Journal of Patient-Centered Journal of Patient-Centered
Research and Reviews Research and Reviews
Volume 10 Issue 3 Article 5
7-18-2023
Calcium Carbonate as a Potential Intervention to Prevent Labor Calcium Carbonate as a Potential Intervention to Prevent Labor
Dystocia: Narrative Review of the Literature Dystocia: Narrative Review of the Literature
Sabahat Raees
Marie Forgie
Rita Mitchell
Emily Malloy
Follow this and additional works at: https://aah.org/jpcrr
Part of the Alternative and Complementary Medicine Commons, Biological Factors Commons,
Chemical and Pharmacologic Phenomena Commons, Family Medicine Commons, Maternal and Child
Health Commons, Obstetrics and Gynecology Commons, Other Chemicals and Drugs Commons,
Therapeutics Commons, Translational Medical Research Commons, and the Women's Health Commons
Recommended Citation Recommended Citation
Raees S, Forgie M, Mitchell R, Malloy E. Calcium carbonate as a potential intervention to prevent labor
dystocia: narrative review of the literature. J Patient Cent Res Rev. 2023;10:128-35. doi: 10.17294/
2330-0698.2010
Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the
Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal
focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes,
and the patient experience.
128 JPCRR • Volume 10, Issue 3 • Summer 2023
I
n the United States, cesarean sections increased by
31% from 1976 to 2019;
1
approximately 30% of all
U.S. births are by cesarean section.
2
While cesarean
sections can be a life-saving intervention, the current rise
in the cesarean section rate has not resulted in improved
maternal or neonatal morbidity or mortality. The most
common indication for a cesarean section is labor
dystocia.
3
Labor dystocia is responsible for one-third of
all cesarean sections, 50% of which are primary cesarean
sections.
3
Labor dystocia is a broad term commonly used
to describe prolonged, slow, or arrested labor. Labor
dystocia may occur for several reasons, including a
large or malpositioned fetus, pelvic structure, inadequate
contractions, or maternal factors such as illness or
medications.
Clinicians use a variety of interventions to treat and
prevent labor dystocia, including intravenous (IV)
oxytocin and maternal position changes aimed at
changing pelvic dimensions and repositioning the
fetus. There are limited current standard prevention
methods for labor dystocia other than amniotomy,
oxytocin administration, and accurate diagnosis of
labor arrest.
4
The American College of Obstetricians
and Gynecologists/Society for Maternal-Fetal Medicine
criteria for labor arrest is diagnosed when all three
of the following are present: 1) The cervix is dilated
6 cm or greater; 2) Membranes are ruptured; and 3)
There is no cervical change after at least 4 hours with
adequate uterine activity or at least 6 hours of oxytocin
administration with inadequate uterine activity.
5
To solve problems with little traditional scientic
evidence, physicians and nurses sometimes consult other
clinicians, and social media groups in which health care
professionals can ask questions and share suggestions
have formed in specic specialties. One example, “Labor
and Delivery Nurses Rock!!,” is a large private group
on Facebook connecting approximately 64,500 U.S.
labor and delivery nurses, midwives, and physicians. In
our experience with such social group forums, we have
observed that the topic of administering oral calcium
carbonate tablets (eg, Tums) to address labor dystocia
Calcium Carbonate as a Potential Intervention to Prevent
Labor Dystocia: Narrative Review of the Literature
Sabahat Raees, BS,
1
Marie Forgie, DO,
2
Rita Mitchell, MM, MLIS,
3
Emily Malloy, PhD, CNM
4
1
Chicago Medical School at Rosalind Franklin University, North Chicago, IL;
2
Obstetrics and Gynecology, Aurora UW
Medical Group, Aurora Sinai Medical Center, Milwaukee, WI;
3
Library, Aurora Sinai Medical Center, Milwaukee, WI;
4
Midwifery and Wellness Center, Aurora UW Medical Group, Aurora Sinai Medical Center, Milwaukee, WI
REVIEW
Corresponding author: Emily Malloy,
Midwifery and Wellness Center, Aurora Sinai Medical Center,
1020 N. 12th St., Milwaukee, WI 53233 (emily[email protected])
Abstract Anecdotally, there are attestations from clinicians of calcium carbonate being used successfully
for laboring people experiencing labor dystocia. The goal of this narrative review was to provide a
synopsis of pertinent literature on calcium use in obstetrics to explore the potential benet of calcium
carbonate as a simple and low-cost intervention for prevention or treatment of labor dystocia.
To answer how calcium and carbonate physiologically contribute to myometrium contractility, we
conducted a literature search of English-language peer-reviewed articles, with no year limitation,
consisting of the keywords “calcium,” “calcium carbonate,” “calcium gluconate,” “pregnancy,”
“hemorrhage,” and variations of “smooth muscle contractility” and “uterine contractions.” Though
no overt evidence on calcium carbonate’s ability to prevent labor dystocia was identied; relevant
information was found regarding smooth muscle contractility, calcium’s inuence on uterine muscle
contractility, and carbonate’s potential impact on reducing amniotic uid lactate levels to restore
uterine contractility during labor. Studies reporting the potential eectiveness of calcium gluconate
and sodium bicarbonate in preventing labor dystocia oer background, safety information, and
rationale for a future randomized control trial to evaluate the ability of calcium carbonate to prevent
labor dystocia and reduce rates of cesarean section. (J Patient Cent Res Rev. 2023;10:128-135.)
Keywords calcium carbonate; pregnancy; labor dystocia; Tums; obstetrics; cesarean
Review
aah.org/jpcrr 129
is commonly discussed among group members. In some
cases, oral calcium carbonate is given in combination
with a 1-hour “pit break” or turning o IV oxytocin; in
other cases, it is used with maternal position changes.
The aforementioned social media group contains many
attestations dating from November 2019 — the date of
the rst comment — to December 2022. Within this
timeline, a total of 92 posts had been made by labor and
delivery nurses and midwives in the United States on
calcium carbonate as a potential solution to correct labor
dystocia and prevent a cesarean section.
Calcium carbonate is sold as an over-the-counter antacid
used to decrease heartburn and treat indigestion. When
taken as directed, it has little to no reported risk of harm
during pregnancy. However, there is not any specic
guidance regarding use of calcium carbonate in labor.
6
This led us to seek evidence and risk versus benet
information about the potential of calcium carbonate as
an intervention to prevent labor dystocia and increase
spontaneous vaginal deliveries. Due to a lack of applicable
data reported on calcium carbonate, this narrative review
evaluates the physiological eects of calcium and
carbonate, independently, on uterine muscle in an eort
to understand how calcium carbonate may function in
obstetrics, specically as a factor in the prevention of
labor dystocia.
Literature Search Strategy, Outcomes
A senior medical librarian (R.M.) customized and
conducted the search strategy for all published articles
on calcium carbonate, calcium gluconate, or general
calcium increasing contractions and improving uterine
contractility or reducing hemorrhage. Also included
were articles about calcium and muscle contractility. The
electronic databases OVID Medline, EBSCO CINAHL,
EBSCO Health Business Elite, EBSCO Psychology &
Behavioral Sciences, Clinical Key, Cochrane Library,
and PubMed were searched using PICO-based inquiries,
controlled vocabulary, and keywords. Central concepts
were identied as calcium, calcium gluconate, calcium
carbonate, reduce hemorrhage, improve uterine
contractility, muscle contractility, and smooth muscle
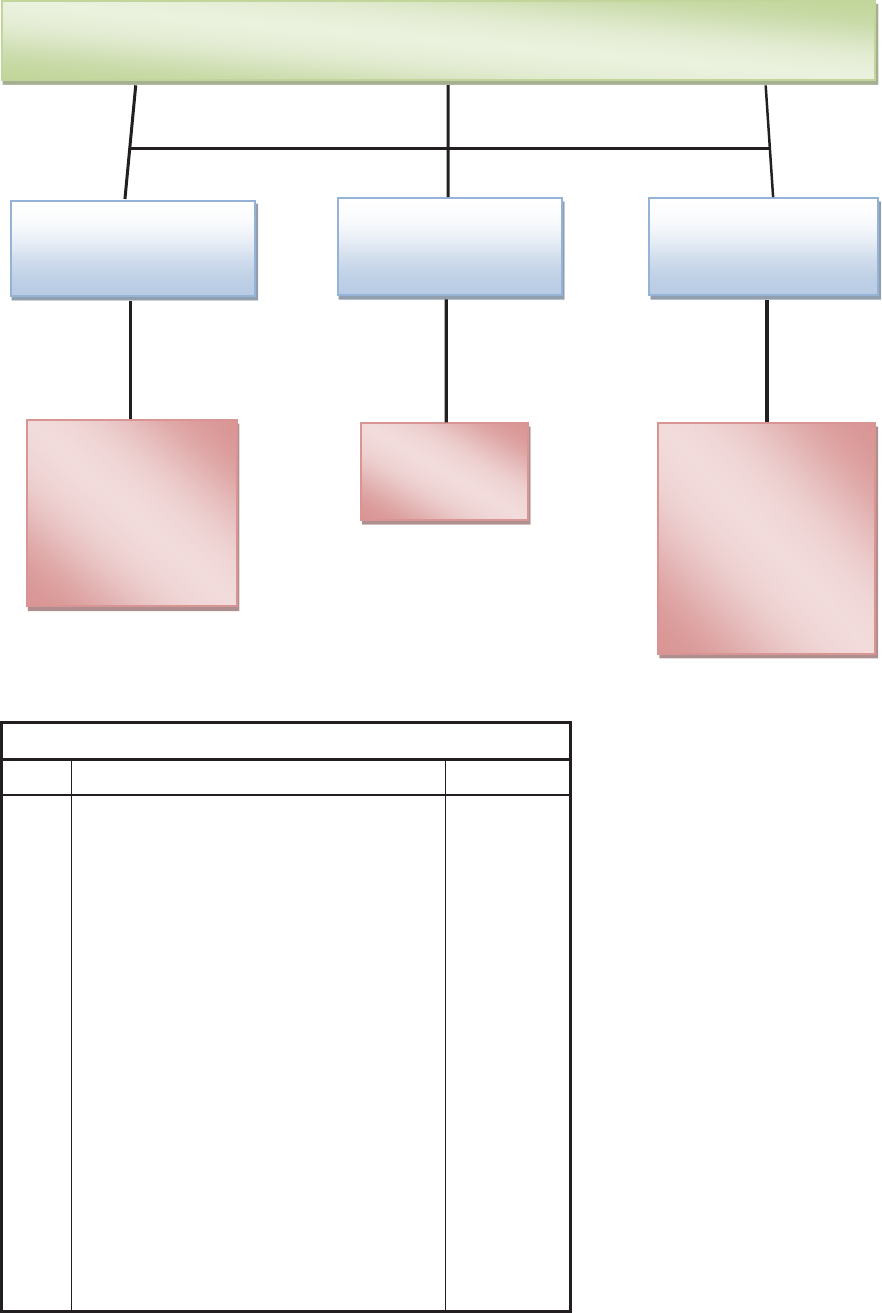
contractility. To determine the appropriate search criteria
for each database, controlled vocabulary, keywords, and
variants were identied (Figure 1). Results were limited
to English language only.
This search strategy yielded 1638 articles. The librarian
(R.M.) screened all titles and abstracts for potential
eligibility, and the other 3 authors (an obstetrician, a
nurse midwife, and a medical student) read the full texts
of those remaining to determine relevance of the nal
selected articles. Overall, 21 articles were included based
on authors’ discretion, and are hereinafter described as
literature reviews, laboratory studies, or randomized
controlled trials.
Uterine Muscle Contractility and Versatility
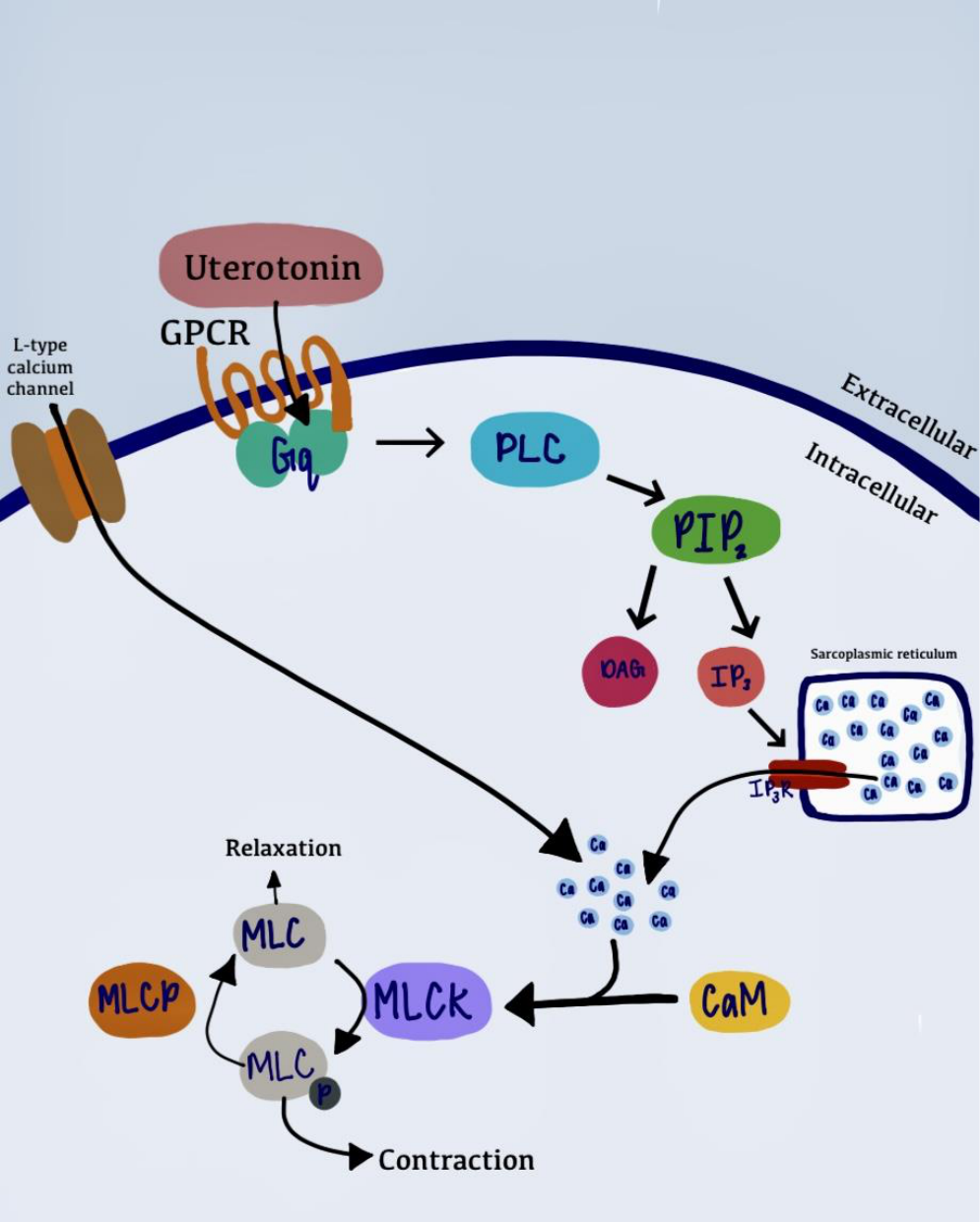
The uterine muscle has a second messenger signaling
system that opens intracellular channels to release the
calcium into the cell and cause contraction.
7
The second
messenger signaling system includes oxytocin receptors,
which are G protein-coupled receptors (GPCR) on the
cell membrane where the uterotonics (oxytocin) bind.
This activates a cascade of events, ultimately releasing
calcium intracellularly to initiate muscle contractility as
outlined in Figure 2. The intrinsic ionic change also opens
L-type calcium channels causing an inux of additional
calcium, resulting in stronger uterine contractions.
7
Calcium release promotes contractility in myometrium,
the uterine muscle. In 2015, Hanley et al determined
L-type calcium channels to be the major route of
entry of calcium ions (Ca
2+
) into uterine muscle.
8
Understanding that calcium promotes contractility in
smooth muscle leads us to further investigate how it
might be used to promote contractility in the uterine
myometrium to prevent labor dystocia. Research by
Pehlivanoğlu and colleagues showed that calcium release
from the sarcoplasmic reticulum is more transient and
rapidly depleted compared to the extracellular calcium
from L-type calcium channels.
7
A research model of
this mechanism explored by Loftus and colleagues
demonstrated that calcium inux is a major contributor to
the rhythmic depolarization of pacemaker areas within the
uterine myocyte and plays an integral role in facilitating
myometrial contraction and coordination.
9
The study
identied additional calcium channels expressed in
the myometrium of birthing people at the time of labor
and an increased number of gap junction development,
which facilitates the carriage of these electrical impulses
supported by calcium.
9
The human myometrium also contains Ca
2+
-activated
chloride (Cl
–
) channels, also known as CaCCs. CaCCs
are activated by increased intracellular calcium levels and
maintain cell depolarization by increasing extracellular
Cl
–
concentration, which depolarizes the myometrial
membrane and activates L-type calcium channels.
10
CaCC expression has been identied in myometrium
of humans and rodents. In 2004, Jones and colleagues
isolated myometrial cells from pregnant rat myometrium
and discovered that CaCC current was evident in 101
of 320 (30%) freshly isolated rat myocytes.
10
Blocking
these channels with niumic acid, a Cl
–
channel
blocker, signicantly decreased the frequency of
contraction in oxytocin-stimulated and spontaneously
Review
130 JPCRR • Volume 10, Issue 3 • Summer 2023
Review
FIGURE 1
A.
B.
MeSH Used in Database Search
# Query Results
1
uterine contraction/
7825
2
Muscle Contraction/
98,805
3
contraction*.ab,ti.
159,322
4
Inotropism.ab,ti.
806
5
((muscle or uterine) adj3 contractility).ab,ti.
4551
6
calcium/
279,763
7
calcium carbonate/
8309
8
calcium gluconate/
1204
9
exp pregnancy/
986,729
10
Postpartum Hemorrhage/
8205
11
pregnant women/
13,306
12
Gestation.ab,ti.
131,613
13
pregnan*.ab,ti.
572,619
14
Muscle, Smooth/
53,285
15
(muscle* adj3 (smooth or involuntary)).ab,ti.
143,461
16
1 or 2 or 3 or 4 or 5
221,589
17
6 or 7 or 8
287,995
18
9 or 10 or 11 or 12 or 13
1,142,473
19
14 or 15
168,606
20
16 and 17 and 18 and 19
307
21
limit 20 to English language
281
Calcium carbonate, calcium gluconate, and general calcium to reduce
hemorrhage or increase contractions and role in muscle contractility
Calcium carbonate,
calcium gluconate,
calcium
Pregnancy,
hemorrhage
Muscle contractility,
contractions,
smooth muscle
Calcium carbonate
Calcium gluconate
Calcium
Calcium signaling
Pregnancy
Hemorrhage
Muscle, smooth
Muscle contractions
Muscle contract*
Myometrium
Uterine contractions
Commented [GJG7]: Julie, this two-panel figure should fit
on one page. The combined legend can appear to the right of
B
Figure 1. A: Schematic showing the
identication of concepts, keywords,
and controlled vocabulary used in the
search strategy of this literature review.
*Indicates wild card truncation when at
the end of a word. B: Medical Subject
Headings (MeSH) used in database
search (<1946 to December 02, 2022>).
aah.org/jpcrr 131Review
Figure 2. Uterine muscle contraction caused by calcium release from L-type calcium channels and inositol
1,4,5-trisphosphate (IP3) receptors via G protein-coupled receptor (GPCR) activation.
FIGURE 2
Figure 2. Uterine muscle contraction caused by calcium release from L-type calcium channels and
inositol 1,4,5-trisphosphate (IP
3
) receptors via G protein-coupled receptor (GPCR) activation.
132 JPCRR • Volume 10, Issue 3 • Summer 2023
contracted strips of myometrium.
10
The increase in
uterine contractility from calcium via various pathways
provides physiological rationale to use calcium as a
supplement to improve uterine contractions and prevent
labor dystocia.
Oxytocin and Uterine Contractility
The synthetic version of oxytocin (trade names: Pitocin
®
,
Syntocinon
®
) is frequently used to induce or augment labor.
Pregnant people have dierent responses to IV oxytocin
use.
11
McAlpine and colleagues determined that exposure
to synthetic oxytocin may contribute to oxytocin receptor
desensitization, resulting in reduced endogenous oxytocin
secretion and therefore decreased uterine contractions.
12
Based on physiological myometrium literature studies
and obstetric investigation, uterine activity and reactivity
are amplied by ionized calcium uterine activity. When
there is decreased uterine activity along with reduced
sensitivity to synthetic oxytocin, it may be due to relative
calcium insuciency.
12
Understanding oxytocin’s
synergetic relationship with calcium to increase eective
uterine contractility oers a potential rationale for using
this method to prevent labor dystocia.
Muscle and Lactic Acid
The carbonate component of calcium carbonate also may
play a role in promoting uterine contractility when amniotic
uid lactate (AFL) levels are elevated.
13
Myometrial
fatigue occurs when the uterine muscle metabolism
switches from aerobic to anaerobic metabolism, resulting
in an accumulation of intramuscular lactic acid.
13
The
lactic acid in the myometrium builds up in the amniotic
uid. Increased AFL levels are associated with labor
dystocia and may lead to operative intervention.
13
In general, lactic acid can aect skeletal muscular
performance in athletes due to muscle fatigue. Athletes
combat increased acid levels by taking oral bicarbonate
before physical activity to prevent muscle fatigue.
14-16
This is a low-cost solution that improves skeletal muscle
performance. In myometrium specically, increased
lactic acid inhibits GPCR function and therefore prevents
calcium’s release in myometrial cells, diminishing uterine
contractility. When used as an intervention, bicarbonate,
a base, alkalinizes the amniotic uid, reducing AFL levels
and restoring the uterine pH for eective myometrium
contractility during labor.
17
Since the experimental data
all utilize bicarbonate, it is unclear if the carbonate
component of calcium carbonate would play a role in
eective myometrium contractility.
Mammalian Studies
There is extensive research in mammal species on the
progression of labor after administration of calcium
versus only administration of exogenous oxytocin. Labor
dystocia occurs in approximately 5% of all parturient
bitches (pregnant dogs) and 3.3%–5.8% of parturient
queens (pregnant cats).
18
A literature review of calcium
therapy in bitches and queens showed that calcium therapy
corrected labor dystocia in cases where bitches had failed
to respond with oxytocin;
18
this protocol is standard of
care for dogs and is deemed to be a helpful therapy in the
medical management of labor dystocia. Calcium therapy
for queens is used less frequently and is controversial
because of the very strong uterine contractions that occur
after calcium administration.
A 2006 prospective randomized controlled trial
consisted of 27 bitches with primary inertia (labor
dystocia) randomly assigned to treatment groups I and
II.
19
Group I was treated with both intravenous calcium
and oxytocin, while group II was treated with oxytocin
only. Blood samples were collected before and after
treatment. Since some bitches started to deliver after
an injection of oxytocin, researchers determined low
oxytocin concentration impaired uterine contractility.
They determined 30% of the dogs did not respond to
the oxytocin treatment alone; however, they did respond
to the oxytocin and intravenous calcium.
19
Bergstrom
and colleagues determined there may be mechanisms
in which calcium functions independently to facilitate
uterine contractility during labor among bitches. Low
plasma oxytocin levels are a cause of labor dystocia in
bitches with normal serum calcium concentrations. While
not statistically signicant, it is noteworthy to recognize
that bitches with hypocalcemia had more instances of
labor dystocia.
19
Hanley et al found that increased lactate levels resulted in
decreased calcium inux into the myometrial cells via the
L-type calcium channel, the main route of calcium entry
into the myometrium.
8
This markedly decreased uterine
contractility and caused labor dystocia. The eect of
lactate on intracellular calcium signaling was investigated
using Indo-1, a calcium indicator, on myometrial strips
of uteruses from pregnant rats and found that lactate
abolished calcium transients and contractional force.
8
The calcium transients did reappear when lactate was
removed, and this was reected by increased force
and amplitude in contractions that returned to previous
control levels.
Human Studies
An in vitro trial in Canada compared contractile responses
to oxytocin of an oxytocin-pretreated human myometrium
with a non-oxytocin-pretreated human myometrium
in the setting of hypocalcemia, normocalcemia, and
hypercalcemia.
20
The study included 36 nonlaboring
term pregnant people undergoing elective cesarean. From
Review
aah.org/jpcrr 133
the cesarean sections, 174 slivers of myometrium were
divided into 6 groups. The myometrium tissue strips were
pretreated with synthetic oxytocin 10-5 M (oxytocin-
pretreated group) for 2 hours or bathed in physiological
salt solution for 2 hours (control group). The myometrium
strips were then exposed to physiological salt solution
with modied calcium concentrations of 1.25 mM
(hypocalcemia), 2.5 mM (normocalcemia), or 3.75 mM
(hypercalcemia), providing a total of 6 study groups. In
oxytocin-naïve myometrium, normocalcemia was found
to have superior uterine contractility when compared
to hypocalcemia and hypercalcemia.
20
In the oxytocin-
pretreated groups, the condence levels were too wide to
draw conclusions and further research is required.
In 2000–2001, a cohort study measured calcium levels of
3 groups of pregnant people: one was measured during
labor at 2–3 cm dilation, 5–6 cm dilation, and at the
time of delivery; one group was measured at the time of
scheduled cesarean; and one group was measured at 38
weeks gestation without labor signs. Previous research has
shown higher levels of serum calcium in pregnant people
who delivered vaginally versus those who underwent
a scheduled cesarean delivery at 38 weeks gestation.
21
The serum calcium levels were compared for those who
had scheduled cesarean sections before surgery and
after delivery. Calcium levels in the neonatal umbilical
vein were also measured for all groups. Serum calcium
levels from the scheduled cesarean section compared
to those who had spontaneous labor were signicantly
dierent (P<0.001).
21
Furthermore, the calcium levels
in the umbilical vein of the newborns born after a
spontaneous labor were higher compared to the calcium
levels of the newborns who were born after a cesarean
section (P<0.001).
21
The level of calcium in the serum
contributes to changes in the myometrium as it causes
an inux of calcium into myometrial cells, contributing
to more eective contractions during labor. Reduced
serum calcium levels provide a diminished reserve of
extracellular calcium for uterine contractility and may
result in weakened contractions during labor. Therefore,
some researchers hypothesize that an increase in serum
calcium by calcium carbonate ingestion during labor may
promote calcium inux and more eective contractions.
Calcium Administered During Labor
Two dated but signicant studies veried labor
enhancement through calcium therapy. In 1947, Grier
conducted a historically controlled study with 129 birthing
people undergoing elective induction of labor who were
given IV calcium gluconate.
22
Of the 129 participants, 36
began labor after the administration of calcium gluconate
alone and 93 were given intramuscular (IM) oxytocin at
30–60-minute intervals to stimulate labor. The results
demonstrated that primiparous and multiparous birthing
people given calcium gluconate along with IM oxytocin
experienced shorter labors compared to the average labor
time (statistics not reported).
22
In 1954, Whyte also conducted a historically controlled
study consisting of 36 primigravida and 166 multigravida
pregnant people. He found calcium gluconate followed
by IM oxytocin was a safe and eective intervention for
those undergoing an induction.
23
The 200 participants
given IM oxytocin and calcium gluconate had successful
labors and delivered vaginally without any indications
of labor dystocia.
23
This pair of mid-20th century studies
demonstrated how calcium’s physiological role can be
portrayed in clinic-based human studies, although the
era of the studies and limited statistical reporting limit
their generalizability and results should be interpreted
with caution.
Studies of Bicarbonate Administered During Labor
A randomized controlled trial conducted by Wiberg-
Itzel et al randomized 200 laboring people into “sodium
bicarbonate” and “non-sodium bicarbonate” groups.
14
IV
oxytocin was administered to both groups. When labor
dystocia was diagnosed, AFL levels were collected. The
bicarbonate group was given 2 packages of Samarin
(totaling 4.26 g of sodium bicarbonate), an over-the-
counter European brand name oral bicarbonate solution,
with oxytocin started 1 hour afterward.
14
New sampling
of AFL was performed after 1 hour in both groups.
Bicarbonate decreased AFL levels (P<0.001), and the
spontaneous vaginal delivery rate after treatment with
bicarbonate was increased (P=0.007).
14
No laboring
person reported stomach pain or gastrointestinal issues,
and there were no dierences in neonatal outcomes.
14
Another more recent randomized controlled trial
by Seyedi and colleagues found that patients given
sodium bicarbonate and oxytocin had increased rates
of spontaneous delivery for those experiencing labor
dystocia. The study included 142 primiparous birthing
people with gestational ages between 39 and 42 weeks.
17
The intervention group was given 4.26 g of sodium
bicarbonate dissolved in 200 mL of water orally as well
as IV oxytocin, while the control group received only IV
oxytocin. The increase in AFL levels directly correlated
with increased labor dystocia. The authors found the
mean duration of the rst and second stage of labor in
the intervention group was shorter than the control
group (P<0.001 for rst stage, P>0.001 for second
stage).
17
Furthermore, in the intervention group, the rate
of spontaneous delivery compared to operative vaginal
birth was signicantly higher (65 cases) compared with
the control group (56 cases); P=0.003.
17
The intervention
Review
134 JPCRR • Volume 10, Issue 3 • Summer 2023
group had fewer cesarean births, but this was not
statistically signicant. Results showed that sodium
bicarbonate reduced the level of AFL, restoring calcium-
mediated contractions, increasing the rate of spontaneous
delivery, and decreasing labor dystocia, although there
was no signicant eect on rate of cesarean delivery.
17
Clinical Implications
This narrative review evaluated available English-
language evidence on the role of calcium or carbonate on
uterine contractility, with a focus on understanding the
role of calcium in cases of labor dystocia. Methodological
aws were evident in several of the 20th century human
studies, as they did not include control groups and
were ethically awed, particularly given that synthetic
oxytocin and calcium gluconate were administered with
minimal awareness of safe dosage and lacked scientic
understanding of oxytocic physiological function. Given
the role of calcium in muscle contractility, we speculate
that calcium carbonate may play a role in decreasing
labor dystocia for pregnant people undergoing induction
of labor by increasing the sensitivity of the uterus to
oxytocin. Physiologically, calcium and carbonate both
enhance myometrium contractility. While there have been
historically controlled studies on calcium gluconate and
randomized controlled trials using sodium bicarbonate,
there have not been any trials of calcium carbonate. It is
important to investigate the eects of calcium carbonate,
as both components play a critical role in promoting
uterine contractility, preventing labor dystocia, and
potentially surgical intervention.
The presented mammalian studies, as well as the 20th
and 21st century human studies, provide insight into a
clinical solution for labor dystocia for birthing people.
A physiological understanding of calcium and carbonate
provides a foundation and rationale for a future clinical
trial. Calcium carbonate is a simple, low-cost treatment
that could yield a potential means of increasing rates of
spontaneous vaginal birth by preventing labor dystocia,
thereby preventing cesarean birth and by extension
improving maternal morbidity. This review supports
calcium’s potential role in preventing labor dystocia
physiologically and clinically. Since calcium carbonate
contains calcium and carbonate, both of which are
physiologically supported by research to prevent labor
dystocia and increase spontaneous delivery rates, it
presents as a promising treatment for further study.
Limitations
The structured assessment of methodological quality,
comprehensive search, and inclusion of published
evidence-based literature and research studies are
strengths of this narrative review. Still, our review was
limited to English language only. Furthermore, the
inclusion criteria did not include additional uterotonics
that may impact labor dystocia. Our focus was solely on
calcium carbonate and its ability to prevent labor dystocia
by increasing the eectiveness of uterine contractions.
Early research conducted by Grier
22
and Whyte
23
did
not use a control group and was thus methodologically
awed. Randomized controlled trials conducted by
Wiberg-Itzel et al
14
and Seyedi et al
17
had small sample
sizes and did not study the inuence of calcium carbonate
but rather sodium bicarbonate.
Summary
Synthetic oxytocin is among the most obstetrically
important and useful medications available, yet the use of
synthetic oxytocin does not always correct or prevent labor
dystocia. We recommend well-conducted randomized
controlled trials with sucient sample size to evaluate
calcium carbonate administration as an intervention to
decrease labor dystocia caused by weak or ineective
myometrial contractions, evaluate maternal and neonatal
outcomes, and identify risks, benets, and any rare or
unexpected outcomes. By exploring the physiological
mechanisms of action of calcium in relation to muscle
contractility and carbonate’s inuence on amniotic uid
lactate, this narrative review indirectly examined the
potential benet of calcium carbonate in labor to prevent
dystocia. Given that labor dystocia is the most common
indication for unplanned cesarean section in the United
States, we theorize that calcium carbonate may be a low-
risk and promising preventive measure that may decrease
the rate of cesarean section.
Patient-Friendly Recap
• Pregnant people experiencing slow or prolonged
labor (aka dystocia) sometimes have an unplanned
cesarean delivery.
• Authors reviewed the literature to learn whether one
means of preventing cesarean and increasing the
rate of vaginal birth might be use of oral calcium
carbonate (Tums) to prevent labor dystocia.
• No results from evaluating the eect of calcium
carbonate during labor were found. However,
studies reporting the eect of calcium on muscle
contractility and carbonate’s inuence on amniotic
uid lactate were reviewed and analyzed.
• Based on the physiological eects demonstrated
by each ingredient, authors concluded that oral
calcium carbonate’s potential to prevent labor
dystocia should be evaluated in suciently
powered randomized controlled trials.
Review
aah.org/jpcrr 135
Author Contributions
Study design: Forgie, Malloy. Data acquisition or analysis: all
authors. Manuscript drafting: Raees, Forgie, Malloy. Critical
revision: all authors.
Conicts of Interest
None.
References
1. Antoine C, Young BK. Cesarean section one hundred years
1920-2020: the Good, the Bad and the Ugly. J Perinat Med.
2020;49(1):5-16. CrossRef
2. Osterman MJ, Martin JA. Trends in low-risk cesarean delivery in
the United States, 1990-2013. Natl Vital Stat Rep. 2014;63:1-16.
3. In: Walls RM, Hockberger RS, Gausche-Hill M, et al (eds).
Rosen’s Emergency Medicine: Concepts and Clinical Practice,
Ninth Edition. Elsevier; 2018.
4. Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade
GR. Preventing the rst cesarean delivery: summary of a joint
Eunice Kennedy Shriver National Institute of Child Health and
Human Development, Society for Maternal-Fetal Medicine,
and American College of Obstetricians and Gynecologists
workshop. Obstet Gynecol. 2012;120:1181-93. CrossRef
5. American College of Obstetrics and Gynecology; Society
for Maternal-Fetal Medicine. Obstetric Care Consensus No.
1: Safe prevention of the primary cesarean delivery. Obstet
Gynecol. 2014;123:693-711. CrossRef
6. Salisbury BH, Terrell JM. Antacids. [Last updated August 15,
2022.] In: StatPearls [Internet]. StatPearls Publishing; January
2023. https://www.ncbi.nlm.nih.gov/books/NBK526049/
7. Pehlivanoğlu B, Bayrak S, Doğan M. A close look at the
contraction and relaxation of the myometrium; the role of
calcium. J Turk Ger Gynecol Assoc. 2013;14:230-4. CrossRef
8. Hanley JA, Weeks A, Wray S. Physiological increases in lactate
inhibit intracellular calcium transients, acidify myocytes and
decrease force in term pregnant rat myometrium. J Physiol.
2015;593:4603-14. CrossRef
9. Loftus FC, Richardson MJ, Shmygol A. Single-cell mechanics
and calcium signalling in organotypic slices of human
myometrium. J Biomech. 2015;48:1620-4. CrossRef
10. Jones K, Shmygol A, Kupittayanant S, Wray S.
Electrophysiological characterization and functional
importance of calcium-activated chloride channel in rat uterine
myocytes. Pugers Arch. 2004;448:36-43. CrossRef
11. Arrowsmith S, Kendrick A, Wray S. Drugs acting on the
pregnant uterus. Obstet Gynaecol Reprod Med. 2010;20:241-7.
CrossRef
12. Mcalpine JM, Vanderlelie JJ, Perkins AV. First do no harm:
intrapartum calcium loading during oxytocic induction of
labor. J Womens Health. 2015;4(4). CrossRef
13. Murphy M, Butler M, Coughlan B, Brennan D, O’Herlihy
C, Robson M. Elevated amniotic uid lactate predicts labor
disorders and cesarean delivery in nulliparous women at term.
Am J Obstet Gynecol. 2015;213:673.e1-8. CrossRef
14. Wiberg-Itzel E, Wray S, Åkerud H. A randomized controlled
trial of a new treatment for labor dystocia. J Matern Fetal
Neonatal Med. 2018;31:2237-44. CrossRef
15. Burke LM. Practical considerations for bicarbonate loading
and sports performance. Nestle Nutr Inst Workshop Ser.
2013;75:15-26.
16. Van Montfoort MC, Van Dieren L, Hopkins WG, Shearman JP.
Eects of ingestion of bicarbonate, citrate, lactate, and chloride
on sprint running. Med Sci Sports Exerc. 2004;36:1239-43.
CrossRef
17. Seyedi M, Ghorashi Z, Sedighi Darijani T. Randomized
controlled trial of oral bicarbonate treatment for labor
stagnation. J Obstet Gynaecol Res. 2021;47:114-8. CrossRef
18. Pretzer SD. Medical management of canine and feline dystocia.
Theriogenology. 2008;70:332-6. CrossRef
19. Bergström A, Fransson B, Lagerstedt AS, Olsson K. Primary
uterine inertia in 27 bitches: aetiology and treatment. J Small
Anim Pract. 2006;47:456-60. CrossRef
20. Talati C, Ramachandran N, Carvalho JC, Kingdom J,
Balki M. The eect of extracellular calcium on oxytocin-
induced contractility in naive and oxytocin-pretreated human
myometrium in vitro. Anesth Analg. 2016;122:1498-507.
CrossRef
21. Papandreou L, Chasiotis G, Seferiadis K, et al. Calcium levels
during the initiation of labor. Eur J Obstet Gynecol Reprod
Biol. 2004;115:17-22. CrossRef
22. Grier RM. Elective induction of labor. Am J Obstet Gynecol.
1947;54:511-6. CrossRef
23. Whyte JC. Calcium gluconate in the induction of labour. Can
Med Assoc J. 1954;70:261-2.
© 2023 Advocate Aurora Research Institute
Review
