Five Year Pediatric Use of a Digital Wearable Fitness Device:
Lessons from a Pilot Case Study
Kimayani D. Butte 1, 2
Amir Bahmani 2
Atul J. Butte 3
Xiao Li 2, 4 *
Michael P. Snyder 2 *
* These senior authors contributed equally.
1 The Harker School, 500 Saratoga Avenue, San Jose, CA USA 95129
2 Department of Genetics, Stanford University School of Medicine, Stanford, CA 94305
3 University of California, San Francisco, Mission Hall, 550 16th Street, 4th Floor, Box 0110,
San Francisco, CA USA 94158-2549
4 Division of General Medical Sciences, School of Medicine, Case Western Reserve University,
OH 44106
Corresponding Author:
Professor Michael P. Snyder
Stanford University School of Medicine
300 Pasteur Drive, M-344A
Stanford, CA 94305 USA
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice.
1
Abstract
Objectives: Wearable fitness devices are increasingly used by the general population, with new
applications being proposed and designed for healthy adults as well as adults with chronic
diseases. Fewer, if any, studies of these devices have been conducted in healthy adolescents
and teenagers, especially over a long period of time. The goal of this work was to document the
successes and challenges involved in 5 years of a wearable fitness device use in a pediatric
case study.
Materials and Methods: Comparison of five years of step counts and minutes asleep from a
teenaged girl and her father.
Results: At 60 months, this may be the longest reported pediatric study involving a wearable
fitness device, and the first simultaneously involving a parent and a child. We find step counts
to be significantly higher for both the adult and teen on school/work days, along with less sleep.
The teen walked significantly less towards the end of the 5 year study. Surprisingly, many of
the adult’s and teen’s sleeping and step counts were correlated, possibly due to coordinated
behaviors.
Discussion: We end with several recommendations for pediatricians and device manufacturers,
including the need for constant adjustments of stride length and calorie counts as teens are
growing.
Conclusion: With periodic adjustments for growth, this pilot study shows these devices can be
used for more accurate and consistent measurements in adolescents and teenagers over longer
periods of time, to potentially promote healthy behaviors.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
2
Background and Significance
Wearable fitness devices are increasingly used by the general population. A recent study
estimates that 19% of Americans currently use a wearable fitness device
1
and an additional 15% of Americans stated they no longer used a fitness tracker, which raises a
question on their long-term use. Forty million new wearable devices were sold in 2017
2
, and
the company Fitbit sold approximately 13.5 million new Fitbit devices in 2019
3
.
While many consumers likely use these devices to track general health and wellness
parameters, there have been several attempts to discover medical utility for these devices.
Gresham, et al, recently showed in a study of 37 patients with cancer that wearable fitness
devices could accurately capture stair climbing and steps with enough accuracy to correlate with
traditional performance status measures assessed by health providers
4
. Similarly, Speier, et.
al., showed that wearable fitness devices could be very useful in monitoring a patient’s health
remotely in order to diagnose health problems more quickly
5
. The study was conducted for only
90 days with 186 participants with ischemic heart disease. Li, et. al., demonstrated that fitness
trackers can detect illnesses caused by infectious diseases such as Lyme and respiratory viral
infections as well as other health conditions
6
. Finally, Rose, et. al., have used fitness trackers to
detect heart conditions, such as atrial fibrillation
7
.
One of the longest studies on the use of wearable fitness devices was by Jakicic, et al, who
studied their utility for weight loss in young adults (ages 18 to 35 years)
8
. The study
randomized 471 participants, of which 351 were still with the study and provided their updated
weights at 24 months. The study showed a significant decrease in weight over time, but
surprisingly with less weight loss in the intervention group using the wearable fitness devices.
Also interestingly, nearly a quarter of the participants did not complete the study over 2 years.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
3
Despite these setbacks, the research use of wearable fitness devices is forecast to continue to
expand, with over 500 biomedical publications specifically mentioning Fitbit. With the flagship
NIH All of Us Research Program studies now adopting wearable fitness data along with
electronic health record data and genomic data, research using these devices is likely to
increase
9
.
To date, the vast majority of research on wearable fitness devices has been conducted in
adults. Fewer studies have been performed in the pediatric population, though companies are
now targeting sales growth of digital wearable devices in this population
10
. The few pediatric
studies that have been performed have targeted cohorts with specific diseases. Bian et al
looked at self-reported sleep quality from 22 participants with asthma as well as self-reported
symptoms of asthma, and compared the reports to the participants’ Fitbit data to show that Fitbit
sleep quality is lower when more asthma symptoms occur
11
. Voss, et al., conducted a study
with 40 participants ages 10-18 with congenital heart disease. The study assessed the validity
of the Fitbit step count by testing the wrist-worn Fitbit Charge HR against the hip-worn
ActiGraph accelerometer and found that the Fitbits recorded more steps than the accelerometer
12
. The study also found that daily Fitbit step counts of over 12,500 steps would meet commonly
promoted physical activity guidelines of over 60 minutes of activity per day. A similar study by
Miropolsky, et al., on 13 young adult cancer survivors between ages 20 and 39 years suggested
a Fitbit device could provide major motivation to engage in physical activity
13
.
Studies on healthy adolescents and teenagers have been even more rare. Kerner, et al. studied
one-hundred participants from two schools using Fitbit devices for 8 weeks, along with the Fitbit
app. They found using Fitbits can initially encourage adolescents (ages 13-14) to exercise, but
the participants were eventually discouraged potentially because Fitbit might be setting
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
4
unrealistic goals
14
. The non-personalized goal of 10,000 steps per day made participants feel
unmotivated and lazy if they did not achieve that goal, which discouraged them from exercising
14
. Also, the competitive aspect of the Fitbit app, such as the leaderboard rankings for who got
the most steps, discouraged those who did not get many steps and sometimes demotivated the
participants who participated in exercise just to get more steps than they usually do. Finally, the
authors did not report on the actual success rate of how many students used the Fitbit for the
full 8 weeks.
These studies show that using a wearable fitness device could be useful for tracking some
health indicators from pediatric-aged individuals, without needing regular physician evaluation.
Almost all of these studies involved the participants using devices for 8 weeks or fewer, a period
too short for many health indicators to significantly improve. Health benefits from wearable
fitness devices might be expected to require longer-term use which could lead to new
discoveries in long-term health effects of exercise on medical conditions and general health.
Objectives
The goal of this work was to document the successes and challenges involved in 5 years of a
wearable fitness device use in a pediatric case study. The findings from this study may have
implications for both encouraging healthy behavior in adolescents as well as recommendations
for wearable device manufactures to improve adoption by adolescents and adults.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
5
Materials and Methods
Ethics: Two authors (including the lead author) collected their own data as citizen-scientists,
with their own devices that they obtained commercially through Amazon.com, initiated the
analyses, then approached the Stanford investigators to enhance the analyses, and both of
these authors contributed to writing this manuscript. This citizen-science research project was
initiated outside of an academic institution, was run by the two authors with their own data, had
no Federal funding, and the research is not related to an FDA or EPA-regulated product, so as
such does not need to undergo Institutional Review Board review, as per Resnik
15
.
Regardless, the two data contributors joined Stanford University research protocol 56378
approved by the Stanford University Institutional Review Board, specifically allowing participants
at or over age 13 years to share their past and current Fitbit measurement data with Stanford
investigators for research purposes, with informed consent.
Two Fitbit One devices were purchased on January 1, 2013 and activated shortly thereafter.
The Fitbit One was designed to track steps walked along with pace, stairs climbed, sleep
duration and activity. Two participants (and co-authors here) simultaneously started to use the
devices to track these measurements. The female participant started use at age 10 years and 4
months, and continued through her teenage years. The adult male participant (father of the
younger individual) started use at age 43 years and 9 months. Neither had any significant prior
medical history at the initiation of use. Both intended the use of these devices for improving and
maintaining general health and wellness. The adult also intended to use the device to increase
his walking and help in weight loss. While these devices (or their subsequent versions) have
still been in use since January 1, 2013, this analysis only covers the 60 months of use after a
pattern of regular consistent use was seen, starting on June 1, 2013. In June 2018, both
participants elected to study their data together for research.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
6
Fitbit enables the downloading of raw level device data, by registering through their Application
Programming Interface (API). Using the API ID number that Fitbit provided, a short program
was written in R to access the Fitbit data, serially downloading blocks of daily step and sleep
data representing every 100 days, to cover the entire 60 months. No outlier measurements
were removed. Sleep amounts in minutes are assigned to the wake up day. Weekend nights
were defined as those leading into a Saturday or Sunday, which are days with no school.
School days were defined as weekdays that were not within a set of five long holiday breaks:
one week mid-winter break in February, one week spring break in March or April, ten week
summer break in June-August, Thanksgiving one week break in November, and two week
winter break between December and January.
Height data for the teen, needed to calculate stride length, was downloaded from her own
electronic medical records, with height measurements made and documented by a physician
assistant or pediatrician.
Analysis was performed using Google Sheets, Minitab Express, R [version 4.0.2 (2020-06-22)],
and RStudio [version 1.3.1073]. R packages used include ggplot2 [version 3.3.2], tidyverse
[version 1.3.0], and corrr [version 0.4.2].
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
7
Results
We wanted to examine the patterns and challenges associated with long term adolescent use of
wearable fitness data. Sixty months of step and sleep data, collected from the Fitbit wearable
fitness devices of a father and daughter (Table 1) were downloaded and analyzed. School for
the teen and work for the adult was generally in session from Monday morning through Friday
afternoon and the teen’s school year consistently ran from late August to early June. For the
first year of the study, the teen had to was required to complete a “mile run” once per year. In
the subsequent 3 years in middle school, the teenager was required to complete a “mile run”
once every month. In the final year of the study (which was during high school), there were no
daily physical education classes, only lower intensity yoga without mandatory walking or
running.
[Table 1 inserted here]
The teen was noted to have more missing measurements than the adult, including a 193 day
gap in measurements in 2016. However, more than 85% of the possible 1826 days of step
counting were available for both individuals. Fewer sleep measurements were made than step
measurements by both individuals, likely due to the need to remember to manually activate and
deactivate the Fitbit One sleep timer before and after sleeping.
[Figure 1 inserted here]
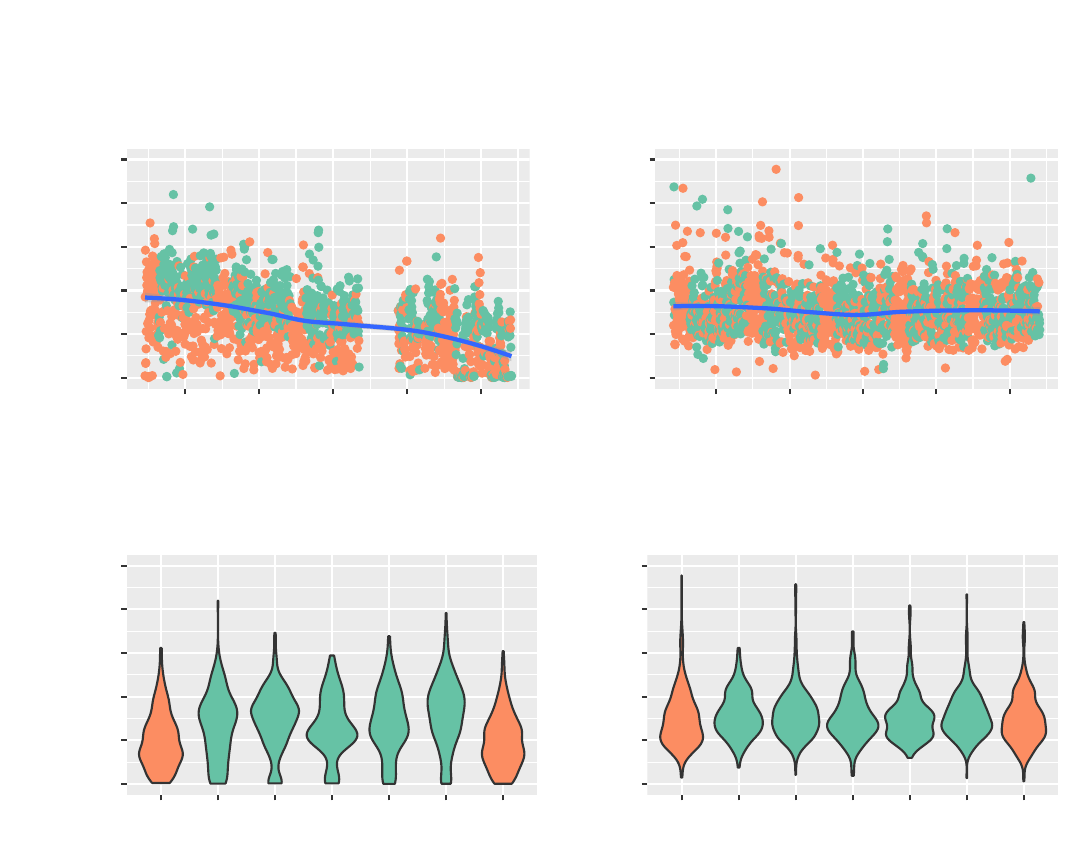
With over 1500 days of step counts available for both individuals, some clear differences are
notable. For the teen, step counts significantly dropped over the five years (Figure 1A, negative
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
8
correlation of date versus steps r = -0.517, p = 1.20 x 10
-107
), whereas step counts only slightly
dropped the same period for the adult (Figure 1B, negative correlation of date versus steps r = -
0.066, p = 0.005). On average, the adult walked significantly more steps than the teen over the
5 years (adult mean 7757.2, standard deviation 2850.7; teen mean 6568.3, standard deviation
3685.9, t-test p < 2.2 x 10
-16
). Interestingly, both individuals walked significantly less on
weekend days (Sundays and Saturdays) than on weekdays, but the difference was more
pronounced in the teen (Figure 1C and 1D, teen t-test p < 2.2 x 10
-16
, adult t-test p = 0.006).
[Figure 2 inserted here]
We further investigated the teen’s step counts. Using six years of school calendars, we
determined the specific dates of five yearly recurring holidays (one week mid-winter break in
February, one week spring break in March or April, ten week summer break from June through
August, Thanksgiving one week break in November, and two week winter break from between
December and January). Approximately 30% of the available step count measurements could
be classified as occurring during one of these holidays (teen: 472 of 1566 measurements; adult:
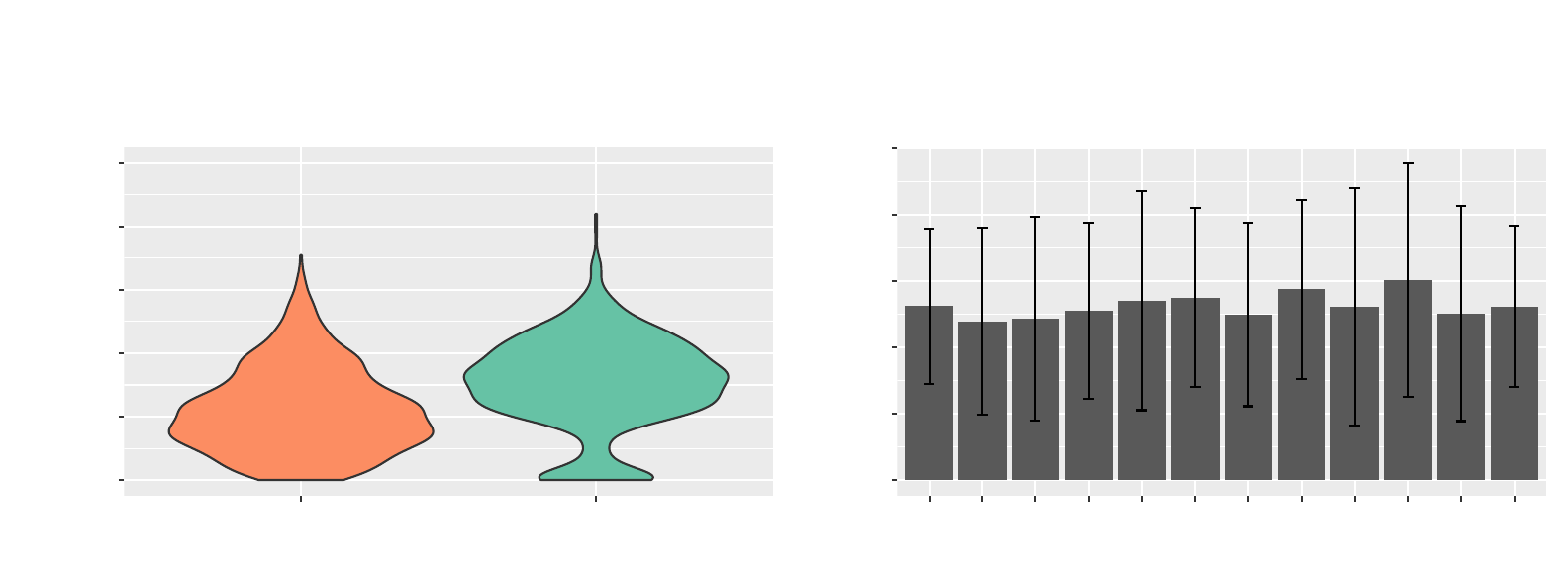
571 of 1823 measurements). The teen walked significantly more on school days compared to
non-school days (combining holiday and weekend days, Figure 2A, 2105.9 more steps on
average, t-test p = 8.17 x 10
-31
). Interestingly, the adult showed no significant difference in step
counts between school days and non-school days. The teen made fewest steps in February
and March compared to August through October (Figure 2B), and there was significant
variability in the steps across the months (Chi-square test p = 3.71 x 10
-67
). To test the effect of
seasonality, we fit a linear regression model on the teen’s step counts, with parameters
representing whether a day was a weekend, in one of the five holiday periods, the year of the
study (first through fifth), and the month of the year. All of these parameters were highly
significant in the fit regression model (Table 2).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
9
[Table 2 inserted here]
On average, the teen walked 9103.1 steps per day during the first year of the study, and only
3646.8 steps per day during the final year of the study, or a drop of 60%. The increasing
heights for the growing teen were used to better understand the context for this marked drop in
step counts. Fourteen height measurements were downloaded for the teen, with measurements
available between ages 2 and 16 years. A cubic spline was then fit to these measurements,
and a height of 144.9 cm was estimated for the teen on June 1, 2013, the starting date for this
study. A height of 162.6 cm (measured close to the date) was used for May 31, 2018, the
ending date for this analysis. The teen’s height is estimated to have increased 17.7 cm (or
12.2%) during the analysis period of this study, and thus only a 12.2% increase in stride length
over the course of the study
16,17
.
[Figure 3 inserted here]
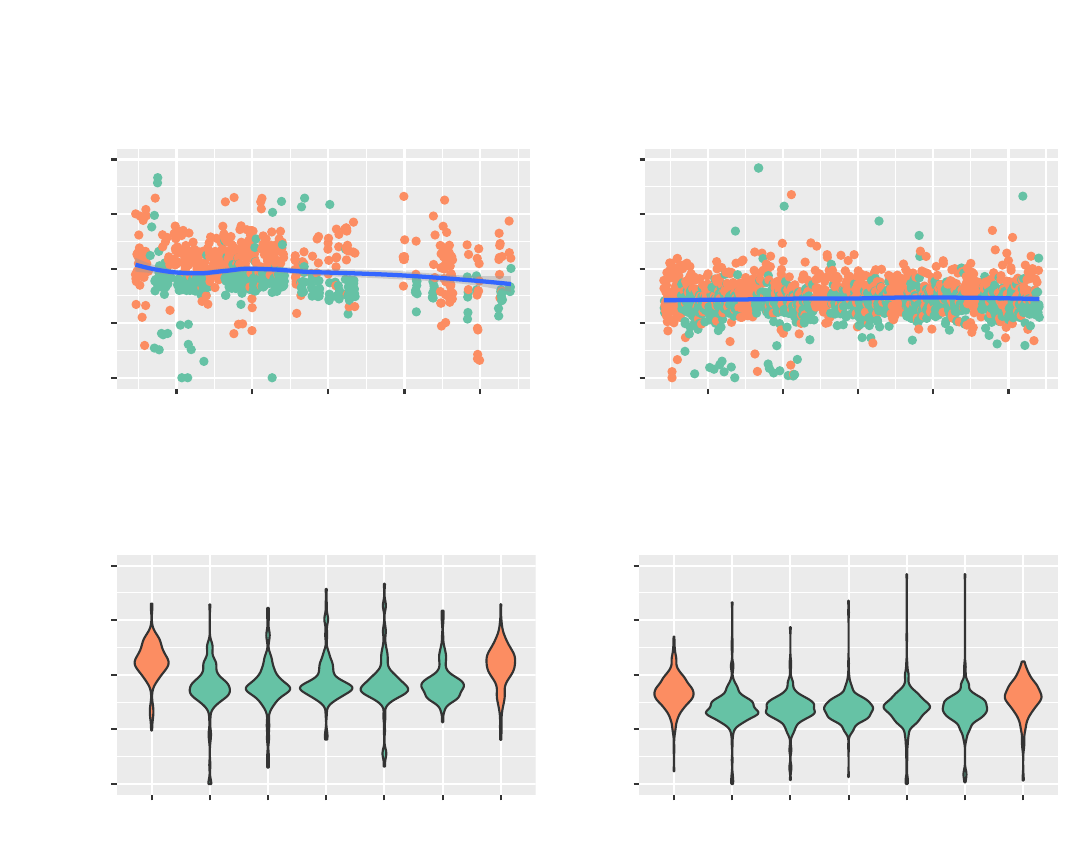
Fewer days of sleep measurements were available for both individuals, but comparisons were
still possible with over 800 nights of data available. The teen slept slightly less towards the end
of the 5 years, compared to the start (Figure 3A, correlation of date versus minutes asleep r = -
0.10, p = 0.003). The adult showed no significant change in sleep over the 5 years (Figure 3B,
correlation of date versus minutes asleep r = 0.036, p = 0.152, not significant). Similar to the
step counts, differences were observed on weekends. Both individuals slept significantly longer
over nights when the morning fell on a weekend day. The teen slept an average of 92.7
minutes longer in weekends (Figure 3C, green weekday mean 457.3, orange weekend mean
550.0, t-test p = 7.23 x 10
-29
) whereas the adult slept 61 minutes longer (Figure 3D, green
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
10
weekday mean 345.5, orange weekend mean 406.3, t-test p = 1.5 x 10
-36
). Overall, the teen
slept an average of 120.1 minutes longer per day than the adult.
[Figure 4 inserted here]
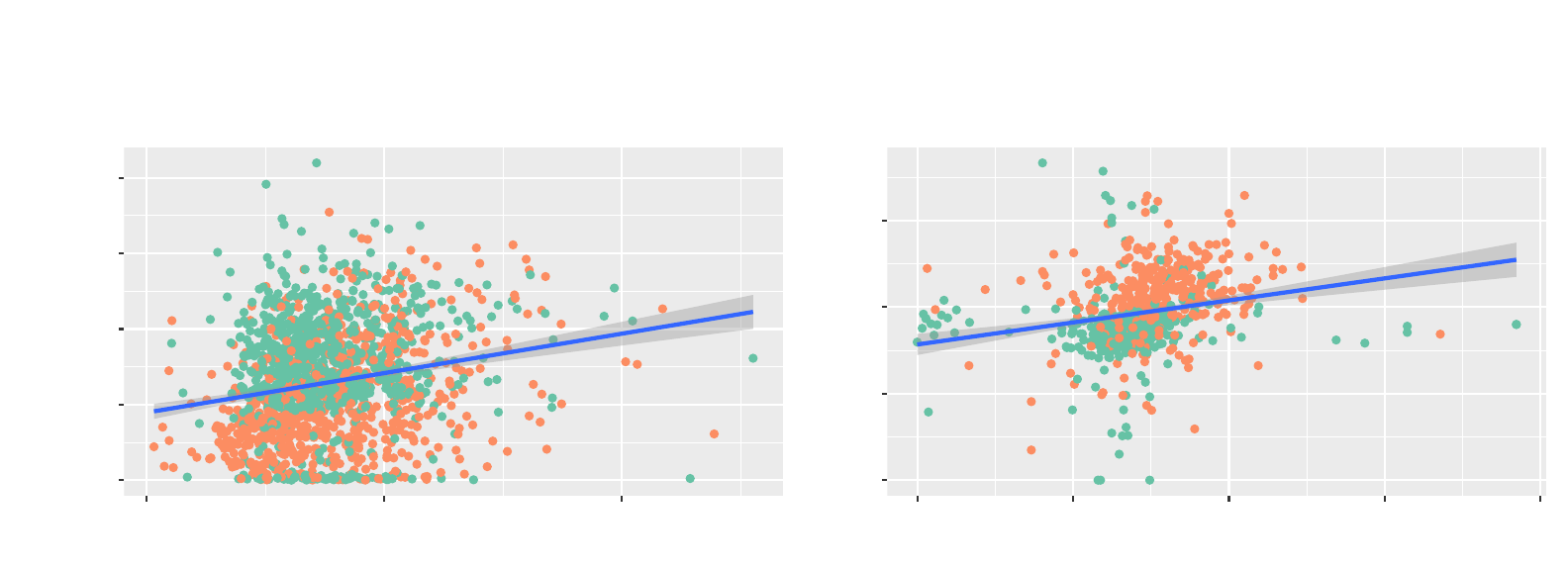
Given the father and daughter living as a family in the same home, we then compared step
counts and sleeping on the same days. Surprisingly, the number of steps walked by the teen
and adult were correlated (Figure 4A, n = 1589 points, Pearson r = 0.2, p = 4.92 x 10
-16
). The
step count correlation was even stronger when considering only the weekend days (n = 449
points, Pearson r = 0.4, p = 1.25 x 10
-18
), suggesting coordinated walking behaviors on the
weekend. Interestingly, the amount of sleep was also correlated between the father and
daughter (Figure 4B, n = 707 points, Pearson r = 0.23, p = 1.32 x 10
-9
), but much weaker when
considering only the weekend days (n = 189 points, Pearson r = 0.17, p = 0.023), suggesting
the daughter’s and father’s sleep were less coordinated on the weekends. In general, both the
teen and adult slept more and walked less on non-school days (Figure 4A and B, in orange)
than on school days (green).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
11
Discussion
We describe here a 5-year longitudinal case study of a wearable fitness device in a teenage
female, comparing these measurements to her adult father, using the same type of device
during the same time period. To our knowledge, this is the longest reported pediatric study
involving a wearable fitness device, and the first simultaneously involving a parent and a child.
We describe five specific findings here. First, the teen appears to be generally walking less
than the adult (who was purposefully trying to walk more for weight loss), and progressively
walking less during the 5 years. Second, both the adult and teen walk significantly less on
weekends and holidays. Third, the teen female sleeps more than the adult and has more
variation in sleep, but both the teen and adult sleep more on weekends. Fourth, on average,
the teenager slept more than the adult. Sleep differences may have been due to travel by the
adult and/or the fact that short naps are often not recorded by these devices, which needed
manual triggers to start the timer. Fifth, interestingly, the number of steps walked and minutes
slept by the teen and adult are correlated. The correlation in step counts may be due to
common activities (e.g. shopping) or longer walks (e.g. hikes) performed together as a family.
Similarly, sleep correlations were likely due to shared behavior: if the teen worked late to
complete homework, one of the two parents often stayed awake with her.
While we have shown that device use for more than 5 years is possible, we note special efforts
that could be taken to enhance continued accurate use in the pediatric setting. First, the
number of steps needed to traverse a distance obviously depends on the stride length. If an
exact stride length is not entered, Fitbit estimates the length given the sex and height of the user
18
using a proprietary formula, which is multiplied by the step count to estimate the distance
walked. However, teenagers gain significant height as they go through puberty, and if the stride
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
12
length is not periodically readjusted, a shorter total distance walked may be misestimated. For
example, an average 10-year-old female at the 50%ile for height at 138 cm would have an
estimated stride length of 57 cm, while the same female 5 years later at the 50%ile for height at
162 cm would have an estimated stride length of 67 cm or 17.5% longer
17,19,20
. Thus, 5000
steps walked at age 15 years cover 2.08 miles, whereas 5000 steps for a 10-year-old would
cover 1.77 miles. However, in this study, we show that the 60% decrease in step counts seen
over the five years greatly exceeds the teen’s 12.2% estimated increase in stride length.
Given that teenager heights change over time, if the teen does not know (or remember) to
periodically change their height in the settings, then the Fitbit may miscalculate the number of
steps and thus distance walked. Similarly, the nutritional needs of teenagers change over time,
and if teens are using calorie counting or diet-related features, the nutritional goals will need to
be periodically adjusted to keep the advice safe and accurate. The device itself should
periodically prompt for such updates, perhaps on the teen’s birthday.
In addition, if teenagers are visiting their primary care physician for regular preventative health,
the physician could remind or offer to update these body-related settings. But currently, most
pediatricians do not have any easy access to the data from the wearable fitness devices of their
patients. Ideally, they would have the data and tools to help provide targeted fitness advice
(e.g. make sure to walk more on weekends), beyond just adjusting the settings.
Despite the obviously small sample size, it is still possible to draw some early conclusions to
potentially inform recommendations. We noted several other issues for wearable device use in
the pediatric age range. The teenage female had a contiguous gap in measurements of 7
months. For many years, there was no reminder or warning issued when measurements were
not being synchronized from the device. This could easily happen if the synchronization device
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
13
(i.e. a smartphone or tablet or home computer) is upgraded or restored from a backup.
Measurements will be lost if devices are not synchronized periodically. For the Fitbit One used
here, the on-device memory only stores 30 days of measurements
21
. Users should ideally
receive a warning if device measurements have not been synchronized to their phones after
several days. Fitbit reportedly made an improvement to address this problem in March 2018
22
.
However, to our knowledge, parents still do not get notifications when their child’s device is not
syncing. This should be addressed before long term pediatric use is recommended.
Similarly, teens (or potentially even younger users) will need to remember to periodically charge
the device. This habit is harder to adopt, as these devices are worn while sleeping, when other
devices (such as phones) are typically charged. Alternative times for consistent charging merit
exploration (e.g. while bathing). If the teen has different devices to track steps and sleep, each
device will need to be charged when it is not in use.
In this study, we noted the teenager completed fewer steps than the adult. This may be due to
a deliberate effort of the adult deliberately to walk at his workplace, whereas the teenager sits in
the classroom for most of the day and only walked between classes. However, we noted both
individuals walked more during these school/workdays compared to weekend days or holidays.
Employers and schools could design layouts that enhance walking activity during the day.
School course schedules are difficult to arrange logistically, but consecutive classes could be
separated away from each other on campus, thereby requiring students to walk more between
classes. In the workplace, conference calls via mobile devices could be encouraged, thus
potentially enabling walking during the calls.
The motivating factors used by the companies making wearable fitness devices can also be
tailored for teens. Smartphone-based reminders to exercise could be tailored around
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
14
teenagers' unique schedules, with bursts of activity potentially clustered around sports
schedules and with periods of less exercise during exam periods.
Anecdotally, the teen started to use the Fitbit One device because she saw her father, the adult
in this study, using his device, and because she wanted to be healthier. The prime reason she
used the device was to measure her sleep each night, as she could not easily estimate it just by
looking at a clock. She could also look at the Fitbit app to see how often she woke up during the
night and judge her sleep quality. Instead of relying on qualitative assessments of her lifestyle,
she could get quantitative assessments for both her exercise and sleep. As a separate reason,
she also used her device because she could see her step count change over time. For example,
she could see when she was walking fewer steps per day in middle and high school than she
had walked in elementary school. However, the step count was not the primary motivator for
continued use of the device. She continued use of the device it because it was easy to
integrate into her lifestyle and did not disrupt her daily routine. She developed a habit of
charging the device when bathing.
There are several limitations to this study. Obviously, only two individuals were studied here.
Others have already been listed above, such as some missing data due to the lack of any
device-issued warning. Fewer days of sleep measurements were made, compared to step
counts. The Fitbit One needs to be worn while in bed, and requires a button to be manually
held down as one is ready to sleep. The same button must then be held down right after waking
up to stop the timer. It was common for both individuals to forget to perform either of these two
manual steps. A more automated way to determine sleep start and end would be ideal and
would enhance accuracy. It is possible that some of these missing measurements might have
biased the analysis, if the data were not missing at random.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
15
Conclusion
Regardless of the limitations, this pilot case study shows that wearable fitness devices can be
useful in tracking the long-term health of both adults and teenagers, and we hope to see more
studies conducted on the long-term use of these devices.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
16
Acknowledgements
We would like to thank The Harker School for providing the Minitab Express software that was
used in analyzing the data. We would also like to thank Chris Spenner (Harker School) for
research mentorship and Dr. Tarangini Deshpande (NuMedii, Inc.) for comments on the
manuscript.
Author contributions
Conceptualization, K.D.B., A.J.B., and M.P.S.; Software, A.J.B.; Analysis, K.D.B., A.B., X.L.;
Resources, M.P.S.; Writing, K.D.B., A.J.B., X.L., and M.P.S.; Visualization, K.D.B., and A.J.B.;
Supervision, X.L., and M.P.S.
Competing interests
Michael Snyder is a cofounder and is on the scientific advisory board of Personalis, Filtircine,
SensOmics, Qbio, January, Mirvie, Oralome, and Proteus. He is also on the scientific advisory
board of Genapsys and Jupiter. Atul Butte is a co-founder and consultant to Personalis and
NuMedii; consultant to Samsung, Mango Tree Corporation, and in the recent past, 10x
Genomics, Helix, Pathway Genomics, and Verinata (Illumina); has served on paid advisory
panels or boards for Geisinger Health, Regenstrief Institute, Gerson Lehman Group,
AlphaSights, Covance, Novartis, Genentech, Merck, and Roche; is a shareholder in Personalis
and NuMedii; is a minor shareholder in Apple, Facebook, Alphabet (Google), Microsoft,
Amazon, Snap, 10x Genomics, Illumina, CVS, Nuna Health, Assay Depot, Vet24seven,
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
17
Regeneron, Sanofi, Royalty Pharma, AstraZeneca, Moderna, Biogen, Paraxel, and Sutro, and
several other non-health related companies and mutual funds; and has received honoraria and
travel reimbursement for invited talks from Johnson and Johnson, Roche, Genentech, Pfizer,
Merck, Lilly, Takeda, Varian, Mars, Siemens, Optum, Abbott, Celgene, AstraZeneca, AbbVie,
Westat, and many academic institutions, medical or disease specific foundations and
associations, and health systems. Atul Butte receives royalty payments through Stanford
University, for several patents and other disclosures licensed to NuMedii and Personalis. Atul
Butte’s research has been funded by NIH, Northrup Grumman (as the prime on an NIH
contract), Genentech, Johnson and Johnson, FDA, Robert Wood Johnson Foundation, Leon
Lowenstein Foundation, Intervalien Foundation, Priscilla Chan and Mark Zuckerberg, the
Barbara and Gerson Bakar Foundation, and in the recent past, the March of Dimes, Juvenile
Diabetes Research Foundation, California Governor’s Office of Planning and Research,
California Institute for Regenerative Medicine, L’Oreal, and Progenity. The other authors
declare no competing interests.
Data Availability
The sleep and step count data for the adult and teen used in this analysis are publicly available
through Github: https://github.com/kimibutte/Fitbit-Data.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
18
References
1. Mccarthy, J. One in Five U.S. Adults Use Health Apps, Wearable Trackers. Gallup
https://news.gallup.com/poll/269096/one-five-adults-health-apps-wearable-trackers.aspx
(2019).
2. Pressman, A. Apple Took a Commanding Lead In Wearables In the Fourth Quarter, As Fitbit
Slipped. Fortune https://fortune.com/2018/03/01/apple-watch-fitbit-wearable-ranking/ (2018).
3. Fitbit. Fitbit Reports Third Quarter Results for the Three Months Ended September 28, 2019.
https://investor.fitbit.com/press/press-releases/press-release-details/2019/Fitbit-Reports-
Third-Quarter-Results-for-the-Three-Months-Ended-September-28-2019/default.aspx (2019).
4. Gresham, G. et al. Wearable activity monitors to assess performance status and predict
clinical outcomes in advanced cancer patients. Npj Digit. Med. 1, 27 (2018).
5. Speier, W. et al. Evaluating utility and compliance in a patient-based eHealth study using
continuous-time heart rate and activity trackers. J. Am. Med. Inform. Assoc. 25, 1386–1391
(2018).
6. Li, X. et al. Digital Health: Tracking Physiomes and Activity Using Wearable Biosensors
Reveals Useful Health-Related Information. PLoS Biol. 15, e2001402 (2017).
7. Schüssler-Fiorenza Rose, S. M. et al. A longitudinal big data approach for precision health.
Nat. Med. 25, 792–804 (2019).
8. Jakicic, J. M. et al. Effect of Wearable Technology Combined With a Lifestyle Intervention on
Long-term Weight Loss: The IDEA Randomized Clinical Trial. JAMA 316, 1161 (2016).
9. Fitbit. National Institutes of Health Launches Fitbit Project as First Digital Health Technology
Initiative in Landmark All of Us Research Program. https://investor.fitbit.com/press/press-
releases/press-release-details/2019/National-Institutes-of-Health-Launches-Fitbit-Project-as-
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
19
First-Digital-Health-Technology-Initiative-in-Landmark-All-of-Us-Research-
Program/default.aspx (2019).
10. Fitbit. Fitbit Launches Fitbit Ace, Inspires Healthy Habits for Kids and Makes Fitness Fun
for the Whole Family. https://investor.fitbit.com/press/press-releases/press-release-
details/2018/Fitbit-Launches-Fitbit-Ace-Inspires-Healthy-Habits-for-Kids-and-Makes-Fitness-
Fun-for-the-Whole-Family/default.aspx (2018).
11. Bian, J. et al. Exploring the Association Between Self-Reported Asthma Impact and
Fitbit-Derived Sleep Quality and Physical Activity Measures in Adolescents. JMIR MHealth
UHealth 5, e105 (2017).
12. Voss, C., Gardner, R. F., Dean, P. H. & Harris, K. C. Validity of Commercial Activity
Trackers in Children With Congenital Heart Disease. Can. J. Cardiol. 33, 799–805 (2017).
13. Miropolsky, E. M. et al. Participant Perceptions on a Fitbit and Facebook Intervention for
Young Adult Cancer Survivors: A Qualitative Study. J. Adolesc. Young Adult Oncol. 9, 410–
417 (2020).
14. Kerner, C. & Goodyear, V. A. The Motivational Impact of Wearable Healthy Lifestyle
Technologies: A Self-determination Perspective on Fitbits With Adolescents. Am. J. Health
Educ. 48, 287–297 (2017).
15. Resnik, D. B. Citizen Scientists as Human Subjects: Ethical Issues. Citiz. Sci. Theory
Pract. 4, 11 (2019).
16. Grieve, D. W. & Gear, R. J. The Relationships Between Length of Stride, Step
Frequency, Time of Swing and Speed of Walking for Children and Adults. Ergonomics 9,
379–399 (1966).
17. Bumgardner, W. How to Set Your Pedometer or Fitness Band for Better Accuracy.
VeryWell Fit https://www.verywellfit.com/set-pedometer-better-accuracy-3432895 (2020).
18. Fitbit. How does my Fitbit device calculate my daily activity?
https://help.fitbit.com/articles/en_US/Help_article/1141.htm.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
20
19. The Relationships Between Length of Stride, Step Frequency, Time of Swing and Speed
of Walking for Children and Adults: Ergonomics: Vol 9, No 5.
https://www.tandfonline.com/doi/abs/10.1080/00140136608964399.
20. Centers for Disease Control and Prevention & National Center for Health Statistics. CDC
growth charts. http://www.cdc.gov/growthcharts/ (2000).
21. Fitbit. Fitbit One Product Manual. (2009).
22. Fitbit. Sync Service Persistent Notification. https://community.fitbit.com/t5/Ionic/Sync-
Service-Persistent-Notification/td-p/2612466 (2018).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
21
Figure Legends
Figure 1: A. and B. Steps per day over time for the teenager and adult, respectively, with green
representing school days and orange as non-school days (i.e. weekends and weeklong
holidays). C. and D. Steps per day on each day of the week for the teenager and adult,
respectively, with green representing weekdays and orange as weekends (Saturday and
Sunday).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
22
Figure 2: A. Distribution of steps per day for the teenager on school days (green) and non-
school days (orange; weekends and weeklong holidays). B. Average and standard deviation of
teenager steps for each month of the year.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
23
Figure 3: A. and B. Minutes asleep per day over time for the teenager and adult, respectively,
with green representing school days and orange as non-school days (i.e. weekends and
weeklong holidays). C. and D. Minutes asleep per day on each day of the week for the teenager
and adult, respectively, with green representing weekdays and orange as weekends (Saturday
and Sunday).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
24
Figure 4: A. Steps per day for the teenager against the number of steps on identical days for the
adult, with green representing school days and orange as non-school days. B. Minutes asleep
per night for the teenager against the minutes of sleep per night for the adult, on identical days,
with green representing school days and orange as non-school days.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
25
Table Headings
Table 1: Data collected over 60 months from the teen and adult.
Table 2: Linear regression model fit on the 1826 step counts from the teen, with variables
representing whether a day was a weekend, in one of the five holiday periods, the year of the
study (first through fifth), and the month of the year.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
Table 1
Teen Female
Adult Male
Starting age 10 years 4 months (ending
4th grade)
43 years 9 months
Available step measurements
(days)
1566 (85.8%) 1823 (99.8%)
Missing step measurements
(days)
260 (14.2%) 3 (0.16%)
Available sleep
measurements (days)
828 (45.3%) 1548 (84.8%)
Missing sleep measurements
(days)
998 (54.7%) 278 (25.2%)
Steps per day, mean
(standard deviation)
6568.3 (3685.9) 7757.2 (2850.7)
Minutes sleep per night,
mean (standard deviation)
482.6 (112.1) 362.5 (85.7)
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
Table 2
Variable
in
linear regression
model
Coefficient
ANOVA p
-
value
Intercept 11215.0
Day is a weekend day – 2194.91 < 2.2 x 10
-
16
Day during one of the five holiday periods – 996.75 < 2.2 x 10
-
16
Every year of the study past the first year
(First year 0, second year 1, …)
– 1299.89 1.953 x 10
-
10
Month (1 for January, 12 for December) – 107.01 1.425 x 10
-
6
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
0
5000
10000
15000
20000
25000
2014 2015 2016 2017 2018
Date
Steps
Teen, number of points: 1566
Date vs. Steps
A
0
5000
10000
15000
20000
25000
2014 2015 2016 2017 2018
Date
Steps
Adult, number of points: 1823
Date vs. Steps
B
0
5000
10000
15000
20000
25000
Sunday Monday Tuesday WednesdayThursday Friday Saturday
Day of Week
Steps
Teen, number of points: 1566
Weekday vs. Steps
C
0
5000
10000
15000
20000
25000
Sunday Monday Tuesday WednesdayThursday Friday Saturday
Day of Week
Steps
Adult, number of points: 1823
Weekday vs. Steps
D
Figure 1
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
0
5000
10000
15000
20000
25000
FALSE TRUE
School day
Steps
Teen, number of points: 1566
School day vs. Steps
A
0
2500
5000
7500
10000
12500
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Month
Mean Steps
Teen, number of points: 1566
Month vs. Steps, Across All Five Years
B
Figure 2
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
0
250
500
750
1000
2014 2015 2016 2017 2018
Date
Sleep (min)
Teen, number of points: 828
Date vs. Sleep
A
0
250
500
750
1000
2014 2015 2016 2017 2018
Date
Sleep (min)
Adult, number of points: 1548
Date vs. Sleep
B
0
250
500
750
1000
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
Day of Week
Sleep (min)
Teen, number of points: 828
Weekday vs. Sleep
C
0
250
500
750
1000
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
Day of Week
Sleep (min)
Adult, number of points: 1548
Weekday vs. Sleep
D
Figure 3
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
Pearson r = 0.2
p = 4.92e−16
0
5000
10000
15000
20000
0 10000 20000
Adult Steps
Teen Steps
Steps, number of points: 1589
Adult Male vs. Teen Female, Steps Per Day
A
Pearson r = 0.23
p = 1.32e−09
0
250
500
750
0 250 500 750 1000
Adult Sleep (min)
Teen Sleep (min)
Sleep, number of points: 707
Adult Male vs. Teen Female, Time Asleep Per Day
B
Figure 4
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted October 26, 2020. ; https://doi.org/10.1101/2020.10.21.20215491doi: medRxiv preprint
