39
Multi-Stage Receptivity Model for Mobile Just-In-Time Health
Intervention
WOOHYEOK CHOI, Korea Advanced Institute of Science and Technology, South Korea
SANGKEUN PARK, Korea Advanced Institute of Science and Technology, South Korea
DUYEON KIM, Korea Advanced Institute of Science and Technology, South Korea
YOUN-KYUNG LIM, Korea Advanced Institute of Science and Technology, South Korea
UICHIN LEE
∗
, Korea Advanced Institute of Science and Technology, South Korea
A critical aspect of mobile just-in-time (JIT) health intervention is proper delivery timing, which correlates with successfully
promoting target behaviors. Despite extensive prior studies on interruptibility, however, our understanding of the receptivity
of mobile JIT health intervention is limited. This work extends prior interruptibility models to capture the JIT intervention
process by including multiple stages of conscious and subconscious decisions. We built BeActive, a mobile intervention
system for preventing prolonged sedentary behaviors, and we collected users’ responses to a given JIT support and relevant
contextual factors and cognitive/physical states for three weeks. Using a multi-stage model, we systematically analyzed the
responses to deepen our understanding of receptivity using a mixed methodology. Herein, we identify the key factors relevant
to each stage outcome and show that the receptivity of JIT intervention is nuanced and context-dependent. We propose
several practical design implications for mobile JIT health intervention and context-aware computing.
CCS Concepts: • Human-centered computing → Empirical studies in ubiquitous and mobile computing;
Additional Key Words and Phrases: Just-in-time intervention, interruptibility, receptivity, prolonged sedentariness
ACM Reference Format:
Woohyeok Choi, Sangkeun Park, Duyeon Kim, Youn-kyung Lim, and Uichin Lee. 2019. Multi-Stage Receptivity Model for
Mobile Just-In-Time Health Intervention. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 3, 2, Article 39 (June 2019),
26 pages. https://doi.org/10.1145/3328910
1 INTRODUCTION
The prevalence of smart devices and sensors allows us to use various intelligent positive computing services
[
42
] which continuously monitor individual health conditions and unobtrusively infer surrounding contexts
and internal states. This enables just-in-time (JIT) health intervention, which aims to provide the right type of
support at the right time [
53
]. There has been a variety of studies on JIT health intervention aiming to resolve
∗
This is the corresponding author.
Authors’ addresses: Woohyeok Choi, Korea Advanced Institute of Science and Technology, 291 Daehak-ro, Yuseong-gu, Daejeon, 34141,
South Korea, [email protected]; Sangkeun Park, Korea Advanced Institute of Science and Technology, 291 Daehak-ro, Yuseong-gu,
Daejeon, 34141, South Korea, [email protected]; Duyeon Kim, Korea Advanced Institute of Science and Technology, 291 Daehak-ro,
Yuseong-gu, Daejeon, 34141, South Korea, [email protected]; Youn-kyung Lim, Korea Advanced Institute of Science and Technology, 291
Daehak-ro, Yuseong-gu, Daejeon, 34141, South Korea, [email protected]; Uichin Lee, Korea Advanced Institute of Science and Technology,
291 Daehak-ro, Yuseong-gu, Daejeon, 34141, South Korea, [email protected].
Permission to make digital or hard copies of all or part of this work for personal or classroom use is granted without fee provided that
copies are not made or distributed for prot or commercial advantage and that copies bear this notice and the full citation on the rst
page. Copyrights for components of this work owned by others than ACM must be honored. Abstracting with credit is permitted. To copy
otherwise, or republish, to post on servers or to redistribute to lists, requires prior specic permission and/or a fee. Request permissions from
© 2019 Association for Computing Machinery.
2474-9567/2019/6-ART39 $15.00
https://doi.org/10.1145/3328910
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:2 • W. Choi et al.
dierent health problems, including habitual smoking [
55
,
67
], stress management for parents with attention
decit hyperactivity disorder children [61], eating disorders [63], and physical inactivity [8, 9, 18, 37, 45, 72].
To perform a target behavior elicited by JIT health intervention, people may be required to allocate a variety
of eorts and resources. Thus, it is important to carefully consider when to deliver JIT health intervention [
53
]. A
simple and widely-employed strategy is to deliver JIT support messages as soon as a user enters into a vulnerable
state that could result in adverse health outcomes (e.g., long sedentary bouts, which contribute to type 2 diabetes
and cardiovascular disease [
7
]). However, if the support is given at an inappropriate moment, this strategy may
disrupt users’ ongoing tasks and negatively inuence adherence. In some cases, it may even cause safety risks,
such as by distracting users from driving.
Fortunately, problems with delivery timing of JIT support can be alleviated if we know when people are
most likely to engage in the target behaviors suggested by JIT support, namely, when people are in a highly
interruptible state. A simple heuristic method is to create xed rules for unavailable situations (e.g., not asking
users to stand up while driving) [
36
]. More elaborate approaches include leveraging Ubicomp literature on
automatic detection of interruptible moments. Prior studies showed that interruptibility for message delivery
depended on message content and perceived disruption levels [
50
], places characteristics [
48
], types of ongoing
tasks [
13
,
48
], and personality traits [
78
]. Although the target behaviors suggested by JIT support typically
demands higher workload than message checking, interruptibility literature clearly indicates that receptivity of
JIT intervention varies widely across a variety of contextual factors, contents, and individual characteristics.
In this work, we aim to deepen the understanding of receptivity for mobile JIT health intervention by leveraging
an interruptibility model (i.e., Decision-on-Information-Gain (DOIG) [
74
,
75
]), which describes multiple stages of
sequential decisions in response to a given notication. We extend this model to capture the JIT intervention
process comprising multiple decision stages: perception of the intervention signal; assessment of availability;
determination of adherence; and actual performance of a target behavior. Note that health behavior promotion is
a complex process, and there are a variety of determinants (e.g., contexts, motivations, and health beliefs) related
to its success. Thus, we limit our scope to well-known contextual and psycho-physiological factors to later allow
researchers and practitioners to use context-aware computing to infer the receptivity of JIT intervention.
Towards this goal, we focus on health interventions designed to prevent prolonged sedentary behaviors. We
build a prototype service, BeActive, that delivers timely suggestions for active breaks (e.g., “stand up and move
around for a minute”) via users’ smartphones and watches whenever uninterrupted sedentary bouts (e.g., 1-hour
sitting) are detected. For each suggestion, we ask the user to report the context (e.g., location, social setting,
and ongoing tasks); cognitive/physical state (e.g., level of focus and physical fatigue), and their decision on
intervention (e.g., perception, availability, adherence, performed behaviors). We conducted a 3-week eld study
with 31 participants and collected 5,409 self-reports. By analyzing these reports with multilevel logistic regression,
we identied key predictors relevant to users’ response behaviors at each stage.
Our results show that the receptivity of JIT intervention is multifaceted and context-dependent. The focus on
ongoing tasks negatively contributes to all stages, and physical fatigue is a major contributor aecting adherence.
Despite the negative eects of social setting on perception and availability, less important social engagements
such casual conversations tend to positively transition to active breaks. Based on these ndings, we propose
several design implications, such as delineations of availability and adherence, contextualized guideline support,
and automatic receptivity inferencing.
2 RELATED WORK
2.1 JIT Health Intervention
Advances in sensor and networking technologies allow us to unobtrusively monitor individual states and
surrounding contexts in real-time, while proactively providing cues and information about users. Such advances
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:3
allow to provide the right type of support at the right time, JIT health intervention [
53
]. Previous work has
employed JIT intervention to deal with a variety of health-related issues, including smoking cessation [
55
,
67
],
prevention of eating disorders [
63
], reducing physical inactivity [
8
,
9
,
18
,
37
,
45
,
72
], and stress management [
61
].
An essential element for JIT health intervention success is the determination of when a support message
should be delivered to a user. Typically, the right time of support delivery is regarded as the time at which users
are vulnerable to adverse health conditions. In the case of smoking cessation, interventions are triggered when
smokers visit a place where they have frequently smoked [
55
] or when they experience high stresses over a short
period [
67
]. To decrease sedentary behavior, opportune timing requires prompts to be delivered when prolonged
inactivity is detected (e.g., step count is less than a certain threshold) [8, 9, 45, 72].
An additional consideration for intervention delivery timing is nding when a user is receptive to a given
JIT support [
52
]. Receptivity of JIT support is dened as the conditions that a user can receive, processes, and
adhere to the support provided [
52
]. JIT support requires users’ perceptual, cognitive, and motor resources and
may even be considered disruptive to ongoing tasks. Thus, JIT support has similar characteristics to interruption.
In the eld of ubiquitous computing, researchers actively striven to understand, dene, and detect opportune
moments for interruption. Understanding interruptibility will help us better estimate receptivity of JIT support.
Prior studies proposed various measures of dening interruptibility for an incoming task, including subjective
sentiment [
50
,
58
,
78
] and/or reaction latency/presence [
4
,
13
,
22
,
48
–
50
,
58
,
68
,
74
,
75
]. In the vehicular contexts,
researchers also considered safety and task performance aspects due to dual-tasking nature of interruption [
34
].
Furthermore, recent studies focused on adherence to incoming interruptions. For example, actual interaction with
incoming content (e.g., tapping on notications) can be regarded as evidence that a user is in a receptive state
[48, 50, 74, 75]. Receptivity may additionally consider the engagement of the non-primary content [59].
Apart from delivery timing, JIT support messages should be carefully tailored for targeted health outcomes,
users’ internal states, and surrounding contexts, because message contents can have a strong inuence on a
user’s receptivity to given support [
23
] and on health outcomes [
37
]. Recent studies proposed a more advanced
concept of JIT intervention, JIT adaptive intervention, where the content and timing of JIT intervention was
tailored per individual characteristics and contexts [
52
,
53
]. These studies highlighted that receptivity was indeed
a complex and multifaceted process. Furthermore, it demanded we further study receptivity.
Referencing a variety of issues about JIT intervention, this work explores users’ receptivity to given JIT health
support across diverse contexts. Our work builds upon previous interruptibility studies that focused primarily on
the receptivity of a relatively simple task with minimal workload (e.g., unlocking/touching the smartphone). Our
work aims to deepen the understanding on the receptivity of JIT support, which often requires users to perform
a more eortful and time-consuming task (i.e., standing up and moving around for a period). Unlike interactions
with the smartphone, this task might be dierently received by users because of its unique characteristics,
including the denite suspension of ongoing tasks and the requirement of physical eort. Whereas this task is
common to health intervention techniques for reducing physical inactivity and sedentariness, there is still a lack
of understanding about how users perceive and react to the intervention messages in situ and what contextual
factors are related dierent stages of human information processing and behavior controlling.
2.2 Technological Intervention for Inactivity and Sedentariness
Researchers have studied a variety of technological interventions to promote physical activities. One widely
employed intervention is to promote self-reection on individual health behaviors by measuring health-related
indicators (e.g., calories, step counts, time to engage physical activities) using a variety of sensors. For example,
commercial tness trackers (e.g., Fitbit) monitor and visualize users’ health-related metrics, including step counts
and calorie expenditures. Additionally, there have been several studies that enhanced the self-reection of physical
activity via aesthetic symbols displayed on a mobile device [
17
], interactions with a reection companion [
38
], and
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:4 • W. Choi et al.
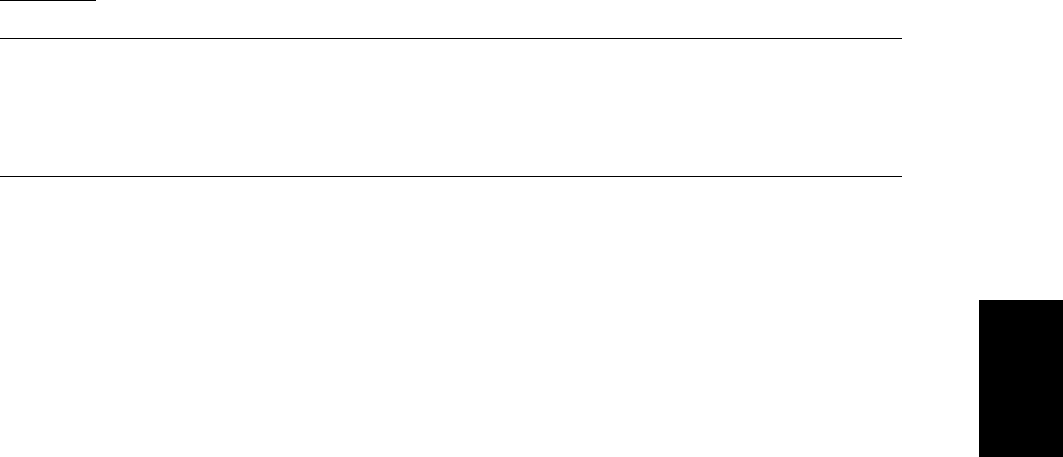
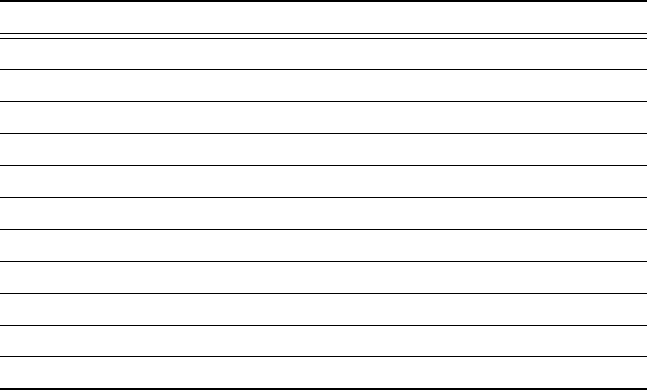
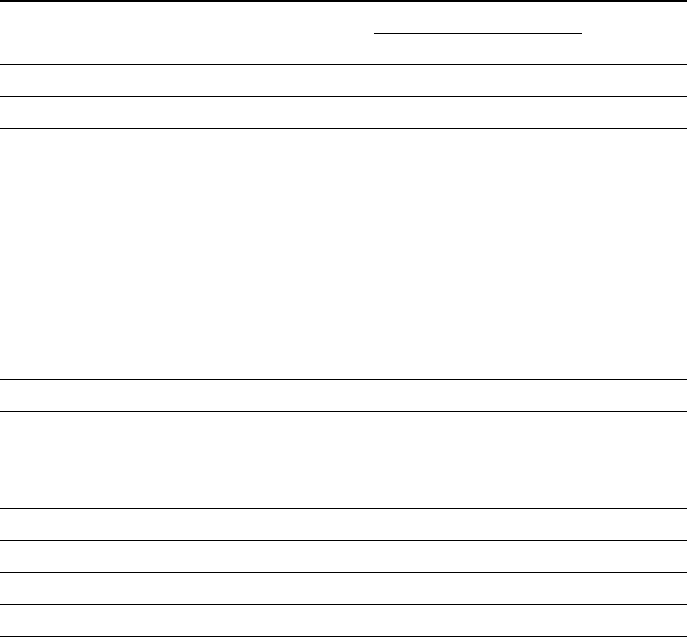
Fig. 1. Decision stages in JIT intervention stage model
Y
N
Is perceived?
Y
N
Is available?
Y
N
Is determined to
adhere?
Actual performance
of the target behavior
Ongoing task
JIT intervention signal
Success
Failure
an ambient light display [
25
]. Social support also has been a frequently used technique for health intervention,
including sharing step counts with friends or an online community [
16
,
26
]. Furthermore, there has been a
variety of studies promoting physical activity, including making activities fun by designing exertion-based games
[
10
,
14
,
15
,
51
], personalized suggestions of physical activities/food using multi-armed bandit [
62
], inconvenient
gadgets requiring users to perform physical activities for operation [
64
], and slowly moving robots for unobtrusive
posture correction [69].
With the promotion of physical activities, there has been increased attention on the intervention of sedentary
lifestyles, which are known to causes a variety of chronic diseases, metabolic dysfunction [
56
,
77
] and hospital
readmission [
5
]. Even for people who engage in a sucient amount of physical activities, uninterrupted sedentary
bouts still contribute to overweight and obesity [
71
]. Thus, increases in breaks from sedentary time are benecial
to reduce waist circumference, independent of the time to engage in moderate-to-vigorous physical activities
[
28
]. To interrupt prolonged sedentariness, studies have often attempted to deliver prompts, including notifying
of prolonged sedentary bouts [
45
,
76
], alerting prolonged sedentariness with a trac-right symbol [
27
], and
suggesting short-bouts of physical activities (e.g., walking, sit-ups, squats) [
8
,
9
,
57
,
72
]. Additionally, active
workstations, which enable workers to perform oce tasks while engaging in a variety of physical activities, has
contributed to reducing sedentary time [3, 6, 12, 32].
Because occupational sitting comprises a large proportion of daily sedentary time and is often prolonged [
47
,
73
],
sedentary interventions typically consider only the work environment. As with conventional smartwatches and
their wearing patterns [
31
], we aim to intervene in prolonged sedentary behaviors occurring not only during
working hours but also at leisure times. Leisure-time sedentary behavior was also revealed to contribute to
obesity in adults [
71
]. Thus, it is meaningful to consider sedentary interventions during non-working hours.
Understanding a variety of contextual factors relevant to receptivity of the JIT support is critical for building
context-sensing systems that can better deliver JIT support messages.
3 JIT INTERVENTION STAGE MODEL
We propose a JIT intervention stage model that unies the entire process from intervention message arrivals
to the actual execution of suggested health behaviors. Our model comprises four stages: perception of the
intervention signal; assessment of availability; determination of adherence; and actual performance (see Fig.
1). This model applies to a range of JIT interventions that deliver timely in situ support as a form of external
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:5
stimuli to draw attention, require timely reaction to a given support message, and demand eort and time to
complete a recommended behavior. For example, Fitbits provide JIT support to achieve a certain level of physical
activities (e.g., more than 250 steps every hour). When detecting the lack of physical activities in the hour, the
Fitbit sends vibrotactile and visual cues to inform users of their insucient physical activities, suggesting further
physical activity. If users perceive these cues, they must then decide decide whether to follow the suggestion
before another hour passes. If suggestions are accepted, users then spend physical eort and time to achieve the
suggested goal.
3.1 Stage 1: Perception of the Signal
The rst stage, perception of the signal (or support message), assesses whether a user perceives external stimuli
triggered by the JIT intervention. The signal is delivered via dierent sensory channels and modailites. For
example, users can commonly receive notications on a smartphone [
8
,
37
,
60
,
61
,
72
,
76
]. A pop-up dialogue on
the desktop computer [
9
,
27
,
45
] or ambient display [
29
,
33
] are also feasible. Previous works proposed a variable
similar to signal perception, such as the seen time of incoming messages or notications, which can be measured
by tracking device events (e.g., unlocking a smartphone, turning the screen on) [
13
,
50
]. However, perception here
implies the concept of interruption detection [
39
]. An undetected interruption is denoted as oblivious dismissal.
These are very dierent from the seen time. Perception is an automatic process of human beings that has nothing
to do with an intent to dismiss or follow a signal [
40
]. However, seen time is a mixture of perception and decision
making and is aected by users’ (mis)interpretation of or intention to dismiss (or consume) incoming signals. For
example, users might ignore a signal when they are too busy or do not want to handle it immediately [
13
], which
leads to a longer seen time.
3.2 Stage 2: Assessment of Availability
After perceiving the signal, users read or interpret the JIT support message provided. For the given context, they
then assess whether they are available to perform the target behavior. A previous study dened availability as
an individual’s capacity to engage in incoming and unplanned activities [
68
]. An available state indicates that
users can respond/react to incoming information without signicant disruptions [
30
] or within a certain amount
of time after the signal is delivered [
68
]. These denitions embody a variety of elements used to determine an
individual’s available state, such as motivational factors, contextual factors, social norms, and characteristics
of target behavior. To simplify our modeling, we omit motivational factors from this stage, but we incorporate
them in the next stage. Thus, we re-dene availability for JIT intervention as when a user is capable of engaging
in a target behavior suggested by the JIT intervention, and it is acceptable based on personal and social norms,
disregarding motivational factors.
3.3 Stage 3: Determination of Adherence
When users are triggered to perform a target behavior suggested by the JIT support, they must decide whether
to actually perform the target behavior. This is adherence. The decisions of this stage are inuenced by health
beliefs, motivations, and individual states. For example, users may intentionally dismiss incoming JIT support
messages, because suggested behaviors are less signicant than their ongoing tasks [
39
], or they feel physically
too tired to perform the suggested behaviors [
45
]. Lack of motivation for behavioral change causes users to reject
the support provided if the target behavior is relatively complicated [
24
]. Additionally, adherence is unlikely to
occur if users believe that the support is not benecial enough or that they are not vulnerable to the health risks
[
65
]. Thus, there are a variety of potential factors contributing to adherence, and our model can be extended to
include sub-decision stages accounting for these factors, which will be a future work.
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:6 • W. Choi et al.
3.4 Stage 4: Actual Performance
If users decide to adhere to the JIT support message, they should suspend their ongoing tasks and switch to the
target behavior suggested. When completing the target behavior, users are expected to resume their ongoing
tasks. Our model includes the method used to actually perform their target behaviors, because it is important to
investigate actual adherence. For example, users may perform dierent activities than suggested, or they may
under- or over-perform. In reality, dierent interventions may stipulate dierent adherence levels. In the case
of encouraging physical activities, for example, people tended to engage in walking longer than the suggested
amount of time once they started [
72
]. For tailoring JIT interventions to enhance intended health outcomes, it is
important to understand how individuals actually performs the target behavior for a given support.
3.5 Discussion
The JIT intervention stage model that we propose builds upon the DOIG-based interruptibility model, which
is focused on the consumption of mobile-phone notications [
74
,
75
]. The DOIG-based model breaks down a
user’s response into a sequence of micro-decisions based on the user’s interactions with the device. Potential
micro-decisions for this model include the reachability stage: whether a user will at least react to an incoming
notication, or will not react at all, leading to a null response; the engage-ability stage: (when perceived) whether
the user will begin to respond, but will discontinue consuming the interruption, leading to a partial response if
discontinued; and the receptivity stage: (when the user decides to continue the consumption) whether the user
will be receptive to completing the requested responses, leading to a complete response if receptive.
While the DOIG-based interruptibility model was originally created to explain the key decision stages of
content consumption for a given notication, it can also partly explain JIT intervention scenarios. Suppose
that JIT support messages are delivered in the form of mobile notications, including vibrotactile feedback for
smartwatches. After perceiving a JIT support message during the reachability stage, users may successfully
consume the message during the engage-ability and receptivity stages. However, the DOIG-based interruptibility
model mainly focuses on the observed response behaviors resulting from interactions with mobile notications.
Thus, whereas perception (or reachability) is common in both models, the other two stages in the DOIG-based
model do not clearly capture the detailed decision factors related to performing the target behavior as prescribed
in the JIT support message.
Beyond mobile notication delivery, our JIT intervention stage model details the latent decision factors for
executing target behaviors in relation to Fogg’s Behavior Model (FBM) [
24
], which proposes three constructs
for behavioral change: motivation, simplicity, and triggers. JIT intervention often requires users to perform
prescribed target behaviors that can be time-consuming, eortful, and even socially-deviant to some extent under
certain situations. To lead users to actually execute the target behaviors, users should believe that they will be
available to perform the target behavior at the time the JIT support message arrives. This points to the availability
assessment stage in our model, which corresponds to the simplicity aspect of FBM. In addition, users should get
motivated enough to perform the target behaviors. The adherence stage in our model is closely related to the
motivation construct in FBM. Likewise, the adherence stage in our model is closely related to the motivation
construct in FBM.
4 CASE FOR PROLONGED SEDENTARY BEHAVIOR INTERVENTION
We elaborate research questions related to users’ receptivity to a given JIT support using the proposed intervention
stage model. As stated, there are a variety of potential factors contributing to each stage, including contexts,
motivational factors, personality traits, and suggestion contents. In this work, we primarily focus on contextual
factors and physical/cognitive states, because the ultimate goal is to facilitate automatic detection of the receptivity
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:7
in the JIT support with contextual and physiological sensing based on ubiquitous computing technologies.
Understanding the eects of motivation and belief factors is a part of our future work.
Among a variety of health concerns, we focus on prolonged sedentariness. There are several reasons for
choosing sedentary intervention. Uninterrupted sedentary behavior is prevalent nowadays and is known as the
cause for a variety of chronic diseases and early mortality [
7
]. There have been many attempts and practices of
sedentary intervention, and prolonged sedentariness is relatively simple to measure using mobile sensors.
Our intervention scenario prompts users with intervention messages via smart devices, similar to prior studies
[
8
,
76
]. In our scenario, the smartphone continuously monitors a user’s sedentary behavior. When detecting a
prolonged sedentariness (e.g., uninterrupted sedentary behavior exceeding a predened duration), the smartphone
delivers a notication that suggests the user to stand up and move around for a minute. This is called an active break.
With our proposed JIT intervention stage model, this scenario can be separated into conscious or subconscious
decision stages.
When the intervention service detects prolonged sedentariness, the smartphone notication is delivered to
stimulate users’ sensory organs (via the current smartphone ringer mode) and draw their attention to the arrival
of the JIT support message. Users then subconsciously perceive or miss the notication. This is the rst stage,
the perception of a signal. Success in this stage results from dierent factors across types of ongoing tasks, social
settings, locations, and/or physical/cognitive states. Our rst research question is as follows:
RQ1. What are the contextual factors and physical/cognitive states that are relevant to the perception of
the signal?
If users successfully perceive the signal, they then check the suggestion contained in the notication. As
stated earlier, our activity suggestion is to stand up and move around for a minute. Users must judge whether
they are available to comply with the suggestion. For example, we can assume that users are unlikely to be
available to stand up and move around while driving or during a wedding. Additionally, users’ physical conditions
can negatively inuence on availability. To understand such potential factors aecting availability, the second
research question is formulated as follows:
RQ2. What are the contextual factors and physical/cognitive states that are relevant to the perceived
availability of active breaks?
When users perceive the intervention signal and think about standing up and moving around, they decide
whether they will voluntarily break their sedentary behavior, suspend their ongoing task (if any), and adhere to
an active break routine. This series of activities is eortful and time-consuming (and sometimes burdensome).
Thus, some users do not want to engage, even though they are available. To reveal the factors that inuence
adherence of the active break, our third research question is formulated as follows:
RQ3. What are the contextual factors and physical/cognitive states that are relevant to the adherence of
active breaks?
Finally, if users make positive decisions in all previous stages, we assume they actually stand up and move
around. This suggestion provides some degrees of freedom to choose types of activities for a session. For example,
users might engage in short bouts of obvious physical activities, such as stretching or walking. However, they
might also go for a walk for refreshment and relaxation with no specic intention to increase in their physical
activity. To explore how users actually perform during a session of active breaks, the nal question is as follows:
RQ4. What are the types of activities during an active break session?
5 STUDY PROCEDURE
To answer our research questions, we implemented a research prototype of sedentary intervention, BeActive,
which provides timely support to break prolonged sedentariness and allows users to report dierent decisions
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:8 • W. Choi et al.
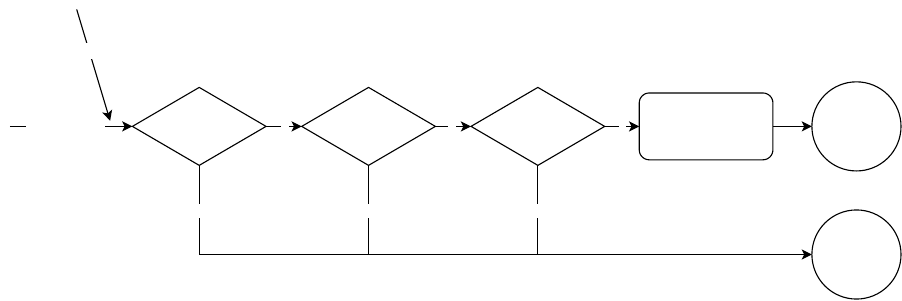
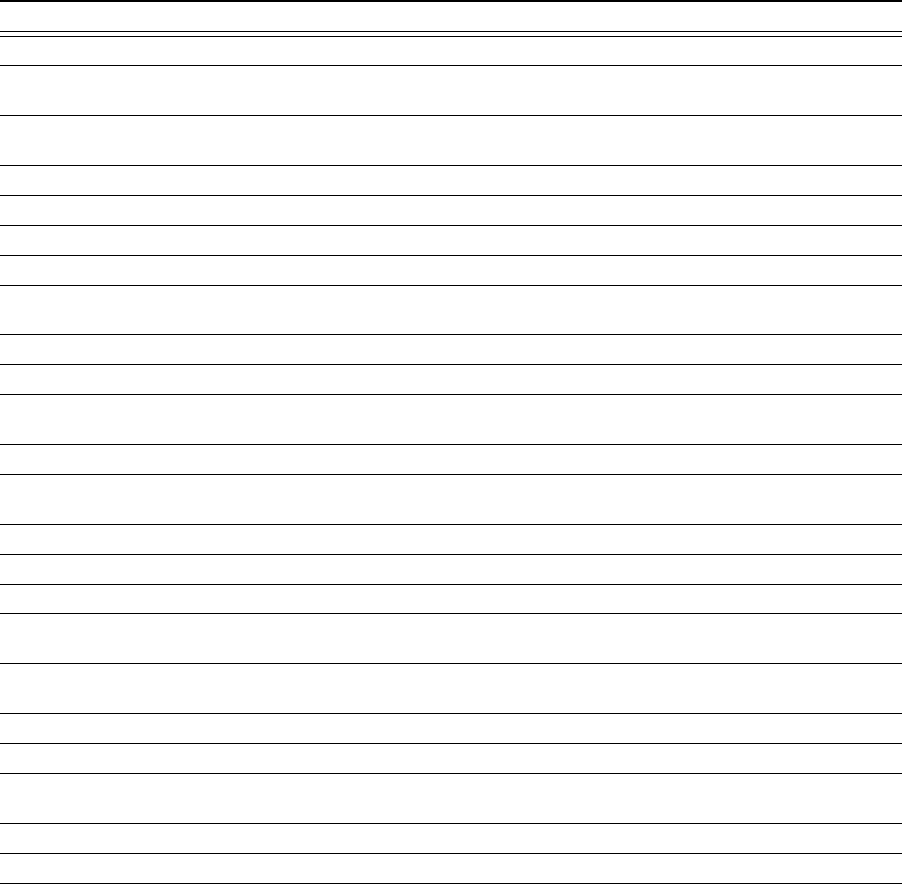
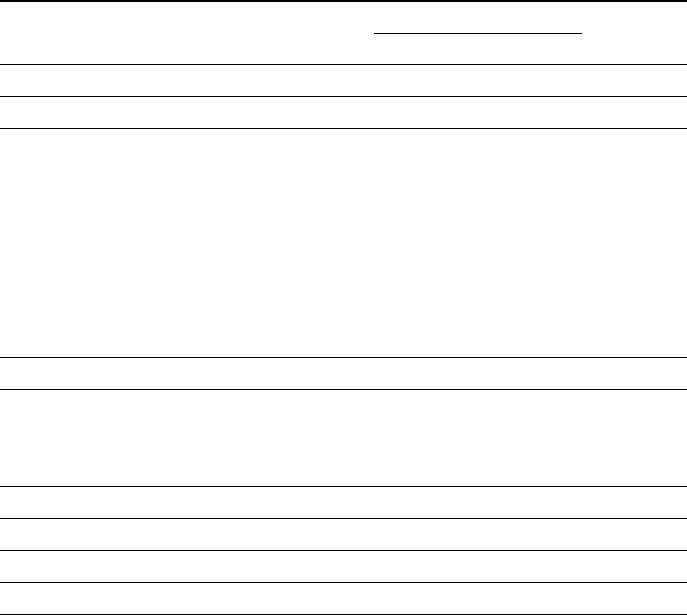
Fig. 2. State diagram of BeActive’s JIT intervention process
STILL/IN_VEHICLE
on ACTIVITY_TRANSITION_EXIT
60-min
passes
Intervention
scheduled
STILL/IN_VEHICLE
on ACTIVITY_TRANSITION_ENTER
Intervention
canceled
Deliver
a prompt
Prolonged
sedentariness
about given support and relevant factors to such decisions. In this section, we begin by presenting how BeActive
works and which types of questions were included for the self-report. We then elaborate on our eld trial that
lasted 3 weeks.
5.1 Implementation of BeActive
Our research prototype of sedentary intervention, BeActive, is comprised of three major components, sedentary
behavior sensing; intervention prompt delivery; and self-reporting on surrounding contexts, cognitive/physical
states, and decisions to a given JIT support message. BeActive is operated on the Android mobile phone whose
operating system version is equal to or higher than 6.0.0 (Marshmallow). During an implementation period,
we employed iterative design process to identify usability and functional issues. We conducted several pilot
tests, including two rounds of low-delity prototype tests with three and four participants, and a high-delity
prototype eld test with seven participants for three days. All prototype tests were conducted with students on
our campus.
5.1.1 Sedentary Behavior Sensing. BeActive continuously monitors a user’s mobility status using Google’s Activity
Recognition Transition API
1
on a smartphone. This API allows applications to subscribe to activity transition
events, such as entering into (ACTIVITY_TRANSITION_ENTER) or exiting from (ACTIVITY_TRANSITION_EXIT)
activities of interest. Supported activities are IN_VEHICLE (i.e., the device is in a vehicle), RUNNING (i.e., the
device is on a user who is running), WALKING (i.e., the device is on a user who is walking), ON_FOOT (i.e.,
WALKING or RUNNING), ON_BICYCLE (i.e., the device is on a bicycle), and STILL (i.e., the device is not moving).
To detect a user’s sedentary behavior, we consider two activities, such as STILL and IN_VEHICLE, because
both activities accompany prolonged sedentariness. When a user’s device becomes stable (e.g., sitting down
or leaving the device on a desk) or begins to travel by car, the API reports STILL/IN_VEHICLE on ACTIV-
ITY_TRANSITION_ENTER, otherwise it reports STILL/IN_VEHICLE on ACTIVITY_TRANSITION_EXIT. When
entering these activities, our service schedules the intervention prompt to be delivered after 60-min that is
reported as preferred work duration [45]. When the API reports exiting these activities, our service cancels the
scheduled prompt, if any (see Fig. 2).
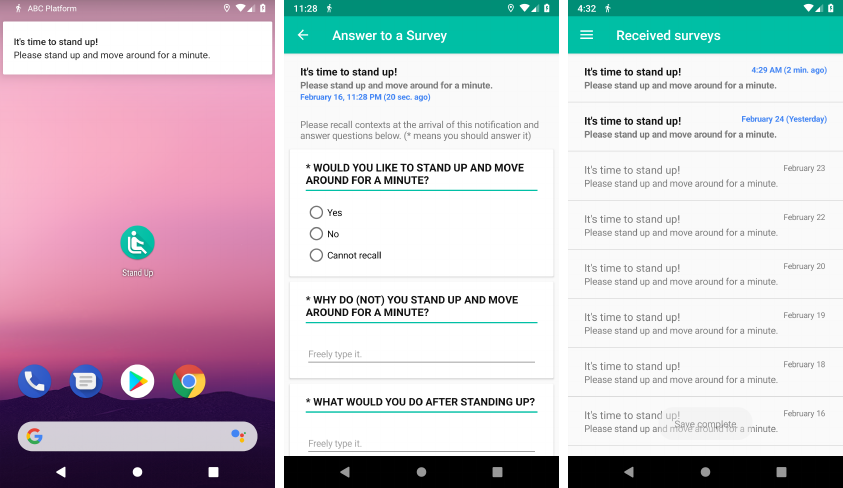
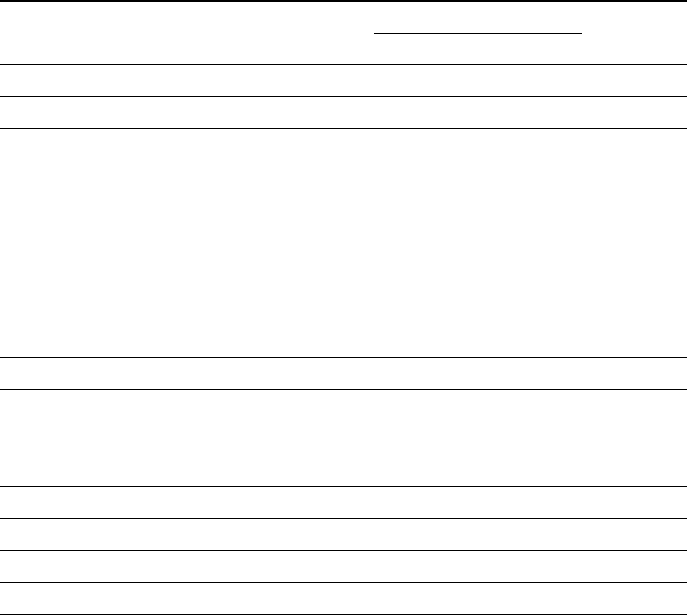
5.1.2 Intervention Prompt Delivery. When a user’s devices remain stable with no mobility changes after an
intervention prompt has been scheduled, the intervention prompts appear on a user’s smartphone in the form of
a push notication, which includes the suggestion of an active break, as shown in Fig. 4a. The sensory channels
1
https://developer.android.com/guide/topics/location/transitions.html
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:9
Fig. 3. Overview of BeActive
(a) Active break suggestion via notifi-
cations
(b) Self-reports
(c) A list of prompts delivered. Unan-
swered ones is highlighted in bold.
for intervention delivery correspond to a user’s current setting of the ringer mode. When the prompt is triggered,
the service re-schedules the next one in 1 hour.
Considering the characteristic of timely support for JIT intervention, we presume that a user’s decision on
given support should be made within a short duration from the moment of support arrival. However, users’
receptivity depends on the current ringer mode. Recent studies have shown that the seen time of the notication
is longer when the ringer mode is set to silent, compared to other modes [
50
]. Additionally, people typically set
their ringer mode to silent or vibrate during working hours and sleep [
13
], as did our participants in the pilot
test. Because the intervention prompts are also delivered in the form of notications, the ringer mode can have
a signicant inuence on the receptivity of the prompts. To mitigate delayed or missing cacused by the ringer
mode, we also used a wrist-worn smartwatch to deliver vibrotactile feedback independent of the smartphone’s
ringer mode.
5.1.3 Self-Reporting on Contexts, Cognitive/Physical States, and Response to JIT Support. To capture users’ contexts
and decisions on a given JIT support message, we provided questionnaires and instructed respondents answer it
by clicking notications. Given that users could miss the notications or defer their responses, we allowed them
to view the list of all prompts (and associated questionnaires) and to answer any missed questions later (see Fig.
4c). As shown in Table 1, we rst asked whether users took an active break after receiving the prompt. We then
asked them to detail the reasons for their decision and their resulting movement behaviors. We asked them to
choose the perception status of the notication, and their availability for an active break. Furthermore, we asked
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:10 • W. Choi et al.
Table 1. estionnaire items to capture contexts, cognitive/physical states, and decision on a given JIT support message.
Question Answer type
Would you like to stand up and move around for a minute? Yes / No / Cannot recall
Why do you (not) stand up and move around for a minute? Free text
What would you do after standing up? Free text
Did you perceive the arrival of this notication? Yes / No / Cannot recall
Are you available to stand up and move? Yes / No / Cannot recall
Please describe your context as follows:
- Where are you? Free text
- Whom are you with? Free text
- What are you doing? Free text
Please rate your level of focus on your ongoing task in 7-point Likert scale
Please rate your level of fatigue in 7-point Likert scale
of their situational context (i.e., place, social setting, and ongoing task) and of their cognitive/physical status
(i.e., level of focus/fatigue on a 7-point Likert scale). For measuring fatigue, we used the Samn-Perelli fatigue
scale (e.g., 1: fully alert, wide awake; 3: okay, somewhat fresh; 5: moderately tired, let down; and 7: completely
exhausted, unable to function eectively) [66].
For accurately capturing contexts and states, at the beginning of the questionnaire, we displayed the arrival
time of a given prompt, and when answering the questions, users were explicitly asked to consider their situation
at the time of message arrival or up to 5-min afterwards. For example, if a user could perceive the arrival of an
intervention prompt during this 5-min period, the message was marked as perceived. The threshold of 5-min was
derived from ndings of people seeing notications within approximately 5-min, except for when the ringer
mode is set to silent [
50
]. We carefully considered the wording of the self-report questions (particularly about
the tense) regarding whether a user takes an active break and what they do during the break. This is because
users could answer these questions right after the prompt arrival, during/after the active break, or even after
several hours. We initially tried to vary the tense of each question based on contexts, but during the pilot trials,
our participants complained that tense variations were confusing. For this reason, we used the present tense
(as shown in Table 1) and explicitly instructed users to answer the questions based on what they had done,
or what they will denitely do within the 5-min period after message arrival. After 5-min of notication, we
simply assumed that a participant did not perceive the notication in time or intentionally dismissed it. Then, all
questions were changed to the past tense so that participants could recall the contexts of their notication times.
The responses were stored in a user’s smartphone and uploaded to the server via a Wi-Fi network.
5.2 Field Study
For the eld study, we recruited 31 participants (14 females; age: M=29.00, SD = 7.03) from an online campus
community, faculty mailing list, and Facebook in October 2018. They were required to have spent at least 6 hours
sitting per day. Their occupations varied, including nine graduates, seven undergraduates, nine oce workers,
ve IT developers, and one plastic surgeon. In an introductory session, we instructed the participants on using the
service and asked them to use it for 3 weeks. To explore a variety of contexts including working hours and leisure
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:11
time, BeActive was set to track prolonged sedentary behavior (i.e., 1-hour sitting) from 8:00 to 23:59 so that the
participants could receive the prompts from 9:00 to 23:59 every day during the study. Thus, participants received
at most 15 prompts per day if they never moved between 8:00 to 23:59. Additionally, we asked participants to
note any erroneously-triggered prompts after having moved during the past hour. This could result from sensing
errors or moving without holding the phone. We excluded those prompts from our analysis.
We also distributed smartwatches, Fitbit Ionic, to help participants perceive the arrival of intervention prompts.
Thus, notications were delivered via both smartphones and smartwatches. We congured the Fitbit Ionic to
deliver feedback triggered by only our service to reduce confusion. Any health-related functions that the Fitbit
Ionic supports by default (including showing physiological stats on the display and hourly activity suggestion)
were deactivated to prevent potential inuences on users’ behavior.
After the 3-week eld study, we conducted in-depth exit-interviews for approximately 1 hour per participant
to explore user experiences. Our interview mainly focused on general tendencies to the reactions to given
JIT support messages and activities performed during active breaks. All interview sessions were recorded and
transcribed for thematic analysis. Each participant was compensated with 145 USD, and no additional incentive
for adhering to the active breaks was given.
6 DATA ANALYSIS
In this section, we present how we analyzed self-reports and interviews from the three-week eld study. We rst
elaborate on the exclusion criteria of responses. Then, we describe strategies to label each response, considering
contextual factors and physical activities performed during active breaks. Using these labeled responses, a
regression analysis was performed to understand how a user’s contexts and cognitive/physical states related to
dierent decision stages (i.e., perception, availability, and adherence) of the JIT intervention model we proposed.
Additionally, we qualitatively analyzed interview and self-report responses to nd reasons for the decisions made
in response to a given support message (i.e., "Why do you (not) stand up and move around for a minute?") to
corroborate our ndings from the regression analysis.
6.1 Exclusion Criteria of Context Self-Reports
During the eld study, a total of 5,409 prompts were delivered to 31 participants. We provided a list of received
prompts (see Fig. 4c) so that participants could answer any missed or non-responded questionnaires later. Thus,
participants completed all 5,409 questionnaires. However, we found that seven participants completed their
questionnaires quite late (i.e., more than 20% of their responses were answered after 24 hours) and four did not
even wear the Fitbit Ionic on a regular basis. Therefore, we excluded 1,337 responses from those seven participants
(P25 to P31). We only considered the remaining responses (n=4.072) from the 24 participants (age: M=30.88,
SD=6.73) for data analysis. We then removed 909 invalid responses, such as those responding that they took
active break but were unavailable to do anything active, those providing inaccurate answers to the question items
(e.g., "Where are you?": "Sleeping"), and those answered to erroneously triggered prompts (i.e., prompts delivered
although participants already have moved in the last hour or were currently moving). The following analysis was
conducted with remaining 3,163 valid responses.
6.2 Labeling Responses
From the self-report responses, we categorized the contextual information (i.e., where they were located and
what they did, including the social setting). For this, two authors manually examined responses using an anity
diagram to iteratively develop a coding scheme for categorizing contextual factors and activities performed
during the active break until consensus was reached. Final themes derived are described in Table 2.
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:12 • W. Choi et al.
Table 2. Categorization criteria
Category Denition Examples from self-report
Location
Home
Primary living spaces used as a permanent residence for an individ-
ual
Home, dormitory, living room
Work
Primary places of employment (for employees) or education (for
students)
Oce, meeting room, laboratory
Restaurant/Cafe Places where meals/drinks are prepared and served Restaurant, cafe, bar
Vehicle Vehicles with wheels and an engine, used for transporting people Car, taxi, bus, train
Miscellaneous All other locations A movie theater, barbershop, hotel
Social setting
Social Co-located and engaging in an activity with someone
Talking with friends, getting a haircut,
taking a class
Asocial
Staying alone or co-located, but no social interaction with someone
Watching TV alone, sitting on a bus
Ongoing task
Working/Studying
Doing something related to a job (for employees) or studying (for
students) by themselves
Doing oce work, programming, home-
work
Sleeping The state of being asleep Sleeping in a bed, taking a nap
Resting/Relaxing Resting for a period of time to relax and refresh
Chilling in bed, lying in a bed, doing
something on the phone
Video watching Watching videos Watching YouTube, watching TV
Class/Meeting Group work for a study or job Having a meeting, taking a class
Eating Eating some food or meal Having lunch, Dining out
Gaming Playing a video game on a computer or a smartphone
Playing League of Legends, playing a
mobile game
Conversing Having a face-to-face conversation with someone
Chatting with a family, talking with a
friend
Getting ready for bed The state of preparing for sleep in a bed Getting ready for bed
Calling/Texting Having an online conversation with someone Making a phone call, online chatting
Right after waking up
The state of having just awakened from sleeping but still being in
bed
Just opened up eyes in a bed, woke up
in a bed
Driving Driving a vehicle Driving a car
Miscellaneous All other activities
Getting a haircut, getting an endoscopy
Table 3 shows the distribution of responses across categorized contexts and decisions on our JIT support. For
location, we used four major categories: home, work, restaurant/cafe, and vehicle. The social setting was divided
into social and asocial, depending on the likelihood of possible social interaction. An asocial setting is one where
either a participant is alone or with other people where social interaction is less likely to happen (e.g., public
transportation). In contrast, a social setting is one where either a participant is co-located with other familiar
people (e.g., friends and families) or engages in activities together with others.
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:13
Table 3. Distribution of the responses across dierent locations, social seings, and ongoing tasks
Total
(n=3,163)
Perception Availability
(Perception=Yes)
Adherence
(Per./Avail.=Yes)
No Yes No Yes No Yes
Location
Home
1,594 748 846 91 755 465 290
Work
1,240 261 979 206 773 510 263
Restaurant/Cafe
181 47 134 35 99 69 30
Vehicle
48 19 29 26 3 2 1
Miscellaneous
100 37 63 36 27 22 5
Social setting
Social
1,768 573 1,195 81 775 503 272
Asocial
1,395 539 856 313 882 565 317
Ongoing task
Working/Studying
1,216 222 994 83 911 602 309
Sleeping
564 564 - - - - -
Resting/Relaxing
360 58 302 19 283 173 110
Video watching
272 37 235 27 208 122 86
Class/Meeting
198 57 141 120 21 19 2
Eating
171 68 103 39 64 43 21
Gaming
102 40 60 14 46 37 9
Conversing
96 25 71 30 41 18 23
Getting ready for bed
55 6 49 15 34 33 1
Calling/Texting
38 7 31 15 16 10 6
Right after waking up
30 7 23 1 22 4 18
Driving
29 11 18 18 - - -
Miscellaneous
32 8 24 13 11 7 4
For ongoing tasks, we used the following major categories: working/studying, sleeping, resting/relaxing, video
watching, class/meeting, eating, gaming, conversing, getting ready for bed, calling/texting, right after waking up,
and driving. We dierentiate gaming and video watching because gaming requires interactivity, whereas video
watching is likely to be passive. While resting/relaxing, our participants were likely to sit on a couch or lie on
a bed, possibly using their phones (e.g., reading news or checking social media). If the participants mentioned
that they were playing games or watching videos while resting/relaxing, we excluded such instances from
resting/relaxing and include them in gaming or video watching, because their level of focus would be generally
higher than other resting activities.
Physical activities performed during a session of active breaks are categorized as follows: stretching/exercising,
going for a walk, moving to other places, doing chores, visiting a restroom (for urination and defecation), water
drinking, and bathing/washing. Because some responses included more than one physical activity (e.g., visiting a
restroom and then going to a cafeteria), we put multiple categories into such responses.
6.3 Regression Analysis
We conducted multilevel logistic regression analysis to understand how a user’s contextual factors aect dierent
stages of the JIT intervention stage model (i.e., signal perception, availability assessment, and adherence to a
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:14 • W. Choi et al.
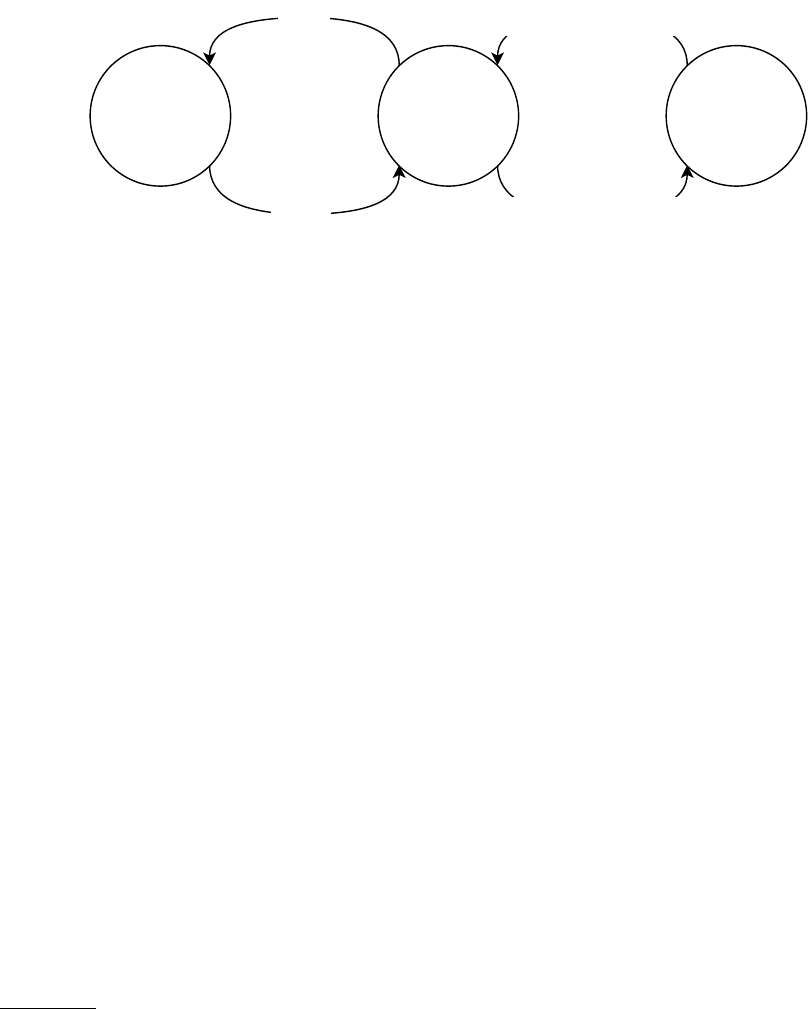
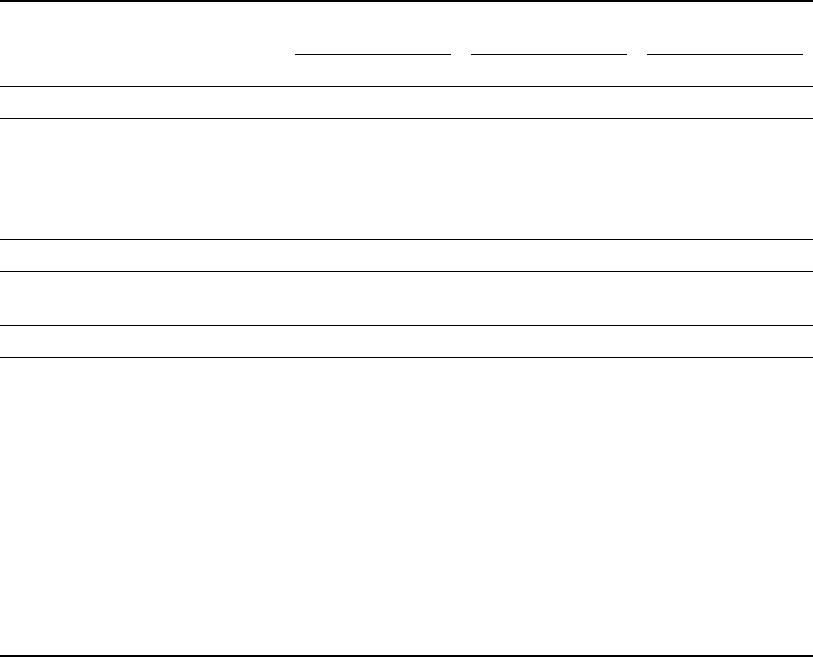
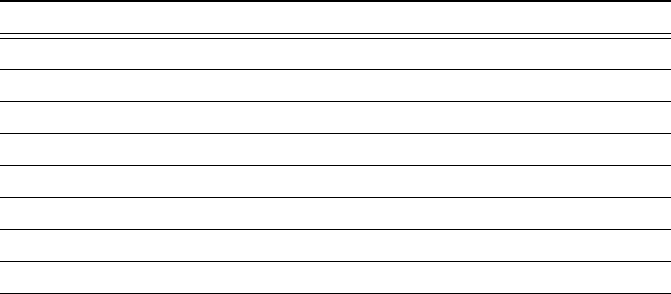
Fig. 5. Summary of regression analysis. “+” and “-” imply statistically significant dependent variables positively/negatively
contributing to each decision stage, respectively.
(+) Ongoing task
Working/Studying, Resting/Relaxing,
Video watching, Getting ready for bed
(-) Ongoing task
Eating, Gaming, Sleeping
(-) Social setting
Social
(-) Level of focus
Is perceived?
(+) Ongoing task
Working/Studying, Resting/Relaxing,
Video watching
(+) Location
Home, Work, Cafe/Restaurant
(-) Ongoing task
Class/Meeting, Eating,
Getting ready for bed, Driving
(-) Location
Vehicle
(-) Social setting
Social
(-) Level of focus
Is available?
(+) Ongoing task
Conversing, Right after waking up
(-) Ongoing task
Getting ready for bed
(-) Level of focus
(-) Level of fatigue
Is determined to
adhere?
Actual performance
of the target behavior
Success
Failure
target behavior). For each stage, we built a multilevel logistic regression model, where a dependent variable was
a decision of the stage, and independent variables were contextual factors categorized and level of focus/fatigue
(as xed eects) and participants (as random intercepts). For the perception of the signal stage, we considered
all responses, in which 2,051 instances were marked as perceived. The model for the assessment of availability
accounted for those 2,051 perceived responses, where 1,657 were reported as available. For the adherence stage,
we employed those 1,657 available instances, in which only 589 had active breaks. We reported the beta coecient,
odds ratio (OR) and condence interval (CI) of each independent variable with xed eects for dierent regression
models. The goodness-of-t of the model is computed with the marginal and conditional
R
2
, where marginal
R
2
indicates variance explained by xed eects and conditional one has variance explained by both xed eects and
random eects [54].
6.4 alitative Data Analysis
We conducted a thematic analysis of interview data to deepen understanding of the participants’ behaviors during
the eld study. Two authors collaboratively performed anity diagramming using ATLAS.ti Cloud
2
. We rst
conducted an open coding process in which codes were assigned to signicant instances and references. This
was performed with repeated iterations until consensus was reached between authors. We examined our coding
schemes and analyzed relevant quotes to build rich descriptions and apposite examples of participants’ behavioral
patterns to corroborate our ndings. In addition to the interview data analysis, we analyzed self-report data
collected during the eld study. The two authors conducted a thematic analysis for free-text responses for the
question, “Why do you (not) stand up and move around for a minute?” to supplement interview data.
7 RESULTS
In this section, we present a result of our regression analysis corresponding to dierent decision stages of the
JIT intervention model. We show dependent variables that have statistically signicant contributions to each
stage. Possible reasons for such contributions are explained with our interviews and self-reports. Fig. 5 describes
a summary of our regression analysis results.
2
https://atlasti.com/cloud/
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:15
Table 4. Results of logistic regression for perception of intervention signal (
∗
p<.05;
∗∗
p<.01;
∗∗∗
p<.001)
Predictors β (SE) z-statistic
95% CI for odds ratio
p
Lower Odds ratio Upper
(intercept) 1.47 (0.35) 4.20 2.18 4.33 8.59 <.001
Ongoing task
Class/meeting –0.04 (0.24) –0.17 0.59 0.96 1.55 .862
Conversing –0.08 (0.30) –0.27 0.51 0.92 1.67 .789
Calling/texting –0.11 (0.51) –0.22 0.33 0.89 2.44 .824
Working/studying 0.45 (0.18) 2.46 1.10 1.57 2.26 .014
∗
Driving –0.39 (0.95) –0.41 0.10 0.67 4.34 .678
Eating –0.70 (0.25) –2.84 0.30 0.49 0.80 .005
∗∗
Resting/relaxing –0.56 (0.21) 2.64 1.16 1.76 2.67 .008
∗∗
Gaming –0.53 (0.26) –2.06 0.36 0.59 0.98 .040
∗
Video watching –0.91 (0.24) 3.74 1.54 2.48 4.00 <.001
∗∗∗
Getting ready for bed 1.02 (0.46) 2.23 1.13 2.79 6.86 .026
∗
Right after waking up –0.76 (0.51) –1.49 0.17 0.47 1.27 .136
Location
Home 0.01 (0.23) 0.05 0.65 0.67 1.58 .959
Work 0.36 (0.24) 1.48 0.89 1.01 2.31 .138
Restaurant/Cafe 0.05 (0.29) 0.18 0.60 1.44 1.86 .857
Vehicle –0.30 (0.75) –0.40 0.74 1.05 3.20 .689
Social setting
Social -0.35 (0.16) -2.21 0.52 0.71 0.96 .027
∗
Level of focus –0.23 (0.06) –3.65 0.70 0.79 0.90 <.001
∗∗∗
Level of fatigue –0.03 (0.05) –0.54 0.87 0.97 1.08 .590
7.1 RQ1. Factors Relevant to Perception of Intervention Signals
We rst examined how the perception of intervention prompts were related to contextual factors and cogni-
tive/physical states. Among 3,163 valid responses, we excluded responses marked as sleeping (n=565), because
the participants did not perceive intervention prompts while sleeping. One predictor, which can completely
predict the dependent variable, gives the largest standard error, leading to a misinterpretation of the model. The
goodness-of-t is .067 (marginal R
2
) and .425 (conditional R
2
). The regression result is shown in Table 4.
7.1.1 Contextual Factors Relevant to Perception. We found that participants signicantly better perceived the
intervention signals when they engaged in working/studying (
β =
0
.
45,
OR =
1
.
57,
p = .
014), resting/relaxing
(
β =
0
.
56,
OR =
1
.
76,
p = .
008), video watching (
β =
0
.
91,
OR =
2
.
48,
p < .
001), and getting ready for bed
(
β =
1
.
02,
OR =
2
.
79,
p = .
026). The possible reasons for better perception were that our participants often held or
checked their smartphones during those tasks. For example, participants commented in self-reports as, “watching
YouTube videos with my smartphone” [P10], “watching TV and doing something with a smartphone” [P22], and
“using my smartphone and about to go sleep” [P22].
7.1.2 Contextual Factors Relevant to Missing. When participants were eating (
β = −
0
.
70,
OR =
0
.
49,
p = .
005)
and playing games (
β = −
0
.
53,
OR =
0
.
59,
p = .
040), intervention signals were unlikely to be perceived. In the
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:16 • W. Choi et al.
Table 5. Results of logistic regression for perceived availability (
∗
p<.05;
∗∗
p<.01;
∗∗∗
p<.001)
Predictors β (SE) z-statistic
95% CI for odds ratio
p
Lower Odds ratio Upper
(intercept) 0.21 (0.35) 0.58 0.62 1.23 2.45 .559
Ongoing task
Class/meeting –3.01 (0.33) –9.03 0.03 0.05 0.09 <.001
∗∗∗
Conversing –0.21 (0.31) –0.68 0.44 0.81 1.48 .495
Calling/texting –0.70 (0.41) –1.71 0.22 0.50 1.11 .088
Working/studying 1.70 (0.22) 7.63 3.54 5.48 8.48 <.001
∗∗∗
Eating –0.62 (0.28) –2.21 0.31 0.54 0.93 .027
∗
Resting/relaxing 1.46 (0.30) 4.85 2.38 4.28 7.71 <.001
∗∗∗
Gaming 0.17 (0.37) 0.47 0.58 1.19 2.45 .635
Video watching 1.01 (0.26) 3.81 1.63 2.74 4.61 <.001
∗∗∗
Getting ready for bed –0.83 (0.37) –2.23 0.21 0.44 0.91 .026
∗
Right after waking up 1.51 (0.96) 1.58 0.69 4.54 9.81 .115
Location
Home 1.67 (0.23) 7.33 3.40 5.30 8.28 <.001
∗∗∗
Work 1.24 (0.26) 4.76 2.07 3.44 5.72 <.001
∗∗∗
Restaurant/Cafe 0.87 (0.30) 2.91 1.33 2.39 4.30 .004
∗∗
Vehicle –3.54 (0.67) –5.28 0.01 0.03 0.11 <.001
∗∗∗
Social setting
Social -0.49 (0.21) -2.29 0.41 0.62 0.93 .022
∗
Level of focus –0.44 (0.08) –5.56 0.55 0.64 0.75 <.001
∗∗∗
Level of fatigue 0.05 (0.08) 0.70 0.91 1.06 1.23 .481
interview, P12 said, “I played a game mostly in an Internet cafe. It was too noisy and distracting. Also, I had to chat
with friends to play the game.” Additionally, our participants denitely missed signals when they were sleeping.
Participants were more likely to miss intervention signals when they were in social settings (
β = −
0
.
35,
OR =
0
.
71,
p = .
027). This might be partly explained using the perceptual load theory, where the perceptual system
automatically consumes the limited perceptual capacity to process incoming information, and the information is
missed when the capacity is exhausted [
41
]. The social setting likely accompanies interaction with others which
might require higher demands on the perceptual system than solitary activities. Thus, our participants might be
less likely to perceive the intervention signals.
7.1.3 Eects of Level of Focus and Fatigue on Perception/Missing. The level of focus has a statistically signicant
contribution to the signal being missing (
β = −
0
.
23,
OR =
0
.
79,
p < .
001). This can be explained by the fact that
the higher working memory load (possibly leading to a higher level of focus) attenuates to process irrelevant
stimuli (i.e., smartphone notications from our service) [70], resulting in missing prompts.
7.2 RQ2. Factors Relevant to Perceived Availability for Active Breaks
We now examine how participants’ availability for engaging in active breaks was related to contextual factors
and cognitive/physical states. Among the 2,051 perceived responses, we exclude 18 responses that mentioned
types of ongoing tasks marked as driving, because those responses were answered as unavailable. The multilevel
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:17
regression analysis was conducted with remaining 2,033 responses, as shown in Table 5. The marginal and
conditional R
2
are .378 and .571, respectively.
7.2.1 Contextual Factors Relevant to Availability. For types of ongoing tasks, we found that three tasks (i.e.,
working/studying (
β =
1
.
70,
OR =
5
.
48,
p < .
001), resting/relaxing (
β =
1
.
46,
OR =
4
.
28,
p < .
001), and video
watching (
β =
1
.
01,
OR =
2
.
74,
p < .
001)), show a statistically signicant contribution to the availability to engage
in active breaks. For location, participants were likely available to engage in active breaks at home (
β =
1
.
67,
OR =
5
.
30,
p < .
001), work (
β =
1
.
24,
OR =
3
.
44,
p < .
001), and restaurant/cafe (
β =
0
.
87,
OR =
2
.
39,
p = .
004).
Because those contextual factors accounted for a greater portion of possible contexts in our self-report data
(i.e., 58.4% and 95.3% of responses for types of ongoing tasks and location, respectively), we expect participants
believed they were available to perform active breaks in most contexts.
7.2.2 Contextual Factors Relevant to Unavailability. We found that participants were unavailable to take an active
break during class/meeting (
β = −
3
.
91,
OR =
0
.
05,
p < .
001), eating (
β = −
0
.
62,
OR =
0
.
54,
p = .
027), and getting
ready for bed (
β = −
0
.
83,
OR =
0
.
44,
p = .
026). Additionally, all driving tasks were reported as unavailable. Our
interviews show possible reasons for unavailability. In a class/meeting, participants mostly were too conscious of
others. In the interview, P12 noted, “If I were to stand up [in a class], I would be spotted, and beyond that, I would be
even asked to explain why I stand up.” While eating, most participants did not want to be disturbed, whereas there
was no social pressure. For example, P11 noted in the interview, “Doesn’t it look strange to stand up while eating? I
won’t stop eating to stand.” For getting ready for bed, our participants felt it bothersome to take active breaks and
marked in as unavailable As P20 answered in his self-reports, “I was tired, so I lay down to take a nap and was
using my phone right before sleeping on my be d. Then I received [the intervention signal]; it was b othersome.”
The regression results show that our participants were less likely to be available when they were in social
settings (
β = −
0
.
49,
OR =
0
.
62,
p = .
022). In particular, when participants were performing activities together,
they were considered unavailable, because standing appeared to inappropriate. In the interview, P20 said, “It
is weird to suddenly stand up in the middle of conversing while drinking at the bar.” Another participant said, “I
don’t even answer phone calls when I am with a professor. I just hang up.” [P19] Additionally, we found that, in
some cases, participants did not want to interrupt social activities. For the watching activity, P23 said, “At that
moment, I could not stop, because I was watching a movie [at home] with my wife.” Furthermore, our participants
almost unanimously said that they were not available for active breaks while in vehicles (
β = −
3
.
54,
OR =
0
.
03,
p < .001).
7.2.3 Eects of Level of Focus and Fatigue on Availability/Unavailability. The level of focus shows statistically
signicant contribution to unavailability (
β = −
0
.
44,
OR =
0
.
64,
p < .
001). Whereas we showed that participants
were more likely to stand up while working, there were also “unavailable” responses because of users’ current
focus on tasks at hand. In the interview, P18 mentioned, “Once I have concentrated on my work, the ow of work
should not be interrupted.”
7.3 RQ3. Factors Relevant to Adherence to Active Breaks
Our participants perceived intervention prompts and said that they were available to take active breaks, but
that it did not always guarantee that they actually took active breaks. There were 1,657 responses (marked as
perceived and available) out of which 589 prompts led to actual active breaks, leading to a success rate of 35.5%.
We perform multilevel regression with 1,657 responses to identify factors related to active break adherence, as
shown in Table 6. The goodness-of-t of the model shows .145 for the marginal
R
2
and .373 for the conditional
R
2
.
7.3.1 Contextual Factors Relevant to Adherence. Our regression analysis shows participants were more likely
to take active breaks during conversations (
β =
1
.
00,
OR =
2
.
71,
p = .
010) or right after waking up (
β =
2
.
42,
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:18 • W. Choi et al.
Table 6. Results of logistic regression for adherence to active breaks (
∗
p<.05;
∗∗
p<.01;
∗∗∗
p<.001)
Predictors β (SE) z-statistic
95% CI for odds ratio
p
Lower Odds ratio Upper
(intercept) –0.41 (0.42) –0.98 0.29 0.66 1.50 .326
Ongoing task
Class/meeting –1.18 (0.75) –1.56 0.07 0.31 1.36 .120
Conversing 1.00 (0.39) 2.58 1.27 2.71 5.78 .010
∗
Calling/texting 0.21 (0.57) 0.37 0.40 1.23 3.76 .713
Working/studying 0.20 (0.21) 0.97 0.82 1.22 1.83 .330
Eating 0.07 (0.34) 0.21 0.55 1.07 2.08 .833
Resting/relaxing 0.08 (0.23) 0.37 0.70 1.09 1.69 .713
Gaming –0.55 (0.44) –1.25 0.24 0.58 1.37 .211
Video watching 0.16 (0.24) 0.68 0.74 1.17 1.87 .499
Getting ready for bed –3.36 (0.95) –3.53 0.01 0.03 0.22 <.001
∗∗∗
Right after waking up 2.42 (0.58) 4.17 3.61 11.26 35.11 <.001
∗∗∗
Location
Home 0.05 (0.32) 0.14 0.55 1.05 1.98 .890
Work 0.37 (0.33) 1.12 0.76 1.44 2.74 .263
Restaurant/Cafe –0.11 (0.37) –0.31 0.43 0.89 1.86 .759
Vehicle 0.88 (1.12) 0.78 0.27 2.41 21.77 .433
Social setting
Social -0.02 (0.15) -0.15 0.73 0.98 1.31 .877
Level of focus –0.45 (0.07) –6.90 0.56 0.64 0.72 <.001
∗∗∗
Level of fatigue –0.22 (0.06) –3.51 0.71 0.81 0.91 <.001
∗∗∗
OR =
11
.
26,
p < .
001). This result somewhat contradicts our previous results, because a conversation is a social
behavior, and active breaks hinder social interactions (thereby lowering availability). From the exit-interviews
and self-report responses, we found several reasons for this discrepancy. First, conversing activities that were
transitioned to active breaks happened to be simple chat session and were not serious discussions, as in a formal
meeting. Our participants could easily stop chatting for active breaks. Alarms provided them with the excuse for
nishing a conversation, particularly when they had planned follow-up activities. In the participants’ self-reports,
P23 noted, “I was chit-chatting with my friends in a cafe [after lunch]. I was so full, and I wanted to move around.”
P10 explained why he stood up, by saying “I was chit-chatting with my colleague in the lab, and I was planning to
go for a meal.” In the case of right after waking up, our participants mostly took active breaks to get out of the
bed and prepare other activities. P14 commented in her self-report, “I got up to go to the kitchen to have breakfast.”
P10 stated, “In my dormitory, I got up for washing.”
Besides contextual factors, our interview analysis shows that participants took active breaks for the purpose
of mental refreshment. P20 said, “Sometimes it is boring to study. I’d like to stand when studying.” Additionally,
health beliefs in active breaks are positive motivators of adherence. P21 said, “I often received notications when I
was watching TV, during online lectures, or when watching YouTube videos. I tried to keep moving. If there were no
alarms, I would have mostly continue d sitting without realizing that my legs hurt. I like the fact that this app helps
me keep moving my legs.”
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:19
Table 7. Physical activities during active breaks
Type Example N = 589
Visiting a restroom Urination and defecation 200 (34.0%)
Water drinking To sip water 95 (16.1%)
Moving to other places To commute to work/school, to go to the hospital 83 (14.1%)
Doing chores Dish-washing, cleaning 81 (13.8%)
Going for a walk Walking around 71 (12.1%)
Stretching/exercising Stretching neck 55 (9.3%)
Bathing/washing To wash face, to brush teeth 50 (8.5%)
Miscellaneous To turn light o, to change clothes 22 (3.7%)
7.3.2 Contextual Factors Relevant to Rejection. Participants were less likely to take active breaks when they were
about to go to bed (
β = −
3
.
36,
OR =
0
.
03,
p < .
001). Interestingly, this activity was also frequently marked as
unavailable, whereas our participants sometimes judged that they would be available for moving. Despite such
availability judgments, our participants tended to ignore notications, because they were ready to asleep and
wanted to stay in bed. For example, P3 answered in her self-reports, “I was in my room alone. I was about to sleep
with lights o, web surng in the bed.”
7.3.3 Eects of Level of Focus and Fatigue on Adherence/Rejection. The regression results show that our partici-
pants were less likely to take active breaks when the level of focus or the level of fatigue was high (
β = −
0
.
45,
OR =
0
.
64,
p < .
001, and
β = −
0
.
22,
OR =
0
.
81,
p < .
001, respectively). Whereas they perceived the alarms
and believe that they would be available, it seems that performing active breaks is highly dependent on their
levels of focus and fatigue. In the interview, P14 wanted to continue concentrating on work, by saying “I might
lose concentration if I do (an active break) while working. Thus, I just kept working.” Another participant also
commented, “The alarm rang when I was really focused on writing a report (at work). I was working alone, so I was
able to stand up. But I did not want to break the ow, so I didn’t stand up.” [P7] Regarding level of fatigue, P18
stated, “After working hard during the weekdays, I felt burned-out during the weekend. I want to lie down or use
computers to take some rest. Anyway, I can stand up after receiving an alarm message, but...” P7 also said that he
did not take active breaks when watching TV dramas and getting rest, “Because, actually, it was so tiring and
troublesome.”
7.4 RQ4: Physical Activities Performed during Active Breaks
Table 7) shows physical activities performed during active breaks. Interestingly, our participants mostly took
active breaks for physiological needs (e.g., 34.2% for visiting a restroom and 16.1% for drinking water), rather
than precise health-related reasons (e.g., 9.3% for stretching/exercising). Indeed, prompt delivery worked as a
trigger for the transition between routine and planned behaviors. In the interview, P4 said, “I have postponed
to go to a restroom because I felt lazy. But when the smartphone alarm sounds, I visited the restroom while I was
standing up and walking around.”
8 DISCUSSION
JIT interventions are known to be complex processes involving human information processing and behavior
controlling for adherence [
52
]. Investigating how people respond to incoming JIT support messages is of great
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:20 • W. Choi et al.
interest to the Ubicomp community because of its close relationship with interruptibility research (e.g., nding
opportune moments for delivering notications). Building upon prior studies of interruptibility [
74
,
75
], our
work deepened the understanding of receptivity by proposing a JIT intervention stage model that detailed
receptivity in four stages: perception, availability, adherence, and performance. After building a mobile JIT service
to prevent prolonged sedentary behaviors, we conducted regression analyses with the self-reported contexts and
cognitive/physical states collected over 3 weeks. Then, we corroborated our ndings via in-depth interviews.
Our results showed that the level of focus had a negative relationship across all stages, and fatigue was one of
the major factors aecting adherence. Whereas prior JIT studies only considered simple cases for availability
(e.g., already performing target behaviors or in unsafe situations, such as driving) [
37
], our work showed that
availability was multifaceted and context-dependent. Unlike an oce setting, we showed that mobile intervention
must carefully consider various ongoing tasks at dierent places. As indicated in a prior work [
45
], participants
perform diverse physical activities during active breaks. From our ndings, we discuss several design implications.
8.1 Considering “Available, But Not Adhering To” Cases
Whereas participants said that they were available, two-thirds of JIT prompts failed to inspire adherence to the
behaviors suggested, owing to higher levels of ongoing task engagement and physical fatigue or getting ready
for bed. Such results highlight that it is critical to better dierentiate availability and adherence. When users do
not adhere to JIT support (assuming it is perceived), prior studies on interruptibility that considered only nal
resulting responses did not dierentiate whether users were available or did not want to perform the behavior
suggested. Dierent decisions underlying nal decisions provide great opportunities for building persuasive
systems for promoting health behaviors. For example, if there are limited opportunities for prompting users to
limit user burdens and prevent disengagement of interventions [
43
], we can better prioritize intervention contexts
to times when users are available. Additionally, given available contexts, we can more rigorously test eects of
dierent contents on JIT support (e.g., walking vs. anti-sedentary suggestions) on adherence to interventions and
health-related outcomes [
37
]. Considering available contexts, we can exquisitely design intelligent interventions
to increase levels of adherence by dynamically changing persuasive elements (e.g., incentives) or learning users’
preference for suggestions [62].
8.2 Providing Contextually Tailored and Personalized Guidelines
Our ndings on factors relevant to availability parallels six elements of simplicity in FBM: time, money, physical
eort, brain cycles, social deviance, and non-routine [
24
]. Our participants believed they would unavailable to
stand up and move around when such behavior goes against the norm (e.g., standing up during a meeting or a
class), is not routine (e.g., standing up while getting ready for bed or eating), and disrupts their concentration.
Such results imply that we can enhance availability by providing dierent behavioral guidelines with simplicity
elements. For example, JIT health intervention suggests collaborative behaviors resulting in certain health benets,
such as walking meetings [
2
]. This may establish shared norms about the target behaviors so that social deviance
may be reduced.
Additionally, participants’ practices during active breaks suggest interesting implications. Our participants
tended to engage in their routine tasks accompanying physical activities, such as visiting a restroom or sipping
water. Such ndings highlight that we can provide dierent behavioral guidelines resulting in similar health
outcomes regarding users’ routine behaviors and contexts. For example, we can deliver JIT prompts that suggest
to getting a drink of water or visiting a restroom on a regular basis. Whereas these suggestions seem irrelevant
to sedentary behaviors, they would provide similar health outcomes if users would adhere to suggestions. Such
varying suggestions could mitigate habituation to interventions [43].
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:21
8.3 Inferring Receptivity of JIT Support
Our JIT stage model provides an opportunity to separately model perception, availability, and adherence. In
addition, our regression analysis showed that contextual factors and cognitive/physical states are good predictors
of each decision point. Leveraging prior Ubicomp literature on context awareness, such as activity recognition
[
20
], location tracking [
35
], emotion sensing [
11
], and even circadian rhythms [
1
,
46
], we can automatically detect
opportune moments for JIT support. Specically, our ndings on factors relevant to availability indicate that
ocial and important work schedules can negatively inuence on availability. Thus, users’ calendar informations
can be used to predict availability [
44
]. Besides passive sensing and self-reports, we can embed various small
tasks as part of typical user interactions to infer users’ status (e.g., alertness tracking with vigilance tasks) as in
cognition-aware systems [19].
9 LIMITATIONS AND FUTURE WORK
There were several limitations of the present study. Our intervention stage model may not fully capture the
real cognitive process of human beings when they are given JIT support. The model basically assumes that a user
goes through a sequence of micro-decisions when reacting to a given JIT support message. While the perception
stage is obviously the rst decision point, the other two decisions (i.e., availability and adherence) may happen
either successively (but even in the opposite order) or in parallel. The current work hypothesized that these
steps exist, and we attempted to validate that through self-reports collection and statistical analysis. According
to the dual-process accounts of reasoning, an individual’s reasoning for action is governed by System 1 (i.e.,
fast, automatic, emotional reasoning) and System 2 (i.e., slow, conscious, controlled judgments) [
21
]. Automatic
and controlled cognitive operations that compete with one another in determining behavioral choices. Our
self-reports (possibly done when they are available to answer) could have made the participants switch to System
2, which helped them to carefully reect upon their decision making processes. In practice, however, at the time
of receiving a JIT support message, it may be possible that users’ reasoning could be dominated by System 1. For
example, users who are less motivated and feel tired may immediately reject the suggestion without carefully
assessing their availability. Even in this case, there may be no clear distinction between the availability assessment
and adherence determination stages. Further studies are required in order to better understand human reasoning
in JIT intervention. One interesting future study would be comparing user responses based on answering delay,
assuming that immediate responses are more inuenced by System 1 than belated responses. Despite such
methodological limitations, our eorts provided a pragmatic framework that helps researchers to understand the
receptivity to JIT support. Our ndings imply how ubiquitous technologies can better dierentiate availability
and adherence, possibly leading to advanced JIT intervention design that reduces the user’s burden and provides
highly motivated suggestions.
Another limitation is that our model only details decisions over a single JIT intervention. However, for
successful health behavior treatments, it is important to achieve retention of JIT intervention. Prior studies have
shown that retention reects motivational issues and intervention fatigue issues [
53
]. Long-term user studies that
model those variables will help us better understand receptivity to JIT intervention. Furthermore, this work only
considers a limited number of factors relevant to receptivity to JIT support. Although our results clearly highlight
contextual factors contributing to the perception and availability stages, there is still a lack of understanding
about how motivational or other potential factors impact adherence to given JIT support. Because JIT support
can increase motivation itself (i.e., spark as trigger in FBM [
24
]), further studies should investigate motivation
that both an individual originally has and that JIT intervention promotes.
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:22 • W. Choi et al.
10 CONCLUSION
We extended previous interruptibility models to deepen our understanding of receptivity for mobile JIT interven-
tion. The extended stage model comprised four stages: message perception, availability assessment, adherence
determination, and actual behavior execution. We built a mobile JIT intervention system to prevent prolonged
sedentary behaviors and collected self-reported context and decision data from a 3-week eld trial. We systemati-
cally explored various contextual factors relevant to each stage outcome using quantitative and qualitative data
analyses. We found that availability for JIT intervention is multifaceted and context-dependent, and contextual
factors aecting availability signicantly diered from adherence. Mobile JIT health intervention is prevalent
nowadays. We believe that our work makes an important step toward deepening the eld’s understanding of
receptivity for these technologies. Our ndings also provide novel opportunities for building less disruptive, but
more eective methods for mobile JIT health intervention.
ACKNOWLEDGMENTS
This work was partly supported by the Institute for Information & Communications Technology Promotion
(IITP) grant funded by the Korea government (MSIT) (No. R7124-16-0004, Development of Intelligent Interaction
Technology Based on Context Awareness and Human Intention Understanding) and the Next-Generation Infor-
mation Computing Development Program through the National Research Foundation of Korea (NRF) funded by
the Ministry of Science and ICT (NRF-2017M3C4A7083534).
REFERENCES
[1]
Saeed Abdullah, Mark Matthews, Elizabeth L. Murnane, Geri Gay, and Tanzeem Choudhury. 2014. Towards Circadian Computing:
“Early to Bed and Early to Rise” Makes Some of Us Unhealthy and Sleep Deprived. In Proceedings of the 2014 ACM International Joint
Conference on Pervasive and Ubiquitous Computing (UbiComp ’14). ACM, 673–684. https://doi.org/10.1145/2632048.2632100
[2]
A. Ahtinen, E. Andreje, C. Harris, and K. Väänänen. 2017. Let’s Walk at Work: Persuasion Through the Brainwolk Walking Meeting
App. In Proceedings of the 21st International Academic Mindtrek Conference (AcademicMindtrek ’17). ACM, 73–82. https://doi.org/10.
1145/3131085.3131098
[3]
Taleb A. Alkhajah, Marina M. Reeves, Elizabeth G. Eakin, Elisabeth A.H. Winkler, Neville Owen, and Genevieve N. Healy. 2012. Sit-Stand
Workstations: A Pilot Intervention to Reduce Oce Sitting Time. American Journal of Preventive Medicine 43, 3 (Sept. 2012), 298–303.
https://doi.org/10.1016/j.amepre.2012.05.027
[4]
Daniel Avrahami and Scott E. Hudson. 2006. Responsiveness in Instant Messaging: Predictive Models Supporting Inter-personal
Communication. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ’06). ACM, 731–140. https:
//doi.org/10.1145/1124772.1124881
[5]
Sangwon Bae, Anind K. Dey, and Carissa A. Low. 2016. Using Passively Collected Sedentary Behavior to Predict Hospital Readmission.
In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing (UbiComp ’16). ACM, 616–621.
https://doi.org/10.1145/2971648.2971750
[6]
Avner Ben-Ner, Darla J. Hamann, Gabriel Koepp, Chimnay U. Manohar, and James Levine. 2014. Treadmill Workstations: The Eects of
Walking while Working on Physical Activity and Work Performance. PLoS ONE 9, 2 (Feb. 2014), e88620. https://doi.org/10.1371/journal.
pone.0088620
[7]
Aviroop Biswas, Paul I. Oh, Guy E. Faulkner, Ravi R. Bajaj, Michael A. Silver, Marc S. Mitchell, and David A. Alter. 2015. Sedentary Time
and Its Association With Risk for Disease Incidence, Mortality, and Hospitalization in Adults. Annals of Internal Medicine 162, 2 (Jan.
2015), 123–132. https://doi.org/10.7326/M14-1651
[8]
Dale S. Bond, J. Graham Thomas, Hollie A. Raynor, Jon Moon, Jared Sieling, Jennifer Trautvetter, Tiany Leblond, and Rena R. Wing.
2014. B-MOBILE - A Smartphone-Based Intervention to Reduce Sedentary Iime in Overweight/Obese Individuals: A Within-Subjects
Experimental Trial. PLoS ONE 9, 6 (2014). https://doi.org/10.1371/journal.pone.0100821
[9]
Andreas Braun, Ingrid Schembri, and Sebastian Frank. 2015. ExerSeat - Sensor-Supported Exercise System for Ergonomic Microbreaks.
In Ambient Intelligence. Springer International Publishing, 236–251. https://doi.org/10.1007/978-3-319-26005-1_16
[10]
Scott A. Cambo, Daniel Avrahami, and Matthew L. Lee. 2017. BreakSense: Combining Physiological and Location Sensing to Promote
Mobility during Work-Breaks. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems (CHI ’17). ACM,
3595–3607. https://doi.org/10.1145/3025453.3026021
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:23
[11]
Bokai Cao, Lei Zheng, Chenwei Zhang, Philip S. Yu, Andrea Piscitello, John Zulueta, Olu Ajilore, Kelly Ryan, and Alex D. Leow. 2017.
DeepMood: Modeling Mobile Phone Typing Dynamics for Mood Detection. In Proceedings of the 23rd ACM SIGKDD International
Conference on Knowledge Discovery and Data Mining (KDD ’17). ACM, 747–755. https://doi.org/10.1145/3097983.3098086
[12]
Lucas J. Carr, Kristina Karvinen, Mallory Peavler, Rebecca Smith, and Kayla Cangelosi. 2013. Multicomponent Intervention to Reduce Daily
Sedentary Time: A Randomised Controlled Trial. BMJ Open 3, 10 (Oct. 2013), e003261. https://doi.org/10.1136/bmjopen-2013-003261
[13]
Yung-Ju Chang and John C. Tang. 2015. Investigating Mobile Users’ Ringer Mode Usage and Attentiveness and Responsiveness to
Communication. In Proceedings of the 17th International Conference on Human-Computer Interaction with Mobile Devices and Services
(MobileHCI ’15). ACM, 6–15. https://doi.org/10.1145/2785830.2785852
[14]
Woohyeok Choi, Jeongmin Oh, Darren Edge, Joohyun Kim, and Uichin Lee. 2016. SwimTrain: Exploring Exergame Design for Group
Fitness Swimming. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems (CHI ’16). ACM, 1692–1704.
https://doi.org/10.1145/2858036.2858579
[15]
Woohyeok Choi, Jeungmin Oh, Taiwoo Park, Seongjun Kang, Miri Moon, Uichin Lee, Inseok Hwang, Darren Edge, and Junehwa
Song. 2016. Designing Interactive Multiswimmer Exergames. ACM Transactions on Sensor Networks 12, 3 (July 2016), 1–40. https:
//doi.org/10.1145/2888399
[16]
Sunny Consolvo, Katherine Everitt, Ian Smith, and James A. Landay. 2006. Design Requirements for Technologies That Encourage
Physical Activity. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ’06). ACM, 457–466. https:
//doi.org/10.1145/1124772.1124840
[17]
Sunny Consolvo, Ryan Libby, Ian Smith, James A. Landay, David W. McDonald, Tammy Toscos, Mike Y. Chen, Jon Froehlich, Beverly
Harrison, Predrag Klasnja, Anthony LaMarca, and Louis LeGrand. 2008. Activity Sensing in the Wild: A Field Trial of Ubit Garden. In
Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ’08). ACM, 1797–1806. https://doi.org/10.1145/
1357054.1357335
[18]
Ding, Xu, Wang, Chen, Thind, and Zhang. 2016. WalkMore: Promoting Walking with Just-In-Time Context-Aware Prompts. In 2016
IEEE Wireless Health (WH ’16). IEEE, 1–8. https://doi.org/10.1109/WH.2016.7764558
[19]
Tilman Dingler, Albrecht Schmidt, and Tonja Machulla. 2017. Building Cognition-Aware Systems: A Mobile Toolkit for Extracting
Time-of-Day Fluctuations of Cognitive Performance. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies
1, 3 (Sept. 2017), 47:1–47:15. https://doi.org/10.1145/3132025
[20]
Genevieve Dunton, Eldin Dzubur, Keito Kawabata, Brenda Yanez, Bin Bo, and Stephen Intille. 2014. Development of a Smartphone
Application to Measure Physical Activity Using Sensor-Assisted Self-Report. Frontiers in Public Health 2 (March 2014), 12. https:
//doi.org/10.3389/fpubh.2014.00012
[21]
Jonathan St.B.T. Evans. 2003. In Two Minds: Dual-Process Accounts of Reasoning. Trends in Cognitive Sciences 7, 10 (Oct. 2003), 454–459.
https://doi.org/10.1016/J.TICS.2003.08.012
[22]
Joel E. Fischer, Chris Greenhalgh, and Steve Benford. 2011. Investigating Episodes of Mobile Phone Activity As Indicators of Opportune
Moments to Deliver Notications. In Proceedings of the 13th International Conference on Human Computer Interaction with Mobile Devices
and Services (MobileHCI ’11). ACM, 181. https://doi.org/10.1145/2037373.2037402
[23]
Joel E. Fischer, Nick Yee, Victoria Bellotti, Nathan Good, Steve Benford, and Chris Greenhalgh. 2010. Eects of Content and Time of
Delivery on Receptivity to Mobile Interruptions. In Proceedings of the 12th International Conference on Human Computer Interaction with
Mobile Devices and Services (MobileHCI ’10). ACM, 103–112. https://doi.org/10.1145/1851600.1851620
[24]
B. J. Fogg. 2009. A Behavior Model for Persuasive Design. In Proceedings of the 4th International Conference on Persuasive Technology
(Persuasive ’09). ACM, New York, New York, USA, 40:1–40:7. https://doi.org/10.1145/1541948.1541999
[25]
Jutta Fortmann, Tim Stratmann, Susanne Boll, Benjamin Poppinga, and Wilko Heuten. 2013. Make Me Move at Work! An Ambient
Light Display to Increase Physical Activity. In 2013 7th International Conference on Pervasive Computing Technologies for Healthcare and
Workshops. IEEE, 274–277. https://doi.org/10.4108/icst.pervasivehealth.2013.252089
[26]
Derek Foster, Conor Linehan, and Shaun Lawson. 2010. Motivating Physical Activity at Work: Using Persuasive Social Media Extensions
for Simple Mobile Devices. CEUR Workshop Proceedings 690 (2010), 11–14. https://doi.org/10.1145/1930488.1930510
[27]
Nicholas D. Gilson, Norman Ng, Toby G. Pavey, Gemma C. Ryde, Leon Straker, and Wendy J. Brown. 2016. Project Energise: Using
Participatory Approaches and Real Time Computer Prompts to Reduce Occupational Sitting and Increase Work Time Physical Activity
in Oce Workers. Journal of Science and Medicine in Sport 19, 11 (2016), 926–930. https://doi.org/10.1016/j.jsams.2016.01.009
[28]
Genevieve N. Healy, David W. Dunstan, Jo Salmon, Ester Cerin, Jonathan E. Shaw, Paul Z. Zimmet, and Neville Owen. 2008. Breaks in
Sedentary Time: Benecial Associations with Metabolic Risk. Diabetes Care 31, 4 (April 2008), 661–666. https://doi.org/10.2337/dc07-2046
[29]
Sen H. Hirano, Robert G. Farrell, Catalina M. Danis, and Wendy A. Kellogg. 2013. WalkMinder: Encouraging an Active Lifestyle Using
Mobile Phone Interruptions. In CHI ’13 Extended Abstracts on Human Factors in Computing Systems (CHI EA ’13). ACM, 1431–1436.
https://doi.org/10.1145/2468356.2468611
[30]
Eric Horvitz, Pau Koch, Carl M. Kadie, and Andy Jacobs. 2002. Coordinate: Probabilistic Forecasting of Presence and Availability. In
Proceedings of the Eighteenth Conference on Uncertainty in Articial Intelligence (UAI ’02). Morgan Kaufmann Publishers Inc., 224–233.
http://dl.acm.org/citation.cfm?id=2073876.2073903
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:24 • W. Choi et al.
[31]
Hayeon Jeong, Heepyung Kim, Rihun Kim, Uichin Lee, and Yong Jeong. 2017. Smartwatch Wearing Behavior Analysis: A Longitudinal
Study. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 1, 3 (Sept. 2017), 60:1–60:31. https://doi.org/10.1145/3131892
[32]
Dinesh John, Dixie L. Thompson, Hollie Raynor, Kenneth M. Bielak, and David R. Bassett. 2010. Eects of Treadmill Workstations as a
Worksite Physical Activity Intervention in Overweight and Obese Oce Workers. Medicine & Science in Sports & Exercise 42 (May 2010),
38. https://doi.org/10.1249/01.MSS.0000384859.60808.5c
[33]
Darla E. Kendzor, Kerem Shuval, Kelley Pettee Gabriel, Michael S. Businelle, Ping Ma, Robin R. High, Erica L. Cuate, Insiya B. Poonawalla,
Debra M. Rios, Wendy Demark-Wahnefried, Michael D. Swartz, and David W. Wetter. 2016. Impact of a Mobile Phone Intervention to
Reduce Sedentary Behavior in a Community Sample of Adults: A Quasi-Experimental Evaluation. Journal of medical Internet research
18, 1 (2016), e19. https://doi.org/10.2196/jmir.5137
[34]
Auk Kim, Woohyeok Choi, Jungmi Park, Kyeyoon Kim, and Uichin Lee. 2018. Interrupting Drivers for Interactions: Predicting Opportune
Moments for In-vehicle Proactive Auditory-verbal Tasks. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2, 4 (Dec. 2018),
175:1–175:28. https://doi.org/10.1145/3287053
[35]
Donnie H. Kim, Younghun Kim, Deborah Estrin, and Mani B. Srivastava. 2010. SensLoc: Sensing Everyday Places and Paths Using
Less Energy. In Proceedings of the 8th ACM Conference on Embedded Networked Sensor Systems (SenSys ’10). ACM, 43–56. https:
//doi.org/10.1145/1869983.1869989
[36]
Predrag Klasnja, Eric B Hekler, Saul Shiman, Audrey Boruvka, Daniel Almirall, Ambuj Tewari, and Susan A Murphy. 2015. Microran-
domized trials: An experimental design for developing just-in-time adaptive interventions. Health psychology : ocial journal of the
Division of Health Psychology, American Psychological Association 34S, 0 (Dec. 2015), 1220–8. https://doi.org/10.1037/hea0000305
[37]
Predrag Klasnja, Shawna Smith, Nicholas J Seewald, Andy Lee, Kelly Hall, Brook Luers, Eric B Hekler, and Susan A Murphy. 2018.
Ecacy of Contextually Tailored Suggestions for Physical Activity: A Micro-randomized Optimization Trial of HeartSteps. Annals of
Behavioral Medicine (Sept. 2018). https://doi.org/10.1093/abm/kay067
[38]
Rafal Kocielnik, Lillian Xiao, Daniel Avrahami, and Gary Hsieh. 2018. Reection Companion: A Conversational System for Engaging
Users in Reection on Physical Activity. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies 2, 2 (July
2018), 70:1–70:26. https://doi.org/10.1145/3214273
[39]
Kara A. Latorella. 1999. Investigating Interruptions: Implications for Flightdeck Performance. Technical Report. NASA Langley Research
Center, Hampton, VA United States. https://ntrs.nasa.gov/search.jsp?R=20000004291
[40]
Nilli Lavie. 2010. Attention, Distraction, and Cognitive Control Under Load. Current Directions in Psychological Science 19, 3 (2010),
143–148. https://doi.org/10.1177/0963721410370295
[41]
Nilli Lavie, Aleksandra Hirst, Jan W. de Fockert, and Essi Viding. 2004. Load Theory of Selective Attention and Cognitive Control.
Journal of Experimental Psychology: General 133, 3 (Sept. 2004), 339–354. https://doi.org/10.1037/0096-3445.133.3.339
[42]
Uichin Lee, Kyungsik Han, Hyunsung Cho, Kyong-Mee Chung, Hwajung Hong, Sung-Ju Lee, Youngtae Noh, Sooyoung Park, and John M."
Carroll. 2019. Intelligent Positive Computing with Mobile, Wearable, and IoT Devices: Literature Review and Research Directions. Ad
Hoc Networks 83 (Feb. 2019), 8–24. https://doi.org/10.1016/j.adhoc.2018.08.021
[43]
Peng Liao, Walter Dempsey, Hillol Sarker, Syed Monowar Hossain, Mustafa Al’Absi, Predrag Klasnja, and Susan Murphy. 2018. Just-in-
Time but Not Too Much: Determining Treatment Timing in Mobile Health. Proceedings of the ACM on Interactive, Mobile, Wearable and
Ubiquitous Technologies 2, 4 (Dec. 2018), 179:1–179:21. https://doi.org/10.1145/3287057
[44]
Tom Lovett, Eamonn O’Neill, James Irwin, and David Pollington. 2010. The Calendar as a Sensor: Analysis and Improvement Using Data
Fusion with Social Networks and Location. In Proceedings of the 12th ACM International Conference on Ubiquitous Computing (UbiComp
’10). ACM, 3–12. https://doi.org/10.1145/1864349.1864352
[45]
Yuhan Luo, Bongshin Lee, Donghee Yvette Wohn, Amanda L. Rebar, David E. Conroy, and Eun Kyoung Choe. 2018. Time for Break:
Understanding Information Workers’ Sedentary Behavior Through a Break Prompting System. In Proceedings of the 2018 CHI Conference
on Human Factors in Computing Systems (CHI ’18). ACM, New York, New York, USA, 1–14. https://doi.org/10.1145/3173574.3173701
[46]
Gloria Mark, Yiran Wang, Melissa Niiya, and Stephanie Reich. 2016. Sleep Debt in Student Life: Online Attention Focus, Facebook,
and Mood Gloria. In Procee dings of the 2016 CHI Conference on Human Factors in Computing Systems (CHI ’16). ACM, 5517–5528.
https://doi.org/10.1145/2858036.2858437
[47]
Shelly K McCrady and James A Levine. 2009. Sedentariness at Work: How Much Do We Really Sit? Obesity 17, 11 (Nov. 2009), 2103–2105.
https://doi.org/10.1038/oby.2009.117
[48]
Abhinav Mehrotra, Sandrine R. Müller, Gabriella M. Harari, Samuel D. Gosling, Cecilia Mascolo, Mirco Musolesi, and Peter J. Rentfrow.
2017. Understanding the Role of Places and Activities on Mobile Phone Interaction and Usage Patterns. Procee dings of the ACM on
Interactive, Mobile, Wearable and Ubiquitous Technologies 1, 3 (Sept. 2017), 84:1–84:22. https://doi.org/10.1145/3131901
[49]
Abhinav Mehrotra, Mirco Musolesi, Robert Hendley, and Veljko Pejovic. 2015. Designing Content-Driven Intelligent Notication
Mechanisms for Mobile Applications. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing
(UbiComp ’15). ACM, 813–824. https://doi.org/10.1145/2750858.2807544
[50]
Abhinav Mehrotra, Veljko Pejovic, Jo Vermeulen, Robert Hendley, and Mirco Musolesi. 2016. My Phone and Me: Understanding People’s
Receptivity to Mobile Notications. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems (CHI ’16). ACM,
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
Multi-Stage Receptivity Model for Mobile Just-In-Time Health Intervention • 39:25
1021–1032. https://doi.org/10.1145/2858036.2858566
[51]
Florian Floyd Mueller, Martin R. Gibbs, Frank Vetere, and Darren Edge. 2017. Designing for Bodily Interplay in Social Exertion Games.
ACM Transactions on Computer-Human Interaction 24, 3 (May 2017), 1–41. https://doi.org/10.1145/3064938
[52]
Inbal Nahum-Shani, Eric B Hekler, and Donna Spruijt-Metz. 2015. Building Health Behavior Models to Guide the Development
of Just-In-Time Adaptive Interventions: A Pragmatic Framework. Health Psychologysychology 34S, 0 (Dec. 2015), 1209–19. https:
//doi.org/10.1037/hea0000306
[53]
Inbal Nahum-Shani, Shawna N Smith, Bonnie J Spring, Linda M Collins, Katie Witkiewitz, Ambuj Tewari, and Susan A Murphy. 2016.
Just-in-Time Adaptive Interventions (JITAIs) in Mobile Health: Key Components and Design Principles for Ongoing Health Behavior
Support. Annals of Behavioral Medicine (Sept. 2016). https://doi.org/10.1007/s12160-016-9830-8
[54]
Shinichi Nakagawa and Holger Schielzeth. 2013. A General and Simple Method for Obtaining Rˆ2 from Generalized Linear Mixed-eects
Models. Methods in Ecology and Evolution 4, 2 (Feb. 2013), 133–142. https://doi.org/10.1111/j.2041-210x.2012.00261.x
[55]
Felix Naughton, Sarah Hopewell, Neal Lathia, Rik Schalbroeck, Chloë Brown, Cecilia Mascolo, Andy McEwen, and Stephen Sutton. 2016.
A Context-Sensing Mobile Phone App (Q Sense) for Smoking Cessation: A Mixed-Methods Study. JMIR mHealth and uHealth 4, 3 (Sept.
2016), e106. https://doi.org/10.2196/mhealth.5787
[56]
Neville Owen, Geneviève N Healy, Charles E Matthews, and David W Dunstan. 2010. Too Much Sitting: The Population-Health Science
of Sedentary Behavior. Exercise and sport sciences reviews 38, 3 (July 2010), 105–13. https://doi.org/10.1097/JES.0b013e3181e373a2
[57]
Scott J. Pedersen, Paul D. Cooley, and Casey Mainsbridge. 2014. An e-Health Intervention Designed to Increase Workday Energy
Expenditure by Reducing Prolonged Occupational Sitting Habits. Work 49, 2 (2014), 289–295. https://doi.org/10.3233/WOR-131644
[58]
Veljko Pejovic and Mirco Musolesi. 2014. InterruptMe: Designing Intelligent Prompting Mechanisms for Pervasive Applications. In
Proceedings of the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing (UbiComp ’14). ACM, 897–908.
https://doi.org/10.1145/2632048.2632062
[59]
Martin Pielot, Bruno Cardoso, Kleomenis Katevas, Joan Serrà, Aleksandar Matic, and Nuria Oliver. 2017. Beyond Interruptibility:
Predicting Opportune Moments to Engage Mobile Phone Users. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous
Technologies 1, 3 (Sept. 2017), 91:1–91:25. https://doi.org/10.1145/3130956
[60]
Laura Pina, Ernesto Ramirez, and William Griswold. 2012. Fitbit+: A Behavior-based Intervention System to Reduce Sedentary Behavior.
In Proceedings of the 6th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth ’12). IEEE, 175–178.
https://doi.org/10.4108/icst.pervasivehealth.2012.248761
[61]
Laura Pina, Kael Rowan, Paul Johns, Asta Roseway, Gillian Hayes, and Mary Czerwinski. 2014. In Situ Cues for ADHD Parenting
Strategies Using Mobile Technology. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcar
(PervasiveHealth ’14). ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering), 17–24. https:
//doi.org/10.4108/icst.pervasivehealth.2014.254958
[62]
Mashqui Rabbi, Min Hane Aung, Mi Zhang, and Tanzeem Choudhury. 2015. MyBehavior: Automatic Personalized Health Feedback
from User Behaviors and Preferences using Smartphones. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and
Ubiquitous Computing - UbiComp ’15. ACM, New York, New York, USA, 707–718. https://doi.org/10.1145/2750858.2805840
[63]
Tauhidur Rahman, Mary Czerwinski, Ran Gilad-Bachrach, and Paul Johns. 2016. Predicting “About-to-Eat” Moments for Just-in-
Time Eating Intervention. In Proceedings of the 6th International Conference on Digital Health Conference (DH ’16). ACM, 141–150.
https://doi.org/10.1145/2896338.2896359
[64]
Jun Rekimoto and Hitomi Tsujita. 2014. Inconvenient Interactions: An Alternative Interaction Design Approach to Enrich Our
Daily Activities. In Proce edings of the 2014 International Working Conference on Advanced Visual Interfaces (AVI ’14). ACM, 225–228.
https://doi.org/10.1145/2598153.2598196
[65]
Irwin M. Rosenstock. 1974. The Health Belief Model and Preventive Health Behavior. Health Education Monographs 2, 4 (Dec. 1974),
354–386. https://doi.org/10.1177/109019817400200405
[66]
Sherwood W. Samn and Layne P. Perelli. 1982. Estimating Aircrew Fatigue: A Technique with Application to Airlift Operations. Technical
Report. Brooks AFB, TX: USAF School of Aerospace Medicine. http://www.dtic.mil/docs/citations/ADA125319
[67]
Hillol Sarker, Karen Hovsepian, Soujanya Chatterjee, Inbal Nahum-Shani, Susan A. Murphy, Bonnie Spring, Emre Ertin, Mustafa
Al’Absi, Motohiro Nakajima, and Santosh Kumar. 2017. From Markers to Interventions: The Case of Just-in-Time Stress Intervention.
In Mobile Health: Sensors, Analytic Methods, and Applications. Springer International Publishing, 411–433. https://doi.org/10.1007/
978-3-319-51394-2_21
[68]
Hillol Sarker, Moushumi Sharmin, Amin Ahsan Ali, Md. Mahbubur Rahman, Rummana Bari, Syed Monowar Hossain, and Santosh
Kumar. 2014. Assessing the Availability of Users to Engage in Just-In-Time Intervention in the Natural Environment. In Proceedings of
the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing (UbiComp ’14). ACM, 909–920. https://doi.org/10.
1145/2632048.2636082
[69]
Joon-Gi Shin, Eiji Onchi, Maria Jose Reyes, Junbong Song, Uichin Lee, Seung-Hee Lee, and Daniel Saakes. 2019. Slow Robots for
Unobtrusive Posture Correction. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems (CHI ’19). ACM,
613:1–613:10. https://doi.org/10.1145/3290605.3300843
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
39:26 • W. Choi et al.
[70]
Patrik Sörqvist, Stefan Stenfelt, and Jerker Rönnberg. 2012. Working Memory Capacity and Visual–Verbal Cognitive Load Modulate
Auditory–Sensory Gating in the Brainstem: Toward a Unied View of Attention. Journal of Cognitive Neuroscience 24, 11 (Nov. 2012),
2147–2154. https://doi.org/10.1162/jocn_a_00275
[71]
Takemi Sugiyama, Genevieve N. Healy, David W. Dunstan, Jo Salmon, and Neville Owen. 2008. Joint Associations of Multiple Leisure-
Time Sedentary Behaviours and Physical Activity with Obesity in Australian Adults. The International Journal of Behavioral Nutrition
and Physical Activity 5 (July 2008), 35. https://doi.org/10.1186/1479-5868-5-35
[72]
J. Graham Thomas and Dale S. Bond. 2015. Behavioral Response to a Just-in-time Adaptive Intervention (JITAI) to Reduce Sedentary
Behavior in Obese Adults: Implications for JITAI Optimization. Health Psychology 34, Suppl (Dec. 2015), 1261–1267. https://doi.org/10.
1037/hea0000304
[73]
Alicia A Thorp, Genevieve N Healy, Elisabeth Winkler, Bronwyn K Clark, Paul A Gardiner, Neville Owen, and David W Dunstan.
2012. Prolonged Sedentary Time and Physical Activity in Workplace and Non-Work Contexts: A Cross-Sectional Study of Oce,
Customer Service and Call Centre Employees. International Journal of Behavioral Nutrition and Physical Activity 9, 1 (2012), 128.
https://doi.org/10.1186/1479-5868-9-128
[74]
Liam D. Turner, Stuart M. Allen, and Roger M. Whitaker. 2015. Push or Delay? Decomposing Smartphone Notication Response
Behaviour. In Proceedings of the 6th International Workshop on Human Behavior Understanding - Volume 927. Springer-Verlag, 69–83.
https://doi.org/10.1007/978-3-319-24195-1_6
[75]
Liam D. Turner, Stuart M. Allen, and Roger M. Whitaker. 2017. Reachable but not Receptive: Enhancing Smartphone Interruptibility
Prediction by Modelling the Extent of User Engagement with Notications. Pervasive and Mobile Computing 40 (Sept. 2017), 480–494.
https://doi.org/10.1016/J.PMCJ.2017.01.011
[76]
Saskia van Dantzig, Gijs Geleijnse, and Aart Tijmen van Halteren. 2013. Toward a Persuasive Mobile Application to Reduce Sedentary
Behavior. Personal and Ubiquitous Computing 17, 6 (Aug. 2013), 1237–1246. https://doi.org/10.1007/s00779-012-0588-0
[77]
E. G. Wilmot, C. L. Edwardson, F. A. Achana, M. J. Davies, T. Gorely, L. J. Gray, K. Khunti, T. Yates, and S. J H Biddle. 2012. Sedentary Time
in Adults and the Association with Diabetes, Cardiovascular Disease and Death: Systematic Review and Meta-Analysis. Diabetologia 55,
11 (2012), 2895–2905. https://doi.org/10.1007/s00125-012-2677-z
[78]
Fengpeng Yuan, Xianyi Gao, and Janne Lindqvist. 2017. How Busy Are You?: Predicting the Interruptibility Intensity of Mobile Users. In
Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems (CHI ’17). ACM, 5346–5360. https://doi.org/10.1145/
3025453.3025946
Received February 2019; revised April 2019; accepted April 2019
Proc. ACM Interact. Mob. Wearable Ubiquitous Technol., Vol. 3, No. 2, Article 39. Publication date: June 2019.
