
GAO
United States Government Accountabilit
y
Office
Report to Congressional Committees
FOREIGN MEDICAL
SCHOOLS
Education Should
Improve Monitoring
of Schools That
Participate in the
Federal Student Loan
Program
June 2010
GAO-10-412
Page i GAO-10-412
Contents
Letter 1
Agency Comments and Our Evaluation 7
Appendix I Briefing Slides 9
Appendix II Objectives, Scope, and Methodology 50
Appendix III Comparison of Average Cost of Attendance of
U.S. and Selected Foreign Medical Schools 56
Appendix IV Performance on Licensing Exam by Number of
Attempts on Each Exam Step, and by Nationality
of IMG
57
Appendix V International Medical Graduates and Residencies 60
Appendix VI Summary of Responses by Focus Group Participants
at the Five Foreign Medical Schools We Visited 63
Appendix VII Comments from the U.S. Department of Education 71
Appendix VIII GAO Contact and Staff Acknowledgments 73
Bibliography 74
Related GAO Products 77
Foreign Medical Schools
Tables
Table 1: Residency Programs by State, Academic Year 2008-2009 60
Table 2: Number of Participants in Student Focus Groups, by
School 63
Table 3: Decision to Attend a Foreign Medical School 64
Figures
Figure 1: Licensing Exam Pass Rates by Number of Exam Attempts
on Each Exam Step, 1998 through 2008 57
Figure 2: Comparison of First-Time Pass Rates for U.S. Citizen
IMGs and Foreign IMGs on Step 1 (Basic Science) and
Step 2 Clinical Knowledge, 1998 through 2008 58
Figure 3: Comparison of First-Time Pass Rates for Both U.S.
Citizen IMGs and Foreign IMGs on Step 2 Clinical Skills,
2004 through 2008, and Step 3 (on Delivery of General
Medical Care), 1998 through 2008 59
Figure 4: Percentage of IMGs in Residencies as a Percentage of All
Residents by State, Academic Year 2008-2009 62
Page ii GAO-10-412 Foreign Medical Schools
Abbreviations
AAMC Association of American Medical Colleges
ACGME Accreditation Council for Graduate Medical Education
AMA American Medical Association
ECFMG Educational Commission for Foreign Medical
Graduates
FFEL Federal Family Education Loans
FSMB Federation of State Medical Boards
HEAL Health Education Assistance Loan
HHS Health and Human Services
IMG International Medical Graduate
MCAT Medical College Admission Test
NBME National Board of Medical Examiners
OB/GYN Obstetrics and Gynecology
USMLE United States Medical Licensing Exam
This is a work of the U.S. government and is not subject to copyright protection in the
United States. The published product may be reproduced and distributed in its entirety
without further permission from GAO. However, because this work may contain
copyrighted images or other material, permission from the copyright holder may be
necessary if you wish to reproduce this material separately.
Page iii GAO-10-412 Foreign Medical Schools
Page 1 GAO-10-412
United States Government Accountability Office
Washington, DC 20548
June 28, 2010
The Honorable Tom Harkin
Chairman
The Honorable Michael B. Enzi
Ranking Member
Committee on Health, Education, Labor,
and Pensions
United States Senate
The Honorable George Miller
Chairman
The Honorable John P. Kline
Ranking Member
Committee on Education and Labor
House of Representatives
Each year, the federal government makes a significant financial
investment in the education and training of the U.S. physician workforce.
A quarter of that physician workforce is composed of international
medical graduates (IMG) and they include both U.S. citizens and foreign
nationals. In fiscal year 2008, the federal government loaned $633 million
to U.S. students enrolled in foreign institutions—including medical
students—through the Federal Family Education Loan (FFEL) program.
1
The government also makes a substantial domestic investment in the
graduate training of the physician workforce. For example, in fiscal year
2008, federal support for residency training in the United States amounted
to nearly $9 billion. As with medical students educated in the United
States, this training is required of all IMGs—U.S. citizens and foreign
1
Until recently, these student loans were made through the Federal Family Education Loan
program, which was the only federal student financial aid program in which foreign
schools could participate. Under newly enacted legislation, the SAFRA Act, which was
included in the Health Care and Education Reconciliation Act of 2010, (Pub. L. No. 111-152
(2010)), the FFEL program will terminate June 30, 2010, after which no new loans will be
made under the FFEL program. The SAFRA Act extends the availability of loans under the
William D. Ford Federal Direct Loan (Direct Loan) program to students at eligible foreign
institutions. Thus, beginning in July 2010, students at foreign medical schools will receive
new loans through the Direct Loan program, instead of the FFEL program. Throughout this
report we refer to the federal student loan program in our findings. Where our findings are
specific to the FFEL program, however, we refer to that program by name.
Foreign Medical Schools
nationals alike—who seek to practice medicine without supervision in the
United States.
The Department of Education (Education), which administers the federal
student loan program, must also monitor foreign schools that seek to
participate in the program with respect to specific statutory requirements.
Among these is the statutory requirement that at least 60 percent of their
students who take the U.S. medical licensing exam must pass the exam.
Most recently, Congress increased the pass rate to 75 percent, effective July
2010.
Little is known about IMGs with respect to how much they borrow overall,
or the outcome of their medical studies, leading some policy makers to
question the federal return on investment in IMGs. Therefore, Congress
mandated that GAO study the performance of IMGs educated at these
schools and other aspects of a foreign medical education, including the
potential effect of the new 75 percent pass rate requirement on school
participation in the federal loan program.
2
This report examines the following questions:
1. What amount of federal student aid loan dollars has been awarded to
U.S. students attending foreign medical schools?
2. What do the data show about the pass rates of international medical
graduates on license examinations?
3. To what extent does Education monitor foreign medical schools’
compliance with the pass rate required to participate in the federal
student loan program?
4. What is known about schools’ performance with regard to the
institutional pass rate requirement?
5. What is known about where international medical graduates have
obtained residencies in the United States and the types of medicine
they practice?
2
Pub. L. No. 110-315, § 1101 (2008). A similar mandate was directed at the Department of
Education’s National Committee on Foreign Medical Education and Accreditation. The
committee issued its report to Congress in 2009.
Page 2 GAO-10-412 Foreign Medical Schools
6. What is known about discipline and malpractice involving foreign-
educated physicians?
On May 26 and 27, 2010, we briefed your staff on the final results of our
analysis in addition to providing interim updates in February and March
2010. This report formally conveys the information provided during the
briefing. (See app. I for the briefing slides.) In summary, we found the
following:
• From 1998 to 2008, U.S. students enrolled at foreign medical schools
borrowed $1.5 billion in FFEL loans to attend free-standing medical
schools.
3
Although this amount represents less than 1 percent of all
federal student loans borrowed during this period, borrowing has
grown significantly, in part because of increases in tuition, student
enrollments, and the availability of additional loan funds for graduate
and professional students.
4
Although our results are not generalizable,
some students who participated in our focus groups estimated that
their student loan debt would range from about $90,000 to $250,000 for
their medical degree alone.
5
In addition, some student borrowers stated
that they lack reliable cost and performance information about foreign
medical schools.
• IMGs, as a group, have consistently passed their medical licensing exam
at lower rates over the past decade than their U.S.-educated peers, but
have narrowed this performance gap for most of the exam steps. In 1998,
for example, average IMG pass rates on the clinical knowledge exam
were 55 percent compared with 95 percent for U.S.-educated graduates.
By 2008, however, IMG rates had increased to 82 percent while they
remained about the same for U.S. graduates. IMGs still lag behind on the
exam step for clinical skills—which involves interaction with patients—
with about a 26 percentage point difference in 2008. They also required
3
Another $1 billion went to students attending foreign schools with a medical program;
however, it is not known what portion of this amount was used to pursue a medical degree
as opposed to some other discipline because the Department of Education does not track
loan volume according to academic discipline.
4
GRADPlus loans are part of the federal student loan program and are non-need-based
loans that graduate and professional students may borrow irrespective of their expected
financial contributions to paying educational expenses. Funds borrowed are limited by
other financial assistance received, such as other FFEL loans, and a student’s cost of
attendance.
5
By comparison, the median loan debt for students pursuing medical degrees in the United
States was $155,000 in 2008.
Page 3 GAO-10-412 Foreign Medical Schools
more attempts to pass the exam than their U.S.-educated counterparts.
However, pass rates on the additional attempts were lower for both
IMGs and U.S.-educated students compared with pass rates on initial
attempts. Many factors are likely to have affected IMG pass rates,
according to experts and others we interviewed, including students’
proficiency in English and the extent to which foreign schools may or
may not focus on preparing students for the exam.
• Education has not been able to fully enforce the institutional pass rate
requirement needed for continued federal student loan eligibility. The
three private organizations that administer each step of the exam have
declined to release student scores on grounds that the data are
proprietary in nature and should not be used for marketing purposes.
As a result, Education reviews pass rates only when a school applies
for the program, when it periodically seeks recertification, or when
there is a change in ownership. More recently, however, two of the
three testing organizations have begun negotiating with individual
schools for the release of aggregate student performance data. On the
basis of this development, Education officials told us that the
department now plans to require pass rate data annually from all
foreign medical schools participating in the federal loan program.
• Our own analysis of 2008 pass rate data of institutions located in
countries that participate in the federal loan program indicates that
while a majority of foreign medical schools in these countries met the
current 60 percent student pass rate requirement, very few—11
percent—would likely meet the newly required 75 percent pass rate.
Meanwhile, officials from the three testing organizations cautioned
against associating student performance on the U.S. medical licensing
exam with institutional quality, given the variability among students,
the fact that some schools restrict who may sit for the exam, and that
other schools may encourage practice runs.
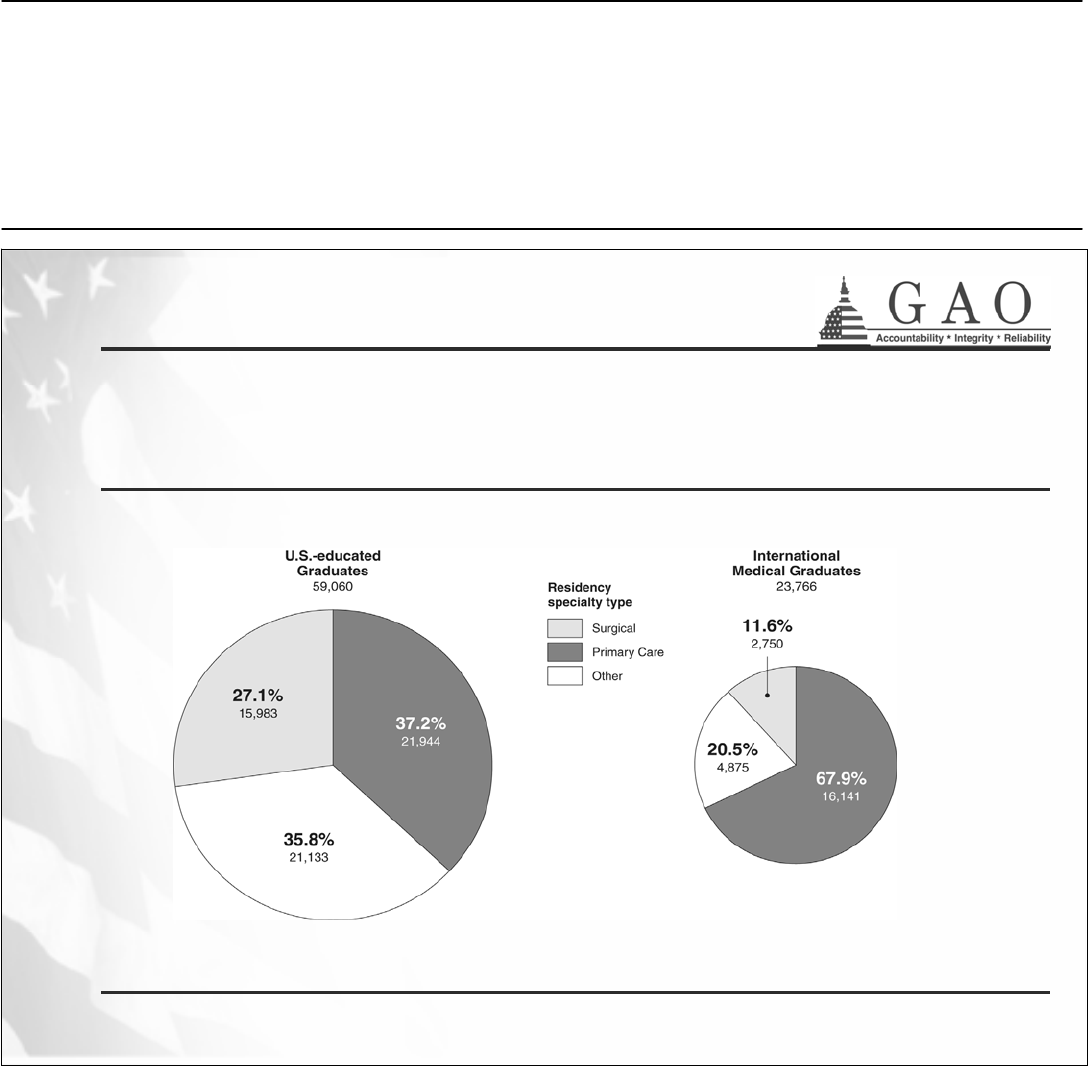
• IMGs have entered into residency programs in all states, though they are
concentrated in the eastern United States, and a larger proportion tend
to practice in primary care than do U.S.-educated graduates. Nationwide,
in academic year 2008-2009 there were 109,482 medical residents, over
30,000 of whom were IMGs (about 27 percent). Of this group of IMGs,
about 78 percent were located in states east of the Mississippi, compared
with 69 percent of all residents. The distribution of IMG residents by
region shows the largest percentage in the Mid-Atlantic and the smallest
Page 4 GAO-10-412 Foreign Medical Schools
percentages in the Mountain states and Puerto Rico.
6
Several factors can
affect the location of IMGs whether in residencies or in subsequent
practice, such as the geographical distribution of residency programs,
which are largely concentrated in the Mid-Atlantic region and in urban
areas. With regard to medical practice, a larger proportion of IMGs go
into residencies in primary care fields (68 percent compared to 37
percent of U.S. medical graduates in academic year 2008-2009).
Moreover, IMGs increased as a percentage of all residents in core
primary care fields (from 31 to 39 percent) between academic years
2001-2002 and 2008-2009.
7
Research shows that IMGs are also more
likely than U.S.-educated graduates to practice as primary care
physicians after finishing their residency training.
• Overall, few significant differences exist between all IMGs and U.S.-
educated physicians with regard to either disciplinary actions that would
revoke or suspend their licenses or with regard to malpractice
payments
8
—and rates of disciplinary actions are low for physicians as a
whole. Our analysis of national data from 2004 to 2008 on license
revocation and suspension showed that IMGs accounted for a somewhat
larger proportion of these actions than would be expected based on their
share of the physician workforce overall, but it was not a statistically
significant difference. With regard to malpractice, which research suggests
is a weak indicator of physician competence; data on the whole suggest
little difference between IMGs and domestically educated graduates.
GAO is making several recommendations to the Department of Education
concerning the lack of student consumer data on foreign medical
institutions and also the department’s monitoring of pass rates for foreign
medical schools whose students take the U.S. medical licensing exam.
Specifically, GAO recommends that the Secretary of Education
• collect consumer information, such as aggregate student debt level and
graduation rates, from foreign medical schools participating in the
6
The Mid-Atlantic states are New Jersey, New York, and Pennsylvania. The Mountain states
are Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, and Wyoming.
7
Core primary care specialties are internal medicine, family medicine, pediatrics, or
internal medicine/pediatrics.
8
Malpractice payments are a monetary exchange as a result of a settlement or judgment of
a written complaint or claim demanding payment based on a physician’s provision of or
failure to provide health care services, and may include, but is not limited to, the filing of a
cause of action, based on the law of tort, brought in any State or Federal Court or other
adjudicative body.
Page 5 GAO-10-412 Foreign Medical Schools
federal student loan program and make it publicly available to students
and their families;
• require foreign medical schools to submit aggregate institutional pass
rate data to the department annually;
• verify data submitted by schools, for example, by entering into a data-
sharing agreement with the testing organizations; and
• evaluate the potential impact of the 75 percent pass rate requirement
on school participation in the federal student loan program and advise
Congress on any needed revisions to the requirement.
For this report, we analyzed the Department of Education’s loan data for
all foreign medical schools participating in the FFEL program between
academic years 1998 and 2008.
9
To assess the performance of international
medical graduates on licensing examinations, we analyzed trends in exam
data from 1998 to 2008. We evaluated Education’s monitoring of foreign
medical schools’ compliance with the minimum licensing exam pass rate
requirement through interviews with agency officials and analysis of exam
data at an institutional level. We also analyzed graduate medical education
data and interviewed cognizant officials to ascertain where graduates
obtained residencies and to identify their medical specialties. With regard
to discipline and malpractice, we analyzed data from the Department of
Health and Human Services, the Federation of State Medical Boards, and
two states—California and Florida—with high populations of international
medical graduates.
10
We also interviewed experts about the relevance and
availability of these data. Because external data were significant to each of
our research objectives, we assessed the reliability of the publicly and
privately held data we obtained. We determined the data to be sufficiently
reliable for the purposes of this report. Finally, we visited five stand-alone
foreign medical schools in the Caribbean and Europe selected based on
federal student loan volume and other institutional characteristics. At each
school, we interviewed school officials and conducted student focus
groups with a nongeneralizable sample of current students.
9
These academic years were chosen because they coincide with reauthorizations to the
Higher Education Act of 1965.
10
Overall, we interviewed officials from four states—California, Florida, New Jersey, and
New York—and conducted data reliability assessments of their disciplinary data. On the
basis of the outcome of these assessments, we included data from California and Florida in
this report.
Page 6 GAO-10-412 Foreign Medical Schools
We conducted this performance audit from June 2009 to June 2010 in
accordance with generally accepted government auditing standards. Those
standards require that we plan and perform the audit to obtain sufficient,
appropriate evidence to provide a reasonable basis for our findings and
conclusions based on our audit objectives. We believe that the evidence
obtained provides a reasonable basis for our findings and conclusions
based on our audit objectives. Our scope and methodology are discussed
in greater detail in appendix II. Additional information related to our
principal findings can be found in appendixes III-VI.
We provided a draft of this report to the Departments of Education and
Health and Human Services (HHS). We also shared relevant excerpts of
the draft report with the private organizations that administer the licensing
exams. Each of them provided technical comments which were
incorporated into the report as appropriate. Education also provided
additional comments which are reprinted in appendix VII.
Agency Comments
and Our Evaluation
Education agreed with our recommendations and plans to collect
consumer information on foreign medical schools. Education will also ask
these schools to submit pass rate information starting with exams taken
during the award year ending June 30, 2010, and will try to establish a
mechanism to verify pass rates in cooperation with the private
organizations that administer the exams. In addition, Education said that
it has already begun evaluating the potential impact of the 75 percent pass
rate requirement through proposed regulations, and that a notice of
proposed rulemaking inviting public comment is scheduled to be
published in summer 2010.
In its comments, HHS noted that increasing the pass rate requirement will
adversely affect federal student loan availability for future students
attending foreign medical schools, adding that IMGs contribute a
significant percentage of primary care residents in the United States.
Page 7 GAO-10-412 Foreign Medical Schools
If you or your staff have questions about this report, please contact George
A. Scott at (202) 512-7215 or [email protected]. Contact points for our
Offices of Congressional Relations and Public Affairs may be found on the
last page of this report. GAO staff members who made key contributions
George A. Scott
to this report are listed in appendix VIII.
Director,
force, and Income Security
Education, Work
Page 8 GAO-10-412 Foreign Medical Schools
A
ppendix I: Briefing Slides
Page 9 GAO-10-412
Appendix I: Briefing Slides
1
Appendix I: Briefing Slides
Briefing to Congressional Committees:
Education and Labor
House of Representatives
Health, Education, Labor, and Pensions
United States Senate
May 2010
Foreign Medical Schools: Education Should Improve
Monitoring of Schools That Participate
in the Federal Student Loan Program
Foreign Medical Schools
Appendix I: Briefing Slides
2
Overview
Introduction
Objectives
Scope and Methodology
Summary of Findings
Background
Findings
Conclusions and Recommendations
Page 10 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
Page 11 GAO-10-412
3
Introduction
Each year, the federal government makes a significant financial investment in the
education and training of the U.S. physician workforce. A quarter of that physician
workforce is comprised of international medical graduates (IMG) and they include both
U.S. citizens and foreign nationals.
• In fiscal year 2008, the federal government provided $633 million in federally
guaranteed loans to U.S. citizens enrolled in foreign institutions, including
medical students. These loans were made through the Federal Family
Education Loan (FFEL) program.
1
• That same year, it spent another nearly $9 billion to sponsor the hundreds of
residency programs that train graduates from foreign and U.S. medical schools
alike, and that are required to practice medicine in the United States.
1. To date, the FFEL program has been the only federal student financial aid program in which foreign schools participated. Under newly enacted
legislation, the SAFRA Act, which was included in the Health Care and Education Reconciliation Act of 2010, (Pub. L. No. 111-152 (2010)), the FFEL
program will terminate June 30, 2010, after which no new loans will be made under the FFEL program. The SAFRA Act extends the availability of loans
under the William D. Ford Federal Direct Loan (Direct Loan) program to students at eligible foreign institutions. Thus, beginning in July 2010, students
at foreign medical schools will receive new loans through the Direct Loan program, instead of the FFEL program. Throughout this report we refer to the
federal student loan program in our findings. Where our findings are specific to the FFEL program, however, we refer to that program by name.
Foreign Medical Schools
Appendix I: Briefing Slides
4
Introduction
Foreign medical schools can differ substantially from U.S. schools in their requirements
for admission and length of study.
• For this and other reasons, the Department of Education, which administers the
federal student loan program, imposes requirements for foreign schools to
participate in the program.
1
• Among these is a statutory requirement that at least 60 percent of IMGs who
take the U.S. medical licensing exam must pass. Recently, Congress
increased the pass rate requirement to 75 percent, effective July 2010.
Little is known about U.S. citizens who study medicine abroad with respect to how much
they borrow in federal loans overall, or the outcomes of their medical studies.
GAO undertook this study pursuant to a mandate enacted in section 1101 of the Higher
Education Opportunity Act.
2
1. To receive federal loan funds, students must be enrolled at eligible institutions located in countries with standards of accreditation of medical schools that
are comparable to the standards of accreditation of medical schools in the United States.
2. Pub. L. No.110-315 (2008).
Page 12 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
5
Objectives
1. What amount of federal student aid loan dollars has been awarded to U.S.
students attending foreign medical schools?
2. What do the data show about the pass rates of international medical graduates on
license examinations?
3. To what extent does Education monitor foreign medical schools’ compliance with
the pass rate required to participate in the federal student loan program?
4. What is known about schools’ performance with regard to the institutional pass rate
requirement?
5. What is known about where international medical graduates have obtained
residencies in the United States and the types of medicine they practice?
6. What is known about discipline and malpractice involving foreign-educated
physicians?
Page 13 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
6
Scope and Methodology
To conduct our work, we:
• reviewed and analyzed federal student loan volume and privately held data on U.S.
licensing exams, residency surveys, and disciplinary actions and malpractice
payments;
• interviewed officials and experts and reviewed information and documents from:
o Department of Education
o Department of Health and Human Services, Health Resources and Services
Administration
o Educational Commission for Foreign Medical Graduates (ECFMG), the National
Board of Medical Examiners, and the Federation of State Medical Boards
o Selected schools participating in the federal student loan program
o Agencies responsible for licensing and disciplining physicians in four states with high
concentrations of IMGs, and found the data from two of these states to be reliable for
our purposes.
• reviewed relevant literature on IMGs published from 1990 to 2009 by various
associations and individual researchers; and
• reviewed relevant federal laws and regulations.
Page 14 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
7
• conducted site visits to five foreign medical schools:
o American University of the Caribbean (St. Maarten),
o Ross University (Dominica),
o St. George’s University (Grenada),
o Royal College of Surgeons (Ireland),
o Poznan University of Medical Sciences (Poland); and,
• conducted a non-generalizable sample of student focus groups—consisting
primarily of U.S. citizens who were receiving federal student loans—at each school
we visited.
• We determined that the data used to address our research objectives were
sufficiently reliable for the purposes of this report.
Scope and Methodology
Page 15 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
8
Summary of Findings
1. From 1998 to 2008, U.S. students borrowed $1.5 billion in federally guaranteed
student loans to study at foreign medical schools. Meanwhile, some student
borrowers stated that they lack reliable cost and performance information about
these schools.
2. Pass rates on the U.S. Medical Licensing Exam have improved for all international
medical graduates, but still lag behind those of U.S.-educated graduates.
3. Education lacks the data necessary to fully enforce foreign medical school
compliance with the pass rate requirement.
4. While a majority of foreign medical schools met the current 60 percent pass rate
requirement in 2008, very few would likely meet the newly enacted 75 percent rate.
5. International medical graduates in residency programs are located primarily in the
eastern U.S. and tend to practice primary care fields.
6. Available data on disciplinary proceedings and malpractice reveal few differences
between international medical graduates and U.S.-educated physicians.
Page 16 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
9
Background
Who Are International Medical Graduates (IMGs)?
• They are physicians who have graduated from medical schools in countries other
than the U.S. and Canada.
1
• IMGs comprise over one quarter (about 244,000 physicians) of the current physician
workforce in the U.S.
• They include both citizens of the U.S. and other countries.
• Of IMGs who practice in the U.S., nearly 20 percent are U.S. citizens or permanent
residents.
1. The definition of IMG may vary. Health workforce experts do not consider Canadian graduates to be IMGs because the accreditor and medical education
standards for Canada are similar to the U.S. Alternatively, the Department of Education’s definition of IMGs includes U.S. students who were educated in
Canadian medical schools. For the purposes of our report, our definition of IMGs excludes graduates of U.S. and Canadian medical schools.
Page 17 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
10
Background
Federal Student Loan Program Requirements for Foreign
Medical Schools
To participate in the program, foreign medical schools must:
• Be located in one of 26 countries
1
whose standards of accreditation are
comparable to those in the U.S. as determined by the National Committee on
Foreign Medical Education and Accreditation;
2
• Meet the statutorily mandated institutional pass rate on certain medical licensing
exams
3
and other specific statutory and regulatory eligibility requirements;
• A few schools have been statutorily exempted from the pass rate requirement in
view of their existing approved U.S. clinical training programs in operation since
1992:
1. According to the Foundation for the Advancement of International Medical Education and Research’s International Medical Education Directory, there were
251 foreign medical schools located in comparable countries, some of which participate in the federal loan program. At various places in this report, the data
presented may pertain to schools that either participate in the federal student loan program or to all foreign medical schools regardless of their participation.
2. 20 U.S.C. § 1002(a)(1)(C), (a)(2)(B); 34 C.F.R. § 600.55(a)(4).
3. 20 U.S.C. § 1002(a)(2)(A)(i)(I)(bb); 34 C.F.R. § 600.55(a)(5)(i)(B).
o St. George’s University, Grenada
o Our Lady of Fatima University, the Philippines
o American University of the Caribbean, St. Maarten
o Tel Aviv University, Israel
o Ross University, Dominica
Page 18 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
11
According to Department of Education guidance, students who are enrolled in eligible
foreign medical schools:
• Must generally be U.S. citizens, nationals, or eligible permanent residents to
qualify for federally guaranteed student loans.
• May borrow up to $20,500 in subsidized and unsubsidized loans
1
annually.
Total borrowing through the program for students enrolled in foreign medical
schools is limited to $138,500.
• May borrow additional loan funds up to the cost of attendance minus other
federal assistance in loans for graduate and professional students, available as
of 2006, if they have met the federal student loan program limit.
By contrast, students enrolled in U.S. medical schools may borrow up to $224,000 in
federal guaranteed student loans to replace loan funds no longer available through the
Department of Health and Human Services’ Health Education Assistance Loan (HEAL)
program.
2
Background
Federal Student Loan Program Requirements for U.S. Medical
Students Abroad
1. Federally subsidized student loans are based on financial need. The interest on subsidized federal loans is paid by the federal government while students
are enrolled at least half-time in college and during periods of authorized deferment. The interest for these loans is paid by the student upon graduation.
Interest on unsubsidized federal loans is paid by the student and accrues from the date the loan is disbursed to a student until it is paid in full.
2. U.S. medical students abroad were not eligible to participate in the HEAL program and thus are ineligible to receive the additional loan funds made
available to students attending U.S. medical schools.
Page 19 GAO-10-412 Foreign Medical Schools

Appendix I: Briefing Slides
12
Background
How Foreign Medical Schools Differ from U.S. Medical Schools
Foreign medical schools can vary considerably from U.S. medical schools.
• Most students must receive a competitive score on the Medical College Admission
Test (MCAT) to be admitted to a U.S. medical school because of educational
standards and limited slots. Unlike U.S. medical schools, foreign medical schools
do not necessarily require an undergraduate degree or an admissions test; and, if
an admissions test is required, the score need not be as competitive as for U.S.
schools.
• Some foreign medical schools can be highly selective in their admissions though
they do not necessarily require the MCAT.
• Some foreign medical schools are for-profit institutions with shortened academic
timelines. Whereas U.S. medical school students typically complete degrees in
four years, students at some schools in the Caribbean can do so in under three.
Page 20 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
13
Background
Requirements for IMGs to Enter a Residency Program in the
United States
Because medical schools outside the United States and Canada vary in their
educational standards and curricula, ECFMG certification is designed to
assure residency program directors and the public that IMGs have met the
minimum standards of eligibility to enter such programs.
1
• To enter a U.S. residency training program, IMGs must first become
certified by the ECFMG whose requirements include:
1. While there is no limit on the number of times a student may take an exam step, test-takers have seven years from the time they first pass a step to pass
all other steps required for certification.
2. The Foundation for Advancement of International Medical Education and Research currently lists more than 2,000 such institutions.
o Passing the first two (i.e. Step 1, Step 2CK and Step 2 CS)
of the three steps of the U.S. medical licensing exam.
1
o Showing evidence of a medical degree from a recognized
medical school.
2
Page 21 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
14
Background
The Steps of the U.S. Medical Licensing Exam
The following exam steps can be taken while attending medical school abroad:
• Step 1 uses a multiple-choice format to assess knowledge and application of
basic science concepts in the practice of medicine.
• Step 2 Clinical Knowledge (CK) uses a multiple-choice format to assess
knowledge of clinical science principles.
• Step 2 Clinical Skills (CS) tests students ability to examine and interact with
patients and colleagues.
The final step of the licensing exam is often taken during residency.
1
• Step 3 uses multiple-choice items and computer-based simulations and provides
a final assessment of a physician’s ability to assume independent delivery of
general medical care.
1. According to ECFMG officials, a number of states allow physicians to take Step 3 prior to entering a residency program and a significant
number of IMGs do so.
Page 22 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
15
Background
Discipline and Malpractice
Physicians—whether educated in the U.S. or abroad—who are licensed to
practice, may be subject to various disciplinary actions taken through state
medical boards, or hospitals, and other medical providers.
o License actions: revocations, suspensions, or other restrictions on a
physician’s license based on a review by state medical boards.
o Malpractice
1
: a finding of negligent care, related to services that a physician
provided or failed to provide.
1. Research indicates that malpractice data are of limited value as an indicator of competence or negligence. Possibly no more than 3 percent of medically
adverse events result in malpractice claims. Moreover, of those that do, an estimated 40 percent are found not to have involved error or injury.
Page 23 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
16
Loans to U.S. Medical Students Abroad Were Concentrated at
Free-standing Medical Institutions
Between 1998 and 2008, a total of 137 foreign medical institutions in 31
countries participated in the FFEL program during at least one academic year.
• School participation has remained relatively constant.
• As of 2008, there were 113 schools.
• Of these, 21 were free-standing medical institutions and the rest were
component schools.
1
From 1998 to 2008, U.S. students borrowed $1.5 billion to study medicine at
the free-standing institutions.
2
• Of that amount, about $1.3 billion (about 90 percent) went to students
at three Caribbean schools (American University of the Caribbean,
Ross University and St. George’s University).
Finding 1: Student Loans at Foreign Medical Schools
1. Free-standing institutions are schools whose principal offering is medical education; whereas, component medical institutions are medical
schools within a larger university system.
2. About another $1 billion was borrowed by students to study at component schools. However, because Education does not capture loan
data by academic discipline, it is unclear what portion of that amount was used to study medicine as opposed to other academic
disciplines.
Page 24 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
17
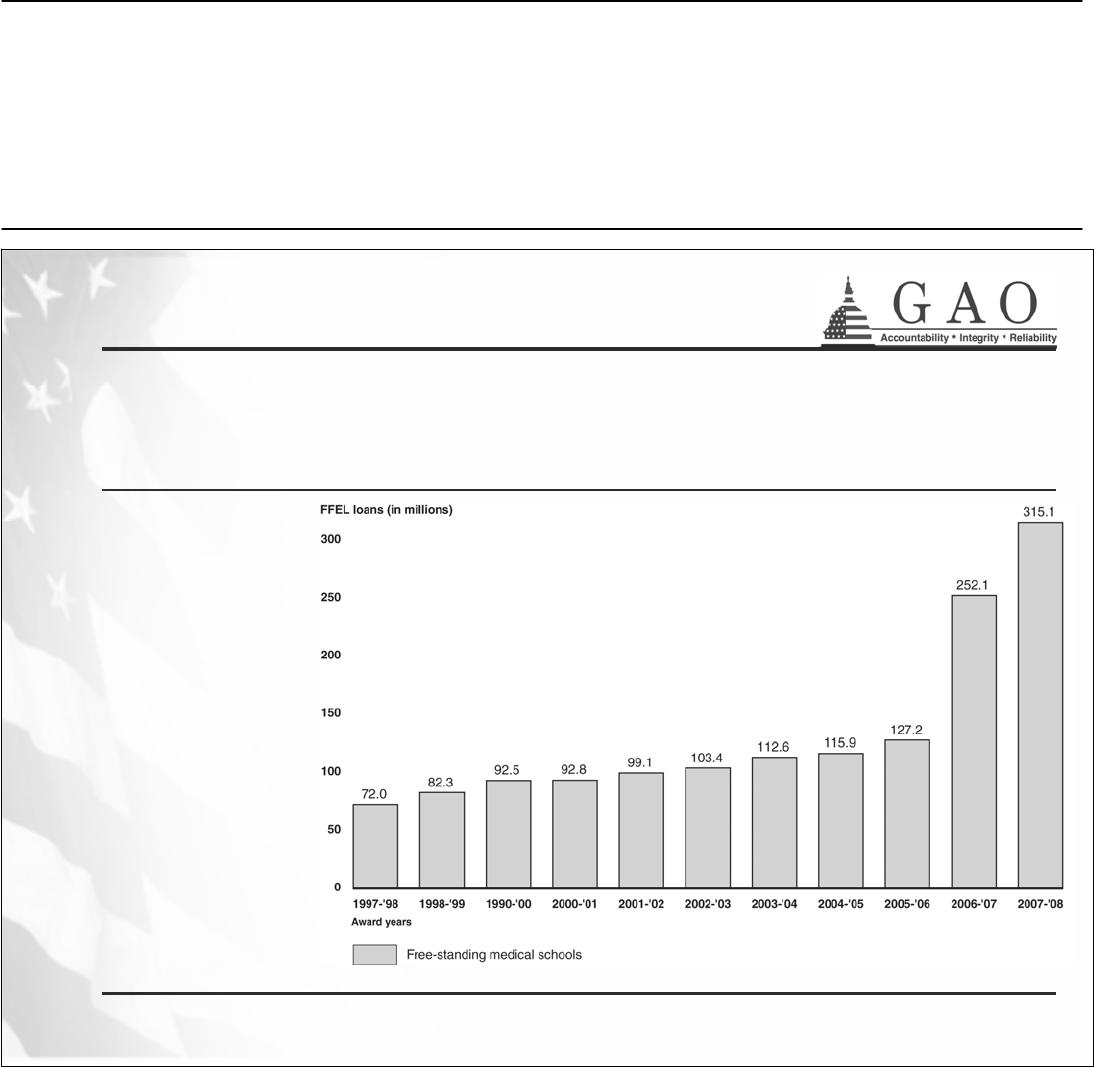
Borrowing at Foreign Medical Schools Has Steadily
Increased Since 1998
Since 1998,
loans at free-
standing schools
grew by 338
percent
compared with a
154 percent
increase in the
FFEL program
overall.
School officials
we met with
attributed loan
growth to
increases in
tuition,
enrollment, and
the introduction
of graduate and
professional
loans in 2006.
Finding 1: Student Loans at Foreign Medical Schools
Source: GAO analysis of Department of Education data
Page 25 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
18
Importance of Federally Guaranteed Student Loans
Of the students who participated in our focus groups, many reported that they relied
heavily on federal student loans to fund their medical education abroad. The majority
were most likely to categorize federal loans as very important in contrast to other forms
of financial assistance, both private and public.
1
• While little is known about the debt burden accumulated by IMGs, focus
group participants we interviewed projected their student loan debt would
range from $90,000 to $250,000 for their medical degree alone.
2,3
• Officials at the foreign medical schools we visited reported total student costs
ranging from just over $30,000 to about $90,000 per year. Most of the tuition
and fees reported by schools fell within the range of average cost for U.S.
medical schools.
Finding 1: Student Loans at Foreign Medical Schools
1. The findings obtained from our student focus groups cannot be generalized to the student population of international medical graduates.
2. Students participating in the student focus groups did not always indicate whether the loan funds borrowed were federal student loans or
private loans.
3. According to the Association of American Medical Colleges, students enrolled in U.S. medical schools incur about $155,000 in student
loan debt for their medical degrees.
Page 26 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
19
Some Focus Group Participants Reported That They Lacked
Reliable Information on Likely Loan Debt and Institutional
Performance
• Some students who participated in our focus groups said that when making their
initial selection of schools, they lacked a centralized source of reliable information
about their likely medical student loan debt or institutional performance such as
graduation rates.
• Many focus group participants said they relied on student-driven websites to guide
their decision-making.
• According to ECFMG officials, IMG oriented websites can vary in both accuracy and
sophistication. Students lack sources that are objective and factual.
Finding 1: Student Loans at Foreign Medical Schools
Comparison of
Sources Available for
Decision-making by
U.S.-educated
students and IMGs
Source:
GAO analysis of U.S.
Department of Education,
association, and
independent websites.
No known reliable sourcesMedical college associationMedical School Loan Debt
No known reliable sourcesMedical college associationGraduation Rates
Multiple school websites and
student-led electronic
bulletin boards
Centralized medical college
association website which
allows comparison of
several school websites
Admission Requirements
IMGsU.S. Medical Students
Known Sources Available…
Page 27 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
20
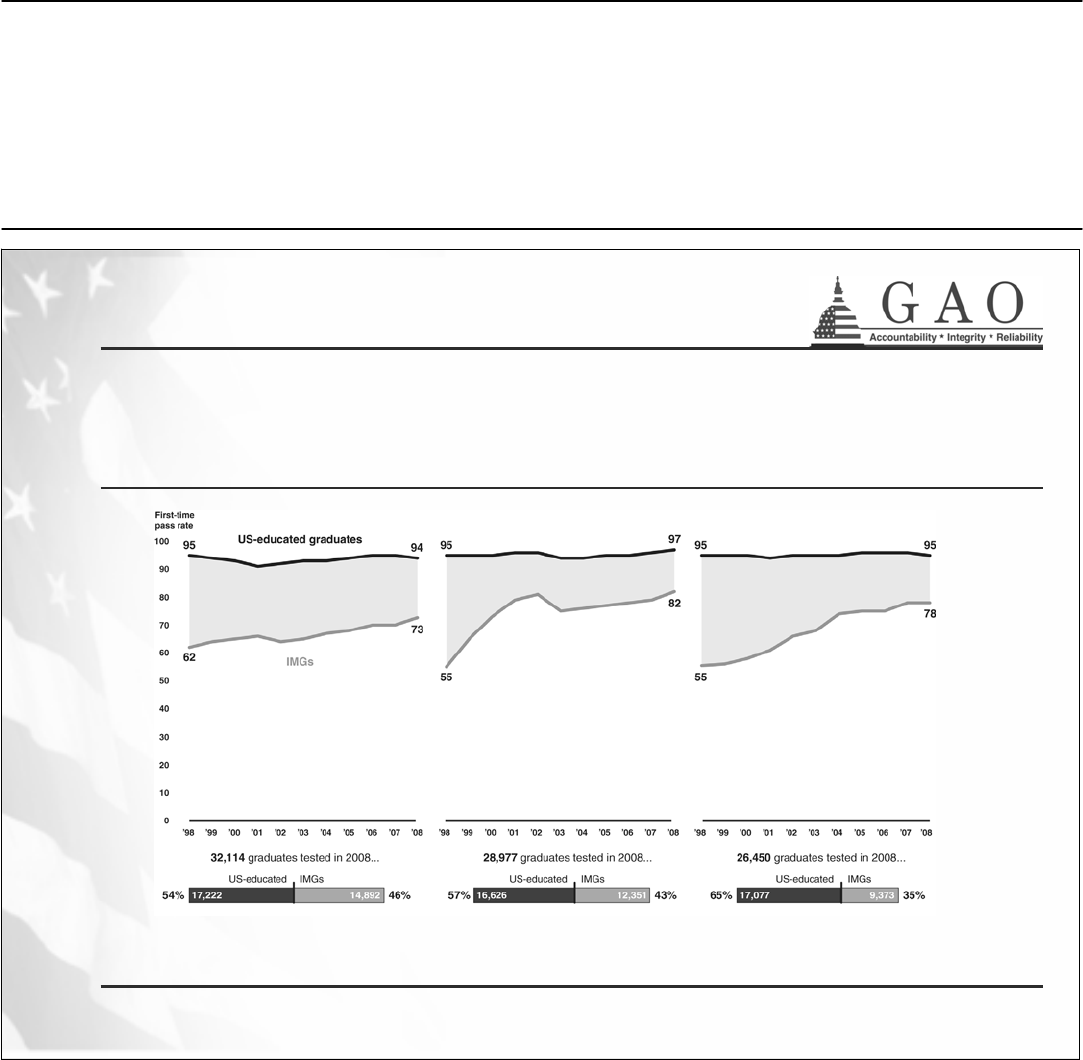
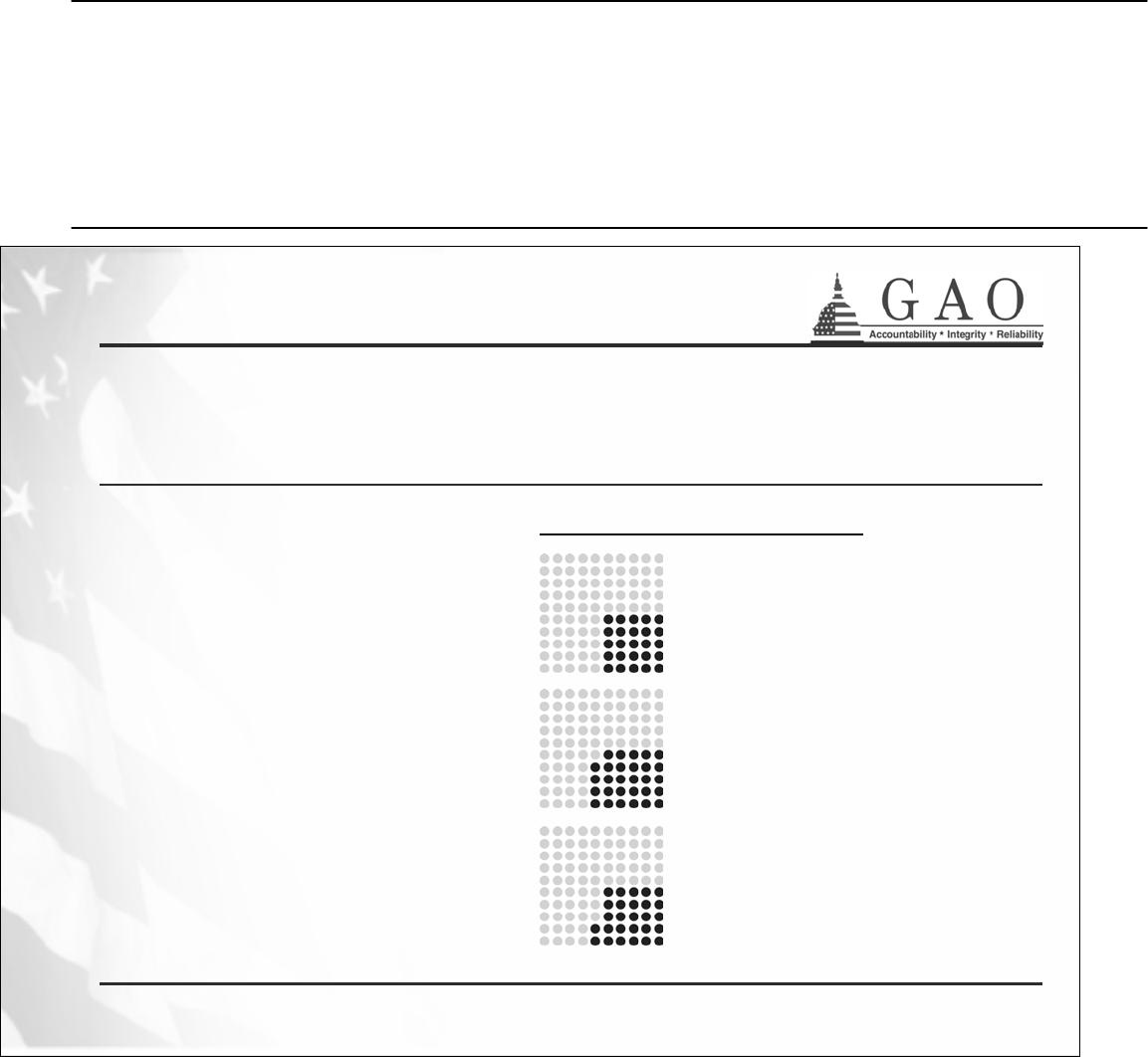
Pass Rates for All IMGs Have Improved on Most Licensing
Exam Steps But Still Lag Behind Those of U.S.-Educated
Graduates
Finding 2: U.S. Medical Licensing Exam Pass Rates
Step 1 (on basic science), 1998-2008 Step 2 Clinical Knowledge, 1998-2008
Source: GAO analysis of Educational Commission for Foreign Medical Graduates and National Board of Medical Examiners data.
Notes: IMGs include both U.S. citizens and citizens of other countries. As such, IMG pass rates reflect performance for individuals who may or may not have
received federal student loans. All test-takers are referred to as “graduates”; however, students are eligible to take the Step 1, Step 2 clinical knowledge, and
Step 2 clinical skills exams while they are still enrolled in medical school.
Step 3 (on delivery of general medical care), 1998-2008
Page 28 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
21
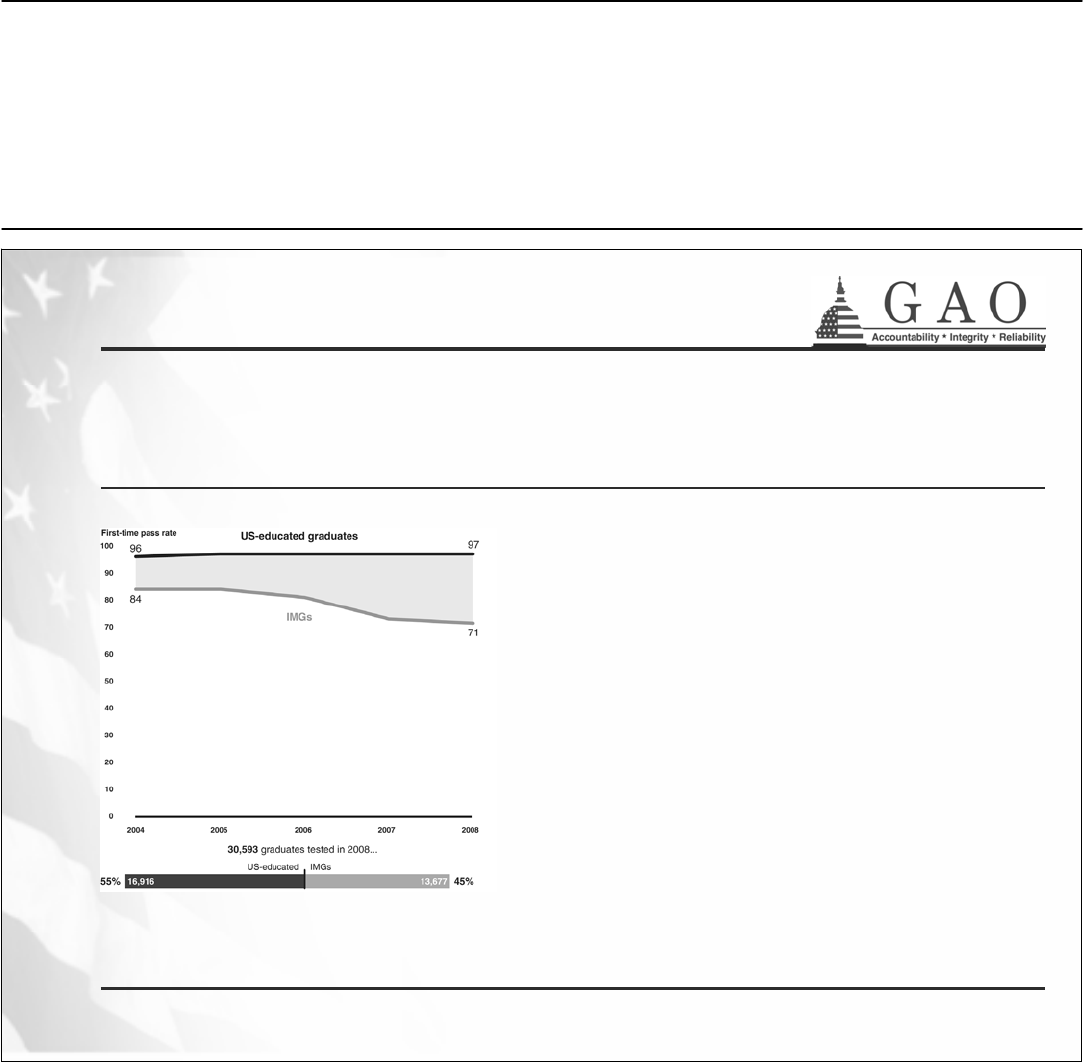
Despite Improvements, IMG First-Time Pass Rates on the
Step 2 Clinical Skills Exam Have Declined
Officials from the two organizations
that maintain licensing exam data told
us that IMG pass rates on the clinical
skills exam, offered since 2004, may
have declined in recent years due, in
part, to increases in the minimum
requirements for passing the exam.
Finding 2: U.S. Medical Licensing Exam Pass Rates
Step 2 Clinical Skills, 2004-2008
Source: GAO analysis of Educational Commission for Foreign Medical Graduates and National Board of Medical Examiners data.
Notes: IMGs include both U.S. citizens and citizens of other countries. As such, IMG pass rates reflect performance for individuals who may or may not have
received federal student loans. Test-takers are referred to as “graduates”; however, students are also eligible to take the Step 2 clinical skills exam. The Step
2 clinical skills exam became a certification requirement on June 14, 2004. Thus, pass rate data for this exam are available only for exam year 2004 and
onward. Prior to that, ECFMG administered the Clinical Skills Exam, starting in July 1998, as a requirement for certification.
Page 29 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
22
IMGs Needed More Attempts to Pass Licensing Exams than
U.S.-Educated Graduates
• IMGs have needed more attempts to pass the licensing exams than their U.S.-
educated counterparts. However, pass rates on additional attempts were lower than
initial attempts for both IMGs and U.S.-educated students. About 27 percent of IMG
test-takers repeated exams during the last ten years, compared to about 6 percent
of U.S.-educated test-takers.
o In 2008, 4,833 IMGs repeated the Step 1 exam at least once and 42 percent
passed on the repeated attempt.
o In the same year, 1,182 U.S.-educated graduates repeated the Step 1 exam at
least once and 69 percent passed on subsequent attempts.
• According to researchers, test takers who require multiple attempts to pass the
licensing exams will likely have difficulty being selected for a residency because they
are viewed by some as less qualified as those passing the exams on their first try.
Finding 2: U.S. Medical Licensing Exam Pass Rates
Page 30 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
23
Factors That May Affect IMG Pass Rates: Limited English
Proficiency and Institutional Focus on U.S. Licensing Exams
• Research indicates that English language proficiency may affect IMGs’ exam
performance on the clinical skills exam, especially in gathering data, sharing
information, and establishing rapport with patients.
1
• Research and experts suggest that other factors are the extent to which exam
preparation is incorporated into a medical school’s curriculum and the proportion of
the school’s students taking the exam.
o Although passing the licensing exam is critical for those seeking to practice in
the U.S., not all schools focus on this as a part of their program.
o Focus group participants at the two European schools we visited told us that
faculty provided limited assistance in exam preparation. Officials at both
schools told us they would provide additional test-preparation support for their
students.
o At the three Caribbean schools we visited, there was significant focus on
preparing students for the exam. Institutional policies at two of the three
schools precluded students from taking the exam if they were not ready and
required successful performance on the exam in order to graduate.
Finding 2: U.S. Medical Licensing Exam Pass Rates
1. According to one study, although research indicates that IMGs who are U.S. citizens are more likely than foreign IMGs to claim English as
a native language and to have received medical school instruction in English, nearly 30 percent of U.S. citizen IMGs are non-native English
speakers. See Boulet, John R., et al, “U.S. Citizens Who Obtain Their Medical Degrees Abroad: An Overview, 1992-2006,” Health Affairs,
vol. 28, no.1 (2009).
Page 31 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
24
Other Factors May Also Explain Lower Pass Rates for IMGs
Who Were U.S. Citizens
• Experts we interviewed suggested that some U.S. citizen IMGs may lack the test-
taking skills of their U.S.-educated counterparts.
• Several focus group participants we spoke with told us that their lower MCAT scores
made them less competitive when applying to U.S. medical schools.
o According to data from the Association of American Medical Colleges, fewer
than one third of 2005-2007 applicants with MCAT scores below 30 were
accepted to U.S. medical schools.
1
• Several focus group participants we spoke with told us that they entered foreign
medical school from other disciplines or applied to medical school years after
finishing college, suggesting that they did not follow the traditional academic
pathway to medical school and may not have had the same exposure to medical
concepts as other students.
Finding 2: U.S. Medical Licensing Exam Pass Rates
1. The highest possible score for all students is 45.
Page 32 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
25
Education Has Not Been Able to Fully Enforce the Pass Rate
Requirement
The three private organizations that administer the licensing exams have not released
their data to schools or to Education on grounds that the information is proprietary and
should not be used for marketing purposes.
• As a result, Education has not been able to collect such data from the schools.
• Education officials said that since federal student loans to foreign medical
schools comprise less than 1 percent of all student loans, they use a risk-based
approach to monitor compliance with the pass rate requirement. They request
the data from schools
1
only when schools:
o apply to participate in the loan program,
o seek recertification for participation—at intervals between 1 to 6 years, or
o change institutional ownership.
• When schools did provide the data, however Education officials noted that they
could not independently verify it.
Finding 3: Monitoring of Licensing Exam Pass Rates
1. Department officials told us that in 2004, when they requested pass rate data from schools, they received data back only sporadically.
Between 1998 and 2008, only one school has lost eligibility based on the pass rate data it provided to Education. Fourteen other schools
have lost eligibility due to not meeting other program rules. Education officials stated that foreign medical schools have been able to obtain
student consent agreements for pass rate data on Steps 1 and 2.
Page 33 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
26
Schools Are Beginning to Negotiate for the Data and Education
Has Recently Reconsidered Its Approach to Enforcement
y
Recently two of the three testing organizations have begun to negotiate, on a
school-by-school basis, to provide the data to schools, which may allow schools to
systematically prove that they are satisfying the pass rate requirement.
o These organizations administer and/or govern Step 1, Step 2CS, and Step 2CK
of the medical licensing exam.
• Education told us that the department will soon fully enforce the pass rate
requirement by requesting schools to provide exam data on an annual basis, but did
not elaborate on how and when it would implement this new approach.
• However, a spokesperson for the testing organization that administers Step 3 said
that the organization would not be entering into such agreements with schools
because it shares exam data only with state medical boards.
• While the National Committee for Foreign Medical Education and Accreditation
recommended the inclusion of Step 3 as part of this requirement, Education officials
indicated that they would not request these data because the testing organization
that administers Step 3 is not specifically covered by the pass rate requirement.
1
Finding 3: Monitoring of Licensing Exam Pass Rates
1. The statutory and regulatory pass rate requirement applies only to examinations administered by ECFMG, which are Step 1 and Step 2. 20
U.S.C. § 1002(a)(2)(A)(i)(I)(bb); 34 C.F.R. § 600.55(a)(5)(B). Because Step 3 is administered by the Federation of State Medical Boards, it is
excluded from the pass rate requirement.
Page 34 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
27
According to our analysis
1
of 2008 institutional pass rate data:
At 60 percent:
A majority (58 percent) of foreign medical schools met or exceeded the current pass
rate requirement.
• For 6 countries, all 30 schools met the pass rate.
• For 3 countries, less than one-third of the 105 schools met the pass rate.
At 75 percent:
Only 24 of 218 schools with test-taking students (or 11 percent) would meet the
newly enacted pass rate were they to post the same performance as in 2008
.
•
Two of the five schools statutorily exempt from the requirement, but which
account for over 50 percent of federal student loans, would not meet the new
standard.
Finding 4: Performance on Institutional Pass Rates
1. The data we obtained from ECFMG and NBME did not allow for the identification of individual schools, but allowed us to look at institutional
performance by country. Because school identities were masked, we could not differentiate between federal loan participants and others. To
the extent that not all schools participated in the federal loan program, our results may be overstated. Our analysis was based on individuals
who took the exam. Because we could not estimate the proportion of students who were allowed to take the exam, we could not identify the
extent to which scores may be overstated.
A Majority of Foreign Medical Schools Met the Pass Rate at 60 Percent
in 2008, But Very Few Would Do So at 75 Percent
Page 35 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
28
Institutional Pass Rates May Be Limited as a Measure of
School Quality
Testing officials cautioned against associating students’ performance on
medical licensing exams with institutional quality for the following reasons:
• Test-takers could be a school’s best or worst students.
• Some schools restrict who may sit for the exam based on student
readiness—thus inflating an institution’s score.
• Other schools may encourage “practice runs” for students who are less
prepared or have no restrictions on who sits for the exams—possibly
lowering institutional scores.
• Performance on Step 3 of the exam—which may occur during residency
training in the U.S.—has little to do with attending school abroad.
1
Additionally, according to some school officials, institutions with small numbers
of test-takers may find it hard to meet the pass rate requirement.
2
1. According to ECFMG officials, a number of states allow graduates to take Step 3 prior to entering a residency program and a significant
number of IMGs do so.
2. Education officials agreed with this assessment and reported to us that they are proposing regulations that would make special provisions for
foreign medical schools that enroll small numbers of U.S. citizens by asking them to provide the data only when the pass rate is based on at
least 8 or more students who took the exam.
Finding 4: Performance on Institutional Pass Rates
Page 36 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
29
Some Schools Have Expressed Concerns About the 75
Percent Rate
Some school and medical association officials we interviewed expressed the
view that the new pass rate could discourage loan program participation:
• They noted that because some non-profit institutions are “highly
selective” and only admit small numbers of U.S. students each year,
these schools would find it burdensome and not cost effective to meet
the terms of the provision.
• They also expressed concern that their pass rate performance, given
small numbers of test-takers, would misrepresent the quality of their
program if the school lost eligibility to participate.
1
Finding 4: Performance on Institutional Pass Rates
1. Education officials reported to us that they are proposing regulations that would make special provisions for foreign medical schools that
enroll small numbers of U.S. citizens.
Page 37 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
30
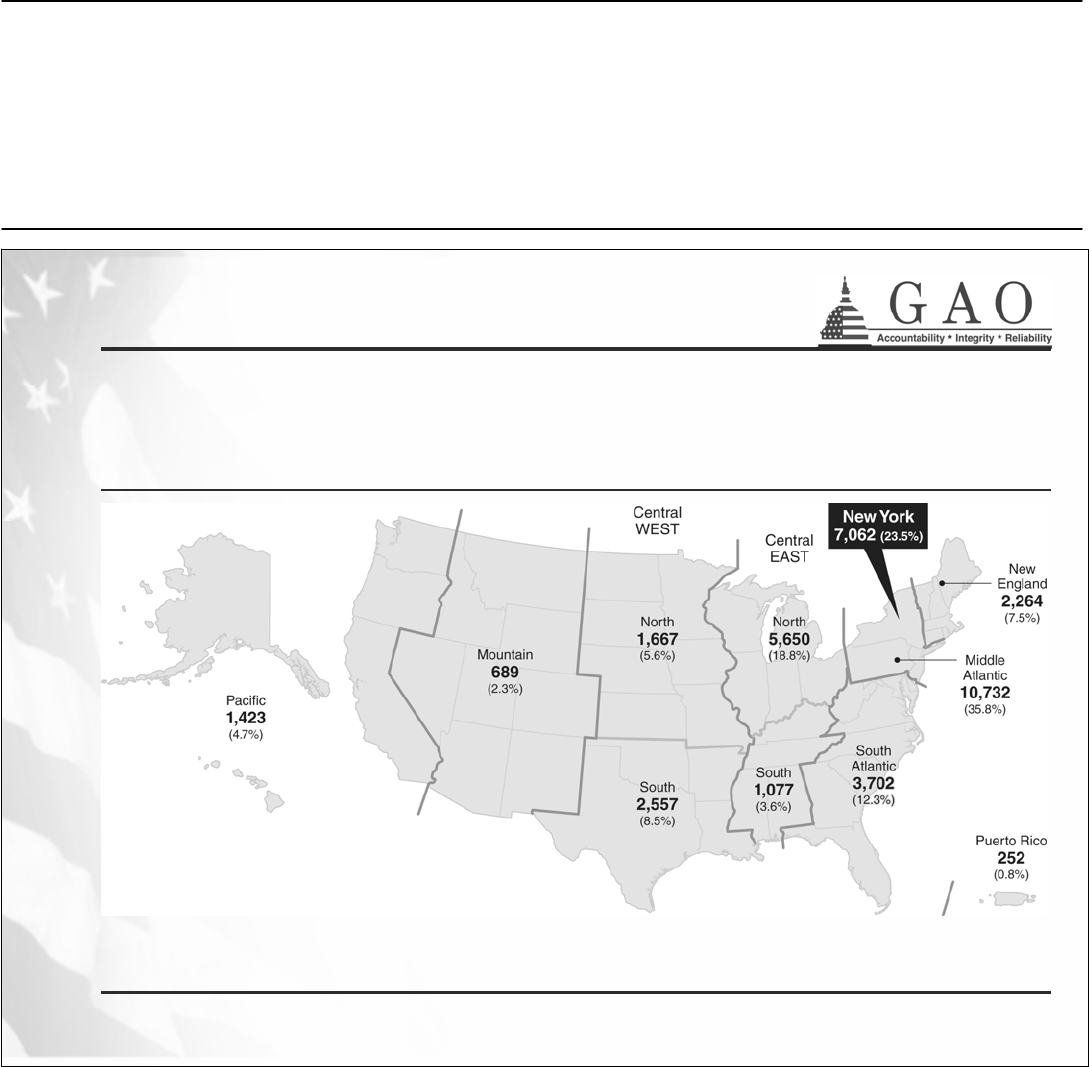
In 2008, a
bout 30,000 IMGs Were in Residencies in the U.S., with 78
Percent of All IMGs Located East of the Mississippi River and 24
Percent in New York Alone
Finding 5: Residencies and Practice
Source: GAO analysis of Accreditation Council for Graduate Medical Education (ACGME) academic year 2008-2009 data.
Note: The geographic location of IMGs in residencies is partly determined by the availability of residency slots in the United States each year.
The map depicts geographic areas as defined by ACGME.
Page 38 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
31
More IMGs than U.S.-Educated Graduates Go into Primary Care-
Related Residencies, And This Pattern Continues into Practice
Source: GAO analysis of ACGME data.
Note: The number of primary care residency slots is determined, in part, by funds available through Medicare payments to hospitals and other
teaching institutions.
Finding 5: Residencies and Practice
Number and percentage distribution of U.S.-educated graduates and IMGs in entry-level residencies,
academic year 2008-09
Page 39 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
32
After completing residencies, some IMGs practice medicine in medically underserved
areas, but it is not known to what extent they do so or whether they are more likely than
U.S.-educated graduates to serve in these areas.
• There are some programs designed to channel foreign physicians into
geographic areas with a shortage of health care professionals.
o The “Conrad 30” J-1 visa waiver allows physicians on Exchange Visitor
(J-1) visas to remain in the U.S. after completing residency, if they agree
to practice for at least three years in an area that is federally designated
as having a healthcare professional shortage.
o These waivers must be requested by a state or federal agency and states
can request such waivers in order to retain foreign physicians for such
designated areas.
Some IMGs Practice in Underserved Areas
Finding 5: Residencies and Practice
Page 40 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
33
Some IMGs Practice in Underserved Areas (continued)
Although J-1 visa waivers for foreign IMGs have been a federal and state
strategy to encourage physicians to practice in underserved areas, HHS,
which defines these areas and coordinates programs for addressing physician
shortages, does not officially collect data on waivers granted or on
placements for physicians who are granted waivers.
1
• According to one estimate, more than 700 foreign IMGs were awarded J-1
visas waivers in 2008 to practice in underserved areas.
2
1. GAO recommended in 2006 that HHS collect and maintain data on waiver physicians in order to better address physician shortages.
According to an official at HHS’ Health Resources and Services Administration, as of September 2008, no action had been taken by HHS
regarding this recommendation. See GAO,
Foreign Physicians: Data on Use of J-1 Visa Waivers Needed to Better Address Physician
Shortages,
GAO-07-52 (Washington, D.C.: Nov. 30, 2006).
2. The Texas Primary Care Office surveys all states annually on their requests for J-1 visa waivers.
Finding 5: Residencies and Practice
Page 41 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
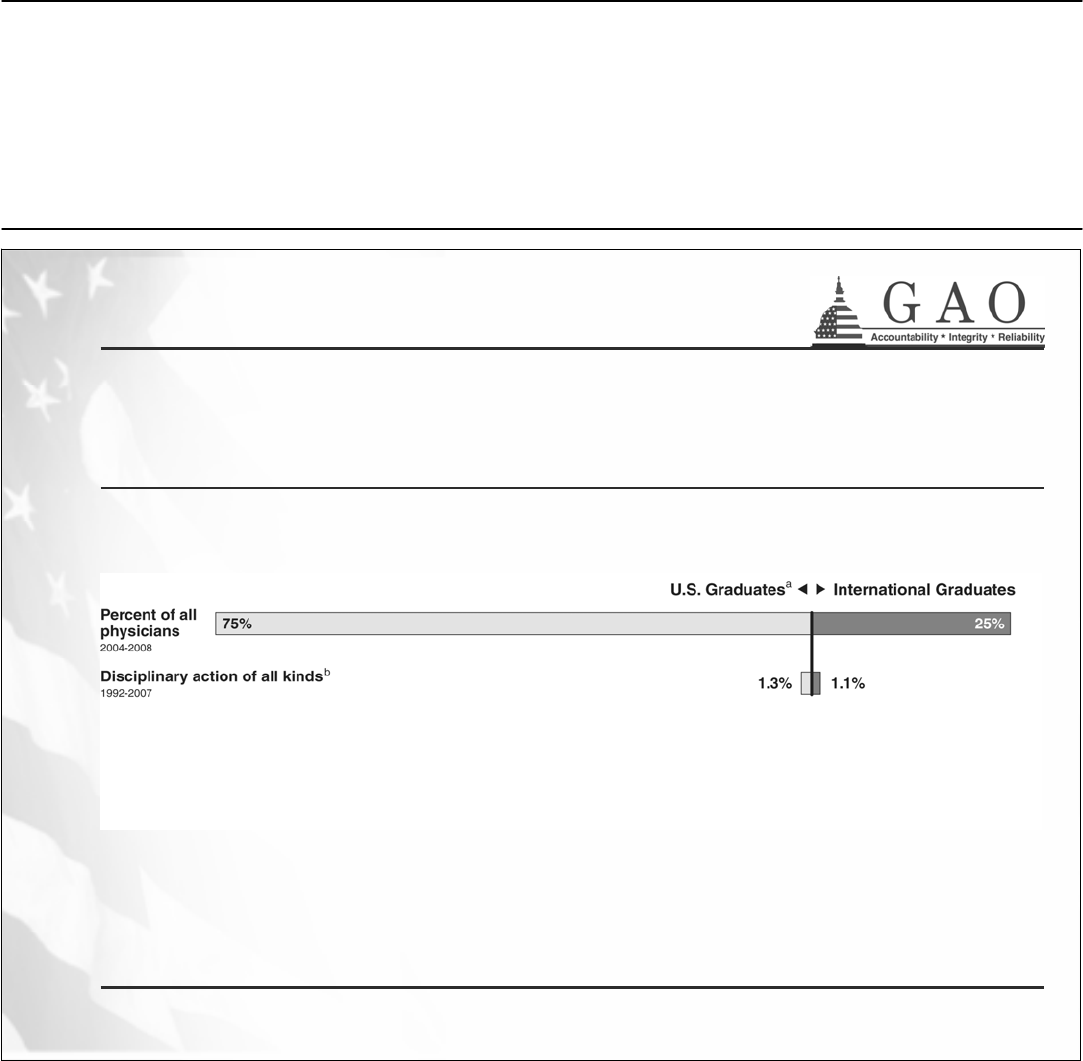
34
Rates of Disciplinary Action Are Low for Physicians Overall,
Both for IMGs As A Group And for U.S.-Educated Graduates
Finding 6: Discipline and Malpractice
Source: Data on percentage of all physicians by IMG and U.S.-educated status: American Medical Association (AMA) Physician Master File
data as analyzed and reported by the Association of American Medical Colleges (AAMC) for 2004 to 2008; discipline data: Federation of
State Medical Boards (FSMB) data prepared for the U.S. Department of Education for 1992-2007.
Notes: a) Canadian medical graduates are counted as U.S. medical graduates for all analyses.
b) “Disciplinary actions” includes license revocations, suspensions, restrictions, and other actions, though not malpractice cases.
Page 42 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
35
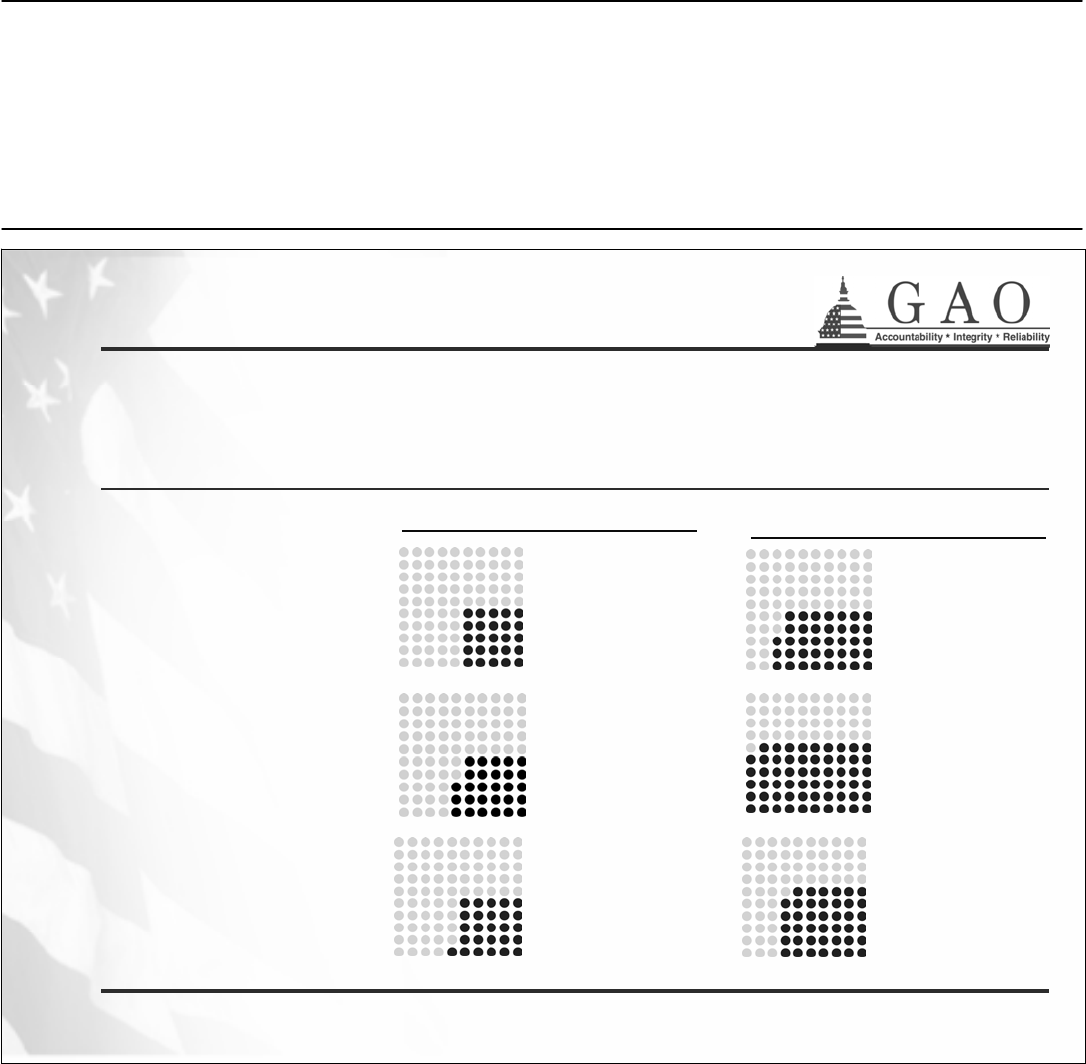
There Are No Significant Differences Nationwide with Regard to
License Revocation and Suspension
Finding 6: Discipline and Malpractice
Source: Data on percentage of all physicians by IMG and U.S.-educated status were obtained from AMA Physician Master File data as
analyzed and reported by the AAMC. License revocation and suspension data were obtained through GAO analysis of FSMB data.
Note: Canadian medical graduates are treated as U.S. medical graduates for all analyses.
National data on license
revocations and suspensions
for the most recent five years
with complete data show that,
while all IMGs represented
about one-quarter of all
physicians, they accounted for
a somewhat larger share of
these disciplinary actions.
These differences were not
statistically significant when
compared to the same
disciplinary actions experienced
by U.S.-educated physicians.
IMGs made up
25 percent of all
physicians in
the U.S. from
2004 to 2008…
… yet accounted
for 29 percent
of license
revocations …
…and
27 percent
of license
suspensions.
NATIONWIDE
(2004 to 2008)
Page 43 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
36
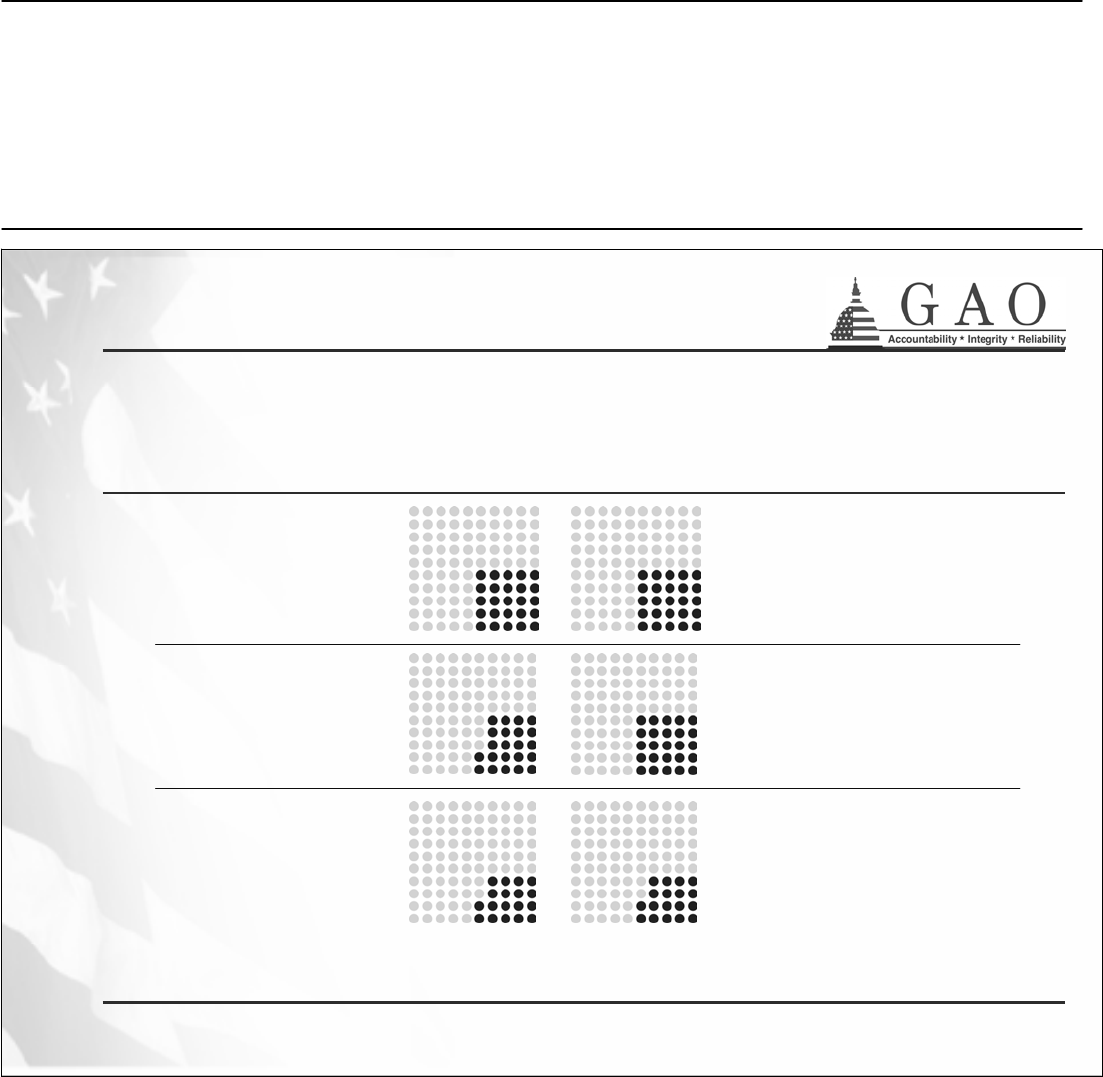
Similarly, for Two Key States, There Are Few Significant
Differences
Finding 6: Discipline and Malpractice
Source: GAO analysis of state license revocation and suspension data, AMA Physician Master File data analyzed and reported by the AAMC.
Note: Canadian medical graduates are treated as U.S. medical graduates for all analyses.
Data from two states
with large numbers of
IMGs generally reflect
the national pattern.
However, our analysis
found significant
differences between all
IMGs and U.S.-
educated physicians in
Florida with respect to
license revocations.
State officials told us
they did not know the
reasons for these
differences.
IMGs made up 25
percent of
physicians from
2004 to 2008,
which is also the
US average…
… yet accounted
for 28 percent
of state license
revocations …
…and
26 percent
of the state’s
license
suspensions.
IMGs made up
38 percent of
physicians, which
is higher than the
U.S. average…
… yet accounted
for 59 percent
1
of state license
revocations …
…and
41 percent
of the state’s
license
suspensions.
CALIFORNIA
(2004 to 2008)
FLORIDA
(2004 to 2008)
1. Denotes a statistically significant difference.
Page 44 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
37
Nationwide, IMGs Did Not Account for A Disproportionate
Share of Malpractice Payments in 2004-2008
1
1. Our analysis of malpractice payments is generally consistent with prior work by GAO and others. See Medical Malpractice: Characteristics of Claims Closed in1984,
HRD-87-55, (Washington, D.C.: April 1987), and S. Mick and M. Comfort, “The Quality of Care of International Medical Graduates: How Does It Compare to That of
U.S. Medical Graduates?” Medical Care Research and Review, Dec. 1997.
2. U.S.-educated OB/GYNs were significantly more likely to have had a malpractice payment during this period than IMG OB/GYNs.
All Physicians
IMGs made up 25 percent
of all U.S. physicians from
2004 to 2008…
… and IMGs accounted for
25 percent of U.S. physicians
with reported multiple malpractice
payments from 2004 to 2008.
Surgeons
IMGs made up 22 percent
of all surgeons working in
the U.S. in 2007…
… and IMGs accounted for
25 percent of U.S. surgeons
with reported malpractice payments
from 2004 to 2008.
Obstetricians/
Gynecologists
IMGs made up 17 percent
of all OB/GYNs working in
the U.S. in 2007…
… and IMGs accounted for
18 percent
2
of U.S. OB/GYNs
with reported malpractice
payments from 2004 to 2008.
.
Finding 6: Discipline and Malpractice
Source: GAO analysis of data reported to the National Practitioner Data Bank.
Note: Percentages have been rounded to nearest whole percentage point. Canadian medical graduates are treated as U.S. medical graduates for all analyses. Malpractice
payments are payments made as a result of a settlement or judgment based on the provision or failure to provide health care services.
Page 45 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
38
Research on IMG Performance Is Limited
Few research studies have compared performance of IMGs with that of U.S.-educated
graduates beyond disciplinary actions, such as on their clinical processes and patient
outcomes.
1
• A 2004 study found IMGs were as likely as other physicians to follow
professional standards.
• A 1991 study found little difference in outcomes for mortality or length of
hospital stay for 16 different medical and surgical conditions.
• A 1990 study found that certain IMGs had higher rates of complications for a
particular surgical procedure.
In addition, a 2004 California study found that of three characteristics—age, gender,
and IMG status—IMG status had the weakest relationship to the likelihood of
professional discipline.
Finding 6: Discipline and Malpractice
1. These studies were among the most recently available research studies conducted on this subject.
Page 46 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
39
Conclusion
While only a very small proportion of all federally guaranteed student loans goes to U.S.
students to study medicine at foreign schools, it does not diminish the valuable role this
funding plays.
• For individual Americans, the loans represent the single most important avenue
available to finance their medical education—without which, they would not
become physicians.
• For the nation as a whole, these loans help assure a steady supply of the U.S.
physician workforce. The fact that foreign educated doctors, including U.S.
citizens, are more likely than their domestically educated peers to practice primary
care medicine fulfills an ever-increasing demand for such physicians.
However, in contrast to those pursuing a domestic medical education, U.S. students
seeking overseas study are at a considerable disadvantage as consumers, given the
absence of reliable information about foreign medical schools—such as their graduation
rates or cost. Yet, the Higher Education Opportunity Act emphasizes the importance of
consumer-based choices.
Page 47 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
40
Conclusion
For policymakers, meanwhile, Education has yet to fully enforce compliance with the
pass rate required for foreign medical schools to participate in the federal loan program
since verifiable data have not been available.
Moreover, while foreign medical schools may soon be able to negotiate access to their
students’ scores, it still remains to be seen whether a specific pass rate is a useful
measure of quality, and, until further evaluation, whether a pass rate of 75 percent is
appropriate.
• Our own analysis of exam scores by country suggests that the new pass rate
requirement may dissuade or even disqualify many schools from participating in
the loan program.
• Such an outcome, would, in turn, severely narrow the choices for U.S. students
who are prepared to undertake the long and difficult road to medical practice.
Page 48 GAO-10-412 Foreign Medical Schools
Appendix I: Briefing Slides
41
Recommendations
To enhance information available for prospective students of foreign medical schools
and strengthen monitoring of foreign medical schools participating in the federal student
loan program, we recommend that the Secretary of Education:
• Collect consumer information, such as aggregate student debt level and
graduation rates, from foreign medical schools participating in the federal
student loan program as recommended by the National Committee on Foreign
Medical Education and Accreditation and make it publicly available to students
and their families;
• Require foreign medical schools to submit aggregate institutional pass rate data
to the Department annually;
• Verify data submitted by schools, for example by entering into a data sharing
agreement with the testing organizations;
• Evaluate the potential impact of the newly enacted 75 percent pass rate
requirement on school participation in the federal student loan program and
advise Congress on any needed revisions to the requirement.
Page 49 GAO-10-412 Foreign Medical Schools
Appendix II: Objectives, Scope, and
Methodology
Appendix II: Objectives, Scope, and
Methodology
Our review focused on the following questions: (1) What amount of federal
student aid loan dollars has been awarded to U.S. students attending
foreign medical schools? (2) What do the data show about the pass rates
of international medical graduates on license examinations? (3) To what
extent does Education monitor foreign medical schools’ compliance with
the pass rate required to participate in the federal student loan program?
(4) What is known about schools’ performance with regard to the
institutional pass rate requirement? (5) What is known about where
international medical graduates have obtained residencies in the United
States and the types of medicine they practice? (6) What is known about
discipline and malpractice involving foreign educated physicians?
With regard to the Federal Family Education Loan (FFEL) program,
program requirements allow only U.S. citizens, nationals, permanent
residents, and certain other eligible noncitizens to obtain these loans. In
view of this fact, our findings for the first objective were limited to U.S.
citizens, nationals, permanent residents, and certain other eligible
noncitizens who were also IMGs. By contrast, our findings pertaining to
the remaining objectives were based on all IMGs educated in medical
schools abroad, including those students who are U.S. citizens or residents
as well as students who are foreign nationals. For these objectives, we
included graduates of Canadian medical schools in the total population of
U.S. medical graduates. According to the body of literature we reviewed,
Canadian schools are generally not considered to be foreign medical
schools since their medical education system is closely comparable to that
of the United States. Similarly, we included graduates of Puerto Rican
medical schools in the total population of U.S. medical graduates because
medical schools in Puerto Rico are subject to the same accreditation
standards as other U.S. medical schools. In addition, our analyses
excluded students in and graduates of osteopathic programs because only
graduates of U.S. osteopathic schools are eligible to become licensed
physicians in the United States.
To determine the amount of federal student loan dollars borrowed abroad,
we analyzed the Department of Education’s loan data for all foreign
medical schools participating in the FFEL program between academic
years 1997-1998 and 2007-2008.
1
We also interviewed Education officials
Objectives
Defining International
Medical Graduates
Data Analysis by
Objective
1
These academic years were chosen because they coincide with reauthorizations of the
Higher Education Act of 1965.
Page 50 GAO-10-412 Foreign Medical Schools
Appendix II: Objectives, Scope, and
Methodology
about participation in the FFEL program as it relates to foreign medical
schools and their graduates. To aid our discussion on this matter, we
adopted the use of the department’s nomenclature (i.e., free-standing
institutions and component institutions).
2
We reviewed relevant federal
laws and regulations that specify the conditions for compliance with the
FFEL program. To understand how determinations of medical
comparability are made for foreign countries and the impacts on
institutional eligibility, we also observed a meeting of the Department of
Education’s National Committee on Foreign Medical Education and
Accreditation during September 2009. This committee is charged with
reviewing the standards that foreign countries use to accredit medical
schools to determine whether those standards are comparable to those
used to accredit medical schools in the United States. If a country is
determined to have comparable medical accreditation standards (i.e.,
comparable countries), then accredited medical schools in that country
may apply to participate in the FFEL program. Throughout this report we
refer to the federal student loan program in our findings. Where our
findings are specific to the FFEL program, however, we refer to that
program by name.
To determine the performance of IMGs on licensing examinations, we
analyzed medical licensing examination trend data covering the period
1998 through 2008. We interviewed officials of the Educational
Commission for Foreign Medical Graduates (ECFMG) and the National
Board of Medical Examiners (NBME) to better understand issues related
to licensing examination pass rates and international medical graduates.
We entered into an agreement with both of these institutions to obtain
their medical licensing examination data. To analyze student achievement
on medical licensing exams, we calculated pass rates by dividing the
number of test takers who passed an exam step by the number of test
takers who attempted this exam step in any given calendar year. We
excluded data from our analysis when information that identified country
and school location was missing. In addition, not all students who attend
foreign medical schools are allowed to sit for the exam. To the extent that
these students are not reflected in the total number of exam takers, our
findings may be overstated. We also interviewed external stakeholders
about factors that may affect IMGs’ pass rates on the licensing exam. In
2
According to Education’s definition, free-standing institutions are schools whose principal
offering is medical education in contrast to component medical schools that are part of a
larger university system.
Page 51 GAO-10-412 Foreign Medical Schools
Appendix II: Objectives, Scope, and
Methodology
addition, we reviewed literature on IMGs’ performance on the U.S. medical
licensing exam. We also obtained information at selected foreign medical
schools from administrators and students about efforts to prepare
students for the medical licensing exam.
To assess Education’s monitoring of foreign medical schools’ compliance
with the licensing examination pass rate requirement, we interviewed
Education officials about their monitoring activities and reviewed
proposed rule changes to these activities. Additionally, we interviewed
ECFMG and NBME officials about their efforts to share aggregate pass
rate data with schools. On the basis of pass rate data we obtained from
these organizations, we calculated the number of schools in comparable
countries whose pass rates met or exceeded the 60 percent requirement
for the 3-year period 2006 through 2008. Because school identities were
masked in the data we received, we could not differentiate those schools
that were FFEL participants from non-FFEL schools. We also looked
theoretically at schools’ performance on the medical licensing exam with
regard to a 75 percent pass rate using 2006 through 2008 data.
To determine where international medical graduates obtained residencies
and what medical specialties were practiced, we analyzed residency data
collected by the Accreditation Council for Graduate Medical Education.
We also interviewed HHS officials about geographic areas experiencing
physician shortages, and what is known about the extent to which IMGs
are practicing in these areas. We interviewed representatives of
organizations and a small number of private, for-profit businesses that
provide clinical and residency placement services to IMGs for a fee, as
well as officials in North Dakota and Texas, who were identified as key
information sources in the tracking of IMG residents in rural areas. We
identified, obtained, and reviewed previous research on IMGs, including
literature on geographic patterns of their field of practice, factors
influencing specialty choice, participation in certain visa programs, and
the extent to which IMGs practice in primary care and in underserved
areas as compared with U. S. medical graduates.
To determine what is known about discipline and malpractice involving
IMGs (i.e., physician discipline or license actions, as well as malpractice
claims), we obtained and analyzed data for the years 2004 to 2008 from the
Federation of State Medical Boards and HHS’s National Practitioner Data
Bank, as well as two states with high populations of IMGs (California and
Florida). In addition, we calculated odds ratios and conducted tests to
determine whether differences in discipline and malpractice rates between
IMGs and U.S. medical graduates were statistically significant. We
Page 52 GAO-10-412 Foreign Medical Schools
Appendix II: Objectives, Scope, and
Methodology
considered such differences to be significant if they had less than a 5
percent chance of occurring from chance or random fluctuations.
Disciplinary action or a malpractice payment
3
may occur throughout a
physician’s career. Because we did not analyze IMGs’ or U.S. medical
graduates’ experience of disciplinary action or malpractice payments by
age, date of medical school graduation, or date of licensure, the age
distribution of the physicians reflected in our analyses is unknown. Our
analysis of malpractice payments is limited to data reported to the
National Practitioner Data Bank. While a wide variety of entities are
required to report to the National Practitioner Data Bank—including state
medical boards, health care facilities, and insurance companies—our
analysis may nevertheless not reflect the full extent of medically adverse
events. In addition, while we analyzed malpractice payments, we did not
analyze the underlying cases to determine the extent to which they
involved error or injury. We interviewed officials from three states about
the licensing and discipline of physicians (California, Florida, and New
York). We also interviewed several experts knowledgeable about
physician discipline and malpractice litigation to determine what is known
about IMGs’ experience of these actions, and to better understand the
value and limitations of discipline and malpractice data. We identified,
obtained, and reviewed research on discipline and malpractice involving
IMGs, as well as research that examined the relationship between
malpractice and negligence, and research that compared IMGs with other
physicians on selected measures of performance, such as compliance with
professional standards.
Because external data were significant to each of our research objectives,
we assessed the reliability of the publicly and privately held data obtained
from federal departments, agencies, and associations.
4
To assess the
reliability of each data set, we administered an automated survey form to
each data manager or individual assigned primary oversight of the data.
Each survey was specifically tailored to the system in question and
addressed data uses, internal controls, and data entry practices. Once each
Data Reliability
3
Malpractice payments are a monetary exchange as a result of a settlement or judgment of
a written complaint or claim demanding payment based on a physician’s provision of or
failure to provide health care services, and may include, but is not limited to, the filing of a
cause of action, based on the law of tort, brought in any State or Federal Court or other
adjudicative body.
4
GAO, Assessing the Reliability of Computer-Processed Data, GAO-09-680G (Washington,
D.C.: July, 2009).
Page 53 GAO-10-412 Foreign Medical Schools
Appendix II: Objectives, Scope, and
Methodology
survey was completed, we reviewed responses to assess the adequacy of
the internal controls and processes in place. In addition, we also tested the
integrity of the electronic data we received by searching for possible
outliers in the data, invalid variable values, and duplicate records. We
determined that each data set was sufficiently reliable for the analytical
purposes of this report.
To supplement our data collection and analysis, we conducted site visits
to five foreign medical schools: American University of the Caribbean (St.
Maarten), Ross University (Dominica), St. George’s University (Grenada),
Royal College of Surgeons (Ireland), and Poznan University of Medical
Sciences (Poland). The schools were selected according to the following
criteria: (1) countries deemed to be comparable by the National
Committee on Foreign Medical Education and Accreditation with free-
standing medical schools, (2) number of free-standing medical schools
eligible to participate in the Federal Family Education Loan Program, as
defined by the Department of Education, and (3) 2008 loan volume for
these institutions, by country.
Institutional Site
Visits
For the site visits, we considered visits only to comparable countries with
free-standing medical institutions eligible to participate in the FFEL
program. The reason is that Education was not able to provide student
enrollment data that distinguishes medical school students from all other
academic disciplines at component medical schools. Therefore, by
considering only free-standing institutions, we were able to determine a
minimum number of medical school students who take out loans to attend
a given institution. According to data provided by Education, there are a
total of 21 free-standing institutions in 10 countries.
The schools visited in the Caribbean represented 3 of the 4 largest
institutions in terms of loan volume and students enrolled, and all were
for-profit schools. To provide institutional diversity, we also selected two
schools in Europe. While both institutions were not-for-profit, one school
was a public institution and the other was a private institution. Both
schools had smaller student loan volumes and enrollments than the
schools in the Caribbean.
At each selected school, we met with administrators and asked them to
solicit participation of students to participate in focus groups. We
conducted a total of eight focus groups that ranged in size from 4 to 14
participants. For each group, we specifically asked for U.S. citizens who
also were federal student loan borrowers. We also allowed a few non-
Page 54 GAO-10-412 Foreign Medical Schools
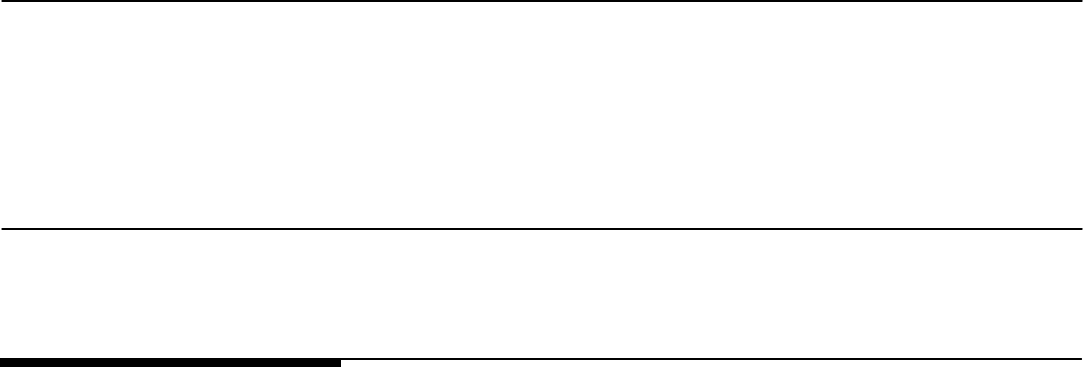
Appendix II: Objectives, Scope, and
Methodology
federal loan recipients as well as non-U.S. citizens to participate to provide
additional perspective. A summary of focus group participants’ responses
captured during the focus groups can be found in appendix VI.
We also reviewed literature published from 1990 to 2009 that included
research articles identified through 11 databases such as ERIC, PsycINFO,
and Wilson Social Sciences Abstracts. To examine trends in students
pursuing medical school abroad, we searched “foreign, medical school,”
“foreign medical graduates,” “trends, physician supply,” and other such
terms. To examine the factors that influence international medical
students’ performance on medical licensing exams, we searched terms
such as “U.S. medical licensing exam,” and “licensing.” We also reviewed
relevant articles from the annual medical education issue of the Journal of
the American Medical Association. We also included in our review
articles that were identified by government officials and representatives of
professional associations we interviewed. Our bibliography can be found
at the end of the report.
Literature Review
Page 55 GAO-10-412 Foreign Medical Schools
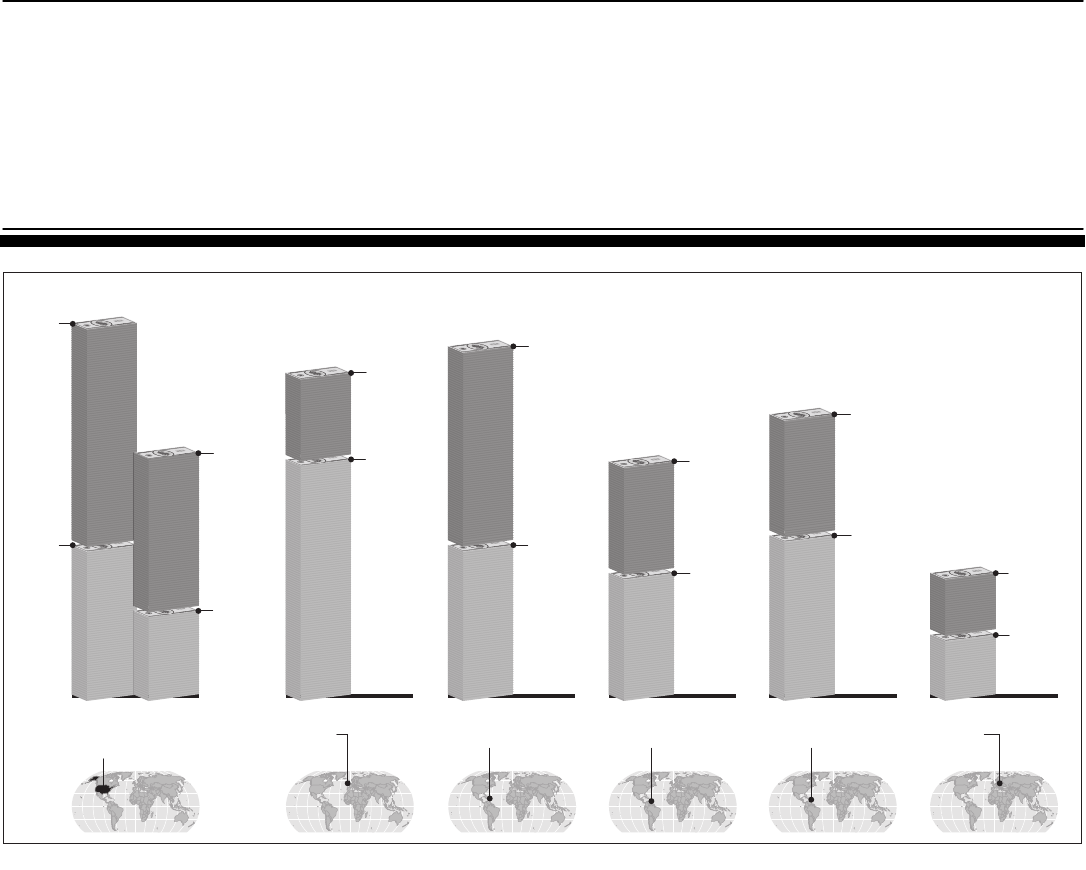
Appendix III: Compariso
Attendance
Medica
n of Average Cost of
at U.S. and Selected Foreign
l Schools
Page 56 GAO-10-412
Appendix III: Comparison of Average Cost of
Attendance at U.S. and Selected Foreign
Medical Schools
Source: GAO analysis of institutional data and published American Association of Medical Colleges, based on academic
year 2008-2009 data.
School B
Caribbean
School A
Europe
Average U.S.
Medical School
School E
Europe
School D
Caribbean
School C
Caribbean
PRIVATE PUBLIC
$62,654
$57,486
Expenses
$39,530
Tuition/
Fees
$97,016
$40,586
Expenses
$21,579
Expenses
$22,068
Tuition/
Fees
$62,217
Tuition/
Fees
$14,909
Expenses
$15,925
Tuition/
Fees
$83,796
$90,800
$60,372
$72,870
$30,834
$39,600
Tuition/
Fees
$28,206
Expenses
$32,166
Tuition/
Fees
$30,762
Expenses
$42,108
Tuition/
Fees
$51,200
Expenses
Notes: Expenses include such cost as room and board, books, transportation, and other
miscellaneous costs identified by institutions, which may vary. Cost expressed in United States
dollars.
Foreign Medical Schools
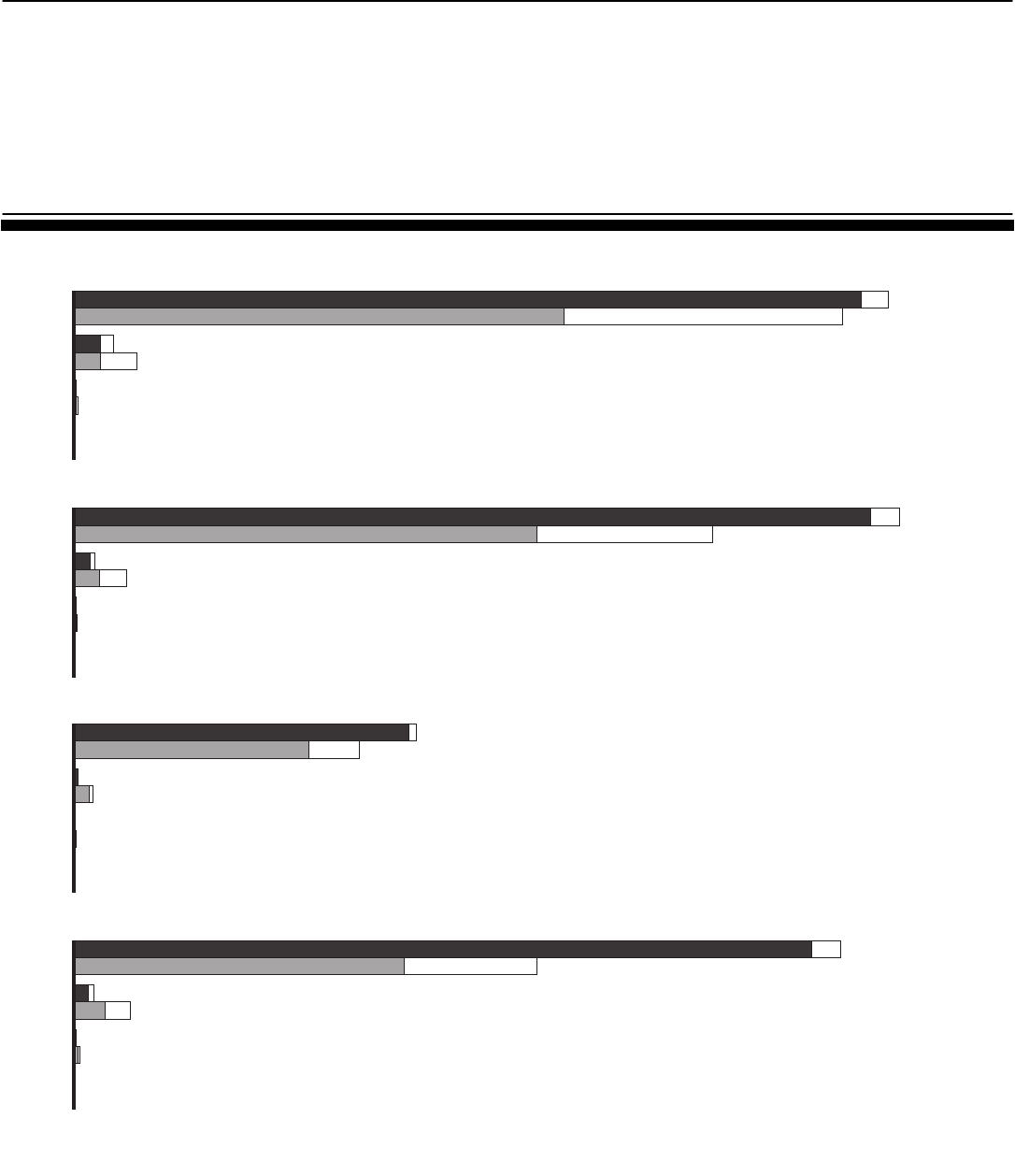
Appendix IV: Performance on Licensing Exam
by Number of Attempts on Each Exam Step,
and by Nationality of IMG
Appendix IV: Performance on Licensing
Exam by Number of Attempts on Each Exam
Step, and by Nationality of IMG
Figure 1: Licensing Exam Pass Rates by Number of Attempts on Each Exam Step, 1998 through 2008
Sources: GAO analysis of Educational Commission for Foreign Medical Graduates and National Board of Medical Examiners data.
0 50,000 100,000 150,000 200,000
U.S.-educated graduates
IMGs
First
Attempt
Graduates taking exam
97%
64%
66
42
314 (66% passed)
649 (41% passed)
1 (100% passed)
11 (27% passed)
Step 1
Step 2 Clinical Knowledge
Step 2 Clinical Skills
Step 3
Second
Third
Fourth
First
Second
Third
Fourth
First
Second
Third
Fourth
First
Second
Third
Fourth
AttemptedPassed
178,744
168,800
97%
72%
181,201
140,254
8,583
13,524
75
48
302 (71% passed)
455 (52% passed)
5 (80% passed)
7 (29% passed)
4,425
11,330
98%
82%
74,974
62,575
77
7 (100% passed)
225 (63% passed)
0
0
665 (95% passed)
4,027 (77% passed)
96%
71%
168,280
101,464
54
75
333 (68% passed)
1,111 (56% passed)
12 (75% passed)
23 (23% passed)
4,069
12,174
Note: All test takers are referred to as “graduates”; however, students are also eligible to take the
Step 1, Step 2 clinical knowledge, and Step 2 clinical skills exams while they are still enrolled in
medical school. Percentages were not indicated for attempts with small numbers of test-takers.
Page 57 GAO-10-412 Foreign Medical Schools
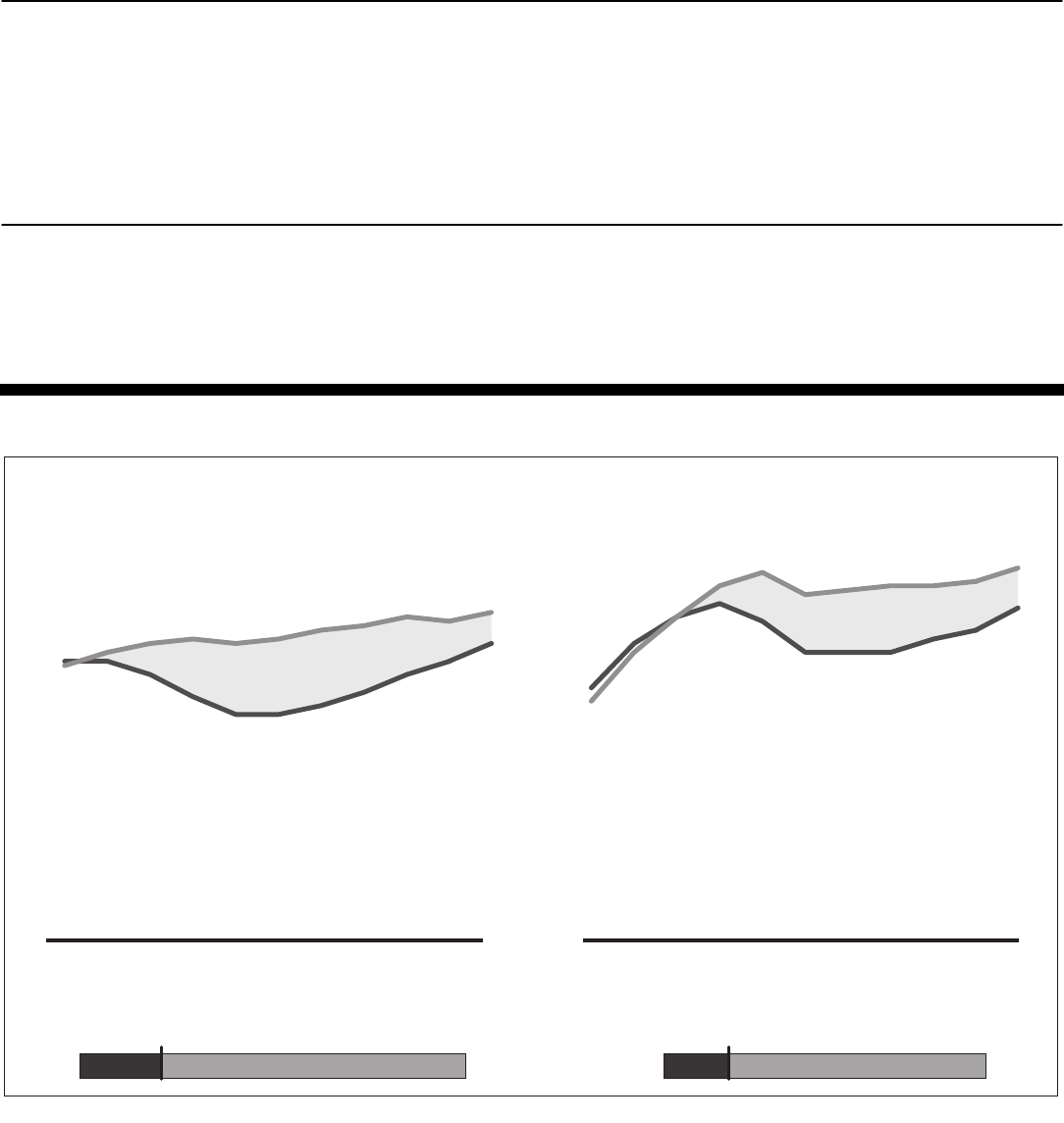
Appendix IV: Performance on Licensing Exam
by Number of Attempts on Each Exam Step,
and by Nationality of IMG
Among IMGs themselves, pass rates for foreign IMGs have generally
exceeded those for U.S. citizen IMGs on Step 1 and Step 2, Clinical
Knowledge, although U.S. citizens have achieved higher pass rates on the
Step 2 Clinical Skills exam and their lead on the Step 3 exam has steadily
been decreasing. (See figs. 2 and 3.)
Figure 2: Comparison of First-Time Pass Rates for U.S. Citizen IMGs and Foreign IMGs on Step 1 (Basic Science) and Step 2,
Clinical Knowledge, 1998 through 2008
Sources: GAO analysis of Educational Commission for Foreign Medical Graduates and National Board of Medical Examiners data.
0
10
20
30
40
50
60
70
80
90
100
'08
'07'06'05
'04'03'02'01'00'99'98
'08
'07'06'05
'04'03'02'01'00'99'98
First-time pass rate
71
64
62
63
84
75
54
57
U.S. citizen IMGs
Foreign IMGs
U.S. citizen IMGs
Foreign IMGs
14,892 graduates tested in 2008
U.S. citizen IMGs Foreign IMGs
21% 79%
11,7693,123
12,351 graduates tested in 2008
U.S. citizen IMGs Foreign IMGs
20% 80%
9,8582,493
Note: All test takers are referred to as “graduates”; however, students are eligible to take the Step 1
and Step 2 clinical knowledge exams while they are still enrolled in medical school.
Page 58 GAO-10-412 Foreign Medical Schools
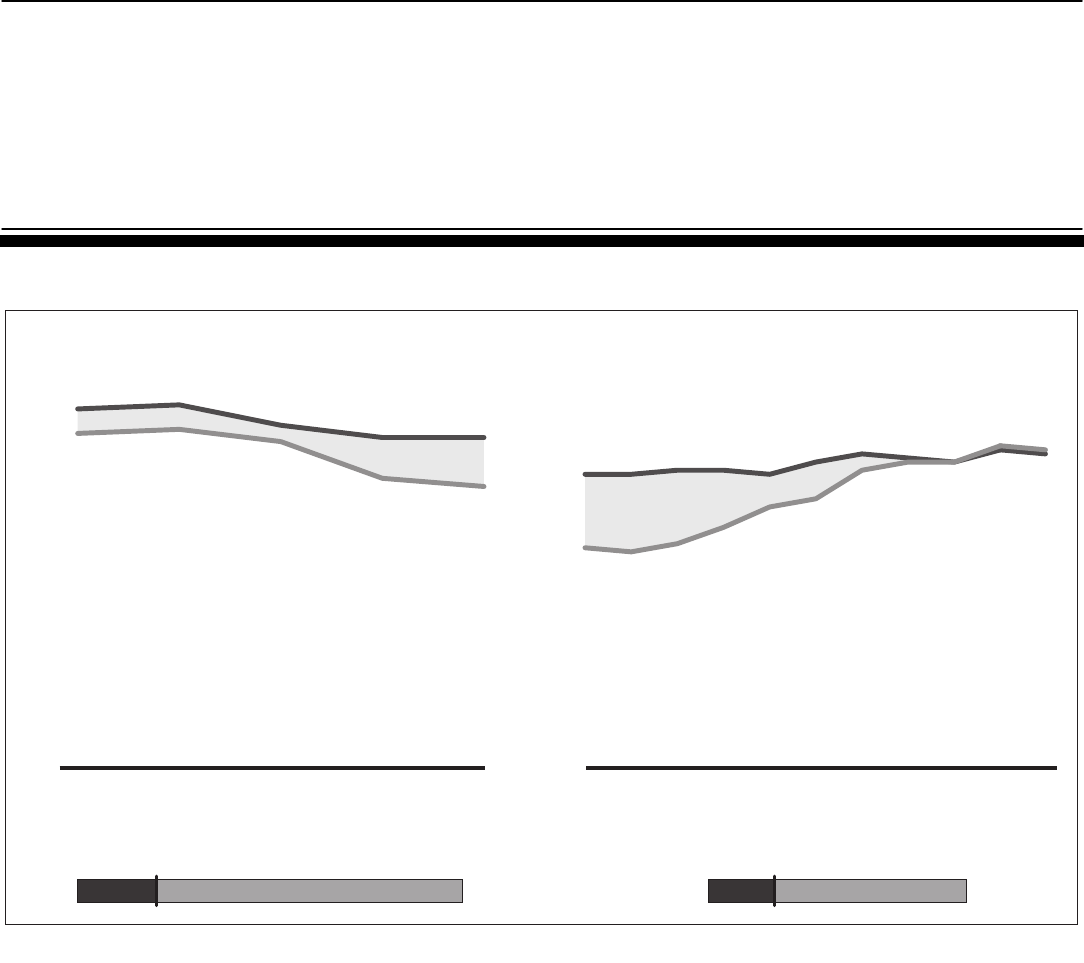
Appendix IV: Performance on Licensing Exam
by Number of Attempts on Each Exam Step,
and by Nationality of IMG
Figure 3: Comparison of First-Time Pass Rates for U.S. Citizen IMGs and Foreign IMGs on Step 2, Clinical Skills, 2004 through
2008, and Step 3 (on Delivery of General Medical Care), 1998 through 2008
Sources: GAO analysis of Educational Commission for Foreign Medical Graduates and National Board of Medical Examiners data.
0
10
20
30
40
50
60
70
80
90
100
20082007200620052004
'08
'07'06'05
'04'03'02'01'00'99'98
First-time pass rate
81
69
82
88
80
78
54
72
U.S. citizen IMGs
Foreign IMGs
U.S. citizen IMGs
Foreign IMGs
13,677 graduates tested in 2008
U.S. citizen IMGs Foreign IMGs
21% 79%
10,8662,811
9,373 graduates tested in 2008
U.S. citizen IMGs Foreign IMGs
27% 73%
6,8192,554
Notes: Test takers are referred to as “graduates”; however, students are also eligible to take the Step
2 clinical skills exam. This exam became a certification requirement on June 14, 2004, so pass rate
data for the Step 2 clinical skills exam are available only for exam year 2004 and onward.
According to ECFMG and NBME officials, there has been a clinical skills exam requirement for
ECFMG certification since July 1998. Prior to then, ECFMG administered the ECFMG Clinical Skills
Assessment (CSA), starting in July 1998, as a requirement for ECFMG certification.
Page 59 GAO-10-412 Foreign Medical Schools
Appendix V: International Medical Graduates
and Residencies
Table 1: Residency Programs by State, Academic Year 2008-2009
State Number of programs Percentage of all programs
Alabama 110 1.3
Alaska 1 0.0
Arizona 110 1.3
Arkansas 63 0.7
California 753 8.6
Colorado 94 1.1
Connecticut 159 1.8
District of Columbia 159 1.8
Delaware 27 0.3
Florida 293 3.4
Georgia 164 1.9
Hawaii 30 0.3
Idaho 4 0.0
Illinois 411 4.7
Indiana 100 1.1
Iowa 80 0.9
Kansas 58 0.7
Kentucky 99 1.1
Louisiana 143 1.6
Maine 21 0.2
Maryland 214 2.5
Massachusetts 387 4.4
Michigan 347 4.0
Minnesota 174 2.0
Mississippi 43 0.5
Missouri 212 2.4
Montana 2 0.0
Nebraska 55 0.6
Nevada 18 0.2
New Hampshire 45 0.5
New Jersey 196 2.2
New Mexico 53 0.6
New York 1,105 12.7
North Carolina 247 2.8
North Dakota 7 0.1
Appendix V: International Medical Graduates
and Residencies
Page 60 GAO-10-412 Foreign Medical Schools
Appendix V: International Medical Graduates
and Residencies
State Number of programs Percentage of all programs
Ohio 447 5.1
Oklahoma 65 0.7
Oregon 74 0.8
Pennsylvania 569 6.5
Puerto Rico 67 0.8
Rhode Island 59 0.7
South Carolina 95 1.1
South Dakota 7 0.1
Tennessee 180 2.1
Texas 544 6.2
Utah 66 0.8
Vermont 35 0.4
Virginia 187 2.1
Washington 131 1.5
West Virginia 59 0.7
Wisconsin 163 1.9
Wyoming 2 0.0
Total 8,734 100
Source: GAO analysis of Accreditation Council for Graduate Medical Education (ACGME) data.
Page 61 GAO-10-412 Foreign Medical Schools
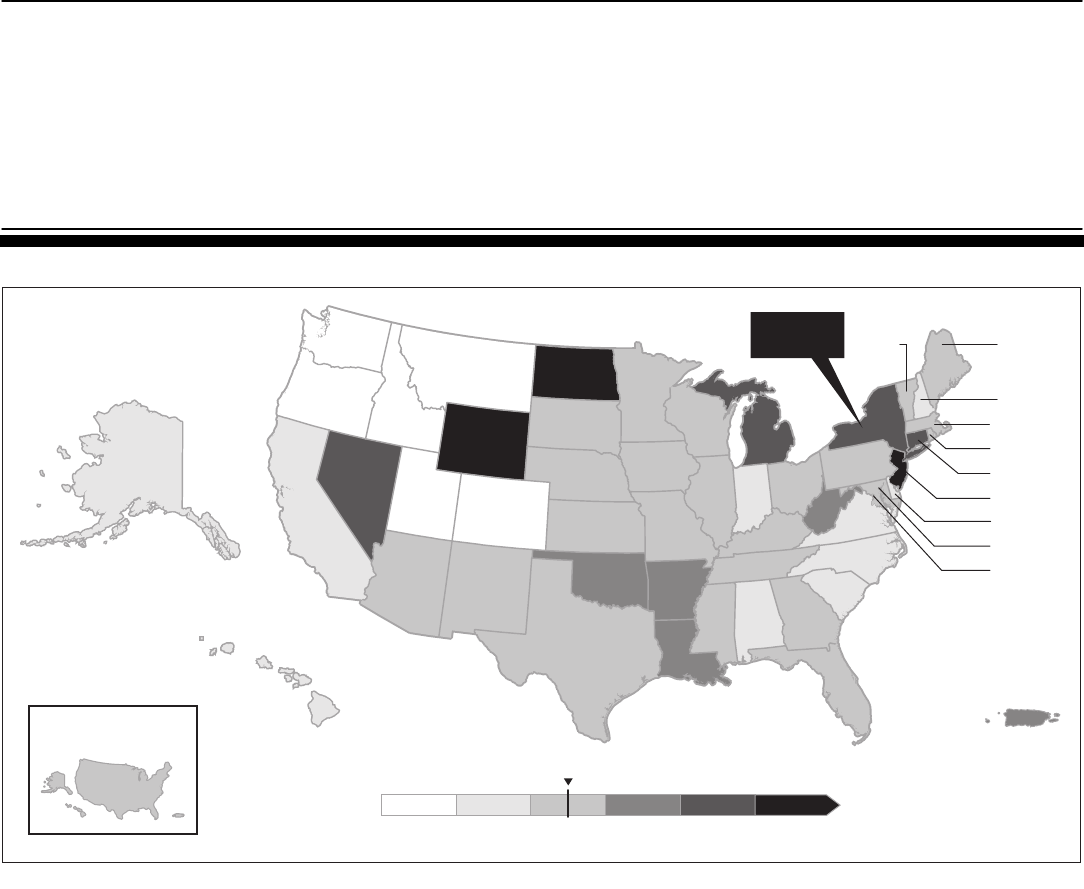
Appendix V: International Medical Graduates
and Residencies
Figure 4: Percentage of IMGs in Residencies as a Percentage of All Residents by State, Academic Year 2008-2009
Sources: GAO analysis of Accreditation Council for Graduate Medical Education (ACGME) data; The National Atlas of the
United States (map).
NH 15.2
■
MA 21.3
■
RI 20.3
■
CT 41.8
■
NJ 58.1
■
DE 16.0
■
MD 23.5
■
DC 23.7
WY
55.0
VT
20.5
MI
MI
40.6
40.6
MI
40.6
ME 20.7
LA
LA
37.5
37.5
AR
30.9
CA
12.0
AZ
23.3
NM
21.0
WI
23.3
KS
22.8
OH
29.5
IL
27.9
IN
19.2
FL
FL
29.6
29.6
FL
FL
29.6
29.6
FL
29.6
WV
WV
37.3
37.3
WV
37.3
UT
9.3
CO
6.2
WA
8.8
OR
7.1
ID
4.0
MT 5.0
VA
17.9
OK
33.2
NE
25.9
TX
21.0
MO
23.8
MS
20.0
27.4
IA
21.9
MN
22.0
GA
25.7
SC
SC
13.1
13.1
SC
13.1
NC 11.1
NV
47.9
AK
17.1
HI
12.8
PA 28.8
TN 24.2
KY
20.9
ND 62.6
SD 27.8
10%0% 20% 30% 40% 50%
State average 24.7
PR 31.5
LA
37.5
AL
19.8
Nationwide
percentage
New York
44.6
Page 62 GAO-10-412 Foreign Medical Schools
Appendix VI: S
Group
Medica
ummary of Responses by Focus
Participants at the Five Foreign
l Schools We Visited
Page 63 GAO-10-412
Appendix VI: Summary of Responses by
Focus Group Participants at the Five Foreign
Medical Schools We Visited
Although findings are not generalizable to all U.S. students studying in
foreign medical schools, we conducted focus groups with 82 enrolled U.S.
citizens or permanent residents at five schools we visited to gain a better
understanding of and perspective on students who attend foreign medical
schools. Table 2 shows a summary of the number of students who
participated in our focus groups by school.
Table 2: Number of Participants in Student Focus Groups, by School
School Number of focus groups conducted Number of participants
School A 2 21
School B 2 19
School C 2 25
School D 1 7
School E 1 10
Total 8 82
Source: GAO analysis of focus group survey responses.
We obtained basic demographic information on students who participated
in our focus groups to learn more about their year of medical school,
gender, age, and citizenship status. This information has been included to
provide some perspective on who participated in our focus groups;
however, this information is not generalizable to all IMG students.
Demographics
• Sixty-eight percent of the students who participated in our focus
groups were enrolled in their second year of medical school abroad.
Another 16 percent were in the first year of study.
• Sixty-six percent of participants were male and the remaining 39
percent were female.
• Almost half the participants were between the ages of 25 and 34.
• Over two-thirds of participants were U.S. citizens and 13 percent had
dual citizenship with the United States and usually the country where
the medical school was located.
Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
We asked participants in our focus groups to tell us about some of the
reasons they decided to pursue a medical education outside the United
States and whether they had applied to any other medical schools. Table 3
summarizes our questions and the most frequent responses provided by
participants in our focus groups.
Reasons for Attending
a Foreign Medical
School
Table 3: Decision to Attend a Foreign Medical School
Question
Most frequent responses by focus group
participants
What are some of the reasons you
decided to pursue your medical
education outside the U.S.?
• Noncompetitive grade point average or Medical
College Admission Test
• Perceived as too old for U.S. medical schools
• Not accepted into U.S. medical schools
• Did not want to wait another year to apply or
retake admission test
• Location of school/living abroad
• Only opportunity to achieve goal of becoming a
doctor
What are some of the reasons you
chose this medical school?
• Opportunity for clinical rotations in U.S with
hospitals affiliated with the medical school
• School’s reputation
• Accelerated program or other admissions
requirements enable student to finish school
quickly
• Availability of federal financial aid or cost of
attendance
How did you learn or find out about
this school?
Internet (student-led bulletin boards)
Word of mouth through friends, family, other
doctors
Did you apply to U.S. medical
schools?
If so, how many U. S. medical
schools did you apply to?
Fifty-nine of the 82 students participating in the
focus groups responded that they had initially
applied to U.S. medical schools.
• Those attending School A: 6.6 schools
• Those attending School B: 7.4 schools
• Those attending School C: 12.6 schools
• Those attending School D: 14.5 schools
• Those attending School E: 4.2 schools
Were you accepted by a U.S.
medical school?
Ten of the 82 participants who participated in our
focus groups indicated that they had also been
accepted by a U.S. medical school.
Other than the medical school you
are enrolled in, did you apply to any
other medical schools outside the
U.S.?
Forty-four of the 82 focus group participants
responded that they applied by another foreign
medical school in addition to the school where they
were enrolled.
Source: GAO analysis of focus group survey responses.
Page 64 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
We asked focus group participants to assess the relative importance of
various forms of financial aid to help finance their medical education. In
addition, we asked them about the extent to which cost of attendance was
a factor in their application decision. For those focus group participants
who have received federal student loans, we also asked them about their
experience in working with the school’s financial aid office.
Financing Medical
Education
Participants in our focus groups ranked the various financial aid sources
in the following order, from most to least important:
• federal student aid,
• personal savings/family resources,
• private loans,
• scholarships, and
• Veterans Affairs Benefits/GI Bill
While the cost of medical school was a factor in the application decision,
the availability of federal financial aid was considered essential and
without which students would not have been able to afford medical
school. Some notable quotes included the following:
• “My dream would have died without Department of Education loans.”
• “Federal assistance makes this possible. I am worried that the program
will go away.”
• “Without federal loans, most of the students could not attend [school
name].”
• “It is vital to maintain this program that has not only been proven by
the long history of graduates who have returned to the U.S., but also
been shown to be necessary to help relieve the shortage of physicians
in the United States.”
Several participants said that they lack consumer information on expected
debt level, and that there is no reliable source of such information to help
decide which medical school to attend.
• One participant explicitly asked about the school’s pass rate on the
licensing exam but got a vague answer from school officials. “[Name of
Page 65 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
school’s] marketing statement says that the school’s pass rate is 98
percent on Step 1. Even U.S. schools don’t hit this mark. But [school
name] only counts those students who actually sit for the exam and
don’t drop out. They warn you but only after you get here and sign for
the loan. [I] would have no problem if they said it was cutthroat
environment. [Your] eyes are open and you know what to expect.
People drop left and right. You can be 25 years old, $75,000 in debt, and
[have to leave] in the 3rd semester with nothing. There should be truth
in advertising … schools should show their numbers. This is ethical. [I]
knew a couple of students with families who failed out. [They]
uprooted [their] life only to get creamed.”
Focus group participants reported that, in general, obtaining financial aid
was a smooth process and that the school’s financial aid office was very
helpful in disbursing the aid on time, and in responding to students’
inquiries. One participant noted that the school even requires students to
obtain financial counseling before getting any loans.
We asked focus group participants about their plans to pursue a residency
and also their long-term career plans.
Residency and
Practice
Almost all participants in our focus groups—69 of the 82—indicated that
they would eventually return to the United States to either pursue a
residency or practice medicine. While 54 of these 69 participants who said
that they would eventually return to the United States indicated that they
preferred to pursue a specialty during their residency, 41 indicated that
they would also consider primary care as either their first choice or one of
their choices. Three of the 69 participants stated they planned to go into
research.
Participants cited a number of factors to consider when deciding which
field of medicine to practice, including scores on medical licensing exams,
earnings potential (which affected ability to pay off student loans),
physician workload, flexible schedule, and having to deal with health
insurance companies. While most participants in our focus groups said
they would like to go into a specialty, several acknowledged “the reality”
that most graduates of foreign medical schools end up in primary care
because residency slots in specialties are extremely competitive and
limited.
Page 66 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
One participant stated, “At a time when there is an increased need for
primary care physicians in the U.S., it should be noted that a substantial
number of our graduates obtain primary care residencies.”
When talking specifically about where they hope to obtain a residency or
eventually practice, most participants—69 of the 82—indicated they
preferred to return to the South Atlantic states, and another 31
participants indicated that New England or the Mid-Atlantic states were
also a possibility. Ten of the 82 participants told us that they had plans to
serve in medically underserved communities or help specific ethnic
populations.
Among the factors influencing their residency decision were being close to
family, desire to help underserved populations, whether the residency
program accepted international medical graduates, and availability of loan
forgiveness programs.
We obtained focus group participants’ perspectives on the quality of
instruction at the school, including the benefits of attending a foreign
medical school.
Quality of Instruction
Many participants said that, overall, the permanent professors were
knowledgeable and accomplished, but a few students at some schools said
that instruction provided by visiting professors varied in quality. A few
notable quotes included the following:
• “We do an evaluation at the end of the semester. I think they [i.e., the
school] pay attention to that. If they [i.e., professors] are not good at
teaching, you don’t see them anymore.”
• “Quality is very high here. The rotations—doctors you’re paired with,
take the effort to teach. [That is] not the case in the U.S. [I] feel I’m
learning more.”
• “All of the faculty are non-practicing. They are available all the time.
They hold your hand more.”
• “In the U.S., many of the professors are practicing doctors or do
research. It’s different at [name of school].…The emphasis is on
teaching so that makes them more accessible.”
Page 67 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
• “They [i.e., visiting professors] may really know a particular subject.
They may really know the research, but when asked ‘how,’ they can’t
explain it.”
• “Teaching quality is highly variable. The awful ones were all visiting
professors. They’re here on vacation for 2-4 weeks from the U.S. [They
were] brought only because [they] happened to be available, not
because [they were] good. Visiting professors make up 20 percent of
the faculty. Most have been coming here for years.”
Focus group participants at one school told us that they valued the
campus’ proximity to a teaching hospital and the resulting opportunities to
gain early exposure to patients. In contrast, a focus group participant at
another school commented that the school did not have a relationship
with surrounding hospitals, which meant that students would have to wait
for a clinical rotation to gain exposure to patients.
Some focus group participants at for-profit institutions said that the
instructional materials were covered quickly or that to prepare for medical
licensing exams students needed to undertake self-study.
Several focus group participants at one school said they would have liked
to have information on student performance on the medical licensing
exam to help them select which foreign medical school to attend.
• Participants discussed various benefits of attending a foreign medical
school that included interacting with a wide spectrum of patients,
developing cultural sensitivity, and obtaining insights into different
health care systems.
In addition to asking them to evaluate the quality of instruction, we asked
focus group participants to comment on the quality of the educational
facilities such as classrooms, laboratories, libraries, and equipment.
Quality of
Educational Facilities
We heard mixed comments regarding educational facilities and whether
they adequately met students’ needs. Some notable quotes included the
following:
• “Comparatively speaking to U.S. medical schools, classrooms are good
with flat screens and projectors.”
• “The university has invested in some new buildings and these are
equipped with state-of-the-art technology.”
Page 68 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
• “You can get video streaming of classes and online learning…but the
system’s been getting crowded.”
• “Cadavers are an advantage. The number of cadavers available allows
for very small groups of four students. Other schools often assign 12
students to a cadaver.”
• “Great that they have access to cadavers. Many colleges do not have
these.”
• “The library is small but has all the books we need.”
• “Library is horrible. Very poor electronic resources but large journal
collection. Library is small given large student population.”
• “[I’m] angry [that] pathology is important, [but] the microscopes are
from 40 years ago.”
Several focus group participants noted that class size was an issue and
that the infrastructure was not keeping up with enrollment growth.
• “Classes [are] expanding faster than infrastructure. They try to keep up
with it, but bigger classes affect individual attention, divert resources
from other things, stretches resources.”
• “Average class size is 500 students and increasing toward 600.”
• “It may not take away from me to be in a big class. I don’t go to class.
Lectures are recorded and placed online for people to watch.” [Student
makes the choice to stay home and watch lectures and considers it a
“waste of time to go to class”.]
• “Teachers don’t agree with the administration’s decision to expand
classes. [They think it is] unwieldy … [and that there is] too much of a
focus on business.”
• “Feeling resentful of increase in enrollment without adequate
infrastructure. [Name of school] is constantly expanding because it’s a
business. But people get what they need from the facilities.”
Another participant provided the following contrasting perspective:
• “While it is certainly true that there has been recent expansion in class
size, the quality of education has not been affected. I can honestly say
that I have never felt that I did not have access to my instructors or
Page 69 GAO-10-412 Foreign Medical Schools
Appendix VI: Summary of Responses by Focus
Group Participants at the Five Foreign
Medical Schools We Visited
clinical tutors. It makes no difference to me if there are 100, 200, or 500
people in the lecture hall. What does matter is how many people are in
my lab groups. For instance, my anatomy dissection group had four
people in it [similar to or better than U.S. schools]…These sessions
provide all students with ample opportunity for discussion and
questions.”
Page 70 GAO-10-412 Foreign Medical Schools
Appendix VII: Comments from the U.S.
Department of Education
Appendix VII: Comments from the U.S.
Department of Education
Page 71 GAO-10-412 Foreign Medical Schools
Appendix VII: Comments from the U.S.
Department of Education
Page 72 GAO-10-412 Foreign Medical Schools
Appendix VIII:
A
GAO Contact and Staff
cknowledgments
Page 73 GAO-10-412
Appendix VIII: GAO Contact and Staff
Acknowledgments
George A. Scott, Director, (202) 512-7215 or [email protected]
In addition to the contact named above, Meeta Engle, Assistant Director;
Carla Craddock, Analyst-in-Charge; James Bennett; Susan Bernstein;
Alexander Galuten; Lauren Gilbertson; Kristen Jones; Mitchell Karpman;
Kathleen King; Ruben Montes de Oca; Christopher Morehouse; Terry
Richardson; and Cynthia Saunders and made key contributions to this
report.
GAO Contact
Staff
Acknowledgments
Foreign Medical Schools
Bibliography
Bibliography
Overview of IMGs
Boulet, John R., Stephen Seeling, John Norcini, Danette McKinley, and
Richard Cooper. “The Contribution of US Citizen International Medical
Graduates to the US Physician Workforce.” Presented at the 2009
Physician Workforce Research Conference, Washington, D.C., April 30 -
May 1, 2009.
Johnson, Karin, Amy Hagopian, Catherine Veninga, and L. Gary Hart. “The
Changing Geography of Americans Graduating from Foreign Medical
Schools.” Academic Medicine, vol. 81, no. 2 (2006).
Licensing Exam Performance
Bates, Joanna, and Rodney Andrew. “Untangling the Roots of Some IMGs’
Poor Academic Performance.” Academic Medicine, vol. 76, no. 1 (2001).
Boulet, John R., Richard A. Cooper, Stephen S. Seeling, John J. Norcini,
and Danette W. McKinley. “U.S. Citizens Who Obtain Their Medical
Degrees Abroad: An Overview, 1992 - 2006.” Health Affairs, vol. 28, no. 1
(2009).
Harik, Polina, Brian E. Clauser, Irina Grabovsky, Melissa J. Margolis,
Gerald F. Dillion, and John R. Boulet. “Relationships among
Subcomponents of the USMLE Step 2 Clinical Skills Examination, The
Step 1, and the Step 2 Clinical Knowledge Examinations.” Academic
Medicine, vol. 81, no. 10 (2006).
Norcini, John, M. Brownell Anderson, and Danette W. McKinley. “The
Medical Education of United States Citizens Who Train Abroad.” Surgery,
vol. 140, no. 3 (2006).
Van Zanten, Marta and John R. Boulet. “Medical Education in the
Caribbean: Variability in Educational Commission for Foreign Medical
Graduate Certification Rates and United States Medical Licensing
Examination Attempts.” Academic Medicine, vol. 84, no. 10 (2009).
Van Zanten, Marta, John R. Boulet, Danette W. McKinley, Andre
DeChamplain, and Ann C. Jobe. “Assessing the Communication and
Interpersonal Skills of Graduates of International Medical Schools as Part
of the United States Medical Licensing Exam (USMLE) Step 2 Clinical
Skills (CS) Exam.” Academic Medicine, vol. 82, no. 10 (2007).
Page 74 GAO-10-412 Foreign Medical Schools

Bibliography
Residency and Practice
American Medical Association. “International Medical Graduates in the
U.S. Workforce: A Discussion Paper.” (2008).
Fordyce, Meredith A., Frederick M. Chen, Mark P. Doescher, and L. Gary
Hart. “2005 Physician Supply and Distribution in Rural Areas of the United
States.” WWAMI Center for Health and Workforce Studies at the
University of Washington Department of Family Medicine, Final Report
#116 (2007).
Hagopian, Amy, Matthew J. Thompson, Emily Kaltenbach, and L. Gary
Hart. “The Role of International Medical Graduates in America’s Small
Rural Critical Access Hospitals.” The Journal of Rural Health, vol. 20, no.
1 (2004).
Hagopian, Amy, Matthew J. Thompson, Karin E. Johnson, and Denise M.
Lishner. “International Medical Graduates in the United States: A Review
of the Literature 1995-2003.” WWAMI Center for Health and Workforce
Studies at the University of Washington Department of Family Medicine,
Working Paper #83 (2003).
Hing, Esther, and Susan Lin. “Role of International Medical Graduates
Providing Office-based Medical Care: United States, 2005-06.” National
Center for Health Statistics Data Brief (2008).
Ogunyemi, Dotun, and Ron Edelstein. “Career Intentions of U.S. Medical
Graduates and International Medical Graduates.” Journal of the National
Medical Association, vol. 99, no. 10 (2007).
Salsberg, Edward, and Joseph Nolan. “The Posttraining Plans of
International Medical Graduates and US Medical Graduates in New York
State.” Journal of the American Medical Association, vol. 283, no. 13
(2000).
Discipline and Malpractice
Kohatsu, Neal D., Dawn Gould, Leslie K. Ross, and Patrick J. Fox.
“Characteristics Associated with Physician Discipline: A Case-Control
Study.” Archives of Internal Medicine, vol. 164 (2004).
Lee, Shoou-Yih D., William H. Dow, Virginia Wang, and Jonathan B.
VanGeest. “Use of Deceptive Tactics in Physician Practices: Are There
Page 75 GAO-10-412 Foreign Medical Schools
Bibliography
Differences between International and U.S. Medical Graduates?” Health
Policy, vol. 67 (2004).
Localio, A. Russell, Ann G. Lawthers, Troyen A. Brennan, Nan M. Laird,
Liesi E. Hebert, Lynn M. Peterson, Joseph P. Newhouse, Paul C. Weiler,
and Howard H. Hyatt. “Relation Between Malpractice Claims and Adverse
Events Due to Negligence: Results of the Harvard Medical Practice Study
III.” The New England Journal of Medicine, vol. 325, no. 4 (1991).
Mick, Stephen S., and Maureen E. Comfort. “The Quality of Care of
International Medical Graduates: How Does It Compare to That of U.S.
Medical Graduates?” Medical Care Research and Review, vol. 54, no. 4
(1997).
Studdert, David M., Michelle M. Mello, Atul A. Gawande, Tejal K. Gandhi,
Allen Kachalia, Catherine Yoon, Ann Louise Puopolo, and Troyen A.
Brennan. “Claims, Errors, and Compensation Payments in Medical
Malpractice Litigation.” The New England Journal of Medicine, vol. 354,
no. 19 (2006).
Studdert, David M., Eric J. Thomas, Helen R. Burstin, Brett I.W. Zbar, E.
John Orav, and Troyen A. Brennan. “Negligent Care and Malpractice
Claiming Behavior in Utah and Colorado.” Medical Care, vol. 38, no. 3
(2000).
U.S. Department of Education, National Committee on Foreign Medical
Education and Accreditation. Report to the U.S. Congress by the National
Committee on Foreign Medical Education and Accreditation
Recommending Institutional Eligibility Criteria for Participation by
Certain Foreign Medical Schools in the Federal Family Education Loan
Program. 2009.
Wolfe, Sidney M., and Kate Resnevic. “Public Citizen’s Health Research
Group Ranking of the Rate of State Medical Boards’ Serious Disciplinary
Actions, 2006-2008 (HRG Publication#1868).” (2009).
http://www.citizen.org/publications/publicationredirect.cfm?ID=7652
(accessed Jan. 6, 2010).
Page 76 GAO-10-412 Foreign Medical Schools
Related GAO Products
Related GAO Products
Graduate Medical Education: Trends in Training and Student Debt.
GAO-09-438R. Washington, D.C.: May 4, 2009.
Primary Care Professionals: Recent Supply Trends, Projections, and
Valuation of Services. GAO-08-472T. Washington, D.C.: February 12, 2008.
Foreign Physicians: Data on Use of J-1 Visa Waivers Needed to Better
Address Physician Shortages. GAO-07-52. Washington, D.C.: November
30, 2006.
Foreign Physicians: Preliminary Findings on the Use of J-1 Visa
Waivers to Practice in Underserved Areas. GAO-06-773T. Washington,
D.C.: May 18, 2006.
Student Loans and Foreign Schools: Assessing Risks Could Help
Education Reduce Program Vulnerability. GAO-03-647. Washington, D.C.:
July 25, 2003.
Foreign Physicians: Exchange Visitor Program Becoming Major Route
to Practicing in U.S. Underserved Areas. GAO/HEHS-97-26. Washington,
D.C.: December 30, 1996.
Student Loans: Millions Loaned Inappropriately to U.S. Nationals at
Foreign Medical Schools. GAO/HEHS-94-28. Washington, D.C.: January 21,
1994.
Medical Licensing By Endorsement: Requirements Differ for Graduates
of Foreign and U.S. Medical Schools. GAO/HRD-90-120. Washington, D.C.:
May 17, 1990.
Medical Malpractice: Characteristics of Claims Closed in 1984.
GAO/HRD-87-55. Washington, D.C.: April 22, 1987.
Federal, State, and Private Activities Pertaining to U.S. Graduates of
Foreign Medical Schools. GAO/HRD-85-112. Washington, D.C.: September
27, 1985.
(130917)
Page 77 GAO-10-412 Foreign Medical Schools
GAO’s Mission
The Government Accountability Office, the audit, evaluation, and
investigative arm of Congress, exists to support Congress in meeting its
constitutional responsibilities and to help improve the performance and
accountability of the federal government for the American people. GAO
examines the use of public funds; evaluates federal programs and policies;
and provides analyses, recommendations, and other assistance to help
Congress make informed oversight, policy, and funding decisions. GAO’s
commitment to good government is reflected in its core values of
accountability, integrity, and reliability.
The fastest and easiest way to obtain copies of GAO documents at no cost
is through GAO’s Web site (www.gao.gov). Each weekday afternoon, GAO
posts on its Web site newly released reports, testimony, and
correspondence. To have GAO e-mail you a list of newly posted products,
go to www.gao.gov and select “E-mail Updates.”
Obtaining Copies of
GAO Reports and
Testimony
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of
production and distribution and depends on the number of pages in the
publication and whether the publication is printed in color or black and
white. Pricing and ordering information is posted on GAO’s Web site,
http://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077, or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card,
MasterCard, Visa, check, or money order. Call for additional information.
Contact:
Web site: www.gao.gov/fraudnet/fraudnet.htm
E-mail: [email protected]
Automated answering system: (800) 424-5454 or (202) 512-7470
Ralph Dawn, Managing Director, [email protected], (202) 512-4400
U.S. Government Accountability Office, 441 G Street NW, Room 7125
Washington, DC 20548
To Report Fraud,
Waste, and Abuse in
Federal Programs
Congressional
Relations
Chuck Young, Managing Director, youngc1@gao.gov, (202) 512-4800
U.S. Government Accountability Office, 441 G Street NW, Room 7149
Washington, DC 20548
Public Affairs
Please Print on Recycled Paper
