Michael Munson
Executive Director
Loree Cook-Daniels
Policy and Program Director
SEPTEMBER 2015
TRANSGENDER SEXUAL
VIOLENCE PROJECT
TRANSGENDER SEXUAL VIOLENCE SURVIVORS
A Self Help Guide
to Healing and
Understanding
PHOTO BY LEIGH HOUGHTALING

2
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Table of Contents
Thank You_____________________________________________________________________ 7
Introduction __________________________________________________________________ 8
Welcome _____________________________________________________________________ 8
Introduction to Self-Help Guide _________________________________________ 10
Guide Contents _____________________________________________________________ 11
Trauma and its Aftermaths __________________________________________ 13
The brain and trauma _____________________________________________________ 13
Additional readings on how trauma affects the brain _____________________________ 16
Aftereffects of sexual abuse or assault ________________________________ 16
Emotional regulation problems ________________________________________________ 18
Isolation / avoidance / denial __________________________________________________ 20
Shame, guilt, and self-blame __________________________________________________ 21
Depression / anxiety / self-harm / suicide ______________________________________ 22
Substance abuse ____________________________________________________________ 23
Physical health problems _____________________________________________________ 24
High need for control versus helplessness ______________________________________ 26
Anger _______________________________________________________________________ 26
Sleep disturbances / irritability ________________________________________________ 27

3
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Revictimization/ reenactment _________________________________________________ 27
Interpersonal problems _______________________________________________________ 28
Additional readings on the aftereffects of sexual assault and/or trauma ___________ 30
Transgender Survivors of Sexual Abuse _______________________ 32
Sexual violence statistics and myths ___________________________________ 32
Being too young and/or feeling responsible _____________________________________ 33
Not understanding that “sexual assault”
encompasses what happened to them _________________________________________ 34
Being male and/or having a female perpetrator _________________________________ 34
Experiencing additional complications due to gender identity or politics ___________ 35
Wanting to deny or avoid thinking about the trauma _____________________________ 35
Transgender sexual violence survivors data __________________________ 36
Most transgender survivors have experienced repeated sexual violence ___________ 36
Most transgender people were first assaulted as a child or youth _________________ 36
Most perpetrators were known to the victim ____________________________________ 37
More than a quarter of transgender survivors have been assaulted by females _____ 37
Gender is sometimes perceived to be the motivator of abuse ____________________ 38
Survivors rarely report the abuse ______________________________________________ 38
The abuse can leave physical scars ____________________________________________ 38
Emotional scars can last a very long time ______________________________________ 39
Relationships are heavily impacted ____________________________________________ 40
Survivors often partner with other sexual assault survivors _______________________ 41
Trans survivors access many types of help. _____________________________________ 42
Trans-specific aspects of sexual assault ______________________________ 43
Anti-trans abuse or sexual abuse? _____________________________________________ 43
Cause and effect _____________________________________________________________ 43
Trans bodies and body dysphoria ______________________________________________ 45
Not being believed or minimizing the assault(s) _________________________________ 45
Transgender perpetrators _____________________________________________________ 46
Service provider perpetrators _________________________________________________ 47
Meeting complex needs within a basic service system ___________________________ 48

4
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Complicated relationship with therapists _______________________________________ 49
Intersectionality ______________________________________________________________ 50
Options for Healing _____________________________________________________ 51
Talk therapy _________________________________________________________________ 51
Medication __________________________________________________________________ 52
Additional readings on medications ________________________________________ 52
Body-based therapies ________________________________________________________ 52
Additional readings on alternative therapies _________________________________ 53
Movement-based therapies ___________________________________________________ 54
Other “alternative” therapies __________________________________________________ 54
Faith-based support__________________________________________________________ 55
Peer-to-peer help ____________________________________________________________ 56
Mainstream and LGBT Services _________________________________________ 57
LGBT anti-violence programs (AVPs) ___________________________________________ 57
State sexual violence coalitions _______________________________________________ 57
National sexual assault hotline ________________________________________________ 58
Rape crisis hotlines or community rape treatment centers _______________________ 58
Sexual assault treatment centers, sexual assault
nurse examiners, and hospitals ________________________________________________ 58
Sexual assault response teams (SART) or
coordinated community response (CCR) _______________________________________ 59
Victim assistance programs ___________________________________________________ 59
Victim compensation _________________________________________________________ 59
LGBT community centers _____________________________________________________ 59
Support groups ______________________________________________________________ 60
Therapy _____________________________________________________________________ 60
Restraining orders ___________________________________________________________ 60
Law enforcement ____________________________________________________________ 60
Trans support groups _________________________________________________________ 61
12-step programs ____________________________________________________________ 61
Suicide hotlines and support __________________________________________________ 61

5
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
FORGE Services____________________________________________________________ 62
For Survivors ________________________________________________________________ 62
For Providers ________________________________________________________________ 63
Self-Help Techniques and Concepts ____________________________ 65
Healing is hard work _________________________________________________________ 66
Techniques for coping with strong emotions ________________ 68
Getting out of the basement _____________________________________________ 68
Breathing ____________________________________________________________________ 69
90 seconds __________________________________________________________________ 69
Getting moving / getting physical _______________________________________ 70
Using your voice ___________________________________________________________ 70
Cross brain actions ________________________________________________________ 71
Checklists ___________________________________________________________________ 71
Use technology _____________________________________________________________ 71
Emergency Standard Operating Procedures (SOP) __________________ 72
Techniques, exercises and concepts for healing __________ 76
Container exercise _________________________________________________________ 76
Coping with anniversary dates __________________________________________ 77
Coping with triggers _______________________________________________________ 80
Triggers: Dialogues _______________________________________________________ 80
Triggers: Coping via a “series of tasks” _____________________________________ 81
Additional readings on coping with triggers _________________________________ 83
Making meaning _____________________________________________________________ 83
Additional readings on making meaning ____________________________________ 84
Mindfulness and meditation ___________________________________________________ 84
Additional readings on mindfulness as a healing tool _________________________ 86

6
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Resourcing __________________________________________________________________ 87
Sexuality _____________________________________________________________________ 87
Additional readings on sexuality _______________________________________________ 89
Breath training ______________________________________________________________ 90
Emotions and healing _____________________________________________________ 91
The five stages of emotions ___________________________________________________ 91
Being witnessed in your emotions _____________________________________________ 93
Additional readings on emotional regulation _________________________________ 93
Challenging maladaptive or problematic beliefs ______________________ 94
Additional readings on coping with maladaptive beliefs ______________________ 96
Problem-solving and conflict resolution _______________________________ 96
Relationship attachment styles and issues __________________________ 100
Additional readings on attachment theory and couples ______________________ 103
Time perspective therapy ______________________________________________ 104
Additional resources on time perspective therapy __________________________ 105
Volunteering ______________________________________________________________ 117
Annotated bibliography of self-help books __________________________ 118
Appendices_______________________________________________________________ 109
Appendix A: If your assault just happened __________________________ 109
Appendix B: If your current relationship is abusive ________________ 111
Trans-specific power and control tactics ______________________________________ 114
Safety planning: A guide for transgender and
gender non-conforming individuals who are
experiencing intimate partner violence ________________________________________ 116
Appendix C: New non-discrimination
protections for trans people _________________________________ 130

7
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
This publication was supported by Grant No. 2009-KS-
AX-K003 awarded by the Office on Violence Against
Women, U.S. Department of Justice. The opinions,
findings, conclusions, and recommendations expressed
in this publication are those of the author(s) and do
not necessarily reflect the views of the Department
of Justice, Office on Violence Against Women.
Some of the research data in this report came from
work supported by grant number 2009-SZ-B9-K003,
awarded by the Office for Victims of Crime, Office of
Justice Programs, U.S. Department of Justice.
Thank you
PHOTO BY MIA NAKANO
8
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Introduction
Welcome
Espavo. Thank you for taking your power and picking up
this publication.
Since some people never get beyond the first page of a book
or report, it is very important to us to make sure you—a
transgender
1
or gender non-conforming person who at some
point has experienced sexual assault, sexual coercion, sexual
threats, unwanted sexual or other physical touch, sexual
violence within a dating or intimate relationship, or sex with
an older person who should have known you were too young
to understand all the implications—hear the most important
things we would like you to know. So if you read nothing else,
please read this Welcome.
1. You are not alone.
Fifty percent (50%) or more of all transgender and gender
non-conforming people have experienced some form of
sexual abuse, sometimes from many different people over
1
Transgender: Throughout this document, we will use fluid language of “trans,” “transgender,” “gender non-conforming, and
“gender non-binary.” We honor and recognize the complexity and multiplicity of gender identities. We use these words in
their broadest meanings, inclusive of those whose identities lie outside of these terms often limiting terms.
TRANS* LANGUAGE
Throughout this document, we will use fluid
language of “trans,” “transgender,” “gender
non-conforming,” and “gender non-binary.”
We honor and recognize the complexity and
multiplicity of gender identities. We use these
words in their broadest meanings, inclusive
of those whose identities lie outside of these
terms often limiting terms.
ABUSE/ASSAULT/TRAUMA LANGUAGE
Throughout this publication, abuse, assault
and trauma will be used interchangeably.
Some people will resonate more with
“abuse,” others with “assault,” and others
still, will prefer “trauma.” You may have
additional words that feel more meaningful to
you. Please mentally substitute the language
you feel most comfortable with so you can
gain the most from this guide.
1
PHOTO BY MIA NAKANO
9
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
many years.
2
So you are not alone in what you have experienced. Right
now there are people who care very much about you surviving, healing,
and thriving. Support and connection is available.
2. People can understand the complexities.
As a transgender or gender non-conforming sexual abuse survivor
3
,
you may feel like your experience is too complex for people—possibly
including you—to understand. Sexual assault already inextricably mixes
up issues of sex, gender, body image, power and self image without the
complication of gender identity issues; add that in, and it may seem like
people just cannot get it. And it may be true that you previously have not
found people capable of understanding. But that is changing. Not only has
FORGE’s staff been working on these issues for more than a decade (as
well as a growing number of trans and LGBTQ individuals and agencies),
but we have been training providers so they can better serve transgender
survivors. There are now people who are prepared and want to walk with
you as you sort through what happened and what you want to have happen next.
3. Healing is possible.
You may have been living with the aftermath of sexual abuse for decades now. You may
not know what parts of you have been shaped by your sexual abuse experiences. You may
think you are going to live the rest of your life carrying the scars of your experience. You
may think you were not affected at all. What we want you to know is that we understand
far more than we ever did before of what sexual assault does to people, and how to
heal that damage. There is no cure-all, no magic wand, but we know of more tools and
techniques than we ever did before.
We hope you join us in the following pages to find out more about how we can help you
help yourself.
2
Abuse/assault/trauma: Throughout this publication, these three words will be used interchangeably. Some people will reso-
nate more with “abuse,” others with “assault,” and others still, will prefer “trauma.” You may have additional words that feel
more meaningful to you. Please mentally substitute the language you feel most comfortable with so you can gain the most
from this guide.
3
Survivor/victim: Most of the time, this guide will use “survivor” language, since we know that many people who have
experienced abuse/assault feel more empowered by it than the word “victim.” There are many ways people classify what
happened to them, and who they are in response to what they experienced. If one word does not feel right for you, please
mentally substitute.
SURVIVOR/VICTIM LANGUAGE
Most of the time, this guide
will use “survivor” language,
since we know that many
people who have experienced
abuse/assault feel more em-
powered by it than the word
“victim.” There are many ways
people classify what hap-
pened to them, and who they
are in response to what they
experienced. If one word does
not feel right for you, please
mentally substitute.

10
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Introduction to this self-help guide
In 2003, Michael Munson and Loree Cook-Daniels, the facilitators of FORGE’s then-
10-year-old transgender and SOFFA (Significant Others, Friends, Family and Allies)
Milwaukee-based peer support group, realized that over half of the people who
attended monthly meetings had survived sexual assault.
We never asked the hundreds of people who attended meetings over those first 10 years,
but participants would often reference past (or current) abuse, and we began to mentally
track the high volume of people who had experienced sexual violence. 2003 was also
the year when a transgender sexual assault survivor attempted to access help from law
enforcement, sexual assault service providers, crime victim compensation, lawyers,
advocates, and therapists, and was repeatedly denied service or revictimized
by the system. We wondered: Is sexual violence against trans* people
this prevalent everywhere? Are services that are supposed to help
survivors this dysfunctional and damaging to trans people in other
parts of the country?
“Yes” was the answer we discovered from the national survey
FORGE conducted in 2004, with 265 trans respondents.
4
Not
only were sexual assault histories ubiquitous among trans
people, but so were negative experiences trying to get help.
In the years since, FORGE has continued to collect and
research the experiences of transgender sexual assault
survivors and their loved ones, as well as develop a
deeper understanding of trauma and the implications
for healing.
Beginning in 2009, we have been awarded several
groundbreaking federal grants to try to improve the
knowledge, skills and cultural competency of victim services
providers about the unique (and not-so-unique) needs of
transgender survivors; and grants to provide direct services to
trans survivors and loved ones.
Although it is critical to improve mainstream services’ ability to
appropriately and respectfully respond to the needs of transgender
sexual assault survivors and their loved ones, our 2004 study found that
many trans survivors turn to the internet and self-help materials rather than, or
in addition to, services from therapists or sexual assault programs. Unfortunately, many
self-help and internet-based materials are highly steeped in binary gender stereotypes,
making them painful reading for some transgender and gender non-binary survivors. In
addition, none of those materials addresses the specific complexities that face survivors
who are not only trying to find their way through the morass of feelings and memories
about the assault(s), but who are also trying to cope with how gender identity issues
interact with and complicate the picture.
4
FORGE. (2004). “Sexual Violence in the Transgender Community Survey,” (n=265) (data has not been formally published).
PHOTO BY KERRI CECIL
11
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
This guide will help fill that void.
For example:
If you are a transgender sexual abuse survivor who is reading this manual as a
self-help tool, congratulations and good work! That action alone demonstrates
hope, a willingness to work on yourself, and self-awareness. Those are things
many survivors do not feel.
At the same time, you may be picking up a self-help manual because you have
learned that other people cannot be trusted to be helpful and supportive.
Particularly if the people who were supposed to care for you as a child failed to
do so consistently, you may have learned that the only person you can count on
is yourself. Those are things that many survivors feel and have experienced, too.
As you continue on your healing journey, you may learn enough skills, and
become confident enough to seek, find, and establish relationships with
people who are trustworthy, who can and will provide you with the support
and connection you probably crave deep down under your fear, anger,
disappointment and other protective emotions.
Guide Contents
There are six main sections to this guide.
1. The Introduction section talks about how the guide came about, what it contains, and
how to use it.
2. Trauma and its Aftermaths addresses what occurs in our brains at the moment
trauma happens, and why trauma memories and reactions are so different from the
rest of our experience. This section also describes many of the long-term effects of
trauma. Some readers will be surprised at what is here; many of us think we are
personally damaged and/or that being trans has caused certain personality traits and
reactions, when the actual cause often lies in the trauma(s) we have suffered.
3. The Transgender Survivors of Sexual Assault section reviews what FORGE and
others have learned about transgender sexual assault survivors over the past decade.
It reviews popular myths about sexual assault, including many that lead to trans
survivors not recognizing their experience as sexual assault or abuse. It reports what
FORGE has learned in its surveys of transgender sexual assault survivors about their
experiences, and includes many quotations from trans survivors. The last section
explores some of the unique and trans-specific issues trans survivors face, again
including many quotations. Although the primary purpose of this section is to show
you that you are not alone, please know that we necessarily had to leave out many
comments and issues due to space constraints. If one or more of your issues are not
reflected here, by no means draw the conclusion that you are the only one who is
grappling with them.

12
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
4. Options for Healing briefly addresses talk therapy,
medications, body-based therapies, movement-based
therapies, other “alternative” therapies, faith-based
assistance, and peer-to-peer help. It then lists and describes
both mainstream and FORGE-sponsored services and resources
that may support your healing efforts.
5. Self-Help Techniques includes a selection of exercises and essays that you may
want to use to help promote your own well-being. The topics covered include: breath
training, challenging maladaptive or problematic beliefs, an emotional container
tool, coping with anniversary dates and triggers, emergency standard operating
procedures, emotions and healing, making meaning, mindfulness and meditation,
problem-solving and conflict resolution, relationship attachment styles and issues,
resourcing, sexuality, time perspective therapy, and volunteering. Some of the
exercises and essays include
additional readings; an annotated bibliography at the end should help guide
you to additional resources.
6. In the Appendices you will find some additional resources, including guidance on
what to do if your assault just happened, and an exciting new federal law that should
help improve the availability and quality of services offered to trans sexual assault
survivors. There is also an appendix with information for those who may currently be
in relationships that are unsafe, including a list of trans-related power and control
tactics and a trans-specific safety planning tool.
Each section has been designed to stand on its own, so feel free to go right to the topic or
topics you are most interested in, and put off or skip the others entirely. There is no 1-2-3
recipe for healing from trauma; in fact, one of the goals of recovery is learning how to
respect and take care of your own individuality. If something in this guide does not fit you
or does not make sense, let it go and move on to something else. It is your life; this guide
is but one of many tools that you might find useful.
PHOTO BY LEIGH HOUGHTALING
One of the goals of
recovery is learning
how to respect and
take care of your
own individuality.
13
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trauma and
its Aftermaths
The brain and trauma
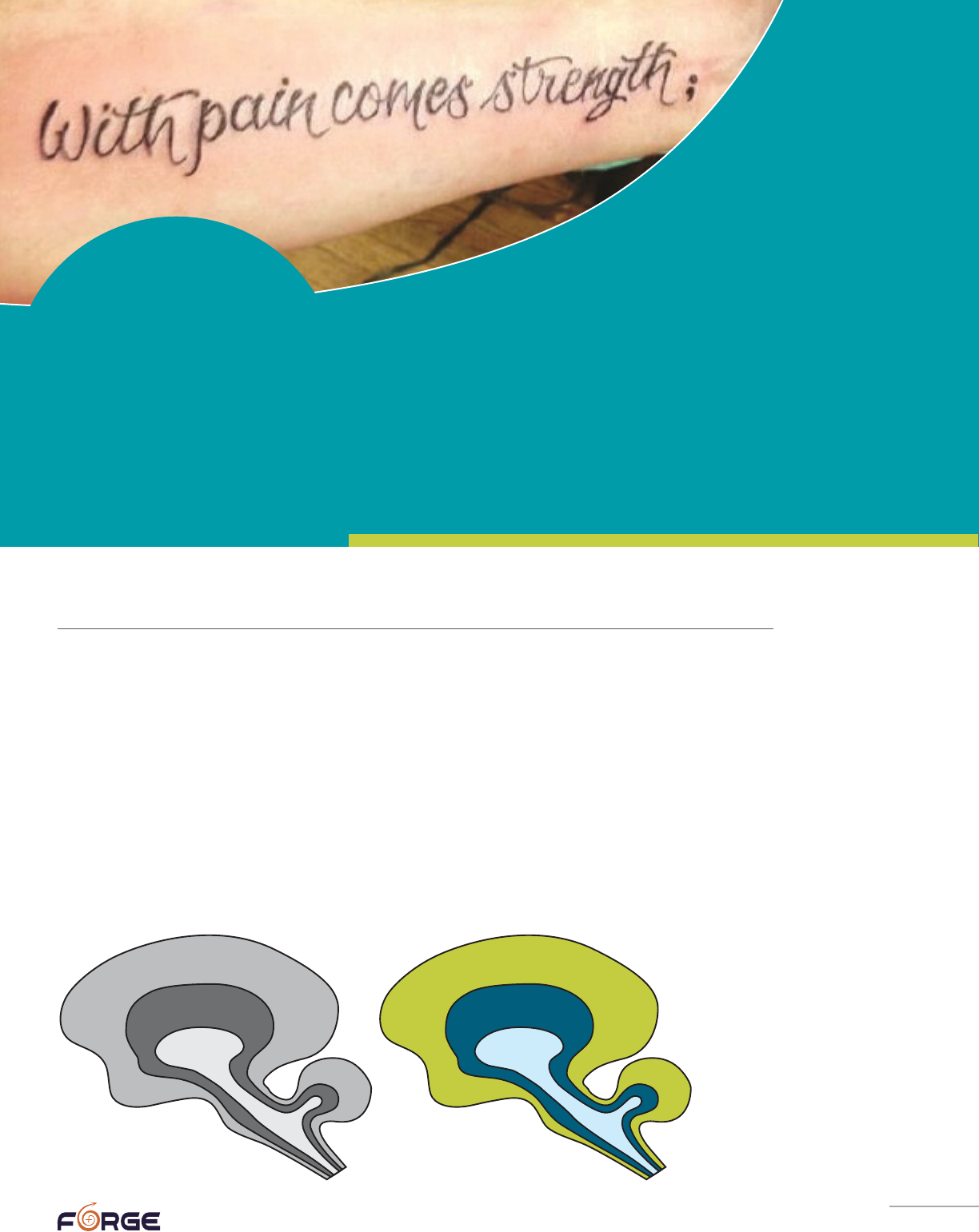
An intriguing and widely-accepted theory about human brains is that they evolved to
become more complex.
This theory says we have a “reptilian” brain that contains the basics for survival. It
processes input from the senses, keeps the system functioning, governs reproduction, and
is in charge of safety. We next developed a “mammalian” or “limbic brain,” found in all
mammals, that evolved around and on top of the central reptilian brain. The limbic brain
contains the circuits that handle emotion, memory, some social behavior, and learning.
The third, most recent and most complex layer is the neocortex. This is our thinking brain,
the part that allows us to think through what is happening and override the reactions of
the reptilian and limbic brains when, for instance, we realize that the person who just
jumped at us unexpectedly is a friend who is smiling and seeking to engage us in play.
2
Neocortex
(neomammalian)
Limbic System
(old mammalian)
Reptilian
Thinking
Emotional
Survival
PHOTO BY BRANDON TAYLOR
14
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
There is a built-in hierarchy among these brain functions. The highest imperative of the
brain is to keep the organism alive, which is the reptilian’s brain first and most basic
function. Faced with a threat to life, the reptilian brain shuts down all “unnecessary”
functions—including not only digestion, muscle building, and reproductive
drive, but also higher-level thinking—in order to divert all available blood
and energy to the heart and muscles to power either “fighting” or “fleeing.”
Should these two options not seem viable, the reptilian brain will choose a
third, less well-known, option: “freezing,” “folding,” or “fainting.” All of these
options can be observed in animals that are faced with becoming someone’s
prey. While the advantages of fighting or fleeing are obvious, freezing or
folding can also be life-saving, if they cause the predator to lose interest
(many predators avoid dead prey in case it died of something that could kill
the animal who dines on it, as well). In addition, there are pain-deadening
aspects of freezing or folding that are merciful if the victim does not
succeed in eluding, defeating, or distracting the predator.
What many trauma survivors do not understand is that the thinking brain,
the neocortex, effectively shuts down when our lives are threatened. Many survivors
harshly criticize themselves later, wondering why they were so “cowardly” or “dumb” that
they could not come up with a way of avoiding or more quickly escaping the situation.
Trauma survivors need to understand that it is literally, biologically impossible for
people to access their thinking brain in life-and-death situations because the more
primitive brain is choosing among its three basic options (fight, flight, or freeze), and
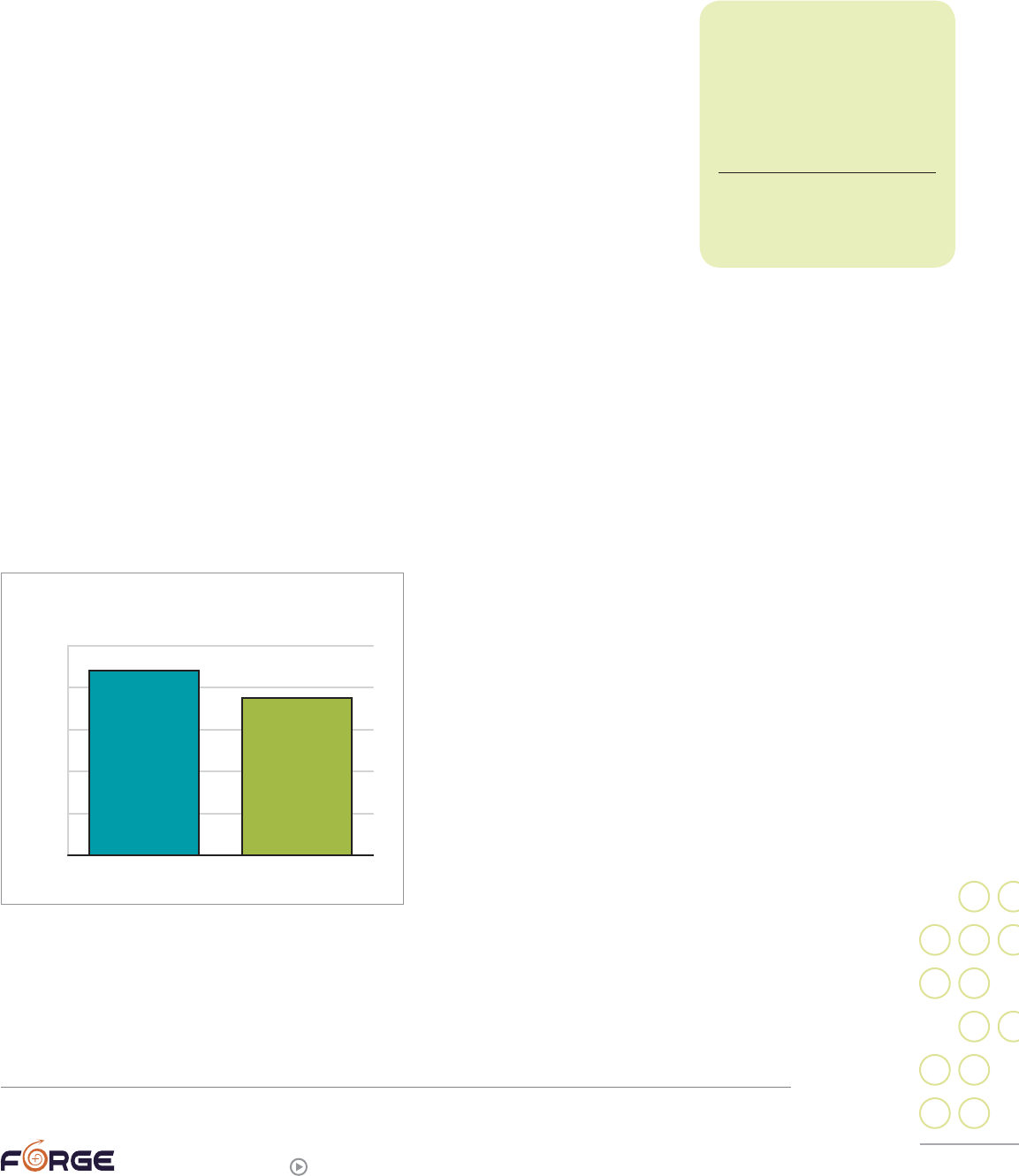
creative problem-solving abilities are for the most part completely off-line. In fact, one
study found that sexual assault seems particularly likely to provoke a biological freeze
response: “88% of the victims of childhood sexual assault and 75% of the victims of adult
sexual assault reported moderate to high levels of paralysis during the assault.”
5
What happens to the brain after the
trauma is less clear, although there is
no shortage of theories. Many theories
focus on memories and why traumatic
memories are so prone to come back
as flashbacks (memories that feel like
they are present reality rather than a
memory), why they are so intrusive,
and why they can be forgotten for
many years and then recovered. Some
of these theories suggest that the
brain’s chemical bath is so different
from normal during a trauma that the
memories are encoded differently. Other
theories suggest that since certain parts
of the brain are off-line during trauma, memories are stored in atypical places. These
trauma theories in turn lead to trauma therapies. For example, one school believes that
it is critical to use your neocortex and language centers of the brain to link your trauma
memories into a story, because that process helps move memories into their more typical
storage mechanisms, in the process draining them of some of their potent emotions.
5
Levine, Peter A. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness, p. 59.
88% of the victims
of childhood sexual assault
and 75% of the victims of
adult sexual assault reported
moderate to high levels of
paralysis during the assault.
Levine, Peter A. (2010). In an
Unspoken Voice: How the Body
Releases Trauma and Restores
Goodness, p. 59.
0%
20%
40%
60%
80%
100%
ADULTCHILDHOOD
88%
75%
PARALYSIS DURING SEXUAL ASSAULT
15
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Some trauma therapies, like EMDR, involve rapidly and repeatedly shifting focus from
one side of the body to the other, in order to activate both hemispheres of the brain and
thereby “integrate” the memories.
Another popular trauma theory is that humans short-circuit the
biological trauma response because of judgments about it. Animals
recovering from a trauma often vigorously shake themselves or engage
in other physical behaviors that “re-set” their systems, whereas human
trauma survivors often repress or suppress such reactions. Trauma
therapies based on this view of trauma help trauma survivors gently
move their body into the last known position before the trauma, and then
carefully and slowly move through the “next actions” the body wants to
take (such as running, shaking, etc.).
Older therapies often focus on having the survivor continually re-live or
re-tell their story until it ceases to hold so much emotional power; newer
analyses indicate this method is only effective if the victim’s primary feeling is fear,
which can be reduced if it is re-lived enough in safe environments. (To learn more about
trauma therapy options, see FORGE’s companion guide, “Let’s talk about it! A Transgender
Survivor’s Guide to Accessing Therapy.”)
What is clear is that during a trauma in which someone feels their life is in danger, their
brain is not operating normally. What is also clear is that memories of what happened
during a trauma are qualitatively different from everyday memories. Although many
people do manage to recover from these traumatic events on their own over time, many
others carry psychological scars that can be debilitating. Some find that their lives begin
to be defined by the trauma, with new experiences and memories all filtered through and
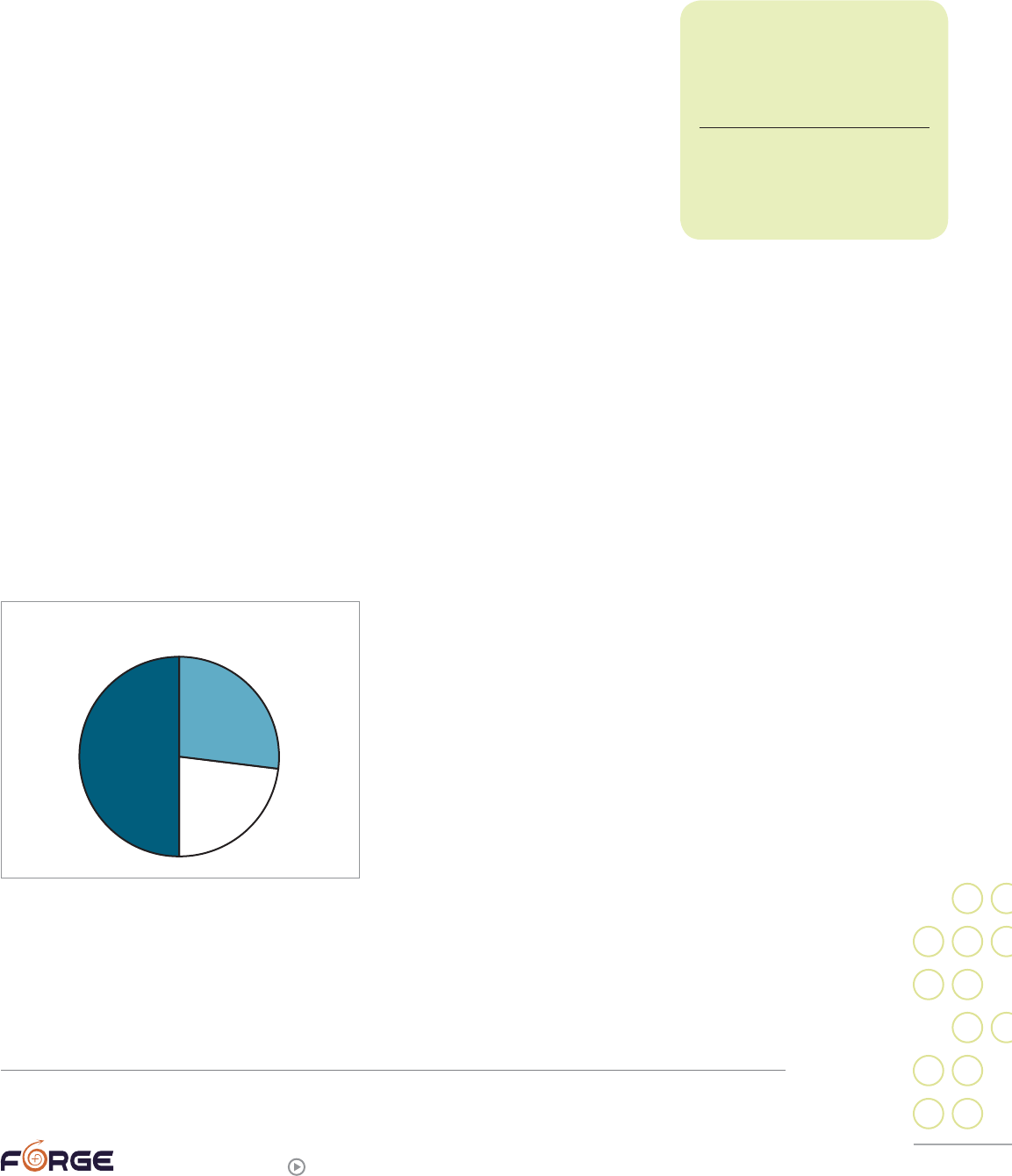
into ways of thinking shaped by the trauma. It appears that sexual abuse is one of the
traumas most likely to lead to Post-Traumatic Stress Disorder (PTSD), the condition most
directly traceable to trauma, with between
50% and 77% of sexual assault survivors
suffering from PTSD at some point.
6
(We talk
more about PTSD in the following section,
“Aftereffects of Sexual Abuse or Assault.”)
Certain personal characteristics and
experiences seem to increase the likelihood
that a sexual assault survivor will develop
long-term symptoms. Experiencing previous
traumas, even if they were caused by natural
disasters rather than human actions, raises
the chances a survivor will develop PTSD. If a
person did not experience strong, supportive
relationships with their adult caretakers as a child, they will be more at-risk. If they
often dissociate (seem to psychologically move out of their bodies into another place
or time), they are at more risk of PTSD, especially if they dissociated at the time of the
trauma itself.
6
Cloitre, Marylene, Cohen, Lisa R., & Koenen, Karestan C. (2006). Treating survivors of childhood abuse: Psychotherapy for
the interrupted life, p. 11.
Between 50 and 77%
of sexual assault survivors
suffer from PTSD at some
point in their life.
Cloitre, Marylene, Cohen, Lisa R.,
& Koenen, Karestan C. (2006).
Treating survivors of childhood
abuse: Psychotherapy for the
interrupted life, p. 11.
PTSD IN SEXUAL ASSAULT SURVIVORS
50%-77%
16
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
If you are a sexual assault survivor, it is critical that you not blame yourself for being
unable to prevent, more quickly end, forget, or just “get past” the experiences you may
now be struggling with. Certain biological processes in your brain and the rest of your
body took over when you were threatened or assaulted, making certain choices literally
impossible. These same chemical and physical processes made semi-permanent changes
in your brain. Although spontaneous healing is possible given enough time and the right
circumstances, it is more likely that you will need to engage in a long period of healing
and self-care, thoroughly grounded in compassion for yourself and the facts of biology.
In the next section we will talk about some of the possible long-term consequences
of trauma.
Aftereffects of sexual abuse or assault
After any sort of trauma, most people recover, either on their own or with the help of
community members or professionals.
However, sexual assault has widely been found to be the type of trauma most likely to
lead to long-term challenges. Studies of Post-Traumatic Stress Disorder (PTSD), the type
of condition most directly traceable to trauma, show that between 50% and 77% of sexual
assault survivors end up meeting the criteria for PTSD.
7
According to the fifth edition
7
Cloitre, Marylene, Cohen, Lisa R., & Koenen, Karestan C. (2006). Treating survivors of childhood abuse: Psychotherapy for
the interrupted life, p. 11.
Additional readings on how trauma affects the brain
Cori, Jasmine Lee. (2008). Healing from trauma: A survivor’s guide to understanding
your symptoms and reclaiming your life. Philadelphia, Pennsylvania:
Da Capo Press.
See especially pages 16-18, “Caught in Lower Brain Centers.”
Levine, Peter A. (1997). Walking the tiger: Healing trauma. Berkeley, California:
North Atlantic Books.
This book is all about the biology of trauma, with a heavy emphasis on how animals
recover from trauma and what humans can learn from them.
Ogden, Pat, Minton, Kekuni, & Pain, Clare. (2006). Trauma and the body:
A sensorimotor approach to psychotherapy. New York, NY:
W.W. Norton & Company.
See especially pages 3-25, “Hierarchical Information Processing: Cognitive, Emotional,
and Sensorimotor Dimensions.”

17
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
of Diagnostic and Statistical Manual of Mental Disorders of the American Psychiatric
Association (DSM-V), PTSD is defined as:
(A) The person was exposed to: death, threatened death, actual or threatened serious
injury, or actual or threatened sexual violence, as follows: (1 required)
(1) Direct exposure.
(2) Witnessing, in person.
(3) Indirectly, by learning that a close relative or close friend was exposed to
trauma. If the event involved actual or threatened death, it must have been
violent or accidental.
(4) Repeated or extreme indirect exposure to aversive details of the event(s),
usually in the course of professional duties (e.g., first responders, collecting
body parts; professionals repeatedly exposed to details of child abuse). This
does not include indirect non-professional exposure through electronic
media, television, movies, or pictures.
(B) The traumatic event is persistently re-experienced in the following way(s):
(1 required)
(1) Recurrent, involuntary, and intrusive memories. Note: Children older than 6
may express this symptom in repetitive play.
(2) Traumatic nightmares. Note: Children may have frightening dreams without
content related to the trauma(s).
(3) Dissociative responses (e.g., flashbacks) which may occur on a continuum
from brief episodes to complete loss of consciousness. Note: Children may
reenact the event in play.
(4) Intense or prolonged distress after exposure to traumatic reminders.
(5) Marked physiological reactivity after exposure to trauma-related stimuli.
(C) Persistent effortful avoidance of distressing trauma-related stimuli after the
event: (1 required)
(1) Trauma-related thoughts or feelings.
(2) Trauma-related external reminders (e.g., people, places, conversations,
activities, objects, or situations).
(D) Negative alterations in cognitions and mood that began or worsened after the
traumatic event: (2 required)
(1) Inability to recall key features of the traumatic event (usually dissociative
amnesia; not due to head injury, alcohol or drugs).
(2) Persistent (and often distorted) negative beliefs and expectations about
oneself or the world (e.g., “I am bad,” “the world is completely dangerous.”).
(3) Persistent distorted blame of self or others for causing the traumatic event
or for resulting consequences.
(4) Persistent negative trauma-related emotions (e.g., fear, horror, anger, guilt
or shame).

18
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
(5) Markedly diminished interest in (pre-traumatic) significant activities.
(6) Feeling alienated from others (e.g., detachment or estrangement).
(7) Constricted affect: persistent inability to experience positive emotions.
(E) Trauma-related alterations in arousal and reactivity that began
or worsened after the traumatic event: (2 required)
(1) Irritable or aggressive behavior.
(2) Self-destructive or reckless behavior.
(3) Hypervigilance.
(4) Exaggerated startle response.
(5) Problems in concentration.
(6) Sleep disturbance.
(F) Persistence of symptoms (in Criteria B, C, D and E) for more
than one month.
(G) Significant symptom-related distress or functional impairment (e.g., social,
occupational).
(H) Disturbance is not due to medication, substance use, or other illness.
8
In simpler terms, trauma survivors are diagnosed with PTSD if they show signs of each of
the following for longer than a month:
Reexperiencing the trauma through flashbacks (memories that feel like they are
present reality rather than a memory), nightmares, remembering the trauma
when they don’t want to, or reacting strongly to things that remind them of
the trauma;
Avoiding normal parts of life that remind them of the trauma;
Altering their thoughts and feelings in a negative way, such as negative beliefs
about the self or the world;
Experiencing hyperarousal, or being overly physically and/or psychologically
reactive to every day events.
Of course, what we just described are the clinical requirements of a medical diagnosis.
In fact, the list of possible consequences of trauma is much, much longer. The following
sections are not exhaustive, but do cover many of the problems sexual assault survivors
may experience.
Emotional regulation problems
One of the most common aftereffects of trauma is having difficulty regulating one’s
emotions. Emotional regulation is the process of keeping your emotions at a level that
does not overwhelm you. Some of this is undoubtedly due to the brain/chemical changes
trauma induces, which lead to the classic PTSD symptoms of re-experiencing, avoiding,
8
Retrieved from http://www.ptsd.va.gov/professional/pages/dsm5_criteria_ptsd.asp, April 2, 2015.
“ the primary effect
of trauma is a chronic
inability to regulate one’s
emotional life.”
Johnson, Susan M. (2005). Emotionally-
focused couple therapy with trauma
survivors: Strengthening attachment
bonds, p. 17.
19
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
and hyperarousal. It is hard to have control over your emotions if your body and mind are
constantly strongly reacting to threats or experiencing threats no one else experiences,
either because you are having flashbacks or have misinterpreted an innocent event like
someone suddenly coughing or laughing loudly.
If someone is traumatized as a child or youth, chances are good that they missed out on
some normal skill-building due to being “distracted” by coping with the trauma. This
may be especially true if the abuser was a parent, family member, teacher or caregiver
who would normally be teaching that child how to cope in the world, including how to
cope with their emotions. Not only will the child have a complicated, possibly fearful
relationship with their abuser/teacher, but the chances are good that the abuser will
themselves not have good emotional regulation skills, which helped lead them to abuse
in the first place. In any case, the young person simply does not acquire the strategies
for calming and self-soothing strong emotions. Asked what help they would like now, one
transgender sexual assault survivor stated they would like:
“ Therapy to help me develop the missing social skills that are a consequence of
my childhood abuse, and my years and years of cognitive dissociation.”
9
Finally, many psychologists and child development experts believe in “attachment theory,”
which holds that how the primary caregiver(s) interact with the infant and young child
not only sets lifelong patterns of relating in that child, but actually physically molds how
the child’s brain develops. This theory says that
even if a parent or caregiver is not an abuser, if
they do not respond adequately to the infant/
child’s needs, that child will develop a brain
that is less capable of handling strong emotions
and bouncing back from adversity (in other
words, resilience) than other peoples’ brains.
One possible aspect of emotional regulation
problems may be an inability to even identify
what emotions one is having. The person who
has this problem, also called alexithymia,
usually answers “I don’t know” or has only a very limited number of answers (“upset,”
9
Unless otherwise specified, all quotes were given to FORGE by transgender/SOFFA survivors in our 2004 study,
“Sexual Violence in the Transgender Community Survey,” (n=265) (data has not been formally published); our 2011 study,
“Transgender peoples’ access to sexual assault services,” a survey approved by the Morehouse School of Medicine’s
Institutional Review Board, (n=1005) (data has not been formally published); or through individual conversations via email,
phone, or in person. Wherever possible quotes are verbatim from the speaker/writer, with only light editing to improve
reader comprehension.
“ And suddenly it had come to her…that
the voice she was hearing was her own,
for the first time in her life.”
Anna Quindlen (1992, p. 393) as quoted in Cloitre, Marylene, Cohen,
Lisa R., & Koenen, Karestan C. (2006). Treating survivors of
childhood abuse: Psychotherapy for the interrupted life, p. 263.
Emotional regulation skills help make you less vulnerable to intense emotions.
Consider a broken thermostat in your apartment or home. When the thermostat is
not functioning at full capacity, it is difficult to regulate the temperature inside your
apartment/home. The inside state is more vulnerable to changes in the weather
outside. (For example, if it drops below freezing outside and the inside thermostat
isn’t able to maintain a steady temperature, it is more likely to get cold on the inside.)
Emotion regulation skills help the thermostat function better, help you realize sooner
when it’s not functioning effectively, and makes you less vulnerable to changes outside.
PHOTO BY MIA NAKANO

20
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
“ok”) when asked how they are feeling. Not only may they not know the
words to put to what they are feeling, but they may even be unable to
distinguish one type of feeling from another. Obviously, if you cannot
even identify what you are feeling, it becomes much harder to learn
strategies for constructively dealing with that feeling. As a result,
many people end up using substances or behaviors (like chronically
working long hours, or playing endless video games) as a way to cope
with any strong feeling.
Isolation / avoidance / denial
Despite how many transgender people are sexual assault survivors,
you may not know many other survivors because trauma survivors
often isolate themselves and/or just do not talk about what happened to
them. Some of this isolation may come from fear of being re-victimized
or an awareness that one’s social skills are not as good as they could
be. Self-isolation can also be a way of simply trying to lower the
chances of being “triggered,” or having something happen that causes a flashback or
otherwise reminds the person of what they’ve experienced in the past. Avoidance is
a similar tactic; if the person can structure their days to avoid being reminded of the
trauma, they will have fewer painful memories and feelings. Denial can take many forms.
One is to claim that while the trauma happened, it had no effect or the person has long
since recovered and has no lingering effects. Another is to wonder if it even happened, or
to claim it was not nearly as bad an experience as others’.
Here are some examples of what trans survivors reported:
“It happened—I got over it.”
“It had nothing to do with who I am today, except for making me a lot stronger, and
a bit harder on the outside, and unable to fully enjoy sex.”
“Large groups are scary—large groups being more than 2 people who I don’t know
or more than 6 people that I do know.”
“[I] just wanted to forget about it.”
“I was hesitant to claim that my abuse was real abuse, and didn’t want to ‘take
away’ services or time from ‘real’ survivors who needed them more.”
“[I made a] deliberate effort to put events behind me and not think of them.”
“This survey is somewhat upsetting. I’d rather forget.”
Trigger:
An event, object, person, etc.
that sets a series of thoughts
in motion or reminds a person
of some aspect of his or her
traumatic past. The person may
be unaware of what is “triggering”
the memory (i.e., loud noises, a
particular color, piece of music,
odor, etc.).
Sidran Institute, downloaded October
27, 2013 from http://www.sidran.org/
sub.cfm?contentID=38§ionid=4
21
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Although it is still a controversial subject, many people forget they were ever sexually
assaulted or abused, sometimes for years or even decades. Various developments may
cause the memories to re-emerge:
“ It [sexual assault history] didn’t come up seriously until I started volunteering for
a group for ‘stopping abuse in the lesbian, bisexual women’s and transgendered
10
communities’—the training I went through kicked it ALL loose.
Other common triggers for the re-emergence of forgotten abuse memories include:
parenting a child who reaches the age when the abuse happened to the parent; revelation
of another family member’s abuse; and illness, loss of a partner, retirement, or some
other major life change. Some people believe they were in some way “protected” from their
memories until they became strong enough to handle them. This does not necessarily
mean the re-emergence process is easy:
I did not think I would have a nervous breakdown. I shattered like glass…
the emotions suddenly overwhelmed me…and I became dysfunctional.
It took over 10 years of psychotherapy, and 5 hospitalizations (mental health
wards) to heal from these events. All of this was at my own expense.
Shame, guilt, and self-blame
Shame is the feeling that you are damaged, unworthy, bad, dirty, wrong, unlovable,
unfixable, dangerous, not good enough, broken, and/or don’t deserve to live. Although
it should be what is felt by the perpetrator—the one who violated another person, used
someone to meet their own needs, or betrayed or manipulated someone’s innocence or
trust—instead, almost like a sexually transmitted infection, it ends up infecting the
victim. Unfortunately, it doesn’t feel like an outside infection to the victim; it just feels
like who they truly are: not good enough or not worthy of love and compassion.
Shame can lead to a whole range of negative outcomes. It may help explain the isolation
many survivors impose on themselves, and/or their avoidance of friendships or other
relationships. It may be part of the reason why survivors often do not feel like they
will live very long, and (perhaps consequently), why they may not bother planning for
the future. It can lead people into partnering with individuals who abuse them again,
because why should they deserve any better? People who feel shame often drown that
feeling in alcohol or drugs, or bury it under a mountain of busy-ness and overwork.
Guilt is related to shame. Shame is about who you think you are, whereas guilt is about
a behavior you may have done. Guilt is a feeling that you have done something wrong. A
sexual assault survivor who feels guilt may think they should have known better than to
have gone to someone’s house on a first date; the survivor who feels shame may think they
are so flawed they deserved to be assaulted. Although both can lead a survivor to blame
themselves for the assault, guilt implies one can learn to not do something again, while
the survivor with shame feels unfixable.
10
We acknowledge that some language in quotes may not align with current community usage of some terms.

22
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Why didn’t you access services?
“ I was ashamed of myself, my identity, my desires, my inner person. They cruci-
fy people like me. It would have been nice to know that I wasn’t a freak and that
there were others like me. But when they asked me what was my problem in
school they always assumed I was just a bad kid. Little did they realize I couldn’t
stand myself. And hated what I was. I felt I needed to be bad to be respected and
left alone.”
“ Shame has kept me silent all these years. This survey is one of the few times that
I have discussed these events. No wants to hear about this [sexual abuse by a
therapist], because therapists are supposed to be God and cannot do any wrong.”
“ In the beginning what stopped me [from getting help] was the belief that I some-
how caused the abuse.”
“Self-hatred.”
“Shame. Mainly shame.”
“I was too ashamed to tell anyone.”
It is important to recognize that the new (DSM-V) diagnostic criteria for PTSD has a new
emphasis on “negative alterations in cognitions and mood,” specifically calling out:
Persistent (and often distorted) negative beliefs and expectations about oneself
or the world (e.g., “I am bad,” “The world is completely dangerous”).
Persistent distorted blame of self or others for causing the traumatic event or
for resulting consequences.
Persistent negative trauma-related emotions (e.g., fear, horror, anger, guilt or
shame).
11
In other words, shame, guilt, and self-blame are hallmarks of having been traumatized;
they seem to come with the territory. That does not, however, mean that you have to
continue to live with them.
Depression / anxiety / self-harm / suicide
The finding that depression and anxiety both frequently accompany PTSD makes a great
deal of sense. If you are having unwanted memories, experiencing emotions that seem out
of control, are staying away from people and activities in order to lessen your chances
of being triggered, are not sleeping well, are reacting strongly to small things most
other people barely notice, blaming yourself for what happened, etc.—feeling depressed
and/or anxious seems pretty normal. It may also be important to note that depression
and anxiety are the most common mental health conditions affecting the general U.S.
population, as well.
Some people cope with depression and anxiety by going to the doctor, a therapist, and/or
obtaining prescriptions for psychotherapeutic drugs. Probably the majority, however,
11 Retrieved from http://www.ptsd.va.gov/professional/pages/dsm5_criteria_ptsd.asp, April 2, 2015.

23
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
attempt to cope on their own by “self-medicating.” This can mean dampening down the
negative feelings through alcohol, prescription or non-prescription drugs, food (over- or
under-eating), becoming completely obsessive about exercise or work or some other
distracting activity, and self-harming behaviors such as cutting. In his doctoral
dissertation lore m. dickey, Ph.D. found that more than 40% of the transgender people he
surveyed had engaged in non-suicidal self-injury.
12
He suggests such self-harm has three
functions. One, which may seem ironic, is self-preservation: the “transgender person is
making an effort to address the pain and distress they are feeling in a manner that
recognizes the value that life has.” In other words, some people self-harm as a way of
avoiding a suicide attempt. The second reason is desperation, which he defines as
“causing pain so as not to feel numb or trying to feel something even though it is physical
pain.” The third reason is emotional abreaction. One source defines this as “reliving an
experience in order to purge it of its emotional excesses; a type of catharsis. Sometimes it
is a method of becoming conscious of repressed traumatic events.”
13
Other people do, in fact, become suicidal.
The National Transgender Discrimination
Study
14
found that overall, 41% of its
transgender and gender non-conforming
respondents had attempted suicide
at least once. For those who had been
sexually assaulted, the attempt rate went
up to 64%. These figures compare to 1.6%
for the general population. In other parts
of this guide you can find the numbers
for suicide hotlines and an “emergency
standard operating procedures” worksheet
that can help you plan how to better
handle suicidal feelings if you have them.
Substance abuse
As previously noted, many survivors
attempt to dampen or alter their difficult
symptoms or painful memories through self-medication, typically alcohol, drugs, or food.
Study after study finds high correlations between those who use substances to cope and
those suffering from PTSD. While substance use can sometimes temporarily diminish
symptoms such as nightmares, panic attacks, depression and numbing, substance use is
also associated with more trauma: violence and accidents are more likely when one or more
people are drunk or high. Although many trauma treatment programs will not accept people
who are actively abusing substances and many substance abuse treatment programs do not
address trauma issues, there is a growing consensus that because of the interrelationships
among trauma and substance use, simultaneous treatment is recommended. One such joint
treatment program has been described in a manual accessible to non-therapists: Seeking
12
dickey, lm, Reisner, SL, & Juntunen, CL. (2015). Non-suicidal self-injury in a large online sample of transgender adults.
Professional Psychology: Research and Practice. Vol. 46, No. 1, 3-11.
13
dickey, lm, Reisner, SL, & Juntunen, CL. (2015). Non-suicidal self-injury in a large online sample of transgender adults.
Professional Psychology: Research and Practice. Vol. 46, No. 1, 3-11.
14
Grant, Jaime M., et al (2011). Injustice at every turn: A report of the national transgender discrimination survey, National
Center on Transgender Equality and National Gay and Lesbian Task Force.
SUICIDE ATTEMPTS
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
GENERAL
NON-TRANS
TRANS SA
SURVIVORS
TRANS
(ALL)
41.0%
64.0%
1.6%
24
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Safety: A Treatment Manual for PTSD and Substance
Abuse, by Lisa M. Najavits.
15
Physical health problems
While many researchers have linked abuse to
various psychological problems, awareness of
their linkage to physical medical conditions that
become apparent only decades later only began in
the mid-1980s. That is when physicians in Kaiser
Permanente’s Department of Preventative Medicine
in San Diego “discovered that patients successfully
losing weight in the Weight Program were the most
likely to drop out. This unexpected observation
led to our discovery that overeating and obesity
were often being used unconsciously as protective
solutions to unrecognized problems dating back
to childhood. Counterintuitively, obesity provided hidden benefits: it often was sexually,
physically, or emotionally protective.”
16
Curious about this linkage, Kaiser developed what
has become known as the Adverse Childhood Experiences (ACE) Study. Initial reporting on
the ACE Study included findings from 17,000 patients, mostly middle-class, who asked for
comprehensive physical exams.
The ACE questionnaires asked people about their
childhood experiences as well as their current
health statuses. Later versions of the survey
asked about ten types of childhood experiences,
including child physical, emotional, and sexual
abuse. Rather than attempting to measure how
severe each type of maltreatment or “adverse
experience” was or how often it happened, the
researchers simply gave one “point” for each type
of adverse experience the patient had experienced.
Thus patients could have scores ranging from 0
(they had experienced none of the listed negative
childhood experiences) to 10 (they had experienced
them all). Only one-third of this middle-class
population had an ACE Score of 0; one in six had
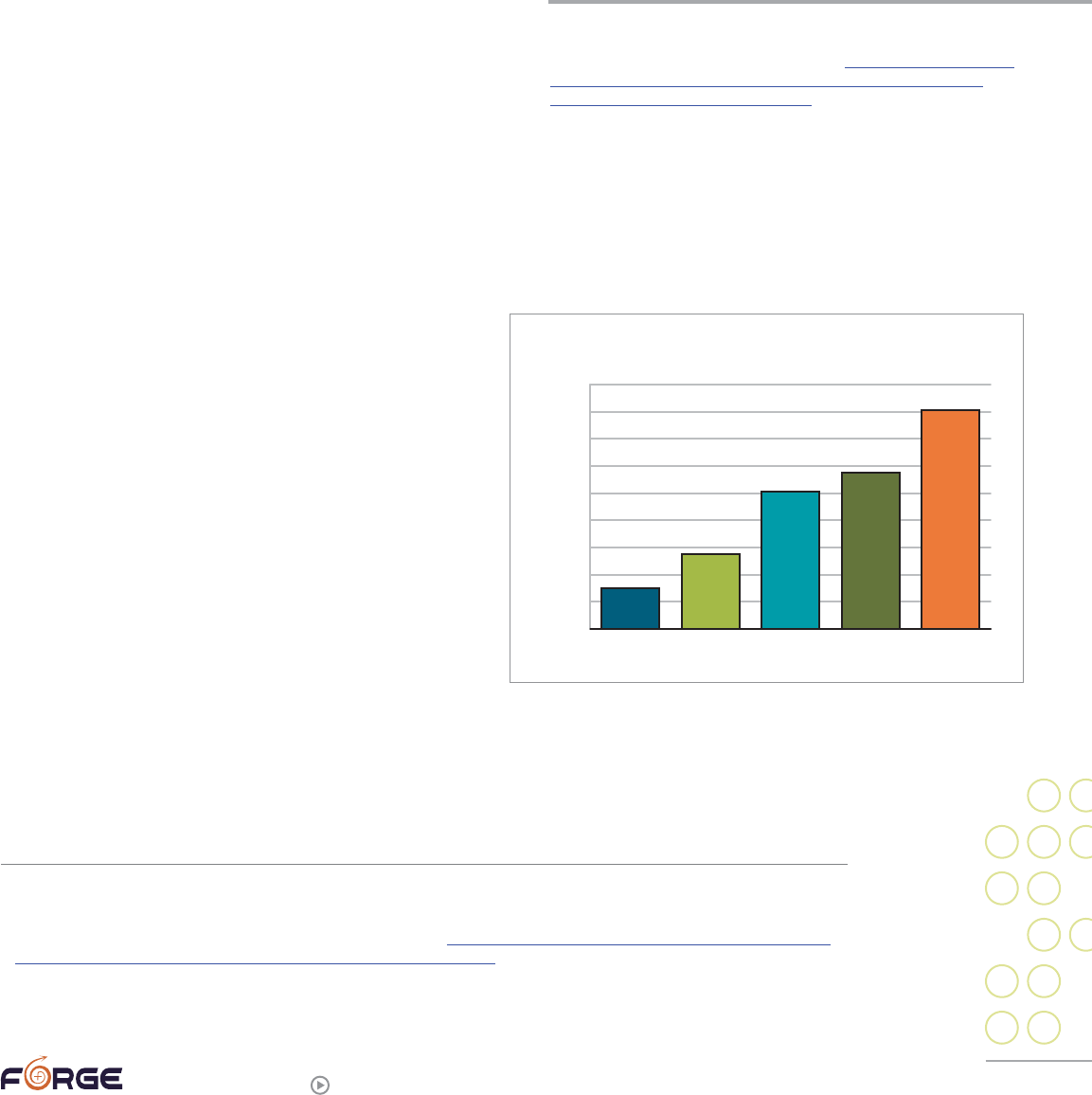
an ACE Score of 4 or more. If any one category of abuse or adversity was experienced,
there was an 87% likelihood that the person would have also experienced at least one
more type.
17
The researchers then matched these patients’ ACE scores with their health records.
When it came to physical health, they looked at the basic causes underlying the 10 most
15
Najavits, Lisa M. (2002). Seeking safety: A treatment manual for PTSD and substance abuse.
16
Felitti, Vincent J. (2004). “The origins of addiction: Evidence from the Adverse Childhood Experiences study.” English
version of an article originally published in German. Available at http://www.nijc.org/pdfs/Subject%20Matter%20Articles/
Drugs%20and%20Alc/ACE%20Study%20-%20OriginsofAddiction.pdf, p. 2.
17
Felitti, Vincent J., & Anda, Robert F. (2010). “The relationship of adverse childhood experiences to adult medical disease,
psychiatric disorders, and sexual behavior: Implications for healthcare.” Chapter in Lanius, Ruth & Vermetten, Eric, (eds.)
The hidden epidemic: The impact of early life trauma on health and disease.
“Our findings indicate that the major
factor underlying addiction is adverse
childhood experiences that have not
healed with time and that are over-
whelmingly concealed from awareness
by shame, secrecy, and social taboo.”
Felitti, Vincent J. (2004). “The origins of addiction: Evidence from the
Adverse Childhood Experiences study.” English version of an article
originally published in German. Available at http://www.nijc.org/pdfs/
Subject%20Matter%20Articles/Drugs%20and%20Alc/ACE%20
Study%20-%20OriginsofAddiction.pdf, p. 8.
0
2
4
6
8
10
12
14
16
18
0
1
2
3
4+
CHILDHOOD EXPERIENCES VS. ADULT ALCOHOLISM
% ALCOHOLIC
ACE SCORE
25
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
common causes of death in America. These include tobacco use (estimated 400,000 deaths
annually), diet and activity patterns (300,000 deaths), alcohol use (100,000 deaths), sexual
behavior (30,000 deaths) and drug use (20,000 deaths). Bar charts of the results could
not be more striking: for nearly every negative behavior that was measured, the bars
steadily rise from the lowest number of drinkers, smokers, etc. among those who had an
ACE score of 0 to, step by step, the highest reported ACE score (usually 4 or more or 6
or more). Perhaps most shocking was how much ACE scores were connected to medical
conditions such as liver disease, chronic obstructive pulmonary disease (COPD), coronary
artery disease, and autoimmune disease(s). Even after removing all known risk factors
such as smoking and high cholesterol, there remained a step-wise increase in the risk of
these diseases by how high a patient’s ACE score was. In other words, it is not enough to
say that adults traumatized as children smoke, eat, and drink more, and therefore have
more chronic illnesses; there are additional factors. The researchers believe that not only
do trauma survivors attempt to self-medicate
through alcohol and cigarettes, but also that
there is wear-and-tear on the biological system
due to chronic stress. The precise biological
mechanisms by which this is taking place have
still not been determined, but that did not stop
the ACE Study researchers from flatly declaring:
“Adverse childhood experiences are the main
determinant of the health and social well-being
of the nation.”
18
The list of other physical health problems
that researchers have linked to a trauma
history is very long. Some of those that show up in the literature most often are: chronic
fatigue syndrome, chronic pain, fibromyalgia, irritable bowel syndrome, and multiple
chemical sensitivities. One researcher explains how trauma might be related to developing
“multiple idiopathic physical symptoms” (MIPS), or physical symptoms that are medically
unexplained. In the first step, a person experiences “symptoms.” What is interesting is that
many child abuse survivors never properly learn about emotions, due in part to having their
emotions ignored or twisted and used against them, such as being told some abuse does
not hurt or that a sexual act is “how parents show love.” As a result of the distortions their
abusers use, the victims may not be able to identify their own emotions and/or talk about
them with others. People with such “alexithymia” may confuse physical signs of emotion—
say, a rapidly beating heart when one is frightened—with medical illness. The second step
in development of a MIPS is the person’s assessment of their symptoms. Here, too, trauma
may play a role: “Psychosocial distress or mental disorders such as depression and anxiety
disorders, including PTSD, may also influence an individual’s appraisal of symptoms. For
example, an individual with depression may develop more pessimistic or catastrophic
symptom appraisals than someone who is not depressed.” In the third step, “the person
responds behaviorally on the basis of the symptom appraisal. For example, he or she may
seek health care, avoid activities or roles, or his or her functioning may be reduced.”
19
Part
18
Felitti, Vincent J., & Anda, Robert F. (2010). “The Relationship of Adverse Childhood Experiences to Adult Medical Disease,
Psychiatric Disorders and Sexual Behavior: Implications for Healthcare,” in Ruth A. Lanius, Eric Vermetten, and Clare Pain,
eds., The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic.
19
Engel, Charles C. Jr. (2004). ”Somatization and Multiple Idiopathic Physical Symptoms: Relationships to Traumatic Events
and Posttraumatic Stress Disorder,” in Paula P. Schnurr and Bonnie L. Green, eds., Trauma and Health: Physical Health
Consequences of Exposure to Extreme Stress, p. 193.
“ Adverse childhood experiences are the
main determinant of the health and social
well-being of the nation.”
Felitti, Vincent J., & Anda, Robert F. (2010). “The Relationship of Adverse
Childhood Experiences to Adult Medical Disease, Psychiatric Disorders and
Sexual Behavior: Implications for Healthcare,” in Ruth A. Lanius, Eric Ver-
metten, and Clare Pain, eds., The Impact of Early Life Trauma on Health and
Disease: The Hidden Epidemic.
26
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
of the isolation and life constriction seen in some sexual assault survivors may grow out of
attempts to avoid interactions that might result in an increase of “symptoms.”
High need for control versus helplessness
Trauma survivors may be highly controlling, totally submissive, or careen wildly between
the two. Childhood sexual abuse expert Mike Lew explains:
“It is important to remember that all abuse involves lies. Children are being lied
to about themselves, about love, and about the nature of human caring. They are
being taught that there is no safety in the world, and they have no right to control
their own bodies. Loss of control of their bodies leads to control being a central
issue of their adult lives. They can become inflexible, controlling, and suspicious—
or helpless and indecisive.”
20
Other experts tie some survivors’ control needs more directly to the symptoms of
PTSD, pointing out that the only way to try to avoid being triggered is to control what’s
happening in your environment and do your best to limit surprises. This often translates
into trying to control others’ actions, and may be one of the mechanisms that underlie
the cycle of violence wherein some victims in turn become abusers. On a related point,
if a person has trouble regulating their emotional responses to another’s behavior, they
may instead try to control that person’s behavior. On the other hand, survivors may find
that it’s too hard to control others or their environment, and may simply give up trying,
instead becoming very passive, helpless, and submissive.
Anger
Anger plays a large role in many survivors’ lives. Some are afraid of anger, as their
abuser’s anger may have been what came before the abuse they experienced; these
survivors may not realize that it is even possible to feel anger without damaging someone.
Many were taught by their abusers that they were not allowed to be angry. Others learned
that anger equals power, and therefore may try to protect themselves by being the most
angry/powerful one in the room. Some anger, obviously, is righteous anger at their
perpetrator(s) and those who may have failed to protect them.
Because many survivors did not learn effective emotional regulation skills, anger is just one
of many emotions that may be problematic for survivors and those around them, simply
because it may feel out of control. In addition, strong emotions provoke chemical changes
in the brain, which tend to diminish the brain’s (more specifically, the neocortex’s) ability to
think things through and problem-solve. In the midst of strong emotions, people tend to act
and react far more easily and quickly than they are able to rationally consider and weigh
alternatives and possible consequences. This can result in less-than-optimal decisions that,
in turn, create more problems and strong negative emotions.
Psychiatrist and psychologist John Bowlby pointed out that anger can be despairing
(coming from a place of powerlessness) or it can be hopeful.
21
An anger that is hopeful
points a person to where changes can be made. This distinction may be helpful to
some survivors.
20
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual child abuse (Second edition), p. 75.
21
Johnson, Susan M. (2005). Emotionally-focused couple therapy with trauma survivors: Strengthening attachment bonds, p. 39.
27
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Sleep disturbances / irritability
Many survivors have sleep problems. Nightmares, both specifically related to the abuse,
as well as other non-abuse-related nightmares, are common. Many people also find it
difficult to fall asleep or stay asleep through the night, frequently waking up. If the
survivor was traumatized at night, perhaps particularly in their own bed, they may
not feel safe enough to relax into sleep. Laura Davis notes that if a survivor is actively
recovering previously unknown memories of their abuse, sleeplessness may precede and/
or follow the emergence of new memories.
22
Lack of sleep can also contribute to increased mental health symptoms, such as
depression and anxiety, as well as create additional challenges concentrating or focusing
during the day. The lack of adequate and restful sleep can also directly impact physical
health—increasing headaches, impacting blood sugar regulation, increasing blood
pressure, and affecting metabolism.
Obviously, sleep disturbances can help lead to daytime irritability, which many survivors
experience for a variety of reasons.
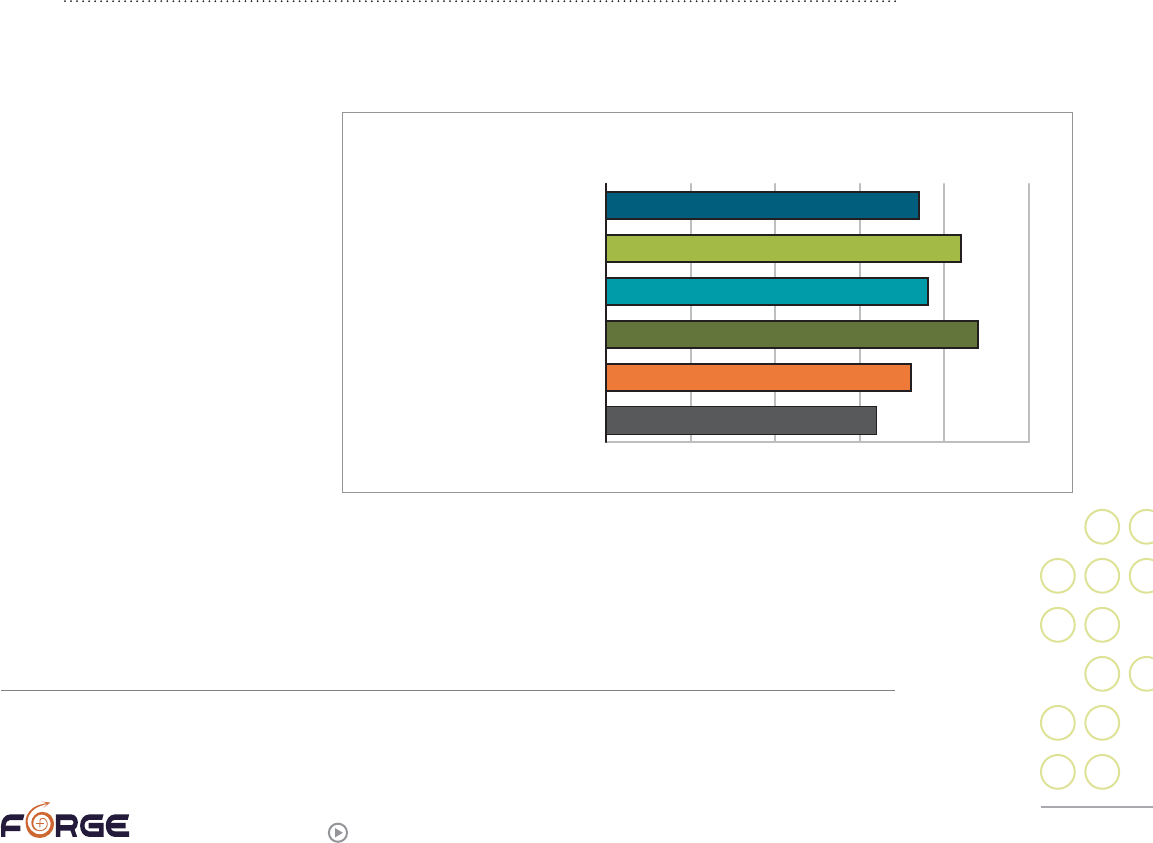
Revictimization / reenactment
“ I’ve been sexually assaulted, raped, molested, harassed many times throughout
my life….There have been way too many.”
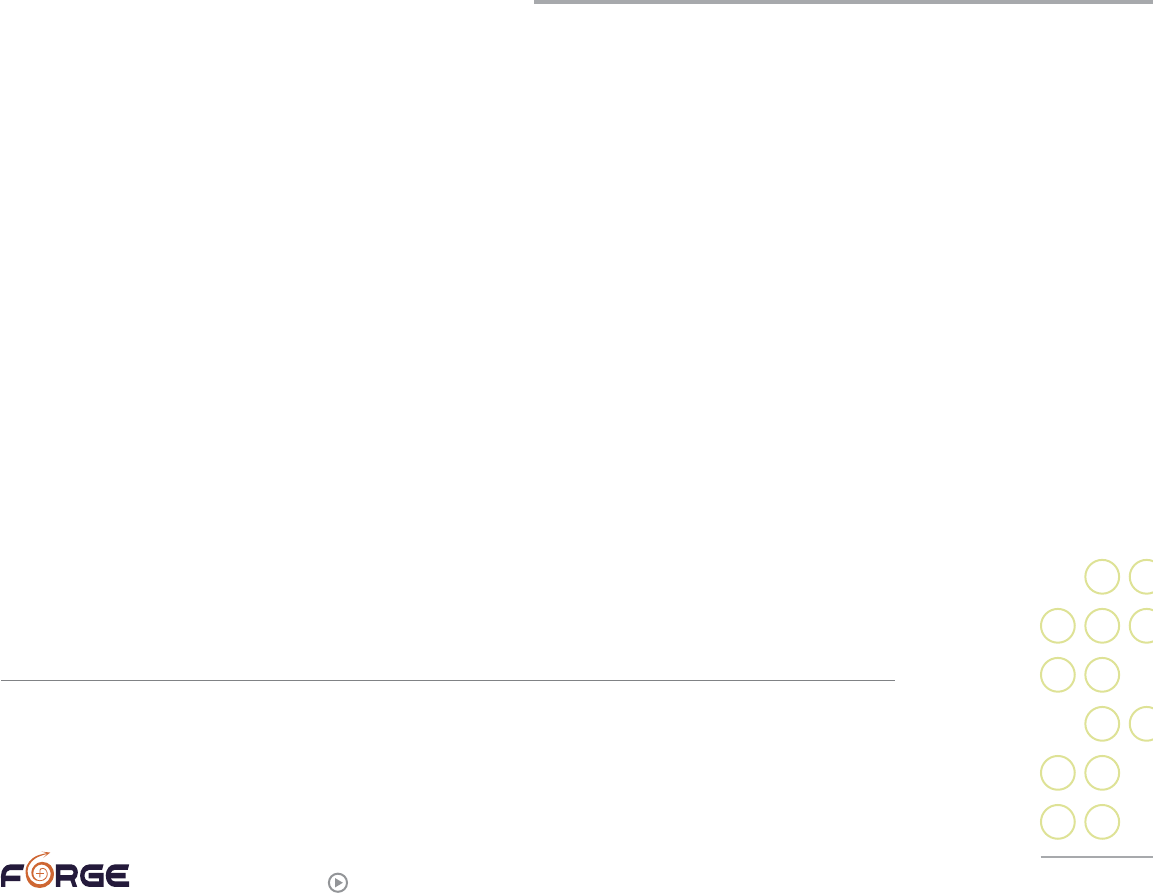
Multiple studies have made clear that people who were abused in childhood have a far
greater likelihood of being abused again in adulthood, and/or in becoming abusers
themselves. “Polyvictimization”
is the current term for people
who have experienced multiple
types of abuse, and a 2011
FORGE study focused on sexual
assault showed how common
this is among trans people. We
asked trans respondents if they
had experienced any of these
types of abuse: child sexual
abuse, adult sexual abuse,
dating violence, domestic
violence, stalking, hate
violence, and other types
of violence. Those who
experienced any one type of
abuse were highly likely to experience other types, as well. For example, 64% of those who
had experienced child sexual abuse went on to experience at least one other type of
abuse, as well.
23
22
Davis, Laura. (1991). Allies in healing: When the person you love was sexually abused as a child, p. 107.
23
2011 study, “Transgender peoples’ access to sexual assault services,” a survey approved by the Morehouse School of
Medicine’s Institutional Review Board, (n=1005) (data has not been formally published).
0% 20% 40% 60% 80% 100%
74%
84%
76%
88%
72%
64%
POLYVICTIMIZATION
HATE MOTIVATED
STALKING
INTIMATE PARTNER VIOLENCE
DATING VIOLENCE
ADULT SEXUAL ASSAULT
CHILDHOOD SEXUAL ABUSE
28
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
How often victims go on to become abusers themselves is less well-documented. A few
mainstream studies of the general public have indicated that men
24
(women abusers are
far less studied) who had been abused as children are twice as likely to abuse as adults
as are men who had not experienced child abuse.
Therapist Francine Shapiro suggests one theory for why this happens:
“ …until their childhood memories are processed the offenders
often have internalized responsibility for their own childhood
abuse. They are blaming themselves—blaming the recipient,
the victim. It is therefore no surprise that as an adult they
perceive the world in the same way and also blame their
own victims. Until they can place full responsibility on the
one that perpetrated against them, they will be unable to take
appropriate responsibility for their own abusive behaviors.”
25
A simpler theory is that people who grew up with adults who abused them may have
decided there are only two types of people: victims and abusers. To avoid being victimized
again, they may seek to gain and maintain the upper hand in all of their relationships.
It is critical to remember that not all victims become perpetrators.
Unfortunately, even some therapists inaccurately believe that past abuse will lead to
abusive behavior in adulthood. For example, FORGE worked with a survivor who was in
the process of transitioning from female to male and who was in therapy with his female
partner. The couple lived in a non-abusing, healthy relationship with each other and with
their children. The couple’s therapist counseled the female partner to leave him in order
to protect their children from abuse by him, a move that would have deprived the children
of a loving parent, destroyed a family, and deeply wounded the adults.
Interpersonal problems
“ As highly adaptive social organs, our brains are just as capable
of adjusting to unhealthy environments and pathological
caretakers as they are to good-enough parents.”
26
Not surprisingly, some sexual assault survivors experience a higher-than-usual number
of interpersonal problems. It may be hard for survivors to trust other people, especially
if the individual(s) who abused them were family members or people they were close to.
If they were abused in childhood, they may never have experienced respectful mutual
communication styles or problem-solving, instead learning that the person with more
24
When referencing studies that specify gender, most of the individuals are likely non-trans. Studies focused on trans
survivors are specifically noted.
25
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the spectrum, p. 213.
26
Cozolino, Louis. (2010). The neuroscience of psychotherapy: Healing the social brain (Second edition), p. 206.
29
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
power gets everything they want, and the person with less gets nothing or, worse, is
hurt. If they learned that in this world there are only two possibilities—being a victim
or being the one with power—they may try to control or have power over their partner,
children, and others. A related problem many have noticed is that survivors may have a
hard time playing: Ogden and her colleagues noted, “Almost invariably, clients are unable
to play, finding that their capacity to experience pleasure, exuberance, and joy in playful
interactions or activities has either diminished, disappeared altogether in the wake of
trauma, or is experienced as paradoxically dangerous and threatening.”
27
Survivors’ relationships may also be affected by their intense emotions, both because they
may not have learned how to regulate their emotions and because the trauma may have
altered their brain chemistry in a way that makes their emotions stronger than usual.
When emotions are intense, the focus of the brain shifts from the neo-cortex or “thinking”
part of the brain to more basic parts of the brain that focus on survival. This is why
people who are very upset may say things they later regret or even deny: brain chemistry
in a highly emotional state is literally different from when emotions are calmer. What can
help is learning to differentiate between when the brain is capable of problem-solving,
and when the task at hand needs to be calming down and regulating emotions.
“ The effects of sexual violence are woven into the fabric of my being, always
have and still do affect every way I sit, walk, talk, stand, breathe, feel, think,
all affects relationship.”
“My marriage was destroyed because of the effects on me, including acting out.”
“My ability to trust people has been severely impacted by these traumas.”
“I can’t hold a relationship.”
“We have to work bloody hard to have a healthy relationship.”
In the next two sections of this guide, we will talk about where trans sexual assault
survivors can get help with these and other problems, and how we can help ourselves.
27
Ogden, Pat, Minton, Kekuni, & Pain, Clare. (2006). Trauma and the body: A sensorimotor approach to psychotherapy, p. 126.
30
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Additional readings on the aftereffects of sexual assault
and/or trauma
Allen, Jon G. (2005). Coping with trauma: Hope through understanding (2nd edition).
Arlington, Virginia: American Psychiatric Publishing.
A thorough book with sections on foundations, effects of trauma, trauma-related
psychiatric disorders, and healing.
Bass, Ellen & Davis, Laura. (2008). The courage to heal: A guide for women survivors
of child sexual abuse (4th edition). New York, New York: HarperCollins.
The Courage to Heal rightfully owns the status of must-have resource for survivors,
with one big caveat: They only address female victims, and only rarely admit there are
female perpetrators. If you wonder if you’re “the only one who…,” The Courage to Heal
will show you that you are not alone. Excellent, if somewhat dated now, resource guide,
divided by topic.
Catherall, Don R. (ed.) (2004). Handbook of Stress, Trauma, and the Family,
New York, NY: Brunner-Routledge.
This textbook contains many excellent chapters on a variety of topics related to how
trauma affects the family. Written for college students and professionals.
Cozolino, Louis. (2010). The neuroscience of psychotherapy: Healing the social brain
(2nd edition). New York, New York: W. W. Norton & Company, Inc.
This book is for readers who want to understand more about the science of the brain
and how it relates to trauma.
Dayton, Tian. (1997). Heartwounds: The impact of unresolved trauma and grief on
relationships. Deerfield Beach, FL: Health Communications, Inc.
This is a particularly good self-help book for partners and partnered trauma survivors:
the major sections are loss and trauma; the effect of trauma on the personality; the
effect of trauma on relationships; transformation and healing through grief; and the
personal journey, which includes many self-help exercises.
Fosha, Diana, Siegel, Daniel J., & Solomon, Marion F., (eds.) (2009). The healing
power of emotion: Affective neuroscience, development & clinical practice,
New York, NY: W.W. Norton & Company.
This book is aimed at college students and/or therapists. It does contain chapters from
some of the most well-known trauma specialists, and will be of interest to those who
have more than a cursory interest in the roles emotion plays in both traumas and our
healing efforts.
Herman, Judith L. (1992). Trauma and recovery: The aftermath of violence—from
domestic abuse to political terror. New York City: Basic Books.
This book is considered a classic, and is referred to by many trauma writers. Very
insightful, but also quite gender-bound: she refers to people with PTSD mostly as
female sexual assault victims, and male military veterans.
31
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from
sexual child abuse (Second edition). New York, NY: HarperCollins.
Victims No Longer is the mirror “opposite” of The Courage to Heal: an excellent,
comprehensive look at many of the results of sexual abuse. Like The Courage to
Heal, Victims No Longer is written for one gender, although Lew is much better about
acknowledging the existence of female perpetrators than are Bass and Davis. This is an
excellent book, specifically focused on men (but may be applicable to others).
Naparstek, Belleruth. (2004). Invisible heroes: Survivors of trauma and how they heal,
New York, NY: Bantam Dell.
Belleruth Naperstek’s healing imagery work is exceptional and unique. Although the
second half of the book includes healing meditations, the first half is a very readable,
compassionate discussion of trauma and its effects. Highly recommended.
Schnurr, Paula P. & Green, Bonnie L., (eds.) (2004). Trauma and health: Physical
health consequences of exposure to extreme stress, Washington, D.C.:
American Psychological Association.
One of the first book-length looks at the physical health consequences of trauma.
Very academic; written for professionals.
Siegel, Daniel J., M.D. (2010). Mindsight: The new science of personal transformation.
New York, NY: Bantam Books.
Siegel is widely regarded as a must-read for people interested in how one human brain
affects another. This book is written for the general public, but requires a fairly high
literacy level. Siegel is fond of acronyms, which will help some readers remember and
integrate his ideas. This isn’t a “trauma book,” but will help those seeking to understand
more about how the brain works and how it can be changed.
van der Kolk, Bessel A., McFarlane, Alexander C. & Weisaeth, Lars. (Eds.,) (1996).
Traumatic stress: The effects of overwhelming experience on mind, body, and
society. New York, New York: The Guilford Press.
Van der Kolk and McFarlane are considered two of the most important trauma
researchers, theorists, and practitioners. This comprehensive look at trauma is a little
old, but is still used as a primary textbook in graduate trauma classes. It’s very good
as an intellectual introduction to trauma, but was not written as a self-help or peer
counseling tool.
Wilken, Tom. (2008). Rebuilding your house of self-respect: Men recovering in groups
from childhood sexual abuse (2nd edition). Erieau, Ontario: Hope and
Healing Associates.
This book heavily quotes men who were sexually abused as children, which may be
especially useful for individuals who have difficulty reading books predominantly
focused on female survivors. The book posits steps in recovery.
Wilkinson, Margaret. (2010). Changing minds in therapy: Emotion, attachment,
trauma & neurobiology. New York, New York: W. W. Norton & Company, Inc.
This book is a good summary of some of the more recent research; aimed at therapists
and academics.
32
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
3
Transgender
Survivors of
Sexual Abuse
Sexual violence statistics and myths
Society has continually reinforced the inaccurate constructs that sexual violence is
between strangers (a man attacking a lone woman in a park or alley); on dates (where
men are drugging their female dates); or in warring countries (again, where women or
girls are the victims).
In recent years, more attention has been drawn to sexual abuse of children of all genders
(such as by coaches, priests, and scout leaders).
What most people don’t know—what we infrequently hear about—is that the actual
statistics paint a very different picture.
The vast majority of victims are assaulted by someone they know, not a stranger.
At least ¼ of perpetrators are female.
At least 33% of all sexual assault victims are male.
An estimated 44% of victims were (first) abused as children.
Many victims are sexually assaulted multiple times over their lifetimes by
different people.
Commonly-cited statistics suggest that in the U.S., 1 in 3 girls/women and 1 in 6 boys/
men experience sexual assault.
PHOTO BY KERRI CECIL
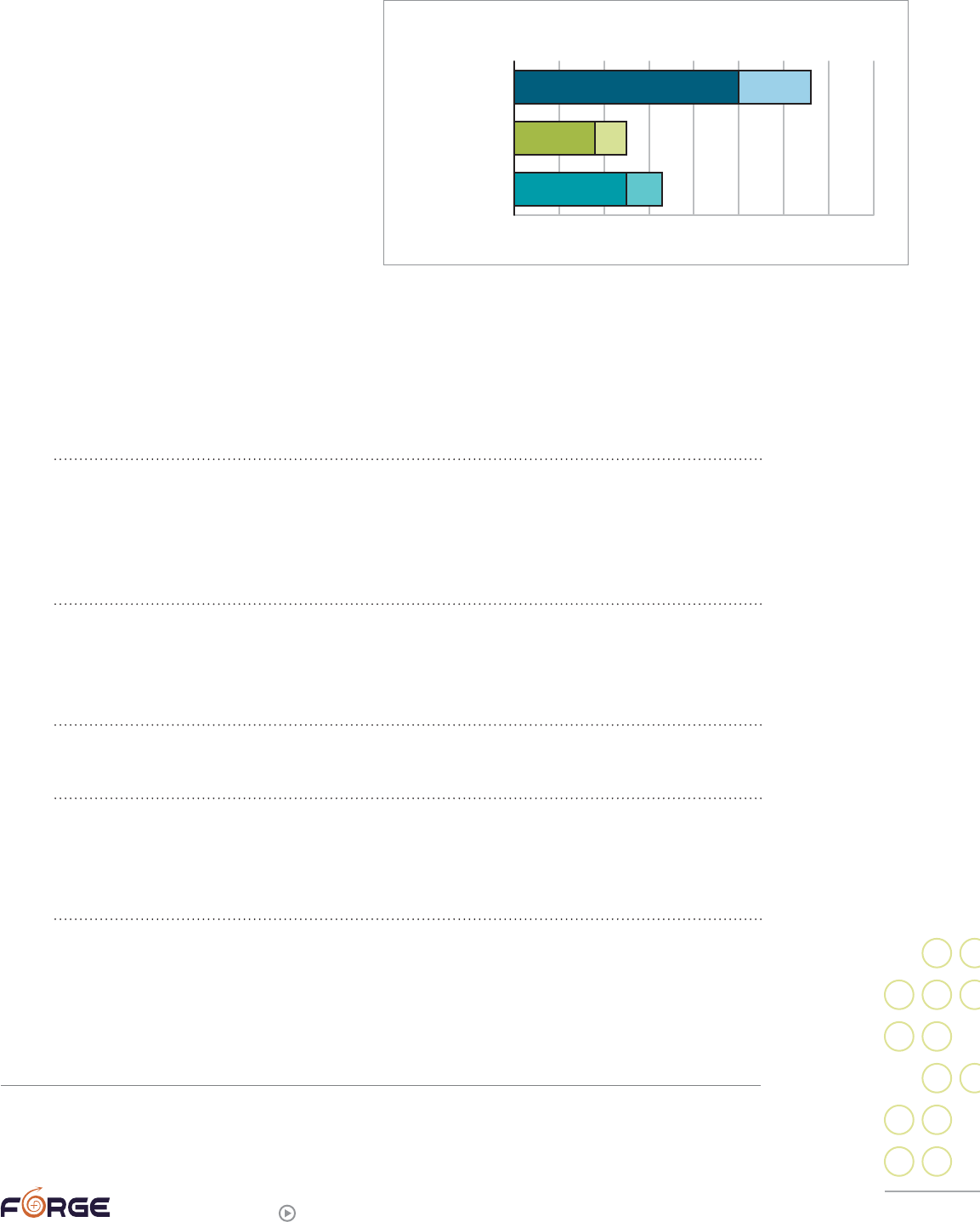
33
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
These statistics are deeply suspect,
however, because many victims either do
not recognize that they were sexually
assaulted, or choose not to discuss their
assault with anyone (and thus are never
counted). This may be especially true for
transgender survivors. The reasons for
this include:
Being too young and/or feeling
responsible
People who were sexually abused as
children may not report or talk about their abuse, often because they do not understand
that what happened was sexual assault and/or because they believe they were
responsible for what happened.
“I didn’t know what to do as a kid, thought it was all my fault. I was raised Catholic
and this was as I was being taught about sin and I thought it was because I WAS
BAD and that everyone would blame me.”
28
“My opinion about the situation varies from time to time. Sometimes I look at it as
just ‘normal stuff that happens’ among adolescents (perp[etrator] was my older
brother). I don’t feel all that ‘damaged’ by it, although it’s hard to say what the real
impact has been. I was not forced to participate, but I was also young and naïve
and couldn’t see how anything my brother wanted to do could be wrong.”
“I was date-raped approximately 6-8 times while I was in high school. I never talk-
ed about it with anyone because I grew up in a time where it was ‘my fault for lead-
ing the person on,’ getting drunk with someone (‘what do you expect?’), that sort
of thing.”
“In the beginning what stopped me [from getting help] was the belief that I some-
how caused the abuse.”
“In the 1960s through the 1970s that was something you did not talk about. As a
child growing up in the 60s you only worried about vampires and werewolves and
the people that would steal candy from children. You did not know that vampires
and werewolves were pedophiles and the candy was the innocence of children.”
28
Unless otherwise noted, all quotes were given to FORGE by transgender/SOFFA survivors in one of two studies: 2004
FORGE data from “Sexual Violence in the Transgender Community Survey,” (n=265), unpublished data. 2011 FORGE
data from “Transgender peoples’ access to sexual assault services,” a survey approved by the Morehouse School of
Medicine’s Institutional Review Board, (n=1005), data has not been formally published.
0% 10%20% 30%40% 50%60% 70%80%
50-66%
18-25%
25-33%
RATES OF SEXUAL ASSAULT
TRANSGENDER
BOYS/MEN
GIRLS/WOMEN
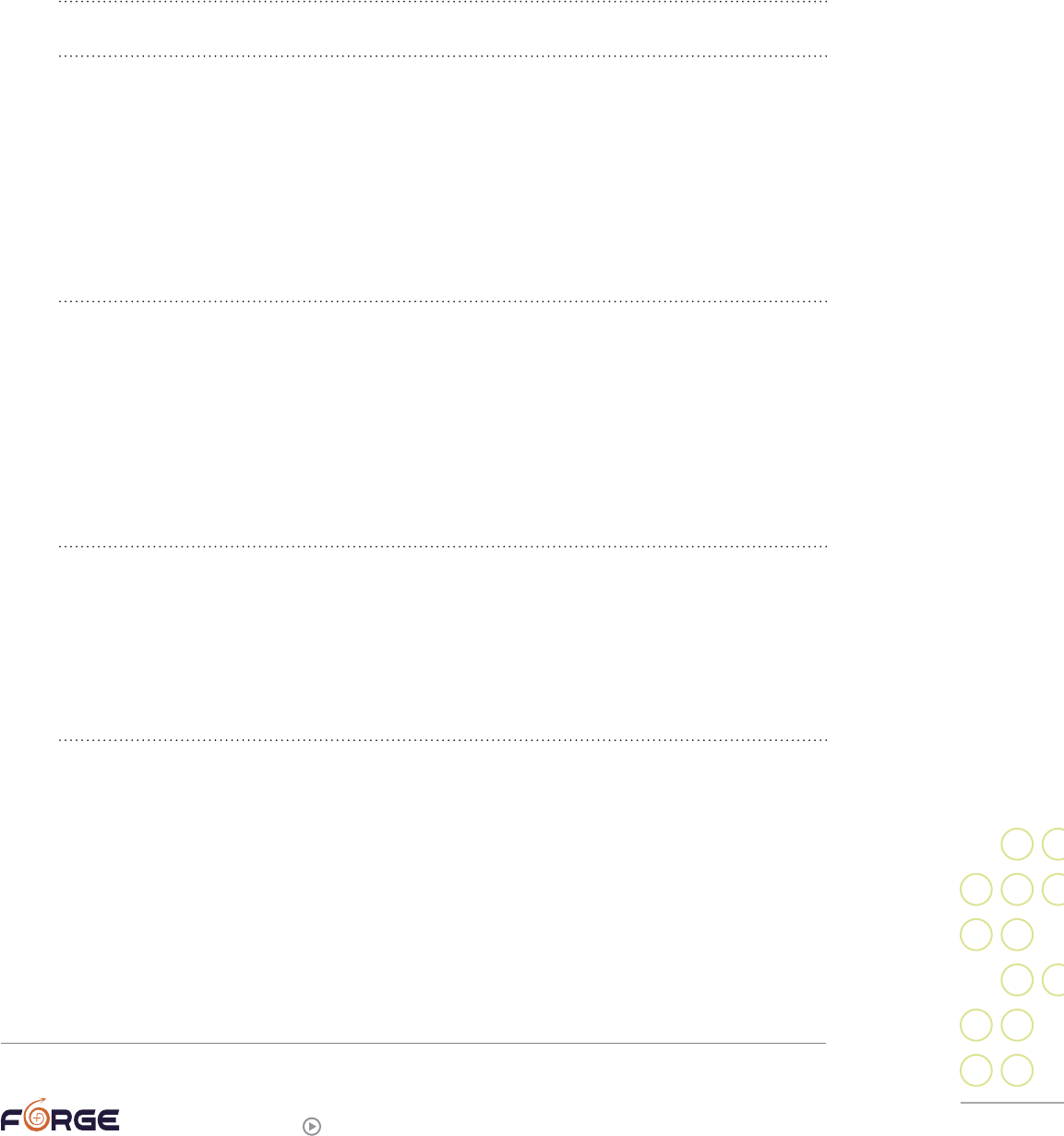
34
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Not understanding that “sexual assault” encompasses what
happened to them
Because of the strong cultural myths of what sexual assault is (and isn’t), survivors may
not see what happened to them as abuse:
“I feel a lot of confusion around those incidents and only have discussed them a
couple of times, including this time.”
“At the time (late 70s) ‘acquaintance rape’ was not a known topic.”
Individuals may not understand the healthy dynamics of consensual BDSM
.29
In these
cases, a perpetrator or abusive partner may take advantage of that lack of knowledge and
frame abusive behavior as BDSM:
“The abusiveness of my relationship was ‘masked’ both to others and myself by
the fact that it was a same-sex relationship and a BDSM relationship. My partner
took advantage of the fact that it was my first experience of the latter. I believed
that I had to consent to anything or could not withhold consent, and the abuse was
couched as ‘play.’”
The myth that sexual abuse is something that happens to us often leads individuals to
believe that being forced to perform sexual acts on another might not be considered
sexual abuse. Any unwanted sexual contact is abuse/assault.
“I’ve had trouble naming what happened as abuse. Although I know that things
happened against my will, I get angry at myself and blame myself for letting it hap-
pen—particularly because I was forced to do things to my partner rather than her
forcing herself on me. I don’t have a name for what that is but it has deeply affect-
ed my relationship to my body and my sexuality.”
It is often believed that sexual assault has to be violent for it to be assault. Threats,
persuasion, and non-forced unwanted sexual contact are all abusive.
“Sexual persuasion is not always violent—and in my case(s), it was *never* violent
per se, but was nonetheless not desired, and was hard to extricate myself from
politely, whether the events happened once or were repeated several times by the
same person.”
Being male and/or having a female perpetrator
The number of female perpetrators and male survivors are likely undercounted. Both
people who had a female perpetrator and those who were male at the time of the abuse
may not classify what happened to them as sexual assault. People who experience either
of these types of abuse dynamics are also far less likely to report these crimes to the
authorities, researchers (surveys), or even loved ones in their life. Respondents to FORGE
surveys have noted:
“D[omestic] V[iolence] theories just don’t work to make sense of a lot of abusive
relationships that seem to contradict social hierarchies, e.g. where the victim is a
29
Bondage and Discipline, Sadism and Masochism.
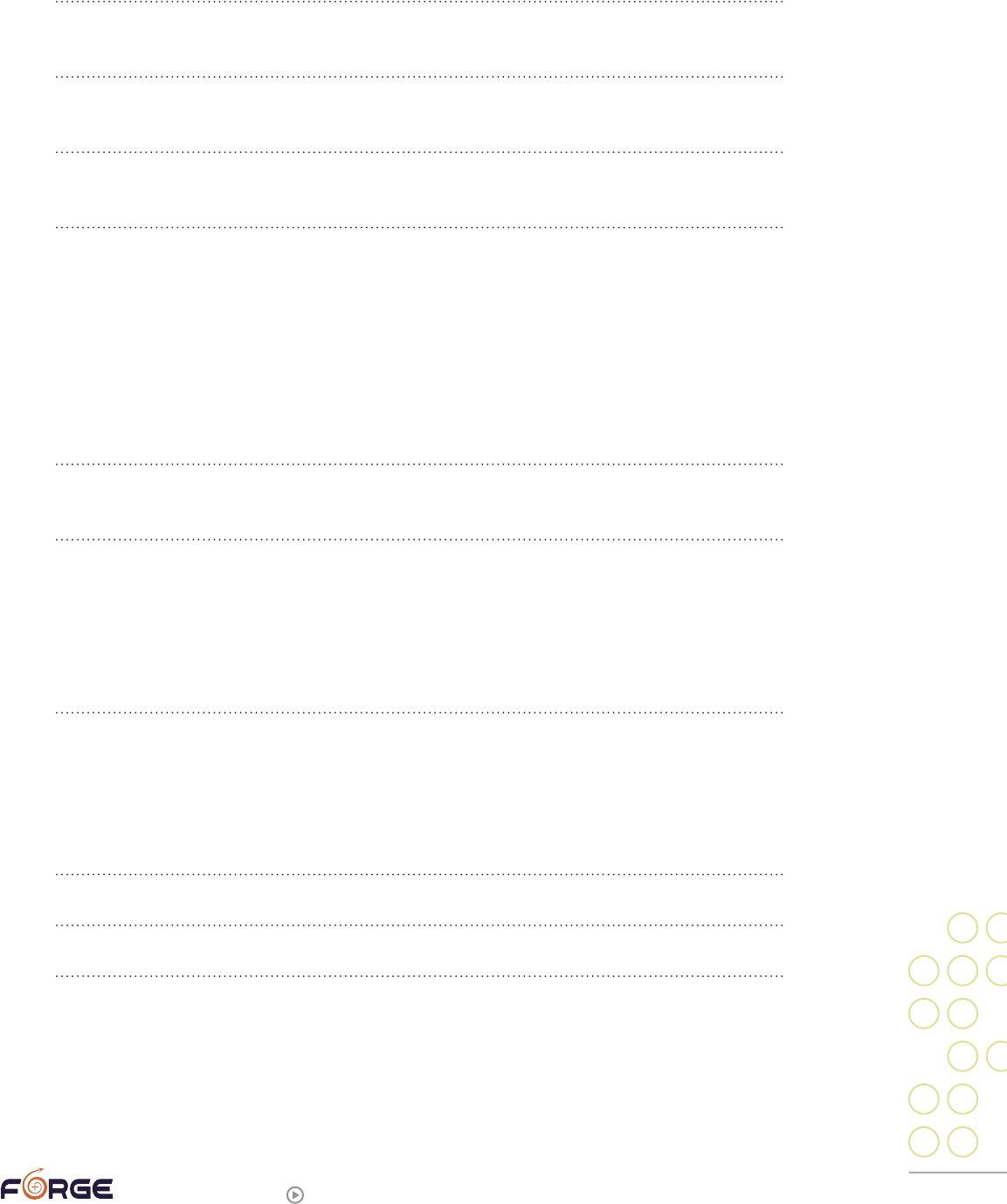
35
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
man or where the abuser is a person of colour. It’s so much harder when you feel
you need to protect a whole community, or that people might not believe you.”
“I didn’t recognize it as ‘sexual assault’ because it didn’t fit the portrayed image
(‘man’ assaulting ‘woman’).”
“I was considered a male at the time; [I didn’t report because] no one would have
believed I was raped by a female.”
“The rape happened in 1984, before anyone really believed women rape
other women.”
Experiencing additional complications due to gender identity
or politics
Transgender and SOFFA survivors may struggle with what happened to them due to their
gender identity or politics:
“I got much less support than I should’ve, as my guilt around transphobia was
key to the abuse. I ‘protected’ [abusive FTM partner] much longer because of the
transphobia [I was afraid he would be subjected to if I told].”
“I was hesitant to claim that my abuse was real abuse, and I didn’t want to ‘take
away’ services or time from ‘real’ survivors who needed them more.”
“For a long time I had a hard time convincing myself it was rape. Then by the time
I started coming to terms with what happened, I was a feminist and there was
a certain amount of shame. I then came out as queer and later became more
comfortable in my trans identity—then there was fear that people would think that
my queer trans identity was a result of being abused/assaulted or that the abuse/
assault compromised my trans identity in some way.”
Wanting to deny or avoid thinking about the trauma
Finally, it is very common for sexual assault survivors of any gender identity or history to
feel tremendous shame and/or desire to “forget” about the abuse:
“I was in denial.”
“This survey is somewhat upsetting. I’d rather forget.”
“It took a long time to even talk about it. I have never talked about some things.”
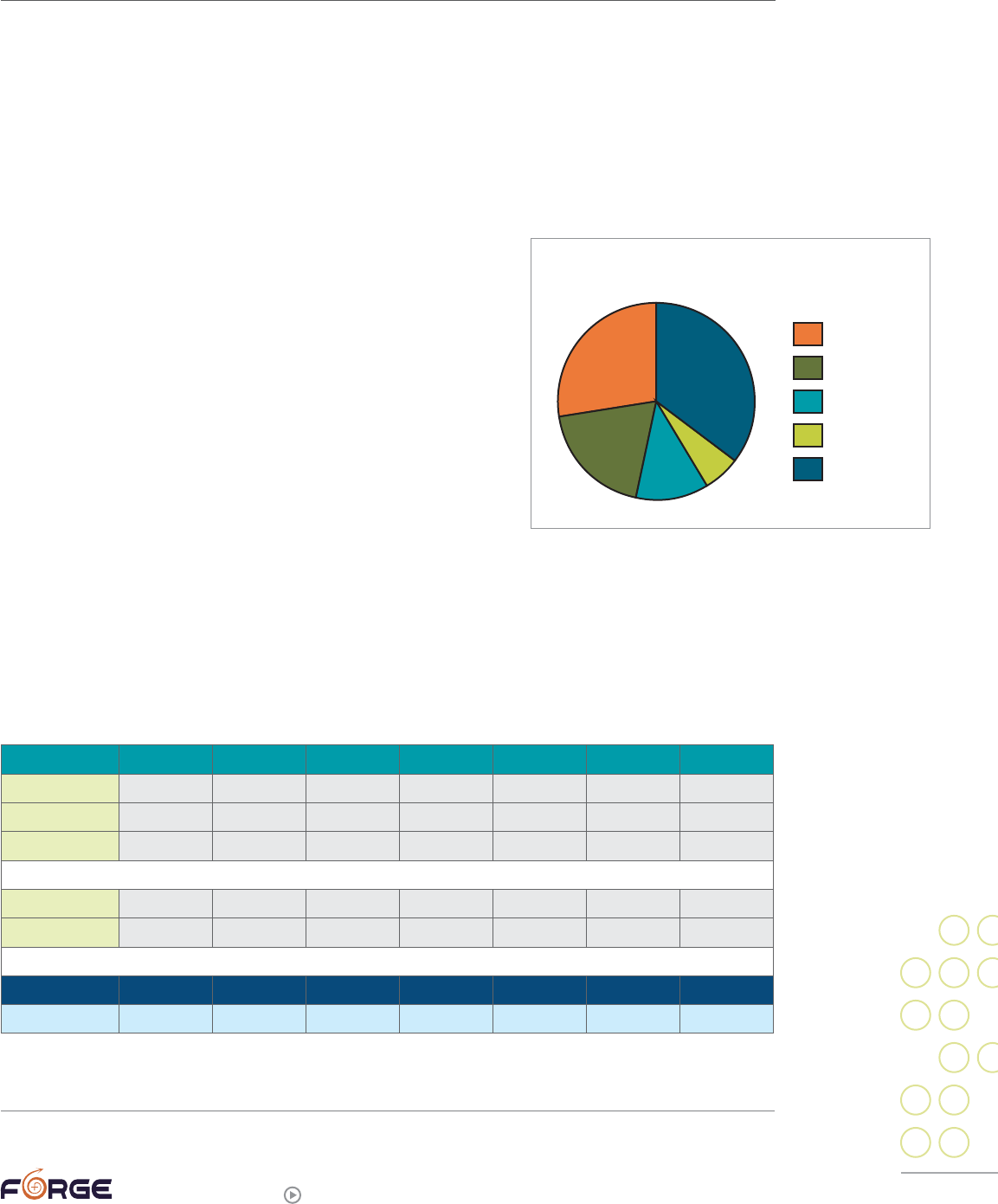
36
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Transgender sexual violence survivors data
While multiple studies have found that approximately 50% of transgender people have
experienced sexual assault at least once, FORGE has conducted the only study so far
focused solely on trans people’s experiences around sexual violence
30
. We conducted the
national study in 2004, and had 265 respondents. Nearly half (47%) were FTMs; 30% were
MTFs. About 20% were non-transgender, most of them female partners. Three percent said
they were assigned intersex at birth. Ages ranged from under 21 (6%) to over 61 (1%), with
the largest number (36%) falling between the ages of 22 and 30. Here are the highlights of
what we learned:
Most transgender survivors have
experienced repeated sexual violence.
About one third of the respondents had never experienced
sexual assault. Most of those who had had been assaulted
had experienced more than one assault: only 27% marked
that they had only been assaulted once.
Most transgender people were first
assaulted as a child or youth.
More than ¾ of the respondents (78%) reported that they
had first experienced “unwanted sexual touch” by age 12.
About one third reported experiencing their first “unwanted
sexual touch” between the ages of 13 and 40. Only 5% of sexual assault survivors reported
that their first sexual assault was when they were 41 or older. Interestingly, while most
of the nontransgender males in our survey never experienced sexual assault, people who
were assigned male at birth who (possibly later in life) identified as MTFs experienced
relatively high rates of abuse as children, youth, and young adults.
AGE OF UNWANTED SEXUAL TOUCH
0-12 13-15 16-18 19-21 22-40 41-60 None
FTM
65 45 47 42 30 1 14
MTF
23 14 8 11 18 6 26
Intersex
2 3 0 1 2 1 1
Natal Female
21 13 9 14 13 0 10
Natal Male
0 1 0 1 1 1 5
Total 111 76 64 69 64 9 56
56% 38% 32% 35% 32% 5% 28%
30
FORGE. (2004). “Sexual Violence in the Transgender Community Survey,” (n=265). Unpublished data.
NUMBER OF TIMES ASSAULTED
1X (ONCE)
2X (TWICE)
3X
4X
5+ TIMES
27%
35%
19%
12%
6%
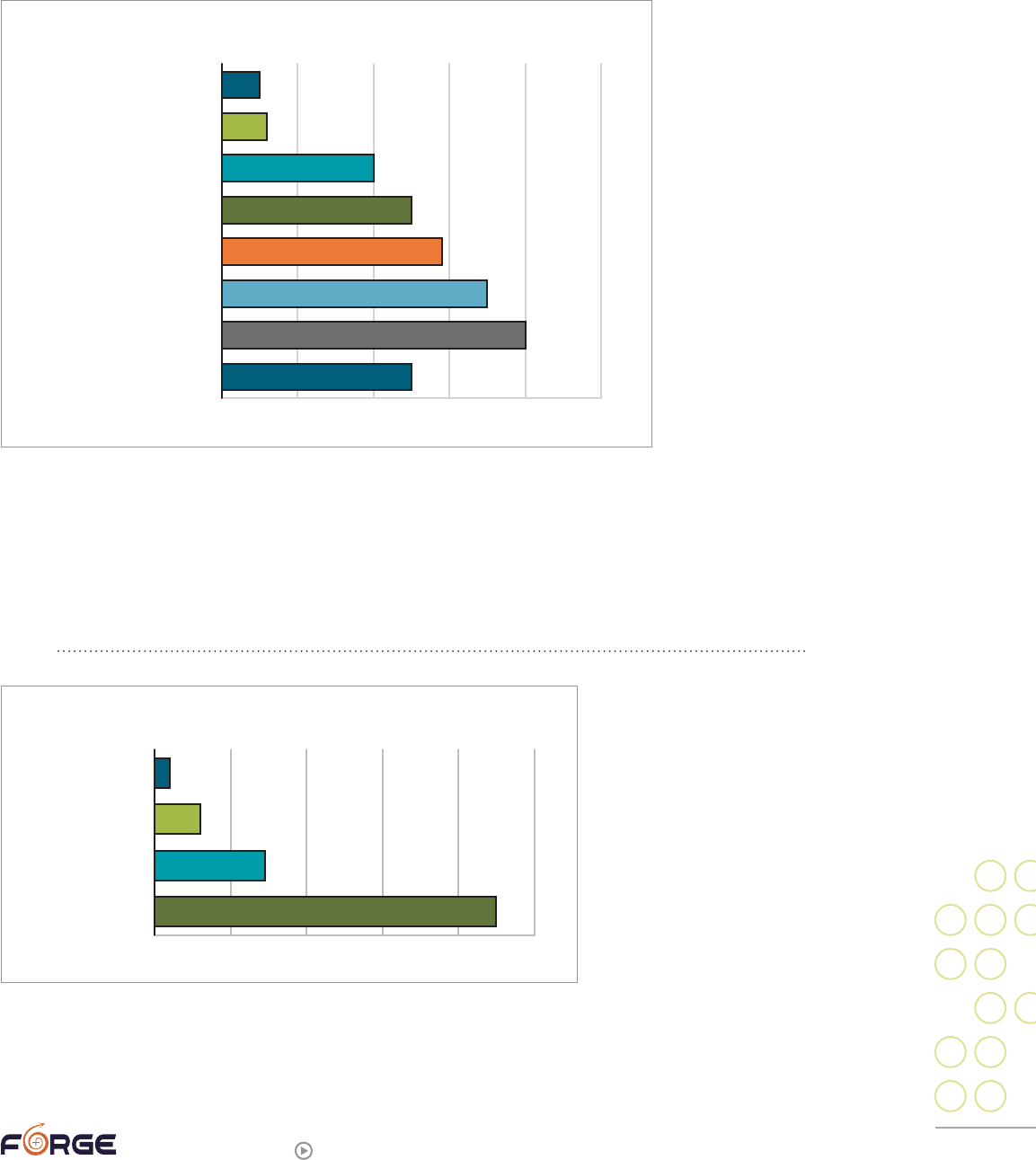
37
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Most perpetrators were known to the victim.
Consistent with what has been learned from the non-trans general public, the vast
majority of transgender survivors knew the person who abused or assaulted them.
Only 25% of perpetrators were reported to be strangers.
More than a quarter of transgender survivors have been assaulted
by females.
Nearly 90% of transgender survivors had been assaulted by at least one male, but nearly
30% had been assaulted by a female (many survivors were abused by both men and
women). Twelve percent reported abusers who were themselves transgender.
“My ex abused me because I wasn’t enough of a man for her, her words.”
0% 10%20% 30%40% 50%
RELATIONSHIP TO PERPETRATOR
A POLICE OFFICER
A HEALTHCARE/
SOCIAL SERVICE PROVIDER
A DATE
A STRANGER
AN INTIMATE PARTNER
SOMEONE ELSE YOU KNEW
A FAMILY MEMBER
OTHER
5%
6%
20%
25%
29%
35%
40%
25%
0% 20%40% 60%80% 100%
GENDER OF PERPETRATOR
UNKNOWN/OTHER
TRANSGENDER
FEMALE
MALE
90%
12%
29%
4%

38
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Gender is sometimes perceived to be the motivator of abuse.
Sometimes people cannot imagine how
gender identity or gender non-conformity might
be linked to abuse. Forty-three percent (42.5%)
of the respondents believed that gender was
a contributing factor in the abuse/assault(s),
while 29.5% said it was not a factor. 20.5% said
they were unsure or did not know if gender was
a factor.
“His abusers had been female, and as
a non-trans person and non-survivor
I ‘owed’ him sexually. It was my duty
to provide for his pleasure, any needs
and boundaries of my own were
supposedly abusive.”
Survivors rarely report the abuse.
The majority of survivors (of any gender identity) do not report their experience to law
enforcement. Only 9% of transgender survey respondents reported to the police. Twenty-
four percent (24%) of trans survivors told someone about the abuse near the time of the
assault(s). Forty-seven percent (47%) said they told no one. Ten percent “tried to” tell, and
5% were unsure or did not remember.
“When it was a man, yes, I did tell someone, when it was a woman perp[etrator]
I did not.”
“Yes [I did tell], but I didn’t perceive the experience as abuse at the time.”
“When the police were not the perp[etrator]s I did not call. I dealt with it.”
“Eventually I had my father charged some 30 years later.”
31
“I was afraid to go to the police for the last one because my attacker was a
woman and I had enough trouble trying to convince them it was a real attack
when my attacker was male.”
The abuse can leave physical scars.
Although 50% of victims reported no long-term physical scars, long-term medical
conditions, or disabilities as the result of the abuse or assault(s), 14% reported they
had physical scarring, 10% had long-term medical conditions, and 4% had disabilities
resulting from the incidents. Another 21% said they had “other” long-term problems, were
unsure, or it was too soon to know if they would have lasting physical effects from the
trauma. Despite the number of physical injuries, only 9% of respondents received
31
It is not possible in many states to prosecute a case this old due to a statute of limitations; check with a knowledgeable
local attorney if you want to explore prosecuting someone who abused you in childhood.
0% 10%20% 30%40% 50%
WAS GENDER A CONTRIBUTING FACTOR?
YES
NO
UNSURE
OTHER
29.5%
7.5%
20.5%
42.5%

39
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
professional medical care at the time
of the assault, while another 4% were
treated at home. Two percent said they
asked for medical services but did not
receive any, and conversely, some people
had physical medical care forced upon
them against their will.
Emotional scars can last a
very long time.
Perhaps in part due to the fact that so
many of the assaults were in childhood, few victims received professional emotional
support soon after they were assaulted. Only 14% got help within the first week, with
another 19% getting help within the first 6 months, and an additional 10% getting help
before the first year was up. However, 57% did not receive their first professional emotional
help until more than a year after the assault(s), with 28% not receiving help until ten or
more years after they were assaulted.
Overall, a slight majority (51%) reported that they had had professional mental health
care at some point after their assault(s). Thirteen individuals had mental health care
forced upon them against their will.
Although mental health care is not essential for healing, the earlier people can access
emotional support following a sexual abuse/assault the less likely they are to experience
severe long-term implications.
“[I didn’t get help.] It was like I had to crawl within myself and block it out.”
“I finally spoke to a shrink about it at age 35.”
“I received mental health services against my will between the ages of 5 and 17,
almost continuously. It was completely unhelpful.”
0%
2%
4%
6% 8% 10%12% 14%
16%
LONG-TERM PHYSICAL EFFECTS
YES: PHYSICAL SCARRING
YES: LONG-TERM
MEDICAL CONDITION(S)
YES: DISABILITY(IES)
15%
10%
4%
0%
5%
10%15% 20%25% 30%
TIME OF FIRST PROFESSIONAL EMOTIONAL SUPPORT
AFTER TEN YEARS
AFTER FIVE YEARS
AFTER ONE YEAR
BETWEEN 6 AND 12 MONTHS
BETWEEN 7 DAYS AND 6 MONTHS
BETWEEN 48 HOURS AND 7 DAYS
BETWEEN 2 AND 48 HOURS
28%
19%
10%
10%
19%
8%
6%
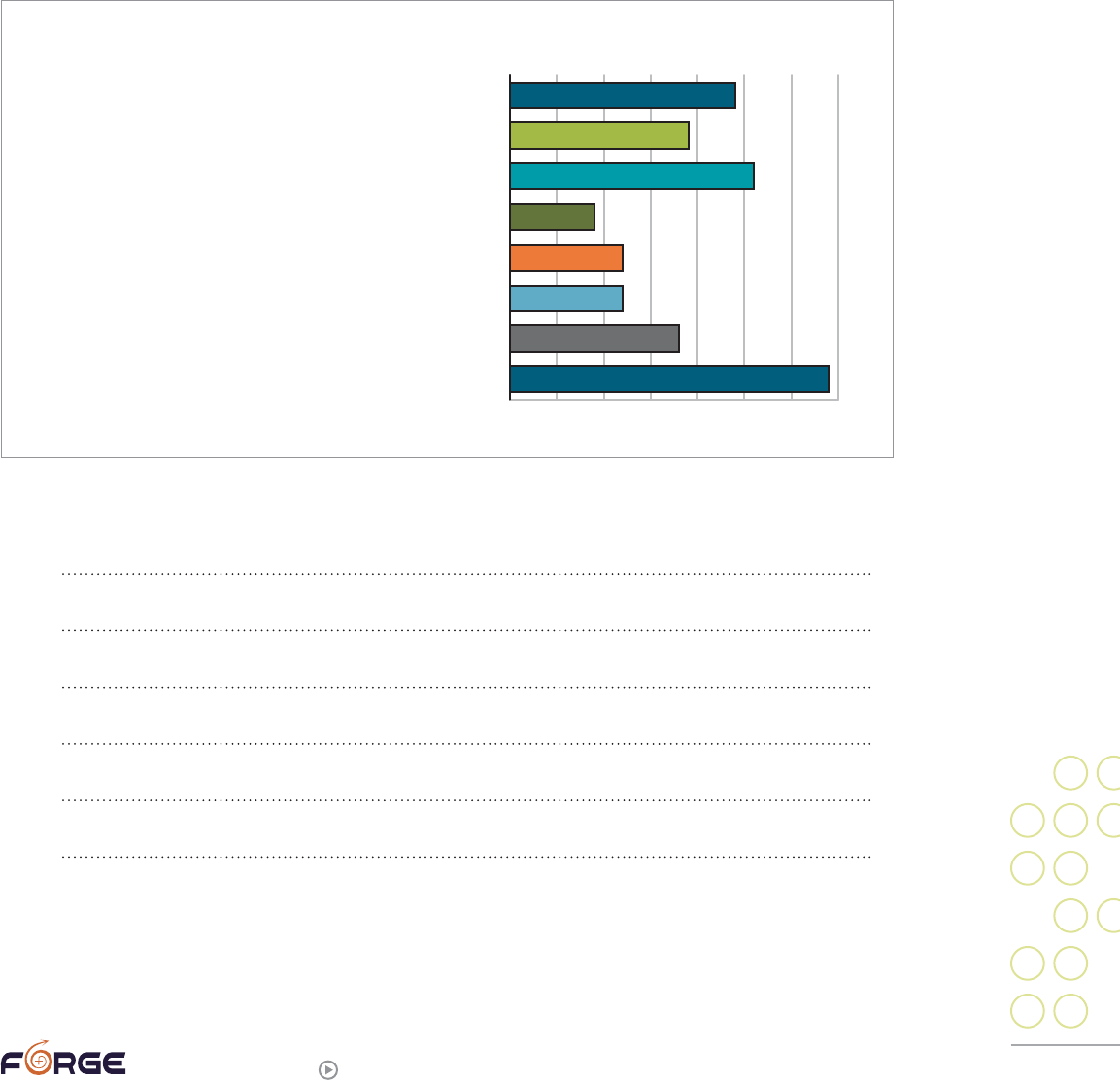
40
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Relationships are heavily impacted.
FORGE asked respondents how the sexual assault(s) had affected their intimate
relationships, allowing people to mark more than one category. The largest percentage of
respondents (34%) said they were not in an intimate relationship currently or at the time
the assault(s) took place, and 18% noted that their partner was the abuser. A total of 20%
said the effect was positive: 9% said their relationship was stronger because of the sexual
assault experience, and 12% said they supported each other through difficult times. An
additional 12% said they did not believe there had been any effect. But 26% said their
relationship was “stressed” by the assault(s), and 19% said they had broken up with a
partner because of the trauma. Another 24% gave an “other” answer.
“The effects of sexual violence are woven into the fabric of my being, all ways
have and still do affect every way I sit, walk, talk, stand, breathe, feel, think, all
affects relationship.”
“My marriage was destroyed because of the effects on me, including acting out.”
“My ability to trust people has been severely impacted by these traumas.”
“I can’t hold a relationship.”
“I am sexually dead. My partner understands this.”
“We have to work bloody hard to have a healthy relationship.”
0%
5%
10%15% 20%25% 30%35%
EFFECT ON PERSONAL RELATIONSHIP(S)
OTHER
WE BROKE UP IN PART BECAUSE OF THE TRAUMA
OUR RELATIONSHIP WAS STRESSED BY THE ASSAULT(S)/ABUSE
OUR RELATIONSHIP IS STRONGER BECAUSE
OF THIS/THESE EXPERIENCE(S)
WE SUPPORTED EACH OTHER THROUGH DIFFICULT TIMES
I DON’T BELIEVE THERE’S BEEN ANY EFFECT
MY PARTNER WAS THE ABUSER
N/A: I AM NOT/WAS NOT IN AN INTIMATE RELATIONSHIP
24%
19%
26%
9%
12%
12%
18%
34%
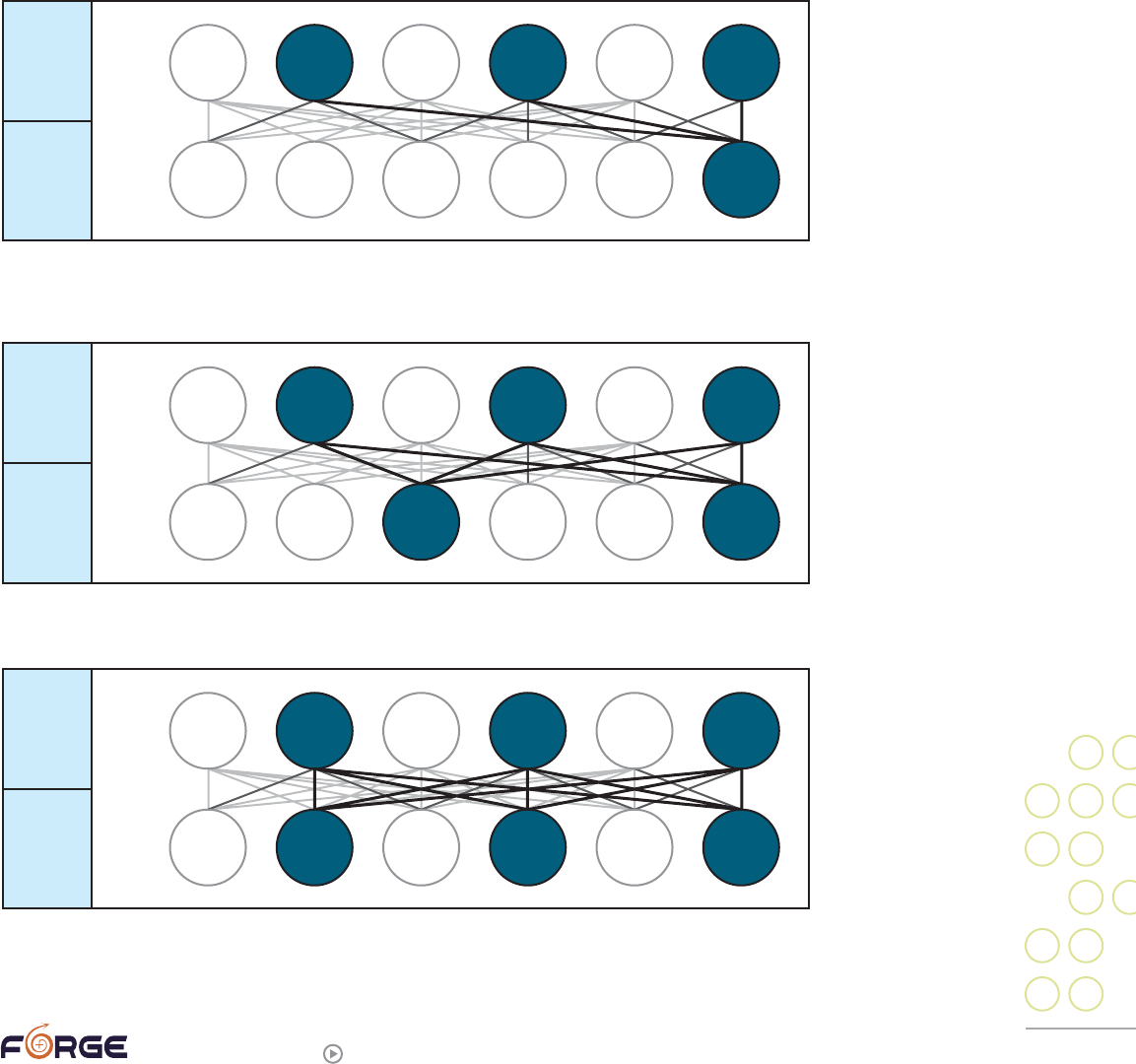
41
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Survivors often partner with other sexual assault survivors.
Of those who answered the question, about 40% said they were themselves a survivor
and had a partner or other close SOFFA who was also a survivor of sexual abuse. Twelve
percent (12.5%) said they were the SOFFA of a survivor, but had not experienced abuse
themselves. The remainder were survivors who were not intimately connected with
another survivor. FORGE created the following diagrams based on general statistics to
help illustrate how many trans couples involve two survivors. The black circles show how
many sexual assault survivors are likely to be present in any six couples with one or two
trans partners:
Sexual assault survivors in couples with one trans person and one non-transgender
male partner:
Sexual assault survivors in couples with one trans person and one non-transgender
female partner:
Sexual assault survivors in couples with two trans people:
TRANS
(1 IN 2)
MALE
(1 IN 6)
T
M
TRANS
(1 IN 2)
FEMALE
(1 IN 3)
T
F
TRANS
(1 IN 2)
TRANS
(1 IN 2)
T
T
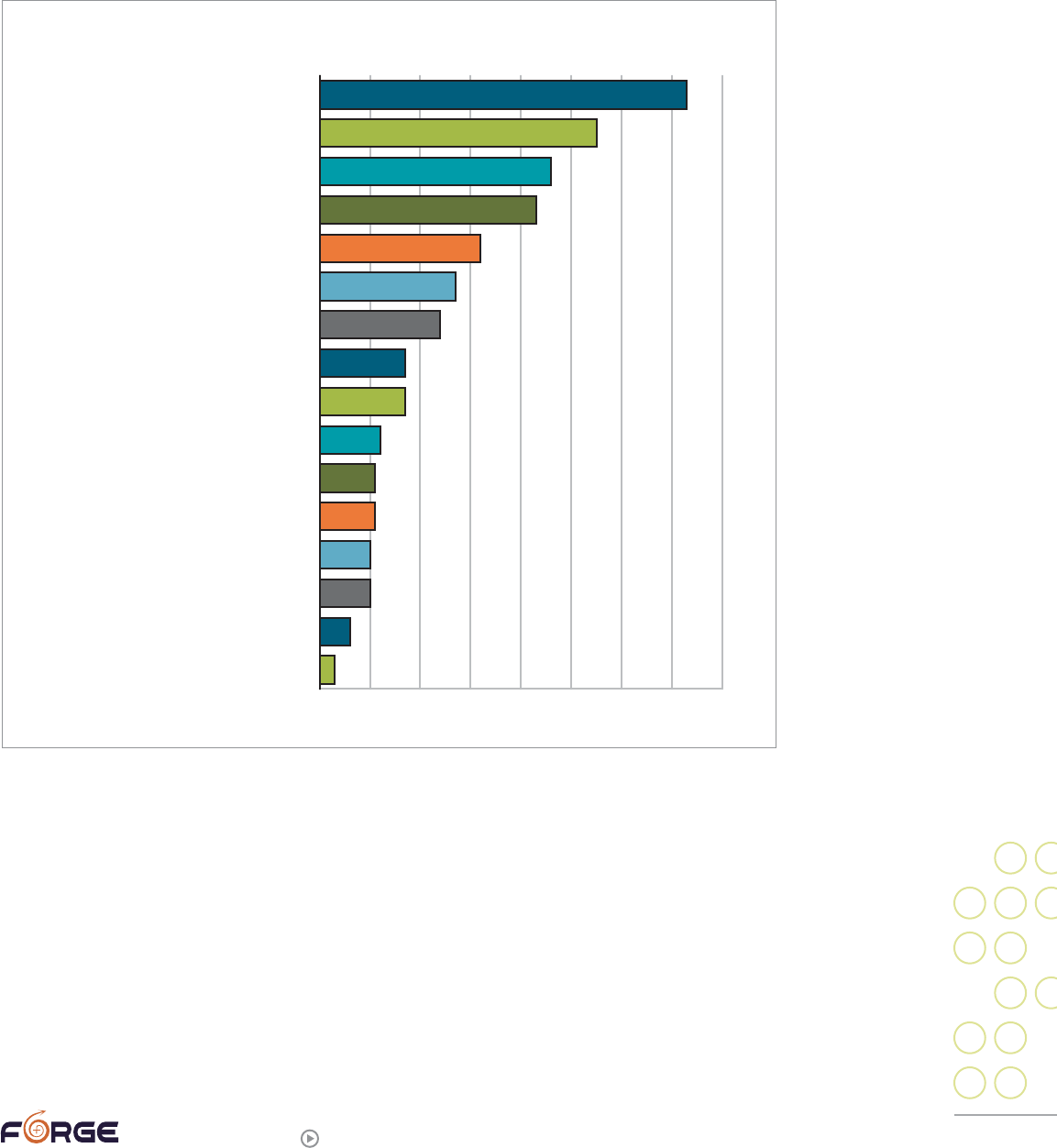
42
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trans survivors access many types of help.
Nearly three-quarters of survivors (73%) had accessed one-on-one therapy as one form
of emotional support. The next highest emotional support sources were friends (55%),
self-help books (45%), partner(s) (43%), websites (32%), and networking with other
survivors (27%). The full list of options is below:
As you can see from this chart, many trans survivors lean on friends, partners, the
internet, and self-help guides for their emotional support. That data is what lead FORGE
to create this guide and its companion piece, “SOFFA Guide”.
0% 10%20% 30%40% 50%60% 70%80%
TYPES OF EMOTIONAL SUPPORT RECEIVED
ONE-ON-ONE THERAPY
FRIENDS
SELF-HELP BOOKS
PARTNER(S)
INTERNET WEBSITES
NETWORKING WITH OTHER SURVIVORS
GROUP THERAPY
SOCIAL SUPPORT GROUP
BODYWORK
ENERGY WORK
COUPLES THERAPY
FAMILY
INTERNET CHAT ROOMS
INTERNET LISTSERVS
PASTORAL COUNSELING
FAITH-BASED SUPPORT
73%
55%
46%
43%
32%
27%
24%
17%
17%
12%
11%
11%
10%
10%
6%
3%
43
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trans-specific aspects of sexual assault
Being sexually assaulted brings a particular set of issues to a person, as does having a
trans or gender non-conforming identity. Put the two together, and some unique issues
ensue. This section will discuss several of these intersections.
Anti-trans abuse or sexual abuse?
Some trans-savvy people may wonder, looking at the list of post-trauma symptoms (see
“Trauma and its Aftermaths” section in this guide), if being transgender or gender non-
conforming by itself might cause post-trauma symptoms. We are not aware of any studies
that have looked specifically at this issue, but we believe the answer is yes. Plenty of
people who were gender non-conforming in childhood or who insisted they were not the
gender others said they were, were subjected to ongoing physical, psychological, and/
or emotional abuse by adults in their family and/or community. This combination of
possibly having been subjected to both gender-related abuse and sexual abuse is part of
what can make healing for transgender survivors more complicated than healing for non-
transgender assault survivors. Here are some things transgender sexual assault survivors
have said about the intersection of these two issues:
“By me putting up with [the sexual abuse], I thought it would help me to be ‘nor-
mal,’ not transgendered or lesbian.”
“I went to the therapist originally 6 months after separation [from ex-spouse], for
transsexualism, but realized nearly two years later, aided by people I volunteer
with, that what I had experienced was abuse.”
“I kept blaming things on trauma from the rape that were really trans-related. But,
I can see how that could be a hard call to make dealing with a queer teenager that
was raped at 8 years old.”
“[Providers could use] *lots* more education and understanding about transgender
issues, the variety of experience, and the unique way it may impact the way we
feel or cope as survivors (understanding the difference between feelings that are
a result of sexual abuse and feelings that are a result of being trans; not trying to
reduce everything to sexual abuse in order to wash over or ignore trans issues).”
Cause and effect
In a culture in which conformity is expected and non-conformity must be “explained,” many
people—trans and non-trans alike—seek explanations of how and why people are trans.
Often these explanations focus on “what went wrong” in the person’s development that led
to a trans identity. Given this framework, being sexually assaulted as a child is frequently
viewed by providers and trans community members alike as a possible “cause” of transness.
Obviously, this view can be deeply unsettling to some trans people. Some of us do not feel
our transness is a problem or something whose “cause” needs to be determined. Many
of us do not want people to view our trans identity as something that was “done” to us
by someone else’s abusive actions. Others deeply resent the implication that we “caused”
44
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
the abuse by being visibly or openly gender variant. Some of us just want to keep the two
issues separate, believing they are not causally related.
“[I’d like providers to] not think…I am trans only because of the abuse.”
“I’m afraid to go anywhere for help, because they will say my transgenderism is
related to abuse, or that I somehow egged it on by being a freak. I do not want to
have it affect my ability to rightfully claim my own identity. I was transgendered
before I was ever abused, but I don’t think they will understand.”
“Mother didn’t want the town to know I’d been raped for cross-dressing and
blamed my cross-dressing for the incident.”
“…[S]everal of the mental health providers whom I saw suggested that my sexual
and/or gender ambiguity was caused by the sexual abuse. I bought that at first.
I don’t believe that to be true anymore. I’ve healed from the sexual abuse—truly—
and I remain sexually/gendered ambiguous.”
“I, all my life was told that I brought on such assaults because of who and what I was.”
“I had to end one course of therapy because the therapist suggested my ex had
‘become’ trans because he was a child [sexual assault] survivor.”
On the other hand, some trans people do trace their gender identity to their sexual
assault history:
“All of the unwanted/persuaded sexual contact in my life has been directly
because of my being seen as female-and-sexually-attractive, and this is a very
strong contributing factor in my renouncing female identity altogether (no matter
what declared orientation), as many straight men simply do not get the clue and
assume that any personable demeanor is an invitation for their advances.”
“I understand that my gender dysphoria arises from the childhood abuse. I had
researched this area fairly carefully, and if useful, I have literature suggesting
abuse as a possible cause of gender dysphoria.”
Still others find that their gender journey has been affected by being a survivor of
sexual assault:
“This attempted rape left me afraid of men, even my father, with whom I had
been very close. I can’t be sure, but I believe that this might have delayed me
in beginning to explore FTM issues.”
Some trans people, particularly trans-masculine individuals, feel that their current
gender identity lowers their chances of being sexually assaulted:
“I live now as a man and hope that I’m less of a target but feel that I might have
even more difficulty accepting sexual assault as a man, especially as a TS man.”
“Presenting as completely male has helped me to avoid sexual/nonsexual abuse.”
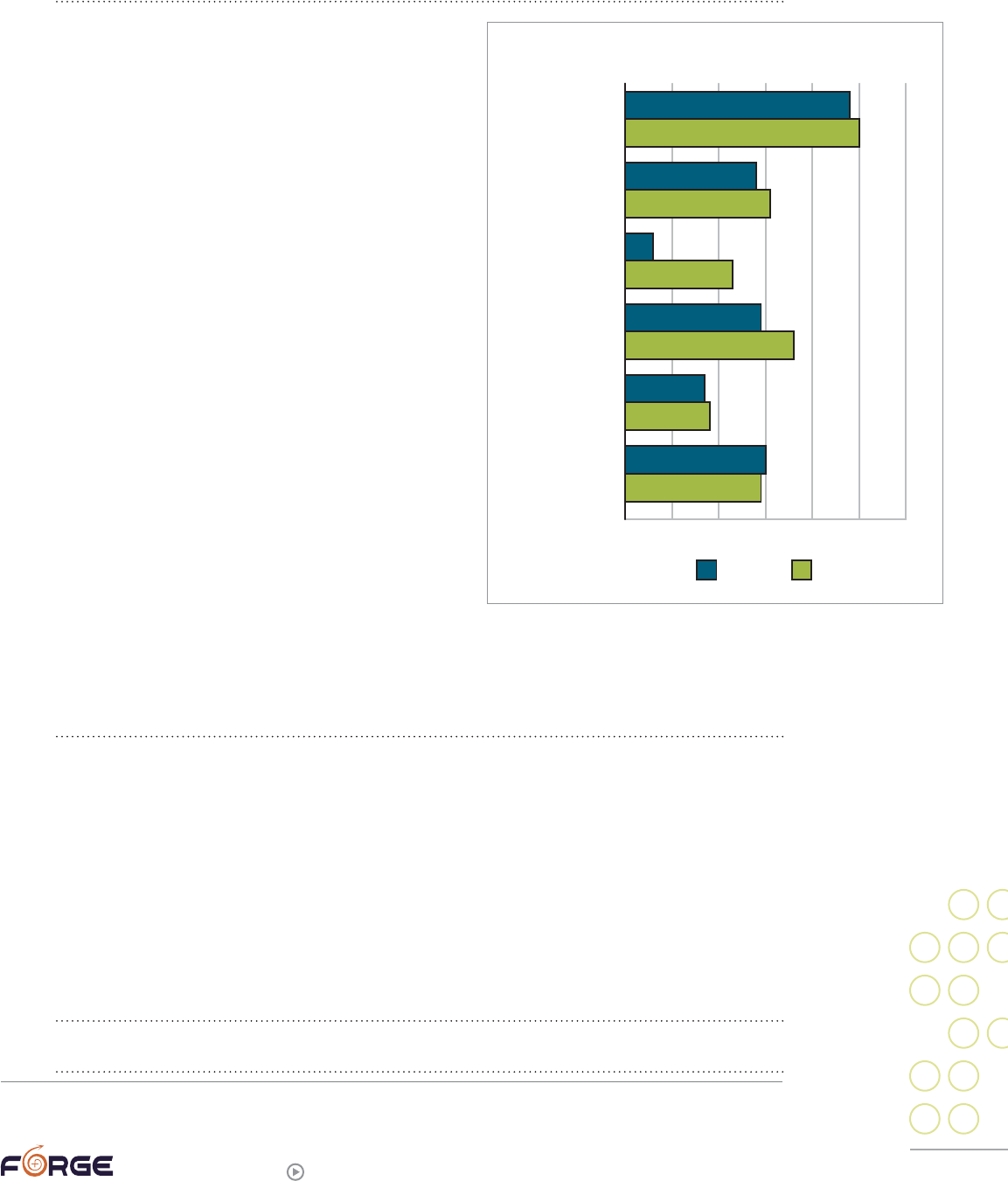
45
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
“I do not feel that Transwomen are a potential victim, as I have noticed that
potential sex offenders are very turned off by the idea. They find something
disgusting about the whole thing.”
Unfortunately, these beliefs are not supported
by statistics FORGE gathered in a 2011 survey,
which found that of 431 trans people who had
experienced a form of violence, 32% had experienced
sexual assault as an adult. Transmen actually
experienced adult sexual assault at a slightly higher
rate—31%—than transwomen, at 28%.
32
(SA=sexual
assault; DV=domestic violence.)
Trans bodies and body dysphoria
Sexual assault by its very nature is physically
invasive and often involves genitals or parts of our
body we perceive as centrally connected to our trans
identity. For many, our genitals and/or secondary
sex characteristics may feel incongruent with our
gender identities (or may even be charged with
feelings shame). People may have used our genitals
against us to oppose, deny, or try to destroy our
gender identity or self-esteem. For those who have
had gender confirming surgery, the attack
on our genitals may feel like an attack on everything
we are. It may be hard enough to expose and talk
about our bodies under typical circumstances;
exposing and talking about them in the context of
sexual assault may feel impossible.
“Had he [therapist] and I needed to explore it, some discussion or emphasis on
how vaginal penetration uniquely emasculates a male-identified biogirl would’ve
possibly been useful.”
Not being believed or minimizing the assault(s)
A pervasive problem for sexual assault survivors of all gender identities is that they are
often not believed when they report or discuss the assault(s), or are told to just “forget
about it and go on.” There are many reasons this happens: (other) people do not want to
admit how widespread sexual assault is; they do not know how to respond helpfully and
so deny there is anything to respond to; they are in denial that they themselves were (or
could be) abused and cannot afford to think about the topic; and they believe common
myths about sexual assault (for example, that it only happens to certain genders).
“Nobody took me seriously; many told me to suck it up and get over it.”
“My family didn’t have any idea what to do.”
32
The sexual assault rate for those for whom we could not determine a gender vector (N=39) was 40%; it is combining these
three gender categories that results in an overall rate of 32%.
0% 10% 20% 30% 40% 50% 60%
RATES OF VIOLENCE BY GENDER VECTOR
CHILD SA
ADULT SA
DATING
DV
STALKING
HATE VIOLENCE
48%
50%
28%
31%
23%
29%
36%
17%
18%
30%
29%
6%
MTF FTM
46
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
“I spoke with a friend who was a lawyer, she was the one who characterized it
as a seduction.”
“Most advice was just to get past it and forget it. Or that’s what I heard and have
“tried to do.”
The ubiquitous disbelief may be even worse for some transgender survivors. Adults who
believe a gender non-conforming child is confused, oppositional, or sinful may make the
same assumptions if that child also reports sexual abuse. Perpetrators may use transphobia
as a weapon, telling their victim no one will believe anything a transgender person says.
“My ex had me convinced she could turn everyone against me and take my kids
and eventually grandkids away from me and that no one would want to deal with a
queer (of whatever stripe I was) like me.”
Clearly, being disbelieved or even blamed when disclosing abuse is extremely traumatic.
Those who have experienced being disbelieved even once (let alone many times) may have
great reluctance to again make themselves vulnerable to a new person who might also
disbelieve or blame.
“I had tried to tell in the past and was either not believed or blamed for the abuse.
It took me a long time to tell someone again.”
Transgender perpetrators
It can be very confusing and upsetting for a trans person to be abused by another trans
person. Many of us believe that if anyone can understand and support us, it should be
another trans person. Because of this widespread belief, it is often difficult to imagine
that another trans person could be abusive towards us. When a trans person we love or
care for responds by assaulting us, the pain can be compounded.
“The most frequent sexual abuse I experienced was by my transgendered partner
who always knew me and valued me as FTM….ALL of the multiple occurrences of
sexual abuse/violence were with people who knew me as transgendered or who
‘valued me’ as such.”
“My ex-girlfriend who was emotionally, sexually, and physically abusive used to use
my gender questioning as ammunition. She would embarrass me by telling people
about it in front of me. She made fun of my attempts to present as a boy. She is
transsexual, and she always said I was just making things up for attention.”
Trans people can also use their experience of being transgender and/or oppressed as
an excuse to abuse others:
“He was FTM. He used him being on testosterone as one of the excuses for
his ‘needs.’”
“His abusers had been female, and as a non-trans person and non-survivor I
‘owed’ him sexually. It was my duty to provide for his pleasure, any needs and
boundaries of my own were supposedly abusive.”
47
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
A particularly knotty problem occurs when both the perpetrator and victim are part of
the same small community.
“My partner’s coerced/nonconsensual sex with another FTM has fractured the lo-
cal community into parties who believe my partner, parties who believe the perpe-
trator, and parties who don’t want to take sides (who are perceived to not believe
my partner as a result). Moreover, there’s no useful way to clear the air or hold the
perpetrator publicly responsible without some degree of ostracizing him. It’s a
really evil situation.”
“My trans ex and I are part of a very small trans community, and as a result of our
breakup, I have become largely alienated from our community. He is a respected
leader in the trans community. He spreads rumours about me.”
“When I left my ex partner I called a local domestic violence hotline that’s
trans-friendly, but it’s a small town and the person who I talked to knew who I was,
and who my ex was.”
“I called the local LGBTQ domestic violence project after I was being stalked by
my abusive (trans) ex. The person I talked to there, a transwoman, said ‘is your ex
a member of the trans community?” I said he was, and she said ‘I can’t help you,
that’s a conflict of interest.’ …Also, people in the trans community don’t take what
happened seriously as domestic violence, sometimes act like I’m just being silly
or petty when I talk about it, and refuse to understand/respect that I am just not
comfortable around that person—indicative of larger problems in the trans
community, I think.”
Service provider perpetrators
FORGE has heard many stories of trans survivors whose perpetrators were police officers,
health care providers, or others from the “public service” or “helping” fields. In our 2004
survey, 5% of perpetrators were police officers, and 6% were health care or social service
providers. These results are mirrored in more recent studies, such as the 2011 Injustice At
Every Turn
33
, which indicates that 7% of trans respondents experienced sexual assault by
police and 10% were assaulted by health care providers. Similarly, the National Coalition
of Anti-Violence Programs
34
continues to find high rates of sexual and other forms of
violence perpetrated by law enforcement and other “helping” professionals.
One assault was in an Emergency Room at a hospital, by a female doctor who I
believe was angered by my appearance (I looked male and my hospital bracelet/
chart said ‘female’).
33
Grant, Jaime M., et al (2011). Injustice at every turn: A report of the national transgender discrimination survey, National
Center on Transgender Equality and National Gay and Lesbian Task Force.
34
National Coalition of Anti-Violence Programs: http://www.ncavp.org
48
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Many others reported being physically assaulted or verbally abused by professionals
from whom they sought help:
“The health care providers were trying really hard to be accepting. But the officers
were horrible. They accused me of deserving it; accused a friend when I went with
her to report it. They actually took us in separate rooms when I went with her and
tried to get me to say that she did it to herself because it was a wiccan thing.”
“My friend and I were both in police custody at the time…during my interrogation,
I was threatened with rape by the officers and mocked for my perceived sexual
orientation [gay male], but I was not physically assaulted. She, however, was
shoved to the ground multiple times, put in painful pinning holds, and had her
genitals grabbed multiple times while the officers mocked and harassed her about
her gender identity.”
“I felt that the residents in the [emergency room] felt that being transgender meant
I had some ‘sexual fetish’ and that I exposed myself to high risk situations (which
wasn’t the case, it was partner-abuse). It pissed me off that they didn’t listen or ac-
knowledge the things I told them! :ugh: They were very judgmental, it was annoying!”
“I was homeless and desperately poor when the worst abuse took place. I was on
welfare. The day I was beaten by 4 cops was at the welfare office. I reached out
for help and I got bashed for it. Every time I tried to get help I was turned away.
The welfare agency treated me as badly as the police did. What stopped me from
getting the help I needed was the people I asked for help. Thankfully I found my
own way within the system to get help. No thanks to the various agencies.”
“All I wanted was [sexually transmitted disease] screening, but they wouldn’t pay
for it unless I filled out a police report. The cops mocked and humiliated me.”
“The only real indignity I suffered, apart from the sexual assault itself, was that the
police referred to me as ‘he/she’ in the police report.”
Meeting complex needs within a basic service system
The current service system
35
for sexual assault survivors was largely designed for
women sexually assaulted by men. The gendered and heteronormative assumptions upon
which the service system is built can make finding suitable services very difficult for
transgender survivors and secondary survivors:
“There was a survivor of male childhood sexual abuse group in my community, but
until I transitioned completely physically, I could not attend it. Once I transitioned,
I didn’t need the group.”
“[I needed] services that either weren’t gender specific or were for trans-identified
people. My experience and emotions surrounding the incest etc. are different from
bio-males or bio-females. I didn’t belong in any men’s groups or women’s groups.”
35
For recent changes to sexual assault services funded by the Violence Against Women Act, see Appendix C.
49
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
“I wanted to be hooked up with other local SV survivors, but no one could do that
for us. Because we are a ‘heterosexual’ queer couple, we were also excluded from
services that were provided for one-sex only and/or because services were not
available to partners.”
Fortunately, even though the majority of services are still focused on non-trans female
survivors, there are a growing number of healing and supportive options for trans
survivors through both mainstream service providers, as well as some LGBT Community
Centers and LGBT Anti-Violence Programs. FORGE also offers virtual/internet-based
support for trans survivors (See page 62 for more details).
Complicated relationship with therapists
Although this is changing, for many years the only way transgender people could access
hormones or gender confirming surgery was to consult with a therapist who, after as
many sessions as the therapist deemed appropriate (often an out-of-pocket cost for trans
people), would write a letter assuring the health care provider that it was okay to provide
the requested health care services. Not surprisingly, many trans people have never told
their gender therapist about being sexually assaulted and/or having trauma symptoms,
to ensure that this “complication” could not be used as an excuse to deny or delay writing
the hormone or surgery “permission” letter.
“I never admitted [being a sexual assault survivor] yet to a therapist.”
Unscrupulous therapists could also use this system to blackmail and coerce their
trans clients:
“I was inappropriately used sexually by my gender therapist…. He began
sexually advancing to show me how to be a ‘real man,’ as a way of modeling
masculine behavior. It became obvious that I needed to be sexual with him in
order to receive the required letter to have chest surgery. We had sex a countless
number of times—sometimes in his office, sometimes my house, sometimes he
would make me take him out to dinner and pay the bill. When I realized that this
was wrong, I asked him for my surgery letter so I could discontinue ‘therapy.’ He
refused and I had to pay thousands of dollars to reestablish a relationship with
another therapist in order to get a surgery letter.”
It can also be very difficult to find a therapist who is simultaneously trans-savvy, trauma-
informed, and affordable:
“Couldn’t afford off-campus therapy while I was a student cuz I was a student
that shit is expensive as is. So I couldn’t access a counselor who actually knew
anything about trans people and was stuck with the free folks on campus who told
me I couldn’t be trans cuz I wasn’t masculine enough.”
One couple’s therapist’s myths about the connections between masculinity, child sexual
abuse, and re-enactment caused serious harm. When one person, a childhood sexual
assault survivor, decided to transition from female-to-male, the therapist he and his
partner saw “warned” his partner that because male sexual assault survivors turn into
perpetrators, their child was no longer safe alone with him.
50
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
And, of course, some therapists simply are not skilled enough to meet some clients’ needs:
“When I was looking for other therapists, I was met with resistance and disbelief
that my former therapist was sexually abusive. There seemed to be an ‘old boys
network’ where all the therapists protect each other—even when there is great
harm perpetrated by one of them.”
“I’ve never been in an emotional support environment where I felt safe discussing
transgender issues.”
Intersectionality
“Intersectionality” refers to the piling-on of issues that happens when people are
members of more than one minority group, or are dealing with multiple issues at the
same time. Belonging to multiple stigmatized minorities seems to raise the chances of
running into problems with service providers, as illustrated by this person talking about
facing barriers to accessing services:
“Yes—race (& sexuality) [were other barriers to service]. Being pathologised as a
mixed-race bisexual, being the only bi [person of color] in my [domestic violence]
groups, not being able to afford long-term therapy.”
Survivors themselves may become overwhelmed by how many issues they seem to
be facing:
“My partner’s father is his grandfather & he was beaten & sexually abused. Mom
was a junkie. What kind of services can really make a difference after those kinds
of traumas?”
Although survivors of sexual assault face many issues in their healing journey and
transgender survivors may face even more, it is critical to remember that just by
surviving as a trans or gender non-conforming person, you have already demonstrated
tremendous resilience. Sexual assault specialist Mike Lew defines the recovery goal
this way:
“Recovery is the freedom to make choices in your life that aren’t determined by
the abuse.”
36
Just by being trans, you already have demonstrated an ability to not be defined by what
others have said and done to you. Other sections of this guide will, we hope, give you
further tools and ideas about what else you can do to shape your life in the way you want
and deserve.
36
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual child abuse (2nd edition), p. xxiv.

51
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Options
for Healing
4
There are more ways to heal and recover from sexual assault or abuse than there
are survivors. What any given survivor finds helpful may seem strange or even
counterproductive to another.
This section will briefly address some of the primary methods some survivors have used,
and then list both mainstream services and FORGE services that you might find helpful.
In the last section of the guide you can find a small selection of self-help techniques that
will illustrate the diversity of what is available to you.
Talk therapy
FORGE has found that around 75% of the trans people we have surveyed have seen
individual therapists at some point. Because there are so many types of therapists and
so many issues for potential therapy clients to think about, we have written a companion
guide specifically on this issue: “Let’s talk about it! A transgender survivor’s guide
to accessing therapy.”
Therapy has many different styles and theoretical approaches. Similarly, therapy may
be one-on-one, focused on healing within an intimate relationship, or may even involve
resolution or support with an abusive family member. Therapy can also be group vs. more
individual/personal.
Often people choose both therapy and other forms of healing, wellness activities, or
services, or may end up trying many different things until they find something that works
for them. What follows are just some of the major options.
PHOTO BY KERRI CECIL
52
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Medication
Many people are opposed to psychoactive medications, preferring to avoid chemicals or
simply “do it on my own.” As this guide’s section on the brain and trauma indicates (see
page 13), however, trauma experiences change the chemistry and the workings of your
brain. Medication may help with some of these imbalances, thereby giving you a more stable
platform on which to build the life you want. In other words, medications are not a cure-all;
they simply may make it easier to get on with your other healing and life-creation work.
Although medical science continues to advance, how some medications work is still
unknown or unclear. We still do not know how an individual may react to any given
medication until they try it, so prescribing can be viewed as a try-and-try-again process.
If one medication does not work for you, it is often worth trying another, since even
medications within the same class of drugs will often have different results. Try to find
a medication prescriber—a psychiatrist, a primary health care provider, or a free or
low-cost clinic—that you feel comfortable with, as the two of you will need to be a well-
communicating team to find what will work for you.
There are many tried-and-true medications to address depression, anxiety, sleep
disturbances, and some of the other common symptoms of PTSD. If you would like to read
more about medication options, there are good sections in the following books:
Body-based therapies
Many people believe that trauma memories are
stored in the body’s tissues as well as in the brain,
and that certain types of body-based modalities like
massage or craniosacral therapy can help your body
physically release them. You do not have to believe
that to find it healing to be touched in a consensual,
respectful, professional way. In fact, negotiating a
massage with a professional can be an excellent way
to practice setting boundaries and experiencing what
it is like to be touched by someone who will respect
those boundaries. It may also teach you things about
your body and its reactions; FORGE interviewed a
survivor who is both trans and living with multiple
disabilities who talked about his first massage, and
what he has learned about massage and survivors;
you can find directions to the audio clip in a sidebar.
JOE MICHAEL
RECORDED INTERVIEW WITH JOE AND MICHAEL
If you are interested in hearing a trans survivor
sexually abused by his mother as a child talk
about his experiences both receiving and giving
therapeutic massage, go to www.forge-forward.
org/event/disability-trans-survivors and click on
the second recording on page, “Interview with
Joe.” The relevant section is from 22:00 to 26:00.
Additional readings on medications
Briere, John & Scott, Catherine. (2006). Principles of trauma therapy: A guide to
symptoms, evaluation, and treatment. Thousand Oaks, California:
Sage Publications, Inc.
See especially pages 185-230, “Biology and Psychopharmacology of Trauma.”
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the
spectrum. New York, NY: W. W. Norton & Company, Inc.
See especially pages 131-135, “Medications.”
JOE’S PHOTO BY RICK MOTZKUS / MICHAEL’S PHOTO BY COLLEEN SWARTZ
53
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Some survivors have also found energy-based work to be very helpful. These modalities,
such as Reiki, are based on the idea that we have energy fields around our bodies that
can be influenced by others, even from far away. You can do an internet search for Reiki
practitioners in your area, or you can access a free, Reiki-based distance healing service
that many trans Reiki practitioners are involved with at http://www.the-dhn.com/
Acupuncture is another modality some survivors use. In this practice, thin sterile needles
are placed in particular places on the body to increase energy flow and resolve physical
and emotional “blockages.”
“Tapping” modalities such as Thought Field Therapy, Emotional Freedom Technique, and
Tapas Acupressure Technique work on a similar premise, in which at least part of the
technique involves the person (or someone else) tapping them on particular parts of the
body in a set pattern.
The list of body-based and/or energy-based therapies is long and constantly growing. If
your area has a “New Age” type newspaper or magazine, that is often a good place to look
for body or energy based services in your area.
Additional readings on body-based and alternative therapies
Cori, Jasmin Lee. (2008). Healing from trauma: A survivor’s guide to understanding your
symptoms and reclaiming your life. Philadelphia, Pennsylvania: Da Capo Press.
This is one of the best self-help books we have seen for trauma survivors. The author is both
a therapist and a trauma survivor, and her book draws on both experiences. She addresses
the reader as “you,” so it’s an easy read for those who don’t see themselves in works
that talk about “men” and “women.” Although not exactly a workbook, each chapter does
include questions readers can ask themselves to help apply the chapter’s topics to their
own experience. This book contains one of the more complete discussions of various types
of body-based trauma therapies.
Levine, Peter A. (2010). In an unspoken voice: How the body releases trauma and
restores goodness. Berkeley, California: North Atlantic Books.
Peter A. Levine, Ph.D., is one of the leaders of those helping people work through their
trauma by moving their bodies in the way they would have wanted to move to escape or
fight back in the original trauma. This book also contains a long exploration of how he sees
this work connected with spirituality.
Ogden, Pat, Minton, Kekuni, & Pain, Clare. (2006). Trauma and the body: A sensorimotor
approach to psychotherapy. New York, NY: W.W. Norton & Company: 139-161.
Although this is a book for therapists, it is devoted to a topic that is rarely discussed
elsewhere: why and how the *body* has to be involved in trauma resolution. It may
therefore be very interesting if you have found that more traditional “talk” therapies are not
working for you. Unfortunately, it does not include advice on finding a therapist who uses “a
sensorimotor approach to psychotherapy.”
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the
spectrum. New York, NY: W. W. Norton & Company, Inc.
This is a good book to consult if you are trying to figure out what kind of trauma therapy
might fit you best. Also includes some techniques from various schools of therapy that might
be useful to SOFFAs or for self-help.
54
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Movement-based therapies
Just about anything you can do to move your body can help your emotional
well-being. Study after study has found that exercise (of virtually any
intensity level or duration) provides physical and emotional benefits, including
the reduction of depression and anxiety. Part of the improvement is immediate,
due to the brain’s release of endorphins (the “feel good” chemicals), and part is more
long-term, resulting from increased circulation and possibly improving your sleep. So
anytime you can make yourself get up and take a walk, let alone engage in something
more strenuous, do so!
People living with physical or other body-based disabilities can also benefit from
movement. For some, this will be passive movement, where others are moving our bodies,
or activities such as floating in a pool.
In addition, certain practices, such as yoga or Pilates, have other benefits for trauma
survivors. These exercise programs can help the sexual assault survivor re-connect in a
good way with their body, re-learning what the body feels like and what it is like to be
“in.” They can also help survivors strengthen their muscles and feel more confident in
what their body can do. Keep in mind that yoga and Pilates are not just for those who
are thin, flexible or able-bodied. There are many emerging resources for people who have
limited range of motion and/or who are larger bodied.
Martial arts or other types of self-defense classes have the above benefits plus can help a
survivor feel more able to defend themselves in an emergency and can provide a feeling of
greater safety in the world.
Apart from the health benefits from exercise, many survivors find that just being in
nature—walking, gardening, or even just sitting—is by itself healing and “grounding,” a
word that some interpret to mean feeling more like you belong on the earth, as well as in
your body.
Other “alternative” therapies
Guided imagery is a powerful way for survivors to reshape their mind and thoughts.
Although there are many books and audio recordings, Belleruth Naparstek is an author
and guided imagery specialist who is also trauma-informed. She wrote the book Invisible
Heroes: Survivors of Trauma and How They Heal (2004) and maintains a multi-media store
at http://www.healthjourneys.com/default.asp. Naparstek’s guided imagery materials
guide the listener through an imaginary journey designed to provide relief and soothing of
a particular troublesome issue. Her inventory includes many topics of interest to trauma
survivors, including imagery to address posttraumatic stress, insomnia, depression,
and addictions. Many people find her voice extremely pleasant and so buy her CDs or
downloads, but for those who would like to make their own recordings (or have a loved one
make them), scripts for many are in her Invisible Heroes book.
Hypnosis is another option that some survivors pursue. A trained hypnotherapist can help
you go into a deeply relaxed state where the “judgmental” part of the mind is bypassed
and the subconscious part of the mind is open to positive suggestions for change. Trans
hypnotherapist Samuel Lurie (www.tghypno.com) notes that “even without addressing
specific ‘issues,’ the deeply relaxed state is itself an invigorating, pleasant experience.”
His website explains more about how this modality can be helpful; the page at
http://www.tghypno.com/Trans.html addresses how he works with clients long-distance.
PHOTO BY KERRI CECIL
55
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Another extremely common modality—one that is incorporated into many other types
of therapy—is breathwork, or using your breathing to help calm your emotions and
thoughts. A couple of breathing exercises are included in the Self-Help portion of this
guide (See page 90).
Faith-based support
A personal non-religious spirituality or belonging to a religious or faith tradition is
an important part of many trans survivors’ lives, and can be the source of a great deal
of comfort. Spiritual or religious gatherings can also be a source of community and
person-to-person support. If you were part of a religious tradition as a child but moved
away because of its anti-trans teachings or practices, you may want to re-investigate
whether there are LGBT-affirming congregations or faith-based organizations now in
your area. Many faith traditions have developed LGBT-affirming policies, and you may
be pleasantly surprised to be able to re-connect with a faith tradition that now overtly
includes you. Another alternative is to seek an LGBT-affirming faith-based group such as
the Metropolitan Community Church (http://mccchurch.org/) or Unitarian-Universalists
(http://www.uua.org).
You do not have to be part of a religion or group to use prayer, read spiritual texts or
connect to a Higher Power. Feel free to find and connect with what brings you comfort,
regardless of whether it brought comfort to or was meaningful for others in your family
or ancestry. You don’t necessarily need to join a church, synagogue, or other religious
home to talk with a pastor, priest, rabbi or other religious leader and/or to join a prayer
group or faith-based discussion group. If you are unsure how they might react to a trans
survivor, ask a local LGBT Community Center or other LGBT organization for leads to
religious leaders they know are LGBT-affirming.
There are a growing number of trans-focused spiritual resources available online and
in person.
TransFaith
TransFaith is a national non-profit that is led by transgender people and
focused on issues of faith and spirituality. They work closely with many allied
organizations, secular, spiritual, and religious, transgender-led and otherwise.
They bring people together to develop conversation, strategy, and community in
order to help us all reach our full potential.
http://www.transfaithonline.org/
The Spirit of Transgender
The Spirit of Transgender and The Tree House is located in Black Mountain,
North Carolina. They host multiple spiritual retreats, specifically for
transgender individuals and loved ones, at a beautiful, secluded, wooded
mountainside private retreat home.
http://www.trans-spirits.org/spirit_of_transgender.html
Cauldron Farm
Cauldron Farm is located in central Massachusetts and hosts many pagan-
focused retreats, rituals and events throughout the year, many of which are free
or very low cost. The Farm has ample space for camping during the retreats.
http://www.cauldronfarm.com/

56
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Raven Kaldera
Raven Kaldera is an author, shaman, educator, activist, and priest. He is
available for in-person shamanic healing at his office in Massachusetts.
His website links to many of his books focused on spirituality, including
Hermaphrodeities, Urban Primitive, MythAstrology, Pagan Polyamory, The
Northern Shamanic Herbal, and Talking to the Spirits: Personal Gnosis
in Pagan Religion.
http://www.ravenkaldera.org/
Easton Mountain
Easton Mountain is a community, retreat center, and sanctuary created by gay
men as a gift to the world. Through workshops, programs, and events they
provide opportunities to celebrate, heal, transform, and integrate body, mind,
and spirit. Some of their events are gender segregated (and some are open to
any gender). They have been welcoming of trans* individuals participating in
their events and many have found both the space and fellowship to be healing
and transformative.
http://eastonmountain.org/
Peer-to-peer help
It can be tremendously healing to share your experiences with another survivor or a
supportive listener. Sharing is particularly important as an antidote to shame, since
shame thrives in secrecy. Being able to talk about what happened to you, how it made you
feel, or how your life has been affected with someone who understands or can listen with
compassion can help relieve some of the toxicity.
Peer-based assistance can be formal or informal, set up by someone else or arranged by
you. Although most trans support groups are not designed to be therapeutic in nature,
you may benefit from attending as a way of gaining general support and connecting with
others who are also survivors. (Since at least 50% of trans people have experienced sexual
assault, you will have a 1-in-2 chance that you may meet another survivor.) Even if you
meet people who are not survivors, you may discover you connect on a friend-to-friend
level and want to pursue deeper conversations outside of the support group structure.
(If you do attend a trans support group, consider pointing the facilitator(s) to FORGE’s
companion guide, “Facilitators’ Guide”)
You may also want to look online for people to connect to, who share similar backgrounds
and experiences. FORGE offers a variety of listservs and social media options specifically
for sexual assault survivors (see http://forge-forward.org/anti-violence/for-survivors/
survivors-listserv/ for one). There are also user areas specifically for trans survivors
and loved ones in the online worlds FetLife (http://www.fetlife.com) and Second Life
(http://www.secondlife.com). These places may be more comfortable for some people,
since anonymity may be easier in these settings, and people may feel more comfortable
interacting through the avatars and profiles they create on these websites. If you find
someone you feel particularly drawn to in one of these online settings, do not forget that
you may talk with them privately by phone, Skype, FaceTime, chat areas…the options
expand daily.
You may also want to consider creating your own support group. One model is a Hachoka,
which is the Lakota word for sacred circle. In a Hachoka, a group of people meet on a
regular basis to support each other in healing (this could be a single-focus group or

57
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
focus on healing whatever participants bring to the circle). Various healing circles are
described in many of psychiatrist Lewis Mehl-Madrona’s books, which seek to suffuse
Native American healing knowledge into modern medicine. The last chapter of Narrative
Medicine: The Use of History and Story in the Healing Process (2007) contains accounts of
several healing circles.
FORGE also offers workshops entitled Writing to Heal: Soothing the Soul (through words,
images, and experiential activities). These dynamic, experiential and reflective writing-
based courses encourage and allow participants to transform feelings about past abuse,
assault or violence into empowered hope. Participants use writing, art, and movement
exercises to address topics that impact many survivors and loved ones. You can find
out more or sign up for the next course at http://forge-forward.org/anti-violence/for-
survivors/writing-to-heal/
Mainstream and LGBT services
Nearly every community has agencies and professionals who can help sexual
assault survivors.
Using the information below, you will likely find a resource that serves your geographic
area or that can connect you to providers and services that are close to you. Many of these
resources support people who are at various points in their healing and address different
needs—from crisis to ongoing therapeutic support.
Note that inclusion of a resource here does not mean it will be trans-welcoming or trans-
savvy. Trans and gender non-conforming survivors should use caution when approaching
an agency for services.
LGBT anti-violence programs (AVPs)
A growing number of communities have agencies that specifically focus on LGBTQI
victims of crime. The majority of these agencies are members of the National Coalition of
Anti-Violence Programs. (You can find a complete listing of all AVPs at www.ncavp.org.)
All should be able to help survivors of sexual assault. These are typically multi-faceted
agencies that can help with advocacy and referrals. Many offer direct services such as
support groups.
State sexual violence coalitions
Every state has a sexual violence coalition, although some are “dual” coalitions that
address domestic violence as well. These coalitions “provide direct support to member
rape crisis centers through funding, training and technical assistance, public awareness,
and public policy advocacy” (U.S. Office on Violence Against Women webpage, http://www.
ovw.usdoj.gov/ovwgrantprograms.htm). They usually do not provide direct services, but
they should be able to direct you to local programs that do. You can locate your state’s
coalition at www.justice.gov/ovw/local-resources. [Note: Not all coalitions or member
organizations have received training to work with transgender/gender non-conforming
clients, although all Coalitions are required to serve survivors of all genders.]
58
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
National sexual assault hotline
1-800-656-HOPE (4673). This is a 24/7 hotline run by the Rape,
Abuse, and Incest National Network (RAINN). It uses a computer
program to automatically connect each caller to the nearest rape crisis
center or community rape treatment center, where trained volunteers
will answer. RAINN says of this arrangement, “Each local center is the best
resource for victims in its community, not only for counseling but also for
information about community resources and emergency protocols. In addition,
because rape and sexual assault laws vary by state, local centers are in the best
position to advise survivors on the legal aspects of the crime.” You can read more about
the hotline at http://www.rainn.org/get-help/national-sexual-assault-hotline.
Rape crisis hotlines or community rape treatment centers
Your community may or may not have its own hotline and/or drop-in center for sexual
assault survivors. The exact services offered will also vary and may include:
Directing survivors to available local services
Sympathetic listening or even on-the-spot counseling
Accompaniment (for example, going with a survivor to the police or hospital)
Support groups and/or individual counseling
Advocacy for individual survivors and/or wholesale systems change.
As noted above, you will automatically be connected to the hotline or treatment center
nearest you by calling 1-800-656-HOPE (4673), or you can search online for your city and
rape crisis center.
Sexual assault treatment centers, sexual assault nurse examiners,
and hospitals
There are formal training programs for registered nurses to become Sexual Assault
Nurse Examiners (SANE). SANEs can conduct a medical forensic exam which can
include interviewing the victim, documenting injuries, and/or collecting physical and
photographic evidence of the assault that may be used in later court proceedings.
SANEs may work within a comprehensive sexual assault treatment center that is either
free-standing or, more likely, part of a hospital, or they may have other duties and
only occasionally be called upon as a SANE. They may also be part of a collaborative,
multidisciplinary group of professionals that helps develop a plan of care for the survivor
after they are discharged from the medical facility. Normally a victim will need to be
seen within 72 hours of an assault to capture evidence that might help in court. Note that
drinking or eating, bathing, changing clothes, and even using the toilet can all destroy
evidence. To find a local SANE, go to http://www.forensicnurses.org/search/custom.
asp?id=2100 [Note: Many survivors will access a Sexual Assault Nurse Examiner after
calling a Rape Crisis Center or other sexual assault agency. These agencies can link
a survivor with an advocate who will help support the survivor through the exam
and beyond.]
PHOTO BY KERRI CECIL

59
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Sexual assault response teams (SART) or coordinated community
response (CCR)
Both SARTs and CCRs are multidisciplinary, interagency teams that address sexual
assault. They typically include representatives of rape crisis centers, sexual assault nurse
examiners, advocacy programs, law enforcement agencies, prosecutors’ offices and other
professionals who serve sexual assault survivors. The Kansas Coalition Against Sexual
and Domestic Violence says, “Ultimately, a SART should coordinate to ensure that victims
of sexual assault receive appropriate services and referrals that promote the safety and
dignity of victims.” Usually the SART or CCR itself does not serve survivors; its member
programs are the service providers. [Note: You may be receiving services from providers
who are part of a SART or CCR. They will respect your confidentiality, but their multi-
disciplinary approach to supporting survivors will benefit you and other survivors by
helping all team members know what resources are available and/or helping create
services where there are gaps.]
Victim assistance programs
Many kinds of programs fall under this category. In this online http://ovc.ncjrs.gov/
findvictimservices/search.asp directory, you can search by state, type of crime, and what
kind of services you are seeking (such as an agency that can help you get a free phone that
will call 911). Other service options you can search for include: assistance in filing for
victim compensation claims, civil legal services, criminal justice support advocacy, crisis
counseling, crisis hotline counseling, emergency financial assistance, emergency legal
advocacy, follow-up contact, forensic examinations, fraud investigation, group therapy,
identity theft counseling, information and referral, personal advocacy, safety plans (for
domestic violence), shelter/safe house, supervised visitation, support groups, telephone
contacts, therapy, transportation, and victim rights legal services. You can also search by
type of agency (hospital, sexual assault center, area agency on aging, etc.). [Note that this
directory is not necessarily up-to-date.]
Victim compensation
A federal fund, administered by state agencies, will reimburse some victims for some
of the costs they incurred in a violent crime, including health care costs for treating
injuries, therapy, replacing personal items taken as evidence, and even lost hours/pay
from work after a crime. Most of the time, however, you can only access these funds if you
promptly report the crime, “cooperate” with law enforcement (which must agree with you
that a crime took place), and file your claim within a specified time period. A directory of
such programs is available at http://www.nacvcb.org/index.asp?sid=5 [Note: If you are
working with an advocate, many will assist you in filing for victim compensation.]
LGBT community centers
Some LGBT Community Centers house an LGBT anti-violence program (see that listing
above), while others provide other types of supports to people who have experienced
abuse. Many maintain referral lists for LGBT-friendly therapists and other professionals.
You can find the LGBT Community Center nearest you through http://www.lgbtcenters.
org/Centers/find-a-center.aspx
60
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Support groups
Support groups for sexual assault survivors might be sponsored by any number of agencies,
including therapists and survivors themselves, rape crisis centers, culturally-specific
agencies, and other organizations. Some of the directories above will indicate whether a
sexual assault agency offers support groups; otherwise, try calling your state sexual assault
coalition and/or rape crisis center first to see if they maintain a list of available support
groups. [Note: Sexual assault support groups are frequently segregated by sex or gender.]
Therapy
If you would like to find a qualified therapist to work with, read FORGE’s companion
document, “Let’s talk about it! A transgender survivor’s guide to accessing
therapy.” It will help you think through the type of therapist that might
be best for you and how to find one that is both trans-savvy and has
expertise in working with sexual assault survivors. If you would
like a referral to a trans-aware therapist in your area, FORGE
maintains a large database of providers online at our website,
www.forge-forward.org.
Restraining orders
Restraining orders are legal documents that direct the
individual(s) who assaulted you to keep away from you.
They are issued by a court and enforced by law enforcement
(police or sheriffs). Some restraining orders are temporary
and may only be valid for a few weeks, while others may be
for a much longer duration. Restraining orders can specify
how far away a person must be from you and make other
stipulations about the type of contact they can or cannot have
with you. They are by no means fool-proof, but they may help
you obtain a better law enforcement response if you are being
stalked or harassed by your abuser(s). The process of obtaining
an order varies by jurisdiction, so call a local police station, lawyer,
advocate, or other service agency for advice.
Law enforcement
Although many trans people have had difficult or even abusive relationships with law
enforcement, 911 and calling the police through non-emergency numbers is often useful
for your protection. Calling 911 can be lifesaving and critical if you have been injured,
recently assaulted, and/or if your perpetrator is actively harming you or threatening
you (or violating a restraining order). You will also need to report the crime to law
enforcement (usually within 5 days after an assault, although this deadline varies by
state) if you think you may ever want to press criminal charges against your abuser(s),
or if you might want to apply for victim compensation. Many urban police departments
have sensitive crimes units, which generally handle sexual assault-related calls. Beyond
these limited circumstances, many trans and gender non-conforming people have found
interacting with law enforcement not necessarily helpful or healing, although there are
many advocacy groups and individual officers who are working hard to change this. Some
larger cities have LGBT police liaisons or police task forces focused on LGBT issues.
PHOTO BY LEIGH HOUGHTALING
61
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trans support groups
Many communities have transgender support groups. These are usually organized and
facilitated by trans community members, activists, or by therapists. They are a good
source for connecting with other trans people and getting referrals to providers who have
knowledge about how to respectfully serve trans clients. If you are or become associated
with a transgender support group, consider bringing some of FORGE’s materials to the
attention of your support group facilitator(s). If you would like to get connected with a
trans support group near you, you can find a group by checking FORGE’s online support
group database at www.forge-forward.org.
12-step programs
Alcoholics Anonymous, Narcotics Anonymous, and related groups are all confidential,
peer-based, usually drop-in groups that provide support to people who have used
substances to cope with their past victimization or for other reasons. Many survivors use
alcohol, drugs, food, or other substances to help manage their symptoms following an
assault. This coping technique can be effective for a while, but often results in addiction
that needs the support of a 12-step program (or therapist). You can find a directory of
local numbers at http://anonpress.org/phone/. Note that some 12-step programs are
organized specifically for LGBT people.
Suicide hotlines and support
It is very common for both trans people and sexual assault survivors to have depression
and feel suicidal. If you are feeling suicidal, reach out for help. The Trans Lifeline U.S.
hotline number is 877-565-8860. The Samaritans hotline (located in Boston, MA) has been
specifically trained to receive calls from and support transgender individuals who are
feeling suicidal. You can reach them at 877-870-HOPE (4673). Another option is to call the
National Suicide Prevention Lifeline at 1-800-273-TALK (8255). It is available 24/7, and
will automatically route the caller to the suicide prevention hotline nearest them. Suicide
hotlines literally save lives, but not every staffer is trans-savvy. If the first person you talk
to is not helpful, try the Trevor Project Lifeline at 1-866-488-7386. This service is aimed at
LGBTQ youth ages 13-24, but their trained counselors will talk to anyone in a crisis.
Fenway Health’s Transgender Program has designed a brochure specifically for
transgender community members who might be feeling suicidal and for those who want
to help someone who is feeling the desire to end their life. You can access their brochure
at the bottom of this webpage: http://fenwayhealth.org/care/medical/transgender-health/
62
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
FORGE Services
FORGE has been serving the transgender and SOFFA
(Significant Others, Friends, Family, and Allies)
community since 1994. Although located in Milwaukee,
Wisconsin, the majority of our work is conducted
nationally (either virtually, or traveling to other
locations for conferences and trainings). In Wisconsin,
we have provided monthly peer support since 1994,
as well as other advocacy, resource development,
and emerging issue support for trans-related
issues. We have also had a national presence from
early on, organizing programming for many of the
American Boyz True Spirit Conferences, founding the
Transgender Aging Network in 1998 (which became a
program of FORGE in 2000), and hosting the Midwest’s
largest trans-masculine and SOFFA conference in 2007.
We formally began some initial work with
transgender survivors of domestic violence in 1999,
and became highly focused on transgender sexual
assault survivors (and the systems that serve them)
in 2004.
Our national services for transgender and SOFFA survivors of violence and the
professionals who serve them have evolved over time and with the availability of funding.
FORGE staff currently devotes 100% of their time to anti-violence issues.
For survivors
The free, core services we expect to offer indefinitely include:
Peer support: FORGE offers several peer support listservs and forums on social
media such as FaceBook. Many survivors find it empowering to know that they
can reach out and connect to other trans* survivors and loved ones at any
time of the day or night. For more information or to sign up, go to http://forge-
forward.org/anti-violence/for-survivors/survivors-listserv/
Referrals: FORGE can help transgender and SOFFA sexual assault survivors
find local resources, including (but not limited to): therapists who are
knowledgeable about transgender issues (including those that have expertise
in working with sexual assault survivors); local transgender/SOFFA support
groups; and LGBT anti-violence programs. Check the online databases on our
website, www.forge-forward.org, or request referrals by emailing AskFORGE@
FORGE-Forward.org or calling 414-559-2123.
Social media: FORGE maintains an active presence on the most popular social
media sites, currently including Facebook, Twitter, and Instagram. In some of
these venues we offer peer support (see above). We also use these to update
people on general trans news, policy developments, survivor-specific links and
www.forge-forward.org
tel: 414.559.2123
www.facebook.com/FORGE.trans
@FORGEforward
@forge_forward
63
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
issues, upcoming FORGE events and publications, and resources. You can find
us on Facebook at http://www.facebook.com/FORGE.trans. Our Twitter handle
is @FORGEforward (http://twitter.com/FORGEforward). On Instagram, we’re at
@forge_forward.
Publications: This Guide is part of a series that is available, along with other
self-help and information resources, at our website at www.FORGE-forward.org.
Transgender conference workshops and tables: FORGE frequently travels to
transgender conferences, often presenting on topics of interest to trans/SOFFA
sexual assault survivors. Our upcoming travel itinerary is available at http://
forge-forward.org/trainings-events/national-events/. Email us at AskFORGE@
FORGE-forward.org or call us at 414-559-2123 if you would like us to attend a
conference in your area.
FORGE is also currently offering the following free services to transgender, gender non-
conforming and SOFFA sexual assault survivors and loved ones:
Online Writing to Heal Workshops: Writing to Heal: Soothing the Soul (through
words, images, and experiential activities) workshops and courses are dynamic,
experiential and reflective writing-based groups that encourage and allow
participants to transform feelings about past abuse, assault or violence into
empowered hope. Participants use writing, art, and movement to address topics
that impact many survivors and loved ones. You can find out more or sign up for
the next course at http://forge-forward.org/anti-violence/for-survivors/writing-
to-heal/
The Espavo Project: “Espavo” means “Thank you for taking your power.” The
ESPAVO Project is a photographic and narrative project designed to increase
personal healing and empowerment for trans, gender non-binary, and gender
non-conforming individuals and loved ones who have experienced sexual
violence. Survivors and loved ones have the opportunity to have their photo
taken by a professional photographer, or can submit their own image. The image
is paired with a statement of survival and resilience, crafted by the survivor
(with support from FORGE staff, for those who would like it). Each participant
receives a frameable copy of their portrait, and all are invited to share their
image with others via online and/or traveling galleries. Portraits are taken at
transgender conferences and in cities where our associated photographers live
or travel. For more information, see http://forge-forward.org/anti-violence/for-
survivors/espavo-project/
64
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
For providers
FORGE also maintains an extensive array of free trainings, publications and technical
assistance for professionals who serve transgender and SOFFA individuals. We encourage
you to bring the following resources to the attention of service providers you work with:
Training webinars for victim service providers. FORGE produces and facilitates
a 90 minute training webinar every month on a topic related to better serving
transgender survivors of violence. These webinars are free to anyone who
wishes to sign up (although they are aimed at those who work with survivors
of domestic violence, sexual assault, dating violence, stalking, and hate
violence). More information and sign-up information can be found at http://
forge-forward.org/trainings-events/upcoming-webinars/ These webinars are
also recorded and are available free on-demand at http://forge-forward.org/
trainings-events/recorded-webinars/
Professional conference workshops & other in-person training. FORGE
frequently presents workshops on transgender survivors’ issues at professional
conferences across the country for those working with domestic violence, sexual
assault, dating violence, stalking, and hate violence survivors. In addition
to conferences, FORGE staff support agencies, Coalitions, and other victim
service providers through by-request, in-person trainings. Our upcoming travel
itinerary is available at http://forge-forward.org/trainings-events/national-
events/; email us at AskFORGE@FORGE-forward.org or call us at 414-559-2123
for more information or if you would like us to provide training in your area.
Publications for professionals. FORGE maintains a large library of free,
downloadable publications at our website, http://forge-forward.org/
publications-resources/anti-violence-publications/. These include a gender-
neutral pronoun conjugation chart, fact sheets on various topics related to
transgender and SOFFA people in general as well as focused on those who are
survivors of violence, policy reports, essays, and best practice guides.
Technical assistance and referrals. FORGE is currently funded to provide
individualized assistance to anyone who works with transgender survivors of
sexual assault, domestic violence, stalking, and dating violence. This assistance
can be in the form of a simple referral all the way through a several month long,
multifaceted consultation and training program. Professionals can contact us
via email at AskFORGE@FORGE-forward.org or by calling us at 414-559-2123.
To access any of these services or to learn more about what
FORGE can offer you, visit our website at forge-forward.org
or call us at 414.559.2123.

65
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
5
Self-Help
Techniques
and Concepts
“Survivors who have actively faced their healing are some of the most lively, spunky,
brave, funny, wonderful people I know. There’s something about diving into the deep-
est pain of life and coming out whole, that leads us to enjoy each precious moment of
life, because we know it’s all we’ve got. Instead of responding to the pain of the past,
survivors learn to appreciate the wild beauty of the present.”
37
There are hundreds of books, webpages, therapists, specialists, bloggers, and scholars
with many good (albeit sometimes contradictory) ideas about healing from trauma. Which
ones will work for you depends a lot on your beliefs about trauma and healing, as well as
your personal preferences.
“Healing” does not necessarily mean you will never have uncomfortable memories and
feelings related to your abuse. “Acceptance and Commitment Therapy,” for example,
teaches trauma survivors how to accept some of these uncomfortable pieces as part of life
and replace trying to stop or control these thoughts/feelings with value-based decision-
making. Instead or in addition, you can always learn new skills and patterns that will
improve your life experience. Indeed, one of the most exciting emerging scientific research
areas is around neuroplasticity: the discovery that the human brain is constantly
remaking itself throughout the lifespan, and that we can direct these changes in positive
directions. It is never too late to change your brain and the way it operates.
Sometimes one concept or idea can be life-changing. A new thought or experience can lead
to a dramatically different (and transformative) understanding. For example, some people
have found it very helpful to realize that shame—the feeling of being unworthy
of love and belonging, of being broken or not good enough—cannot survive when
37
Davis, Laura. (1991). Allies in healing: When the person you love was sexually abused as a child, p. 238.
PHOTO BY LEIGH HOUGHTALING
66
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
there is empathy.
38
Shame cannot exist when you are with a caring friend who listens
with empathy.
Similarly, some people find that journaling, talking with others, making art or using other
means of self-expression, reading self-help books or doing self-help workbooks can also
lead to “ah-ha” moments that can radically shift a survivor’s feelings about themselves or
what happened to them.
Other times, what is needed is more patience and persistence. This is the case when
you need to re-train your brain so that it discontinues going down negative or harmful
pathways (like the spiral that often starts with self-doubt or self-criticism) and instead
pursues more positive pathways. For instance, you may find it helpful to keep in your
pocket, backpack, or purse/wallet a short written list of things to put your mind to
when it keeps wandering down unwanted pathways. You may have a song that you can
start singing to yourself (or out loud!). Or perhaps you have a favorite poem or spiritual
passage that you want to mentally recite and reflect on. Maybe your brain can be more
actively creative, thinking about a project you want to start, or a piece of art you’d like to
create, or an assignment you are working on in class. If you do not have a project to focus
on, think about topics that help you feel connected to others: Who could you thank for a
recent (or long-past) kindness? What is a new way to show your partner or a friend how
much you care about them? What new experience might bring delight to you, either alone
or with someone else? What random act of kindness could you do for a stranger?
Still other times, we need to acquire new skills. This is especially the case for those of us
who need to learn more techniques for calming down raging emotions, ramping up our
emotions or thoughts, or shifting what we do or how we perceive our world or our selves.
The breathing exercises in this section are examples of emotional regulation tools. Most
of us also need better skills for negotiating and resolving conflict with others; we have
included some essays and exercises for those, too.
Healing is hard work.
Healing is often only possible if some basic needs have been met:
Are you eating well? (enough food / not too much, nutritious food, often enough)
Sleeping enough? (or not too much)
Exercising? (or doing something else that moves your body in healthful ways)
If you are on medication, are you taking it regularly and as prescribed?
Have you built into your life things that sustain and rejuvenate you?
38
A concept proposed by author and researcher Brene Brown. For just one example of Brown’s work, listen to her TED talk
on shame: http://www.ted.com/talks/brene_brown_listening_to_shame.html
What we know with certainty is that
change is possible. Healing is possible.
PHOTO BY MIA NAKANO

67
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Living with the aftermath of trauma can be exhausting and debilitating; having regular
experiences of the good things life has to offer can be important to overall health,
wellness, and healing. Some people find that having a reminder list taped to their
refrigerator or tucked into their wallet can serve as a useful reminder of what brings
enjoyment. These types of lists or other forms of reminders can help encourage us to
bring things that sustain us and rejuvenate us into our lives on a more regular basis.
Just paying attention to the basics of self-care can be tremendously helpful.
What follows are a selection of exercises and essays that provide some other ideas for
addressing common post-trauma issues. Much, much more is available; these are just
samples and examples of the wide range of self-help techniques that exist. You can
find many more by reading one or more of the books we have included in the annotated
bibliography (see page 106).
68
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
6
Techniques
for Coping
with Strong
Emotions
Everyone experiences strong surges of emotions every once in a while.
Trauma survivors frequently have emotional spikes and valleys that are sometimes
difficult to resolve without some form of intervention. When we feel strong emotions,
our thinking brain often is inaccessible, so it’s useful to have some pre-planned, pre-
practiced skills readily available to you that will help you get out of intense emotional
states more quickly.
In general, most people who are experiencing strong emotions will need to take actions
that fall into one of these three categories:
1. Ramping up: getting out of stuck emotions, getting moving
2. Slowing down: literally slowing down breathing, movement and thoughts
3. Modulating: shifting emotions from their current state where the primal survival
brain is dominant to a state where the thinking brain is back online.
Although there is no magic answer for everyone, some of the techniques presented in this
section, as well as the exercises in the longer-term healing techniques section, may be
useful to help regulate your immediate and long-term strong emotions.
Getting out of the basement
The amygdala in our brains takes over when we are in highly emotional states, or are
triggered by a traumatic memory or stimulus. The amygdala is located in the lower
portion of the brain. Some researchers talk about “being in the basement” when our
emotions (amygdala) is in control. It is important to:
PHOTO BY LEIGH HOUGHTALING

69
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
1. Recognize you are in the basement
2. Get out of the basement
3. Hold off on any decision-making until you are out of the basement
The mere concept of “being in the basement” may be useful in and of itself as a way to put
a label on what you are feeling and that your emotions are in control.
[Hint: Some of the techniques below will help you get out of the basement.]
Breathing
If at all possible, be aware of your breathing. See if you can determine if your breathing is
fast, slow, shallow, deep, even or sporadic (for example, if you notice you are holding your
breath). Even if you cannot focus on determining how you are breathing, you might benefit
from focusing on trying to breathe in a more steady way. The goal isn’t necessarily to
breathe deeply, but rather to return to a more natural state of breathing for you. The trick
is concentrating on your breath and trying to smooth it out to a more even pace.
90 seconds
Our brains and brain chemistry are remarkably efficient—and quick. Neurotransmitters
are chemicals in the brain released in response to a stimulus. [Most of us are familiar
with neurotransmitters like adrenaline.] They are how neurons—nerve cells in the brain—
communicate with each other. For people living with trauma, the powerful impact of
neurotransmitters can render us paralyzed or cause extreme agitation or distress.
Sometimes the neurotransmitters stay in the
synapse and are not absorbed by the receiving
neuron. When there are too many neurotrans-
mitters in the synapse the result is often a strong
physical and emotional response. [Think about
when you feel really anxious or jittery; this can be
the result of an abundance of neurotransmitters
that haven’t yet been absorbed.]
Neurotransmitters are released from one neuron
into the synapse (gap). The adjacent neuron has a
receptor that will absorb the neurotransmitters that
are in the synapse.
SYNAPSE
neurotransmitter
receptors
SYNAPSE
neurotransmitter
receptors
70
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
In general, neurotransmitters will clear the synapse in less than 90 seconds if the
neuron is not re-stimulated. What that means is that if we can stop the neurons/
neurotransmitters from re-firing, the intense emotions we are feeling will STOP!
When you are not in a state where your neurotransmitters are unbalanced, think about
all of the things you can easily do for 90 seconds that will keep your mind busy, so the
unwanted neurotransmitters will not continue to stay in the synapse.
Some sample activities might include making a cup of tea or coffee (especially if it
involves grinding, heating, pouring, and other multi-step brewing methods), walking
in place (taking 90 steps), drawing a small sketch, or listening to one piece of music.
Many people have found it useful to set up a play list on their phone or computer with
90-second songs.
Getting moving / getting physical
Many people find they feel paralyzed or immobile when they are experiencing strong
emotions. The process of literally starting to physically move will often quickly shift
these emotions.
The type of physical movement can range from very small to very large. Nearly everyone,
including individuals living with disabilities and people with limited energy or flexibility,
can engage in some form of movement.
Some examples of “small” movement include: tapping your leg/arm/desk with your
finger, crossing or uncrossing your legs, standing up, getting out and chewing a new piece
of gum, scrolling through photos on your phone, stretching your arms above your head,
taking off your shoes or tightening the laces, or making a fist and letting it go.
Some examples of “medium” movement include: moving to a different room or place,
getting a drink of water, going across the room to open a window, moving to a different chair,
deciding to stand up for a few minutes (perhaps to look out a window or stare at a bookshelf),
tossing a ball for your dog, taking a shower, changing your clothes, or making a meal.
Some examples of “large” movement could include: taking a walk around the block (or
farther), going for a bike ride, getting in the car to drive to a park, going to the grocery
store, running any other kind of errand, engaging in any kind of house cleaning (vacuuming,
picking up clutter), doing yard work (gardening, mowing), walking your dog, etc.
Using your voice
Although it may sound silly to some, using your voice can be a very powerful way to stop
traumatic memories or symptoms our body is experiencing related to trauma. Frequently,
during sexual abuse or assaults, we were told to be silent, or others afterward told us to
not talk about what happen to us. If you are stuck in an intense emotion, try using your
voice to break the pattern.
If you are alone or in a space where it is safe to make noise, allow your body to make the
noises that may want to come out—from a soft trembling breath, to saying out loud “yes”
or “no” or “stop,” to talking to a pet or object in your environment, to calling a friend to
talk to, to screaming into a pillow.
71
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Cross brain actions
There are many actions we can take that use both sides of our brain.
When we do things that involve multiple parts of our brain—
especially when it crosses the middle—we can start to process
memories and emotions more effectively, and begin to think better.
If you remember the childhood challenge of patting your head
and simultaneously rubbing your stomach in circles, this is just
one of thousands of examples of using both sides of your brain.
One easy suggestion for using both sides of your brain is to
position yourself in a “butterfly hug.” As the photo shows, it’s quite
simply hugging yourself, crossing your arms across your chest.
In addition to the hug, you can gently alternate squeezing each
arm with your hands, or tap each arm/shoulder - going back and
forth between sides of your body. The tapping technique can be
done without using a hug, too. Placing your hands on your thighs
and tapping one thigh then the other will be just as effective.
Checklists
Checklists can be very useful to help you remember what to do if you feel paralyzed,
anxious, or cannot think of how to shift your emotional state to one that is more
tolerable. One of the most powerful checklists is described in more detail on page 72:
Standard Operating Procedures. We encourage you to review and complete this exercise
(or modify it to meet your needs).
If you prefer a more simple checklist, you may want to jot down some of the 90 second
activities mentioned above, or a list of ways to start moving your body, or a reminder of
what you have agreed with yourself to do when you get in an intensely emotional state.
We all need reminders, but we especially do when we are “in the basement” and our
emotions have taken control.
Use technology
The constantly growing types and accessibility of technology is improving many peoples’
lives. You can store your checklists in your phone or on your computer. You can set up a
play list of 90-second songs. You can find one of dozens of apps that help you breathe in a
more consistent and conscious way.
Your phone, tablet or computer can act as a timer (for the 90 seconds) or to help
you gauge how long you have been “in the basement.” You might want to highlight a
prioritized list of people to call when you are in crisis.
There are unlimited ways you can use technology to help you shift your emotions and
return to a place that feels more emotionally tolerable and comfortable.
PHOTO BY JOHN HALCYON STYN

72
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Emergency Standard
Operating Procedures (SOP)
When we feel very strong emotions, our brain literally changes. Various chemicals,
depending on the emotion, are released by the brain, and these chemicals can change the
way the brain works. Particularly likely to be affected is the neocortex, the “thinking” part
of the brain. Many of us seem to developmentally devolve when we are very emotional,
and that is, in many ways, true: the thinking part of our brain loses dominance, and our
more primal emotions take control—often in ways that are destructive to self or others.
This is one of the reasons why it is such a good idea to think through your “Standard
Operating Procedures” (SOP) for emergencies—i.e., when your emotions are getting (or
threatening to get) the better of you. Preparing an SOP is particularly important for those
who are prone to feeling suicidal. We need to be able to have a pre-prepared list where we
can easily find it of what we have committed to doing when we feel out of control or self-
destructive.
FORGE’s SOP worksheet (see page 74) starts with
a checklist:
Sleep (have I had the right amount of sleep in the past 24 hours?)
Eat (have I eaten in the past 8 hours?)
Medication (did I take my prescription and over-the-counter medications today?)
Human contact (have I had human contact with anyone in the past 24 hours?)
Shower (have I showered/bathed in the last 24 hours?)
Relax (have I had any time off, time to do something fun or relaxing, in the past
24 hours?)
These questions are meant to help you determine, when you are feeling emotionally
overwhelmed or in crisis, if you have overlooked any of your basic bodily maintenance
needs. Sometimes we get cranky because we have forgotten to eat or have not had a break
from concentrating in way too long. The checklist helps us make sure the basics have been
covered. If not, that might be the place to start!
The second part of the SOP is the things you have found to be helpful when you feel
intense, strong, or overwhelming feelings of sadness, hopelessness, severe depression,
and/or overwhelm. The worksheet asks you to write down:
People you can call when you are in crisis (a partner, best friend, family
member, therapist, spiritual leader, co-worker, etc.)
Things that bring you pleasure and/or calmness from the following categories:
Things you can see (flowers, TV, a favorite object, funny animal videos...)
Things you can hear (music, silence, kids, animals, traffic, leaves rustling...)
Things you can smell (coffee, grass, shampoo, incense, your favorite
cookies baking...)

73
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Things you can taste (chocolate, fruit, tea...)
Things you can touch (your favorite stuffed animal, soft sheets, firm chair,
human caress, pet’s fur, sexual stimulation, shower...)
Things you can do or ways you can move (write, walk, drive, play music, make
arrangements to meet with a friend, make plans for later in the day, start on a
project or puzzle...)
Other (an herbal calming agent like Rescue Remedy, go to the Emergency Room,
set up time with a therapist, read, take a bath, go to bed....)
We also include a category for people or things to avoid when you are overwhelmed or
in crisis because past experience has taught you these things or people tend to make
you feel worse or threaten your safety when you are already having emotional difficulty.
Examples might be staying away from public places, avoiding your ex-partner, not
driving, not drinking, etc.
Once you fill out your SOP worksheet, make copies. Ideally, if you feel comfortable doing
so, give a copy to those on your “people to call” list so that they can help remind you of
good options when you may not be able to remember them on your own. Also place copies
where you can readily see or find them: in your wallet, on the bathroom mirror, at your
desk, on your phone.
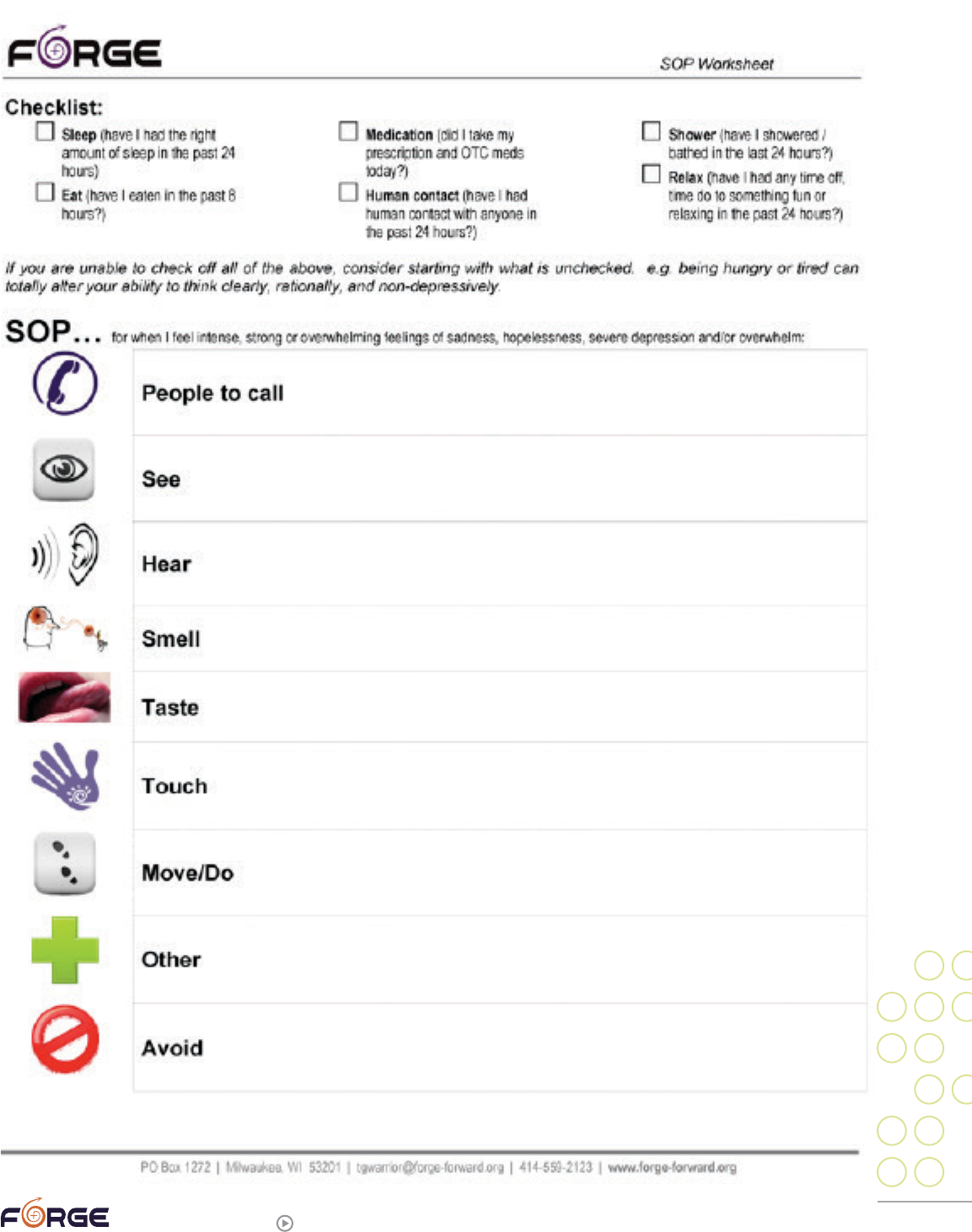
74
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
[Insert SOP Worksheet here]
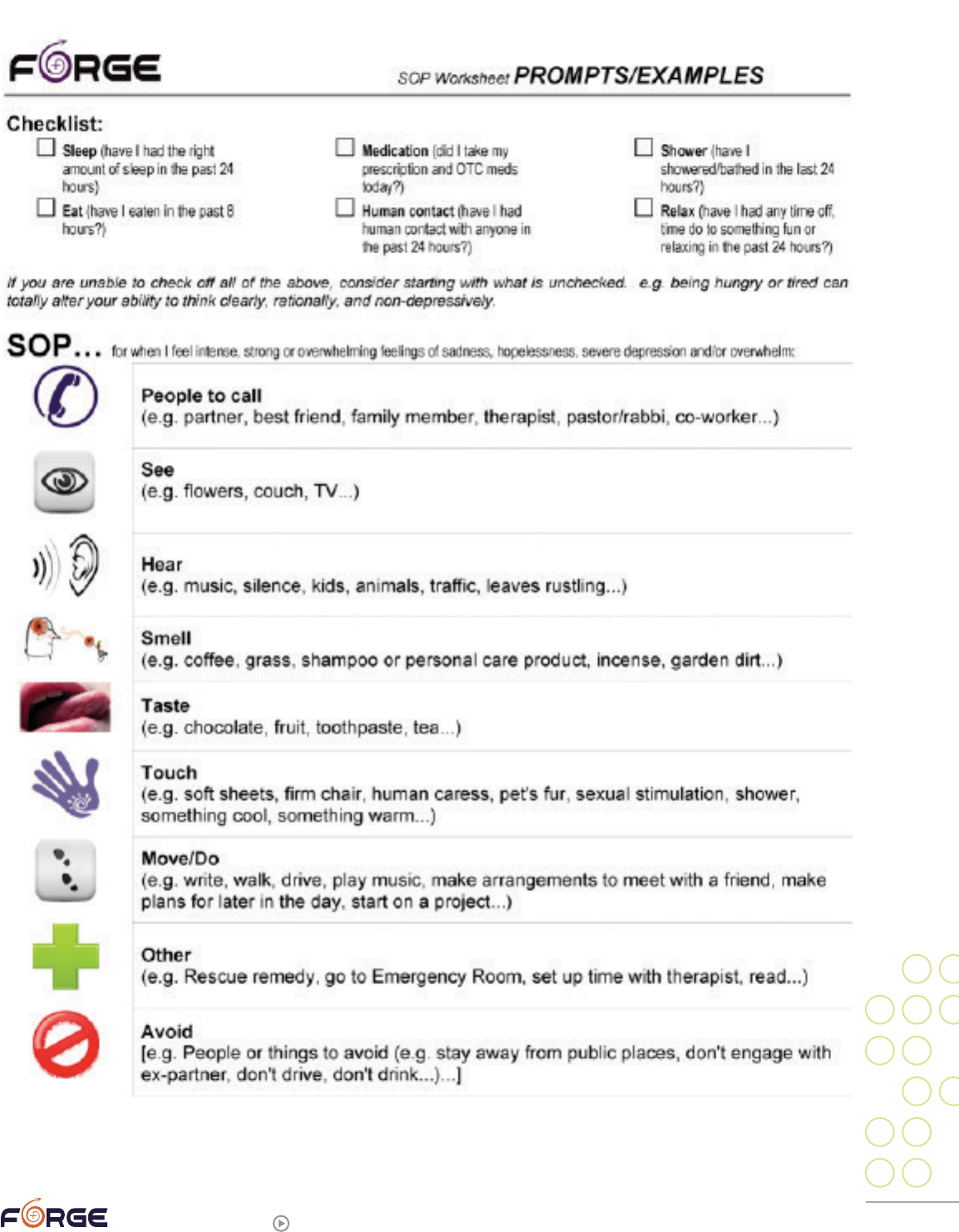
75
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
76
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
7
Techniques,
Exercises
and Concepts
for Healing
Container exercise
If you have overwhelming emotions or physical sensations that are too much to process
all at once, try “containing” them.
This exercise is adapted from Robin Shapiro’s book The Trauma Treatment Handbook:
Protocols Across the Spectrum.
39
1. Imagine a container that is big enough and strong enough to hold all your feelings
and distressing sensations. It could be anything from boxes to bottles to small-town
water tanks or huge oil tankers.
2. Pour your distressing emotions into that container. Make sure you get them all in.
3. When they are all in, find a way to lock that container up so that nothing leaks out.
4. Now install a tap or special airlock on your container so that when the time is right,
preferably with a therapist or other support person, you can bring the sensations and
emotions out a little at a time, for clearing.
5. If anything new triggers you into big, distressing feelings, or a flashback, you can send
all those feelings into the container, as well.
39
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the spectrum, p. 51.
PHOTO BY LEIGH HOUGHTALING

77
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Coping with anniversary dates
Many trauma survivors have emotional reactions on or around the anniversary dates of
their assault(s) or trauma(s).
40
Some people even have emotional upsets on anniversary
dates when they are not consciously aware that it is an anniversary date, as though the
body is keeping score without the mind’s involvement.
If you know you have difficulty around trauma anniversary dates, you have the
opportunity to plan how you want to cope. There are many options, including:
Distraction
For most people, it is nearly impossible to not think about something after it has come
into your awareness. You can, however, busy your mind with something else to think
about. Distractions need to be very mentally involving. If you get carried away watching
movies and do not think about other things while you are involved in the story, that is one
option. Another option is getting involved in a mentally engaging task (such as building a
model ship, helping a child with homework) or a physically taxing task (such as building
a garden wall or vigorously cleaning the garage). It is important to not choose a task that
is repetitive, since these tasks can easily allow your mind to wander other places once it
has established the routine.
Create new memories
One couple meticulously planned a long, romantic, and involved date designed to
create new memories on the anniversary of one of their sexual assaults. You can create
compelling memories by visiting a museum or other place you have long wanted to see,
by indulging in something adrenaline-producing like going to a major amusement park or
adventure movie, or holding a game night with friends.
Grieve
You may choose to mark an anniversary date by being fully present with it. Maybe you
will want to journal about what happened, what your losses were, and what you have
learned from it. It might appeal to you to create a ritual to honor your survival. Perhaps
you could write a letter you will never send to your perpetrator(s). Some people tap into
below-the-surface feelings by watching a sad movie or listening to melancholy music.
Remember that tears can be very cathartic.
Help others
Many, many people feel most whole and human when they are helping someone else.
You may find that you prefer to help people you know or volunteer your time with others
you may not already have a relationship with. Offering to drive your neighbor to the
store, helping a family member with a household repair project, calling an ill friend
and offering to cook them a meal or clean their bathroom can be highly rewarding. Just
the process of thinking about how you can help someone can be useful! If you prefer to
volunteer, you can help out at a soup kitchen or see if your neighborhood nursing home
will let you come in and entertain the residents or simply sit with a few residents and
40
If you were regularly abused, you likely cannot point to any specific dates.
78
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
massage lotion into their hands (nursing home residents typically suffer greatly from
lack of caring touch). Your geographic area may have an online volunteer bank that
lists volunteer opportunities that may include one-time efforts. You could take a local
homeless person to lunch.
Self-care day
Trauma survivors frequently have trouble taking time to care for themselves. An
anniversary date is a good time to plan a period of time (or even a whole day if you are
able) for self-care. You might find that it feels good to cook your favorite meals, or take
yourself out to a restaurant. Watch your favorite movie, take a long hot bath, indulge in a
re-read of your favorite book. If touch is something that feels good to you, see if you can
arrange for a massage (either by a friend, partner, or professional who feels safe). Pretend
that you are charged with making a “special day” for your favorite person—even if your
favorite person is not yourself—and plan as indulgent of a day as your creativity will
allow. (Remember, there are a lot of ways to engage in self-care that are free.)
To help plan how you want to spend an anniversary date, consider filling out this
worksheet to brainstorm some ideas for each category.
Distraction Ideas
Create new memories ideas
Grieving ideas
79
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Serving others ideas
Self-care day ideas
What type of day feels most compelling to you? Do you want to combine ideas from two or
more boxes?
Write down what you intend to do.
On anniversary date ______________________________, I am going to:
1.
2.
3.
4.
5.

80
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Coping with triggers
Many sexual assault survivors get “triggered,” meaning they have some sort of (usually
unpleasant) response to something that consciously or unconsciously reminds them of
the trauma they survived.
Triggers: dialogues
Staci Haines, in her book Healing Sex: A Mind-Body Approach to Healing Sexual Trauma,
goes beyond identifying and strategizing about triggers, instead suggesting that it is
possible to have a productive dialogue with them. She calls the exercise, “Feeding
the Triggers: A Tool for Healing Triggers.”
41
(We have neutralized some of her
gendered language.)
This is a very powerful and effective exercise for healing and attending to triggers.
Although it might seem daunting at first, once you get the hang of it, it is really quite
simple. This exercise can be done alone or with a friend, partner, or therapist whose role
will be to facilitate, witness, and be present for the experience.
1. Arrange two pillows or chairs so that they are facing each other. Sit on one. Close your
eyes and get in touch with the trigger you want to work with. Where is it in your body?
How does it feel? (e.g., I feel a constriction in my chest and back, or My stomach gets
tight and I feel terrified.) Fully feel the trigger and be clear about where in your body
you feel it.
2. Next, let the trigger float out of you onto the pillow across from you, taking some form.
It could look like a monster, a small child, a color or shape. Just let it take shape. An
image or sense will appear. Now describe the creature/shape sitting across from you as
specifically as you can. What color is it? How large? Does it have a face, a look in its eye?
3. Once you have a clear sense of the representation of the trigger, ask it out loud, “What
do you need?”
4. Switch seats, so that you now occupy the creature or shape’s seat. Take a moment
to imagine yourself becoming the creature or shape. What does it feel like to be this
creature/shape? Now respond as the creature/shape. Tell the “you” on the other pillow/
chair what it is you need. Speak in “I” statements: “I need,” “I want.”
5. If the trigger wants you, for example, to die, to quit ignoring it, or to eat all the food
in the house, ask it (or have your partner ask it) what purpose that would serve. “If I
died, quit ignoring you, or ate all that food, how would that make you feel?” You want
to discover the need beneath the need. Continue to ask these questions until you get
to the base of the trigger’s needs. Most often, the needs at this point will be for love,
safety, acceptance, and forgiveness.
6. Once you have discovered the needs of the trigger you are working with, switch
seats and become yourself again. Then, as if by magic, evoke an infinite quantity of
love, safety, acceptance, and forgiveness, or whatever it is the trigger needs. Feed the
trigger sitting on the other pillow/chair what it needs until it is fully and completely
satisfied. If you find it difficult to imagine yourself feeding the creature to complete
41
Haines, Staci. (2007). Healing sex: A mind-body approach to healing sexual trauma, second edition, pp. 168-169.
81
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
satisfaction, then just imagine that it has been fully fed. Know that all triggers can
be fed to their complete satisfaction. Different triggers take in this sustenance in
different ways; some eat it, others breathe it in or absorb it into their bodies. Still
others take it in best as sounds or colors. Be creative and use what works for your
trigger creature.
7. Once the trigger is completely satisfied, or you have imagined that it is, sit quietly. Sit
in the emptiness or wholeness. Don’t fill it with the next problem, or the next trigger;
just sit quietly for a few moments. At this point, many triggers will transform in
shape and size. Just notice whatever yours does and be with that. When you are ready,
complete the exercise by thanking the creature and yourself.
8. Repeat this exercise with the same or different triggers as needed. Because of the
depth of childhood sexual abuse, many triggers will need this feeding more than once.
Repeated over time, this approach to healing triggers can be amazingly successful.
With practice you can also begin to do this exercise in your own mind. It is a handy
tool to carry with you.
Triggers: coping via a “series of tasks”
Triggers can be hard to deal with, but John Briere and Catherine Scott, in their book
for therapists, Principles of Trauma Therapy: A Guide to Symptoms, Evaluation, and
Treatment (2006), say that identifying and coping with triggers can be “taught as a series
of tasks.”
42
We have lightly revised their three steps to make them more user-friendly.
1. Identify a given thought, feeling, or intrusive sensation as posttraumatic.
This is relatively easy in some cases. For example, it may be easy to identify the
sound of a door slamming as the trigger that reminds you of a loud noise you heard
during your traumatic event. In this case, the feeling of being startled or fearful are
the feelings associated with the trigger of the loud noise. In other cases, however,
the thought, feeling or intrusive sensation may be more difficult to identify as
posttraumatic—for examples, diffuse feelings of fear or anger, or intrusive feelings of
helplessness that emerge within conversation. Typical questions to ask include:
a. Does this thought/feeling/sensation ‘make sense’ in terms of what is happening
around me right now?
b. Are these thoughts or feelings too intense, based on the current context?
c. Does this thought or feeling carry with it memories of a past trauma?
d. Am I experiencing any unexpected alteration in awareness (dissociation,
depersonalization, etc.) as these thoughts/feelings/sensations occur?
e. Is this a situation in which I have been triggered before?
2. Find the trigger.
Sometimes the trigger might be obvious (as in the door slamming in the above
example). However, usually finding the trigger involves a certain level of detective
work. Objectively evaluate the environment to see what might be “trauma
42
Briere, John & Scott, Catherine. (2006). Principles of trauma therapy: A guide to symptoms, evaluation, and treatment,
pp. 104-105.

82
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
reminiscent,” and thus potentially a trigger. Types of triggers you might learn to
recognize, depending on your trauma history, include:
a. Interpersonal conflict
b. Sexual situations or stimuli
c. Interactions with an authority figure
d. People with physical or psychological characteristics that are in some way similar
to your past perpetrator(s)
e. Boundary violations
f. Sirens, helicopters, gunshots, or other loud noises
g. The sound of crying
h. Smells
3. Construct an adaptive strategy.
The goal here is to “improve the moment” by reducing the likelihood of your emotions
escalating. Some possibilities include:
a. Intentional avoidance or ‘time outs’ (for example, leaving a party when others
become intoxicated; intentionally minimizing arguments with authority figures;
learning how to discourage unwanted flirtatious behavior from others)
b. Reanalyze “until a greater understanding changes one’s perception and thus
terminates the trigger” (for example, carefully examining the behavior of an
individual who is triggering posttraumatic fear, and eventually becoming more
aware of the fact that he or she is not acting in a threatening manner; or coming to
understand that a given individual’s seemingly dismissive style does not indicate
a desire to reject or ignore as much as it does interpersonal awkwardness)
c. Increasing support systems (for example, bringing a friend to a social
gathering where one might feel threatened, or calling a friend to ‘debrief’
an upsetting situation)
d. Positive self-talk (for example, working out beforehand what to say to oneself
when triggered, such as ‘I am safe,’ ‘I don’t have to do anything I don’t want to do,’
or ‘This is just my past talking, this isn’t really what I think it is’)
e. Breathing / relaxation exercises (for example, use a phone app to help remind you
to breathe, or excuse yourself to go to the bathroom if in a public setting so you
can have a private moment to focus on your breath)
f. Strategic distraction, such as starting a conversation with a safe person, reading a
book, or going for a walk, as a way to pull attention away from escalating internal
responses such as panic, flashbacks, or “catastrophic cognitions” (i.e., thoughts
that a catastrophe is seconds away)
[Note: Sometimes when triggers occur, it is difficult—or sometimes nearly impossible—
to engage our thinking brain. This technique may be out of reach for some people or in
some situations. Different techniques will work at different times, in different situations,
and for different people.]
83
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Making meaning
“Freedom is what you do with what’s been done to you.”
43
“If your goal is only a relief from symptoms, you’re not aiming high enough.”
44
Nearly every trauma survivor asks themselves, “Why did this happen to me?” This could
be a very helpful question except that it is nearly always focused in the wrong direction:
the past.
Human brains are story-tellers. We automatically try to link things into a cause-and-
effect story. Someone cuts us off on the highway, and without consciously thinking
about it, our brain gives us a reason they did so: they are an idiot, they are distracted by
their phone, we were in their blind spot. When we experience a trauma, our brains seek
the cause. What did we do wrong that led to this horrible event? Note that it is almost
impossible to ask, “What did I do right that led to this horrible event?” Brains do not work
that way. If something bad happens, something bad must have caused it.
Unfortunately, the answer to “something bad must have caused it” almost never focuses
on the perpetrator. Instead, we focus on what we did wrong. We should have known better,
we should have seen that person was untrustworthy, our gender non-conformity caused
it. Not only does this make us responsible for something that the perpetrator did, but
it undermines our whole sense of self. If we were the cause of the horrible things that
happened, we cannot be trusted in the future, either. This is part of the dynamic that keeps
past traumas present in our day-to-day life and allows them to contaminate our future.
A far better alternative is to “make meaning” out of the trauma by projecting into the future.
Pretend you are 20 years in the future. Looking back, ask yourself what good came out of
the trauma? Did it lead you into a new career or volunteer work helping others? Did you
meet the love of your life at a trauma survivors’ support group? Did it make you appreciate
the moment-by-moment little things in life in a way you never did before the trauma?
Obviously, some of the good that will come out of your trauma is unknowable until you
have lived it; it will be recognizable only in retrospect. The magic in taking the future
perspective on “making meaning out of the trauma” lies in choosing to make something
positive happen. Practice trying to imagine what good you can make happen as a result of
being a sexual assault survivor. Write some possibilities in the box below.
43
Jean-Paul Sartre, quoted in Cloitre, Marylene, Cohen, Lisa R., & Koenen, Karestan C. (2006). Treating survivors of child-
hood abuse: Psychotherapy for the interrupted life, p. 311.
44
Cori, Jasmin Lee. (2008). Healing from trauma: A survivor’s guide to understanding your symptoms and reclaiming your life,
p. 107.
Additional readings on coping with triggers
Boon, Suzette, Kathy Stelle, & Onno van der hart (2011). Coping with trauma-related
dissociation: Skills training for patients and therapists. New York, New York: W.W.
Norton & Company, Inc.
See especially pages 165-200, “Coping with Trauma-Related Triggers and Memories.”
84
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
To hopefully inspire you, let us offer you this: This Guide was conceived in just that way.
Mindfulness and meditation
“Building the human brain is vastly complex. Rebuilding it is a difficult and
fascinating challenge.”
45
For many trauma survivors, the mind is a scary place. That is where those horrible
memories reside, memories that can sneak up and tackle us when we least expect them.
That is where the voices are that tell us we are not worthy, we are damaged, we are
in danger. For some of us, that is where the overwhelming emotions of terror, anger,
helplessness, hopelessness, and all the rest come from. Even those of us who live in our
minds, cut off from our bodies and their feelings, may at times feel at the mercy of what
our brains produce.
As a result, many trauma survivors avoid “meditation” and “mindfulness” like the plague:
Why would you want to cut out all activities and distractions and focus solely on your
breath or what is going through your mind? What a disaster that would be!
In truth, however, meditation and mindfulness—two very related practices—are
extremely potent healing tools. J.L. Cori, author of Healing From Trauma: A Survivor’s
Guide to Understanding Your Symptoms and Reclaiming Your Life, says: “Training the
mind has some real benefits to trauma survivors who need to be able to drop a negative
impulse or train of thought, move away from a mesmerizing image, or back out of a
difficult emotion.”
46
Meditation is one of the best ways to train the mind. Meditation usually involves sitting
or lying comfortably in silence or with calming music and concentrating on the breath
going in and out of your body or on a “mantra” or saying. Although the goal is to keep your
mind on your breath or your mantra, the real point is the endless practice of noticing
your mind has wandered off and bringing it back to its task. Like the “reps” one does with
45
Cozolino, Louis. (2010). The neuroscience of psychotherapy: Healing the social brain (Second edition), p. 9.
46
Cori, Jasmin Lee. (2008). Healing from trauma: A survivor’s guide to understanding your symptoms and reclaiming your life,
p. 202.
Additional readings on making meaning
Maisel, Eric (2007). The Van Gogh blues: The creative person’s path through
depression. New World Library.
Eric Maisel specializes in coaching artists and writers, but the point of his book is that the
way to get out of depression or other mental ruts is to create meaning. This book gives lots
of advice on that.
85
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
weights, the constant repetition of noticing your mind has wandered and bringing its focus
back where you want it builds a sort of mental muscle. P. Ekman, in Emotions Revealed:
Recognizing Faces and Feelings to Improve Communication and Emotional Life, says that
focusing on “an automatic process that requires no conscious monitoring [like breathing]
creates the capacity to be attentive to other automatic processes… benefiting emotional
behavior awareness and eventually, in some people, impulse awareness.”
47
There is no sharp line between meditation and mindfulness; the following exercise from
Bass and Davis’s seminal book, The Courage to Heal (2008), combines them both. In this
meditation, you become “mindful” of what is going on in your body.
“If any particular sensations become strong and call your attention, allow those
sensations, instead of the breath, to become the primary object of mindfulness. You
might feel heat or chills, tingling, aching, twisting, stabbing, vibrating. With a soft,
open awareness just feel the sensations as they are. Are they pleasant or unpleasant?
As you fully attend to them, do they become more intense or dissipate? Notice how
they change. When the sensations are no longer a strong experience, return to the
mindfulness of breathing. Or if the sensations are so unpleasant that you are unable
to regard them with any balance or equanimity, feel free to rest your attention again
in the breath. In a similar way, you can bring mindfulness to strong emotions—fear,
sadness, happiness, excitement, grief...What does this emotion feel like as sensations
in the body? Where do you feel it most strongly? Is it static or moving? How big is it?
Are your thoughts agitated and vivid? Are they repetitive and dull? Does your mind
feel contracted or open? As you pay attention, notice how the emotion changes. Does
it becomes more intense or weaken? Does it change into a different state? Anger to
grief? Happiness to peace?”
48
Notice that the directions above assume that your emotions and the feelings in your
body will change as you pay attention to them. This is another aspect of the muscle-
building purpose of meditation: it helps you really learn that whatever you are feeling,
it will change. For those of us whose depression or rage or some other strong emotion
sometimes feels overwhelming and endless, truly internalizing that our feelings always
change can be literally life-saving.
Focusing on your body as a meditation is also designed to help those of us who have
survived in part by cutting off or ignoring our bodies. Among the problems with this survival
strategy is that it can also limit how much enjoyment we can get from our bodies, and it
certainly limits the amount of information we have about ourselves. Learning to feel and
deal with your emotions is an important part of healing, and learning how various parts of
your body feel in conjunction with certain emotions is a great way to start. Another benefit of
learning the unique ways in which your body reacts to emotions is that labeling a feeling—
“when my stomach feels all knotted up like this, I’m angry”—engages different parts of the
brain. John Arden, in Rewire Your Brain: Think Your Way to a Better Life, says, “The process
of labeling emotional states with words reduces anxiety and negative emotions.”
49
Moving further along the spectrum, pure mindfulness allows you to always be able to be an
“observer” of your mind—one step removed from whatever ideas and emotions are floating
47
Ekman, Paul. (2007). Emotions revealed: Recognizing faces and feelings to improve communication and emotional life,
p. 239, emphases in the original.
48
Bass, Ellen & Davis, Laura. (2008). The courage to heal: A guide for women survivors of child sexual abuse (4th edition), p. 181.
49
Arden, John B. (2010). Rewire your brain: Think your way to a better life, p. 202.
86
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
through—even in the midst of daily life. Some therapists suggest you pretend you are in the
audience of a theater, watching a movie of your life. You can see the emotions and activities,
but you are not in them. This can be particularly helpful when dealing with trauma
memories. You can even be in a theater watching yourself in a theater watching yourself
on the screen; move back as many times as necessary to recognize that there can be a “you”
above and beyond the one who is experiencing things. Mindfulness therapy guru Dan Siegal
suggests placing yourself on the outside hub of your wheel of life, watching the spokes flow
by. This mindfulness perspective helps you maintain perspective by separating you from
your thoughts/memories/emotions, so that you can recognize that as compelling as those
are, they are not all of who you are, and they will change. This is critically important for
those of us who are prone to suicidal helplessness and hopelessness; if we can remember
in the moment of crisis that things always change, we have gained a very important self-
help tool. Mindfulness can also help you remember that if your mind generates a thought or
memory that is uncomfortable, you can change it by focusing somewhere else.
Mindfulness is also a useful therapy tool that you may be able to use for self-help. For
instance, a therapist might ask a client in the middle of a flashback to try to focus on
and describe how their body feels right now, asking questions like, “What sensation do
you feel in your body as you remember this incident? What happens inside as your hand
makes a fist?” Or, a therapist may ask a client to focus in the opposite direction, pulling
away from a panicky feeling in the body to describe the items they can see in the room
they are in now. Therapists Pat Ogden, Kekuni Minton, and Clare Pain, in their book
Trauma and the Body: A Sensorimotor Approach to Psychotherapy, recommend helping
trauma survivors practice these in-and-out observations as “a means to help them
observe, firsthand, how their chronic orienting tendencies
50
toward reminders of the past
recreate the trauma-related experience of danger and powerlessness, whereas choosing to
orient to a good feeling can result in an experience of safety and mastery.”
51
Here, too, “[t]hese orienting [mindfulness] exercises need to be practiced again and again
for mastery.”
52
As the opening quote reminds us, it takes a lot of practice to lay down new
positive thinking patterns in a brain shaped by surviving trauma, but the end result is
worth the work.
50
The direction in which your mind usually wanders, an insight you can pick up from meditation, as well.
51
Ogden, Pat, Minton, Kekuni, & Pain, Clare. (2006). Trauma and the body: A sensorimotor approach to psychotherapy, p. 175-6.
52
Ogden, Pat, Minton, Kekuni, & Pain, Clare. (2006). Trauma and the body: A sensorimotor approach to psychotherapy, p. 176.
Additional readings on mindfulness as a healing tool
McKay, Matthew, Wood, Jeffrey C., and Brantley, Jeffrey (2007). The dialectical
behavior therapy skills workbook: Practical DBT exercises for learning mindfulness,
interpersonal effectiveness, emotion regulation and distress tolerance. Oakland,
California: New Harbinger Publications, Inc.
Siegel, Daniel J., M.D. (2010). Mindsight: The new science of personal transformation.
New York, New York: Bantam Books.
Siegel is widely regarded as a must-read for people interested in how one human brain
affects another. This book is written for the general public, but requires a fairly high literacy
level. This isn’t a “trauma book,” but will help those seeking to understand more about how
the brain works and can be changed.
87
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Resourcing
It is not possible to survive as a transgender, gender non-binary, or gender non-
conforming person without developing considerable internal strengths. Unfortunately,
it is easy to lose sight of these strengths when you are confronting a new problem or
dilemma that may feel overwhelming. This exercise, adapted from Robin Shapiro’s 2010
book The Trauma Treatment Handbook: Protocols Across the Spectrum,
53
is designed to
help you remember and access your strengths.
1. Think of a current problem.
2. Think about what internal quality or strength you will need to surmount this problem.
3. Now think of a time when you used that quality effectively.
4. When you think of that time, what emotion do you feel right now? Where do you feel
that in your body?
5. What word would go with that quality and your feeling when you think of it?
6. Think of a recent time when it would have been helpful to be in touch with that
internal resource and imagine using it more.
7. Now think of using it successfully on the current problem.
8. And think of more times in the future when you could successfully use that resource.
Sexuality
As in other areas, trauma survivors often find themselves going to black-and-white
extremes with sexuality. Some swear off sex entirely, at least when it comes to being
touched themselves. Others seem to have internalized the abusers’ belief that their
body and sexuality belong to other people, and have sex whenever asked or demanded.
A healthier goal is to own your own sexuality. An expert in working with sexual assault
survivors to reclaim their sexuality, Staci Haines, puts it this way in her book Healing
Sex: A Mind-Body Approach to Healing Sexual Trauma: “You now have the first, middle,
and last word on what you choose sexually.”
54
So what will you choose? The options are endless, but sexual assault survivors are often
limited by having internalized myths from the culture at large or from their perpetrators.
Here we briefly list some sexuality facts that sexual assault survivors often do not know
or remember:
It is okay to choose to have sex, and okay to choose not to have sex. Being in
a relationship is not a requirement or bar to either choice. It is okay to take a
break from sex, even if you are at the moment engaged in sexual activity. What
is important is that you remember to retain choice and control over when,
where, how, and whether to engage in sexual activity. Sexual activity does not
have to be reciprocal or “have parity”: it is okay for one person to focus on
giving or receiving pleasure in any given encounter.
53
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the spectrum, pp. 50-51.
54
Haines, Staci. (2007). Healing sex: A mind-body approach to healing sexual trauma, second edition, p. 105.
88
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Having boundaries—things you do not want to ever do, or might want to do
under the right circumstances, body parts that you do not want touched, or
words you do not want to hear in a sexual encounter—is more than okay;
they are almost essential, particularly for sexual assault survivors who have
experienced “sex” with someone who used them only for their own needs. It is
also okay for boundaries to be fluid, changing over time or even in the midst of
a sexual experience. You have a right to have sexual partners who respect these
boundaries.
A lot of things can be part of being sexual. If you can only think of one or a few
ways “sex” is done, consider expanding your options by reading books, watching
videos, or talking to others, especially those with a focus on sensuality
as opposed to sexuality. Perhaps thinking of sex as being touched and
remembering that all of your skin can be a “sexual organ” may help you realize
other options you might want to try.
Orgasm is not the only appropriate goal for sex. Indeed, many people find their
sexual experiences are deeper and more fulfilling when the goal is having a
high-quality connection with your partner (or yourself!).
It is okay to talk about sex. In fact, talking about
sex outside of as well as in the middle of a sexual
encounter is recommended! Talking allows you and
your (potential) sexual partner to understand what
you each like and do not like, including what makes
each of you feel good, loved, or connected and what
does the opposite. If you are sometimes triggered
during sex, it is particularly important to talk to
your partner about this beforehand and when it
happens (or at least soon after), so that your partner
knows that you are not rejecting them and so the two
of you can decide together what you are going to do
if/when triggered. It can be very helpful to set up a
“safe word” you can say when you become triggered
to signal to your partner what is happening (one
couple used “ghosts”). If you are among the survivors
who find it difficult or impossible to talk when
triggered, consider developing a hand signal or other
non-verbal cue.
Never sacrifice your long-term safety. Even if you are already HIV+, it is
critical to avoid engaging in behaviors that may transmit sexually transmitted
infections. Too often a trans person—whether they are a survivor of sexual
abuse or not—may sacrifice or skip safer sex negotiations because they are
“ One day, our therapist asked Roger, ‘How
do you feel when Karen’s not responding
to you [during sex], when she’s closed
off?’ And he started talking about being
flat-out terrified. To hear him talk about
being terrified that our relationship was
going to end made me stop and realize
that I wasn’t the only one who was going
through terrible, awful feelings. Here was
another human being, who I loved very
deeply, who was bleeding, and some of
that was a wound I had inflicted by being
so wrapped up in myself.”
Bass, Ellen & Laura Davis (2008). The courage to
heal: A guide for women survivors of child sexual
abuse, 4th edition, pp. 307-308.
Therapist Mike Lew points out that many people confuse sexual assaults or abuse
with sex. He points out the difference: “If you hit someone over the head with a
frying pan, you wouldn’t call it cooking.”
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual child abuse (Second edition), p. 64.
89
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
desperate for connection and affirmation. You are worth more than that; do
not risk your long-term safety and well-being by engaging in unsafe sex. If you
are unsure what sexual behaviors are considered safe and unsafe, particularly
when it comes to trans bodies, check out some trans safer sex guides. We
have listed a couple at the end of this section. We also recommend that people
look into the new HIV-prevention medication regime, PrEP (pre-exposure
prophylaxis). You can find out more at the U.S. Centers for Disease Control and
Prevention PrEP website, http://www.cdc.gov/hiv/prevention/research/prep/.
One exercise you might like to try with a partner is to have a sexual encounter where
you or your partner agree to ask for explicit consent before every new type of touch
or activity. Both of you may find this exercise very eye-opening as it slows the action
down and requires both partners to think about what they really want. If the two of
you end up laughing and/or crying as a result, good job! You have just had a successful
communication that you can build on for future encounters.
Additional readings on sexuality
Bass, Ellen & Laura Davis (2008). The courage to heal: A guide for women survivors of
child sexual abuse, 4th edition. New York, New York: HarperCollins Publishers.
See particularly, “Healthy Intimacy” and “Reclaiming Your Sexuality.” Note that this book was
explicitly written for women.
Davis, Laura (1990). The courage to heal workbook: For women and men survivors of
child sexual abuse. New York, New York: HarperCollins Publishers.
The Appendix, “Guidelines for Healing Sexually,” includes several worksheets and exercises
that may help you think through sexual issues.
FORGE. Hot, safe sex for transfeminine folks and partners. http://www.forge-forward.
org/wp-content/docs/HIV-MTF-web.pdf
FORGE. Hot, safe sex for transmasculine folks and partners. http://www.forge-forward.
org/wp-content/docs/HIV-FTM-web.pdf
Fradkin, Howard (2012). Joining forces: Empowering male survivors to thrive.
Carlsbad, California: Hay House.
See particularly, “Dare to Dream You Can Connect Safely, Intimately, and Romantically.”
Note that this book was explicitly written about men.
Haines, Staci. (2007). Healing sex: A mind-body approach to healing sexual trauma,
2nd edition. San Francisco, California: Cleis Press, Inc.
We highly recommend this book. Haines explicitly supports all sexual orientations and a wide
range of sexual practices, including polyamory and BDSM. We particularly recommend the
chapters on embracing triggers and the emotions of healing. Note, however, that Haines has
the unfortunate tendency to write as though all sexual abuse survivors are female.
Lew, Mike (2004). Victims no longer: The classic guide for men recovering from sexual
child abuse, updated and revised. New York, New York: HarperCollins Publishers.
See particularly, “Sex, Trust, and Caring” and “Sexual Feelings.” Note that this book was
explicitly written about male victims of child sexual abuse.
90
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Breath training
This protocol is adapted from John Briere and Catherine Scott’s book, Principles of
Trauma Therapy: A Guide to Symptoms, Evaluation, and Treatment.
55
Learning to pay attention to breathing, and learning to breathe deeply, can both help with
relaxation and reduce anxiety. When we get anxious or have a panic attack, one of the first
things that happens is that our breathing becomes shallow and rapid.
Initially some people become dizzy when they start breathing deeply, which is a normal
reaction. For this reason, it is encouraged that you try breathing exercises sitting down
(vs. standing up) until you have become experienced and comfortable with them.
Breathing exercises may feel strange at first because it is something many of us take
for granted and don’t think about. They may feel awkward, too, since many breathing
exercises instruct us to breathe more deeply into our belly, which is not common for
many people. Most of us are used to holding our stomachs in, because of tight clothes
or because we are conscious of weight or how we look. Try to give yourself literal and
figurative room to breathe. Until you internalize the steps of this exercise, it may help to
have someone slowly read you the steps as you go through them.
1. Sit in a comfortable position.
2. Close your eyes or, if it is more comfortable, focus them on a spot on the wall or floor,
softening your gaze.
3. Try to stay “in the moment” while doing breathing exercises. If your mind wanders
(e.g., begins thinking about what to make for dinner or ruminating over an argument
with someone), note where it has wandered to and then gently bring it back to the
immediate experience of breathing.
4. Begin breathing through your nose, paying attention to the breath coming in and
going out. Pay attention to how long each inhalation and exhalation lasts. Do this for 5
or 6 breaths.
5. Start breathing more deeply into your abdomen. This means that the belly should
visibly rise and fall with each breath. This sort of breathing should feel different from
normal breathing, and you should notice that each breath is deeper than normal. Do
this for another 5 or 6 breaths.
6. Imagine that each time you breathe in, air is flowing in to fill up the abdomen and
lungs. It goes into the belly first, and then rises up to fill in the top of the chest cavity.
In the same way, when breathing out, the breath first leaves the chest, and then the
abdomen. Some people find it helpful to imagine the breath coming in and out like a
wave. Do this for another 5 or 6 breaths.
7. Once you are breathing deeply and fully into the belly and chest, the next step is to
slow the breath down. Slowly count to three with each inhalation and exhalation—in
for three counts, out for three counts. With practice, you may be able to slow your
breath even further. No specific time is necessary; the goal is to try to slow your
breathing. Do this for 5 or 6 breaths.
55
Briere, John & Scott, Catherine. (2006). Principles of trauma therapy: A guide to symptoms, evaluation, and treatment,
pp. 279-280.
91
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Briere and Scott recommend that their clients practice this
breathing 5 to 10 minutes a day, ideally at a specific time of
day to make the exercise a regular part of your daily routine.
Eventually you should be able to extend this exercise to other
times in the day as well, especially when relaxation would be
a good idea (e.g., before important meetings, in stressful social
situations, or whenever you feel especially anxious). Remember
to count during each inhalation and exhalation, since counting,
by itself, will come to stimulate the relaxation response.
Emotions and healing
Emotions and their regulation are typically major concerns for
survivors of trauma. As noted in “The Brain and Trauma”
section in this Guide, trauma actually changes the brain in
lasting ways. In addition, experiencing emotions releases
different chemicals in our brains, changing the way our
brains operate in the moment.
If you were abused as a child, you are particularly likely to
have problems with emotional regulation. Therapists Sandra
C. Palvio and Antonio Pascual-Leone, in their book Emotion-
Focused Therapy for Complex Trauma: An Integrative
Approach, say, “Children learn to rely on avoidance to cope
with the painful, powerful, and confusing feelings generated
by these [abuse] experiences. When experiential avoidance
is chronic, it is associated with a number of disturbances,
including substance abuse, self-injurious behavior,
interpersonal problems, and impoverished social support…
Moreover, chronic avoidance is thought to perpetuate trauma symptoms, interfere with
recovery, and contribute to immune system breakdown…”
56
Because so many survivors
choose to handle their emotions by trying to control or avoid them, what follows is a
discussion of the stages of emotion and why going through them can be very healing
for survivors. It is lightly adapted from Staci Haines’ book Healing Sex: A Mind-Body
Approach to Healing Sexual Trauma, 2nd edition.
57
The five stages of emotions
“Emotions and emotional expression follow a predictable cycle. The cycle of emotions can
be like a wave building to fullness and crashing on the beach, then reintegrating into the
ocean only to come to shore once more.
1. First, the emotion shows up as a sensation or feeling. The emotion may be a response
to either a current or past experience. Of course, emotions from the past will emerge
as you heal.
56
Paivio, Sandra C., & Pascual-Leone, Antonio. (2010). Emotion-focused therapy for complex trauma: An integrative
approach, p. 37.
57
Haines, Staci. (2007). Healing sex: A mind-body approach to healing sexual trauma, second edition, pp. 175-177.
“The ability to tolerate and
regulate affect [emotion]
creates the necessary
condition for the brain’s
continued growth
throughout life.”
Cozolino, Louis. (2010). The neuroscience of
psychotherapy: Healing the social brain
(Second edition), p. 47.
Some people may find that 5-10 minutes
feels too difficult, or that this series of
instructions may not be reachable. There
are many phone apps that may offer briefer
and overtly guided support for focusing
on your breath. One example is Centering
Practice, an app by Channel Capital.
Explore and find what is right for you.
92
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
2. Then you have a choice. You can turn away from the emotion or you can open toward
it. There are times when putting an emotion on hold is a good way of taking care of
yourself. (See “Container Exercise,” above, for an example of a tool to put emotions
on hold.) Holding emotions down doesn’t work as a way of life, however. The longer
you brace against emotions, particularly those wrought by abuse, the longer those
emotions will run your life.
Instead of turning away from emotions, you can choose to welcome them. In stage two
of the cycle, you attend to the emotion, feeling your way into the sensation. When you
do this, the emotion tends to intensify and reveal itself. This stage can often be the
scariest. Just as in healing from dissociation, feeling your emotions means learning to
tolerate these sensations in your body.
3. Stage three brings the emotion to fullness. The emotion grows in
its charge and sensation. You may feel like you are about to cry.
Your chest may overflow with joy and pleasure. You may want
nothing more than to throw a major tantrum.
4. Stage four brings release. Depending upon the emotion, you
may experience this release as gentle or very intense. You
may sweat or blush, sob, shake, tremble, kick, laugh, yell, or
become overheated or chilled. This expression is the release of
the emotion. Surprisingly, the full expression of even the most
intense and scary emotions usually lasts only twenty minutes
at most.
5. After the full expression of the emotion, you may find relief, peace, renewed energy,
and a sense of healing or transformation. This is the completion of the cycle, or what
some people call integration. Take time to be with yourself. Breathe. Check in with
your internal sense of safety and well-being. Notice that you are alright, that you are
complete with this piece of your healing; it can be helpful to say this out loud. Bring
intentionality to this part of the process.
Pay attention to the completion stage. Sometimes you may find yourself pouring out
emotion with no experience of change or integration. You could be recycling the trauma
rather than healing it. This does not happen often—most people who are not ready for
healing try to repress emotions related to the abuse. But if this is happening to you, ask
yourself, ‘What would it take to complete this feeling?’ If you don’t know the answer, make
one up. Imagine you know what completion would feel like. Try it on for size.
Take a moment to consider which stages in the cycle of emotions you are good at and
which you need to practice. Are you able to express your emotions, or do you tend to hold
or repress them? Can you complete a cycle of emotion and move to integration? Where can
you use more support or learning?”
“...[M]any survivors of child abuse
have learned to be externally vigilant
at the expense of attention to their
own internal experience and have
difficulties recognizing and
describing their feelings.”
Paivio, Sandra C., & Pascual-Leone,
Antonio. (2010). Emotion-focused therapy
for complex trauma: An integrative
approach, p. 50.
93
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Being witnessed in your emotions
Staci Haines, in her book Healing Sex: A Mind-Body Approach to Healing Sexual Trauma,
2nd edition, also has described a partnered exercise you may want to try.
58
(Again, this
passage has been lightly edited.)
“Being witnessed in the midst of your emotions is a powerful experience. Being
witnessed means just having someone be present with you as you feel your feelings.
Your friend, lover, or support does not need to change or fix your feelings. She or he
can simply witness. You can learn from others’ acceptance of your emotions that you
are truly okay. Other survivors are often relieved and happy when they see someone
finally express anger, grief, or longing. Everyone seems to breathe a big sigh of relief.
You can ask for specific support from your witness or support person. You may want
to be held or to rant and rave uninterrupted for twenty minutes. You can ask your
support person to take care of his or her own needs and boundaries. If the experience
gets too intense, he or she can take a break.
Some people are comfortable with certain emotions and not with others. Your friend
may be fine holding you when you cry, but freak out when you get really angry. Your
emotions are not ‘too much’ or ‘too intense.’ Expressing any degree of anger, loss,
or shame in a safe way is just fine. Your partner may simply not have developed the
capacity to hang with that depth of emotion. Let your partner take care of his or her
needs and limitations. Find a support person who can go with you where you need
to go.
You may find yourself wanting to ask for reassurance. Go ahead and ask. Look at
your partner. Let yourself see that someone is there. Ask, ‘Do you think this is bad?’
‘Am I hurting you?’ ‘How is this for you?’ You may need a reality check as you are
learning to express this depth of emotion.”
58 Haines, Staci. (2007). Healing sex: A mind-body approach to healing sexual trauma, second edition, pp. 187-188.
Additional readings on emotional regulation
Boon, Suzette, Kathy Stelle, & Onno van der hart (2011). Coping with trauma-related
dissociation: Skills training for patients and therapists. New York, New York: W.W.
Norton & Company, Inc.
Pages 263-322, “Coping with...Anger, Fear, Shame and Guilt, the Needs of Inner Child
Parts, Self-Harm.”
McKay, Matthew, Jeffrey C. Wood, and Jeffrey Brantley (2007). The dialectical
behavior therapy skills workbook: Practical DBT exercises for learning mindfulness,
interpersonal effectiveness, emotion regulation and distress tolerance. Oakland,
California: New Harbinger Publications, Inc.
The subtitle says it all.
Weisinger, Hendrie D. (1985). Anger work out book: Step-by-step methods for
greater productivity, better relationships, healthier life. Oakland, California:
New Harbinger Publications.
Old but good workbook and manual for those dealing with anger issues.
94
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Challenging maladaptive or problematic beliefs
“[To recover, it] may be necessary to think, react, and behave in ways that feel
impossibly dangerous.”
59
“I have learned that I am more than other people’s reactions to me.”
60
One of the most common and damaging aftermaths of abuse is that the victims often
draw dangerous conclusions and develop destructive beliefs about themselves as a
result of the abuse. These beliefs might include: believing that they deserved the abuse;
believing that they could have stopped the abuse; believing that they are “broken”
or “destroyed” because of their experience, etc. Many of these beliefs become deeply
embedded in survivors and require a lot of work to uproot. Some people depend heavily
on logic; if you are one of those, you might find the following cognitive approach useful.
In their book chapter, “Cognitive Therapy for Posttraumatic Stress Disorder,” Jillian
Shipherd, Amy Street and Patricia Resick lay out a series of questions that have
helped some survivors successfully challenge the beliefs they hold as a result of being
traumatized.
61
We have listed the questions first and given their example next.
Below is a list of questions to be used in helping you challenge your maladaptive or
problematic beliefs. Not all questions will be appropriate for the belief you choose to
challenge. Answer as many questions as you can for the belief you have chosen
to challenge.
1. What is the evidence for and against this idea?
2. Are you confusing a habit with a fact?
3. Are your interpretations of the situation too far removed from reality to be accurate?
4. Are you thinking in all-or-none terms?
5. Are you using words or phrases that are extreme or exaggerated (i.e., ‘always,’
‘forever,’ ‘never,’ ‘need,’ ‘should,’ ‘must,’ ‘can’t,’ and ‘every time’)?
6. Are you taking selected examples out of context?
7. Are you making excuses? (e.g., ‘I’m not afraid. I just don’t want to go out.’;
‘Other people expect me to be perfect,’; or ‘I don’t want to make the call because
I don’t have time’).
8. Is the source of information reliable?
9. Are you thinking in terms of certainties instead of probabilities?
10. Are you confusing a low probability with a high probability?
11. Are your judgments based on feelings rather than facts?
12. Are you focusing on irrelevant things?
59
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual child abuse (Second edition), p. 153.
60
Cloitre, Marylene. & Rosenberg, Anna. (2006). “Sexual revictimization: Risk factors and prevention.” In Follette, Victoria M.
& Ruzek, Josef I. (eds.) Cognitive-behavioral therapies for trauma (second edition), p. 354.
61
Shipherd, Jillian C., Street, Amy E., & Resick, Patricia A. (2006). “Cognitive therapy for Posttraumatic Stress Disorder.”
In Follette, Victoria M. & Ruzek, Josef I. (eds.) Cognitive-behavioral therapies for trauma (second edition), pp. 109-111.

95
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Example belief:
I take blame for the abuse and feel I did something bad to cause it.
1. What is the evidence for and against this idea? For—I should have walked away or
said no. I feel as if I could have done something. Against—they would have done what
they wanted, regardless of what I said or did.
2. Are you confusing a habit with a fact? Yes. I have always told myself that it happened
to me because I was bad or did something wrong. I have always told myself, ‘if only I
had done something different,’ like it was all about what I did or was doing.
3. Are your interpretations of the situation too far removed from reality to be accurate?
Yes. I have distorted the reality of the situation. I have blamed myself for being bad
and allowing this to happen to me. In reality, I had no control or power over the
situation. The abusers were in total control or power over the situation. The abusers
were in total control and they are to blame.
4. Are you thinking in all-or-none terms? Yes. I have always used terms such as ‘bad’ and
‘wrong’ and considered the events as my fault. ‘I was bad,’ ‘I did something wrong,’ is
what I have told myself.
5. Are you using words or phrases that are extreme or exaggerated (i.e., ‘always,’
‘forever,’ ‘never,’ ‘need,’ ‘should,’ ‘must,’ ‘can’t,’ and ‘every time’)? Yes. I used a lot of
‘shoulds’ in my statements when describing the abuse.
6. Are you taking selected examples out of context? Yes. I am saying that there was
something I could or should have done or changed myself to have prevented it from
happening.
7. Are you making excuses? (e.g., ‘I’m not afraid. I just don’t want to go out.’; ‘Other
people expect me to be perfect,’; or ‘I don’t want to make the call because I don’t have
time’). Yes. I am afraid that I might let this happen again. I make excuses not to go into
the world and excuses that if I take blame then nobody else has to deal with it.
8. Is the source of information reliable? No. All the sources were straight from the
mouths of my abusers. They were only interested in hurting me, and nothing they said
was true of me or who I was.
9. Are you thinking in terms of certainties instead of probabilities? Yes. I have never
been objective about abuse. It has always made me feel unsafe with others, and when
things felt uncomfortable, I always wondered, what is wrong with me?
10. Are you confusing a low probability with a high probability? The probability of this
happening again is low, but I still feel as if it could, and I believe the probability to be
higher than it actually is.
11. Are your judgments based on feelings rather than facts? Yes. I feel guilty so I assume
that I did something wrong. That is not the fact at all.
12. Are you focusing on irrelevant things? My focus has always been on what I did or
could have done—things I had no control over. The abuse took place because the
abuser wanted it to, not because of something I did.
96
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Problem-solving and conflict resolution
If you grew up in an abusive household and/or were in an abusive relationship, your
very survival is testimony to the fact that you have developed very effective tools and
strategies for surviving in an abusive relationship. That does not mean, however, that
you have developed the communication and problem-solving skills you need to have
peaceful, nonviolent relationships. In fact, you may believe many things about conflict
and relationships that are counter-productive to respectful collaboration.
Some of those beliefs may be:
Every conflict ends with one winner and one loser. Victims often learn that in
relationships, one person gets his or her way and the other gets nothing.
People lie and manipulate. Abusers lie and manipulate. They make promises
they do not keep. They may have said what they were doing was in the victim’s
best interests, but in actuality the abuser was acting on her or his own behalf.
Abusers also manipulate, providing something the victim may desperately need
(like access to food or shelter, attention, or touch), but taking something much
bigger (like total compliance or dignity) from the victim in return.
Don’t know or say what you need or want. Victims in abusive relationships
learn that even if they can identify what they want, asking for it is usually not
a good idea. Not only are you likely to be disappointed, but you may have your
want used against you through manipulation or via belittling comments.
These sorts of beliefs are life-saving in abusive settings, but are actually damaging when
applied to relationships between equal, respectful adults. Not only may you not have
problem-solving skills, but you may well approach conflicts angry and/or fearful, making
it hard for you to access any memories of when the two of you have previously found
mutually-acceptable solutions.
Additional readings on coping with maladaptive beliefs
Boon, Suzette, Kathy Stelle, & van der hart, Onno. (2011). Coping with trauma-related
dissociation: Skills training for patients and therapists. New York, New York: W.W.
Norton & Company, Inc.
Pages 236-253, “Identifying Cognitive Errors” and “Challenging Dysfunctional Thoughts
and Core Beliefs.”
Rosenbloom, Dena, Williams, Mary Beth, & Watkins, Barbara E. (2010).
Life after trauma: A workbook for healing (2nd edition). New York, New York:
The Guilford Press.
Pages 34-40, “Coping with Negative Feelings about Yourself,” pages 49-75, “Thinking
Things Through,” and pages 204--210, “Thinking Through a Belief about Value and
Self-Esteem,” and “Weighing the Evidence on Beliefs about Value and Self-Esteem.”
97
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Since many of us have not learned problem-solving skills, we are presenting four skills
that, put together, can help you and someone else reach positive, mutually-pleasing,
solutions. The four skills are:
Why Chains can help people identify what it is they really want, a digging-deep
process that opens up many more options.
Joint Problem Statements help couples stay focused on finding options that
meet both people’s needs.
Brainstorming is a very useful method of generating multiple options to
choose from.
Fixing Bad Ideas is a technique for turning bad ideas into ones that may be
perfect for resolving a difficult issue.
Why Chains
Many people think there are only a handful of ways to resolve a problem where one
person wants one thing and the other person wants something else: One can give in, they
can take turns, or someone—maybe even both of them—can compromise and get only
part of what they want. In actuality, there are many ways these sorts of problems can be
solved. One of the most useful techniques is to figure out why each person wants what
they want. Each time someone can answer “why” they want something, they nearly always
see that there are more ways to fulfill their needs than they initially thought. Let us
illustrate with an example.
Partners Chris and Kerry have carefully saved a part of every paycheck for a vacation for
a very long time, and the sum is finally big enough to spend. Unfortunately, their first
conversation on the topic results in a conflict: Chris wants to go on a guided tour to India,
and Kerry wants to spend a week in a rented cabin in the forest. When Kerry asks Chris
why ze
62
wants a guided tour, Chris explains that for hir, the purpose of vacations is to
explore the world. Kerry realizes the thought of traipsing around and looking at various
tourist sites sounds like work, and that leads Kerry to realize that what ze really wants
from a vacation is lots of time to nap, read, and do nothing. Just this one round of “why
chain” has opened a broader set of options: Chris wants to explore the world on their
vacation, and Kerry wants plenty of time to just lounge around. Those needs still feel like
they conflict, so we will return to the couple in the Joint Problem Statement section.
Conflict resolution specialists call this process moving from your position—the thing you
initially asked for—to your interest—what you expect or hope to get from that thing.
Joint Problem Statements
In workshop settings, we often ask participants to pair up on opposite sides of a table
narrow enough that when they put their right elbows on the table, they can meet and
grasp hands in the middle. “This is the M&M game,” we say, “Where the purpose is to
win M&Ms. You will earn an M&M every time the back of your partner’s hand touches
the table. You will have 60 seconds. Any questions? Then, 1-2-3-go!” When the 60 seconds
are up, we ask to whom we owe one M&M, to whom we should give two M&Ms, etc. After
asking about people we owe four to, we ask, “And is there anyone we owe more than four
62
Ze and hir are two of many non-gendered pronouns. You can learn more at http://forge-forward.org/wp-content/docs/gen-
der-neutral-pronouns1.pdf
98
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
M&Ms to?” Nearly always there is at least one pair where each partner has earned more
than 30. This shocks everyone else, who can’t understand how they did that, until we have
them demonstrate: holding hands, they quietly and calmly take rapid turns touching the
back of their hands to the table.
As we noted above, both survivors and non-survivors often believe that conflicts are win/
lose propositions. When a conflict is identified—just like the workshop participants when
asked to place their elbows on a table and grasp hands—we tend to get into position
to compete, to ensure that we win and our “opponent” loses. At best, we look for
a compromise, where both people get some—but not all—of what they want.
Joint Problem Statements are designed to remind us there is another option, one
where both parties can win. Joint Problem Statements encourage us to work harder
at coming up with one or more options that meet all of what both people want. The first
step is to use at least one round of a Why Chain to get to both individuals’ interests. The
next step is to write down both people’s goals with a large “and” in the middle:
It may be particularly important for couples with one or two survivors to physically write
out their joint problem statement and keep it in front of them as they continue to work.
Make sure you draw a circle or other border around the joint problem statement to help the
two of you to remember that neither person’s needs are to be sacrificed in this process.
Brainstorming
The next stage is to begin brainstorming. Brainstorming, for those who are not familiar, is
a process in which there should be no judgment or censorship. The goal is simply to come
up with as many ideas as possible in a short time, without cutting down the number of
ideas through censorship (“people would think I am weird if I said that”) or practicality
(“they are not taking civilians to the moon yet”). The nice thing about brainstorming is
the more brains involved in storming, the better. This is an excellent place in which to
use your friends and acquaintances via social media. Simply post your joint problem
statement and invite people to suggest possible solutions. Make sure you encourage
people to build on each others’ ideas, as that can be especially fruitful.
When Chris and Kerry brainstormed, their list included such items as:
We could go on separate vacations
We could have a restful vacation for Kerry in the first half of our vacation,
and then go world exploring next, when Kerry might feel more up to it
We could get a whole bunch of travel documentaries for Chris and have a
stay-at-home vacation
We could go on a cruise and Kerry could stay aboard while Chris went on the
shore excursions
“OUR GOAL IS TO FIND A VACATION IDEA THAT…
Allows Chris to explore the world
AND
Gives Kerry plenty of time to lounge around.”
99
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Fixing “Bad” Ideas
This technique comes from Barbara Sher’s classic 1979 book, Wishcraft: How to Get
What You Really Want; A Unique Step-by-Step Plan to Pinpoint Your Goals and Make
Your Dreams Come True.
63
Take one of the “worst” ideas in your brainstormed list. In
one workshop, a single man who was looking to meet people but who felt shy in social
situations picked the idea “wear a big sign saying, ‘I’m single’” as the worst idea on the
list workshop attendees had brainstormed for him. The first step in fixing a “bad” idea
is to identify what is good about the idea. After working at it awhile, the man finally
said what was good about the idea is that it got people’s attention. The second step is to
identify what is bad about the idea. For him, a sign was just too obvious. In step three, the
goal is to keep what is good about the idea and fix what is bad. So the group brainstormed
a second list of things that get people’s attention but aren’t too obvious. His final choice
from this list: he began wearing buttons with various sayings on them to social events.
They caught people’s attention and often prompted them to ask him what the saying
meant, thereby opening a conversation he could then pursue.
Chris and Kerry were pleased with the idea of a cruise since it did combine both lots of
opportunity for rest and visits to new places. However, Chris was not too happy with the
thought of going on those shore excursions alone; exploring just did not seem too fun
without someone to share it with. So the couple tried to fix the bad part of the idea and
came up with a solution that turned out to work perfectly: they asked an adventurous
friend if he would like to join them on the cruise, and he and Chris went on all the shore
tours together, then came back at night and shared their experiences with a rested and
therefore much more appreciative Kerry.
Putting It All Together
In addition to run-of-the-mill issues like vacations and spending money, survivors
and their partners may find themselves in conflict over issues related to the abuse. For
instance, Jesse and Sam were arguing over whether to visit Jesse’s father, who had failed
to intervene when told of child sexual abuse. Asked why ze wanted to visit, Jesse said ze
didn’t want to feel like an orphan. Sam opposed the visit because ze felt the visit would
be emotionally damaging to Jesse. This round of the Why Chain didn’t seem to get them
too far, so they pursued it for another round. Jesse said hir fear of feeling like an “orphan”
was about having no one to talk to who knew about hir childhood. Sam said what ze
wanted was for Jesse to feel loved, not ignored or unworthy of protection, which was how
Jesse had felt after previous visits with Dad. This round of the Why Chain seemed to hold
more promise, so they wrote down their joint problem statement:
63
Sher, Barbara. (1979). Wishcraft: How to get what you really want; A unique step-by-step plan to pinpoint your goals and
make your dreams come true, pp. 131-134.
“OUR GOAL IS TO FIGURE OUT HOW TO HAVE A VISIT WHERE…
Jesse can talk about hir childhood with someone who knows about it
AND
Jesse leaves feeling loved.”
100
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Their brainstorm included ideas like:
Jesse could write a letter to hir father explaining exactly what ze wanted out of
the visit
Sam could accompany Jesse, and if the visit ended up making Jesse feel bad,
Sam could work on helping Jesse feel loved by Sam
Jesse could ask hir father to answer some questions by letter or email, and Sam
could edit out any bad parts before ze gave it to Jesse to read
When they asked their social network for ideas, one friend wrote:
“Bring me a photo album, and we can go through it together.”
Although the idea of going through a photo album excited Jesse, one of the things
Jesse realized ze wanted was someone who could add to what ze remembered about
hir childhood. Holding on to the photo album idea and looking for someone who knew
something about Jesse’s childhood led Jesse think of hir father’s best friend Joe, whom ze
had always liked. They called Joe, who turned out to be very happy to go through a photo
album with the two of them and talk about what he knew about Jesse’s family. The result
was both informative and healing for both Jesse and Sam.
Relationship attachment styles and issues
“Relationships are our natural habitat…”
64
“A look not given, a message not understood, a yearning for closeness not met,
become magnified into a re-creation of emotions around early trauma. Feelings
related to dependency needs and deep unfulfilled yearnings are replaced by rageful
feelings and blaming attacks.”
65
“Once partners know how to speak their need and bring each other close, every trial
they face together simply makes their love stronger.”
66
“There is no injury-proof relationship. But you can dance together with more verve
and panache if you know you can recover when you step on each other’s toes.”
67
“New evidence indicates that reparative adult experiences enable those with
attachment traumas to increase their ability to cope with stress and restore a sense
of security.”
68
There is now little scientific debate over whether we are more influenced by our genes
(“nature”) or our experiences (“nurture”): the consensus is they both influence the other.
And so it is when a baby is born. Totally dependent for its survival on a handful
to people—or as few as just one—the baby’s inborn personality interacts with the
64
Cozolino, Louis. (2010). The neuroscience of psychotherapy: Healing the social brain (Second edition), p. 179.
65
Solomon, Marion F. (2003). “Connection, disruption, repair: Treating the effects of attachment trauma on intimate
relationships.” In Solomon, Marion F. & Siegel, Daniel J. (Eds.), Healing trauma: Attachment, mind, body, and brain, p. 324.
66
Johnson, Susan. (2008). Hold me tight: Seven conversations for a lifetime of love, p. 48.
67
Johnson, Susan. (2008). Hold me tight: Seven conversations for a lifetime of love, p. 184.
68
Solomon, Marion F. (2003). “Connection, disruption, repair: Treating the effects of attachment trauma on intimate
relationships.” In Solomon, Marion F. & Siegel, Daniel J. (Eds.), Healing trauma: Attachment, mind, body, and brain, p. 331.

101
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
characteristics of its caregiver(s) in a way that literally shapes its brain. If the caregiver
is “good enough” in responding appropriately to the baby’s needs, the baby learns to
trust that both it and the world are good and safe. If, on the other hand, the caregiver(s)
repeatedly fail to meet the baby’s needs and hence threaten its sense of wellbeing and
safety, or, even worse, actively frighten the baby by yelling at it, shaking it, or seeming
indifferent to the baby’s cries, the baby’s brain gets organized in a very different way.
That, in a nutshell, is “attachment theory”: how secure you felt in the care of your first
caregivers will influence not just how you see the world and how you relate to other
people, but also actually influences how your brain developed.
Well-cared-for infants and children learn they can depend on adults (i.e., the world they
live in) to meet not just their physical needs, but their emotional needs, as well. When
they are hurt or upset or frightened and turn to these adults, the adults will comfort and
soothe their upset feelings. Robin Shapiro explains what children learn from this kind
of care: “When our parent or caregiver mirrors our affect, soothes us, or appropriately
responds to us, we learn that we can expect a response, that we are worth responding to,
and that we can be soothed.”
69
These well-cared-for infants grow up “secure,” able to have
positive intimate relationships as adults. Attachment expert Louis Cozolino explains it
this way: “A secure attachment indicates that we have learned to successfully utilize our
relationships with others to quell our fears and modulate our arousal.”
70
On the other hand, if the primary caregiver is depressed, mentally ill, abusive, or
traumatized themselves, they are frequently unable to help the child soothe themselves.
Worse, they may even “create alarming experiences” for their child such as being
completely unresponsive, yelling at the child, or punishing the child for being upset or
bothering them. If the child has nowhere else to go for soothing, the caregiver’s response
creates a Catch-22: “the more an individual is injured or terrorized, the stronger his
or her need for protection and comforting.”
71
These children grow up with “attachment
styles” that are variously described as fearful, preoccupied, avoidant, insecure, anxious,
ambivalent, and disorganized. A “normative” sample found that about half of adults are
securely attached, but samples of abuse survivors show that the vast majority fall into
one of the non-secure categories.
What does it mean to have a non-secure attachment style? Psychotherapist Marion
Solomon has three very good descriptions:
[T]he relationship always feels tentative, and there is a tendency to test the love to
alleviate the constant doubts, even when things are going well. At the same time, any
sign that needs might be ignored or denied is met with avoidance, numbness, and
criticism, often along with self-doubt and self-blame. The internal message,
‘I am defective, destructive, and unlovable,’ is repeatedly confirmed.
From their early experience, they have learned that it is not safe to depend on
others, and when disagreements erupt, they become defensive. In stressful
situations they utilize various coping strategies, including walling themselves off from
another to avoid emotional engagement, hiding a true self while showing a façade
that seems more acceptable, or acting out angrily when they experience disruptions
69
Shapiro, Robin. (2010). The trauma treatment handbook: Protocols across the spectrum, p. 32.
70
Cozolino, Louis. (2010). The neuroscience of psychotherapy: Healing the social brain (Second edition), p. 233.
71
Cloitre, Marylene, Cohen, Lisa R., & Koenen, Karestan C. (2006). Treating survivors of childhood abuse: Psychotherapy for
the interrupted life, p. 15.
102
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
with significant others. These are methods of self-protection developed over time
during repeated painful encounters with important figures in their lives.
It is the proneness to overreact to differences, the inability to accept another’s views,
and inability to reengage after disrupted interactions that are so harmful
to intimate relationships.
72
Securely attached adults have good self-esteem and generally trust
that their partnerships will withstand the ups-and-downs and
disagreements all relationships experience. Insecurely attached adults
doubt themselves and their partners and so are prone to overreaction
and panic when they experience a relationship problem. Some
insecurely attached adults try to compensate by saying they do not
need relationships at all, but a growing number of experts are saying
that this is biologically impossible: humans depend on each other in
really critical and not always obvious ways. Susan Johnson, for
example, says flatly: “We need emotional attachments with a few
irreplaceable others to be physically and mentally healthy—to survive.”
73
Can attachment style be changed? Although most theorists say the pattern, once laid down,
is hard to break, “…recent studies confirm that insecurely attached people who are married
to securely attached partners can, within a period of 5 years’ time, modify an insecure
attachment pattern.”
74
More importantly, couples can learn skills to help them understand
that, as Susan Johnson says, “most fights are really protests over emotional disconnection.”
75
Once that is understood, they can work on making each other feel secure before attempting
to resolve the issue at hand.
A chart from Leah Leonard, Victoria Follette, and Jill Compton may help you keep in mind
the possible difference between what your partner may say and what they may actually
want in terms of being reassured that the two of you are securely connected:
76
WHAT MAY BE SAID WHAT MAY BE MEANT
“I am feeling vulnerable.” “Please sit with me,” “Please give me a few minutes to myself,” or
“Please hold me while I cry.”
“I am feeling angry.” “Listen to what I am telling you,” “Let me tell you about what is
bothering me,” or “You do not have to fix this situation—all I want
is for you to let me talk about it.”
“I am feeling scared.” “Please sit with me.” “Please let me tell you what I am afraid of,” or
“Please use a quieter voice when we talk.
“I am feeling happy (excited).” “Let me tell you about why I am excited,” “Celebrate with me,” or
“Let me be happy.
72
Solomon, Marion F. (2003). “Connection, disruption, repair: Treating the effects of attachment trauma on intimate relation-
ships.” In Solomon, Marion F. & Siegel, Daniel J. (Eds.), Healing trauma: Attachment, mind, body, and brain, pp. 326-327.
73
Johnson, Susan. (2008). Hold me tight: Seven conversations for a lifetime of love, p. 15.
74
Solomon, Marion F. (2003). “Connection, disruption, repair: Treating the effects of attachment trauma on intimate
relationships.” In Solomon, Marion F. & Siegel, Daniel J. (Eds.), Healing trauma: Attachment, mind, body, and brain, p. 331.
75
Johnson, Susan. (2008). Hold me tight: Seven conversations for a lifetime of love, p. 30.
76
Leonard, Leah M., Follette, Victoria M., & Compton, Jill S. (2006). “A principle-based intervention for couples affected by
trauma.” In Follette, Victoria M. & Ruzek, Josef I. (eds.) Cognitive-behavioral therapies for trauma (second edition), p. 379.
“If both of you are needy children
at the same time and no one is the
adult, you’ve got two unsupervised
kids going at it, and that generally
means trouble.”
Davis, Laura. (1991). Allies in healing:
When the person you love was sexually
abused as a child, p. 59.
103
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
One way to put these relationship “attachment” concepts to use is a technique called
“Three Reasons.” When you find yourself reacting negatively to something someone has
done, try to come up with at least three different “stories” of what may have motivated
their behavior, at least one of which must be positive. For example, if
your partner is late meeting you again, possible reasons might be:
they are meeting with a (secret) lover; they have been in an auto
accident; or (the positive one) they suddenly remembered how much
they love you, and stopped to buy you flowers. Here is another example
which combines attachment theory and “Three Reasons.” You and your
partner have an argument, and your partner suddenly clams up and
refuses to speak to you. Possible reasons might include: your partner
has decided to leave you (a thought that might occur to someone who
is insecurely attached); your partner is thinking how they are going to
get back at you (another thought that might occur to someone who is
insecurely attached); or your partner very much loves you and values
the relationship, and is afraid if they say anything more in their current (very upset) state,
it will be hurtful and so is being silent until they get their emotions under better control.
Trying to come up with three possible reasons why someone is acting the way they are
can be extremely helpful. Most importantly, our brains tend to look for evidence to bolster
whatever we are thinking. If you make yourself actively consider several possible reasons,
your brain stays open to seeing more of what is actually going on. This is an excellent
conflict resolution tool, helping prevent you from escalating a situation that may not
actually call for escalation. In addition, for those of us who did not benefit from “securely
attached” childhoods, making ourselves think of a way in which a conflict might be a sign
of how much our partner loves us and wants a continued relationship may help us avoid
creating the very break we most fear.
“Love is everything it’s cracked
up to be… It really is worth fight-
ing for, being brave for, risking
everything for. And the trouble is,
if you don’t risk anything, your
risk is even greater.”
Erica Jong, quoted in Johnson, Susan.
(2008). Hold me tight: Seven conversa-
tions for a lifetime of love, p. 9.
Additional readings on attachment theory and couples
Jonson, Susan. (2008). Hold Me Tight: Seven Conversations for a Lifetime of Love.
[Add rest of citation here].
Add a note here if you want, just notice the length of the box.
Allen, Jon G. (2005). Coping with trauma: Hope through understanding (2nd edition).
Arlington, Virginia: American Psychiatric Publishing.
See especially pages 25-41, “Attachment.”
Dayton, Tian. (1997). Heartwounds: The impact of unresolved trauma and grief on
relationships. Deerfield Beach, FL: Health Communications, Inc.
Includes sections on the effect of trauma on the personality and on relationships.
Fruzzetti, Alan E. (2006). The high-conflict couple: A Dialectical Behavior Therapy
guide to finding peace, intimacy & validation. Oakland, California: New Harbinger
Publications, Inc.
This is a good self-help book for couples or others in intimate partnerships.
Karen, Robert (1994). Becoming attached: First relationships and how they shape our
capacity to love. Oxford: Oxford University Press.
This large book is as much of a history of the development of attachment theory and its
major researchers as it is an explanation of attachment theory.
104
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Time perspective therapy
“We heal out of the past and into the present.”
77
Many trauma survivors feel like they are constantly revisiting—voluntarily or through
unwanted flashbacks—their past trauma and/or negative beliefs stemming from the
trauma. This focus on the “negative past” tends to lead people to feel that they cannot
control what happens to them, so they become fatalistic about the future and therefore
do not feel very motivated to do much in the present. Because they are not able to make
and carry out positive plans, they are more vulnerable to others’ decisions, which are not
always in their interests. The subsequent negative outcome reinforces the cycle and their
belief that they are not in control of what happens to them.
To address this problem, psychologists Philip Zimbardo and Richard and Rosemary
Sword developed Time Perspective Therapy (TPT), an extremely simple process that they
claim has had remarkable success in reducing PTSD symptoms, including anxiety and
depression.
The theory says that our personal mix of views about our past, present, and future
determines how we make decisions:
“Past-oriented people make decisions based on negative or positive memories of
similar situations. Present-oriented people take immediate action based on pleasure
or avoidance, without thought for consequences. Future-oriented people make deci-
sions based on a reasoned assessment of the future consequences.”
78
The focus of TPT is developing habits and strategies that focus on coping with the mental
injury of trauma, which can unbalance survivors’ time perspectives as described above.
They explain the process to their clients this way:
“Then we engage them in a visualized narrative, a time metaphor that contrasts the
current negatives being experienced with imagined positives that could be possible
for them. First, we ask them to imagine that they have one foot stuck in the quicksand
of the past, and the other resting on the mud of the fatalistic present. The fatalistic
view is reasonable given that nothing has worked to help them out of the quicksand.
In this state of imbalance they are emotionally immobilized. To make a start, all they
need to do is lift that one foot out of the muck and mire of the past and put it on the
solid ground of the future. Then they need to bring the other foot out of the mud of
present fatalism and rest it on the more solid ground of present hedonism. Now they
are beginning to get a firm footing.”
79
Step one of the therapy is to identify past positive memories and substitute one of those
whenever a negative past memory pops up.
Step two is to replace “present fatalism” (the idea that there is not much a survivor can
do to make their own life better) with “selected present hedonism.” By that the therapists
mean choosing to engage in pleasant activities, ideally with other people. This could be
77
Cori, Jasmin Lee. (2008). Healing from trauma: A survivor’s guide to understanding your symptoms and reclaiming your life,
p. 227.
78
Zimbardo, Philip, Sword, Richard, & Sword, Rosemary. (2012). The time cure: Overcoming PTSD with the new psychology
of time perspective therapy, p. 60.
79
Zimbardo, Philip, Sword, Richard, & Sword, Rosemary. (2012). The time cure: Overcoming PTSD with the new psychology
of time perspective therapy, p. 74.
105
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
spending time with friends or family, joining a support group, starting an exercise regime,
attending religious services, or engaging in volunteer work helping others. This step
breaks the isolation that is common to trauma survivors, and begins to chip away the
survivor’s sense that they will never feel good again.
Step three is selecting and working on “a brighter future.”
“We’ve found that the best way to help PTSD sufferers overcome their past traumas is
to encourage them to envision a better future. This is accomplished by setting goals
and figuring out specific means by which these goals can be achieved. In turn, this
encourages feelings of a sustainable and secure future.”
80
Volunteering
Many of the self-protection impulses trauma survivors have are actually counter-
productive. A key example is the impulse to withdraw from people and social activities.
The theory behind that impulse is that if you do not leave the house, you have more
control over what happens in your vicinity; if you do not have contact with anyone, you
cannot be hurt by them.
The problem with the isolation impulse is that while it may feel self-protective, part of
the core damage of trauma comes from feeling alone and helpless at the time. Sexual
assault advocate Mike Lew says, “Abuse is committed in isolation; recovery takes place in
the company of others.”
81
Trauma expert Judith Herman concurs, “Recovery can take place
only within the context of relationships; it cannot occur in isolation.”
82
In our search for healing spaces and relationships, some of us focus only on trying
to locate those that are specifically labeled for “healing”: support groups, therapists,
a tremendously compassionate friend, etc. Our options become much wider when we
realize that we create a healing space whenever we help another person. Judith Herman
prescribes such outreach, urging people to adopt a “survivor mission”: “In taking care of
others, survivors feel recognized, loved, and cared for themselves…As each participant
80
Zimbardo, Philip, Sword, Richard, & Sword, Rosemary. (2012). The time cure: Overcoming PTSD with the new psychology
of time perspective therapy, p. 74.
81
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual child abuse (Second edition), p. 325.
82
Herman, Judith L. (1992). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror, p. 133.
Additional resources on time perspective therapy
Time Perspective Inventory
http://www.thetimeparadox.com/zimbardo-time-perspective-inventory/
This free online, automatically scored 61-question self-test will help you determine what your
past, present, and future time orientations are. You can compare your scores to the average
of other people’s and to the author’s “ideal” time perspective.
Time Cure: Overcoming PTSD with the New Psychology of Time Perspective Therapy.
(2012) Philip Zimbardo, Richard Sword, & Rosemary Sword. San Francisco,
California: John Wiley & Sons, Inc.
106
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
extends herself to others, she becomes more capable of receiving the gifts that others
have to offer. The tolerance, compassion, and love she grants to others begin to rebound
upon herself.”
83
Here are some of the ways transgender sexual assault survivors told FORGE
they healed:
84
I contacted GLBT organizations after the fact and I became an activist as a result
of police abuse. I have been doing activism for over 7 years now. They did not help
me at the time so I took matters into my own hands and got involved in change and
community support. Getting beat up and abused inspired me to work for change.
Showed them assholes!
I volunteered for Take Back the Night and other anti-violence organizations and
events, to help feel a sense of empowerment.
I am very involved in support group and educational services in my area. I do
outreach to schools, service providers, and do the quarterly education for first-re-
sponse teams at a local sexual assault response organization.
Note that you do not need to volunteer specifically with sexual assault survivors; virtually
any kind of volunteer work can be healing as it will connect you with others and give you
a sense of purpose and meaning. A national volunteer-matching clearinghouse is available
at http://www.volunteermatch.org/; you may also want to try doing a web search for your
geographic area and “volunteering” or “volunteer clearinghouse.”
Annotated bibliography of self-help books
There are literally hundreds of books on sexual assault and healing. The books in this
section are ones we feel may be particularly useful to trans, gender non-binary, and
gender non-conforming survivors.
83
Herman, Judith L. (1992). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror, pp. 209-216.
84
FORGE. (2004). “Sexual Violence in the Transgender Community Survey,” (n=265) (data has not been formally published).
Allen, Jon G. (2005). Coping with trauma: Hope through understanding (2nd edition).
Arlington, Virginia: American Psychiatric Publishing.
Some people hate workbooks and/or self-help books. If that describes you, you may
want to pick up this book, which focuses on helping the reader “understand” trauma.
Includes sections on foundations, effects of trauma, trauma-related psychiatric disorders,
and healing.
Boon, Suzette, Stelle, Kathy & van der hart, Onno. (2011). Coping with trauma-related
dissociation: Skills training for patients and therapists. New York, New York: W.W.
Norton & Company, Inc.
This book is especially good for anyone who has multiple personalities or distinct parts and/
or those who have problems with dissociation. However, a lot of its advice and exercises
would be useful to trauma survivors who do not experience dissociation.
107
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Cori, Jasmin Lee. (2008). Healing from trauma: A survivor’s guide to understanding
your symptoms and reclaiming your life. Philadelphia, Pennsylvania:
Da Capo Press.
This is one of the best self-help books we’ve seen for trauma survivors. The author is both
a therapist and a trauma survivor, and her book draws on both experiences. She addresses
the reader as “you,” so it’s an easy read for those who don’t see themselves in works
that talk about “men” and “women.” Although not exactly a workbook, each chapter does
include questions readers can ask themselves to help apply the chapter’s topics to their
own experience. This book contains one of the more complete discussions of various types
of body-based trauma therapies.
Davis, Laura. (1990). The courage to heal workbook: For women and men survivors of
child sexual abuse. New York, New York: HarperCollins Publishers, Inc.
If you want a self-help manual, this is a great place to start. Davis sets out a step-by-step
process for addressing sexual assault trauma, asking the reader many questions and
providing ample room to write the answers in the book.
Dayton, Tian. (1997). Heartwounds: The impact of unresolved trauma and grief on
relationships. Deerfield Beach, FL: Health Communications, Inc.
This is a particularly good self-help book for partners and partnered trauma survivors: the
major sections are loss and trauma; the effect of trauma on the personality; the effect of
trauma on relationships; transformation and healing through grief; and the personal journey,
which includes many self-help exercises.
Fradkin, Howard. (2012). Joining forces: Empowering male survivors to thrive,
Carlsbad, California: Hay House, Inc.
The author of this book is a co-founder of MaleSurvivor and helps run weekend recovery
workshops for men. This book tries to translate those materials and experiences to the
written page, with some success. Includes multiple commentaries from a selection of
survivors and their partners. Each chapter addresses a specific topic, so it’s possible to skip
around to what most calls you. Includes affirmations, some exercises, and t-shirts designed,
created, and annotated by survivors. Acknowledges the existence of female survivors, and
male survivors are of different sexual orientations, ages, and partnership structures.
Lew, Mike. (2004). Victims no longer: The classic guide for men recovering from sexual
child abuse (Second edition). New York, NY: HarperCollins.
Victims No Longer is the mirror “opposite” of The Courage to Heal: an excellent,
comprehensive look at many of the results of sexual abuse. Like Courage, No Longer is
written for one gender, although Lew is much better about acknowledging the existence of
female perpetrators than are Bass and Davis. If the focus on men doesn’t faze you, this is an
excellent book. Although the subtitle includes “Guide,” this is not a workbook and does not
include exercises. Rather, Lew tells you what he has learned from other (male) survivors.
McKay, Matthew, Wood, Jeffrey C., and Brantley, Jeffrey. (2007). The dialectical
behavior therapy skills workbook: Practical DBT exercises for learning mindfulness,
interpersonal effectiveness, emotion regulation and distress tolerance. Oakland,
California: New Harbinger Publications, Inc.
This is a very practical training manual and workbook.
108
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Najavits, Lisa M. (2002). Seeking safety: A treatment manual for PTSD and substance
abuse. New York, New York: The Guilford Press.
If you deal with both trauma and substance abuse, get this book! Although it is written as
a manual for therapists, it includes all the materials, worksheets, and homework for clients,
and can easily work as a self-help manual.
Naparstek, Belleruth. (2004). Invisible heroes: Survivors of trauma and how they heal,
New York, NY: Bantam Dell.
Belleruth Naperstek is the best healing imagery expert there is. This book contains word-for-
word scripts if you would like to tape your own healing meditations. She offers many, divided
into three stages of healing from trauma. The early part of the book explains how imagery
works with trauma survivors, and contains many stories. Extremely compassionate and
highly recommended.
Rosenbloom, Dena, Williams, Mary Beth, & Watkins, Barbara E. (2010). Life after
trauma: A workbook for healing (2nd edition). New York, New York:
The Guilford Press.
This is a very comprehensive handbook that has whole sections on basic trauma
information, coping, thinking things through, safety, trust, control, valuing yourself and
others, feeling close to others, and healing for the long term.
Shapiro, Francine. (2012). Getting past your past: Take control of your life with self-
help techniques from EMDR therapy. New York, NY: Rodale Inc.
This is an absolute must-read for people who are trying to heal themselves. Shapiro helps
you figure out what’s too complicated or dangerous to do on your own, but gives lots of
easy-to-understand techniques for helping yourself with many other outcomes. Perhaps
most importantly, she explains—in part through *many* examples—how memories affect
what’s happening in the present, which can be extremely helpful to trauma survivors who
don’t quite understand what the big deal is about “healing.”
109
forge-forward.org
>
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
8
Appendices
Appendix A:
If your assault just happened
If you were just recently sexually assaulted, you likely have pressing short term issues
you need to take care of and decisions you need to make. The majority of this guide
focuses on longer-term healing. We encourage you to access what you need from this
guide now—and keep it in mind for later review after your urgent needs are addressed.
Reach out
If there is someone you know and trust, consider reaching out to them as soon after the
assault as possible. For nearly every survivor, the sooner you can have support around
you, the better off you will be in both the short and long term.
Get a forensic exam?
You have the right to choose whether or not to have a forensic exam. If you were assaulted
within the last 72 hours, your body may still have evidence that could be collected
and used to prosecute your assailant(s). In many places, you can have a “rape evidence
kit” collected and decide later whether to involve the police, but this may not be the
case where you are. Call the National Sexual Assault Hotline (1-800-656-HOPE) or your
local hospital to find out the best place to go if you decide to pursue forensic evidence
collection. If you are going to have an exam done, try to avoid going to the bathroom,
bathing, changing clothes, and even eating and drinking, as all these activities can wash
away evidence. If possible, bring a complete change of clothes with you to the exam site
(usually an emergency room or hospital). These examinations can be very invasive and
upsetting all by themselves, and many times law enforcement is less than helpful. On the
PHOTO BY LEIGH HOUGHTALING
110
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
other hand, there is very little chance your assailant(s)
can be prosecuted if evidence is not collected.
Involve law enforcement?
You have the right to choose whether or not to involve
law enforcement. If you are in immediate danger
from your perpetrator, you may want to contact
law enforcement. Likewise, if you are considering
pressing charges or pursuing legal action against your
perpetrator, you may want to contact law enforcement.
Sexual assault victims are usually eligible for crime
victim compensation (which can pay for medical and
other expenses associated with the crime), however, in
order to qualify, you must report the crime to the police.
Many transgender survivors and sexual assault survivors
of all gender identities have found encounters with law
enforcement to be less than helpful.
Rally immediate support
Friends and loved ones can be a great source of support by helping, listening, and
just being with you, as can advocates accessed through rape crisis lines or LGBT
anti-violence programs. A companion or advocate can be particularly helpful if you are
pursuing evidence collection or interacting with the police. A trained advocate can advise
you about the process as well as help you with both emotional and practical concerns. As
soon as possible, start mobilizing emotional support for yourself.
Healing
Healing is a long-term goal. What you may want to find is “crisis counseling,” often
available at no charge from the local rape crisis hotline or sexual assault center. These
counselors may not be equipped to deal with any trans-related concerns or questions you
have, but they are trained about how to help sexual assault victims and their loved ones
get through the first few days and weeks.
This guide will be here for you whenever you need it.
PHOTO BY MIA NAKANO
111
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Appendix B:
If your current relationship is abusive
More than one-quarter (29%) of the transgender sexual assault survivors FORGE surveyed
in 2004 had been assaulted by their intimate partner, and another 20% said they had
been assaulted by a date. When we surveyed transgender people in 2011,
85
results
indicated that of the 1005 respondents, 29% of trans-feminine and 36% of trans-masculine
individuals had experienced domestic violence. In addition, statistics from studies
conducted by both FORGE and those researching the general public show that many
sexual assault survivors are re-victimized, often by their partners. This re-victimization
may or may not be sexual in nature; sexual assault survivors make up a large percentage
of victims of domestic violence.
How do you know if your relationship is abusive? The following has been adapted
from a webpage FORGE co-wrote. (http://www.rm2bsafe.org/index.php/familyfriends/
recognizing-unhealthy-relationships)
Warning signs of an unhealthy relationship:
PSYCHOLOGICAL ABUSE
Abuse can come in many forms. Even if an abuser doesn’t leave physical marks
on their partner, a relationship may still be abusive. Some people are emotionally
abusive. Emotional abuse can take many forms such as: making a survivor feel guilty,
blaming a survivor for their anger, having extreme mood swings, or denying the existence
of their relationship. The following example describes a case of emotional abuse.
David and Kyle, two out gay men, are both highly involved in the trans community.
David leads an LGBT teen group and Kyle participates in Pridefest meetings at the
local community center. The two men are known to be friends and begin dating.
While their closest friends know that they are dating, Kyle insists on keeping the
relationship a secret. At a recent event, Molly sees Kyle flirting with another man
while David is in the room. Molly asks Kyle about the relationship and David lets
her know that Kyle insists on keeping their relationship a secret and refuses to give
up dating other men.
HUMILIATION / LACK OF RESPECT
Lack of respect is another sign of an abusive relationship. An abusive partner can
demonstrate lack of respect by name calling, criticizing, belittling their partner’s thoughts
or looks, ignoring their partner, or being unavailable when their partner wants to do
something special. The example below highlights what lack of respect or humiliation
might look like in a relationship.
Sandy and Jesse have been dating for a year and a half. Sandy works as part of
the AIDS resource center. The AIDS resource center holds a major fundraiser every
March. The couple has invited a number of their friends over to their house to get
85
FORGE. (2011). “Assessing training needs to better serve transgender victims of sexual violence,” a survey approved by
the Morehouse School of Medicine’s Institutional Review Board. Data is the process of being analyzed.
112
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
ready for the event. Jesse finishes getting ready and sits in the living room to wait
while some of their other friends finish getting dressed. When Sandy comes out
Jesse says, “Are you really wearing that? You know that you don’t look good when
you dress like that! Why don’t you dress more butch?” An argument continues
regarding Sandy’s appearance.
CONTROLLING BEHAVIOR
Abuse can also take the form of an abuser tightly controlling what happens in their
relationship or in their partner’s life. Most forms of abuse involve some sort of controlling
behavior. This type of behavior may be a warning sign of other abuse in the future. A
controlling person might isolate their partner from friends and family, discourage a
survivor from being involved with trans- or survivor-focused groups, become jealous
easily, tell their partner what to wear or how to behave, use technology to stalk their
partner, monitor or take control of their Facebook pages, text or call constantly, or force
their partner to be out or to be closeted.
Tina just started dating Jason. Once a month Jason goes out to dinner on a Friday
night with his friends from work. On Thursday Jason reminded Tina that he would
not be able to hang out, because he is going out with friends after work. During
the dinner Friday night, Tina texts Jason ten times asking him what he is doing
and when he would be free to meet her.
THREATS/INTIMIDATION
Survivors don’t have to be hit or sexually assaulted to be abused. Abusers may use threats
to control their partner. Threatening a person without carrying out the threat is a form of
abuse. It is used to manipulate a survivor into doing what an abuser wants them to do.
An abuser may threaten to hurt themselves, hurt their partner, reveal a survivor’s trans
or LGB identity, or disclose their HIV status. An abuser may also scare their partner with
looks or gestures, demand time even when their partner is busy, or use violence or objects
to scare their partner.
Taylor is an out, straight, transgender man who is dating Jackie. Taylor wants
Jackie to move in with him and start dating more seriously. Jackie just ended
a 5-year relationship and does not want to move in with him right away. Taylor
threatens to kill himself by overdosing on pills if she does not agree to do what
he wants.
VIOLATES BOUNDARIES
Another way abusers attempt to control their partners is by violating their boundaries.
Abusers may read their partner’s diary, email, letters, or texts without permission. They
may constantly pressure their partner for sex when their partner is uninterested. They may
also constantly tease, make fun of, or pick on their partner even after being asked to stop.
Adam is a gay male who is in a relationship with Jay, a bisexual man. Adam is
jealous and suspicious of Jay’s female friends. Adam often says he is afraid that
Jay will leave him for a woman. After having a phone conversation with a female
co-worker Jay finds Adam going through the call history on his cell phone.
113
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Other Signs
Some relationships are unhealthy even if there are no major signs of abuse. Similarly,
some people engage in behaviors that may not be abusive, but are certainly unhealthy.
Signs that a person might be an unhealthy partner include: abusing alcohol or drugs and
using it as an excuse for negative behavior, having a history of troubled relationships,
treating pets poorly, being violent toward others, having a history of cheating on their
partner, or shaming their partner about their sexual orientation or gender identity.
Abusers often can seem wonderful when they are not engaging in abuse. Prior to and/
or after an episode of abuse, abusers may be sweet or apologetic. This periodic charming
and loving behavior might make it hard for a survivor to label other negative behavior
as abusive.
What behaviors might a survivor engage in?
There are some behaviors that a survivor might engage in as a result of being
abused. Sometimes people who have been abused make sacrifices like giving up friends,
activities, or ambitions due to a controlling partner. At times survivors blame themselves
or make excuses for their partner. A survivor might think “If only I hadn’t bugged my
abuser, they would not have gotten mad,” or “My abuser is only like this when they are
stressed or drinking.” A survivor might feel more insecure than they did prior to being
in the unhealthy relationship. They may rehearse what they will say to their abuser,
apologize often for their behavior, try to predict their partner’s mood, or find that
someone is expressing concerns about their relationship.
Trans-specific tactics
In addition to the kinds of tactics any abusive partner might engage in, both transgender
people and their partners (trans or non-trans alike) have additional vulnerabilities that
an abusive partner might exploit. See the two pages after this section, which reprints
a FORGE handout on trans-specific power and control tactics. (You can download the
Tactics separately at http://forge-forward.org/2013/04/power-and-control-tactics/)
Becoming safer
If your current partner makes you feel unsafe, you may want to consider strategies to
increase your safety. After the two page chart on trans-specific power and control tactics
is a reprint of FORGE’s “Safety Planning: A Guide for Transgender and Gender Non-
Conforming Individuals Who Are Experiencing Intimate Partner Violence,” which can help
you investigate and think through your options. (You can download the Safety Planning
guide directly by going to: http://forge-forward.org/wp-content/docs/safety-planning-
tool.pdf)
114
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trans-Specific Power and Control Tactics
http://forge-forward.org/2013/04/power-and-control-tactics/
TACTICS USED AGAINST
TRANS PARTNERS
TACTICS USED BY
TRANS PARTNERS
Safety.
Outing.
Disclosure.
Threatening to “out” you to
your employer, friends or
family members
Threatening to take the children
or turn them against you
Threatening to tell your family,
friends, employers that you aren’t
who you say you are (e.g. straight,
lesbian…)
Turning the children against you
Community
Attitudes
Ridiculing or belittling your identity
as bisexual, trans, femme, butch,
genderqueer…
Claiming they are more “politically
correct” and using their status as an
L, G, B, and/or T person against you
Stating you would harm the LGB
and/or T community if you exposed
what was happening
Ridiculing or belittling your identity
as bisexual, trans, femme, butch,
genderqueer…
Claiming they are more “politically
correct” and using their status
as an L, G, B, and/or T person
against you
Stating you would harm the LGB
and/or T community if you exposed
what was happening
Using “cisgender” as a slur
and insult
Gender
Stereotypes
(& Transphobia)
Telling you they thought you liked
“rough sex” or “this is how real
men/women like sex”
Declaring you are not a real
man/woman
Telling you that nobody will ever
love you
Telling you that you don’t deserve
better and/or would never find a
better partner
Claiming they know what’s best for
you, how you should dress or wear
makeup (or not), etc.
Claiming they are just being
“butch” or that “it’s the hormones”
(to explain their violent behavior)
Telling you that there is no way
to have safer sex with trans
bodies, so you’ll have to have
unprotected sex
Threatening suicide, especially
while reminding you of how many
trans people commit suicide
Demanding a greater share of
clothing/grooming funds because
their safety is at stake
Claiming they make a better or
more attractive man or woman
than you do
115
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Trans-Specific Power and Control Tactics
http://forge-forward.org/2013/04/power-and-control-tactics/
TACTICS USED AGAINST
TRANS PARTNERS
TACTICS USED BY
TRANS PARTNERS
Using or
Undermining
Identity
Using pronouns not preferred by you
or calling you “it”
Calling you pejorative name
Ridiculing how your body looks
Telling you that nobody would
believe you because you’re
transgender
Accusing you of not allowing hir to
have a “proper adolescence”
Claiming that your identity
“undermines” or is “disrespectful”
to theirs
Stating that trans people are
superior because they don’t limit
themselves to a restrictive binary
and sex role stereotypes
Violating
Boundaries
Eroticizing/fetishizing your body
against your will
Touching parts of your body you
don’t want touched, or using terms
about your body they know you
find offensive
Forbidding you to talk to others
about transgender topics
Denying that you are affected by
transition or by being partnered
with a trans person
Charging you with “not being
supportive” if you ask to discuss
questions of transitioning timing
and/or expense
Forbidding you to talk to others
about transgender topics
Restricting
Access
Denying access to medical
treatment or hormones or coercing
you to not pursue medical treatment
Hiding or throwing away
hormones, clothes, prosthetics or
other trans-specific items
Negating your personal decisions
Controlling finances to not allow
for purchase of hormones, surgery,
clothes, make up, prosthetics
Not allowing you to talk to or see
your friends
Denying access to parts of the
house or apartment (where
hormones or clothes may
be stored)
Negating your personal decisions
Controlling finances in order to
prioritize paying for hormones,
surgery, trans-related items
(even if risking not paying for
rent, food or mutual expenses)
116
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Safety Planning: A Guide for Transgender and
Gender Non-Conforming Individuals Who Are
Experiencing Intimate Partner Violence
About This Document
There are many sections to this safety planning document in order to provide a more
comprehensive tool. It may feel long and overwhelming. Consider reading only a few
sections at a time. Remember also that any step you take to improve your safety is
important; you do not need to take them all.
Ideally, people using this Safety Planning tool should write out their answers and notes,
to help solidify their thinking and so they can access help remembering their plans if they
are under stress, such as during an episode of violence. HOWEVER, it is EXTREMELY
important that these notes—whether they be on paper or electronic—NOT be left
anywhere where an abuser could find them. Possible places where it may be safe to make
and leave notes include: your computer at work; on a thumb drive you always carry with
you or hide at a friend’s house, a public (i.e., library) computer where you can store the
answers “in the cloud”
86
under a password your abuser doesn’t know; a friend’s computer;
or at a helping agency or professional’s office, such as your therapist’s office or your local
domestic violence program. It is also advised that any lists of friends’ contacts, bank
accounts, service options, etc. that you generate be kept separately, to minimize the risks
should one fall into your abuser’s hands.
The Purpose of Safety Planning
There are some very common, but mistaken, beliefs about intimate partner violence (IPV).
Some of the primary myths include:
The victim
87
believes it is their/zir/his/her behavior that causes the abuser
88
to
“lose control.” This belief is often fostered by the abuser, who usually blames
the victim for “provoking” the victim. That means the abuser doesn’t have to
take responsibility for their abusive actions. It also, perversely, helps the victim
imagine they
89
/ze/he/she has some control over the situation.
86
GoogleDrive, Dropbox, SugarSync and other cloud-based providers offer small amounts of free storage.
87
“Victim” may be a word that doesn’t resonate with you. This document uses victim to include anyone who is currently or
previously experiencing abuse or violence by their partner (from dating partners or long term relationships).
88
“Abuser” may also not be a word that feels comfortable or relatable. Throughout this document, the use of “abuser” is a
date or partner who is exhibiting abusive behavior, power, control, or violence against you.
89
To be inclusive of all genders of victims and abusers, this document will list multiple pronouns or use “they” as a
singular pronoun.
Click on the link below to download and/or print the
standalone PDF version of this safety planning tool:
http://forge-forward.org/wp-content/docs/safety-planning-tool.pdf

117
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
The victim and/or abuser may believe that relationship violence is normal and
to be expected.
The victim and/or abuser may believe that the violence was a one-time
occurrence that will not be repeated.
The victim and/or abuser may believe that it’s only domestic violence if it’s a
man abusing a woman.
Through safety planning, friends, family, advocates, and concerned professionals can
help victims understand that these beliefs are dangerous myths and help the victim focus
on where they/ze/he/she actually does have power and control: planning for and taking
concrete actions that can enhance their/zir//his/her safety.
What is Intimate Partner Violence (IPV)?
IPV is known by many names, including domestic violence, family violence,
abuse, and battering. While most people think IPV involves physical violence,
it can also include forced sexual activity, financial exploitation, stalking,
blackmail, coercion, isolation, harassment, and emotional abuse. The line
between normal disagreements or tension between within a relationship and
IPV may be subtle. Many people say that it is IPV when one person routinely
tries to control the other through violence, threats, and manipulation. If you
feel afraid at home or when you are with your partner, there’s a good chance
you are experiencing IPV.
Another sign of IPV is realizing that your partner has slowly managed to isolate you,
separating you from your normal supports, activities, and friendships. Abusers tend to
do this to make their victims more dependent on them, and to lower the chances that the
victim will decide to leave. A third possible sign of IPV is realizing that your partner has
made you feel chronically ashamed of yourself or worthless.
Some abusive relationships will only contain one or two of these components, while
other relationships will have many, complicated, forms of abuse woven throughout
multiple aspects of their relationship dynamic. Any amount of abusive behavior is abuse.
You deserve to access support that will help you live without abuse. Everyone deserves
relationships that are free from abuse of all kinds.
How Often Does IPV Occur?
IPV is very common. A lot of research indicates that roughly 1 in every 4 intimate
relationships—be they heterosexual or lesbian, gay, or bisexual; people who are
transgender, gender nonconforming, or non-transgender; people of any race, age, level
of disability, income level, religion—experiences IPV. Despite how common it is, it is not
something you have to live with.
Many people grew up in abusive households and never learned that living together
peacefully is normal and something they should have. Transgender
90
people, often having
90
FORGE uses “trans,” “transgender” and “gender non-conforming” as very large umbrella terms that are fully inclusive of
hundreds of gender identities, histories, experiences, and expressions. Although this document will primarily use the terms
“trans” and “transgender,” FORGE includes and presumes that many individuals will more closely align with terms such
as genderqueer, gender fluid, bi-gender, omni-gender, two-spirit, androgynous, femme, butch, transsexual, crossdresser,
woman of transsexual experience, man of transsexual history, trans man, trans woman, boi, T-girl, stud, aggressor, and
many other terms.
Approximately
1 in 4
relationships
experience IPV.
118
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
grown up subject to others’ hurtful name-calling and/or abuse because they are gender
non-conforming, seem particularly likely to believe that they are lucky to ever find love,
even if that love turns violent. No person should have to be in a relationship that is
abusive. Transgender people can and should have loving partnerships that are free from
violence or coercion.
Can Abusers Change?
Some abusers do eventually learn how to have an intimate relationship without hurting
or trying to control their partner. However, this is not an easy process and almost never
happens after an abuser simply promises they will never be violent again. Instead, violent
or coercive partners have to unlearn habits of thought and behavior that lead them to
try to control their partners’ behavior rather than their own behavior and emotions.
Oftentimes, they have to work through and heal their own experiences of having been
abused. Then they have to learn and practice new interpersonal skills to a point where
even under substantial stress, they are able to control their emotions and behavior, which
result in making choices that are healthy for both partners. Making these changes takes a
lot of time and effort, and usually requires therapy or other professional assistance.
Some domestic violence advocates urge partners who are being harmed to not attend
couples counseling with their abuser. Their fears include:
the therapist may agree with the abuser that the victim needs to make all the
changes;
the victim may say something in therapy the abuser may use against him or her
later; and
the abuser may use therapy as just another setting in which to make the victim
feel bad.
However, you know your abuser better than anyone else, and only you can decide if
couples counseling will be safe for you and might be helpful to both you and your partner.
For a variety of reasons, many people who experience IPV choose to stay with their
partner, either temporarily or permanently. (Individuals who experience harm from their
partners also frequently leave and then return, sometimes more than once before they
are able to permanently stay away.) If this is true for you, you can and should think about
how you can lower the chances of you and/or your children and pets being harmed by
your abusive partner. Safety planning can help you do this.
What Is a Safety Plan?
91
A Safety Plan is a set of actions you can take if you stay with the abuser, while preparing
to leave the abuser, and/or after you have left. This document will help you identify ways of
being more prepared to keep yourself (and your children and pets, if you have them) safe.
Work through the sections in this safety planning tool that are relevant to you—by
yourself, or ideally with a friend, advocate or provider.
91
FORGE is grateful for other LGBTQ organizations who have constructed safety plans. Some content in this document has
been adopted from the online Safety Planning guide of the Gay Men’s Domestic Violence Project (http://gmdvp.org/domes-
tic-violence/safety-planning) and the “Intimate Partner Violence Safety Plan” developed by Outfront Minnesota (http://www.
outfront.org/programs/avp).
119
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Remember that a Safety Plan can’t prevent abuse, because that’s under the control of the
abusive partner (no matter how much they claim you provoked it). But if you:
Plan what to do ahead of time;
Prepare to carry out your plan; and
Rehearse the steps you need to take…
you are far more likely to be successful at avoiding the worst.
Note that the suggestions in this Safety Plan are written for a wide range of situations.
You know your situation best, so make sure you think through what is best for you and
make whatever changes or additions feel right to you.
Laying the Groundwork
You can’t always predict an incidence of violence, and many victims find that they are
either gradually or suddenly being subjected to much worse violence than they were at
first. For both these reasons, seriously consider laying important groundwork that may
later prove lifesaving, even if you think your current situation doesn’t warrant such
measures.
IDENTIFY SERVICE AND SUPPORT OPTIONS
Find out what domestic violence services are offered in your area, and what their phone
numbers are. There are over 40 LGBTQ
92
anti-violence programs (AVPs) across the
country. AVPs exist to support people who have or are experiencing abuse or assault.
They work hard to identify local, state and regional resources for LGBTQ people who have
experienced violence and need help. You can find a list of the AVPs at http://www.avp.
org/storage/documents/NCAVP_member_and_affiliate_list_October_2012.pdf). If one is
near you (in your state or region), include them first on your resource list.
Identify other local domestic violence services. One place to start looking for referrals is
The National Domestic Violence Hotline at 1-800-799-SAFE (7233). (Their TTY number is
1-800-787-3224).
When you are ready to call an AVP, the National Domestic Violence Hotline, or any other
DV program, call them from a safe place (see “Become aware of your electronic trail,”
below) and find out what their policies are about serving transgender people and what
services, if any, they may be able to offer you while you remain with your abuser and/or if
you choose to leave.
Start a dated journal of your abuse.
Include threats, stalking, and destruction of property. Add photos if you can. This
information will be useful in securing a restraining order or any other legal action you
may need to take later on. Obviously, it is critical that this journal be kept somewhere
where your abuser will never find it. Consider renting a safety deposit box to keep hard
copies of journal entries or photos. A second relatively secure option is to use a password
protected cloud-based electronic file service, so no electronic file is on your computer’s
hard drive, and no photos are on your phone or hard drive.
92
LGBTQ = Lesbian, Gay, Bisexual, Transgender, Queer/Questioning
120
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Begin recruiting supporters and develop code words. Transgender people may need
to think very carefully about who they know who they can trust to keep confidential
information from the abuser. Such individuals may be friends (particularly if they are
not also friends with the abuser), neighbors, co-workers, or other people you know. When
you identify such individuals, begin sharing your situation and ask them specifically if
they would be willing to help you if the situation got worse. Set up a code word or phrase
that will tell them you are in danger and need them to call for help (make sure you are
explicit about what kind of help you want them to call). Find out if they would be able to
offer other concrete help such as housing you in an emergency, storing duplicate copies of
important papers, or keeping your safety bag of packed clothes/supplies.
Stock your wallet and its backup
Keep your wallet with important identification, credit cards, and other material with
you at all times. Make copies of critical documents and account numbers and keep them
someplace safe, such as a friend’s house, at work, or in a password protected computer
file stored outside of the house. A following list includes most of the documents you might
need if you leave for a lengthy period of time:
Driver’s license/state identification card, car registration, and proof
of insurance
Work ID/work permit
Health care insurance or Medicaid/Medicare ID cards
Social Security card
Birth certificate
Passport
Green card, visa, or other immigration papers
Carry letter if your identification has not been completely updated
Surgeon’s letter if your identification has not been completely updated
Court order for name/gender change
Copies of any restraining order, if you have obtained one
Welfare identification
Lease or home deed, house or renters insurance information
Children’s identification/adoption records
Paternity or custody records
School and vaccination records (self and children)
Marriage license or divorce papers
Medical records
Other court documents
List of possible service organizations (see Laying the Groundwork)
List of friends’ and therapist’s addresses and phone numbers
121
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
It is common for abusers to become angry and increase the level of violence when their
partner leaves, even if they intend to come back. Leaving is therefore a very dangerous
time for victims. Begin planning for this eventuality by developing two useful habits.
1. Become aware of your electronic trail. With many people carrying cell phones that
can be tracked by GPS and using computers that keep traces of users’ searches and
communications, it is becoming increasingly easy for knowledgeable individuals who
wish to control or stalk their partners to track down where their victims have gone.
Your travels may be traceable through credit card bills, debit card statements, your
cell phone, and, of course, your social media updates. If you search for shelters on
your home computer or a tablet you leave behind, your abuser may
be able to learn where you might be. Don’t trust your cell phone to
keep all of your friends’ and resources’ phone numbers (it might
be left behind or broken), but don’t leave a paper or computerized
directory around where your abuser can find it, either. Make sure
you have multiple ways of accessing important numbers, and that
they are kept in places your abuser doesn’t have access to, like
at friends’ houses, work, or electronic storage not accessed by
computers/phones at home. Whenever possible, do your resource
scouting at public computers and/or public phones, or borrow a
friend’s. Hide critical computerized information behind passwords
your abuser would never guess, not your usual ones.
2. Develop habits that regularly take you out of the home. Develop a regular habit that
takes you out of the house, such as daily taking out the garbage, going for a walk,
or getting a newspaper. This activity can be used as an excuse to leave if you have
warning that abuse is about to occur. Or if you are planning to leave, the activity can
be a safe way to get out of the home.
Staying Safe at Home
SCOUT OUT YOUR HOME
Sometimes when it’s not possible to avoid a peak violent episode, a victim can still
maneuver that outburst to a safer spot.
You want to avoid:
Being cornered in closets, small spaces, or bathrooms;
Rooms where weapons (guns) or potential weapons (knives, fireplace tools, or
fire extinguishers) are stored; and
Stairways, unless you are using them to flee the home.
You do want:
Rooms with a phone and/or a door or window you can escape out of.
Try not to have your abuser standing between you and an exit. Think ahead. Before an
incident, practice how to get out. Teach the escape plan to your children, if you have any. If
you live in a tall building, consider what elevators, stairwells, or fire escapes you can use.
CULTIVATE 2 HABITS:
1. Become aware of
your electronic trail.
2. Develop habits that
regularly take you
out of the home.
122
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
RECRUIT YOUR NEIGHBORS
While some trans and gender non-conforming people do not feel like calling the police
is helpful, others do. If you do want the police called when you are indanger, consider
talking to trustworthy neighbors and asking them to call the police if they hear
suspicious noises coming from your house. You may also want to develop a code phrase or
visible sign (like a towel hung in a window) that will signal them that you are in trouble
and want them to call the police.
Emergency Safety Bag
Abuse can get worse over time or quite suddenly. If you have ever felt in danger from your
abuser, consider preparing an “emergency safety bag” that can save you precious time
if you suddenly need to leave your home. This bag should be stored in a safe and easily
accessible place, such as a friend’s or family member’s home, at work, in a car trunk, or
any place to which the abuser will not have access.
POSSIBLE CONTENTS INCLUDE:
Finances
Cash
Credit cards and ATM cards
93
Checks
94
Essential resources
Keys to car, house, work, safety deposit/post office boxes
List of possible service organizations (see Laying the Groundwork)
List of friends’ and therapist’s addresses and phone numbers
Spare glasses or contact lenses
Medications, prescriptions, contact information for doctor(s) and pharmacy
Cell phone and charger
95
Any assistive devices you need
Photos of the abuser
Your journal of abuse, if you do not already store it elsewhere, and/or photos of
injuries your partner has inflicted on you
Public transportation schedule
93
If your credit card and bank charges statements go to an address you share with the abuser, they can be used by the
abuser to trace where you are. Ideally, change the address where these statements go so they do not fall into your abuser’s
hands. If the accounts are in both names, the abusive partner can still request access to the account information from the
bank. It is safest to consider using only cash and/or opening new accounts if you leave.
94
See above.
95
Your cell phone may have a GPS that your abuser can use to track you. You definitely do not want to leave your cell phone
where your abuser has access to it—it will contain too much information about your friends and contacts—but it may be
safer for you to stash it someplace after you leave and purchase a new, limited-use phone. You can also ask a domestic
violence program to assist you in obtaining a free cell phone that can only dial 911 in emergencies.
123
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Identification and paperwork
Driver’s license/state identification card, car registration, and proof of insurance
Work ID/work permit
Carry letter if your identification has not been completely updated
Surgeon’s letter if your identification has not been completely updated
Health care insurance or Medicaid/Medicare ID cards
Social Security card
Birth certificate
Passport
Green card, visa, or other immigration papers
Court order for name/change change
Copies of any restraining order, if you have obtained one
Welfare identification
Lease or home deed, house or renters insurance information
Children’s identification/adoption records
Paternity or custody records
School and vaccination records (self and children)
Marriage license or divorce papers
Medical records
Other court documents
Hormones and prosthetics
Hormones, prescriptions, contact information for doctor and pharmacy
Binders
Stand to urinate devices
Packies or penile prosthetics
Wigs
Gaffing materials
Shaving/plucking tools
Breast/hip forms or other feminizing prosthetics
Makeup
Clothing
Change of clothes and shoes
Note: if you have difficulty finding clothes and/or shoes in your size, consider
buying extra items when you find them and asking friends or colleagues to keep
them for you. Also add your favorite clothing sources to the list of addresses
and phone numbers you take with you.
124
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Other things to consider taking
Jewelry, personal photographs, and other valuables
Personal items that bring you comfort or peace
Small saleable items
Items of special sentimental value
If you do leave and you have the time, clear the browser history on any computer left
where the abuser can access it.
Note that if you want to leave, you do not have to wait for the violence to escalate or
something terrible to happen. It’s ok for you to go whenever you want to or can.
Financial Planning
Many transgender people are living paycheck (or benefits check) to paycheck and find
it extremely difficult to put aside money that can be used in an emergency. Whatever
you can put aside, however, even if it is just the change from your pocket every day, will
increase your options should the abuse you have experienced gets worse.
Just as important, you can take some steps now to make you safer in
the future. Remember that account information now typically includes
all uses of your debit card as well as checks, and can be accessed online
as well as by mail and in person; if your abuser shares your account(s)
or even simply knows your passwords, they/ze/he/she may be able to
access information that might help track down where you are if you
leave. Therefore, if possible, open a new account that does not have your
abuser’s name on it, and have the statements sent to an address you do
not share with the abuser (such as a post office box). (Alternatively, find
an online bank that doesn’t send statements at all. Make sure, however,
that you use a password your abuser doesn’t know and wouldn’t guess.)
Use only this account if you leave your abuser.
Also pay attention to what happens to paperwork concerning any large asset you both
own, such as a house or other property. Abusers may work to put assets in their names
only, often offering very convincing reasons why this is a good idea (tax benefits, avoiding
potential problems with antagonistic family members, avoiding the confusion that might
result if you are planning to change your name, etc.). Given how few transgender people
are protected by marriage and/or community property laws, allowing any asset to be
held only in your abuser’s name may mean you will lose whatever equity you put into the
asset. Make sure you consult a trans-knowledgeable lawyer so that assets are held in a
way that protects you and your interests.
If you hold any joint credit cards with your abuser, find out which ones you are liable
for and make sure you monitor how much your abuser charges to them. You can
request one free credit report every 12 months by contacting Central Source at www.
annualcreditreport.com or calling them at 877-FACT-ACT (322-8228). You may then need to
call each credit card issuer to determine how the card is held and what your liability is.
If you need to start disentangling yourself from debts your abuser should be responsible
for, contact your local credit counseling agency, domestic violence program, or United Way
for a referral in your area that can help you begin the process. If you do leave and end up
Open an account
in your name only.
Ensure statements and
notices do not go to an
address you share with
the abuser.
125
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
responsible for credit card debt, be sure to contact the issuing company or companies to
discuss the situation and see if they will suspend late fees or interest, let you negotiate
lower payments, or otherwise accommodate your situation. Any proactive effort you make
to address debt problems will result in a better outcome than simply abandoning those
accounts and financial responsibilities.
Safe Havens
Transgender people who experience domestic abuse have fewer options for finding
safety than most non-transgender (female) victims. Most domestic violence shelters do
not house men (non-transgender or transgender), and many will not accept transgender
women, either. Some will provide hotel vouchers, but these are typically only for a
very few nights. If you live in an area with an LGBTQ anti-violence program (a list is
available at http://www.avp.org/storage/documents/NCAVP_member_and_affiliate_list_
October_2012.pdf), contact them first, as they may know who might serve you and will
advise and advocate for you no matter what other services you may be able to access. If
there is no local AVP, you can call the National Domestic Violence Hotline at 1-800-799-
SAFE (7233) for a list of local referrals. (Their TTY number is 1-800-787-3224).
Every shelter has a different policy about who they house and what specific requirements
need to be met. For example, there is no consensus among shelters as to whether
transwomen who live in a female gender role, have identification in their current name
and female gender will be allowed access into a women-only shelter. There are also pros
and cons about if a transgender person should disclose their trans status to shelter staff
(prior to or after being accepted into shelter). Some individuals have found it safer to have
disclosed, others have noted it has increased their risk of discrimination or even ability
to access shelter services. You will need to make the decision about whether or not you
disclose your transgender status/history based on your own values, safety considerations,
and what other options, if any, you have.
Options beyond public shelters may be limited, as well. Family members may be
estranged, and friends may feel divided loyalties if they are also friends with the abuser.
If you need to get out but can’t find a place to stay, hospitals, airports, bus terminals,
convenience stores, and some restaurants are often open 24 hours. If you choose to go to
an emergency room, you do not need to go into detail with the staff about your situation,
but alerting a triage nurse that you are in flight from your abuser will allow you access to
some assistance. Most emergency rooms have social workers on call who are available to
help secure shelter, work with police, and contact family or friends. You will also be safe,
while you are at the emergency room, which may buy you some time to consider your next
steps. If you wish to remain anonymous and/or not contact the police or try to enter an
emergency shelter (which are often unprepared to shelter transgender people and/or keep
trans people safe), simply ask the triage nurse if you can stay in the waiting room because
you are not safe on the street.
Obviously, LGBTQ community centers, transgender support groups, service organizations,
and social groups may be unsafe if you leave your abuser and your abuser frequents
these settings, as well, or knows that you do. Consider calling ahead and discussing the
situation with staff members to problem-solve and/or make emergency plans in case your
abuser should seek you out at these sites.
126
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Safety in Your New Place
Abusers tend to be very emotionally tied to their victims, and frequently attempt to find
them to “bring them back” if or when they leave. Here are some ways to increase your
safety after you have relocated. (If you relocate to a domestic violence shelter, the staff
can also help you think about how to stay safe.)
Consider getting a restraining order. If you have not previously done so, now
would be a very good time to think about getting a restraining order. See the
“Restraining Order” section for more information.
Recruit allies. Give neighbors, any security guards, workplace security or
colleagues, landlord or rental property manager and friends a picture of your
abuser, tell them that the abuser does not live with you, and ask them to call the
police if they see them/zir/him/her near your home. If you have a restraining
order against your abuser, by all means share copies of that with others, as it
may make them realize the seriousness of your situation and encourage them to
help you. Make sure that friends and family members know to never give your
new address to the abuser.
Revisit your safety plan and repack your emergency safety bag. Now that you
have new surroundings, develop and rehearse a safety plan in the event the
abuser shows up at your new home, including an escape route and where you
would go in an emergency.
Repack an emergency safety bag in case you need to leave suddenly.
Install home security measures. Add a peephole to outside doors and increase
outside lighting if appropriate. Consider an alarm system, security cameras, as
well as a smoke alarm and fire extinguishers. Make sure all windows have locks
or window bars to prevent them from opening from the outside. If your outside
doors are wood, consider replacing them with metal doors. Purchase home rope
ladders to be used for escape from a second floor window.
Stop your electronic trails. Change all passwords and PIN numbers, such as on
telephones, ATMs, computers, etc. If you have any kind of credit card, bank, or
cell phone statements going to the abuser’s home, change those immediately
by closing the accounts and reopening new ones. If your abuser may be able
to track you using the GPS on your cell phone, discontinue using that phone
and obtain a new phone and cell phone plan, which might be a limited-use
one. Change to an unlisted number. If you cannot afford another phone and
cannot borrow one from someone, consider asking police or a domestic violence
program if they can give you a free 911 phone that will at least allow you to
call police in an emergency. If you are on government assistance programs, you
may qualify for a free cell phone with 240 minutes per month through SafeLink
(http://www.safelinkwireless.com). An additional benefit of this program is that
they don’t have billing statements or require a credit check.
If you change your address with the department of motor vehicles, be sure to
ask them to use a number other than your Social Security number to identify
you, and ask them to code your address to keep it confidential. (You may have
to explain that you have a pursuing abuser who you need to shield your new
address from.) If your abuser seems to know where you go, there is a possibility

127
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
that they/ze/he/she may have placed a GPS device on your car or somewhere in
your possessions. Carefully go through all your belongings and have your car
inspected to see if you can find and then destroy or disable any such device.
Screen incoming and outgoing calls. Use caller ID and voice mail or answering
machines to avoid accidentally answering a call from your abuser. If you want
to try to block calls coming from telephone numbers you know your abuser
might use, read a how-to guide at http://electronics.howstuffworks.com/
blocking-incoming-call.htm. To limit how many people know your new number
(and can therefore accidentally share it with your abuser), start all calls by
dialing *67 before the number, so that the caller’s phone will display only
“Blocked Number.”
Keep records of abuser attempts to contact you. Keep copies of all emails and
phone messages and logs of all of your abuser’s attempts to contact you. These
may be useful if further legal efforts are necessary.
Safety on the Job and In Public
Recruit allies. Abusers commonly come to the workplaces of victims who have
left them. If your company or building has security personnel, give them a
photograph and name of the abuser and tell them you are not interested in
speaking with them/zir/him/her. If you have a restraining order, give security a
copy and tell them to call police if the abuser shows up. You may want to do the
same with your Human Resources department and/or supervisor. If your abuser
has visited your workplace on a friendly basis in the past, you may need to
inform your co-workers about your situation and ask them to help. If possible,
have someone screen your calls at work, especially if your workplace does not
have caller ID.
Create a workplace safety plan. As you did with your home, scout out your
workplace to identify where you will go and how you will get help if your
abuser shows up. You may need to recruit help from co-workers. Check if
your workplace has policies regarding domestic violence and/or workplace
violence and remind receptionists not to give out your home address or
telephone number to anyone other than authorized individuals. If you encounter
resistance from your supervisor or co-workers, consult with a domestic
violence program or attorney to see what laws protect you.
Vary your route to and from work. Use a variety of routes and times to arrive
and depart work, if you can. Travel with others when possible. Rehearse a safety
plan in the event that something were to happen on the way to or from work.
If you will be leaving after dark or working late, try to move your car closer to
the entrance during lunch or a break, and if possible, leave the building with a
co-worker. If you commute by bus, consider getting off at a different stop than
your abuser might expect, or only get off when other people are exiting as well.
Vary your other routines. Consider switching your usual grocery store, bank
branch, etc. Go at times that are different from what you habitually did when
you were partnered with the abuser. Arrange for direct deposit, or ask someone
to make deposits for you.
128
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Orders of Protection
All states permit some people to obtain a legal order of protection (also called restraining
order, a “stay away” order, and other names) against someone who threatens them.
However, state laws differ and some do not cover same-sex couples and/or people with
varying household and legal arrangements. You can do an initial check of whether your
state’s domestic violence order of protection law may cover your situation by checking the
chart at http://www.americanbar.org/content/dam/aba/migrated/domviol/pdfs/dv_cpo_
chart.authcheckdam.pdf.
Although procedures for obtaining an order of protection vary from state to state, they
all involve contact with the court and, possibly, law enforcement, and some trans people
therefore do not wish to try to obtain one. It is also true that the court may not grant
you the order, and that the abuser may not obey the order even if it is granted. However,
having an order of protection may help get you faster and more cooperative help from
law enforcement and other security personnel if your abuser does show up at your home
or workplace.
A general description of orders of protection and state-specific information is available
at http://www.womenslaw.org/laws_state_type.php?statelaw_name=Restraining%20
Orders&state_code=GE (note that some descriptions only describe abusers as “he” which
may not correspond with your situation).
Most LGBTQ anti-violence programs (a list is available at http://www.avp.org/storage/
documents/NCAVP_member_and_affiliate_list_October_2012.pdf), and most domestic
violence programs (The National Domestic Violence Hotline at 1-800-799-SAFE (7233) can
give you local referrals; their TTY number is 1-800-787-3224) can provide advocates and/
or advice on how to file for a protective order in your jurisdiction.
If you obtain an order, make sure it is listed in the registries of counties where you live,
work, and travel by calling the Clerk of the Court and/or the sheriff’s office for each
county. Make copies of your order and keep them at work, in your car, and on your
person. Give copies to security personnel at home and work.
Protecting Children and Pets
If you have children living with you, they are almost invariably already
aware of your partner’s anger and/or abuse. They will most likely be less
afraid, not more, if you teach them what they can do when you are abused
and/or they are afraid.
Therefore, teach them not to get in the middle of a fight between you and
your abuser. Develop a signal you can use if you want them to summon help
or call 911. Make sure they know their own names, addresses, and phone
numbers, and teach them how to call 911 and what to say. If you do not want
them calling the police, teach them who else to call. Teach them about where
to go to be safer during an incident, based on whether your abuser is likely to go
after them as well, or will concentrate on you. You may want to teach them to run to
a neighbor’s house or nearby public place. Tell them how to call you (including making
a collect call) if your abuser takes them somewhere without your knowledge or consent.
If your children are very young or liable to get confused in an emergency, prepare a
laminated card for them to carry with important information on it. Make sure your
PHOTO BY LEIGH HOUGHTALING

129
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
children know what other adults you trust and what information you do not want shared
with others.
Make sure that the people who care for your children—teachers and school
administrators, day care staff, babysitters, Sunday school teachers, and others—know
who has permission to pick up your children, and give them a copy of any restraining
order. Make sure the school or daycare knows not to give your address and phone number
to anyone, and set up a password so they can be sure it is you on the phone when you call
for information. Make sure your children know who to tell at school if they see the abuser.
If you have pets, you will need to make plans for them in case you need to or decide to
leave. Some shelters will temporarily board the pets of people who are fleeing domestic
violence, so call your local shelter ahead of time to find out if this is a possibility for
you. Perhaps a friend or relative who cannot shelter you would be willing to shelter your
pet(s). Your vet may even be willing to donate some boarding time if you let them know the
reason and how soon you think you can make alternative arrangements.
Emotional Support
A common hallmark of domestic violence is that the victim has become isolated from
other people. This may have happened slowly and subtly, without your conscious
awareness, or it may be clear that your abuser is trying to control who you see. Either
way, it is important to recognize that everyone needs other people, and that if you are
isolated, you need to take steps to bring more people into your life. This may be by
attending support groups, volunteering in places where you work with other people, or by
reaching out to people who are already around you, like coworkers. Remember that while
some people prefer to pretend domestic violence doesn’t exist, 1 in 4 people have been in
a situation similar to what you are experiencing. You are not alone, and you need others’
input to help you stay safe and sane if you are living with an abusive partner or have just
left one.
Domestic violence programs and LGBTQ anti-violence programs often have emotional
support services at no cost. Ask about support groups that are open to any gender,
therapists, social workers, or other supports that can connect you with others.
This safety planning guide project was supported by Grant No. 2011-TA-AX-K121
awarded by the Office on Violence Against Women, U.S. Department of Justice. The
opinions, findings, conclusions, and recommendations expressed in this publication /
program / exhibition are those of the author(s) and do not necessarily reflect the views of
the Department of Justice, Office on Violence Against Women.
130
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
Appendix C: New non-discrimination
protections for trans people
Due to persistent and effective lobbying, a strong coalition, and maybe some
elements of luck and timing, the 2013 Reauthorization of the Violence
Against Women Act (VAWA)—the federal program that funnels around
$400 million dollars a year into programs addressing sexual assault,
domestic violence, stalking, and dating violence—included a
groundbreaking new nondiscrimination provision.
The 2013 VAWA Reauthorization included, for the first
time in the history of federal laws, a provision forbidding
discrimination based on “gender identity.”
96
Specifically, what
has been labeled “the New Civil Rights Provision” added
sexual orientation and gender identity to VAWA’s prohibition
against discrimination:
No person in the United States shall, on the basis of ac-
tual or perceived race, color, religion, national origin, sex,
gender identity (as defined in paragraph 249(c)(4) of title
18, United State Code), sexual orientation, or disability, be
excluded from participation in, be denied the benefits of, or
be subjected to discrimination under any program or activity
funded in whole or in part with funds made available under the
Violence Against Women Act of 1994 (title IV of Public Law 103-
322; 108 Stat. 1902), the Violence Against Women Act 2000 (division B
of Public Law 106-386; 114 Stat. 1491), the Violence Against Women and
Department of Justice Reauthorization Act of 2005 (title IX of Public Law 109-
162; 119 Stat. 3080), the Violence Against Women Reauthorization Act of 2013, and
any other program or activity funded in whole or in part with funds appropriated for
grants, cooperative agreements, and other assistance administered by the Office on
Violence Against Women.
Unlike many new non-discrimination statutes, the new VAWA law has the potential to
remodel the system it affects—in this case, the nation’s sexual assault and domestic
violence service system. VAWA’s name itself demonstrates who the system was originally
designed for: women. Many programs have not served men at all, or have provided men
with vastly inferior separate services, such as a limited number of hotel vouchers instead
of accepting them into a group shelter where more integrated and supportive services
are provided. Transgender people have routinely reported being denied services and even
denigrated when they tried to access services. Although the new law may allow some sex-
or gender-segregated services to exist, the exemption is quite narrow: sex segregation
or sex-specific programming is permitted only when it is “necessary to the essential
operation of a program.” Depending on how the law is interpreted and implemented,
this provision, could result in substantial integration of nearly all programs, including
emergency shelters for victims of domestic violence and sexual assault.
96
“Gender identity” was referenced in only one previous federal law, the 2009 Matthew Shepard and James Byrd, Jr. Hate
Crimes Prevention Act.
PHOTO BY LEIGH HOUGHTALING
131
forge-forward.org
A SELF-HELP GUIDE TO HEALING AND UNDERSTANDING
As of October 1, 2013, the non-discrimination provisions in the re-authorized VAWA take
effect. Because the re-authorized VAWA is inclusive of LGBT individuals, survivors who
are lesbian, gay, bisexual or transgender (both trans-masculine and trans-feminine)
should be able to access the majority of services offered by agencies that receive funding
from the Office on Violence Against Women. Since some programs may still be allowed
to be sex-segregated, it is unclear as to how programs will determine who is eligible
for gender-based services. It is our hope that more and more programs that currently
divide by gender, will value trans peoples’ rights to self-determination and honor every
individual’s gender identity. For those who are gender non-conforming or identify
outside of binary gender, it is also our hope that programs will offer equal options for
involvement, support, and services.
Individuals who experience discrimination or unequal treatment when attempting to
access services can file a complaint with the Department of Justice’s Office of Civil Rights
(OCR). The OCR webpage offers a complaint form as well as more information: http://
www.ojp.usdoj.gov/about/offices/ocr.htm We also recommend that trans people claiming
discrimination send FORGE a copy of their complaint, so that we can provide you with
support (and possibly additional referrals) and follow-up.