to emerging road safety
issues including e-bikes, drugs other than alcohol, fleet safety, urban mobility, micro mobility options,
air and noise pollution, public transport, and technological advances.
As a result of these developments, the good practice manuals required revision so that they can continue
to be key references for road safety policy implementation and research. This is particularly important,
given the emphasis placed on road safety within the framework of the 2030 Agenda for Sustainable
Development and because of the global impetus to reduce road deaths and injuries resulting from
the declaration of the two United Nations’ Decades of Action for Road Safety (2011–2020 and 2021–
2030). The manuals have been revised to reflect these developments as they continue to be valuable
resources providing evidence-based and cost-eective solutions to save lives and reduce injuries. An
extensive literature review has informed the revision and updating of all the manuals, and additional
information has been collated to allow more contemporary case studies to be showcased. In addition,
there was an identified need to broaden the topics covered in the manuals to include aspects such as
qualitative research methods, and participatory approaches to designing and evaluating interventions.
An emphasis on shifting traditional thinking away from blaming road users towards more contemporary
frameworks, such as the Safe System Approach is key in the revised manuals. An area requiring ongoing
consideration is decolonising knowledge and practice within the road safety field.
Introduction 1

Safe System approach
The Safe System approach recognizes that road transport is a complex system and places safety at its
core (1). It also recognizes that humans, vehicles and the road infrastructure must interact in a way that
ensures a high level of safety (Figure 1). A Safe System, therefore:
anticipates and accommodates human errors;
incorporates road and vehicle designs that limit crash forces to levels that are within human tolerance
to prevent death or serious injury;
motivates those who design and maintain the roads, manufacture vehicles, and administer safety
programmes to share responsibility for safety with road users, so that when a crash occurs, remedies
are sought throughout the system, rather than solely blaming the driver or other road users;
pursues a commitment to proactive and continuous improvement of roads and vehicles so that the
entire system is made safe rather than just locations or situations where crashes last occurred; and
adheres to the underlying premise that the transport system should produce zero deaths or serious
injuries and that safety should not be compromised for the sake of other factors such as cost or the
desire for faster transport times (1).
Figure 1. Safe System approach
W
o
r
k
t
o
p
r
e
v
e
n
t
c
r
a
s
h
e
s
t
h
a
t
r
e
s
u
l
t
i
n
d
e
a
t
h
o
r
d
e
b
i
l
i
t
a
t
i
n
g
i
n
j
u
r
y
HUMAN
TOLERANCE
OF CRASH
IMPACTS
SAFE
SPEEDS
SAFE ROAD
USERS
SAFE
VEHICLES
I
n
n
o
v
a
t
i
o
n
D
a
t
a
a
n
a
l
y
s
i
s
,
r
e
s
e
a
r
c
h
a
n
d
e
v
a
l
u
a
t
i
o
n
R
o
a
d
r
u
l
e
s
a
n
d
e
n
f
o
r
c
e
m
e
n
t
L
i
c
e
n
s
i
n
g
a
n
d
r
e
g
i
s
t
r
a
t
i
o
n
E
d
u
c
a
t
i
o
n
a
n
d
i
n
f
o
r
m
a
t
i
o
n
M
o
n
i
t
o
r
i
n
g
,
m
a
n
a
g
e
m
e
n
t
a
n
d
c
o
o
r
d
i
n
a
t
i
o
n
SAFE ROADS
AND ROADSIDES
Source: (2)
2 Drink driving: a road safety manual for decision-makers and practitioners
References
1.
Global Plan: Decade of Action for Road Safety 2021-2030. Geneva, Switzerland: World Health Organization,
2021. https://cdn.who.int/media/docs/default-source/documents/health-topics/road-traic-injuries/
global-plan-for-road-safety.pdf?sfvrsn=65cf34c8_33&download=true. Accessed 24 January 2022.
2. Department of Transport and Main Roads, Queensland Government, Australia. Safer roads, safer
Queensland: Queensland’s road safety strategy 2015–21. Department of Transport and Main Roads,
Queensland Government, Australia, 2015.
Introduction 3

1

Module 1
Why must we address drink
driving?
Alcohol has many functions in society and represents cultural, religious and symbolic meanings in most
countries. However, it is also a drug with many toxic eects and other dangers such as intoxication and
dependence. It is not the only substance that can impair driving performance. Impaired driving can result
from various things including alcohol consumption, use of licit and illicit drugs, and being unable to
function at optimal capacity because of fatigue. While all aspects of impaired driving deserve appropriate
attention, the focus of this manual is on drink driving. This module provides information on the global
problem and risks associated with drinking and driving. The information and recommendations in this
module can be useful in persuading political leaders and the public to support interventions that reduce
the prevalence of drink driving and associated harms.
1.1 The context and magnitude of the drink driving problem
worldwide
An extensive body of literature identifies that driving after drinking alcohol significantly increases the
risk of a crash and the severity of that crash, resulting in deaths and serious injuries. In its latest reports,
the WHO estimates that between 5% and 35% of global road deaths are alcohol related (1, 2). In most
high-income countries about 20% of fatally injured drivers have blood alcohol concentration (BAC)
levels above the legal limit (1). Studies in low- and middle-income countries have shown that between
33% and 69% of fatally injured drivers and between 8% and 29% of non-fatally injured drivers had
consumed alcohol before their crash (1). Figure 2 depicts the attribution of road traic deaths to alcohol
from a range of countries.
Module 1 Why must we address drink driving? 5

Figure 2. Attribution to road traffic deaths to alcohol [2013, 2014 data]
0%
5%
10%
15%
20%
25%
30%
35%
Costa Rica
Canada
USA
New Zealand
Sweden
Russian Federation
Mexico
Cyprus
Australia
Thailand
Chile
UK (exludes NI)
Poland
R of Korea
R of Moldova
Peru
Germany
Ecuador
Romania
Ethiopia
India
Morocco
UR of Tanzania
Uganda
Denmark
% of annual RT fatalities attributed to alcohol.
Over the national legal limit
Note: Data on legislation and policies represent the country situation in 2014 while data on fatalities and vehicle registrations
are for 2013, or the most recent year for which these data were available. For method of estimation please refer to https://www.
who.int/data/gho/indicator-metadata-registry/imr-details/208.
Source: (3) with author’s elaboration.
1.2 How is alcohol measured?
Although it can be diicult to attribute a crash to a particular cause or causes, decisions about whether a
crash was alcohol-related are often based on how much, if any, alcohol was present in the bloodstream
or breath of the road users involved. To quantify the extent of the drink driving risk in a jurisdiction,
the most reliable measurement is the number of drivers fatally injured and found to have a
blood alcohol concentration (BAC) over the legal limit. The amount of alcohol contained within
the bloodstream or breath can be measured by testing a small sample of blood, urine, or through
analysis of exhaled breath. The results of a breath analysis may be expressed in terms of blood alcohol
concentration (BAC). For example:
mg/100ml:– milligrams of alcohol per 100 millilitres of blood
g/dl:– grams of alcohol per decilitre of blood.
The results of a breath analysis may also be expressed directly in terms of breath alcohol concentration
(BrAC) as below:
mg/L:– milligrams of alcohol per litre of breath
mcg/L:– micrograms of alcohol per litre of breath.
Table 1 shows the relationship between these various terms.
6 Drink driving: a road safety manual for decision-makers and practitioners
Table 1. Relationship between various blood and breath alcohol concentration levels
BAC BrAC
mg/100ml g/dl mg/L mcg/L
20 0.02 0.10 100
50 0.05 0.24 240
80 0.08 0.38 380
Complete data showing the involvement of alcohol in all crashes are not always available. However, this
can be assisted by thorough investigation of crashes, the collection of evidence to identify risk factors,
and a system to analyse data and facilitate the development of road safety interventions.
Furthermore, the available data from dierent countries may not be comparable because of dierences
in the legal definitions of drink driving and in alcohol testing requirements for crash-involved drivers.
Despite these issues, data from various countries clearly demonstrate the major role that alcohol plays
in driver, passenger, and other road user deaths and serious injuries:
26%– 31% of non-fatally injured drivers in South Africa have BAC levels exceeding the country’s limit
of 0.05 g/100 ml (4);
in Thailand, nearly 44% of traic injury victims in public hospitals had BAC levels of 0.10g/100ml or
more (5);
in Colombia, 34% of driver fatalities and 23% of motorcycle fatalities are associated with speed and/
or alcohol (6);
in the United States of America, half a million people are injured and 17,000 killed every year in drink
driving-related traic crashes, and almost 40% of all youth road fatalities are directly related to alcohol
consumption (7);
in Sweden, the Netherlands and the United Kingdom, the proportion of fatally injured drivers with
excess alcohol levels is around 20%, although the legal limits in these countries dier considerably,
being 0.02 g/100 ml, 0.05 g/100 ml and 0.08 g/100 ml, respectively (8);
in Mexican municipalities, 19.5% of car occupant deaths due to road traic injuries were attributable
to alcohol consumption (9);
in Peru and the Dominican Republic, self-reported data from road users treated for road traic injuries
in emergency departments indicated that approximately 15% had consumed alcohol in the six hours
prior to their injury (10).
1.3 Effects of alcohol
The immediate eects of alcohol on the brain can be depressing or stimulating in nature, depending
on the quantity consumed, which causes degradation of driving performance directly related to BAC
levels. Alcohol results in impairment which increases the likelihood of a crash because it produces
poor judgement, increased reaction time, lower vigilance and decreased visual acuity. Physiologically,
alcohol also lowers blood pressure and depresses consciousness and respiration. It can take two to
three hours for the body to metabolise alcohol from one to two drinks, and up to 24 hours to process
the alcohol from eight to ten drinks.
Module 1 Why must we address drink driving? 7
A common issue in all jurisdictions is the lack of awareness of how much alcohol is required to adversely
impact a person’s coordination and concentration. As a result, some jurisdictions have used the concept
of a ‘standard drink’ to help inform the public about how much of what types of alcohol can reasonably
be expected to be consumed by a person before they reach the legal BAC limit. Importantly, it takes
very little alcohol to result in a person being over the legal limit. Because of this, the message
from all road safety partners needs to be clear – ‘don’t drink and drive’.
Alcohol can impair judgement and increase crash risk, even at relatively low BAC levels and the eects
become progressively worse as the BAC increases. In 1964, a case-control study was carried out in
Michigan in the United States, known as the Grand Rapids study (11). It showed that drivers who had
consumed alcohol had a much higher risk of involvement in crashes than those with a zero BAC, and
that this risk increased rapidly with increasing blood alcohol levels. These results were corroborated and
improved upon by studies over subsequent decades (12, 13, 14, 15). Many of these studies provided the
basis for setting legal blood alcohol limits and breath content limits in many countries around the world.
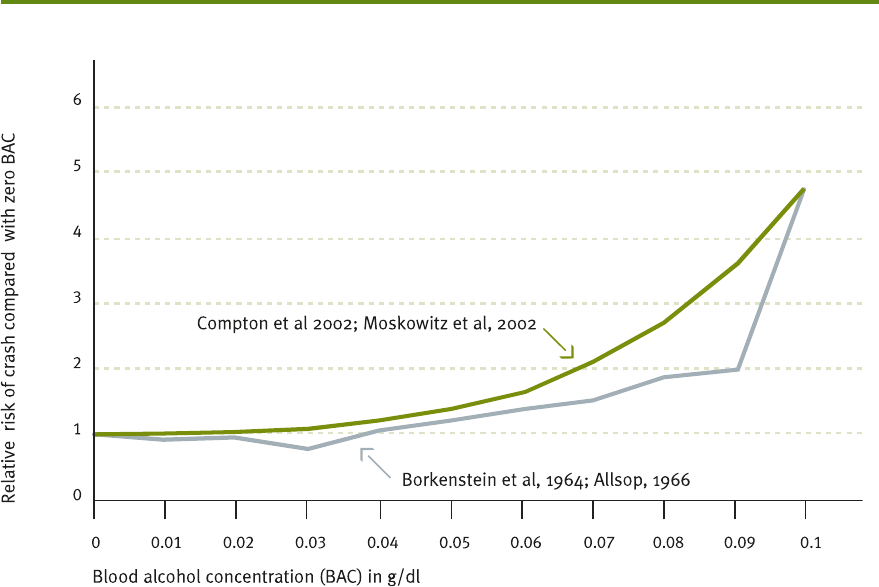
An extensive body of research demonstrates that the higher the blood alcohol level, the more rapidly
the risk of being involved in a casualty crash increases. The relative risk of crash involvement starts to
increase significantly at a BAC level of 0.04 g/dl (see Figure 3).
Figure 3. Relationship between driver’s BAC and relative risk of involvement in a casualty crash
Source: (original sources 11, 14, 17, 18. Combined graphic source 16)
Due partly to its tendency to reduce inhibition, the consumption of alcohol is often associated with other
risk behaviours such as non-use of seat-belts or helmets, unsafe speed choice, and the use of other
drugs which can further impact upon driving performance (19). In addition, the presence of alcohol in
the body adversely aects the diagnosis, management, and treatment of and recovery from injuries
8 Drink driving: a road safety manual for decision-makers and practitioners
because alcohol intoxication can complicate patient assessment and management (e.g., alcohol eects
can mimic head injury symptoms), and can exacerbate underlying medical conditions.
1.4 Prevalence and economic impact
Despite the well-known risks, drink driving remains prevalent around the world. A report from 32
countries indicated that the proportion of car drivers who report driving after drinking alcohol ranges
from 5% in Hungary to 34% in Portugal, from 4% in Japan to 24% in Australia, below 15% in Morocco and
Egypt to 32% in South Africa (20). Additionally, self-report data from road users treated for road traic
injuries in emergency departments in Peru and the Dominican Republic indicated that approximately
15% had consumed alcohol in the six hours prior to their injury (10). The estimated economic costs of
drinking and driving are also significant. In the United States, the total economic cost of motor vehicle
crashes in 2000 was estimated at US$ 230.6 billion, with drink driving-related crashes accounting for
US$51.1 billion, or 22% of all economic costs (7).
In the low- and middle-income country context, applying recent data on the incidence of drink driving
crashes to estimates of the total cost of road crashes in such countries (as outlined in the World report
on road traic injury prevention) established robust estimates (21). For example, in South Africa, applying
the estimate that alcohol is a factor in 31% of non-fatal crashes to the estimated hospital costs of US$
46.4 million attributed to road crashes, crashes involving drink driving cost the health system around
US$14 million. Using the same application in Thailand, where at least 30% of crashes are linked to alcohol
and the total cost of road crashes is estimated at $US3 billion (22), crashes involving drink driving cost
approximately $US 1 billion.
1.5 Risk factors for drink driving crash involvement
Drink driving oenders are commonly classified as first-time oenders or repeat oenders. Research
(largely from high-income countries) indicates that drink drivers are commonly characterised as (10, 23, 24):
male
18–44 years old
from a low socio-economic grouping
single or divorced
in a blue-collar occupation
of low education and limited literacy
of low self-esteem and
having started drinking at an early age (at age 14 or younger) (24).
Drink driving crashes commonly exhibit a number of characteristics:
Single vehicle crashes and high speed – drink driving crashes often involve high speed and a single
vehicle running o the road. Many of these crashes also result in the vehicle hitting a fixed roadside
object. In urban areas these can be signs or electricity poles, while in rural areas it is usually trees,
culverts, bridge ends and fence posts.
Module 1 Why must we address drink driving? 9
Night and/or weekend crashes – drink driving crashes occur more often at night (when more
alcohol is consumed) and generally on weekends or periods of high leisure activity.
Increased severity of injury – this is partly because once a crash and the injury-causing impact
has occurred, the existence of alcohol in the body of the injured works to limit the extent and level
of recovery from injury.
A study from India highlights the issue of severity of injuries: the National Institute of Mental Health
and Neurosciences, Bangalore [NIM-HANS] estimated that 21% of people who sustained brain injuries
during a crash were under the influence of alcohol (physician confirmed diagnosis) at the time, and
that 90% had consumed alcohol within three hours prior to the crash. (25)
Although much of the research on alcohol-related crashes has focused on car crashes, many of the
characteristics of alcohol-related motorcycle crashes are the same. A study in Thailand (26) indicated
that compared to non-drinking riders, drinking riders tended to crash at night, to have more non-
intersection crashes and more crashes on curves, were more likely to lose control, run o the road,
violate a red signal, be inattentive, and for rider error to be a contributing cause of the crash. Drinking
riders were five times more likely to be killed than non-drinking riders. It is also important to recognise
that alcohol consumption by drivers of four-wheelers puts pedestrians, cyclists, and riders of motorised
two- and three-wheelers at risk.
In parts of the world where the incidence of drink driving-related crashes is considered to be relatively
low (for example, where motorisation levels are low or where alcohol use is forbidden) countries should
be proactive in monitoring the situation so that it can be managed and prevented from escalating. The
magnitude of the drink driving problem, and its harmful consequences in terms of deaths and serious
injuries, highlights the critical need to invest in countermeasures to reduce this risky behaviour. Eective
interventions are presented in the next module.
Module Summary
Drink driving is a major road safety problem in many countries.
Even in quite modest amounts, alcohol impairs the functioning of several processes required for safe
road use, and drink driving can result in severe crashes involving deaths and serious injuries.
Alcohol consumption is associated with other risk behaviours such as non-use of seat-belts or helmets,
unsafe speed choice, and the use of other drugs which can further impact upon driving performance.
Research indicates that crashes involving drink driving and those who are more likely to drink and
drive display common characteristics, which may inform intervention targets.
10 Drink driving: a road safety manual for decision-makers and practitioners
References Module 1
1.
Global status report on road safety 2018. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA
3.0 IGO.
2. Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018. Licence: CC
BY-NC-SA 3.0 IGO
3. World Health Organization. The global health observatory indicators. Attribution of road traic deaths to
alcohol %.https://www.who.int/data/gho/data/indicators.Accessed20 December 2021.
4.
Parry CD, Pliiddemann A, Donson H, Sukhai A, Marais S, Lombard C. Cannabis and other drug use among
trauma patients in three South African cities, 1999–2001. South African Medical Journal. 2005;95(6).
5. Lapham SC et al. Use of audit for alcohol screening among emergency room patients in Thailand.
Substance Use and Misuse, 1999, 34:1881–1895.
6. Posada J, Ben-Michael E, Herman A. Death and injury from motor vehicle crashes in Colombia. Pan
American Journal of Public Health, 2000, 7:88–91.
7.
Traic safety facts 2000: alcohol. Washington DC, National Highway Traic Safety Administration (Report
DOT HS 809 3232001) cited in Drinking and Driving: a road safety manual for decision-makers and
practitioners. Geneva, Global Road Safety Partnership, 2007.
8.
Koornstra M et al. Sunflower: a comparative study of the development of road safety in Sweden, the United
Kingdom and the Netherlands. Leidschendam, Institute for Road Safety Research, 2002.
9.
Santoyo-Castillo, D., Perez-Nunez, R., Borges, G., & Hijar, M. (2018). Estimating the drink driving attributable
fraction of road traic deaths in Mexico. Addiction, 113(5), 828–835.
10. Cherpitel CJ, Witbrodt J, Ye Y, Monteiro MG, Málaga H, Báez J, Valdés MP. Road traic injuries and
substance use among emergency department patients in the Dominican Republic and Peru. Revista
panamericana de salud publica. 2021 Apr 30;45:e31.
11. Borkenstein RF, Crowther RF, Shumante RP, et al. The role of the drinking driver in traffic
accidents.Bloomington, IN: Department of Police Administration, Indiana University; 1964.
12. McLean AJ, Holubowycz OT. Alcohol and the risk of accident involvement. In: Goldberg L, ed. Alcohol,
drugs and traic safety. Proceedings of the 8th International Conference on Alcohol, Drugs and Traic
Safety, Stockholm, 15–19 June 1980. Stockholm, Almqvist & Wiksell International, 1981:113–123.
13. Hurst PM, Harte D, Frith WJ. The Grand Rapids dip revisited. Accident Analysis and Prevention, 1994,
26:647–654.
14. Crompton RP et al. Crash risk of alcohol-impaired driving. In: Mayhew DR, Dussault C, eds. Proceedings
of the 16th International Conference on Alcohol, Drugs and Traic Safety, Montreal, 4–9 August 2002.
Montreal, Societe de l’assurance automobile du Quebec, 2002:39–44.
15. Keall MP, Frith W & Paterson TL, The influence of alcohol, age and number of passengers on the night-
time risk of driver fatal injury in New Zealand, Accident Analysis and Prevention, 2004, 36(1): 49–61.
16. Racioppi, Francesca, et al.Preventing road traic injury: a public health perspective for Europe. No.
EUR/04/5046197. Copenhagen: WHO Regional Oice for Europe, 2004:47. Data from Crompton et. al,
2002; Borkenstein et al, 1964; Allsop, 1966; and Mokovitz et al, 2002. https://www.euro.who.int/__data/
assets/pdf_file/0003/87564/E82659.pdf Accessed 21 January 2022.
17. Allsop, R. E. Alcohol and road accidents: a discussion of the Grand Rapids study. RRL Report No.6. 1966.
Module 1 Why must we address drink driving? 11
18.
Moskowitz H et al. Methodological issues in epidemiological studies of alcohol crash risk. In: Mayhew DR,
Dussault C, eds. Proceedings of the 16th International Conference on Alcohol, Drugs and Traic Safety,
Montreal, August 2002. Quebec, Société de l'assurance automobile du Québec, 2002:45–50.
19. Marr JN. The interrelationship between the use of alcohol and other drugs: overview for drug court
practitioners. Washington DC, Oice of Justice Programs, American University, 1999. https://www.ojp.
gov/pdiles1/bja/178940.pdf Accessed 10 December 2021.
20. Achermann Stürmer, Y., Meesmann, U. & Berbatovci, H. (2019) Driving under the influence of alcohol and
drugs. ESRA2 Thematic report Nr. 5. ESRA project (E-Survey of Road users’ Attitudes). Bern, Switzerland:
Swiss Council for Accident Prevention.
21. Peden M et al., eds. World report on road traic injury prevention. Geneva, World Health Organization,
2004.
22. The Cost of Road Traic Accidents in Thailand. Accident Costing Report AC9. Asian Development Bank,
2005 cited in Drinking and Driving: a road safety manual for decision-makers and practitioners. Geneva,
Global Road Safety Partnership, 2007.
23. Esser MB, Wadhwaniya S, Gupta S, Tetali S, Gururaj G, Stevens KAet al.Characteristics associated with
alcohol consumption among emergency department patients presenting with road traic injuries in
Hyderabad, India.Injury. 2016 Jan 1;47(1):160–165.
24. Hingson RW, Zha W. Age of drinking onset, alcohol use disorders, frequent heavy drinking, and
unintentionally injuring oneself and others after drinking. Pediatrics. 2009 Jun;123(6):1477–84.
25. World Health Organization. Alcohol and injury in emergency departments: summary of the report from
the WHO Collaborative Study on Alcohol and Injuries. World Health Organization; 2007.
26. Kasantikul V, Ouellet JV, Smith T, Sirathranont J, Panichabhongse V. The role of alcohol in Thailand
motorcycle crashes. Accid Anal Prev. 2005 Mar;37(2):357–66.
12 Drink driving: a road safety manual for decision-makers and practitioners
Module 1 Why must we address drink driving? 13

2

Module 2
Evidence-based interventions
This module provides guidance on a range of interventions that can be included in drink driving
prevention programmes including laws, setting blood alcohol concentration (BAC) limits, enforcement
of these laws, public awareness and advocacy campaigns, and use of technology and rehabilitation
and treatment to help people separate drinking from driving.
Over recent decades, many countries have been successful in reducing the number of drink driving-
related crashes (for an example, see Box 1). While some adaptation may be required to suit dierent
contexts, experiences from countries that have succeeded in reducing drink driving-related deaths
and injuries (generally high-income countries) can be used to guide programmes in low- and middle-
income countries where alcohol plays a significant role in road crashes.
Module 2 Evidence-based interventions 15
Australia embarked on a sustained programme to tackle drink driving-related crashes from the mid-1970s
onwards. Substantial research information on the impairment eects of alcohol was collected, leading to
support for legislation setting out a maximum BAC level for drivers.
Following the adoption of legal BAC limits, large-scale police enforcement of these limits was undertaken
in the 1980s, through widespread and highly visible Random Breath Testing (RBT). This was supported
by a range of other interventions, including publicity, community announcements, community activity
programmes, and variations in licensing and distribution arrangements for alcohol (for a case study summary,
refer to this publication (1). There was also ongoing monitoring of performance involving blood tests on drivers
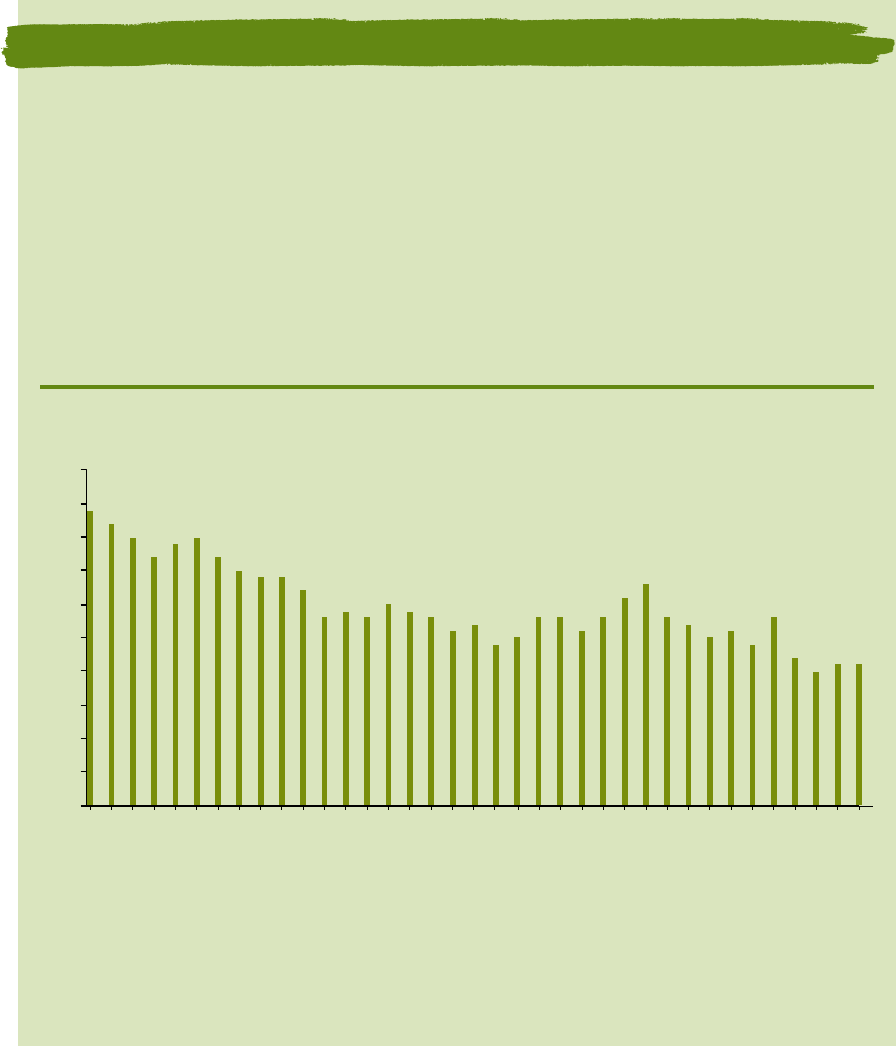
involved in crashes. Over this 30-year period, alcohol as a factor in crashes was almost halved in Australia
(see Figure 4), and community attitudes towards drink driving changed substantially, such that there is a
strong community view that the behaviour is socially irresponsible and unacceptable.
Figure 4. Percentage of drivers and riders killed with BAC of 0.05 or more in Australia:
1980-2017 (where BAC is known *)
44
42
40
37
39
40
37
35
34 34
32
28
29
28
30
29
28
26
27
24
25
28 28
26
28
31
33
28
27
25
26
24
28
22
20
21 21
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1981 1984 1987 1990 1993 1996 1999 2002 2005 2008 2011 2014 2017
Year
*Excludes Victoria and Western Australia; excludes drivers with a special licence (Provisional, Learner, Heavy Vehicle)
that exceeded their special range limit but were below 0.05; some data cleaning applied to two jurisdictions.
Data sources: ATSB (undated). Alcohol and road fatalities. Monograph 5. Canberra: Australian Transport Safety
Bureau; BITRE. Data provided by Bureau of Infrastructure, Transport & Regional Economics. Canberra: Department of
Infrastructure & Transport. Source: (2)
Box 1. Changes in prevalence of and community attitudes towards drink driving – Australia
Success in addressing drink driving requires:
strong political commitment;
legislation that clearly defines illegal (for driving) BAC levels and a tiered suite of supporting penalties
for drink driving oences;
strong, well-publicised, highly visible and sustained enforcement through high visibility random or
compulsory breath testing (RBT/CBT) resulting in swiftly applied penalties when caught breaking
the law;
16 Drink driving: a road safety manual for decision-makers and practitioners
targeted social marketing campaigns to change attitudes and behaviours – the public must:
– know why drink driving is both unsafe and anti-social;
– be aware that there are laws in place;
– perceive a high risk of being caught if they break the law; and
– know that if they are caught, there will be a heavy price to pay that cannot be avoided.
Table 2 provides an overview of existing interventions and a rating of their eectiveness: eective,
promising, insuicient evidence, and ineective. It is strongly recommended that programmes aimed at
reducing drink driving include “eective” or at least “promising” interventions.
Table 2. Evidence status of drink driving interventions
Interventions Eective Promising Insuicient
evidence
Ineective
Legislation (Section 2.1)
Setting BAC limits – e.g. BAC limit for the general
population not exceeding 0.05g/dl; BAC limits for other
driving groups (young/novice drivers, professional/
commercial drivers not exceeding 0.02g/dl).
Penalties that reflect the seriousness of oence (higher
penalties for higher BAC levels), and that are graduated
for recidivists
Enforcement of BAC levels (Section 2.1.2)
Random breath testing (preferred)
Sobriety checkpoints
Restrictions on young/inexperienced drivers: (Section 2.2)
Licensing restrictions – e.g. graduated driver licensing
(GDL), including lower/zero BAC for young drivers
Oender management: (Section 2.3)
Oender programmes
Alcohol ignition interlocks
Alcohol rehabilitation and/or treatment programmes
Public education: (Section 2.4)
Designated driver programmes
Public awareness campaigns (alone)
2.1 Legislation
Drink driving legislation that is evidence-driven, context relevant, consistently enforced, and well
understood by enforcement oicials and the public has been eective in saving lives in many
jurisdictions. The 2018 WHO Global Status Report on Road Safety (3) identified that only 45 countries
had drink driving laws that align with best practice. More information about best practice legislation
Module 2 Evidence-based interventions 17
is contained in various WHO documents, including this one: Strengthening road safety legislation: A
practice and resource manual for countries (4).
Various steps need to be taken when designing eective drink driving legislation. The first step in this
process is undertaking an assessment of relevant legislation already in place. If you identify that laws
need reforming, or that new laws are required, consider the following:
– address the absence of legislation and ensure that best practice recommendations are included;
– strengthen or complement an existing law using evidence and best practice recommendations;
–
provide greater legitimacy for the law and provide appropriate implementation and penalty mechanisms
so that laws can be eectively enforced and serve as a deterrent to drink driving.
It is important to remember that road safety is a dynamic field and that best practice continually
evolves. Therefore, countries must constantly review their legislation, revising and updating it to meet
the latest evidence (5). Consider the following elements when formulating or improving drink driving
laws or regulations.
The WHO requires that three minimum aspects are met to enable a country to be assessed as meeting
best practice drink driving legislative requirements:
1. presence of a national drink driving law
2. BAC limit for the general driving population not exceeding 0.05 g/dl and
3. BAC limit for young and novice drivers not exceeding 0.02 g/dl.
Appendix A contains sample wording to assist in drafting drink driving legislation.
Box 2 describes how the legislative situation in the state of Jalisco, Mexico evolved to help reduce drink
driving.
18 Drink driving: a road safety manual for decision-makers and practitioners
In 2008, as part of the Bloomberg Philanthropies Global Road Safety Programme, a new road safety initiative
was piloted in four locations in Mexico, including the state of Jalisco. One focus of the initiative was to help
the government identify gaps in legislation relating to key risk factors and provide support to facilitate
improvements to these laws. To this end, a review of road safety laws in Jalisco identified the need to
strengthen the law on drink riving, including reducing the existing BAC limit, which was above recommended
best practice.
Strong relationships were established with dierent stakeholders, including federal and state authorities, local
legislators and civil society in order to advocate for legislative change. These eorts included: open forums
with civil society and media; expert meetings and informative sessions; and sessions with local authorities
and legislators from the main political parties.
After extensive consultation among local, national and international stakeholders, legislative recommendations
were drafted. In November 2010 the new state law, locally known as the “Ley Salvavidas” (“Lifeguard/life-
saving law”), was amended to incorporate these provisions, which included lowering the blood alcohol
concentration limit from 0.15 g/dl to 0.05 g/dl (in line with international best practice) and stier penalties
for transgressing this law. Continued monitoring of the law’s implementation resulted in findings that it was
not having the intended impact because of enforcement challenges. Notably the 2010 law specifically did not
provide for the establishment of random alcohol checkpoints, shown to be eective at reducing drink–driving.
Between 2010 and 2012, civil society and international road safety organizations engaged with policy-makers
to advocate for regulations that would allow for random breath testing, a process which culminated in 2013,
when the Jalisco state government adopted an amendment to the 2010 law that formally provided for the
establishment of random alcohol checkpoints and a protocol for their implementation. The occasion of
amending the law was also used to further increase penalties related to drink–driving.
The law amendment was accompanied by a hard-hitting social marketing campaign that supported
dissemination of the new regulations and penalties, and communicated the risk of drink driving (see https://
www.youtube.com/watch?v=boxRNvH5WEo&list=PL9S6xGsoqIBWAhPnNtIDoxP3OcRYqaQa0&index=30).
Alongside this legislative reform process and its dissemination, major capacity building eorts also took
place to train and support police in eectively running random alcohol checkpoints.
The eects of the initiative are being monitored. Short-term results have shown significant changes in the
proportion of alcohol-related deaths and collision rates in Jalisco following the implementation of the Global
Road Safety Programme.
Source: (3, 6)
Box 2. Reforming drink driving legislation in Jalisco, Mexico
2.1.1 BAC Limits (Effective)
Globally, legal BAC levels vary significantly. For instance, for the general driving population, BAC levels
range from 0.00 g/dl (e.g., Hungary, Paraguay) to 0.12 g/dl (e.g., Sao Tome and Principe). Specific details
of drink driving laws, BAC levels, enforcement, and the number of road traic deaths attributed to alcohol,
by country/area, can be found in Table A5 of the 2018 Global Status Report on Road Safety (3). The
table provides legal BAC levels for three driving groups: the General driving population, Young/Novice
drivers, and Professional/Commercial drivers.
In law enforcement investigations, BAC is estimated from breath alcohol concentration (BrAC) measured
with a machine commonly referred to as a breathalyser (note that dierent machines may have dierent
conversion factors applied to relate BrAC to BAC). Breath alcohol concentration (BrAC) is expressed
as the weight of alcohol, measured in grams, in 210 litres of breath, or, measured in milligrams, in
210 millilitres of breath. There is accurate correspondence between blood alcohol and breath alcohol
Module 2 Evidence-based interventions 19
levels (7). Because of the ease of administration, breath alcohol is more commonly measured in the
road safety context. As described in section 1.3, the presence of any amount of alcohol can impair
driving behaviour and there is a rapid, exponential increase in risk for BAC levels that exceed 0.05g/
dl. Therefore, international evidence and experience demonstrates a critical need to legislate lower
maximum BAC rates in order to reach, at least, the WHO recommended minimum requirements to limit
the harm caused by alcohol consumption and driving.
Screening for Alcohol – Breath testing at the roadside (Effective)
In general, there are two roadside breath testing approaches:
1.
Random breath testing (RBT) (recommended) – the statutory authority for an enforcement oicer to
stop a vehicle and test the driver at random, anywhere at any time, without the need to establish that
the driver committed another oence, nor that the driver showed any signs of impairment prior to
being stopped. This is primary enforcement of a drink driving law, is common in some European
countries, and throughout Australia and New Zealand, and is an eicient use of resources because
it allows for a greater number of drivers to be tested (high volume testing), per hour of enforcement
activity (as compared to a sobriety checkpoint), and if challenged, can be justified on civil and human
rights grounds, through a greater good, public interest argument. Note that RBT can be conducted
at a roadside checkpoint where every vehicle is stopped and every driver tested. However, if vehicle
volume through a checkpoint becomes such that it is no longer practical or safe for sta or road users
to stop every vehicle, the testing can be continued by stopping a random number of vehicles that
allows for overall volume of traic to be managed. This process ensures randomness and equity in
relation to who is stopped and tested. RBT can also be conducted away from a checkpoint operation,
where enforcement oicers can intercept a vehicle and test the driver.
2. Sobriety checkpoints – enforcement oicer is required to form a suspicion of alcohol impairment
before a driver can be intercepted and tested. This is also referred to as Selective breath testing
(SBT). This testing strategy, used in the United States of America, is generally less eicient because
of lower testing volumes for each hour of enforcement activity.
Overall, while both types of roadside breath testing approaches have shown positive road safety
impacts (8), RBT has produced superior results and is recognised as the more eicient way to allocate
enforcement resources and to deter drink driving, especially because it can expose every driver stopped
at the RBT site to a breath test (9, 10). Another approach to detect and apprehend drink drivers is to
conduct targeted enforcement based on intelligence. This can involve targeting vehicles as they depart
from known drinking venues (e.g., bars, nightclubs, restaurants). This approach may lead to detection
of some drink driving oenders but is less eective at creating a general deterrent eect (for the whole
driving population) because it is generally not highly visible, nor publicised (11).
2.1.3 Additional legislative considerations
Refusal to submit to a breath test: Legislation must address the consequences of a driver refusing
to submit to a breath test. In some jurisdictions, the penalty for failing to submit a breath sample
is equivalent to the penalty associated with the highest range drink driving oence. It is highly
recommended that the penalty for refusing to submit to a breath test are substantial and unavoidable.
An additional consideration is what mechanism/s can be used to dispute a test result.
20 Drink driving: a road safety manual for decision-makers and practitioners
Requirement for mandatory alcohol testing for road crashes. This is an important strategy to help
determine crash causation as well as provide valuable information on level of intoxication of drivers,
passengers, and any other road users involved in a crash (e.g., pedestrians, cyclists) so that appropriate
intervention strategies can be developed.
Penalties: A range of penalties are used to deter drink driving, including monetary fines, demerit points,
licence suspension, licence loss, vehicle impoundment, and the requirement to fit and use an interlock
device for a specified time. It is critical that penalty severity reflects the severity of the oence. In other
words, it is important that riskier behaviours (i.e., driving with higher BAC levels, or repeat oending)
incur harsher penalties, to communicate the seriousness of the oence or reoending to the broader
community. It is also important to ensure that penalties for drink driving oences are appropriate
when compared to other traic oences. More severe penalties are often used for recidivist (repeat)
oenders. Additional information on the use of penalties to improve road safety can be found in the
guide produced by the Global Road Safety Partnership (GRSP) (A Guide to the Use of Penalties to
Improve Road Safety) (12).
Per se or impairment provisions: Consideration should be given to whether the legal framework of a
country is based on a per se law or an impairment law. ‘Per se’ is a Latin phrase meaning ‘by itself’. In
relation to drink driving, a per se law means that a person is breaking the law by having a BAC above
the legal limit, irrespective of whether there is any sign of impairment or any other evidence.
This issue is of particular importance for enforcement actions as well as to create a legislative system
that actively deters drink driving. Because of the wealth of evidence that shows increasing levels of
impairment with increasing BAC, it is common in many jurisdictions for graduated penalties to apply,
with penalties increasing in severity as driver BAC levels increase.
Identification of relevant enforcement agency: Specifically identifying the enforcement authority/
ies that will be responsible for enforcing the law, as well as their specific responsibilities, is necessary.
Restrict availability and aordability of alcohol: Approaches such as increasing taxes on alcohol,
regulation on point of sale, density of locations of sale, and minimum age for purchase and consumption
of alcohol can assist to reduce the level of harm created by alcohol consumption and drink driving (13).
Additionally, consideration should be given to making it an oence to sell or supply alcohol to an
intoxicated person. More details about these issues as well as topics such as national control of
production and sale of alcoholic beverages, restrictions on drinking in public, restrictions on alcohol
advertising, regulations on alcohol product placement and alcohol sales promotions, labelling, and
responsible beverage service training can be found in the Global status report on alcohol and health (14).
Testing and calibrating breath alcohol testing equipment considerations: It is recommended that
legislation covers: a) the approval of breath alcohol testing instruments for enforcement purposes,
resourcing mechanism necessary to procure relevant testing equipment and train relevant people how
to use and calibrate it, and b) testing and calibration protocols – to preserve evidence and mitigate risk
of litigation – this may include technical specifications for testing and calibrating devices and testing
facility protocols to ensure that all tests are administered properly and in a timely manner by fully
competent, trained personnel.
Employer provisions: It is recommended that legislation contains information that allows employers
to be held accountable for the safe operation of the work vehicle fleet, which could include monitoring
driver compliance with drink driving laws through workplace breath-testing and protocols. This might
include the necessity for vehicles to be fitted with interlock devices or random testing programmes.
Module 2 Evidence-based interventions 21
2.2 Licence Restrictions (Effective)
Novice drivers generally lack experience in regard to safe driving/riding skills when they enter the
licensing system. To help manage their exposure to risk, a range of programmes have been developed
and refined that consist of various restrictions which can ease over time, as more experience is gained.
These schemes are commonly known as Graduated Driver Licensing (GDL) or Graduated Licensing
Schemes (GLS) (15).
Specific components of GDL systems vary across jurisdictions. Common components include measures
such as: a reduced (or zero) BAC level (8), a minimum learner age and learner period, a minimum
supervised practice hours requirement, a minimum provisional period, peer passenger restrictions,
night driving restrictions, phone/other technology restrictions, and vehicle power restriction (16, 17).
The impact of various components on GDL systems have been examined. Significant reductions have
been found for the zero BAC component. For example, a 9–23% reduction in alcohol-related fatal
crashes among 15–19 year olds; a 4–17% reduction in fatal and injury crashes among 15–19 year olds,
and a 22% reduction in night-time single vehicle fatalities have been associated with zero BAC limits
that form part of GDL systems (for a comprehensive summary refer to (18).
2.3 Offender Management
Greater understanding of the factors that contribute to drink driving, together with access to in-vehicle
technology, has changed the way oenders (especially recidivists) are managed. Historically, penalties
for drink driving oences have commonly included jail sentences, monetary fines, demerit point
sanctions, and licence bans (suspension or revocation). However, a licence sanction (e.g. suspension)
does not necessarily mean that an oender will cease driving. Additionally, traditional types of penalties
did little to support oenders with alcohol dependence issues. As a result, countermeasures such as
interlocks, oender programmes, and rehabilitation/treatment programmes have been implemented
in various high-income countries in recent decades.
2.3.1 Offender programmes (Promising)
Programmes to educate and deter reoending dier considerably and can range from an education-
only programme to more tailored treatments that include components such as behaviour change
training, the use of case management to monitor progress, and referral to specialist help to deal with
alcohol dependency (see section 2.3.3 for more detail about alcohol rehabilitation programmes). Some
jurisdictions have programmes only for first oenders, others mandate programme completion for
all drink driving oenders; while some are only for oenders with mid- or high-range BAC threshold
oences or for recidivists. A summary of the wide range of oender programmes used across Australian
jurisdictions, for example, can be found in Table 8.1 of an Austroads publication from 2020 (19). Despite
the intuitive appeal of many of these programmes, robust evidence about which type of programme
oers greatest impact requires further research.
22 Drink driving: a road safety manual for decision-makers and practitioners
2.3.2 Alcohol ignition interlocks (Effective)
An alcohol ignition interlock (also commonly known as an alcoholinterlock device oran alcolock) is an
electronic breath-testing device which prevents a vehicle from starting if alcohol (above a designated
threshold) is detected in the breath of the driver and then requires breath samples to be provided
randomly while the vehicle is being driven. An interlock device generally consists of two parts which:
1) measure breath alcohol concentration, and 2) immobilise the vehicle engine if a pre-programmed
BAC limit is exceeded. Interlocks have generally been used as a punitive, rather than a preventative
measure, and have aimed to reduce drink driving among two key groups: 1) repeat oenders, and
2) high-range BAC first time oenders. However, in Victoria, Australia, interlocks were introduced in
2018 as a mandatory penalty for anyone apprehended with a BAC level of 0.05 or higher, irrespective
of whether they were a first-time or repeat oender. An evaluation of the eectiveness of this sanction
in reducing oending and alcohol-related crashes was not available at the time of writing. In some
jurisdictions, interlocks are also used as a preventative measure in some occupational settings (e.g.,
heavy vehicle and bus fleets).
The interlock device can store data (e.g., number of attempts to start the vehicle and associated BAC
levels during such attempts, as well as attempts to tamper with the device) which can be used by
authorities to monitor compliance levels and rehabilitation outcomes. This kind of information is
particularly useful in jurisdictions where a violation-free period is needed in order for an oender to be
relicensed. Various additional features to help ensure integrity of a device while it is installed in a vehicle
are in use or in development and include: face recognition, biometric (fingerprint) recognition, real-time
reporting of violations, GPS tracking, and the use of PIN so that multiple users can use a single device.
Advances in technology continue to enhance capacity and functionality of interlock devices. For instance,
less obtrusive measurement mechanisms include passive options such as skin sensors, transdermal
perspiration measurements and alcohol ‘snier’ systems (sensors in a vehicle that measure alcohol in
the breath at a distance, rather than from a direct breath sample, also known as PAS – passive alcohol
sensor technology) that are integrated into the cabin of a vehicle and do not require a driver to provide
a direct sample of breath. More information about the various interlock capabilities and programmes
throughout Europe and Australasia can be found in a range of publications (20, 21). Additional information
about aspects of interlock programmes, including cost, installation, programme duration, and removal
requirements, can be found in Tables 2.1 and 2.2 of a 2015 Austroads publication (22).
Interlock evaluation research across many jurisdictions consistently demonstrates that the devices
are highly eective in reducing drink driving episodes (and re-arrest rates for alcohol-impaired
driving) while installed in the vehicle, but that this positive eect diminishes when the device is
removed (23, 24). Information is available on the use and eectiveness of interlocks in Europe (22), the
United States of America (25), and Australia (19). It is important to note that interlock programmes can
create financial hardship for some oenders because in some jurisdictions, oenders are responsible
for paying costs associated with installation and monitoring of interlock devices. A range of financial,
judicial and logistical issues should be explored and resolved by relevant authorities before launching
a new interlock programme.
2.3.3 Alcohol Rehabilitation Programmes (Effective)
As noted above, interlocks are eective at reducing drink driving while installed in a vehicle. The
return to oending, once the device is removed, indicates that for some people, problematic alcohol
Module 2 Evidence-based interventions 23
use is likely to play a large role in reoending and may not be addressed at all by the installation of
an interlock (26). As such, therapeutic (treatment) and educational rehabilitation programmes have
been implemented in some jurisdictions to address problematic alcohol use. These programmes vary
widely in content, length, cost, and quality, making evaluation diicult. Providers of these programmes
need to be accountable for delivery of their services and assessed by qualified agencies to ensure that
programmes are delivered to a high standard and are evidence-based.
They also vary in intent. For instance, some treatment or rehabilitation programmes focus specifically
on managing alcohol dependency and abuse, while others focus on separating drinking from driving. In
some jurisdictions, courts can impose alcohol treatment programmes as part of the sentencing process.
Medical consultations or alcohol assessments are undertaken in some jurisdictions, including Great
Britain, Sweden, Canada and New Zealand, to determine whether treatment for alcohol rehabilitation
is needed.
A summary of dierent types of rehabilitation programmes can be found in Tables 2.1 and 2.2 of a 2015
Austroads report (22) and examples from Europe can be found in the 2016 Best Practice guide (27).
Overall, eectiveness is diicult to assess because of the wide range of programmes and their aims.
However, the evidence indicates that a combination of education and treatment programmes can
reduce drink driving recidivism.
2.4 Public Education
2.4.1 Designated Driver programmes (Insufcient evidence)
These programmes generally aim to separate drinking and driving and change attitudes and societal
norms associated with drinking alcohol and driving by providing the opportunity for a sober person to
transport others who have consumed alcohol to a level that would mean they are not able to legally
drive. The programmes take many forms. For instance, some licensed premises oer courtesy vehicles to
return their patrons home; others invoke the desire for friends to look after each other when out drinking
in a group by deciding, in advance, that one person will remain sober and carry the responsibility of
transporting all others in the group safely home. Various incentives have been associated with these
kinds of programmes, including free entry to licensed venues or free non-alcoholic drinks for the
designated driver.
Generally, these programmes aim to reduce alcohol-related crashes by:
1. providing an alternative to driving under the influence of alcohol
2. promoting a non-drink driving norm, and
3. encouraging responsible travel planning (28)
Various names are associated with designated driver programmes that have been conducted in various
countries such as the Netherlands, Canada, Italy, the United States of America, France, Greece, Belgium,
and Australia, and include ‘Euro Bob’, ‘DES’, ‘Sober Bob’, and ‘The Skipper’. Evaluations have shown positive
changes, in some cases, in the proportion of people willing to use or actually using a designated driver,
though not necessarily an increase in people willing to be a designated driver. Overall, evaluation data
24 Drink driving: a road safety manual for decision-makers and practitioners
is limited and inconclusive, with findings generally indicating no impact on drink driving rates or on
involvement in alcohol-related crashes (29, 30, 31, 32).
2.4.2 Public awareness campaigns (alone) (Ineffective)
A substantial body of evidence indicates that public education and awareness campaigns are important
tools to:
inform the community about the risks of unsafe road use
inform the community about road safety laws and the consequences (penalties) of not complying
with them,
promote the general deterrent eect of enforcement activities by informing the community that laws
are actively being enforced, and in doing so, raising the ‘perceived risk of being detected’ among the
community.
However, education, alone, is not eective in changing drink driving behaviour and must work in tandem
with eective enforcement of robust legislation to reduce the incidence of drink driving. As highlighted
in the Save LIVES Road Safety Technical Package published by WHO (5)
“Strong and sustained enforcement of road safety laws, accompanied by public education, has
positive eects on road user behaviour and thus has the potential to save millions of lives”.
Public awareness or social marketing/advocacy campaigns may require the services of a public relations,
advertising agency, or production company and a research agency, unless a government agency has
the expertise to provide these services. Overall control of the campaign should, however, stay with the
responsible government agency. It is important to specify the campaign objective/s from the outset so
that the campaign can be properly planned, conducted and monitored, and an appropriate evaluation
can be planned and implemented. Drink driving campaign objectives may include:
informing the public of new drink driving legislation, regulations, or penalties;
notifying the public about increased drink driving enforcement;
advising the public not to take the risk of drink driving, while highlighting a variety of dierent
consequences of doing so;
educating road users about the crash risk associated with consuming any alcohol;
quantifying the personal risks and legal consequences of driving while over the legal BAC limit;
warning people about social consequences of their drink driving to other (“innocent”) parties;
emphasising the risk of detection;
emphasising the social unacceptability of drink driving;
sharing personal stories related to adverse impacts of drink driving, while advocating for behavioural
change; and
warning drivers about the wide-ranging consequences of being detected and prosecuted for drink
driving.
Module 2 Evidence-based interventions 25
Figure 5 depicts a simplified version of the process that should be undertaken in developing a social
marketing/behaviour change campaign to reduce drinking and driving. No campaign will be eective
unless it identifies and develops appropriate, well-targeted messages. There is no easy formula for
determining the correct message, however there are some key steps that may assist in achieving this.
Working with skilled and experienced professionals is critical for campaign success. Market research
is used to determine peoples’ knowledge of legislation as well as the opinions, beliefs, fears, and
motivations of high-risk groups that are known to be involved in drink driving crashes.
A first step in this process is to identify the target groups involved and collect information from them that
is relevant for the campaign (diagnostic tone and message testing). On the basis of the information you
receive from testing with the target group, a range of messages and campaign materials are developed
to encourage a change in thinking and behaviour in relation to drinking and driving (e.g. don’t drink and
drive – your family is waiting for you at home). The draft campaign messages and materials should then
be tested with small groups who represent the target group before the final campaign message/s is
determined and the campaign is launched. It is important to consider and strategically chose relevant
channels (e.g., television, radio, social media) and times (e.g., immediately before public holidays) through
which the target audience can best be reached.
26 Drink driving: a road safety manual for decision-makers and practitioners

Figure 5. Steps involved in a drinking and driving publicity campaign
Initiate agency meetings to ensure support
and understanding of publicity role
Conduct target group diagnostic research
to identify profile and motivations
Conduct communications testing research
to obtain likely eective messages
Publicity campaign agreed as component
of anti-drink driving programme
No
No
No
No
No
Yes
Yes
Yes
Yes
Yes
Target group profile and behavioural
motivations are known
Eective communication messages are
known
Advertising agency contracted for
materials production
Good-quality, high-impact campaign
materials are available
Yes
Yes No
Commission
materials market
testing research
Eectiveness
of materials is
known
Initiate agency meetings to ensure
support and understanding of publicity
role
Most eective media mix for
communication is known
Commission media monitoring to
ensure media plan is delivered.
Commission communications
eectiveness research as
campaign is conducted
Commission advertising agency
to prepare media purchase plan in
accord with campaign budget
Run
Campaign
Module 2 Evidence-based interventions 27
Source: (33) with author elaboration.
Additional information about road safety public awareness programmes and social marketing campaigns
can be found in the 2016 manual produced by WHO– Road Safety Mass Media Campaigns: A Toolkit
and on the WHO website. https://www.who.int/publications/i/item/road-safety-mass-media-campaigns-
a-toolkit (34)
2.5 Other effective legal measures
Licensing laws
The licensing laws of a country regulate the general availability and promotion of alcohol. A series of
measures can be employed to control criteria for granting licences for the sale of alcohol; places and
hours during which business may be conducted; the number of licensed premises within a local area,
the setting of a minimum drinking age, and restrictions relating to marketing of alcohol in the media
(e.g., restrictions on advertising alcohol products in prime time or in media accessible to children/
adolescents). Additional information on alcohol marketing regulation can be found in numerous
publications, including a special issue of the academic journal, Addiction, published in 2017 (35).
These laws, typically carried out by a “licensing board” (or similar entity), should require that stringent
requirements are met before a licence to sell alcohol is granted. Licensing laws aim to:
prevent crime and disorder;
maintain public safety;
prevent public nuisance;
protect children/vulnerable people.
Minimum legal drinking age
Legislation specifying BAC limits is central to addressing drink driving but other laws regulating access
to and consumption of alcohol also indirectly influence drinking and driving. In some countries, minimum
legal drinking age (MLDA) laws specify an age below which people cannot purchase or publicly
consume alcohol and there is strong evidence to suggest that MLDA laws are eective in preventing
crashes involving drinking and driving (36), while reducing the risk of developing harmful consumption
of alcohol at a later stage (37).
The Global Status Report on Alcohol and Health 2018, states that increasing the national legal minimum
age for purchase of alcohol can reduce alcohol consumption and related harms among young people
and particularly drink driving crashes (14). Age restrictions can apply to the consumption of alcohol
on-premises or o-premises. One hundred and fifty-two countries (93%) reported a national or
subnational minimum legal purchase age for on-premise beer and wine sales and 151 countries (92%)
reported a minimum legal age for purchase of spirits. By far, the most common age limit is 18 years: 108
countries have an on-premise and o-premise 18-years legal purchase age for beer and wine, while three
further countries have an 18-years legal purchase age for either on-premise or o-premise spirits (14).
28 Drink driving: a road safety manual for decision-makers and practitioners
Restrictions on drinking in public
Some countries also have restrictions on alcohol consumption in public places. Such restrictions are
most commonly applied to educational buildings (146 countries), followed by health-care establishments
(139 countries). Restrictions were least common at leisure events (73 countries) and in parks (71
countries) (14).
Alcohol sales points
Restricting physical access to alcohol is eective, feasible and cost-eective in low- and middle-income
countries. Some regions have implemented laws limiting the hours during which alcohol can be sold,
or the density of outlets selling beverage alcohol. Recent evidence confirms associations between
alcohol outlet density, hours during which alcohol can be sold, and alcohol-related harms. (38, 39, 40).
In addition, research has shown that the chances of binge drinking/heavy episodic drinking (i.e., the
excessive consumption of alcohol within a short period of time) increases by 5% for every additional
o-licence liquor outlet that exists within easy walking distance of home [1km] (38).
The WHO’s global strategy recommends (3):
implementing licensing systems to monitor the production, wholesaling and serving of alcoholic
beverages;
regulating the number and location of retail alcohol outlets;
regulating the hours and days during which alcohol may be sold;
establishing a national legal minimum age for purchase and consumption of alcohol; and
restricting drinking in public places; and
regulating or banning alcohol advertising and publicity.
Measures may be most eective when they impact upon large geographic areas to minimise
opportunities for circumvention.
Responsible beverage service and sales legislation generally aims to reduce sales of alcohol to
minors and to intoxicated people. This can also include making retailers liable for injuries caused by
intoxicated adults or by minors (e.g., those under 18 years of age) to whom they sold alcohol. In some
cases, this liability extends to injuries caused by the intoxicated person to themselves. Responsible
beverage service and sales legislation can apply to premises which sell alcohol to be consumed on-site
or o-site and should include policies that promote:
outlet sta awareness of legal responsibility;
sta awareness of outlet policies and of consequences for violating these;
the checking of age of all patrons under a certain age (e.g., to meet minimum age requirements);
guidelines and training as to what constitutes acceptable serving practice;
retailer-initiated compliance checks and enforcement (41).
Module 2 Evidence-based interventions 29
2.6 Engineering countermeasures
Road engineering treatments may also help reduce drink driving crashes and the severity of their
outcomes. A high proportion of drink driving crashes are “run-o road” crashes and may be more
severe if they result in a collision with fixed roadside objects such as trees or electricity poles. As such,
action to relocate, guard, or remove fixed roadside objects where drink driving crashes are likely to
occur may reduce crash severity. Visual, perceptual, and cognitive skills are adversely aected by
alcohol. Therefore, providing information in a clear, easy to understand manner will be important in
minimising the crash risk of people who are impaired by alcohol. Some elements that may assist include
improved guidance around curves and audio-tactile edge lining. Drink driving crashes may also involve
pedestrians who are particularly vulnerable in a crash. Engineering solutions including lower speed
limits, traic calming measures, pedestrian fencing, refuge islands and medians where pedestrians
are likely to cross the roadway, and good street lighting for better pedestrian visibility, may all help to
minimise crash outcomes for pedestrians.
2.7 Post-crash response
Appropriate post-crash response can also help to minimise death and long-term debilitating injury from
drink driving crashes. Medical treatment of people involved in crashes is made more diicult if they are
alcohol impaired. Below are some key points to consider in the post-crash phase:
Scene management
Alcohol-impaired patients tend to be more aggressive, non-compliant and diicult to communicate
with and manage.
Where they are mobile, they may get in the way of rescue personnel trying to assist other injured
patients in the vehicles.
In extreme circumstances, it may be necessary for medical sta to withdraw from the immediate
scene and allow police to regain control of the situation.
Patient assessment/treatment diagnosis
Alcohol can reduce the response to pain which is critical for determining spinal injuries and suspected
head injuries.
As alcohol intoxication produces a neurological impairment, it is often impossible to clinically exclude
a significant head or spinal injury, resulting in otherwise unnecessary investigations or prolonged
hospital assessments.
Alcohol can aect accurate history and assessment (e.g., reporting of high blood pressure, allergies,
medication, drug taking and diabetes may also aect the physiological signs).
Alcohol may inhibit the patient response to medications.
30 Drink driving: a road safety manual for decision-makers and practitioners
Injury aggravation
There is the increased possibility of further self-injury where alcohol-impaired patients do not have full
control of their actions. Serious injuries may be made worse. This includes risk of spinal injury in the
context of unstable vertebral fractures, where intoxicated patients may not comply with instructions
to remain still.
There is a tendency not to remain still or calm during normal treatment.
There is potential for the patient to vomit.
It is important to appreciate the problems which can be confronted by health professionals and rescue
workers. Policies and procedures must clearly describe the processes and authorisations necessary to
ensure the delivery of eective, timely medical treatment and safe transportation. Training for dealing
with alcohol-impaired patients can be included in regular training for dealing with aggressive or violent
individuals. For countries where compulsory blood tests are not taken in hospital, both law enforcement
oicers and medical sta must be aware that some drink drivers will exaggerate or fake injury from a
collision to seek the refuge of a hospital or medical services to avoid arrest or prosecution.
Several WHO publications provide technical details of on how to improve trauma care: Guidelines for
essential trauma care (42) and Pre-hospital trauma care systems (43).
Module Summary
Successful reduction of drink driving requires strong political commitment, clear legislation, and
strong, well-publicised, highly visible and sustained enforcement through highly visible breath testing
operations (random breath testing is most eective) that results in swiftly applied and appropriate
penalties.
Interventions proven to be eective at reducing drink driving include; setting BAC limits according to
best practice guidelines; using penalties that reflect the seriousness of the oence (higher penalties
for higher BAC levels); random breath testing and sobriety checkpoints to enforce BAC levels; using
licence restrictions for young/inexperienced drivers; use of alcohol ignition interlocks; and use of
alcohol rehabilitation/treatment programmes.
Interventions that are considered promising include: oender programmes.
Interventions that have insuicient evidence to support their use include designated driver programmes.
Interventions that are ineective at reducing drink driving include public education and social
marketing campaigns – when used alone. However, such campaigns are critically important to support
enforcement of BAC limits and must work in tandem with enforcement operations so that the public
are aware that the risk of them being detected while drink driving is high.
Other legal measures that should be used to combat drink driving include: licensing laws, a minimum
legal drinking age, restrictions on drinking in public, limiting alcohol sales points, legislation covering
responsible beverage service and sales.
A range of engineering treatments and considerations for post-crash care are also important
considerations in reducing the harm caused by drink driving.
Module 2 Evidence-based interventions 31
References Module 2
1. Fleiter, J,Lewis, I,Kaye, S,Soole, D,Rakotonirainy, A,&Debnath, A., Public demand for safer speeds:
Identification of interventions for trial: Publication no: AP-R507–16. Austroads Ltd, Australia. 2016.
2. Watson, B. & Watson, A. The long-term trend in alcohol-related crashes and associated policy responses
in Queensland, Australia. Paper presented at: The 22nd International Conference on Alcohol, Drugs &
Traic Safety; 2019 August, 18–21; Edmonton, Canada.
3. Global status report on road safety. Geneva, World Health Organization, 2018. Licence: CC BYNC-SA 3.0
IGO.
4.
Strengthening road safety legislation: a practice and resource manual for countries. Geneva: World Health
Organization, 2013.
5. Save LIVES– A road safety technical package. Geneva: World Health Organization; 2017. Licence: CC
BY-NC-SA 3.0 IGO.
6. Gómez-García L, Pérez-Núñez R, Hidalgo-Solórzano E. Short-term impact of changes in drinking-and-
driving legislation in Guadalajara and Zapopan, Jalisco, Mexico. Cad Saude Publica. 2014;30(6):1281–92.
7. Gibb KA, Yee AS, Johnston CC, Martin SD, Nowak RM. Accuracy and usefulness of a breath alcohol
analyzer. Ann Emerg Med. 1984 Jul;13(7):516–20.
8. Macaluso, G., Theofilatos, A., Botteghi, G., Ziakopoulos, A. (2017), Law and enforcement: Random and
selective breath tests, European Road Safety Decision Support System, developed by the H2020 project
SafetyCube.
9.
Solomon R, Chamberlain E, Abdoullaeva M, Tinholt B. The case for comprehensive random breath testing
programs in Canada: reviewing the evidence and challenges. Alta. L. Rev.. 2011;49:37.
10. Voas RB, Fell JC. Strengthening impaired-driving enforcement in the United States. Traic injury
prevention. 2013 Oct 3;14(7):661–70.
11.
Shults RA, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande-Kulis VG, Zaza S, Sosin DM, Thompson RS,
Task Force on Community Preventive Services. Reviews of evidence regarding interventions to reduce
alcohol-impaired driving. American journal of preventive medicine. 2001 Nov 1;21(4):66–88.
12.
Sakashita, C. Fleiter, J.J, Cli, D., Flieger, M., Harman, B. & Lilley, M (2021). A Guide to the Use of Penalties to
Improve Road Safety. Global Road Safety Partnership, Geneva, Switzerland. https://www.grsproadsafety.
org/wp-content/uploads/Guide_to_the_Use_of_Penalties_to_Improve_Road_Safety.pdf. Accessed 21
January 2022.
13. Anderson P, Chisholm D, Fuhr DC. Eectiveness and cost-eectiveness of policies and programmes to
reduce the harm caused by alcohol. The lancet. 2009 Jun 27;373(9682):2234–46.
14. Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018. Licence: CC
BY-NC-SA 3.0 IGO.
15. Hay, M., Etienne, V., Paire-Ficout, L. (2017), Driver training and Licensing: formal pre-license training,
graduated driver licensing and probation, European Road Safety Decision Support System, developed
by the H2020 project SafetyCube.
16. Williams AF, McCartt AT, Sims LB. History and current status of state graduated driver licensing (GDL)
laws in the United States. Journal of safety research. 2016 Feb 1;56:9–15.
32 Drink driving: a road safety manual for decision-makers and practitioners
17.
Masten SV, Foss RD, Marshall SW. Graduated driver licensing program component calibrations and their
association with fatal crash involvement. Accident Analysis & Prevention. 2013 Aug 1;57:105–13.
18.
Senserrick TM, Williams AF. Summary of literature of the eective components of graduated driver licensing
systems. No. AP-R476/15, 2015 Feb.
19. Howard E, HARRIS A, McIntyre A. Eectiveness of drink driving countermeasures: national policy
framework. Austroads Publication AP-R613–20, 2020.
20. Fitzharris M, Liu S, Peiris S, Devlin A, Young K, Lenne M, Bowman D, Gatof J. Options to extend coverage
of alcohol interlock programs. No. AP-R495–15.2015 Sep.
21. Alcohol interlocks in Europe: An Overview of Current and Forthcoming Programmes, 2020 European
Transport Safety Council, Brussels, Belgium, 2020.
22.
Filtness AJ, Sheehan M, Fleiter J, Armstrong K, Freeman J. Options for rehabilitation in interlock programs.
Austroads Publication AP-R484/15, 2015 Mar.
23. Elder RW, Voas R, Beirness D, Shults RA, Sleet DA, Nichols JL, Compton R, Task Force on Community
Preventive Services. Eectiveness of ignition interlocks for preventing alcohol-impaired driving and
alcohol-related crashes: a Community Guide systematic review. American journal of preventive medicine.
2011 Mar 1;40(3):362–76.
24.
Willis C, Lybrand S, Bellamy N. Alcohol ignition interlock programmes for reducing drink driving recidivism.
Cochrane Database of Systematic Reviews. 2004(3).
25. Richard CM, Magee K, Bacon-Abdelmoteleb P, Brown JL. Countermeasures That Work: A Highway
Safety Countermeasure Guide for State Highway Safety Oices, 2017. No. DOT HS 812 478United States.
Department of Transportation. National Highway Traic Safety Administration; 2018 Apr 1.
26. Wells‐Parker El, Bangert-Drowns Ro, McMillen R, Williams M. Final results from a meta‐analysis of
remedial interventions with drink/drive oenders. Addiction. 1995 Jul;90(7):907–26.
27. Houwing S. Alcohol interlocks and drink driving rehabilitation in the European Union: best practice and
guidelines for member states. 2016.
28.
Nielson AL, Watson B. Driver Programs. Journal of the Australasian College of Road Safety. Journal of the
Australasian College of Road Safety. 2009;20(2):32–7.
29. Winsten JA. Promoting designated drivers: The Harvard alcohol project. American journal of preventive
medicine. 1994 May 1;10(3):11–4.
30.
Watson A, Watson B. An outcome evaluation of the ‘Skipper’ designated driver program. Accident Analysis
& Prevention. 2014 May 1;66:27–35.
31. Simons-Morton BG, Cummings SS. Evaluation of a local designated driver and responsible server
program to prevent drinking and driving. Journal of Drug Education. 1997 Dec;27(4):321–33.
32. Ditter SM, Elder RW, Shults RA, Sleet DA, Compton R, Nichols JL. Eectiveness of designated driver
programs for reducing alcohol-impaired driving: a systematic review. American journal of preventive
medicine. 2005 Jun 1;28(5):280–7.
33. World Health Organization. Drinking and driving: a road safety manual for decision-makers and
practitioners. Drinking and driving: a road safety manual for decision-makers and practitioners. 2007.
34. Road safety mass media campaigns: a toolkit. Geneva: World Health Organization; 2016. Licence: CC
BY-NC-SA 3.0 IGO.
Module 2 Evidence-based interventions 33
35. Babor TF, Jernigan D, Brookes C. The regulation of alcohol marketing: From research to public health
policy. Addiction. 2017 Jan;112(s1):1–27.
36.
Shults RA et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. American
Journal of Preventive Medicine, 2001, 21:66–88.
37.
Babor TF, Caetano R, Casswell S, et al.Alcohol: No Ordinary Commodity: Research and Public Policy. 2nd
edition ed. Oxford University Press; 2010. https://oxford.universitypressscholarship.com/view/10.1093/
acprof:oso/9780199551149.001.0001/acprof-9780199551149. Accessed January 21, 2022.
38.
Connor JL, Kypri K, Bell ML, Cousins K. Alcohol outlet density, levels of drinking and alcohol-related harm
in New Zealand: a national study. J Epidemiol Community Health. 2011 Oct 1;65(10):841–6.
39. Kypri K, Bell ML, Hay GC, Baxter J. Alcohol outlet density and university student drinking: a national
study. Addiction. 2008 Jul;103(7):1131–8.
40. Grube JW, Stewart K. Preventing impaired driving using alcohol policy. Traic injury prevention. 2004
Sep 1;5(3):199–207.
41.
Toomey TL, Kilian GR, Gehan JP, Perry CL, Jones-Webb R, Wagenaar AC. Qualitative assessment of training
programs for alcohol servers and establishment managers. Public Health Reports. 1998 Mar;113(2):162.
42. Mock C, editor. Guidelines for essential trauma care. World Health Organization; 2004.
43.
Sasser S, Varghese M, Kellermann A, Lormand JD. Prehospital trauma care systems. 2005. Geneva: World
Health Organization.
34 Drink driving: a road safety manual for decision-makers and practitioners
Module 2 Evidence-based interventions 35

3

Module 3
Enforcing drink driving laws
For a drink driving law to be eective, the community must understand and believe that if they drink and
drive, there is a strong likelihood of detection, prosecution and receipt of penalty. The principal objective
of police intervention is to save lives and reduce drink driving-related road trauma. Apprehending
oenders is a by-product of the intervention, not the main objective. Figure 6 provides an outline of the
steps required for strategic enforcement of drink driving laws.
Module 3 Enforcing drink driving laws 37
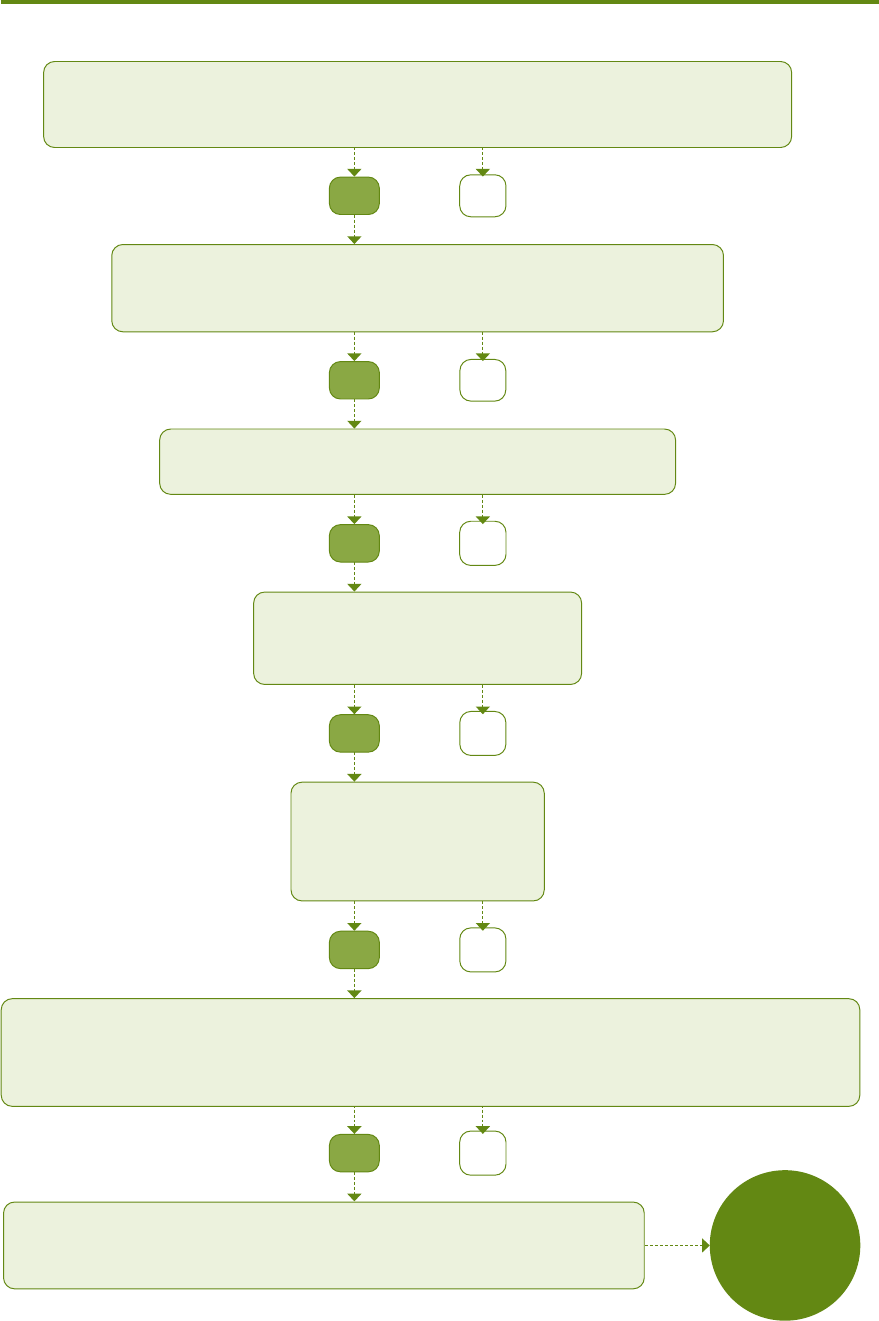
Figure 6. Flow chart showing the strategic enforcement of drinking and driving regulations
Continue
sustained
operations
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
Establish the context
Accurate data on crashes involving drinking (numbers, times etc)? Political will and community
support to reduce road trauma? Senior Police oicer to champion the cause?
Workable legislation
Compulsory breath test at crash scenes? Compulsory blood samples in
hospitals? Random breath testing?
Strategic Plan
Is the road safety plan in operation?
Training
Are police well trained?
Are police competent with legislation?
Equipment
Simple and manageable?
Maintenance programme?
Services within the country?
Operational strategy
Highly visible, rigorous and sustained enforcement that is focussed on high alcohol hours (i.e., times and days of the
week when alcohol-related road crash deaths and injuries peak) and which is random, unpredictably located, and well
publicised. Rurally-based breath testing requires operational dierences compared to that conducted in urban areas (1).
Programme focus
Generic advertising warnings and education, observable police enforcement,
perception ANYWHERE/-ANYTIME, target education of specific groups
Source: (2) with authors’ elaboration.
38 Drink driving: a road safety manual for decision-makers and practitioners

3.1 Enforcement methods
Enforcement methods that have been used successfully to change driver behaviour include alcohol
screening of drivers (random and based on “good cause to suspect”), and targeted enforcement
based on intelligence. These enforcement methods are not mutually exclusive and should ideally be
employed in combination to achieve maximum eect. Ranked from most to least eective are the
following enforcement actions:
Random breath testing (RBT): based on the principle of ‘anywhere at any time’; RBT can occur
when there is the statutory authority for an enforcement oicer to stop a vehicle and test the driver
at random, without need to establish that the driver committed another oence, nor that the driver
showed any signs of impairment prior to being stopped;
Sobriety checkpoints: where police are required to form a suspicion of alcohol impairment before
they can administer a breath test (less objective and less eicient than RBT);
Targeted programmes: for example, waiting for drivers to leave bars and then testing them. This
approach is least eective because it impacts on a very small number of drivers and should be a
lesser focus than an RBT programme
Highly visible, high volume random breath testing reminds drivers of the possibility of being detected
if they have been drinking and provides an eective deterrent to motorists who are not stopped.
Roadside testing can take place at designated testing stations (checkpoints or roadblocks) or during
normal police interceptions (see Box 3). The Global Status Report on Road Safety 2018, recognises that
enforcement that incorporates random breath testing (RBT) is eective in increasing both the perceived
and actual probability of being caught. It is estimated that RBT can reduce fatal drink driving crashes
by approximately 20% if it is publicised, highly visible and frequently used (3). Roadside drug
testing also occurs in some jurisdictions. Details of an evaluation of both alcohol and drug testing and
enforcement protocols in Victoria, Australia have been described in an evaluation report published by
the Monash University Accident Research Centre (4).
This image depicts checkpoint operations in the metropolitan areas of São Paolo, Brazil. The highly
visible checkpoints help to promote the general deterrent eect of enforcement operations.
Photograph: Checkpoint
operations in São Paolo, Brazil.
Municipio de Guarujá-SP. January
21, 2022. Programa "Operação
Direção Segura Integrada – ODSI”.
Decreto nº 58.881/2013. DETRAN-
SP. Retrieved: 14.04.2022.
Module 3 Enforcing drink driving laws 39

In Victoria, the use of special-purpose “booze buses” – clearly identified as random alcohol- screening
vehicles and immediately recognisable by the public – have been highly successful in reducing drink driving.
These vehicles contain all the equipment needed to operate as a mobile police station for the eicient testing
of drivers and oender processing. The enforcement process is complemented by a highly professional and
intense public advertising campaign using television, radio, print media and billboards (1). Key components
of this enforcement strategy include large volume testing, random and unpredictable test sites, and a focus
on high alcohol hours. Once random drug testing was introduced in Victoria, these vehicles were also used
for roadside screening of drivers.
Photograph: Victoria Police Roadside Testing Bus
Box 3. Random breath testing in Australia
The eect of drink driving checkpoints can be maximised by (5):
a. Making them highly visible:
– operating at random and unpredictable locations with a focus on high alcohol hours
– working in teams and following a standard protocol in safe operational environments
– using flashing warning lights to draw attention to the programme and enhance safety for all
involved
40 Drink driving: a road safety manual for decision-makers and practitioners
– displaying signage at the checkpoint indicating the reasons for the enforcement activity (for
example, “drink-driving enforcement”)– this will provide a clear deterrent message to all drivers
going through the site or driving near the checkpoint.
– deploying many police oicers and police vehicles– to this end it is important to have mobile
units with the capacity to provide evidential testing and processing of oenders at the site of
interception. This gives the public the impression of a higher level of enforcement activity than
is actually being delivered as the police should move their enforcement or checkpoint zone to
dierent locations during a single shift so that drivers cannot predict where enforcement will be
operating. Having evidential testing equipment at the point of interceptions also avoids the drain
on resources and wasted time in having to transport suspected oenders to a police station for
an evidential breath test.
b. Rigorously enforcing drink driving laws to ensure credibility:
– If the law is not enforced, drivers will generally not comply. They must be informed about the
legitimacy of the intervention and believe that this will improve their safety.
– Everyone is equal – no exemptions, no bargaining, no special circumstances (i.e., no corrupt
practices). Everyone stopped should be breath tested (in line with RBT principles).
–
In keeping with the principles of procedural justice and procedural fairness in policing, enforcement
oicers must always be polite, fair, respectful and firm when processing oenders (6).
c. Setting up checkpoints as often as possible, over a long period of time:
– Drivers must consistently see enforcement activities and consistently hear about them, to gain
the understanding that they can occur anywhere, any time.
– The same enforcement strategy and protocol must be repeated often in multiple locations.
– Conduct night-time blitzes involving teams of police oicers working in well-lit, safe areas.
– Where the law permits, conduct continual random testing – that is, every driver intercepted for
any oence is tested for alcohol.
The points listed above form the basis of an intervention strategy that can be highly successful in
bringing about a general perception that drivers or riders can be tested anywhere, any time. Accurate
measuring of alcohol in the bloodstream is also a vital component of eective enforcement. It is critical
to have suicient screening devices which are practical, reliable, and easy to use, and that are fully
maintained and calibrated on a regular (six-monthly) basis to ensure accuracy and support enforcement
legitimacy.
A minimum annual target of alcohol screening tests should be set and maintained. The minimum
targets set should relate to the percentage of the driving population tested during the year. A solid
strategy aims to test 1:3 drivers annually, although the more progressive enforcement bodies in some
high-income countries aim at 1:1 – on average every driver would expect to be tested once per year.
Targeted enforcement based on intelligence (see Box 4 for additional information) involves
detection of drink drivers at specific locations, times, and under specific circumstances. This kind of
enforcement activity represents a ‘specific deterrent’ strategy aimed at oenders, rather than a ‘general
deterrent’ strategy aimed at the general driving population) and involves:
Module 3 Enforcing drink driving laws 41
stopping drivers as they leave selected alcohol distribution premises such as hotels, entertainment
venues/locations, night clubs, sporting and gaming venues that should be the subject of police
attention on account of the high possibility that drinking and driving may take place;
at collision zones or high-risk areas;
breath testing all drivers intercepted by police, regardless of the reason for interception, if legislation
permits random breath testing;
breath testing all drivers involved in road traic collisions;
breath testing individual drivers who are known to continue to drink and drive after initial detection
(i.e., repeat drink-drivers);
as a principal enforcement measure, covert operations should support the major operational strategies
but never take precedence; the main focus must be on high visibility enforcement for the whole
driving population; and
during high-risk alcohol times or days of the week; (see example below).
42 Drink driving: a road safety manual for decision-makers and practitioners
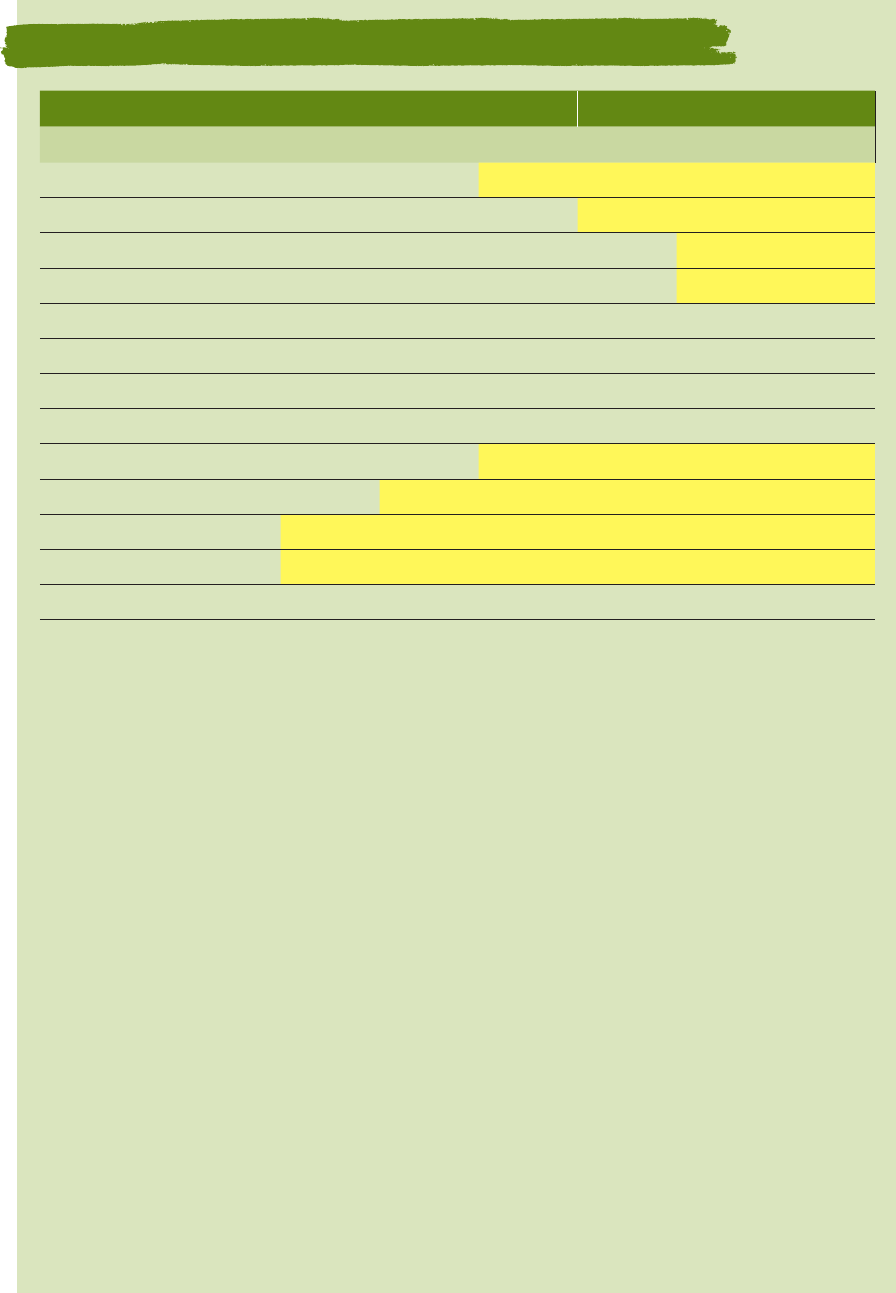
Number of Alcohol-related fatal/injury crashes Greater than average (91)
Time of Day MON TUE WED THU FRI SAT SUN
00.00 – 1.59 am 64 48 80 124 161 319 327
2.00 – 3.59 am 31 32 54 68 130 256 295
4.00 – 5.59 am 22 15 34 48 62 180 215
6.00 – 7.59 am 19 15 22 35 45 104 132
8.00 – 9.59 am 15 17 12 22 26 45 51
10.00 – 11.59 am 10 12 22 23 20 41 37
12.00 – 1.59 pm 21 19 25 28 30 50 55
2.00 – 3.59 pm 33 47 43 46 57 80 66
4.00 – 5.59 pm 38 76 84 94 104 108 103
6.00 – 7.59 pm 73 86 108 101 182 183 135
8.00 – 9.59 pm 69 103 134 161 229 256 131
10.00 – 11.59 pm 65 121 158 200 291 299 96
TOTAL 460 591 776 950 1337 1921 1643
*This table demonstrates how ‘high alcohol’ hours are identified using data from New Zealand. The data
records the number of alcohol-related fatal and injury collisions by time period, shown in two-hour blocks
across a week using five years of data between 2008 and 2012. The yellow shaded areas show days of the
week and times of day when alcohol-related crash trauma peaks. These yellow shaded areas show that
the most high-risk periods are between 10pm to 2am on Friday/Saturday and Saturday/Sunday nights. This
method allows police to identify the highest risk time periods and to target breath testing to these periods.
Source (7)
NOTE. Data that can guide intelligence-led enforcement
Accurate statistics on fatalities, serious injuries, injuries and crashes, and the role alcohol plays as a causal
factor.
Crash data as it relates to times of the day, days of the week and particularly critical locations. If presented
in an appropriate format, this data will provide the profile on high alcohol times, days of the week and
locations upon which to focus police resources for maximum eect.
Accurate statistics on the amount of alcohol consumed by oending drivers.
Locations where drivers consumed the alcohol – this information can assist with targeted enforcement
(including holding liquor licence holders accountable for supplying alcohol to those who are intoxicated,
where relevant) and educational intervention campaigns.
Blood alcohol readings of drivers admitted to hospital.
BAC readings obtained from apprehended oenders.
Toxicology reports from a Coroner’s court for all deceased drivers.
Identification of high-risk user groups by age or social standing, thereby assisting strategies for targeted
enforcement and specific education.
Data must be accurate and analysed for trends to determine enforcement strategies and, most importantly,
must be maintained for assessing performance outcomes.
Box 4. Drink Driving Enforcement – High Alcohol Hours (2008 to 2012) *
Module 3 Enforcing drink driving laws 43
3.2 Safely intercepting vehicles
Intercepting moving vehicles in the flow of traic for random or targeted enforcement requires the
utmost attention to planning and risk assessment. The safety of enforcement oicers, all road users, and
oenders/suspects is vital when setting up a checkpoint or roadblock. No site should be in operation
without a designated safety oicer who has the responsibility of ensuring overall safety. Even where
only two or three oicers are operating, one oicer should be the designated safety oicer. These
mobile checkpoints (intercepts) can achieve the same results as conventional checkpoints, but with
fewer people. They are mobile and typically will not last as long as full-scale checkpoints. Managing
these kinds of checkpoints includes:
3.2.1 Choosing a safe location:
Consider:
locating the site where approaching drivers have suicient time and visibility to adjust their driving
in order to safely negotiate and stop at the checkpoint -if in doubt, choose another location;
safety factors for oicers when setting up and dismantling the site –persistent bad weather or poor
visibility (e.g., from heavy fog) can render a site impractical or unsafe;
moving the site to multiple locations during the course of the work period to maximise the visible
police presence;
sun glare for drivers approaching the site (the sun will change position during the course of the day);
visibility for motorists, which is of particular concern at dusk and dawn, so extra precautions should
be taken if the operation is taking place over that period;
locating night-time operations where there is eective illumination and providing additional lighting
for high visibility;
control of vehicles moving into the site as well as those vehicles passing it;
the avoidance of unnecessary traic congestion– judgement as to what constitutes unreasonable
congestion is subjective, but as a general rule, if you cannot see the end of the traic in the distance,
it is time to suspend testing operations and allow it to flow until you can; and
the use of natural barriers where traic calming is achieved (e.g., toll gates).
For an example of good alcohol checkpoint practices, please refer to the Global Road Policing Network (GRPN)
site which hosts a video from New Zealand Police https://www.youtube.com/watch?v=xVkDOiLfMdk (8).
Documents produced by the Federal Ministry of Health in Mexico (9) and by the municipal government
of Fortaleza, Brazil (10) also contain useful information. (https://www.gob.mx/cms/uploads/attachment/
file/249279/Protocolo_2a_edici_n.pdf). (https://diariooficial.fortaleza.ce.gov.br/download-
diario?objectId=workspace://SpacesStore/1a1c4cc9-f89c-4c34-a440–3b418eeb19d8;1.1&
numero=15884.)
44 Drink driving: a road safety manual for decision-makers and practitioners
3.2.2 Choosing the right method to select vehicles
Methods include random and specific selection:
Random selection can include directing the following vehicles into the site:
– cars (at random), or
– every tenth vehicle (depending upon traic flow), or
– five cars, then let the traic continue to flow.
Specific selection will depend upon intelligence gained about drinking patterns and collision data or
prior history of alcohol consumption among sub-groups in the community and can include:
– all vehicles
– all taxi drivers or professional drivers
– all vehicles of a particular type
– all heavy vehicles.
3.2.3 Using equipment to ensure safety
Safety is paramount. The right equipment must be used properly to ensure the safety of enforcement
oicers and road users at all times.
All those on site must wear reflective vests or jackets, both day and night.
All enforcement agents must be in the relevant uniform.
Use police vehicles as traic protection.
Use marked police vehicles with lights flashing to maximise visibility (be conscious of the battery life
with lights flashing and engine o).
If there are any “oicial” observers, they must not be permitted on site without reflective vests, should
maintain an appropriate safety distance, and carry appropriate credentials/identification.
Equipment should include illuminated torches fitted with a red cone to provide a contrasting colour.
Delineation of the site should be with strobe lighting and/or red safety cones.
Consider if any of the surrounding equipment could be used as a safety barrier.
Consider natural barriers or natural interception points (e.g., toll gates, service stations, parking centres,
entry/exits) or the use of portable speed humps for the roadway approaching the checkpoint.
Ensure there are suicient police numbers for a safe, eective, and eicient operations.
Ensure the Operations Command Centre is aware of the site location.
Consider photographic and/or video evidence (following local protocols and respective permits as
required).
Module 3 Enforcing drink driving laws 45
3.2.4 Contingency planning
As part of any planned enforcement activity there will inevitably be detections of oences that may
not necessarily be the focus of the operation. These other oences can include uncooperative drivers
needing to be dealt with for aggressive behaviour and non-compliance of legislated requirements;
persons wanted on warrants and arrests on criminal matters.
Large scale checkpoints will always detect a range of oences. This must be taken into account in the
planning stages by ensuring there is a process in place to deal with:
warrants to arrest,
unlicensed or disqualified drivers,
unregistered vehicles (this contributes to the functioning of automated enforcement),
fake and obscured number plates, driving licences or permits,
stolen vehicles,
drug possession or drug dealing oences,
possession of oensive weapons (anything that is carried to cause injury),
drivers who fail to stop for or fail to remain at the checkpoint.
These oences need to be dealt with in an environment that is safe for both sta and other road users.
The evidence obtained during this process must be entered into a secure chain of custody system for
subsequent prosecution, by ensuring that a process for dealing with oences is written into any Standard
Operating Procedure (SOP) and operation orders.
3.2.5 Getting the message across
The most important aspect of this method of policing is to provide a deterrent to those being checked
for alcohol (specific deterrent eect) and to drivers who pass by but are not checked (general deterrent
eect). Drivers passing the site should be made aware of the purpose of the checkpoint by means of
either a “variable message sign” or large fixed sign advising “Drink and driving enforcement”. If this is
not done, other drivers may assume it is an ordinary police security check or other traic checkpoint,
and no change to their attitude will likely occur.
3.2.6 Processing offenders quickly
Drivers should be processed with minimum delay. Testing should be compliant with any statutory
requirements, as should access to legal advice for the driver. Observations should be clearly stated to
the driver and corroboration from fellow oicers sought if there is denial by the driver. Evidence should
be recorded without argument or bargaining. It must also be secured to ensure the chain of evidence
is maintained to support subsequent prosecution. Police must always be courteous, respectful, and
polite, and maintain a high degree of skill and professionalism.
46 Drink driving: a road safety manual for decision-makers and practitioners
3.2.7 Meeting statistical requirements
The following information should be recorded:
number of breath tests conducted;
number of oenders processed and over the BAC limit;
date/time and location data;
number and details of other incidents, if any.
3.3 A dedicated alcohol intervention unit
Many countries that have succeeded in reducing the prevalence of drink driving have dedicated alcohol
intervention units within the police. These units are responsible for the coordination of policing eorts
and countermeasures relating to drink driving. A dedicated unit provides the benefits of centralised
coordination and ability for expertise to be established. It should be responsible for:
integration with other road safety strategies for road trauma reduction;
facilitating education, awareness and social marketing campaigns directly supporting enforcement;
facilitating training for general police personnel;
gathering statistical data and intelligence to improve enforcement and detection methods;
working with private and public sector organisations in the provision of education, seminars and
workshops on the eects of drink driving. The dedicated unit can provide comprehensive advice and
education to assist in reducing drink driving in these organisations and their employees;
developing partnerships with government, semi-government agencies and large representative groups
such as those within the transport industry and professional drivers. Drink driving is a community
problem needing community-based solutions. Police cannot and should not be expected to achieve
the results without a cooperative and consultative approach.
maintaining direct links to research organisations. This will enable police to seek independent
evaluation and research before, during and after implementing any programmes.
3.4 Penalties for drink driving offences
Operating a vehicle when over the legal BAC limit should be represented in legislation as one of the most
serious driving oences possible and the punishment should reflect that while remaining reasonable and
proportionate to the level of oending in order to maintain legitimacy and the support of the community.
Punishment must also be culturally and economically appropriate. Commonly applied penalties include:
Monetary fines, which may rise with multiple convictions, as BAC levels increase, or with the oender’s
income. Fines must take account of local economic circumstances and be seen as appropriate relative
to fines for other oences in the traic law;
Suspension or withdrawal of driving licence, which, in theory, prevents the person from driving until
the end of the suspension/disqualification period. In practice, many disqualified drivers may continue
Module 3 Enforcing drink driving laws 47
to drive illegally, and the eectiveness of this sanction will depend on the chances of the driver being
stopped in any subsequent police check and their willingness to risk driving illegally;
For crashes which result in a fatality or injury, a drunk driver may be jailed for several years and/or
have their driving licence permanently revoked;
Vehicle impoundment (sometimes also referred to as vehicle immobilisation or forfeiture) has been
used in some jurisdictions (e.g. Canada, the United States of America, New Zealand, Australia) for
repeat drink driving oenders as a mechanism to separate the driver from their vehicle for an extended
period of time (e.g. 30 days to up to six months). Impoundment of the vehicle is often at the expense
of the oender, and has been found to be eective at reducing the incidence of drink driving and
alcohol-related crashes (11, 12),
Vehicle licence plate seizure has been found to be eective when it can be undertaken by police at the
time of the arrest. Fees are typically charged to obtain plates so this activity can be revenue neutral (11).
Vehicle registration cancellation – cancelling vehicle registration is likely to have limited applicability
in low- and middle-income countries unless registration rates are high. Even where this is the case,
vehicle registration cancellation is typically only applied in cases where the drink driving oender is
the sole driver of the vehicle.
Alcohol interlocks – see discussion in section 2.3.2.
Additional information about penalties can be found in the guide produced by the Global Road Safety
Partnership (13).
Module Summary
It is essential to adopt a multifaceted approach, combining legislation, enforcement, and public
awareness and social marketing campaigns, to combat drink driving.
Appropriate and enforceable laws must be in place – mandating use of roadside testing equipment
and the use of their results as evidence.
Laws on a maximum BAC limit for drivers/riders is essential. Legislation must specify how BAC levels
are to be enforced and what powers are to be given to the police in their enforcement eorts.
Legal BAC limits generally range from 0.00 to 0.05 g/100ml. Many countries have lower BAC limits
for specific driver groups, such as young drivers, drivers of commercial vehicles, which have proven
eective in reducing crashes involving drinking and driving.
Several devices which permit roadside testing of breath alcohol levels are available to facilitate the
enforcement of drink driving laws, and results are admissible in court in a number of countries.
Legislation should state the type of oence and realistic penalties for those oences.
Enforcement activities should be combined with public awareness and social marketing campaigns
to gain community understanding and acceptance.
Enforcement objectives should be casualty reductions, not apprehensions.
Enforcement eorts should be intelligence-led and aimed at promoting the perception among the
driving public that they can be tested anywhere and at any time.
Enforcement should prioritise highly visible, random, high alcohol hour alcohol screening which
provides a general deterrent eect for the wider population. Targeted enforcement should be a lesser
48 Drink driving: a road safety manual for decision-makers and practitioners
focus as it serves to facilitate prosecution of drivers who refuse to stop drink driving. Both enforcement
methods should be employed in combination for better results, but a clear priority should be placed
on enforcement that promotes general deterrence.
Public awareness and social marketing campaigns are an important tool but in isolation, will not
change behaviour. They must be used in conjunction and coordination with the implementation of
eective enforcement. All campaign messages and materials should be market-tested.
Long timeframes must be allowed for changing public perceptions and behaviour. The lessons learned
through the monitoring and evaluation of the campaign impact on drink driving should be used to
improve the quality and impact of future campaigns.
References Module 3
1. Delaney A, Diamantopoulou K, Cameron M. Strategic principles of drink-driving enforcement (report no
249). Melbourne: Monash University Accident Research Centre. 2006.
2. World Health Organization. Drinking and driving: a road safety manual for decision-makers and
practitioners. 2007.
3.
Global status report on road safety. Geneva, World Health Organization, 2018. Licence: CC BYNC-SA 3.0 IGO.
4. Newstead, S., Cameron, M., Thompson, L., & Clark, B. (2020). Evaluation of the Roadside Drug Testing
Expansion and Roadside Alcohol Testing Enforcement Programs in Victoria (report no 355). Melbourne:
Monash University Accident Research Centre. 2020.
5. Homel R. Policing and punishing the drinking driver: A study of general and specific deterrence. New
York, NY, Springer-Verlag, 1988.
6. Mazerolle L, Bennett S, Davis J, Sargeant E, Manning M. Procedural justice and police legitimacy: A
systematic review of the research evidence. Journal of experimental criminology. 2013 Sep;9(3):245–74.
7. New Zealand Police. Road Policing Support Group, Police National Headquarters. New Zealand, 2013.
8.
New Zealand Police. Compulsory breath Testing Checkpoint with English subtitles [video file] year, month,
[cited 2021 Dec 21]. https://www.youtube.com/watch?v=xVkDOiLfMdk Accessed 24 January 2022.
9.
Secretaría de Salud. Protocolo para la Implementación de Puestos de Control de Alcoholimetría. Ciudad de
México: Secretaría de Salud, STCONAPRA y Organización Panamericana de la Salud, 20 Enero 2017. https://
www.gob.mx/cms/uploads/attachment/file/249279/Protocolo_2a_edici_n.pdf. Accessed 24 January 2022.
10. Fortaleza (Brazil) Autarquia Municipal de Transito e Cidadania. AMC Manual de Procedimentos
Operacionais da AMC – MPO/AMC, DiÁrio Oficial do Municipio. Portaria N° 1198/2016. https://diariooficial.
fortaleza.ce.gov.br/download-diario?objectId=workspace://SpacesStore/1a1c4cc9-f89c-4c34-a440
–3b418eeb19d8;1.1&numero=15884. Accessed 29 January 2022.
11. Voas RB, Fell JC, McKnight AS, Sweedler BM. Controlling impaired driving through vehicle programs:
An overview. Traic injury prevention. 2004 Sep 1;5(3):292–8.
12.
Watson B, Angela N. Submission to Travelsafe: vehicle impoundment for drink drivers. Centre for Accident
Research and Road Safety– Queensland (CARRS-Q), QUT, Brisbane, Qld. 2006.
13.
Sakashita, C. Fleiter, J.J, Cli, D., Flieger, M., Harman, B. & Lilley, M (2021). A Guide to the Use of Penalties to
Improve Road Safety. Global Road Safety Partnership, Geneva, Switzerland. https://www.grsproadsafety.
org/wp-content/uploads/Guide_to_the_Use_of_Penalties_to_Improve_Road_Safety.pdf. Accessed 21
January 2022.
Module 3 Enforcing drink driving laws 49

4

Module 4
Implementing evidence-based
drink driving interventions
Programmes aimed at reducing the number of road crashes involving alcohol must have a long-term
commitment. They will have a long-term objective, such as reducing the number of road crashes
involving drink driving by a certain percentage within a specific time period. They will also contain
a number of specific components that will help “deliver” the programme objective. Long-term and
sustainable changes in public perception and driver behaviour are not achieved easily or quickly.
Depending on the existing situation of the country/jurisdiction, the timeframe from implementation of
the law to full enforcement and issuing of penalties for non-compliance can range from a couple of
months to several years.
This module provides guidance on the following issues:
Cycle of improvement – a continuous examination of programme implementation and outcomes.
Pathways to change – a systematic approach to understanding the pathway to change in order to
reach a long-term goal.
How to assess the situation– numerous types of assessments can provide the information needed
to design, deploy and maintain an eective programme.
Opportunities and challenges in implementing drink driving interventions– implementation
success can be maximised by understanding the challenges and seizing opportunities.
Evaluation of progress and using results for improvement – evaluating results is vital in eective
decision-making and modifying a course of action.
4.1 Cycle of improvement
Improving the road safety situation in a country by reducing the incidence of drink driving requires
continued eorts in planning, executing and evaluating programmes. It is not a one-o undertaking and
should be seen as a continuous cycle of improvement. There are opportunities as well as unexpected
challenges that need to be managed as this cycle continues. Implementing a continuous cycle of drink
driving prevention improvement begins with an assessment of the existing system, followed by the
development, execution, evaluation, and refinement of a national or a local plan of action. A plan of
action will not yield improvements unless it is translated into practical solutions in a country. In addition
to identifying and prioritising actions that should be taken, there are key ingredients that need to be
considered and made available or developed: human and financial resources, sharing responsibility
among dierent agencies, and political commitment, as specified in the Global Plan of Action (2021).
(1, 2, 3, 4).
Module 4 Implementing evidence-based drink driving interventions 51
4.2 Pathways to change
Applying the Safe System Approach to road safety results in a complex set of interacting interventions
which make them quite diicult or sometimes even unethical to implement and evaluate using traditional
research methods such as a randomised controlled trial. For this reason, some researchers have
proposed that “understanding the public health intervention’s underlying theory of change and its
related uncertainties may improve the evaluation of complex health interventions” (2).
A Theory of Change is therefore basically the pathway(s) that will be followed to achieve the objective of
a programme. It “explains how activities are understood to produce a series of results that contribute to
achieving the final intended impacts. It can be developed for any level of intervention implementation –
an event, a project, a programme, a policy, a strategy or an organization” (3) or the evaluation of such
interventions or set of interventions (impact evaluation). It encourages “systems thinking” through the
understanding of the complex social change processes, dierent perspectives, assumptions and the
contexts needed to optimise success.
A Theory of Change is a systematic approach to understanding the pathway to change in order to reach
a long-term goal. It should always begin with a good situational assessment in order to understand the
causes, risk factors, opportunities and challenges in the local situation where an intervention is to be
implemented. It should then be guided by a participatory approach – bringing together multiple key
stakeholders, through a workshop for example, to discuss the proposed approaches or interventions
that need to be implemented to optimise impact. Although developing a Theory of Change is an iterative
process, and there are many ways it can be developed, it should include the following basic steps (4):
1. Identify the long-term outcome
2. Develop a pathway of change
3. Operationalise outcomes
4. Develop interventions
5. Articulate assumptions
6. Monitor and evaluate the process
As a final output of stakeholder discussions, a visual map of the change being explored should be
developed to show the relationships between proposed actions/interventions and outcomes and how
these interact in order to achieve the goal.
The benefits of developing a realistic and implementable Theory of Change are articulated in Box 5.
In general, this process challenges the status and gets stakeholders to “think outside the box” so that
mistakes are not made when interventions are implemented. It also forces stakeholders to think about
resources and how these will be best utilised to bring about the required change. Finally, the process
develops a shared understanding of the actions to be taken and expected outcomes on one hand, and
accountability on the other.
52 Drink driving: a road safety manual for decision-makers and practitioners

It will provide:
A clear and testable hypothesis about how change will occur that not only allows you to be accountable for
results, but also makes your results more credible because they were predicted to occur in a certain way;
A visual representation of the change you want to see in your community and how you expect it to come
about;
A blueprint for evaluation with measurable indicators of success identified
An agreement among stakeholders about what defines success and what it takes to get there
A powerful communication tool to capture the complexity of your initiative
Source: (3)
Box 5. How a Theory of Change would benefit your programme
The following sections outline some of the steps you would need to undertake in order to assess,
implement and evaluate and eective drink driving intervention in your country.
4.3 Assessing the situation
It is vital to understand the current situation (e.g., prevalence and locations of drink driving, oender
demographics) before launching an intervention. Assessment of the existing situation in your country
or region helps you design and implement a programme that is relevant and successful. This ‘baseline
data’ will enable you to accurately evaluate the eects of any multi-sectoral road safety interventions
that are implemented. There are four key assessments:
health and crash investigation data on incidents involving alcohol to assess the extent of the problem
in your community and identify main target groups. It is important to note that a prerequisite for this
first step is accurate alcohol-related crash data, and the first step to gaining this information is
ensuring that police are breath/blood testing after every crash and accurately recording the
results in crash investigation reports;
existing laws on or relevant to drink driving to understand the current legal framework and what
changes are needed;
stakeholders to identify the interest groups, their positions and how to eectively involve them in the
programme;
community perceptions to assess the level of community understanding of the problem, trust in the
police, and support for interventions and to determine possible ways to address the gaps.
Since the first Global Status Report on Road Safety was published in 2009 (5), much has been advanced
to assemble road crash data. Data on the incidence, severity, types and causes of crashes provide
insights into drink driving patterns and how to target interventions on those at greatest risk. For instance,
it may turn out that busy urban roads are a high-risk area; or that young males may be the group found
to be at greatest risk of drink driving (see this example of use of monthly monitoring of BAC limits from
Mexico (6). Key data which can be used to assess the situation include the following.
Percentage of drivers and riders killed with a BAC over the legal limit – In some countries,
this information is routinely available, although coverage is rarely complete. Even if there is a legal
Module 4 Implementing evidence-based drink driving interventions 53
requirement that blood samples are taken on admission to hospital, the pressure of work in emergency
departments often means that this is not done.
Number of alcohol oences detected – This measure can give reasonably complete numbers of
driving oences involving alcohol impairment over time, but it is dependent on the extent of police
eort put into alcohol enforcement. Therefore, caution is required on whether it provides a true
reflection of the actual situation.
Percentage of drivers stopped with a BAC over the legal limit – This can be a useful measure,
particularly where random breath testing checkpoints are used and large numbers of drivers are tested
during high alcohol hours. However, the proportion of drivers with a BAC over the legal limit can be
expected to fluctuate, depending on where and when enforcement operations are conducted. This
measure should therefore be treated with caution when assessing individual operations, or operations
over a short period. If the intensity, timing and type of location for operations are stable over the long
term, then it can be a useful measure.
Driver surveys – Levels of drink driving and trends can be assessed via independent surveys where
researchers stop vehicles, or, in a controlled environment, approach vehicles stopped at lights, and
request breath samples. Care must be taken in deciding which times of day and which locations
to use to ensure that the breath sample is representative of driving over the time period and road
network for which the information is required (see examples from the Netherlands (7) and from three
South American countries (8). Another eective measure is to work closely with police and ask them
to conduct breath tests on all drivers involved in crashes (if they have ready access to breathalysers).
In some countries this is required by law.
Analyses of the types of data above by age, sex, times, and location help to prioritise activities, and
to plan and focus interventions where they are most needed. The following entities generally collect
and maintain road crash and road crash injury data that could be helpful in gauging the extent and
understanding the nature of the problem.
Police authorities: In most jurisdictions, investigating crashes is the responsibility of police. Since
police are responsible for detecting breaches of traic law, it is probable that police crash records
would include details of any involved road user being aected by alcohol. In countries where breath
or blood tests may not be regularly collected, the presence and role of alcohol can be subjective
rather than objective.
Road authorities: Crash records may also be maintained by the road authority. However, these
records may not include comprehensive information about crashes. The primary interest of the road
authorities is to identify shortcomings in the road system for which they have responsibility, so it is
probable that alcohol involvement may well not be covered in their records.
Health system: In some countries, the health system is the only comprehensive source of data on
road crash injuries. For most countries, this is likely to be confined to admissions to the hospital
system and, therefore, to consider only the more serious injuries. Since the primary responsibility of
the hospital is the care of injured people, details of the location of the crash, the events associated
with it and the blood alcohol content (BAC) of the injured person may not be part of the records. For
instance, frequently, those admitted to Trauma and Emergency departments are simply recorded as
having been involved in a road crash, without being identified as a driver, passenger or pedestrian.
Other potential information sources about alcohol involvement in crashes include employee and
insurance records. Even if comprehensive crash records can be assembled from one or more of the
54 Drink driving: a road safety manual for decision-makers and practitioners
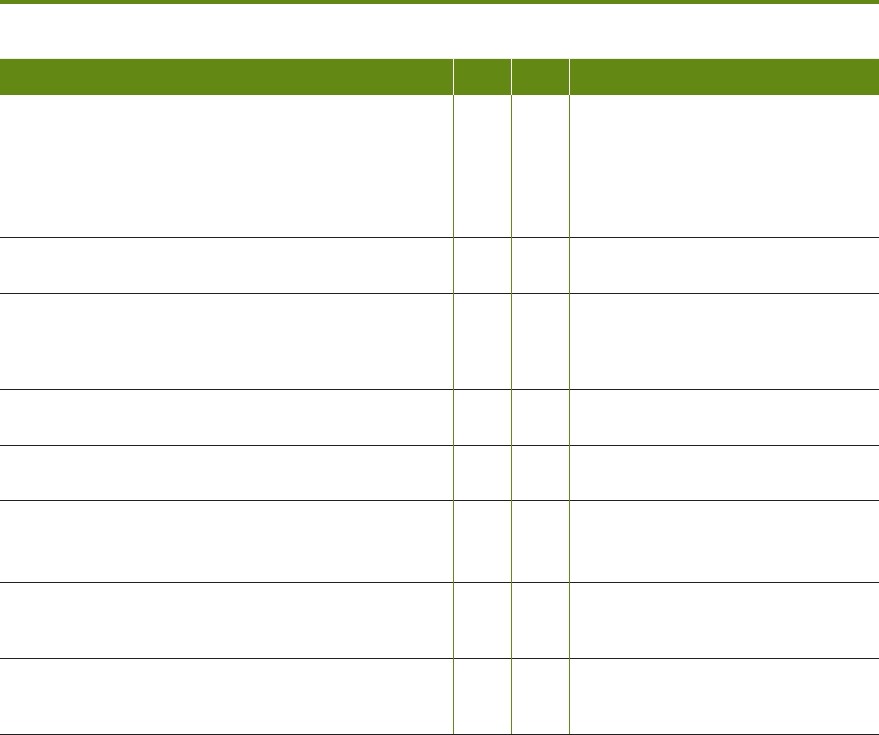
sources described above, the extent of alcohol involvement in crashes needs to be determined in order
to make an overall assessment of the true scope of the problem. Ideally, alcohol involvement in crashes
should be based on objective breath or, where appropriate, blood testing of drivers at the roadside and/
or of those injured at the hospital. If the record of alcohol involvement is based on subjective reports
such as “alcohol consumed” or “drunk”, there is likely to be considerable underestimation of the problem
because an investigating police oicer or a medical practitioner is unlikely to consider a driver impaired
until a relatively high BAC is reached.
If available crash data includes reliable information on BAC for a reasonable proportion of the drivers and
riders involved in crashes, then assessing overall alcohol involvement is a relatively straightforward process.
Should information on BAC levels not be available, another alternative is to conduct cross tabulations using
existing crash data. Cross-tabulations that include location, month, day of week, time of day, speed limit
and road class can be used to build a picture of where and when crashes occur. Cross-tabulating alcohol
involvement by age, gender and type of vehicle can be expected to give guidance about which drivers to
target in publicity and social marketing campaigns. Table 3 provides a guide to assessing road traic data.
Table 3. A guide to assessing road traffic data
Question YES NO DATA/EXAMPLE
1. How many injuries and deaths occur as a result of road
traic crashes in the project region?
(Note that it is important for the working group to
predefine the project unit or region of assessment. For
example, this may be the entire country, or it may be a
particular province/state, town or community)
e.g. from police records, hospital records
2. Is data available on road crashes involving alcohol that
can be analysed?
e.g. from police test records, hospital
blood tests
3. What is the scale of the problem of alcohol related
crashes in terms of the number of crashes and the
number of fatalities? What proportion of all road traic
crashes does this comprise?
e.g. from police records, hospital records
4. Does the data provide detailed information on where
and when the crashes occur and who is involved?
e.g. police records of crash locations
5. Who are those most likely to be involved in crashes
involving alcohol?
e.g. police crash records, hospital
records, surveys of alcohol users
6. Are the primary risk factors known?
(Example risk factors may include age, gender, time of
day, prior history of drinking and driving.)
e.g. studies on drinking patterns within
society
7. Are hospitals equipped and legally allowed to take
blood samples?
e.g. does legislation support medical
practitioners taking blood samples on
request from police?
8. Are police trained and equipped for on-road
enforcement of drinking and driving laws?
e.g. are oicers certified to use devices,
and are passive and evidential breath
test devices available?
Understanding what laws exist in your country and whether they are adequately enforced is a critical
part of understanding the situation and identifying priority actions. It is therefore useful to begin by
reviewing the current state of the laws, as in Table 4.
Module 4 Implementing evidence-based drink driving interventions 55
Table 4. Checklist for assessing the comprehensiveness of drink driving legislation
YES NO
1. Blood alcohol concentration limits
• Imposes limits that are consistent with evidence and recommendations on drink driving (0.05 g/dl
or below)
• Sets limits for novice or young drivers (BAC, 0.02 g/dl or below)
• Sets a zero limit for commercial drivers (i.e., trucks, taxis, public transport vehicles)
2. Restrictions on availability of alcohol
• Specifies a minimum legal drinking age
• Imposes restrictions on sale and supply of alcohol to underage people
• Restricts or bans alcohol advertisement/marketing
3. Enforcement
• Provides for enforcement by random breath testing and/or sobriety checkpoints (noting that for
reasons explained earlier, sobriety checkpoints are less eicient and hence less eective)
• Requires alcohol testing of everyone involved in a crash (in hospital or at crash scene)
• Establishes who has authority for enforcement
• Device used to provide evidential BAC readings (i.e. can be used as evidence in a court of law)
• Regular maintenance and calibration of testing devices
• Conducting according to established Standard Operating Procedure and relevant protocols
• Authority for the use of alcohol ignition interlock programmes, including criteria for oenders
• Provides notice requirements for certain enforcement activity, if applicable
4. Penalties
• Provides a mechanism to monitor sale or supply of alcohol to underage people in certain facilities
• Defines penalty based on degree of severity of infraction above established BAC limit
• Provides specific financial penalties proportionate to average income, or based on individual means
testing
• Includes provision for driver remediation
• Provides for licence suspension based on degree of severity of infraction above established limit
• Includes provisions pertaining to vehicle impoundment
5. Other drink–driving measures
• Specifies whether the penalty includes criminal punishment, with reference to the penal code if
applicable
Source (10) with authors’ elaboration
A stakeholder assessment can shed light on the social environment in which a drink driving programme
will be developed and implemented. Experience has shown that it is important to involve members of
a wide variety of groups, representing diverse interests. Such an approach can often overcome initial
concerns and opposition before reaching the public sphere. It is important to identify supporters and
opponents and, moreover, to appreciate the reasons for their respective positions, to be able to develop
a marketable package that satisfies all concerned parties. Experiences from countries including Brazil,
Colombia, Australia, and France show that concerted eorts to implement eective interventions can
have substantial impact on the level of injuries sustained in drink driving-related crashes. Dierent
stakeholders can play dierent but complementary roles to maximise the success of a drink driving
programme (See Table 5).
56 Drink driving: a road safety manual for decision-makers and practitioners
Table 5. Potential roles and responsibilities for stakeholders involved in anti-drinking and
driving programmes
Authority Major role and responsibility
Road safety authority
Legislation
Funding
Programme coordination, strategy, monitoring and reporting
Major publicity/social marketing campaigns
Police
Enforcement of drink driving laws
Collection of quality data from crash investigations to inform road safety interventions
Public commentary
Participant in community education activities
Hospitals/Health Authorities
Political lobbying in support of interventions
Community leadership in discussion and debates
Highlighting health benefits from eective programmes
Data collection of injured patients (including BAC)
Insurance companies
Provision of important funding for interventions (and in some countries, funding for
national road safety agencies) (11)
Risk-based premiums policy
Data sharing
Education department
Include information about alcohol and its influences in school programmes
Monitor to ensure there are no alcohol points of sale or advertisements close to school
premises
Community road safety groups
Community education activity
Localisation of major social marketing campaigns
Citizen advisors/observers at alcohol checkpoints to help improve social acceptance
and ensure their integrity (relevant in jurisdictions where trust and confidence in
police is low)
Citizen advocacy groups
Promoting community-driven initiatives (see Box 7)
Producers, distributors and
retailers
Responsible marketing in the context of road safety server training and programme
sponsorship
On-premises education, awareness and social marketing campaigns
Road safety research authority
Problem identification
Programme evaluation
Generation and publication of evidence
Road authority
Road engineering treatments and maintenance
Vehicle speed and traic management policies
Employer
Company policies regarding drink driving
Employee education regarding drink driving
Promotion and enforcement of fleet safety management policies
Media
Communicating to the public about the drink driving situation in the country, and risks
of consuming alcohol and driving
Communicating about a national programme or campaign to reduce drink driving
Beverage alcohol licensing
authority
Licensed premises supervision
Responsible alcohol-serving policies and training
Restricting and/or banning alcohol advertisement/publicity
Source: (9)
Module 4 Implementing evidence-based drink driving interventions 57

As noted in Table 5, the alcohol industry – producers, distributors, and retailers – has a role to play. The
industry has funded and/or conducted initiatives that are claimed to reduce drink driving. However,
the research evidence does not support such claims (13). Additional information can be found in the
Fact Sheet produced by the Global Road Safety Partnership that provides a summary of research
evidence (13).
Conclusion
A review of the literature reveals that there is signicant investment by the alcohol industry in
activities that are claimed to be part of the industry’s corporate social responsibility initiatives.
However, the majority of initiatives supported by the alcohol industry are not evidence-based
and do not reduce alcohol-related harm. Most initiatives claimed under the banner of corporate
social responsibility serve as marketing opportunities for the alcohol industry in order to
maximise prot. Eective investment by the industry should focus on supporting evidence-
based interventions that demonstrably reduce alcohol-related harm; for example, through
commitments to a minimum alcohol pricing structure, and commitments to support reductions
in illegally traded alcohol (Anderson et al., 2009) rather than through alcohol marketing,
ineective drink driving control measures, and/or inuencing policy to maximise prot.
The commercial activities of the alcohol industry are in contradiction to those of the road safety
community. Most of the alcohol industry’s actions to reduce drink driving and improve road
safety lack evidence of eectiveness and/or have not been suciently studied. The industry
argues that they are, as the supporter of road safety CSR, a legitimate road safety actor and
therefore has a right to participate in road safety policy-making. However, as illustrated, it
is not a legitimate actor because its objectives are in direct conict with the evidence-based
objectives of the road safety community.
Hosted by
Alcohol Industry
3
The driving population’s knowledge of laws can be assessed through focus group discussions, interviews
(face-to-face, telephone, online) or surveys. When assessing community knowledge of drink driving
legislation and enforcement and the risks associated with drink driving, it is important to find out:
how well people understand the basis of the law, e.g. the BAC limit (where one applies), or the definition
of impaired driving where there is no set limit;
how well people understand how alcohol impairs judgement and the ability to drive a motor vehicle
safely;
how well people understand the relationship between drinking and the BAC limit, or the definition
of impaired driving, as appropriate;
people’s estimate of the probability of being detected if driving while impaired by alcohol;
how well people understand the punishments if convicted for drink driving, including fines and
disqualification, and the likely impact on their livelihood and social life;
perception of police and enforcement activities such as random alcohol checkpoints.
Information gathered through a survey, such as that outlined in Table 6, combined with information on
the respondent (e.g. age group, gender), can help identify target groups who may drink and drive. This
is useful information to plan and evaluate a drink driving intervention.
58 Drink driving: a road safety manual for decision-makers and practitioners
Table 6. Sample community survey on drinking and driving
Questions Possible responses
1. Do you know the BAC limit in your country? (If yes, check BAC value is correct)
Alternatively, if there is no BAC limit, the question could be: “Do you know the
legal definition for impaired driving in your country?”
1 yes (with correct or incorrect
value)
2 no
3 don’t know what BAC is
2. In your opinion, is operating a motor vehicle after consuming alcohol
dangerous?
1 yes
2 no
3 don’t know/unsure
3. In your opinion, does the consumption of alcohol before operating a motor
vehicle increase the risk of causing a road crash?
1 yes
2 no
3 don’t know/unsure
4. Have you consumed alcohol before operating a motor vehicle? 1 regularly
2 occasionally
3 no
4 don’t know/unsure
5. Have you travelled as a passenger in a motor vehicle with someone who has
consumed alcohol before driving?
1 regularly
2 occasionally
3 no
4 don’t know/unsure
6. In your opinion, what is the likelihood of being stopped by the police on
suspicion of drink driving?
1 high
2 moderate
3 low
4 don’t know/unsure
Source: (9)
Additional issues which may be explored as part of the general assessment include:
Operational issues
Are there agencies that are enthusiastic about the intervention and could act as “champions”?
Can the intervention be mounted with some agencies not involved initially?
Does the intervention require special training or equipment? Are these items available? What training
needs are there?
Does an intervention rely on new laws? If so, what lead times are required to prepare?
Do police have the capacity to enforce a new law?
Are key agencies prepared to coordinate their eorts?
Financial issues
What are the costs involved in financing an initiative?
What sources of funds are available for financing an initiative?
Is the scale of funding required for the intervention likely to be available? If not, is there potential for
a prior activity designed to generate funding?
Can a pilot scheme be established with available funds to show eectiveness?
Module 4 Implementing evidence-based drink driving interventions 59
Political issues
Are politicians aware of the problem?
Is there a need to sensitise them to the issues?
Will the intervention create community opposition? If so, how can this be addressed?
Are there political benefits which can be provided through the programme?
4.4 Opportunities and challenges in implementing drink
driving interventions
For maximum eectiveness, drink driving legislation needs strong support from politicians and high-
level community decision-makers, sending a clear message to society that tackling drink driving and
reducing road trauma are vital national issues (see Box 6 for examples from Brazil and France).
FORTALEZA, BRAZIL:
As a participating city in the Bloomberg Philanthropies Initiative for Global Road Safety (BIGRS 2015–2019),
the oices of the Mayor and the Municipal Department of Conservation and Public Services (SCSP) strongly
committed to expanding enforcement operations in the city of Fortaleza, in the State of Ceará, Brazil. They
ensured that coordination between municipal and state level enforcement agencies became a priority.
Following Article 25 of the National Traic Code, the SCSP and the Municipal Traic and Citizenship Authority
(AMC) established agreements with the State Highway Police (PRE), the Municipal Civil Guard (GCM), and
the State Military Police (PEM) to deliver joint drink driving enforcement operations as well as for other key
behavioural risk factors.
Several barriers were identified including: lack of coordination between enforcement bodies; traic oicers
mainly focused on traic flow (generally unaware of their role in saving lives); activities were not data-oriented
and did not follow standard operational procedures; and the general public did not recognise enforcement
as an instrument to prevent road trauma.
Records from Fortaleza show that an impressive 47.5% reduction in deaths attributable to road traic injuries
was achieved between 2014 and 2019 (14, 15), noting that the BIGRS 2015–2019 cross-cutting policies were a
major contributing factor to this success. From the perspective of traic law enforcement, three elements related
to road policing eorts were fundamental to achieving this outcome and changing the enforcement paradigm:
I. Political commitment from, and the eagerness of, the managerial level of the AMC to professionalise the
workforce, using evidence-based policing principles and deterrence strategies was crucial. The Global
Road Safety Partnership (GRSP) worked with local agencies to deliver capacity building support. This saw
the adoption of an internal training scheme and continuous roadside coaching and support. In the span
of five years, GRSP provided training to 1,700 oicers from the AMC, and its main enforcement partners–
PRE and GCM– across key behavioural risk factors and other areas of need (14). The programme was
delivered to selected members of the Federal Highway Police, the Criminal Police, and the Drink Driving
Dry law (Lei Seca) squad at the State Transport Department in Ceará (DETRAN Ceará). In addition, GRSP
further supported the AMC municipal police by providing breathalysers (active and passive), mouthpieces,
traic cones, and safety fences to ensure safe conduct of highly visible enforcement checkpoints.
II. A data-led, sustained operation to reduce drink driving, by a dedicated road safety squad was put in
place.The city of Fortaleza developed Standard Operating Procedures for Drink Driving enforcement and
other primary risk factors, which were published in the Oicial Gazette in 2016 (reviewed in 2018) (16).
Box 6. Political commitment assisted in reducing the number of crashes
60 Drink driving: a road safety manual for decision-makers and practitioners
In 2017, the AMC municipal police started using the ‘Enforcement reporting tool’ to record essential
information when conducting enforcement operations (time/place of operations; number of drivers tested,
refused to be tested, fined; and number of oicers and testing devices deployed per operation). These
developments allowed oicers to follow guidelines for strategic and safe operations, and to understand
their role in producing data and how it can be used to guide eective enforcement to save lives. This tool
was also allowed the local enforcement coordinator to track enhanced enforcement campaigns and bring
other agencies on board.
III. The most important achievement in the Fortaleza road policing
programme was the constitution of a dedicated squad with abilities
to continue performing enforcement operations through a multi-
agency approach to drink driving checkpoints. Led by AMC Traic
Police, this collaborative eort included five municipal, state and
national level agencies: the AMC Traic Police, State Highway
Police, Federal Highway Police, Fortaleza Municipal Guard, and
DETRAN Ceará. Together, the agencies planned and ran large-
scale Drink Driving enforcement operations at night on the main
arterial roads in Fortaleza, displaying a strong deterrent eect
at entry points, and on secondary streets and surrounding local
roads. The media activities (mass
+
and earned media) were an
essential supportive measure to increase the perceived risk of
detection and change the enforcement operation’s image among
the public.
This multi-agency approach was the culmination of four years of inter-
agency planning eorts which included: inter-sectorial committees
to share data and experiences; agreement established between AMC
and each of the four involved agencies; social marketing campaigns
with a focus on enforcement; and a rigorous training scheme of
refresher training sessions and in-situ coaching practice with police. These inter-agency collaborative
eorts saw checkpoints and alcohol tests increase dramatically: from 20,568 drivers invited to undertake a
breath test in 2017, to 106,366 in 2019 (or 103 per 1,000 drivers). The primary outcome was a reduction from
4.5% to 1.7% in the number of drivers who tested positive or refused to test between 2015 and 2019 (15). In
Brazil, the traic authority can legally fine drivers who refuse to submit to a breath test and can apply other
administrative penalties (such as driver license retention). The graph below contains information pertaining
only to drivers who tested positive during roadside observational studies.
+
Mass media campaign: https://www.
youtube.com/watch?v=Wlmf_3oJbOg
Photograph: Inter-agency
drink driving enforcement
checkpoint planning,
Fortaleza, Brazil.
Module 4 Implementing evidence-based drink driving interventions 61
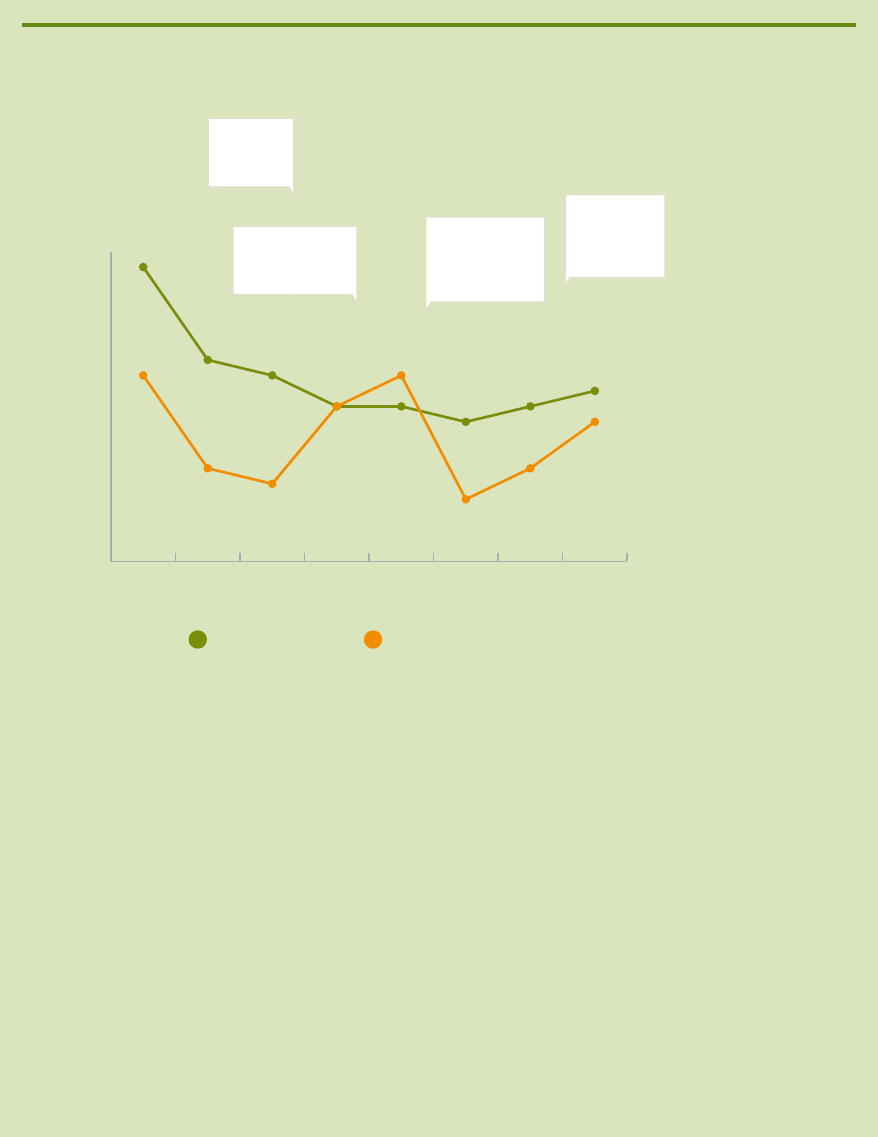
Figure 7. Percentage of drivers and motorcyclists who tested positive (2015–2019) during
observational data collections, Fortaleza, Brazil – excludes percentage of drivers refusing
to provide breath sample
0.0
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
1.8%
2.0%
Feb-Mar
2019
Jul-Sep
2018
Jan-Feb
2018
Jul-Sep
2017
Mar-Apr
2017
Aug-Sep
2016
Feb-Mar
2016
Oct-Nov
2015
1.2%
1.9%
1.3%
1.2%
1.0%
1.0%
1.0%
1.1%
0.6%
0.5%
1.0%
1.2%
0.6%
0.9%
0.4%
0.9%
All drivers
Motorcycle drivers
PERCENTAGE OF OBSERVED
DRINK DRIVING
DEC 2016
“Lei Seca”
enforcement
campaign
DEC 2018
“Do not risk.
Never drink and
drive” mass
media campaign
JUL 2017
First wave: “Se Beber, não
dirija” and “Lei Seca”
mass media campaign
NOV 2017
Second wave: “Se Beber,
não dirija” and “Lei
Seca” mass media
campaign
Source: (17)
Author elaboration with sources (14, 15, 16, 17).
FRANCE:
In 2002, French President Jacques Chirac publicly declared that road safety would be one of the three major
priorities of his presidential mandate. This type of political leadership is essential if diiculties with new,
harsher, legislation are to be overcome. Penalties for driving under the influence of alcohol were increased
and new laws were introduced.
France’s road safety performance over the period 2002–2004 was spectacular – road deaths decreased by
32%. This is attributed to a combination of measures, but focused particularly on speeding and alcohol-
impaired driving (18). With respect to alcohol-related crashes, measures included reducing the BAC level from
0.08 (set in 1978) to 0.05, and to 0.02 for bus drivers. Enforcement was increased; for example breath tests
were increased by 15%. Stricter sanctions were introduced, increasing penalty points from 3 to 6 for a BAC
between 0.05 and 0.08 (12 points lead to disqualification). As a result, alcohol-impaired driving decreased
dramatically – almost 40% fewer incidents in 2004 compared with 2003. One researcher attributed 38% of
the lives saved between 2003 and 2004 to improved behaviour in terms of alcohol-impaired driving (19).
Source: (9)
It is likely that any significant new drink driving intervention will generate a national debate. Such debate
should be supported (and amplified), since it will allow the arguments to be aired and the public to
be informed. Such promotions can be initiated by ministerial statements at conferences (political or
otherwise) or workshops to which the media can be invited. If the person championing the programme
is a high-profile celebrity, s/he could also be involved in the promotion as this can help to personalise
62 Drink driving: a road safety manual for decision-makers and practitioners
and de-politicise the campaign. Promotion is especially important at the start of any programme and
should be maintained. In many countries, ongoing promotion can be tied to local holidays or festivals.
Box 7 provides an example of how civil society can help legitimise and champion enforcement eorts.
The Challenge
In 2014, the Guanajuato State legislature approved the establishment of random alcohol checkpoints for
drivers. However, in areas like Guanajuato, where widespread distrust of the police exists, gaining public
support can be a challenge. In Guanajuato State, the proposed checkpoints in the city of León were initially
unpopular due to perceptions of road police operations. Given the public’s negative perceptions of police,
it was important that the police and the alcohol checkpoints be seen as legitimate and working to advance
public health. The Mexican Red Cross Society (MRCS) believed that, given their strong reputation in Mexico,
they could forge a partnership with the police that would encourage public acceptance, improve enforcement,
and save lives.
The Tactic
To aid in enforcement of the legislation, the MRCS’s Guanjuato State branch decided to oer their expertise
and volunteers to support police checkpoints. Working with the local police in León, the MRCS set up a
schedule that would begin in May 2014 and continue for a year, every weekend. Each checkpoint would
be “staed” by a team of MRCS volunteers working alongside police. The volunteers received introductory
training about drink driving and how the law was being implemented and enforced. To increase visibility, an
ambulance was stationed at checkpoints. The partnership was formally launched at a press conference to
“kick-o” the campaign, educate the public about drink driving statistics, and bring visibility to the initiative.
Speakers included representatives from government, police and traic agencies, as well as the Mexican Red
Cross. This diversity of voices confirmed to the public and the media that the eort was a united partnership
between government and civil society. Over the next year, the volunteer-staed checkpoints helped to
increase public support for the checkpoints. Other unexpected benefits included several cases in which
volunteers were able to provide first aid to police and drivers.
Summary
Strong enforcement of road legislation requires public and political support, and civil society can help to build
and maintain that support. In this case, Mexican Red Cross volunteers increased legitimacy of an enforcement
campaign and helped gain public support through a creative partnership with the government to save lives.
Source: (20)
Box 7. Forging an innovative partnership to increase effectiveness of Alcohol
Checkpoints in Guanajuato, Mexico– GRSP/ IFRC/ Mexican Red Cross
4.5 How to evaluate progress and use results for improvement
In general, monitoring the programme against the baseline data established prior to any road safety
intervention being put in place, involves keeping a close check on all measurement indicators, to
ensure the programme is on track towards the goals, to help refine programme delivery, and to
provide evidence for continuing support. Successfully sustaining a programme also requires that each
component is evaluated against the objectives to determine what worked and what did not. Evaluation
will not only provide feedback on programme eectiveness, but will also help to determine whether it
is appropriate for the target population, whether there are any problems with its implementation and
support, and whether there are any ongoing concerns that need to be resolved during implementation.
The results of this evaluation should be fed back into the design and implementation of future drink
driving enforcement activities.
Module 4 Implementing evidence-based drink driving interventions 63
The programme objectives are developed by examining the baseline data collected in the situational
assessment and may include:
reduction in alcohol-related crashes;
reduction in fatal injuries resulting from crashes involving drink driving;
reduction in the incidence of drink driving;
increase in level of community concern about drink driving;
increase in community support for initiatives to reduce drink driving;
increase in drivers and riders acting to change their drink driving behaviour;
increase in driver perception of stronger enforcement of drink driving laws.
Once the main problems are clear and the general objectives have been set, specific targets can be set.
The objective to decrease the incidence of drink driving, for instance, might be stated as “decreasing
the number of crashes caused by a driver impaired by alcohol by a specified amount, over a given time
period”. It is generally preferable to set measurable, time-limited objectives; these can be expressed in
terms of a target, for example, percentage reduction (or improvement) to be achieved by a certain date.
Having targets generally results in more realistic road safety programmes, a better use of public
funds and other resources, and greater credibility of those operating the programmes (21). A range of
targets for dierent objectives is outlined in Table 7 (the best range for a particular country will depend
on what information is available, or collectable). Performance targets should be developed in close
consultation with partner agencies that may be responsible for initiating action to achieve the targets.
Joint acceptance of targets is a critical requirement and is a key part of the coordination role required
of agency with primary responsibility for reductions in drink driving.
Table 7. Possible targets for drink driving programme objectives
Programme objective Example performance targets
Reduction in the number of
crashes involving drink driving
• Reduction in the number of fatal crashes involving at least one driver/rider with an
illegal BAC
• Reduction in the number of fatal crashes per registered vehicle involving at least
one driver/rider with an illegal BAC
Reduction in fatalities and
serious injuries resulting from
crashes involving drink driving
• Reduction in the number of killed riders and drivers with a recorded illegal BAC
• Reduction in the number of serious injuries occurring in crashes where an illegal
BAC has been recorded for at least one rider or driver
Reduction in the incidence of
drink driving
• Reduction in the proportion of drivers with an illegal BAC recorded at (standard)
random road checks
• Reduction in the proportion of drivers with an illegal BAC identified at police
random breath testing stations
Increase in level of community
concern about drink driving
• Proportion of population sample survey who identify drink driving as a crime or a
major community problem
Increase in community support
for drink driving initiatives
• Level of community support, measured in survey, for strong (or stronger)
enforcement and penalties for drink driving
Increase in drivers and riders
acting to change their drink
driving behaviour
• Number of drivers/ riders agreeing not to drink and drive in self-reported surveys
• Number of drivers/ riders using breath-alcohol testers prior to driving after drinking
• Proportion of population prepared to not drive if planning to drink in a social setting
Increase in driver perception of
stronger enforcement of illegal
alcohol laws
• Number of drivers/ riders believing enforcement activity is more extensive than
previously through survey
• Number of drivers/ riders charged with drink driving oences
Source: (22).
64 Drink driving: a road safety manual for decision-makers and practitioners
Once targets are set, performance indicators that will measure progress towards the target must be
agreed upon. Performance indicators are measures that indicate changes and improvements in areas
including:
legislation in place;
legislation being enforced – e.g. number of breath tests carried out;
number of convictions for illegal BAC levels;
proportion of drivers/riders above legal limit – from roadside surveys;
percentage of road crash victims admitted to hospital with illegal BAC levels;
numbers of police trained to use BAC equipment and the number of breath tests conducted;
public attitudes to drink driving – from surveys.
In order to show changes and improvements over time, these data need to be compared to the baseline
data, which need to be collected before the drink driving intervention is implemented. Comparing
changes in absolute numbers in injury and death outcomes, or in riders/drivers at a certain BAC level,
before and after a programme is of limited value, as absolute numbers may change because of an
increase or decrease in the number of riders and drivers, registered or otherwise, and the numbers of
breath or blood tests carried out. Therefore, it is important that rates be calculated. Denominators may
include number of drivers, registered vehicles, or kilometres travelled. For example, for injury outcomes, a
rate may be the number of drink driving injuries per licenced vehicle or licenced driver/rider, or number
of drink driving injuries per 100,000 km travelled. For alcohol intoxication rates, the appropriate rate
would be the proportion of drunk drivers/riders over the total number for which alcohol was measured.
Module Summary
It is critical to have a comprehensive understanding of the drink driving problem in your country or
region in order to design a relevant and eective programme.
To develop an understanding of the problem, a situation analysis should be undertaken that examines:
– crash and health data on road traic incidents involving alcohol;
–
laws pertaining to drink driving such as maximum BAC/BrAC levels for motorists, how these laws
are enforced, and why compliance with laws may be low;
– relevant stakeholders and their potential role in a programme aimed at deterring drink driving;
– drinking patterns and community perceptions of drink driving.
Interventions chosen should be relevant to the country’s specific drinking and driving situation.
Key factors that are essential for successful drink driving interventions:
– Assess available data to identify target groups
– Ensure drink driving laws are clear and enforceable
– Enforce laws fairly and firmly, with appropriate punishments
– Ensure that public information supports the law and its enforcement.
– Monitor and evaluate the intervention.
Module 4 Implementing evidence-based drink driving interventions 65
Drink driving interventions require high-level support which must be garnered from many dierent
agencies.
Evaluation should be seen as an integral component of any intervention; an evaluation plan needs to
be determined at the beginning so that a plan for data collection for this purpose is built into project
implementation.
It is important that evaluation results are shared with appropriate parties, and that they are used in
planning future interventions.
References Module 4
1.
Global Plan: Decade of Action for Road Safety 2021–2030. Geneva, Switzerland: World Health Organization,
2021. https://cdn.who.int/media/docs/default-source/documents/health-topics/road-traic-injuries/
global-plan-for-road-safety.pdf?sfvrsn=65cf34c8_33&download=true, Accessed on 24 January 2022.
2. De Silva MJ, Breuer E, Lee L, Asher L, Chowdhary N, Lund C, Patel V. Theory of change: a theory-driven
approach to enhance the Medical Research Council’s framework for complex interventions. Trials. 2014
Dec;15(1):1–3.
3. Rogers, P. Theory of Change, Methodological Briefs: Impact Evaluation 2. Methodological Briefsno. 2,
Florence, UNICEF. 2014. https://www.unicef-irc.org/publications/pdf/brief_2_theoryofchange_eng.pdf.
Accessed on 24 January 2022.
4. Anderson AA. The community builder’s approach to theory of change. A Practical Guide to Theory
Development. New York: The Aspen Institute. 2006. https://www.aspeninstitute.org/wp-content/uploads/
files/content/docs/rcc/rcccommbuildersapproach.pdf. Accessed on 24 January 2022.
5.
Global status report on road safety: time for action. Geneva, World Health Organization, 2009. https://apps.
who.int/iris/bitstream/handle/10665/44122/9789241563840_eng.pdf. Accessed on January 24 2022. (2).
6. Colchero MA, Guerrero-López CM, Quiroz-Reyes JA, Bautista-Arredondo S. Did “Conduce Sin Alcohol”
a Program that Monitors Breath Alcohol Concentration Limits for Driving in Mexico City Have an Eect
on Traic-Related Deaths?. Prevention science. 2020 Oct;21(7):979–84.
7. Houwing S, Stipdonk H. Driving under the influence of alcohol in the Netherlands by time of day and
day of the week. Accident Analysis & Prevention. 2014 Nov 1;72:17–22.
8. Vecino-OrtizAI,AllenKA,CuntoF, et al. PW 1092 Prevalence of behavioral risk factors for road traic
injuries in three south american cities. Injury Prevention2018;24:A66.
9. World Health Organization. Drinking and driving: a road safety manual for decision-makers and
practitioners. 2007.
10. World Health Organization. Strengthening road safety legislation: a practice and resource manual for
countries. World Health Organization; 2013.
11. Gaviria Fajardo R, Cruz Moreno P, Ponce de León Valdés, M, et al. Diagnóstico “Movernos Seguros”,
seguridad vial a través del seguro vehicular en América Latina y el Caribe. BID. División de Transporte.
VII. Título. VIII. Serie. IDB-TN-1803. 2019.
12. Hoe C, Taber N, Champagne S, Bachani AM. Drink, but don’t drive? The alcohol industry’s involvement
in global road safety. Health policy and planning. 2020 Dec;35(10):1328–38.
13. The Global Road Safety Partnership. Fact Sheet: Alcohol Industry [Internet] March 2021. https://www.
grsproadsafety.org/wp-content/uploads/Alcohol-Industry-Fact-Sheet-.pdf. Accessed 22 January 2022.
66 Drink driving: a road safety manual for decision-makers and practitioners
14.
Prefeitura de Fortaleza, Brasil. BIGRS Fortaleza. Reviewing progress and looking and the future. February
18 2019. [power point presentation]. Secretaria Municipal de Conservação e Serviços Públicos.
15. Prefeitura de Fortaleza, Brasil. Relatório Anual de Segurança Viária. Fortaleza 2019. https://vida.
centralamc.com.br/files/annual_reports/Relat%C3%B3rio%20Anual%20de%20Seguran%C3%A7a%20
Vi%C3%A1ria%202019.pdf. Accessed 30 January 2022.
16. Fortaleza (Brasil) Autarquia Municipal de Transito e Cidadania. AMC Manual de Procedimentos
Operacionais da AMC – MPO/AMC, Diário Oficial do Municipio. Portaria N° 1198/2016. https://
diariooficial.fortaleza.ce.gov.br/download-diario?objectId=workspace://SpacesStore/1a1c4cc9
-f89c-4c34-a440–3b418eeb19d8;1.1&numero=15884. Accessed 30 January 2022.
17. Five-year Report, 2015–2019. Fortaleza, Brazil. Baltimore: Johns Hopkins International Injury Research
Unit. Bloomberg Philanthropies Initiative for Global Road Safety. Baltimore: JH-IIRU; 2021.
18. World Health Organization.Alcohol and injury in emergency departments : summary of the report from
the WHO collaborative study on alcohol and injuries.World Health Organization 2007.https://apps.who.
int/iris/handle/10665/43581. Accessed 25 January 2022.
19. Gerondeau C. Road safety in France: reflections on three decades of road safety policy. London, FIA.
Foundation for the Automobile and Society, 2005.
20. Global Road Safety Partnership, Advocacy and Grants resource centre. December, 2015. https://www.
grsproadsafety.org/wp-content/uploads/NewCase-1cMexico.pdf. Accessed 25 January 2022.
21.
Elvik R. Quantified road safety targets – a useful tool for policy making? Accident Analysis and Prevention,
1993, 25:569–583.
22. World Health Organization. Drinking and driving: a road safety manual for decision-makers and
practitioners. 2007.
Module 4 Implementing evidence-based drink driving interventions 67

A

Appendix A. Suggested wording
for draft drink driving legislation
Section 1: Who must undergo a breath screening test
1. An enforcement oicer may require any of the following persons to undergo a breath screening
test without delay –
(a) a driver of, or a person attempting to drive, a motor vehicle on a road;
(b) a person whom the oicer has good cause to suspect has recently committed an oence against
this Act that involves the driving of a motor vehicle;
(c) if a crash has occurred involving a motor vehicle (i) the driver of the vehicle at the time of the
crash, or if the enforcement oicer is unable to ascertain who the driver was at the time of the
crash, a person whom the oicer has good cause to suspect was in the motor vehicle at the
time of the crash.
Section 2: Adult drink driving
Breath
1A. A person commits and oence if the person drives or attempts to drive a motor vehicle on a road
while the proportion of alcohol in the person’s breath, as ascertained by an evidential breath test,
exceeds 250 micrograms of alcohol per litre of breath.
Blood
1B. A person commits an oence if the person drives or attempts to drive a motor vehicle on a road
while the proportion of alcohol in the person’s blood, as ascertained from an analysis of a blood
specimen taken from the person, exceeds 50 milligrams of alcohol per 100 millilitres of blood.
Failing to remain or accompany
2A.
A person commits an oence if they fail or refuse to remain at the place where the person underwent
a breath screening test until after the result of the test is ascertained or fails or refuses to accompany
without delay an enforcement oicer to a place or places when required to do so for an evidential
breath test, blood test or both.
Failing to provide blood sample
2B.
A person commits an oence if the person fails to permit a blood specimen to be taken without delay
after having been required to do so by an enforcement oicer, medical oicer or health practitioner.
2C. It is a defence to proceedings for an oence against subsection 2B if the Court is satisfied, on the
evidence of a health practitioner, that the taking of a blood specimen from the defendant would
have been prejudicial to the defendant’s health.
Appendix A. Suggested wording for draft drink driving legislation 69
Penalty
3. If a person is convicted of an oence against subsection 1 or 2 –
(a) the maximum penalty is imprisonment for a term not exceeding 3 months or a fine not exceeding
$ (dependent on local average earnings); and
(b) the Court must order the person to be disqualified from holding or obtaining a driver licence for
6 months or more.
Section 3: Zero alcohol for under 20 / novice drivers
Breath
1A. A person younger than 20 commits an oence if the person drives or attempts to drive a motor
vehicle on a road while the person’s breath, as ascertained by an evidential breath test, contains
alcohol.
Blood
1B. A person younger than 20 commits an oence if the person drives or attempts to drive a motor
vehicle on a road while the person’s blood, as ascertained from an analysis of a blood specimen
taken from the person, contains alcohol.
Penalty
2. If a person is convicted of an oence against subsection 1 –
(a) the maximum penalty is imprisonment for a term not exceeding 3 months or a fine not exceeding
$ (dependent on local average earnings); and
(b) the Court must order the person to be disqualified from holding or obtaining a driver licence for
3 months or more.
Section 4: Drink or drug driving causing injury or death
1. A person commits an oence if the person drives a motor vehicle and causes injury to or the death
of a person while–
(a) the proportion of alcohol in the breath of the person, as ascertained by an evidential breath test
exceeds 250 micrograms of alcohol per litre of breath; or
(b) the proportion of alcohol in the blood of the person, as ascertained from an analysis of a blood
specimen, exceeds 50 milligrams of alcohol per 100 millilitres of blood; or
(c) the blood of the person, as ascertained from an analysis of a blood specimen, contains evidence
of the use of a qualifying drug specified in Schedule 1 of (could be this Act or a specific piece of
legislation addressing drug oences).
Penalty
2. If a person is convicted of an oence against subsection 1, –
(a) the maximum penalty is imprisonment for a term not exceeding 5 years or a fine not exceeding
$ (dependent on local average earnings); and
(b) the Court must order the person to be disqualified from holding or obtaining a driver licence for
1 year.
70 Drink driving: a road safety manual for decision-makers and practitioners

Global Road Safety Partnership
PO BOX 303
Chemin des Crêts 17,
1209 Genève, Switzerland
Email: [email protected]
Website: www.grsproadsafety.org
