
Canada’s Guidance on Alcohol
and Health: Final Report
This document was published by the Canadian Centre on Substance Use and Addiction
(CCSA).
Suggested citation: Paradis, C., Butt, P., Shield, K., Poole, N., Wells, S., Naimi, T., Sherk, A., &
the Low-Risk Alcohol Drinking Guidelines Scientific Expert Panels. (2023). Canada’s Guidance
on Alcohol and Health: Final Report. Ottawa, Ont.: Canadian Centre on Substance Use and
Addiction.
© Canadian Centre on Substance Use and Addiction, 2023.
CCSA, 500–75 Albert Street
Ottawa, ON K1P 5E7
613-235-4048
Production of this document has been made possible through a financial contribution from
Health Canada. The funding body did not influence guideline content. The views expressed
herein do not necessarily represent the views of Health Canada.
This document can also be downloaded as a PDF at www.ccsa.ca
Ce document est également disponible en français sous le titre :
Repères canadiens sur l’alcool et la santé : rapport final
ISBN 978-1-77871-046-9
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances
Table of Contents
Acknowledgements .......................................................................................... 1
About this Document ......................................................................................... 4
Public Summary .......................................................................................................... 5
Technical Summary ..................................................................................................... 6
Aim and Approach ............................................................................................ 6
Risk Associated with Weekly Levels of Alcohol Use ......................................... 7
Risk Associated with Alcohol Use Per Occasion ................................................ 8
Risk when Pregnant, Trying to Get Pregnant or Breastfeeding ......................... 9
Sex and Gender ................................................................................................ 9
Risk for Women ................................................................................................ 9
Risk for Men ...................................................................................................... 9
Youth .............................................................................................................. 10
When Zero’s the Limit ..................................................................................... 10
Reasons for the New Guidance on Alcohol and Health ................................... 10
Alcohol and Cancer ................................................................................... 10
Alcohol and Heart Disease ......................................................................... 10
Alcohol and Liver Disease ......................................................................... 11
Alcohol and Violence ................................................................................ 11
Policy Implications .......................................................................................... 11
Technical Report ....................................................................................................... 12
Introduction .................................................................................................... 12
Awareness and Adherence to the 2011 LRDGs by People Living
in Canada ........................................................................................................ 12
Time to Update ............................................................................................... 13
Aim and Scope of This Report ......................................................................... 14
Part 1: Development of Experts’ Recommendations ................................................. 15
1.1 Defining Research Questions .................................................................... 15
1.2 Estimating the Lifetime Risk of Alcohol-Related Death and
Disability in the Canadian Population ............................................................. 15
1.3 The Evidence Base for Updating the Guidelines ....................................... 16

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances
1.4 Reaching Conclusions and Formulating Recommendations ...................... 17
Part 2: Evidence Used to Construct the Recommendations ....................................... 18
2.1 Global Evidence Review on the Effects of Alcohol on Health .................... 18
2.1.1. Methods ........................................................................................... 18
2.1.2 Results ............................................................................................... 20
2.1.3 Quality of Evidence ........................................................................... 21
2.1.4 Implications ....................................................................................... 21
2.2 Mathematical Modelling of the Lifetime Risk of Death for
Various Levels of Average Alcohol Consumption ........................................... 21
2.2.1 Methodological Principles ................................................................ 22
2.2.2 Results and Implications .................................................................... 24
2.3 Alcohol Use Per Occasion ......................................................................... 30
2.4 Rapid Reviews ........................................................................................... 32
2.4.1 Association Between Alcohol Use, Aggression and
Violence .................................................................................................... 32
2.4.2 Association Between Alcohol Use and Mental Health ........................ 35
2.5 Women’s Health and Alcohol .................................................................... 36
2.5.1 What Are Some Sex-Related Factors? ............................................... 36
2.5.2 What Are Some Gender-Related Factors? ......................................... 36
2.5.3 How Do Sex and Gender Interact and Intersect with
Other Factors? ........................................................................................... 37
2.5.4 How Does Alcohol Affect Reproduction? ........................................... 37
2.5.5 Discussion ......................................................................................... 37
2.5.6 What Are the Key Messages for Women? .......................................... 38
2.6 Views, Preferences and Expectations About Guidelines of
People Living in Canada ................................................................................. 38
2.6.1 Summary of Evidence on Understanding and Response
to Alcohol Guidelines ................................................................................ 38
2.6.2 Public Consultation on Alcohol Guidelines ....................................... 39
2.6.3 Interviews with Stakeholders ............................................................ 39
2.6.4 Focused Discussions with Indigenous People ................................... 41
Part 3: Experts’ Recommendations ........................................................................... 43
3.1 Canada’s Guidance on Alcohol and Health ............................................... 44
3.2 Limitations ................................................................................................. 46
3.3 Moving Forward ........................................................................................ 47
3.4 Future Update of Canada’s Guidance on Alcohol and Health .................... 49

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances
3.5 Conclusion ................................................................................................ 49
References ................................................................................................................ 51
Appendix 1: Lifetime Risk of Alcohol-Attributable Death and
Disability: Shadow Analysis ...................................................................................... 63
Purpose ........................................................................................................... 63
Method............................................................................................................ 63
Summary of the Comparison of Findings ........................................................ 63
Appendix 2: Confidence Intervals for Risk of Disease and Injury ............................. 66
Appendix 3: Specific Messages for Girls and Women to Supplement
the Guidance on Alcohol and Health ......................................................................... 70
Appendix 4: Update of Canada’s Low-Risk Alcohol Drinking
Guidelines: Open Consultation ................................................................................. 71
Public Summary .............................................................................................. 71
Technical Summary ........................................................................................ 71
Technical Report ............................................................................................. 72
Public Consultation: Summary of Key Actions Taken ...................................... 75

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 1
Acknowledgements
The Canadian Centre on Substance Use and Addiction (CCSA) would like to extend its appreciation
and gratitude to the following individuals for their contributions to the project.
Scientific Expert Panels
Members of the Low-Risk Alcohol Drinking Guidelines Scientific Expert Panels provided their
expertise and guidance, and made other invaluable contributions.
Co-chairs for the project
• Catherine Paradis, CCSA
• Peter Butt, College of Medicine, University of Saskatchewan
Members (in alphabetical order)
• Mark Asbridge, Dalhousie Medical School
• Danielle Buell, University of Toronto
• Samantha Cukier, Health Canada
• Francois Damphousse, Health Canada
• Jennifer Heatley, Public Health, Government of Nova Scotia
• Erin Hobin, Public Health Ontario
• Harold R. Johnson, Lawyer and Author
1
• Ryan McCarthy, previously with CCSA
• Chris Mushquash, Lakehead University
• Daniel Myran, Ottawa Hospital Research Institute
• Tim Naimi, Canadian Institute for Substance Use Research, University of Victoria
• Nancy Poole, Centre of Excellence for Women's Health
• Justin Presseau, Ottawa Hospital Research Institute
• Adam Sherk, Canadian Institute for Substance Use Research, University of Victoria
• Kevin D. Shield, Institute for Mental Health Policy Research, Centre for Addiction and Mental
Health
• Tim Stockwell, Canadian Institute for Substance Use Research, University of Victoria
• Sharon Straus, University of Toronto
• Kara Thompson, St. Francis Xavier University
1
Harold R. Johnson passed away during the development of this report. We greatly appreciate his important contributions to this process,
and we extend our sincere condolences to his family and friends.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 2
• Samantha Wells, Institute for Mental Health Policy Research, Centre for Addiction and Mental
Health
• Matthew Young, Gambling Research Exchange Ontario, Carleton University and CCSA
The following members and their colleagues led the production of reports and reviews (as indicated)
that informed development of Canada’s Guidance on Alcohol and Health (in alphabetical order):
• Sharon Bernards, Jesus Chavarria, Jean-Francois Crépault, Tavleen Dhinsa, Kathryn Graham,
Bryan Tanner and Samantha Wells: Association Between Alcohol Use and Aggression and
Violence: A Rapid Overview of Reviews to Inform Canada’s Low-Risk Alcohol Drinking Guidelines
• Sam Churchill, Tim Naimi and Adam Sherk: Lifetime Risk of Alcohol-Attributable Death and
Disability: Shadow Analysis (Appendix 1)
• Tim Naimi: Per occasion alcohol use
• Nancy Poole and Lorraine Greaves: Sex, Gender and Alcohol: What Matters for Women in Low-
Risk Drinking Guidelines?
• Nancy Poole and Lorraine Greaves: Specific Messages for Girls and Women to Supplement the
Guidance on Alcohol and Health (see Appendix 3)
• Kevin Shield: Lifetime Risk of Alcohol-Attributable Death and Disability
Other Contributors
The project has benefited from the efforts and contributions of the following organizations and
individuals (in alphabetical order):
• Autrement dit: Plain language summary of Canada’s Guidance on Alcohol and Health
• Cochrane Canada: Update of a Systematic Review of the Effect of Alcohol Consumption on the
Development of Depression, Anxiety and Suicidal Ideation
• Cochrane Canada: Update of Canada’s Low-Risk Alcohol Drinking Guidelines: Summary of
Evidence on Understanding and Response to Alcohol Consumption Guidelines
• Christine Levesque, Nitika Sanger and Hanie Edalati: Assistance in all aspects of the evidence
review portion of this project
• Jennifer Reynolds: Assistance in overseeing the first public consultation and the stakeholder’s
consultations
• Bryce Barker, Manon Blouin, Patricia-Anne Croteau, Christina Davies, Ahmer Gulzar, Lauren
Levett, Victoria Lewis, Wendy Schlachta, Virginia St-Denis, Sheena Taha, John Thurston and Lili
Yan: Assistance with project management, communications, editing, translation as well as
planning project next steps.
Observers
• Kate Morissette, Public Health Agency of Canada

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 3
Executive Committee
Members of the Low-Risk Alcohol Drinking Guidelines Executive Committee generously contributed
their time and expertise throughout this project.
Co-chairs
• Alexander Caudarella, CCSA
• Shannon Nix, Health Canada
• Rita Notarandrea, previously with CCSA
Members (in alphabetical order)
• Ally Butler, Substance Use and Strategic Initiatives, Government of British Columbia
• Ian Culbert, Canadian Public Health Association
• Scott Hannant, CCSA
• Carol Hopkins, Thunderbird Partnership Foundation
• Jennifer Saxe, Health Canada
• Candice St-Aubin, Public Health Agency of Canada
• Robert Strang, Council of Chief Medical Officers of Canada
• Sam Weiss, Canadian Institute of Health Research
Conflict of Interest
The list of potential conflicts of interest for all participants in the project is available on CCSA’s
website: Disclosure of Affiliations and Interests
.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 4
About this Document
This report contains three documents produced for three different target groups.
Public Summary
The Public Summary is a one-page summary intended for the general public.
Technical Summary
The Technical Summary is intended for health organizations, health professionals (e.g., physicians,
nurses, counsellors) and people who would like to learn about the update of the Low-Risk Alcohol
Drinking Guidelines, its key takeaways, the risks associated with alcohol and the implications.
Technical Report
The Technical Report is intended for alcohol scientists, policy makers and healthcare professionals
who are interested in understanding the detailed process followed, the types of evidence and the
way they were used to update the Low-Risk Alcohol Drinking Guidelines.
The three documents in this report were made available for public consultation from Aug. 29 through
Sept. 23, 2022. The report has been modified in response to that consultation. For details on the
comments made during the consultation and the response to those comments, see Appendix 4.
Notes on Sex and Gender Terminology
Alcohol use has risks, effects, influences and consequences specific to sex and gender. In real life
experience, sex and gender interact with each other, and with other intersectional characteristics
to shape the impacts of alcohol use.
The effects and impacts of sex and gender on alcohol use among sub-populations such as
Indigenous Peoples, older people, sexual minorities and gender minorities remain under-
researched or unknown. As evidence about alcohol and social patterns of drinking evolves, it will
be important to continuously reassess the impact of alcohol on all populations, and to create
appropriate public health and health promotion advice for all populations.
Throughout this report, when presenting sex-related risks, the terms female and male are used.
When presenting gender-related risks, the terms women and men are used. When a section or
topic involves the entanglement of sex and gender, the terms women and men are used.
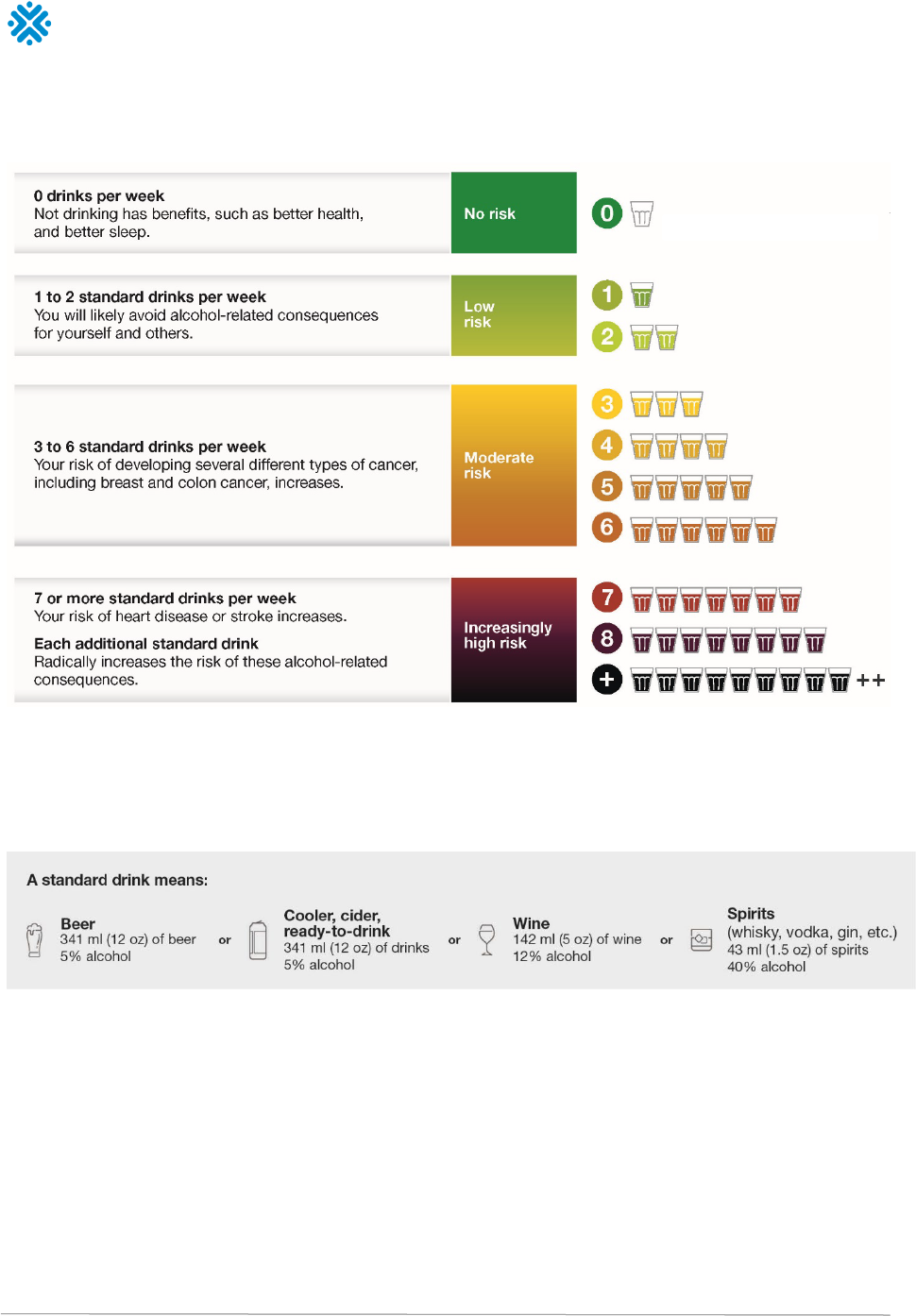
Notes on a Standard Drink
In Canada, a standard drink is 17.05 millilitres or 13.45 grams of pure alcohol, which is the
equivalent of:
• A bottle of beer (12 oz., 341 ml, 5% alcohol)
• A bottle of cider (12 oz., 341 ml, 5% alcohol)
• A glass of wine (5 oz., 142 ml, 12% alcohol)
• A shot glass of spirits (1.5 oz., 43 ml, 40% alcohol)
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 5
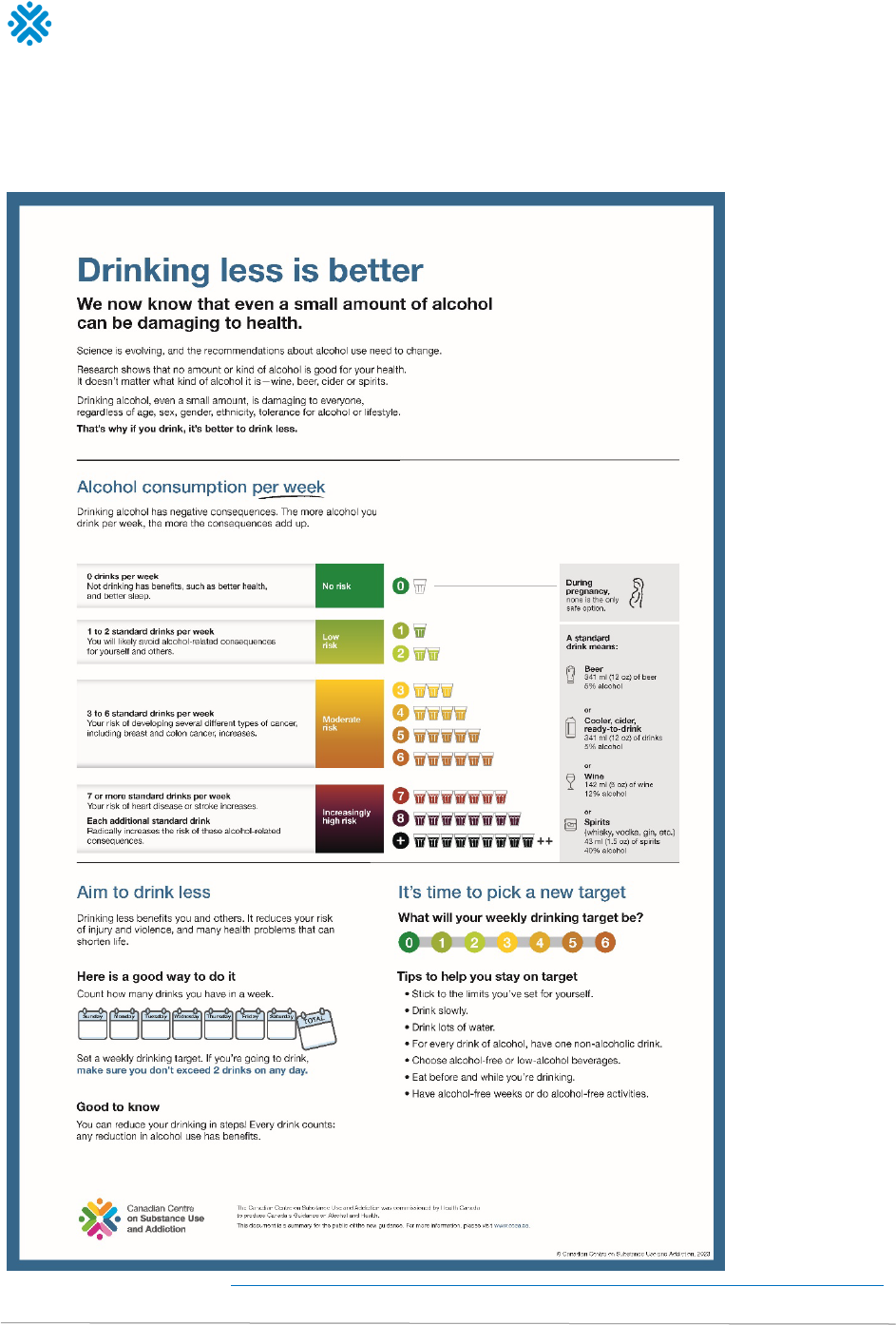
Public Summary
Note. For a PDF of this image, visit https://ccsa.ca/canadas-guidance-alcohol-and-health-public-summary-drinking-less-better-infographic
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 6
Technical Summary
Alcohol is a psychoactive substance used by about three-quarters of people living in Canada. It is
often used in connection with social events or to mark special occasions. However, alcohol can
cause harm to the person who drinks and sometimes to others around them. Alcohol is a leading
preventable cause of death, disability and social problems, including certain cancers, cardiovascular
disease, liver disease, unintentional injuries and violence. In 2017, alcohol caused 18,000 deaths in
Canada. That same year, the costs associated with alcohol use in Canada were $16.6 billion, with
$5.4 billion of that sum spent on health care.
To make more informed decisions about alcohol use, people living in Canada must be aware of
important information about alcohol and health, assess their personal risk and consider reducing
their alcohol use. Taken together
, overwhelming evidence confirms that when it comes to drinking
alcohol, less consumption means less risk of harm from alcohol.
Aim and Approach
Canada’s Guidance on Alcohol and Health is informed by a public health perspective. It is intended
to replace Canada’s Low-Risk Alcohol Drinking Guidelines. It provides accurate and current
information about the risks and harms associated with the use of alcohol. The guidance should help
people make well-informed and responsible decisions about their alcohol consumption.
Canada’s Guidance on Alcohol and Health
To reduce the risk of harm from alcohol,
it is recommended that people living in Canada consider
reducing their alcohol use
.
The reasons to do so derive from the following facts:
a. There is a continuum of risk associated with weekly alcohol consumption where the risk of
harm from alcohol is:
•
Low
for individuals who consume
2
standard drinks or less per week;
•
Moderate
for those who consume between
3 and 6
standard drinks per week; and
•
Increasingly high
for those who consume
7
standard drinks or more per week.
b. Consuming more than
2
standard drinks per drinking occasion is associated with an increased
risk of harms to self and others, including injuries and violence.
c. When pregnant or trying to get pregnant, there is no known safe amount of alcohol use.
d. When breastfeeding, not drinking alcohol is safest.
Sex and Gender
Above the upper limit of the moderate risk zone for alcohol consumption, the health risks
increase more steeply for females than males.
Far more injuries, violence and deaths result from men’s alcohol use, especially in the case of
per occasion drinking.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 7
The guidance is based on the principle of autonomy in harm reduction and a fundamental idea
behind it is that
people living in Canada have a right to know.
It is hoped that the guidance will be used to develop messaging that speaks directly to the unique
concerns of people with diverse backgrounds and personal experiences. It should serve to improve
alcohol literacy, providing information and suggestions so people are able to make their own choices
about how much they drink. The guidance will support health professionals, family doctors and
nurses who are crucial allies to help people assess their individual risk of harm from alcohol use.
The Guidance on Alcohol and Health is also intended to contribute to an evidence base for future
alcohol policy and prevention resources, with a view to changing Canada’s drinking culture and
curbing the normalization of harmful alcohol use in society.
The production of the Guidance on Alcohol and Health followed a rigorous and transparent approach
to assess the impact of various levels of alcohol use on deaths and disabilities. The analyses were
based on the most recent data and methods, which have evolved since the Low-Risk Alcohol
Drinking Guidelines were released in 2011. Analyses were supplemented by additional reviews on
specific topics and consultations with the public and experts.
Risk Associated with Weekly Levels of Alcohol Use
Throughout the life course, there are established thresholds of mortality risk that people are willing
to accept. For example, for involuntary risks such as air pollution, a 1 in 1,000,000 lifetime mortality
risk has been used as a gold standard. That is, people are willing to accept a negligible 1 in
1,000,000 risk of premature death when exposed to these risks.
• For risks associated with activities that people undertake deliberately and by choice, such as
unprotected sexual practices, smoking and so on, people may accept a level of risk that is about
1,000 times greater than the one for involuntary risk. Hence, advice and recommendations
made to people about voluntary activities generally use a
low risk level, equivalent to a 1 in
1,000 risk of premature death.
• However, for drinking alcohol, it is not unusual for guidelines to be based on a higher risk
threshold, 10 times that of voluntary activities. Recommendations for alcohol use have often
used a
moderate risk level, equivalent to a 1 in 100 risk of premature death.
Using these different thresholds, this project’s estimates make it possible to put forward a clear
continuum of risk whereby
the risk for those who consume 2 standard drinks or less per week is low,
it is moderate for those who consume between 3 and 6 standard drinks per week, and it is
increasingly high for those who consume above 6 standard drinks per week, with increasing risk
conferred by every additional drink.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 8
Figure 1. Continuum of risk associated with average weekly alcohol consumption
People should not start to use alcohol or increase their alcohol use for health benefits. Any reduction
in alcohol use is beneficial. This applies even for those who are unable or unwilling to reduce their
risk to low or moderate levels. In fact, those consuming high levels of alcohol have even more to gain
by reducing their consumption by as much they are able.
Figure 2. Illustration of examples standard drinks
Risk Associated with Alcohol Use Per Occasion
On any drinking occasion, the risk of acute outcomes such as unintentional injuries and violence is
strongly associated with cognitive and physical impairment from consuming too much alcohol.
The
risk of negative outcomes begins to increase with any alcohol use and consuming more than 2
standard drinks per occasion is associated with a significant increased risk of harms to self and
others.
Binge drinking, usually defined as consuming five or more standard drinks in one setting for men, or
four or more standard drinks in one setting for women, is a pattern of consumption that results in
legal impairment for most people. It is a well-established risk factor for death from any cause,

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 9
including unintentional injuries, violence, heart disease and high blood pressure, and inflammation
of the gastrointestinal system, and for developing an alcohol use disorder (i.e., alcohol dependence).
Many of the complications arising from acute impairment and binge drinking involve second-hand
effects that affect someone other than the person who drinks alcohol (e.g., violence, road crashes,
child abuse and neglect).
Risk when Pregnant, Trying to Get Pregnant or
Breastfeeding
Alcohol is a teratogen or agent that can cause malformation of the fetus. It can lead to learning,
health and social effects with lifelong impacts on the fetus as well as brain injury, birth defects,
behavioural problems, learning disabilities and other health problems typically referred to as fetal
alcohol spectrum disorder (FASD). These adverse effects are also observed at low levels of exposure
or short-term exposure to high levels of consumption. For this reason,
when pregnant or trying to get
pregnant, there is no known safe amount of alcohol use. Reproductive health is compromised by
alcohol use. Possible impacts of alcohol on pregnancy and delivery outcomes include increases in
miscarriage, hypertensive disorders of pregnancy and placental abnormalities.
Alcohol consumption can also negatively impact breastfeeding by causing a decrease in milk
production, early cessation of breastfeeding and effects on infant sleep patterns. Moreover, alcohol
enters breast milk through passive diffusion meaning that breastfeeding infants, who are less able to
metabolize alcohol, can be exposed to it. Therefore
, when breastfeeding, no alcohol use is safest for
the baby. Consuming a standard drink on occasion can be okay, as long as it is planned. It takes
about two hours for the alcohol contained in a standard drink to be eliminated from the body and
leave the breastmilk.
Sex and Gender
Alcohol use and harms are influenced by both sex-based physiological differences, as well as many
gender-related factors, including alcohol marketing tactics, and gender roles, attitudes and
expectations. Many harms from alcohol use are gender-related, including stigma, sexual assault and
intimate partner violence.
Risk for Women
The physiological differences between females and males at low levels of alcohol use have only a
small impact on lifetime risk of death. However, it is unequivocal that
above the upper limit of the
moderate risk zone for alcohol consumption (above 6 standard drinks per week), the health risks
increase more steeply for females than for males. Enzymes, genes, lean body weight and size, organ
function and metabolism are important in processing alcohol and are affected by sex-related factors.
These biological factors enhance the impact of alcohol on females, causing higher blood alcohol
levels, faster intoxication, more risk for disease, including breast cancer, and more long-term harm,
such as liver damage and injury.
Risk for Men
Men drink more alcohol than women and are more likely to drink in excess. Consequently, they are
more likely to be involved in alcohol-impaired driving collisions, to be treated in hospitals and
hospitalized for alcohol-related medical emergencies and health problems, to be diagnosed with an

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 10
alcohol use disorder and to die from alcohol-related causes. Alcohol is also more strongly associated
with perpetration of violence for men than for women.
Men are also more likely than women to take other risks (e.g., use other substances, drive under the
influence) that when combined with alcohol further increase their likelihood of experiencing and
causing alcohol-related harms. Overall,
far more injuries, violence and deaths result from men’s
alcohol use, especially in the case of per-occasion drinking.
Youth
Alcohol use is a leading behavioural risk factor for death and social problems among youth and
young adults, and alcohol is the most common psychoactive substance used by this age group. A
high proportion of alcohol consumed by youth is in the form of binge drinking with its attendant risks
of injuries, aggression, violence and other age-important consequences such as dating violence and
worsening academic performance. In addition, even for the same number of drinks consumed per
drinking occasion, the risk of adverse outcomes from alcohol consumption is greater for youth than
for adults. This may be due to several factors, including greater impulsivity and less emotional
maturity among youth, lower body mass on average, less experience doing complex tasks that are
made more dangerous by alcohol (e.g., operating a motor vehicle) and faster drinking speeds.
For this reason, recommendations related to the risks associated with weekly levels of alcohol use
and alcohol use per occasion do not apply to youth under the legal drinking age. For them, the main
message should be to
delay alcohol use for as long as possible.
When Zero’s the Limit
There are circumstances when no alcohol use is safest. For example, when:
• Driving a motor vehicle;
• Using machinery and tools;
• Taking medicine or other drugs that interact with alcohol;
• Doing any kind of dangerous physical activity;
• Being responsible for the safety of others; and
• Making important decisions.
Reasons for the New Guidance on Alcohol and Health
Alcohol and Cancer
Cancer is the leading cause of death in Canada. However, the fact that alcohol is a carcinogen that
can cause at least seven types of cancer is often unknown or overlooked. The most recent available
data show that the use of alcohol causes nearly 7,000 cases of cancer deaths each year in Canada,
with most cases being breast or colon cancer, followed by cancers of the rectum, mouth and throat,
liver, esophagus and larynx. According to the Canadian Cancer Society, drinking less alcohol is
among the top 10 behaviours to reduce cancer risk.
Alcohol and Heart Disease
After cancer, heart disease is the second leading cause of death in Canada. For many years, the
commonly held belief that drinking in moderation offered protection against coronary artery disease
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 11
has been widely publicized. Research in the last decade is more nuanced with the most recent and
highest quality systematic reviews showing that
drinking a little alcohol neither decreases nor
increases the risk of ischemic heart disease, but it is a risk factor for most other types of
cardiovascular disease, including, hypertension, heart failure, high blood pressure, atrial fibrillation
and hemorrhagic stroke.
Alcohol and Liver Disease
Statistics show that liver disease is on the rise in Canada, and alcohol is one of its main causes.
Drinking a large amount of alcohol, even for just a few days, can lead to a build-up of fat in the liver.
This is called alcohol-associated fatty liver. A more severe form of alcohol-related liver disease is
called alcohol-associated hepatitis, which is generally caused by alcohol abuse or, less commonly,
when people consume large amount of alcohol in a short period of time (binge drinking). Eventually,
ongoing alcohol-related liver injury can lead to the development of scar tissue in the liver, termed
fibrosis, which can lead to life-threatening cirrhosis and liver cancer.
Alcohol and Violence
Alcohol is frequently associated with violent and aggressive behaviour, including intimate partner
violence, male-to-female sexual violence, and aggression and violence between adults. Alcohol can
also increase the severity of violent incidents. No exact dose–response relationship can be established
but consuming alcohol increases the risk of perpetrating alcohol-related violence. It is therefore
reasonable to infer that individuals can reduce their risk of perpetrating aggressive or violent acts by
limiting their alcohol use. Based on consistent evidence, it is highly likely that
avoiding drinking to
intoxication will reduce individuals’ risk of perpetrating alcohol-related violence.
Policy Implications
To support people living in Canada who will want to drink less, governments, working in close
collaboration with employers, healthcare providers and community stakeholders, need to implement
policies that promote public health. Such policies include strengthening regulations on alcohol
advertising and marketing, increasing restrictions on the physical availability of alcohol, and adopting
minimum prices for alcohol.
As a priority, people living in Canada need consistent, easy-to-use information at the point of pour
to track their alcohol use in terms of standard drinks. They also have a right to clear and
accessible information about the health and safety of the products they buy. A direct consequence
of the current project is that a particular effective policy change could be the
mandatory labelling
of all alcoholic beverages with the number of standard drinks in a container, Canada’s Guidance
on Alcohol and Health and health warnings.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 12
Technical Report
Introduction
Canada’s first Low-Risk Alcohol Drinking Guidelines (LRDGs) were originally published by the
Canadian Centre on Substance Use and Addiction (CCSA) in November 2011 (Butt et al., 2011). The
guidelines were developed by an independent expert working group, with members drawn from
Canadian addiction research agencies. The 2011 LRDGs provided people living in Canada with
advice on how to minimize relative long-term risk of serious diseases caused by the consumption of
alcohol over a number of years (e.g., liver disease, some cancers) and relative short-term risk of
injury or acute illness due to the overconsumption of alcohol on a single occasion (Stockwell et al.,
2012). In addition, specific recommendations were provided for situations and individual
circumstances that are particularly hazardous and for which abstinence or only occasional light
intake was advised (e.g., just before or during pregnancy, teenagers, people on medication). The
guidelines also included tips for safer drinking and the definition of a standard drink. The 2011
LRDGs were a significant step to providing consistent information and messaging for minimizing the
risk associated with drinking alcohol. They have provided the cornerstone for undertaking a variety of
health promotion, prevention and education initiatives across the country (Paradis, 2016).
Still, there were important limitations with the research evidence used to develop the 2011 LRDGs.
In the LRDG technical report
(Butt et al., 2011), the working group noted the under-reporting of
personal alcohol use in self-reported surveys, the failure to take account of heavy drinking episodes
in many epidemiological studies, the misclassification of former and occasional drinkers as lifetime
abstainers, and the failure to control for confounding effects of personality and lifestyle factors
independent of alcohol. In its quality appraisal, using the AGREE II instrument, the Public Health
Agency of Canada (PHAC) further noted limitations, particularly with respect to the rigour of
development and editorial independence, two domains that did not receive the minimum acceptable
score of 60%. Consequently, the 2011 LRDGs received an overall assessment of 60.7% and so did
not meet the criteria for high quality guidelines. They were recommended for use with modifications,
and since then it has been known that careful consideration would need to be paid to these
limitations when developing alcohol guidelines.
Awareness and Adherence to the 2011 LRDGs by People
Living in Canada
Since their publication, the 2011 LRDGs have been promoted to varying degrees across the country
and adopted differently by key demographics. In 2012, just a few months after the release of the
guidelines, a national survey indicated that a quarter (26%) of people living in Canada had seen or
heard of the LRDGs. Since then, a few provincial studies have recorded people’s awareness of the
LRDGs. In 2017, Public Health Ontario surveyed 2,000 adults in Ontario aged 19 and older who
consume alcohol and found that less than a fifth (17%) were aware of the 2011 LRDGs (Public
Health Ontario, 2017a). In 2019–2020, the new Canadian Postsecondary Education Alcohol and
Drug Use Survey (CPADS) surveyed students in colleges and universities in Canada about their
knowledge of the 2011 LRDGs (Health Canada, 2021). Not surprisingly, within this young group,
awareness was negligible with only 16% reporting to have heard about the guidelines and less than
a third of those (28%), being able to accurately report what the guidelines were.
In Quebec, significant resources have been invested to disseminate and promote the 2011 LRDGs
(Paradis, 2016). No study has specifically surveyed Quebecers’ knowledge of the guidelines, but a
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 13
study conducted by the Institut national de santé publique du Québec found that 55% of Quebecers
thought the 2011 LRDGs were adequate, while 37% believed they were too high, that is, corresponded
to larger amounts of alcohol than what they consider to be low-risk drinking (Bergeron et al., 2021).
According to the most recent data from the
Canadian Alcohol and Drugs Survey (CADS, Health
Canada, 2019), a majority of people living in
Canada indicated drinking within the 2011
LRDGs. In 2019, 83% of the people aged 15 years
and older who consumed alcohol in the past year
reported to drink within the guidelines for short-
term risk and 77% within those for long-term risk.
While more females than males reported to drink
alcohol within the guidelines for short-term risk
(85% vs 81%), the percentages were similar for
the long-term risk guideline (76% for males vs
78% for females). Young adults between the ages
of 20–24 were less likely than other age groups to
drink within the guidelines. In 2019, three-
quarters (74%) followed the guideline for short-
term risk of injury and harm while 69% reported to
follow the guidelines for long-term health risk.
While the percentages seem to indicate general adhesion to the 2011 LRDGs, the reality may be
otherwise. The CADS estimates are based on the alcohol consumption in the previous seven days,
meaning that people who consumed alcohol in the past year but did not have a drink in the week
preceding the survey are automatically considered as not exceeding the 2011 LRDGs. This seems
very unlikely given Canada’s timeout culture where people drink to mark special occasions rather
than on a regular daily basis. In fact, a study conducted in 2015 explored adherence to the LRDGs
while attempting to adjust for the under-reporting of alcohol consumption (Zhao et al., 2015). It was
found that 73% of people living in Canada over the age of 15 followed the weekly limits while 61%
followed the daily limits recommended by the LRDGs. In Ontario, the Public Health Ontario survey
found that 39% of people who used alcohol in the Ontario sample regularly exceeded the LRDG daily
limits and 27% the weekly limits (Public Health Ontario, 2017a). According to CPADS , a majority
(88%) of students who use alcohol reported following the guidelines for long-term risk, but only 36%
indicated drinking within the recommendations for short-term risk (Health Canada, 2021). Zhao and
colleagues (2015) also found that, after adjustment for under-reporting, more than 80% of all drinks
consumed in Canada were consumed in a fashion inconsistent with the LRDGs.
Time to Update
There are no set criteria for updating health guidelines to ensure they remain current and evidence
based, but an update is typically recommended when new evidence is identified that is relevant and
important or could alter current guidelines (Vernooij et al., 2014). Over the last decade, several
reasons that justify an update of the 2011 LRDGs have been identified.
First, knowledge on and estimates of relations between different dimensions of alcohol use and
particular diseases, disorders or injuries have been evolving since 2011. Research now confirms the
importance of alcohol use as a risk factor for an increasing number of diseases including at least
seven types of cancers, dementia and sexually transmitted diseases (International Agency for
Research on Cancer, 2012; Lu et al., 2017; Rehm et al., 2017). Second, a Canadian study showed
Canada’s 2011 LRDGs
The 2011 LRDGs recommended people who
consume alcohol to reduce:
• Long-term health risk by drinking no
more than 10 standard drinks a week for
women, with no more than two drinks a
day most days, or 15 standard drinks a
week for men, with no more than two
drinks a day most days.
•
Short-term risk of injury and harm by
drinking no more than three standard
drinks for women or four standard drinks
for men on any single occasion.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 14
that more than 50% of alcohol-attributable cancer deaths in British-Columbia are among former
alcohol users and people using alcohol within the 2011 LRDGs for long-term risks (Sherk et al.,
2020). People living in British-Columbia who use alcohol within the LRDG’s weekly limits also
account for 65% of hospital stays due to unintentional injuries and a substantial percentage of
deaths due to digestive conditions (18%) and injuries (40%), suggesting that reducing the burden of
disease requires revising the 2011 LRDGs (Sherk et al., 2020). Third, countries like the United
Kingdom, France, Denmark, Holland and Australia recently reviewed new evidence on alcohol and
health and released updated guidelines with limits significantly different from the 2011 LRDGs, with
weekly limits ranging from the equivalent of 5.2 to 8.3 Canadian standard drinks for women and
men alike.
2
Finally, given recent reports on the extent to which alcohol use causes social problems
for individuals other than the drinkers themselves (Laslett et al., 2019), there has been curiosity as
to what alcohol guidelines would be if social and mental health harms were also included in addition
to diseases, disorders and injuries.
The Canadian 2011 LRDGs did not include an expiration date but given the limitations and in light of
the new evidence, in early 2019, CCSA, Health Canada, PHAC and members of the Canadian 2011
LRDGs working group engaged in discussions to update the guidelines. In July 2020, Health Canada
confirmed funding to CCSA to update Canada’s LRDGs and make recommendations for knowledge
mobilization to maximize dissemination and application of the updated guidelines. The mandate
specified building on the guidelines from the United Kingdom (U.K. Chief Medical Officers, 2016) and
Australia (National Health and Medical Research Council, 2020), which had provided access to the
underlying evidence base supporting their alcohol guidelines. It was further agreed that CCSA would
be responsible for overseeing and facilitating the updating process. Health Canada would provide
advice, support and guidance through membership on the project’s various committees, plus
administrative support. PHAC would provide methodological advice and support.
Aim and Scope of This Report
Canada’s Guidance on Alcohol and Health is intended to replace Canada’s Low-Risk Alcohol Drinking
Guidelines. It provides accurate and current information about the risks and harms associated with
the use of alcohol. The guidance should help people make well-informed and responsible decisions
about their alcohol consumption. The Guidance on Alcohol and Health is also intended to contribute
to an evidence base for future alcohol policy and prevention resources, with a view to changing
Canada’s drinking culture and curbing the normalization of harmful alcohol use in society.
In the interests of transparency and because developing best practices for defining alcohol drinking
guidelines remains a work in progress (Holmes et al., 2019), this report will describe the updating
process, so that others can learn from the Canadian experience. The report is divided into three
main parts:
1. The construction of experts’ recommendations;
2. The evidence used by the experts; and
3. The experts’ recommendations for updated alcohol guidelines in Canada.
2
Around the world, what constitutes a standard drink ranges from 8 to 20 grams of pure alcohol. In Canada, it is defined as 13.45 grams
(Paula et al., 2020). Some say that Canada’s particular standard drink was chosen because it corresponds to the measure of whisky
traditionally available in Canadian bars (Miller et al., 1991). A more probable reason is that it corresponds to the amount of pure alcohol
contained in 341 ml bottles of 5% beer, which has traditionally been the alcoholic beverage of choice in Canada.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 15
Part 1: Development of Experts’ Recommendations
To update the 2011 LRDGs, four committees were convened. An executive committee with members
from federal, provincial and territorial governments, and national organizations was established to
provide project oversight and advice. Three scientific expert panels were established to review the
evidence for updating the guidelines and making recommendations on how best to mobilize this new
knowledge effectively. One panel focused on the impacts of alcohol consumption on physical health,
a second one on the social and mental health effects, and a third on knowledge mobilization.
To provide scientific support to members of scientific expert panels (hereafter referred to as the
experts), CCSA further established an internal Evidence Review Working Group responsible for
evaluating and summarizing evidence, leading consultations and conducting new research as
needed.
Members of the executive committee and the experts were required to disclose affiliations and
interest, as per Schünemann et al. (2013). The list of potential conflicts of interest was published on
CCSA’s website in Disclosure of Affiliations and Interests
.
1.1 Defining Research Questions
The general research question underlying the 2011 LRDGs update is as follows: To minimize the risk
of developing alcohol-related physical and mental health disorders and social problems, which level
or pattern of use should be recommended to people living in Canada?
For this question to lead to evidence-based guidelines, three more specific questions were
developed, each one specifying a particular target population, the level of exposure to alcohol and
the type of outcomes being considered. (For more information, see
Update of Canada’s Low Risk
Alcohol Drinking Guidelines: Development of Research Questions.) It is these three specific research
questions that have guided this project’s evidence collection, analyses and conclusions:
1. What are the short-term risks and benefits (physical and mental health, and social impact)
associated with varying levels of alcohol consumption (including no alcohol consumption), in
different contexts, associated with a single episode of drinking in the general population?
2. What are the long-term risks and benefits (physical and mental health, and social impact)
associated with varying levels and patterns of alcohol consumption (including no alcohol
consumption) in the general population?
3. What are the risks and benefits (physical and mental health, and social impact) associated with
varying levels and patterns of alcohol consumption (including no alcohol consumption) during
pregnancy or breastfeeding, for fetal, infant and child development?
The specific questions were formulated to encompass all effects, so that studies focusing on both
positive and negative effects could be identified.
1.2 Estimating the Lifetime Risk of Alcohol-Related Death
and Disability in the Canadian Population
From the outset of this project, there was a common understanding among experts that to update
the 2011 LRDGs, the specific research questions would be answered through mathematical
modelling. Modelling had previously been used to establish the 2011 LRDGs as well as alcohol
guidelines in Australia (National Health and Medical Research Council, 2020), the U.K. (U.K. Chief
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 16
Medical Officers, 2016) and France (Santé publique France & Institut national du cancer, 2017).
Moreover, since 2016, the European Union Joint Action on Reducing Alcohol-Related Harm has
recommended the use of cumulative lifetime risk of death from alcohol-related disease or injury as a
common metric for assessing the risks from alcohol at the country level; the metric should also
inform discussions by experts to establish alcohol guidelines (Broholm et al., 2016).
Modelling requires alcohol mortality risk functions for all disease or injury categories causally related
to alcohol consumption. These risk functions can be found in meta-analyses that assess the dose–
response relationship between alcohol and the risk of disease mortality
. The quality of modelling
depends upon the quality of the risk functions and therefore on the identification of the highest
quality meta-analyses. Such identification is a complex and lengthy process that could have gone
over the 21 months allocated to update the 2011 LRDGs. However, the project’s mandate stipulated
that the update should be informed by the 2016 alcohol guidelines from the U.K. (U.K. Chief Medical
Officers, 2016) and the 2020 Australian guidelines to reduce health risks (National Health and
Medical Research Council, 2020). Therefore, a quality assessment of these alcohol guidelines was
performed. (For more information, see
Updating Canada's Low-Risk Alcohol Drinking Guidelines:
Evaluation of Selected Guidelines.) With regards to its methodology for identifying and selecting
evidence on the risks and benefits associated with alcohol consumption, the Australian guidelines
received top ratings.
Hence, to update Canada’s LRDGs, the global evidence review did not start from scratch, but rather
built upon the rigorous and systematic work previously done by the Australian Alcohol Working
Committee (AAWC), which covered the January 2017 to February 2021 period. (The overall process
is explained in section 2.1.) Besides ensuring the quality of the modelling, the global evidence review
on the risks and benefits associated with alcohol consumption identified areas where high quality
systematic reviews were missing; for these areas, the experts agreed to commission additional
reviews to formulate the updated guidelines for Canada.
1.3 The Evidence Base for Updating the Guidelines
A range of inputs was considered in updating the 2011 LRDGs:
• Global evidence review of the effects of alcohol on health;
• Mathematical modelling of the lifetime risk of death and disability for various levels of average
alcohol consumption;
• Rapid review on alcohol and mental health;
• Rapid review on alcohol and violence; and
• Comprehensive multi-part review of recent literature on women’s health and alcohol.
This project’s mandate also required recommendations for knowledge mobilization of the updated
alcohol guidelines. To this end, a series of activities was undertaken to better understand people’s
views, preferences and expectations on alcohol guidelines. Discussions on formulation and
presentation of the finalized guidelines were further informed by the following activities:
• Summary Evidence on Understanding and Response to Alcohol Consumption Guidelines
;
• Public consultation to hear what alcohol, health and well-being issues matter most and what is
most useful to people in Canada;
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 17
• Interviews with representatives from different health-related organizations that have an interest
in alcohol-related issues; and
• Focused discussions with Indigenous People serving on the LRDG executive committee and
scientific expert panels.
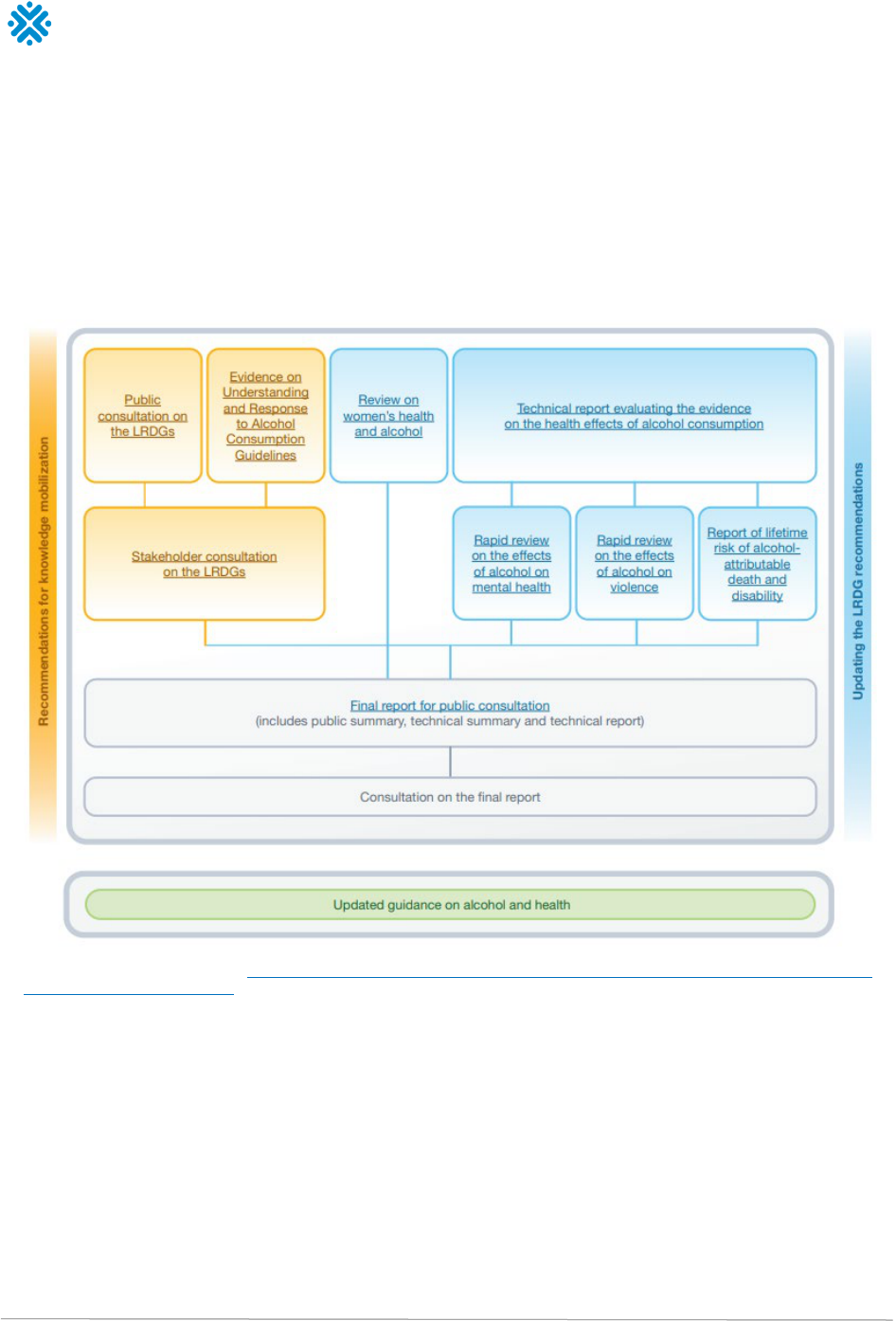
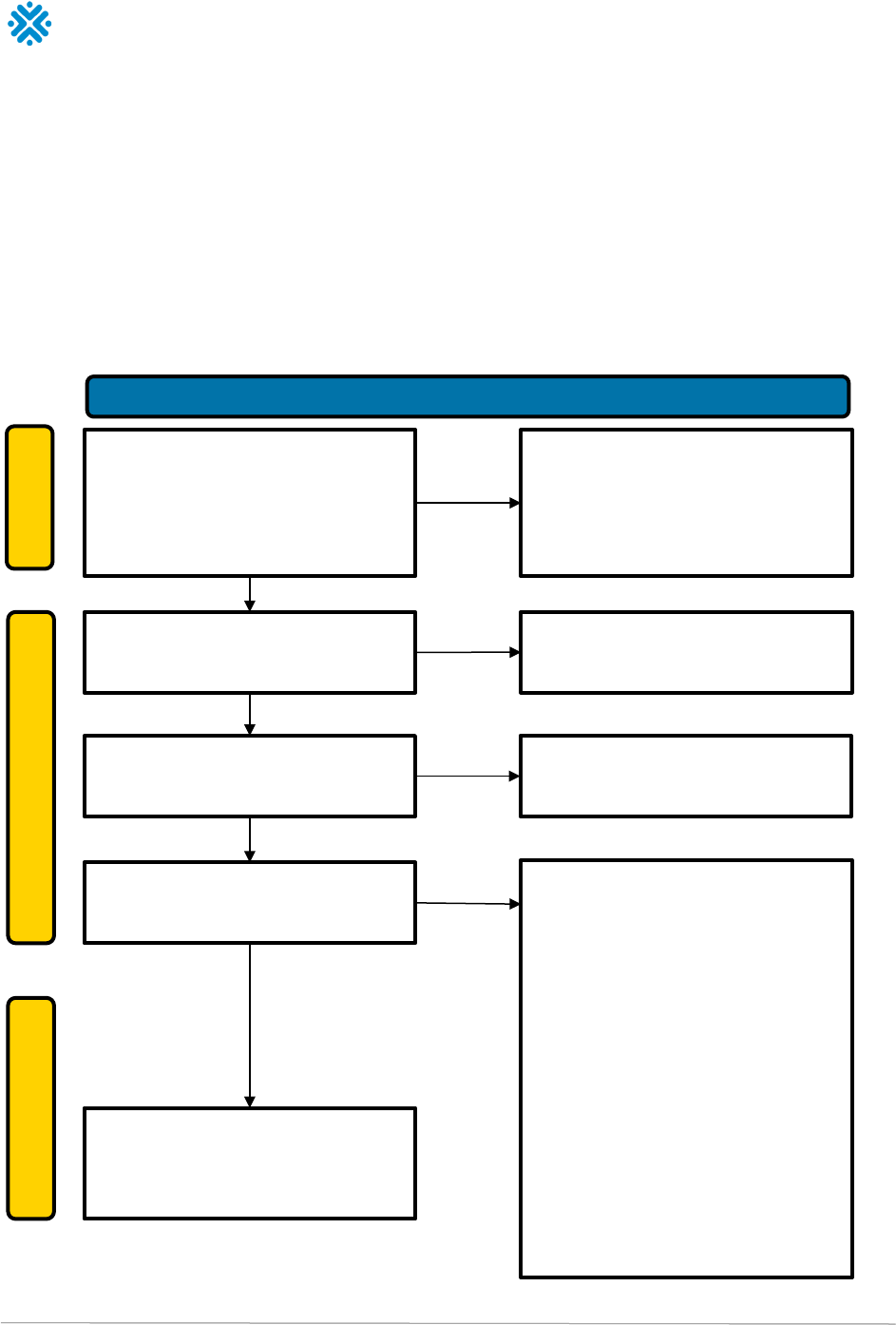
The overall process by which the recommendations were developed is illustrated in Figure 1.
Figure 1: Process for updating Canada’s LRDGs
Note. For a PDF of this image, visit https://ccsa.ca/sites/default/files/2023-01/CCSA-LRDG-Lower-Risk-Drinking-Guidelines-Process-
and-Documentation-2023-en.pdf.
1.4 Reaching Conclusions and Formulating
Recommendations
This project was conducted during the COVID-19 pandemic and its associated stay-at-home and
travel restrictions. Therefore, all meetings held during this project were conducted online, except the
last three-days meeting to review the results of the open consultation, which was held in-person.
Despite the challenging context, the co-chairs of the scientific expert panels created an online
environment that was conducive to respectful dialogue and the healthy exchange of ideas. The
project comprised three scientific expert panels, but due to the overlap and interest in all the panel
evidence-review activities, experts were invited to attend all panel meetings.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 18
Between September 2020 and October 2022, members of the scientific expert panels met on 18
occasions to discuss the process and the evidence used to develop the recommendations. Efforts
were deployed for panel members to engage in a dialogue and share information for the purpose of
increasing the understanding of the issues and to provide a rationale for choosing a particular position.
The main conclusions and agreement on final recommendations was reached through consensus.
Part 2: Evidence Used to Construct the
Recommendations
The studies and evidence reviews informing the update to the 2011 LRDGs are available on the
CCSA webpage dedicated to this project
. Those interested in understanding in detail the types of
evidence and the way they were used to update the guidelines are encouraged to visit the webpage
to access the full reports. The following sections provide summaries of each report, to give readers
an overview of the material reviewed by the experts to reach their conclusions.
2.1 Global Evidence Review on the Effects of Alcohol on
Health
Several studies have quantified the risk relationships between alcohol use and the occurrence of and
mortality from all disease or injury categories causally related to alcohol consumption. However, the
quality of these studies varies greatly. To provide an answer to this project’s three research questions
and estimate the impact of alcohol consumption on individuals, a systematic search and review was
performed of meta-analyses that reported alcohol dose–response curves between different average
levels of alcohol use, disease and injuries. The aim was to identify the highest quality systematic
reviews and meta-analyses using a standard set of quality criteria. (For the full report, see
Update of
Canada’s Low-Risk Alcohol Drinking Guidelines: Evidence Review Technical Report.)
2.1.1. Methods
A systematic electronic search was performed using PubMed, PsycNET, Embase, Cochrane Library,
Database of Abstracts of Reviews of Effects, Health Technology Assessment Database, International
Health Technology Assessment Database, Joanna Briggs Institute, Database of Systematic Reviews
of Effects, and Epistemonikos. The search was limited to articles published from Jan. 6, 2017, to
Feb. 17, 2021. It provided an update to the AAWC systematic review for 2007 to 2017. All articles
included in the Australian’s systematic review were also included in this review (National Health and
Medical Research Council, 2020).
An information specialist screened the search results and removed duplicates and any articles that
were clearly outside of the scope of the project based on titles and abstracts. Two independent
investigators assessed articles for title and abstract, and subsequently for full-text eligibility against:
• The study design and the Population, Exposure, Comparator and Outcome (PECO) criteria;
• Methodological quality criteria selected from A MeaSurement Tool to Assess systematic Reviews
(AMSTAR 2; Shea et al., 2017) and Risk of Bias in Systematic Reviews (ROBIS; Whiting et al.,
2013) tools;
• Methods of analyses criteria; and
• Mathematical modelling criteria.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 19
If a particular disease or injury category was considered by more than one systematic review or
meta-analysis, priority was given to the article that met the most methodological quality criteria. In
the event that the same number of criteria were met, the most recent article was given priority.
Finally, the quality of each e
ligible systematic review and meta-analysis was assessed by two
independent investigators using two international standard tools: A MeaSurement Tool to Assess
systematic Reviews (AMSTAR 2; Shea et al., 2017), and the Grading of Recommendations,
Assessment, Development and Evaluations system (GRADE; Schünemann et al., 2013). Studies were
also evaluated for the inclusion of sex- and gender-based analysis (Brabete et al., 2020).
Figure 2. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram
Records identified from:
• Databases (n = 5884)
• Grey literature (n = 31)
• Australian search (n=38)
Records removed by information
specialist:
• Duplicate records removed (n = 325)
• Records outside of the scope of the
project removed (n = 4848)
Records screened
(n = 780)
Records excluded
(n = 541)
Reports sought for full-text retrieval
(n = 239)
Reports not retrieved
(n = 0)
Reports assessed for inclusion eligibility
(n = 239)
Reports excluded:
• Did not met the PEO/study type
criteria (n = 146)
• Methods of analysis insufficient
(n = 11)
• Newer review identified and/or met
more criteria (n = 20)
• No ICD-10 code available (n = 4)
• No dose-response (n = 6)
• No causal relationship with alcohol
consumption (n = 26)
• Reverse causality with alcohol
consumption (n = 1)
• Not a fatal disease (n = 4)
• Alcohol consumption while
pregnant (n = 5)
Reports included in the mathematical
modelling (n = 16)
Identification of studies via databases and registers
Identification
Screening
Included

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 20
2.1.2 Results
In addition to the 38 systematic reviews already identified by the AAWC, a total of 5,915 systematic
reviews were initially retrieved from the updated search. The PRISMA (Preferred Reporting Items for
Systematic Reviews and Meta-Analyses) flow diagram presented in Figure 2 illustrates that after
removing duplicates and any articles that were outside of the scope of the project,
a subset of 780
systematic reviews were screened for title and abstract and a total of 239 systematic reviews (37
identified by the AAWC and 202 identified by this update) were subsequently screened for full-text
eligibility.
The 31 reports identified by the search of the grey literature were excluded as PECO and study
design criteria were not met. Most of the grey literature items were found to be informative
brochures, reports, fact sheets and books.
In the end, a total of 16 systematic reviews fulfilled all the inclusion criteria for this project for all
three research questions and were selected for inclusion in the mathematical modelling.
Research Question 1: Short-Term Risks and Benefits
Twenty-nine systematic reviews on the short-term risks and benefits of alcohol were evaluated. Two
systematic reviews were selected for inclusion in the mathematical modelling. One selected review
focused on road injury (Taylor & Rehm, 2012) and the other on intentional and unintentional injuries
(Taylor et al., 2010).
Research Question 2: Long-Term Risks and Benefits
A total of 154 systematic reviews across eight categories of diseases associated with the long-term
health risks and benefits of alcohol were evaluated.
Fourteen reviews were selected for inclusion in
the mathematical modelling. The selected reviews assessed the relationship between alcohol use
and liver cirrhosis (Roerecke et al., 2019), ischæmic heart disease (Zhao et al., 2017; for relative
risks, see fully adjusted relative risks for people 19 to 55 years of age at baseline outlined in Table
3), hypertensive heart disease (Liu et al., 2020), breast cancer (Sun et al., 2020), liver cancer (World
Cancer Research Fund International, 2018), pancreatitis (Samokhvalov et al., 2015), lower
respiratory infections (Samokhvalov et al., 2010a), epilepsy (Samokhvalov et al., 2010b) ischemic
stroke, intracerebral hemorrhage, subarachnoid hemorrhage (Larsson et al., 2016), atrial fibrillation
(Larsson et al., 2014), colon and rectum cancers (Vieira et al., 2017), diabetes mellitus (Knott et al.,
2015), larynx cancer, mouth and oropharynx cancers, esophagus cancer (Bagnardi et al., 2015) and
tuberculosis (Imtiaz et al., 2017). The relative risks obtained from systematic reviews were not
adjusted for misestimation of alcohol use. Although there is a hypothesis of a slight underestimation
of alcohol use in medical epidemiology studies (Stockwell, 2018), the direction of alcohol use
measurement bias in cohort studies is unknown (Biemer et al., 2013; King, 1994).
Research Question 3: Pregnancy and Child Development Risks and
Benefits
Twenty-five systematic reviews focusing on the risks and benefits associated with alcohol
consumption during pregnancy or breastfeeding for fetal, infant and child development were
evaluated.
None were selected for inclusion in the modelling because none met the mathematical
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 21
modelling criteria. The studies focused on alcohol-attributable mortality and morbidity to others
rather than the person who consumes alcohol.
2.1.3 Quality of Evidence
The quality of each retained systematic review was assessed with AMSTAR 2 and GRADE. (For the
full AMSTAR and GRADE assessments, see
Update of Canada’s Low-Risk Alcohol Drinking
Guidelines: Evidence Review Technical Report.)
The systematic reviews used PECO questions and clearly presented inclusion criteria. All were based
on strong and rigorous methods for statistical combination of their results. Retained reviews also
examined dose-dependent relationships through pooled analyses, which is indicative of high-quality
methods. The majority of retained reviews also described the included studies with a good amount of
detail justifying their inclusion. The review search strategies were detailed and many of the studies
conducted the screening steps in duplicate. Most of the retained reviews had no imprecision and
indirectness according to GRADE. However, many of the retained reviews did not assess risk of bias.
Heterogeneity was also reported for many of the reviews and, despite conducting sensitivity
analyses, the source for heterogeneity was seldom identified. Hence, the overall quality score of
most retained reviews was low but this was expected.
Tools used to assess the quality of identified systematic reviews consider randomized clinical trials
the gold standard. However, for examining the association between alcohol consumption and health,
this study design is neither practical nor ethical. For example, it would be unethical to randomize one
group of females to drink alcohol on a daily basis for 10 years and another one to abstain, and then
test who develops breast cancer. In fact, in the field of alcohology most evidence is derived from
cohort and observational studies that have inherent limitations that explain why many systematic
reviews retained for this project did not receive a high-quality score. However, in no way does this
mean that the quality of evidence is insufficient to provide guidance on alcohol and health to people
living in Canada. In fact, there is a high level of confidence among members of the scientific expert
panels and the Evidence Review Working Group that the identified reviews covered in this report are
the latest and most high-quality evidence available to examine this public health issue.
2.1.4 Implications
The global evidence review identified the most recent and highest quality systematic reviews and
meta-analyses available to examine the relationship between alcohol consumption and the various
outcomes covered by this project’s research questions. The methodology used to select these
systematic reviews is based on the Australian guidelines, which received a top score according to a
previous evaluation, further strengthening our certainty that our results are based on the highest
quality evidence. (For more information, see
Update of Canada's Low-Risk Alcohol Drinking
Guidelines: Evaluation of Selected Guidelines.)
Through this work, we identified areas where high quality systematic reviews are currently missing
(e.g., mental health, violence) and for which the experts agreed to commission additional reviews to
complete the LRDG update (see section 2.4). A decision was also taken to commission a report on
women’s health and alcohol that would address, among other things, the issues of pregnancy.
2.2 Mathematical Modelling of the Lifetime Risk of Death
for Various Levels of Average Alcohol Consumption
To establish alcohol guidelines, modelling the lifetime risk of death for various levels of average
alcohol consumption has been recommended (Broholm et al., 2016; Rehm et al., 2014) and applied
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 22
(e.g., in Australia, the U.K., France and Canada). Modelling allows for the estimation of the “excess
risk” of mortality and disability associated with various levels of average consumption and the
specification of the level of risk from negligible to high associated with each level of consumption.
The aim of modelling is not to set a “threshold” of consumption below which there is no risk, but to
provide “benchmarks” based on which recommendations can be formulated.
For this project, the lifetime risk approach was adopted to estimate the lifetime risk of death,
premature death (< 75 years of age), years of life lost (YLLs) and disability-adjusted life years (DALYs)
lost. A full report presenting all analyses is available in
Lifetime Risk of Alcohol-Attributable Death
and Disability. Every estimation and result presented in the report was subsequently the object of a
shadow analysis that confirmed the accuracy of the primary analyses (Appendix 1).
Discussions among experts led to a decision to use risk thresholds associated with YLLs. Compared
to using lifetime risk of death or premature death, YLLs allows researchers to consider the deaths of
older individuals and, more importantly, factors the unequal health loss caused by death among
people relatively younger in age. While DALYs can be an optimal outcome for the measurement of
health loss attributable to alcohol, there is limited data on the DALYs alcohol cause and this project’s
analyses resulted in identical risk thresholds whether they were based on YLLs or DALYs.
3
Since
DALYs is conceptually more difficult to understand than YLLs, the experts fixed their choice on YLLs
estimations. Results are presented and discussed below, after a review of methodological principles.
2.2.1 Methodological Principles
Calculating Alcohol-Attributable Deaths
In epidemiology, the concept of an attributable fraction makes it possible to express the proportion
of risk for a particular health event (in this case death), due to exposure to a particular cause (in this
case alcohol consumption). An attributable fraction is classically calculated from the number of
deaths that could be avoided if the exposure was eliminated.
The proportion depends on the risk of death according to sex and age but also on the “trajectory” of
exposure, which is the history of alcohol consumption before the subject’s death. Establishing
alcohol-attributable deaths in the population requires access to the population’s mortality rate and
knowledge of the individuals’ lifetime exposure to alcohol in standardized terms, such as average
grams of alcohol per day. With this data, alcohol-attributable deaths can be calculated for various
levels of consumption, provided that it is considered identical among individuals and constant over
time for each of them until death. In this model, lifetime abstainers are the reference group in relation
to which the risks associated with different average levels of alcohol consumption are calculated.
By varying the average level of consumption in such a scenario, it becomes possible to summarize
the relationship between the risk due to alcohol and different levels of consumption. In return, this
informs the benchmarks for different levels of risk.
3
For example, there is evidence that DALYs can be influenced by mental disorders such as depression but because the evidence search
did not identify high-quality systematic reviews assessing the relationship between alcohol use and mental health, it is likely that the
current project underestimates alcohol-related DALYs.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 23
Diseases and Injuries Included in the Modelling
A total of 34 cause categories for alcohol-related diseases, conditions and injuries and more than
200 three-digit International Classification of Disease, version 10 (ICD-10-CA) codes were included in
the modelling of alcohol-attributable deaths. To be included, there were three criteria:
1. The disease or injury had to be causally related to alcohol use;
2. A dose–response risk function needed to be available for the risk relationship between alcohol
consumption (measured in grams per day) and the disease or injury of interest that also passed
the GRADE criteria; and
3. Either death or disability needed to be measured specifically for the disease or injury causally
related to alcohol use.
What Evidence Has Changed Since the Release of the 2011 LRDGs?
• Animal, mechanistic and epidemiological evidence published since the publication of the
Canadian LRDGs in 2011 has led to changes in the diseases that are known to be causally
related to alcohol use.
• Alcohol has been found to causally increase the risk of lower respiratory infections
(Samokhvalov et al., 2010a).
• Systematic reviews on the risk relationship between alcohol use and the diagnosis of and
death from cancer have observed no lower risk threshold (Bagnardi et al., 2015; Sun et al.,
2020; Vieira et al., 2017; World Cancer Research Fund International, 2018).
• The risk relationship between alcohol use and hypertensive heart disease has been observed
to have no lower risk threshold (Liu et al., 2020).
• Risks for hemorrhagic stroke have been investigated further, with the risk functions for
intracerebral hemorrhage showing protective effects at lower levels of alcohol use but for
subarachnoid hemorrhage, detrimental effects at lower levels of alcohol use (Larsson et al., 2016).
• Alcohol’s protective impact on ischemic heart disease at lower levels of alcohol use is more
uncertain than previously estimated. The risk is modified by binge drinking (Roerecke & Rehm,
2010; Sundell et al., 2008) and genetics (Chikritzhs et al., 2015; Larsson et al., 2020).
Data Sources
Several data sources were used to make the necessary calculations:
• Data on death and disability for 2017 to 2019 were obtained from Statistics Canada and the
Institute for Health Metrics and Evaluation’s Global Burden of Disease study (2018).
• Alcohol exposure data were obtained from the Canadian Alcohol and Drug Use Monitoring Survey
and the Canadian Tobacco, Alcohol and Drugs Survey. Survey data were corrected for total
consumption in Canada (adult per capita consumption) using data from Statistics Canada (2021)
and the World Health Organization’s Global Information System on Alcohol and Health (2021).
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 24
• Relative risk estimates for diseases and injuries were obtained following the evidence review
(see previous section) that enabled us to identify the highest quality meta-analyses.
The calculations for this project are based on the health harms cause by ethanol in alcoholic
beverages. They do not distinguish between harms caused by beer, wine, spirits and other
alcoholic beverages. Harms caused by beer, wine, spirits and other alcoholic beverages are based
mainly on ethanol content, regardless of the form in which ethanol is consumed. Alcohol
poisonings, which are caused predominately by the consumption of spirits, are the one exception
where the type of alcoholic beverage makes a difference (Rehm, et al., 2017).
2.2.2 Results and Implications
The relative risk estimates by cause of disease and average weekly alcohol consumption are
outlined in Table 1 for females and Table 2 for males. The absolute risk estimates (measured in
YLLs) by cause of disease and average weekly alcohol consumption are outlined in Table 3 for
females and Table 4 for males. For most diseases and injuries, alcohol had a net negative impact on
health at all levels of alcohol use, with net impacts being defined by confidence intervals not
crossing a zero effect. For diabetes mellitus (females only), ischemic stroke and pancreatitis
(females only), alcohol was associated with a protective effect at lower levels of alcohol use.
However, for ischemic heart disease and intracerebral hemorrhage, alcohol was neither associated
with a negative nor protective net effect at lower alcohol use amounts. (Confidence intervals
associated with increased risk of diseases and injuries are presented in Appendix 2.)
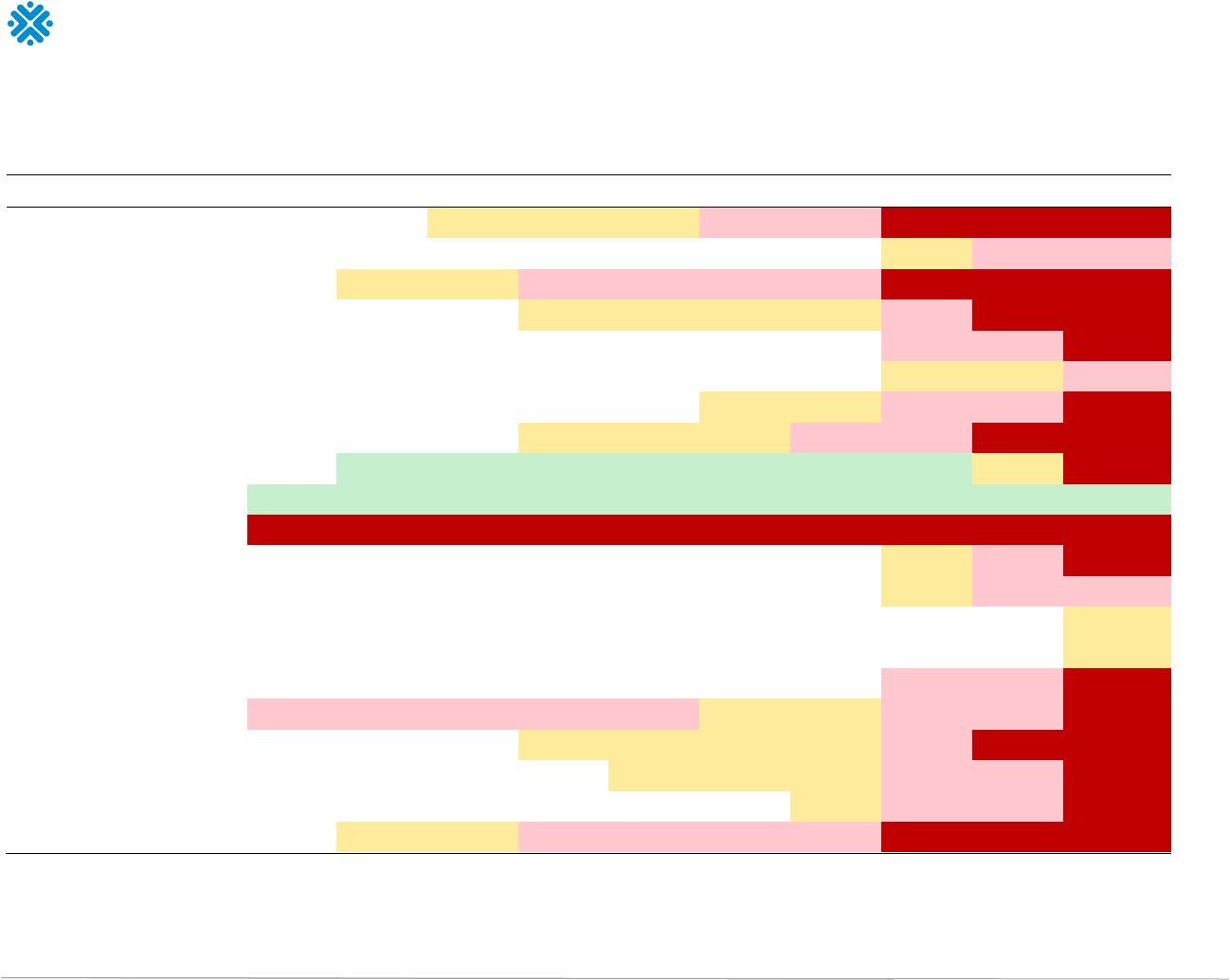
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 25
Table 1. Increased risk of diseases and injuries for females based on average weekly alcohol use (standard drinks per week)
Disease or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 3.7% 7.5% 11.4% 15.5% 19.7% 24.1% 26.3% 62.4% 105.2% 233.3%
Lower respiratory infections 1.0% 1.9% 2.9% 3.9% 4.9% 5.9% 6.4% 13.7% 21.0% 37.6%
Oral cavity and pharynx cancer 5.1% 10.3% 15.8% 21.6% 27.6% 33.8% 37.0% 89.4% 152.3% 338.4%
Oesophagus cancer 2.7% 5.4% 8.2% 11.1% 14.1% 17.2% 18.7% 42.7% 69.1% 139.3%
Colorectal cancer 1.4% 2.7% 4.1% 5.6% 7.0% 8.5% 9.2% 20.0% 31.1% 57.4%
Liver cancer 0.8% 1.6% 2.4% 3.2% 4.0% 4.8% 5.2% 11.2% 17.0% 30.1%
Breast cancer 1.8% 3.7% 5.6% 7.6% 9.5% 11.6% 12.6% 27.9% 44.0% 84.2%
Larynx cancer 3.0% 6.0% 9.1% 12.3% 15.5% 18.8% 20.5% 46.3% 73.8% 143.5%
Pancreatitis -5.3% -10.3% -15.0% -19.2% -22.7% -25.5% -26.7% -20.8% 14.8% 173.9%
Diabetes Mellitus -15.2% -19.9% -23.0% -25.2% -26.9% -28.3% -28.9% -33.5% -34.6% -32.7%
Liver cirrhosis 61.5% 94.3% 124.3% 153.3% 182.1% 211.0% 225.5% 444.7% 685.5% 1337.2%
Atrial fibrillation and flutter 1.3% 2.6% 3.9% 5.3% 6.6% 8.0% 8.7% 18.9% 29.2% 53.7%
Hypertension 1.2% 2.4% 3.6% 4.8% 6.0% 7.1% 7.7% 16.1% 24.8% 45.2%
Ischemic heart disease -5.0% -5.0% -5.0% -5.0% -5.0% -5.0% -5.0% 4.0% 4.0% 15.0%
Ischemic stroke -10.0% -10.0% -10.0% -10.0% -10.0% -8.0% -8.0% 8.0% 8.0% 14.0%
Intracerebral hemorrhage -8.0% -8.0% -8.0% -8.0% -8.0% -1.0% -1.0% 25.0% 25.0% 67.0%
Subarachnoid haemorrhage 21.0% 21.0% 21.0% 21.0% 21.0% 11.0% 11.0% 39.0% 39.0% 82.0%
Epilepsy 3.1% 5.7% 8.3% 11.0% 13.8% 16.6% 18.0% 40.2% 64.5% 129.2%
Road injuries 1.9% 3.9% 5.9% 8.0% 10.1% 12.2% 13.3% 29.6% 46.8% 90.2%
Other unintentional injuries 1.6% 3.2% 4.8% 6.4% 8.1% 9.8% 10.6% 23.3% 36.5% 68.3%
Intentional injuries 5.1% 10.5% 16.1% 22.1% 28.3% 34.9% 38.3% 96.1% 171.2% 431.9%
Dark red > 50%; light red 20% to 50%; yellow 10% to < 20%; green < -10%
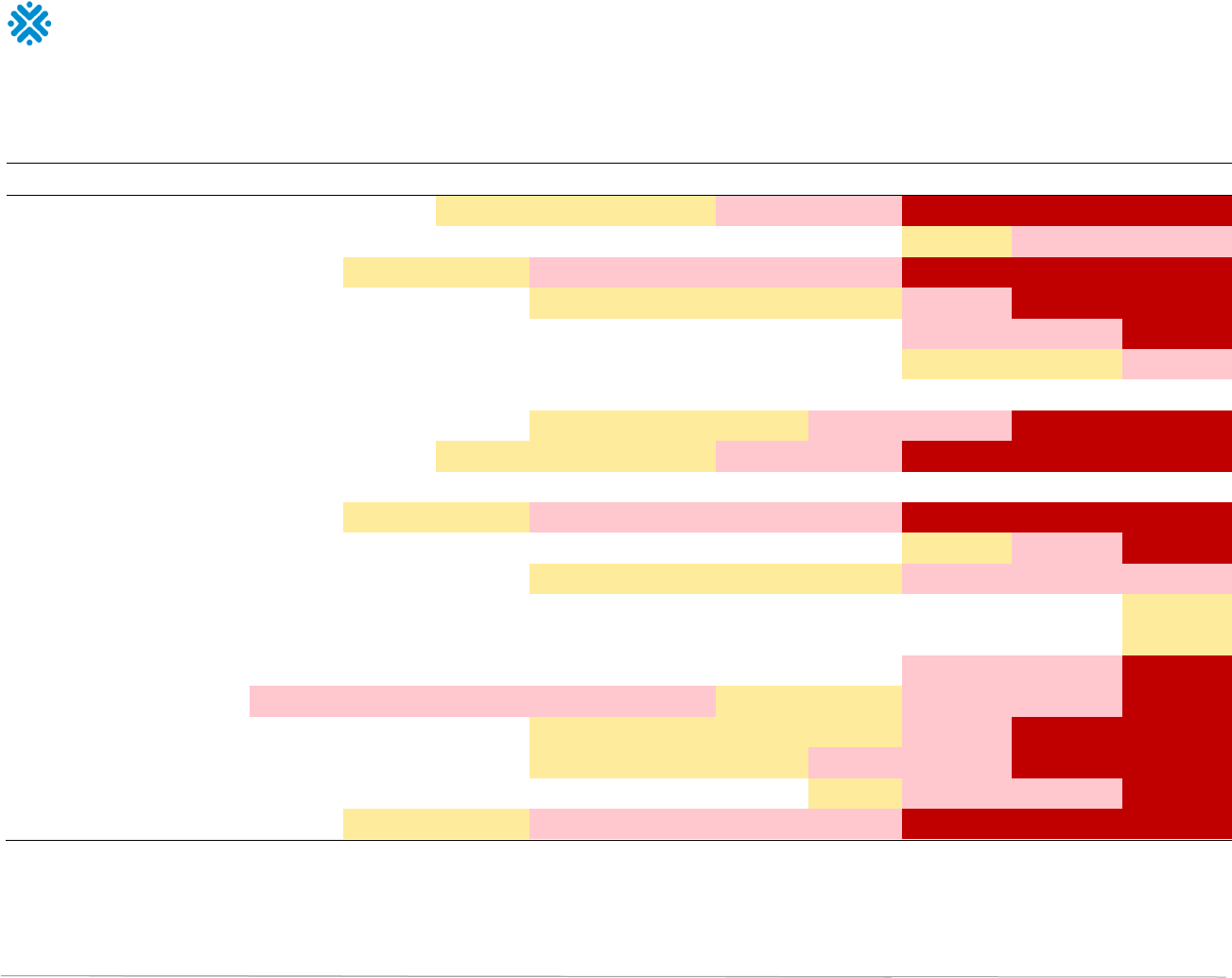
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 26
Table 2. Increased risk of diseases and injuries for males based on average weekly alcohol use (standard drinks per week)
Disease or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 3.7% 7.5% 11.4% 15.5% 19.7% 24.1% 26.3% 62.4% 105.2% 233.3%
Lower respiratory infections 1.0% 1.9% 2.9% 3.9% 4.9% 5.9% 6.4% 13.7% 21.0% 37.6%
Oral cavity and pharynx cancer 5.1% 10.3% 15.8% 21.6% 27.6% 33.8% 37.0% 89.4% 152.3% 338.4%
Oesophagus cancer 2.7% 5.4% 8.2% 11.1% 14.1% 17.2% 18.7% 42.7% 69.1% 139.3%
Colorectal cancer 1.4% 2.7% 4.1% 5.6% 7.0% 8.5% 9.2% 20.0% 31.1% 57.4%
Liver cancer 0.8% 1.6% 2.4% 3.2% 4.0% 4.8% 5.2% 11.2% 17.0% 30.1%
Breast cancer 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Larynx cancer 3.0% 6.0% 9.1% 12.3% 15.5% 18.8% 20.5% 46.3% 73.8% 143.5%
Pancreatitis 3.5% 7.2% 11.0% 14.9% 18.9% 23.1% 25.3% 59.7% 100.1% 219.7%
Diabetes Mellitus 0.0% 0.0% 0.1% 0.1% 0.2% 0.2% 0.3% 1.1% 2.4% 5.9%
Liver cirrhosis 6.2% 12.4% 18.8% 25.6% 32.9% 40.5% 44.5% 113.6% 207.1% 553.0%
Atrial fibrillation and flutter 1.3% 2.6% 3.9% 5.3% 6.6% 8.0% 8.7% 18.9% 29.2% 53.7%
Hypertension 2.8% 5.7% 8.7% 11.8% 15.0% 16.6% 17.4% 29.3% 35.9% 47.2%
Ischemic heart disease -5.0% -5.0% -5.0% -5.0% -5.0% -5.0% -5.0% 4.0% 4.0% 15.0%
Ischemic stroke -8.0% -8.0% -8.0% -8.0% -8.0% -8.0% -8.0% 8.0% 8.0% 14.0%
Intracerebral hemorrhage -8.0% -8.0% -8.0% -8.0% -8.0% -1.0% -1.0% 25.0% 25.0% 67.0%
Subarachnoid haemorrhage 21.0% 21.0% 21.0% 21.0% 21.0% 11.0% 11.0% 39.0% 39.0% 82.0%
Epilepsy 3.1% 5.7% 8.3% 11.0% 13.8% 16.6% 18.0% 40.2% 64.5% 129.2%
Road injuries 3.0% 6.1% 9.2% 12.5% 15.9% 19.3% 21.1% 48.8% 80.2% 168.0%
Other unintentional injuries 1.6% 3.2% 4.8% 6.4% 8.1% 9.8% 10.6% 23.3% 36.5% 68.3%
Intentional injuries 5.1% 10.5% 16.1% 22.1% 28.3% 34.9% 38.3% 96.1% 171.2% 431.9%
Dark red > 50%; light red 20% to 50%; yellow 10% to < 20%; green < -10%
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 27
Table 3. Cause-specific lifetime number of years of life lost (YLLs) per 1,000 females based on average weekly alcohol use (standard drinks per week)
Disease or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 0.1 0.2 0.3 0.4 0.5 0.6 0.7 1.4 2.4 5.1
Lower respiratory infections 2.3 4.6 6.9 9.3 11.6 13.9 16.3 31.4 48.1 79.4
Oral cavity and pharynx cancer 1.1 2.3 3.5 4.7 6.0 7.4 8.8 19.3 33.6 71.6
Oesophagus cancer 0.9 1.8 2.7 3.6 4.6 5.5 6.6 13.6 22.5 43.5
Colorectal cancer 3.8 7.6 11.4 15.3 19.2 23.2 27.2 54.0 85.0 149.3
Liver cancer 0.5 1.1 1.6 2.2 2.7 3.3 3.9 7.6 11.7 19.8
Breast cancer 7.6 15.3 23.2 31.1 39.3 47.5 55.9 113.3 182.2 335.5
Larynx cancer 0.1 0.2 0.4 0.5 0.6 0.8 0.9 1.9 3.1 5.7
Pancreatitis -0.8 -1.5 -2.2 -2.8 -3.3 -3.7 -3.9 -2.9 2.6 24.3
Diabetes Mellitus -30.3 -39.5 -45.5 -49.8 -53.2 -55.9 -58.0 -64.9 -66.0 -59.3
Liver cirrhosis 24.1 37.0 48.8 60.1 71.3 82.6 93.9 172.7 272.0 515.3
Atrial fibrillation and flutter 1.3 2.6 3.9 5.2 6.5 7.8 9.1 17.7 27.4 45.6
Hypertension 1.4 2.8 4.2 5.7 7.1 8.4 9.7 18.4 28.3 47.6
Ischemic heart disease -39.4 -39.3 -39.3 -39.2 -39.1 -39.0 -38.9 30.3 29.7 104.8
Ischemic stroke -7.7 -7.7 -7.7 -7.7 -7.7 -6.1 -6.1 5.9 5.8 9.5
Intracerebral hemorrhage -8.5 -8.5 -8.5 -8.5 -8.4 -1.1 -1.1 25.8 25.3 64.6
Subarachnoid haemorrhage 7.6 7.6 7.6 7.6 7.6 4.0 4.0 14.0 13.9 28.4
Epilepsy 0.3 0.6 0.9 1.1 1.4 1.7 2.0 4.1 6.8 13.1
Road injuries 1.3 2.7 4.1 5.5
6.9 8.3 9.8 20.1 32.7 61.8
Other unintentional injuries 3.9 7.8 11.8 15.8 19.8 23.9 28.1 55.4 87.2 151.5
Intentional injuries 6.2 12.8 19.7 26.9 34.5 42.5 50.8 116.7 215.7 536.0
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 28
Table 4. Cause-specific lifetime number of years of life lost (YLLs) per 1,000 males based on average weekly alcohol use (standard drinks per week)
Disease or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 0.1 0.2 0.3 0.4 0.5 0.7 0.8 1.7 2.9 6.0
Lower respiratory infections 2.1 4.1 6.1 8.1 10.2 12.2 14.3 27.6 42.3 69.6
Oral cavity and pharynx cancer 1.8 3.7 5.6 7.7 9.8 12.0 14.3 31.2 54.5 115.2
Oesophagus cancer 2.4 4.8 7.3 9.9 12.5 15.1 17.9 37.2 61.3 117.6
Colorectal cancer 3.6 7.2 10.8 14.5 18.3 22.0 25.9 51.3 80.7 140.8
Liver cancer 1.0 2.0 2.9 3.9 4.9 5.9 6.9 13.5 20.9 35.2
Breast cancer 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Larynx cancer 0.5 1.0 1.5 2.0 2.6 3.1 3.6 7.5 12.1 22.2
Pancreatitis 0.5 0.9 1.4 1.9 2.4 2.9 3.5 7.5 12.8 26.8
Diabetes Mellitus 0.0 0.1 0.1 0.2 0.4 0.5 0.7 2.5 5.4 12.6
Liver cirrhosis 4.1 8.1 12.4 16.8 21.6 26.5 31.8 73.7 138.7 356.6
Atrial fibrillation and flutter 0.8 1.7 2.5 3.4 4.2 5.1 6.0 11.6 17.9 29.8
Hypertension 2.6 5.3 8.1 10.9 13.8 15.2 16.7 26.2 31.9 39.4
Ischemic heart disease -64.4 -64.3 -64.1 -64.0 -63.9 -63.8 -63.7 49.9 49.0 174.0
Ischemic stroke -5.8 -5.8 -5.8 -5.8 -5.7 -5.7 -5.7 5.6 5.5 9.0
Intracerebral hemorrhage -7.7 -7.7 -7.6 -7.6 -7.6 -1.0 -0.9 23.2 22.8 57.8
Subarachnoid haemorrhage 4.4 4.4 4.4 4.4 4.4 2.3 2.3 8.1 8.0 16.4
Epilepsy 0.3 0.5 0.8 1.1 1.3 1.6 1.9 3.8 6.3 12.2
Road injuries 3.2 6.4 9.8 13.3 16.8 20.5 24.3
51.5 87.1 178.8
Other unintentional injuries 4.5 9.1 13.7 18.3 23.1 27.8 32.7 65.0 102.9 181.5
Intentional injuries 10.8 22.1 34.0 46.5 59.7 73.5 88.0 201.7 372.4 921.4
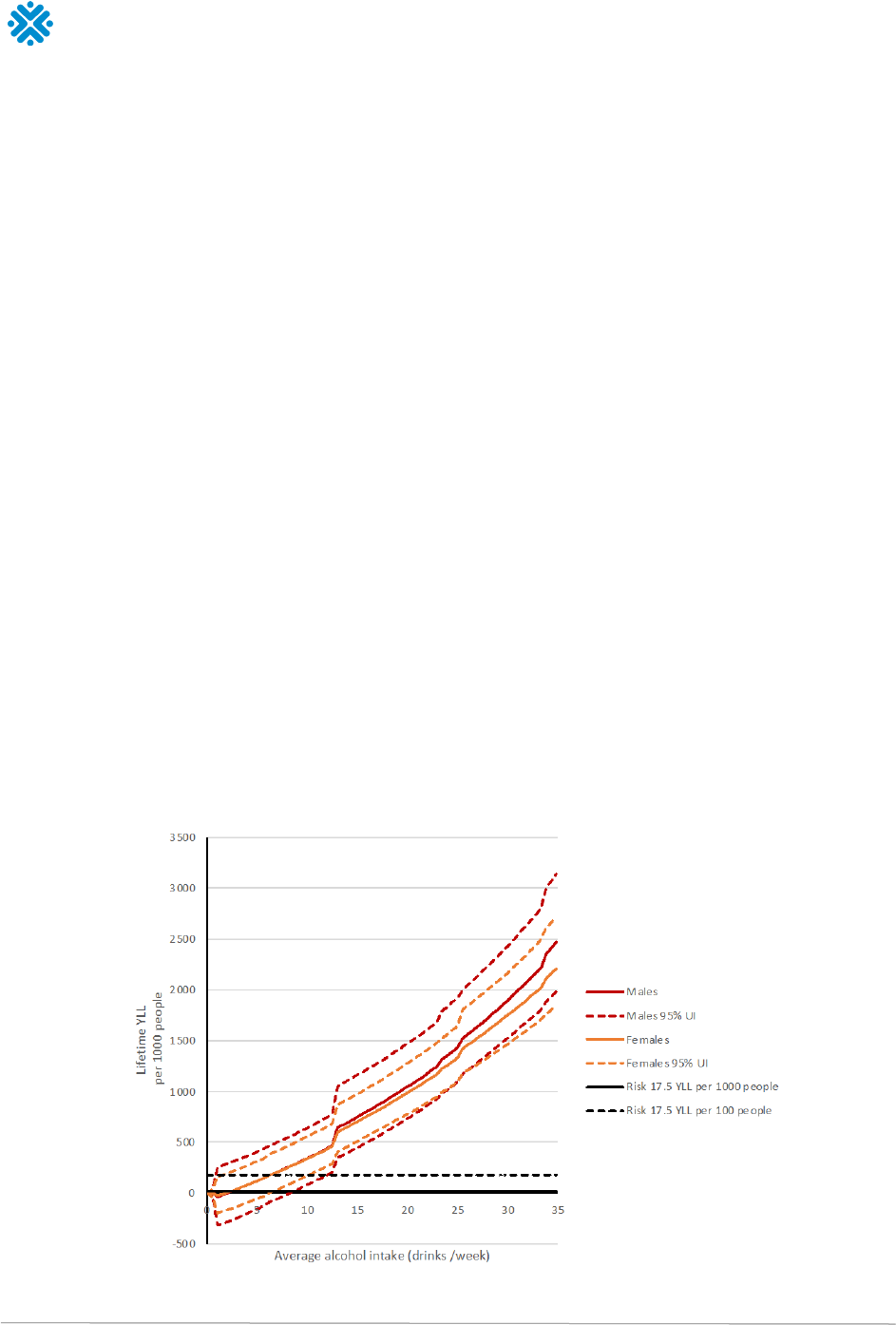
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 29
Lifetime Risk of Alcohol-Attributable Disability-Adjusted Years of
Life Lost by Sex
YLLs were used to model the alcohol-attributable burden of disease as it accounts for the age at
which a death occurs. The acceptable risk threshold for a lifetime death can also be stated based on
the average YLLs per death, which is 17.5 YLLs (Institute for Health Metrics and Evaluation, 2021).
Figure 3 presents lifetime risk of a YLL because of alcohol use, for both males and females, for
average levels of alcohol intake varying from one to 35 standard drinks per week. All models of
alcohol-attributable harms used grams of alcohol per day. In Canada, where a standard drink is
13.45 grams of pure alcohol, this corresponds to consuming zero to three (2.97) standard drinks per
day in an average week.
The modelling reveals that the number of YLLs increases as alcohol use increases among both
males and females. Among males and females, a protective association was observed for those
consuming one drink per week when compared to people who engaged in lifetime abstention. In all
cases, the 95% uncertainty intervals (UIs) crossed the null hypothesis threshold, which means there
is not enough evidence to confirm the protective effect.
The risk threshold based on one in 1,000 deaths (17.5 YLLs in 1,000 lifetimes) would be:
• 2 (95% UI: <1, 6) standard drinks/week for females
• 2 (95% UI: <1, 8) standard drinks/week for males
The risk threshold based on one in 100 deaths (17.5 YLLs in 100 lifetimes) would be:
• 6 (95% UI: <1, 10) standard drinks/week for females
• 6 (95% UI: <1, 11) standard drinks/week for males
Figure 3. Lifetime risk of a year of life lost (YLL) attributable to alcohol use at varying levels of average alcohol intake
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 30
Based on the systematic review of the published literature on the risk relationships between alcohol
use and disease and injury occurrence, this study estimated that for people in Canada,
the lifetime
risk of death and disability attributable to alcohol use increases as the amount of alcohol use
increases. The selected model did not demonstrate a significant negative nor protective net effect at
lower levels of alcohol use; that is, we did not observe a J-shape curve. This is likely due to more
recent and higher quality meta-analyses on the association between average alcohol use, ischemic
stroke and ischemic heart disease. (See box entitled “What Evidence Has Changed Since the
Release of the 2011 LRDGs?” for more details.) Therefore, alcohol should not be promoted or used
as a product to improve health.
As the lifetime risk of mortality and morbidity is similar for males and females, one guideline for
alcohol consumption can be used for Canada. According to established definitions of acceptable
risks and based on the risk thresholds of 17.5 YLLs attributable to alcohol per 1,000 and 100
lifetimes,
risk thresholds for alcohol use should be set at either two or six standard drinks per week
respectively, for both females and males in Canada.
Canada’s 2011 LRDGs Pose Higher Risks in Light of Current Evidence
To reduce the risk of long-term harm, Canada’s 2011 LRDGs recommended consuming no more
than 15 drinks a week among males (~29 grams/day) and 10 drinks a week for females (~19
grams/day). Based on today’s data sources and the life course approach to estimate the risk of an
alcohol-attributable death, the 2011 recommendations would be associated with the following risk
thresholds:
• Consumption by males of 29 grams/day would result in
757 YLLs per 1,000 lifetimes
• Consumption by females of 19 grams/day would result in
336 YLLs per 1,000 lifetimes
Put differently, the 2011 LRDGs would be associated with a risk for males that is between 76 and
757 higher than established definitions of acceptable risk, and with a risk for females that would
be between 34 and 336 higher than those definitions.
2.3 Alcohol Use Per Occasion
The risks from alcohol use for most health outcomes (e.g., death, certain cancers, heart disease,
injuries) are usually based on how much alcohol is consumed on average or the total amount
consumed over the past week or month (see tables 1 and 2). That is why the mathematical
modelling led to results expressed in an average number of standard drinks per week, that is, 2 or
less, between 3 and 6, or more than 6 standard drinks per week, depending on which level of risk is
considered.
However, most people do not drink their average amount every day. On days they use alcohol there
is considerable variability in how much they use on different drinking “occasions.” For this reason,
many people who drink relatively low weekly or monthly amounts of alcohol may in fact drink large
quantities on a single occasion, which may put them at risk for harm (Naimi et al., 2003). In the
context of personal well-being, the experts discussed the latest evidence on alcohol use per drinking
occasion to be able to advise people in Canada on this issue.
With alcohol use during any drinking occasion, each drink increases one’s blood alcohol concentration
(BAC). An increased BAC is what leads to alcohol impairment (a reduced ability to think clearly or
perform certain activities) and intoxication (which is the appearance or sensation of being drunk). The

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 31
risk begins to increase with any use of alcohol, and with more than two standard drinks, most
individuals will have a demonstrably increased risk of “acute” problems. For example, compared to no
alcohol use, studies of injuries in emergency departments show increasing risk for each drink
consumed for both men and women (Cherpitel et al., 2015; Vinson et al., 2003) Similarly, studies of
motor vehicle crash fatalities demonstrate increasing risk above a BAC of 0.02% (Blomberg et al.,
2009; Compton & Berning, 2015; Voas et al., 2012), which corresponds to about one drink. After
about two standard drinks consumed within an hour, one’s BACs may be approximately 0.05% (the
level will differ on the basis of body mass and other factors). Above this level, risk gets progressively
and substantially higher the more one drinks on any occasion and the higher one’s BAC. It is important
to recognize that people typically exhibit behaviour changes or become impaired starting at BAC levels
below those at which they feel “drunk” or appear intoxicated (Midanik, 1999).
Binge drinking, usually defined as consuming five standard drinks or more for men or four standard
drinks or more for women in one setting (National Institute of Alcohol Abuse & Alcoholism, 2004;
Wechsler & Austin, 1998) is a common yet dangerous pattern of consumption that results in legal
impairment (i.e., a BAC > 0.08%) for most persons, and is significantly associated with a range of
alcohol-related health and social problems (Centers for Disease Control and Prevention; Fillmore &
Jude, 2011).
4
Specifically, binge drinking and resulting BAC levels are well-established risk factors for
death from any cause, including unintentional injuries (road crashes, drownings, falls), physical and
sexual violence, cardiovascular disease (hypertension, myocardial infarction, stroke), inflammation of
the gastrointestinal system (gastritis, acute pancreatitis), and the development of an alcohol use
disorder (Alpert et al., 2022; Brewer & Swahn, 2005; Dawson et al., 2005; Devries et al., 2014; Dietary
Guidelines Advisory Committee, 2020; Mukamal et al., 2005; Roerecke & Rehm, 2014).
Many of the complications arising from acute impairment and binge drinking involve second-hand
effects that affect someone other than the person who drinks (e.g., domestic violence, child abuse
and neglect). Because binge drinking is common and involves large volumes of alcohol consumption,
binge drinking occasions account for a substantial proportion of all alcohol consumed in the
population. Binge drinking is also an important contributor to long-term health problems like liver
disease and certain cancers (Llerena et al., 2015). For example, binge drinking increases risks of
breast cancer and proliferative benign breast disease, as increased blood alcohol levels exceed the
capacity to metabolize and eliminate alcohol. Not only are alcohol and its metabolites carcinogenic,
but consuming multiple drinks in one setting can increase inflammatory toxins, sex hormone levels
and mutagenic DNA, and induce the activity of additional enzymes that can result in the formation of
cancer cells (White et al., 2017). The mechanism may be especially risky for young females since
breast tissue is most susceptible to neoplastic transformation between menarche and first
pregnancy (Liu et al., 2015).
Fortunately, effective alcohol control policies can reduce rates of binge drinking and related
problems (Naimi et al., 2014; Wagenaar et al., 2009; Wagenaar et al., 2010). Although most
persons who engage in binge drinking do not meet criteria for an alcohol use disorder, virtually all
persons with an alcohol use disorder engage in binge drinking.
In sum, the evidence is clear and consistent: in terms of health, fewer standard drinks per drinking
occasion means less risk of harm to the person consuming the alcohol and reduced risk of second-hand
effects to those other than that person. Although some risk begins at one drink and increases more
4
Some scientists have questioned this criteria and suggested that a lowered standard defining impairment should be used for women
(Canadian Centre on Substance Abuse, 2014; Thomas et al., 2014).
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 32
substantially with more than two standard drinks, risks are higher and increase very rapidly at or above
binge drinking levels (five or more standard drinks for men, four or more standard drinks for women).
2.4 Rapid Reviews
At the beginning of this project, a public consultation was held to hear what alcohol, health and well-
being issues mattered most and were most useful to people living in Canada. (We will return to this
topic in section 2.6.) A key finding from the consultation was that from a list of eight topics, the one
respondent asked to be prioritized in the updated guidelines was the impact of drinking alcohol on
mental health. It was followed by the impact of drinking alcohol on physical health and how alcohol
can impact people’s lives via, for example, violence and sexual assaults.
Unfortunately, the updated evidence review on the effects of alcohol on health did not identify high
quality-evidence systematic reviews on alcohol use and mental health nor on alcohol use and social
harms. Not a single review met all the selection criteria. (See section 2.1 and
Update of Canada’s
Low-Risk Alcohol Drinking Guidelines: Evidence Review Technical Report.) This means that the
modelling presented in the previous section ignores the impact that alcohol may have on mental
health and violence and, therefore, on people’s overall risk of death and disability. To overcome this
blind spot, the experts agreed to commission two rapid reviews, one on the effects of alcohol on
violence and another one on the effects of alcohol on mental health.
2.4.1 Association Between Alcohol Use, Aggression and Violence
In the absence of recent high-quality systematic reviews or meta-analyses on alcohol and violence
and to inform experts opinion, an overview of recent reviews of the literature on alcohol and
aggression and violence (A/V) was commissioned.
Alcohol is associated with many health and social harms, including various forms of aggression and
violence. There are multiple factors affecting the relationship of alcohol and A/V, including the
effects of alcohol experienced by people who consume alcohol; their personalities, beliefs, attitudes
and other characteristics; the immediate drinking situation; and the culture within which the drinking
occurs (Choenni et al., 2017; Exum, 2006; Graham et al., 1997; Graham et al., 1998; Parrott &
Eckhardt, 2018).
Three common forms of A/V that have shown high rates of alcohol involvement and that experts
agreed to consider to update Canada’s 2011 LRDGs are intimate partner A/V (IPV), male-to-female
sexual A/V (SV), and non-intimate and non-sexual A/V between adults or general A/V (GV). The role
of alcohol in both A/V perpetration (being aggressive or violent toward another adult) and
victimization (having an act of aggression or violence done toward them) was considered.
5
Relevant
details about findings related to sex/gender differences are reported where available.
6
The full report,
Update of Canada's Low-Risk Alcohol Drinking Guidelines: Overview of Reviews of the
Association Between Alcohol Use and Aggression and Violence, including references, is available on
CCSA’s LRDG 2022 webpage. A summary of the report is presented in here.
5
In the context of this overview, “perpetrator” refers to the person who was aggressive or violent toward another person or persons.
“Perpetration” refers to the act of carrying out A/V. “Victim” refers to the person or persons to whom the aggressive or violent act was done
(commonly referred to in the literature as the victim, target or survivor); that is, the person who was victimized by the perpetrator.
“Victimization” refers to the process of being victimized. These terms are not meant to label those who experience violence. Use of terms
“victim” or “victimization” is by no means intended to assign blame, imply weakness or guilt, or otherwise stigmatize those who experience
A/V, nor is it meant to imply any particular response or impact of the A/V on the person.
6
We use the term “sex/gender” in this overview because, while some studies restricted their analyses to sex (biological attributes), both
alcohol consumption and A/V are inextricably linked to gender (socially constructed roles, norms, values and behaviours).
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 33
Method
A comprehensive search was performed of the literature published from the year 2000 to January
2022, including systematic reviews (i.e., meta-analyses and narrative literature reviews), using the
following databases: Medical Literature Analysis and Retrieval System Online (MEDLINE) and
Excerpta Medica Database (Embase) using the OVID platform, and PubMed, PsychINFO, PsychNET,
Web of Science, Criminal Justice Abstracts, Cochrane CENTRA and other reviews from our collection.
• The search resulted in 3,826 records.
• After removal of duplicates, 2,744 titles and abstracts were retrieved.
• After screening by two independent screeners, 54 reviews were included (30 IPV, 10 SV and 14
GV). Results are reported separately for IPV, SV and GV, and separately for perpetration and
victimization.
Key Findings
Alcohol and Intimate Partner Violence (IPV) Perpetration
Event-level alcohol consumption (i.e., having consumed alcohol at the time or prior to the A/V
incident) was associated with perpetration of IPV, but the strength of the relationship varied by
sample and the sex/gender of the perpetrator (larger for male than for female perpetrators). In terms
of usual drinking pattern (e.g., usual number of standard drinks consumed per occasion, frequency
of consumption over a specific time period, a regular pattern of drinking to intoxication), heavy
episodic drinking (or binge drinking) and drinking to intoxication were positively associated with IPV
perpetration, with weaker associations found for drinking frequency. As with event-level drinking, the
relationship between usual drinking pattern and IPV perpetration was stronger for men than for
women. Drinking problems and alcohol use disorders were positively associated with IPV
perpetration, with stronger relationships for male than for female perpetrators (although some
inconsistent findings were also reported). Some evidence suggested that alcohol use was also
associated with more severe IPV perpetration.
Alcohol and IPV Victimization
Event-level drinking was associated with greater risk of being the victim of IPV. Findings were
inconsistent relating to drinking pattern of the victim, but generally suggested that IPV victimization
was associated with a pattern of heavy episodic drinking and intoxication, as well as drinking
problems and alcohol use disorders. However, estimates of associations were usually smaller than
were found for drinking by perpetrators, and some estimates were non-significant.
Alcohol and Male-to-Female Sexual Violence (SV) Perpetration
Small-to-medium effect sizes were found for the relationship between event-level alcohol
consumption and male-to-female SV perpetration, although some experimental paradigms did not
produce a significant effect of alcohol on SV. As well, moderating factors such as personality and
attitudes were noted in the relationship. Associations were found between perpetration of SV and
both drinking patterns and drinking problems, particularly for heavy episodic drinking. However, not
all studies found significant associations, especially when key variables such as past perpetration
were controlled.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 34
Alcohol and Male-to-Female SV Victimization
Consuming higher amounts of alcohol prior to SV was associated with greater severity of SV
experienced by victims in some, but not all studies. This finding may relate to heavier drinking by the
perpetrator because drinking by perpetrators and victims is highly correlated. Although there is
relatively little research, some evidence suggested that women who engaged in a pattern of heavy
episodic drinking, drinking to intoxication or problem drinking were more likely to be victims of SV.
Alcohol and General Violence (GV) Perpetration
Experimental, laboratory-based and other research indicates that alcohol increases aggressive
behaviour (medium effect sizes), with variability related to how aggression was measured in the
laboratory and sex/gender of aggressors. The research also identified important moderators of the
association. Research suggests positive associations between GV perpetration by individuals and
heavier drinking patterns as well as drinking problems. However, the evidence is less clear for usual
quantity consumed per occasion (i.e., average number of drinks usually consumed) by individuals
and frequency of drinking than for alcohol in the event (i.e., consumption during or prior to an A/V
event), and the reviews in this area have methodological weaknesses.
Alcohol and GV Victimization
A large proportion of homicide victims tested positive for alcohol (larger for women than men), and
many were defined as intoxicated (BAC > 0.08 or 0.10), although these studies found large
variability in estimates. Homicide rate was found to be positively correlated with per capita
consumption in some countries but not others. Emergency department studies indicated that
patients with violence-related injuries were significantly more likely to have consumed alcohol than
were patients with non-violence-related injuries, with some evidence suggesting the relationship was
stronger for men than for women. There were insufficient data on drinking patterns of GV victims to
draw conclusions about the relationship between alcohol consumption and being the victim of GV.
Discussion
Although the exact mechanisms by which alcohol is associated with A/V are unknown, there is
overwhelming evidence that alcohol consumption, especially intoxication, is associated with
perpetration of A/V, and some evidence indicates that alcohol may increase the severity of A/V.
However, there are insufficient data to define the exact dose–response relationship. Thus, although
existing research does not allow the calculation of a risk curve for alcohol and A/V
, it is reasonable to
infer that individuals can reduce their risk of perpetrating A/V by limiting their alcohol consumption.
Based on consistent evidence, it is highly likely that avoiding drinking to intoxication will reduce
individuals’ risk of perpetrating alcohol-related violence. Therefore, efforts to reduce or eliminate
alcohol-related A/V need to focus on reducing alcohol use, especially among those who may be likely
to perpetrate A/V or get involved in violent incidents. Because A/V decreases with age and is
perpetrated more by men than women, prevention efforts should focus on young adults, particularly
young men. Overall, people should be encouraged to avoid drinking high levels of alcohol or avoid
drinking altogether to reduce their risk of perpetrating violence. Persons who have a history of
alcohol-related violence should avoid any consumption of alcohol.
The literature on the association between alcohol and A/V victimization is less clear. The findings
suggest there is likely an association, but there are some mixed and null findings, and noteworthy
limitations of this literature. Alcohol’s role in victimization likely reflects many different mechanisms
that may work in combination, such as alcohol intoxication reducing the ability to avoid or escape
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 35
danger, use of alcohol by victims due to trauma, increased exposure to risk in drinking settings,
targeting by perpetrators of people who are intoxicated, and use of substances to control victims.
Attributing A/V victimization to alcohol contributes to beliefs that victims of A/V who had used
alcohol are responsible or blameworthy for being victimized. Moreover, evidence suggests that
interventions that place the burden to avoid risk of victimization on women and girls are ineffective.
While alcohol might be a contributing factor in A/V victimization, we state unequivocally that drinking
alcohol does not make a person responsible for A/V perpetrated on them. Thus, we conclude that
lower risk drinking guidelines should focus on reducing alcohol use by potential perpetrators.
2.4.2 Association Between Alcohol Use and Mental Health
In 2016, when Australia’s National Health and Medical Research Council was asked to revisit their
2009 alcohol guidelines, their systematic review on the health effects of alcohol consumption
revealed there was actually very little synthesized evidence on how different levels of alcohol
consumption influence mental health (National Health and Medical Research Council, 2020).
Because this question was of interest for drafting updated alcohol guideline recommendations, the
Adelaide Health Technology Assessment, University of Adelaide, was contracted to conduct a
systematic literature review on the latest and best scientific evidence on the mental health risks and
benefits of alcohol consumption (Newton et al., 2018). The Newton et al. systematic review, plus six
new systematic reviews on the association between alcohol consumption and mental health and
substance use disorders were evaluated for the current project (see
Update of Canada’s Low-Risk
Alcohol Drinking Guidelines: Evidence Review Technical Report). None of the reviews met the criteria
for inclusion.
Given the previously mentioned importance that people living in Canada associated with the
relationship between alcohol and mental health, the experts decided to commission Cochrane
Canada, McMaster University, to conduct a rapid update of a systematic review of the effect of
alcohol consumption on the development of depression, anxiety and suicidal ideation. The full report,
Effect of Alcohol Consumption on the Development of Depression, Anxiety and Suicidal Ideation:
Update of a Systematic Review, is available on CCSA’s LRDG 2022 webpage.
Limitations of the Rapid Update and Experts’ Decision
With this rapid update, the intention was to be able to pool together results across studies using
statistical analyses. Unfortunately, as with the 2018 review prepared by Newton et al., thresholds
and definitions for alcohol quantity or frequency varied across studies and so a statistical analysis
could not be performed. In addition, studies often failed to report odds ratios with standard errors or
confidence intervals so results could not be easily pooled. The review also found that many studies
did not report results that could be easily interpreted and even the most recently published studies
provided little data that could be used to make healthcare decisions. Experts highlighted that just as
was the case for many studies on the relationship between alcohol and physical health, many
studies on alcohol and mental health misclassified abstainers. Specifically, to assess the impact of
alcohol on mental health, the reference group against which those who use alcohol were compared
were people who do not consume alcohol, including people who quit using alcohol because of health
problems, such as mental health issues.
For these reasons, the experts agreed that further work would be required for mental health
outcomes to be considered when making alcohol guidelines recommendations. The experts were
unanimous in opting to make the rapid review publicly available but agreed that it would not inform
their final discussions on formulating and presenting updated guidelines.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 36
2.5 Women’s Health and Alcohol
The mathematical modelling revealed identical risk thresholds for females and males at low levels of
alcohol consumption. This was not unexpected. When the U.K. and Australia updated their alcohol
guidelines, both made identical recommendations for men and women. Since 2017, France also
recommends the same alcohol limits for both sexes and when Denmark released its new alcohol
guidelines in spring 2022, they recommended the same alcohol limits for adult women and men
alike, and no alcohol consumption for those under 18 years old.
The results obtained by our modelling align with the global trend to not differentiate between
females and males when formulating alcohol guidelines. This conclusion is because at low levels of
consumption the physiological differences between women and men have only a small impact on
lifetime risk of death. However, above low risk, lifetime risk increases more steeply for women than
for men.
The experts are mindful of the complexity of this reality and the necessity to describe it well. Proper
understanding of sex-related and gender-related factors on women’s health and reproductive issues
is key to reach and inform audiences in a meaningful way. Updated alcohol guidelines need to be
shared with the appropriate nuances. To this end, a comprehensive multi-part review of the recent
literature on sex, gender, alcohol and health was commissioned.
The full report prepared by Galvanizing Equity, including references, is available here:
Sex, Gender
and Alcohol: What Matters for Women in Low-Risk Drinking Guidelines? and was recently published
(Greaves et al., 2022). A short version is presented below. This section concludes with evidence-
based key messages that health professionals and policy makers may want to consider in their
programs, practices and communications about alcohol.
2.5.1 What Are Some Sex-Related Factors?
The four main categories of sex-related biological factors that are important to understanding how
alcohol affects male and female bodies are hormones and enzymes, physiology and anatomy,
genetics, and neurobiology. Within these categories, various sex-related differences, factors or
processes exist. The absorption, distribution and metabolism of alcohol is affected by sex-related
factors. For example, females absorb ethanol faster than males, and reach a higher BAC due to
faster absorption and slower elimination. Significantly, females generally experience more risk of
damage or disease, such as liver disease, at lower levels of alcohol consumption than do males. In
general, males are more likely to develop alcohol use disorders, but females are more likely to
develop organ and other bodily damage from drinking alcohol.
2.5.2 What Are Some Gender-Related Factors?
There are different impacts on women or men or gender and sexual minorities as a result of alcohol
consumption. The four main aspects of gender that account for these impacts are gender roles and
norms, gender relations, gender identity and institutionalized gender. Gender identity matters in that
the strength of adherence to masculinities or femininities affects style and volume of drinking
behaviour, with men and sexual and gender minorities often drinking larger quantities of alcohol and
more often than women as a group. Gendered relations often mean that women are influenced by a
partner’s drinking and the impacts of alcohol reflect gender inequities such as vulnerability to sexual
assault and violence. Gender roles lead to women using alcohol to cope with stresses of caregiving
roles, trauma and IPV. Institutionalized gender differentially impacts women by applying increased
stigma to women who drink, and barriers to treatment for women and mothers who use alcohol.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 37
2.5.3 How Do Sex and Gender Interact and Intersect with Other
Factors?
All these factors and processes are exacerbated by sex–gender interactions. For example, sex-
related and gender-related factors coincide to create specific and heightened negative impacts of
alcohol during pregnancy on both women’s and fetal health. Pregnancy-related processes affect the
pharmacokinetics of ingesting alcohol, while stigma and social policing are heightened during
pregnancy. Vulnerability to sexual assault is enhanced by being young, female and intoxicated, amid
pervasive gender-based violence. Intersections, such as those with poverty, racialization, past
trauma, or sexual and gender minority status merge to create more harms.
2.5.4 How Does Alcohol Affect Reproduction?
Reproductive health is compromised by alcohol use, particularly during pregnancy and
breastfeeding. Long-term damage to children can occur after being exposed to alcohol in the womb,
and alcohol use during breastfeeding can reduce milk production. Furthermore, alcohol passes into
breastmilk and therefore exposes the infant to alcohol. During pregnancy, increased water and blood
volume, along with the impact of alcohol on glucose and insulin lipid metabolism, create complex
effects on the body.
There is mixed evidence on the impact of alcohol on pregnancy and delivery outcomes, with possible
increases in miscarriage and placental abnormalities. However, exposure to alcohol in the womb
results in a well-established risk for learning, health and social effects with lifelong impacts on the
fetus as well as brain injury, birth defects, behavioural problems, learning disabilities and other
health problems typically referred to as fetal alcohol spectrum disorder (FASD). Recent reviews that
considered
low levels of exposure have also found some adverse effects, reinforcing the message
that it is safest not to drink during pregnancy. Effects of alcohol consumption on breastfeeding
include a decrease in milk production, early cessation of breastfeeding and effects on infant sleep
patterns.
2.5.5 Discussion
Women are particularly susceptible to the negative effects of drinking alcohol. This is due to factors
related to both sex (biological) and gender (social). The female body’s response to alcohol results in
faster intoxication and more damage from lesser amounts of alcohol, and in a shorter time.
Gendered social and cultural factors about alcohol negatively affect girls and women via enhanced
stigma, social pressures, exploitative marketing and increased vulnerability to sexual assault and
IPV. Sex and gender, along with the determinants of health and intersecting factors, such as race,
age, income and education, shape the overall impacts of alcohol, resulting in differential impacts on
women, men and gender and sexual minorities. While all people living in Canada can benefit from
nuanced information and messaging about alcohol use and safe drinking levels, it is especially
important for women and girls.
Alcohol use also presents numerous sex- and gender-specific risks for reproductive processes such
as fertility and conception, pregnancy, breastfeeding and childcare. Males and females experience
differential alcohol-related reproductive risks and effects, at different life stages. Alcohol use during
pregnancy is particularly unsafe, as it heightens the risk of FASD in offspring, often with lifelong
disabilities and impacts. Gendered social attitudes about alcohol use and reproduction mean that
those who use alcohol during pregnancy experience negative, punitive and stigmatizing attitudes. In
some jurisdictions, these manifest as state sanctioned interventions, barriers to treatment or child
apprehension.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 38
2.5.6 What Are the Key Messages for Women?
The collective impact of sex, gender and interactive and intersectional factors on alcohol use has
particular importance for girls and women. It is necessary to transmit this emerging and growing
body of evidence to women, service providers, practitioners and policy makers to improve health
literacy and inform more specific and tailored prevention, treatment and harm reduction efforts.
• Female bodies can be more damaged by drinking, compared to males.
• Sex-related (biological) factors enhance the impact of alcohol, causing more harm and faster
intoxication in girls and women from lesser amounts.
• Gender-related (social) factors contribute to the negative impacts of alcohol in real life,
increasing vulnerability to marketing exploitation, stigma, sexual assault and IPV.
• Sex, gender and factors such as trauma and poverty interact and make dependence on alcohol,
treatment and recovery more difficult for women.
• Practitioners need to recognize both biological and social factors affecting alcohol use that
create differential impacts on and require tailored responses for women, men and gender and
sexual minorities.
2.6 Views, Preferences and Expectations About Guidelines
of People Living in Canada
Throughout this project, there was a commitment to consider the views, preferences and
expectations of people living in Canada about alcohol guidelines to improve the strength of updated
recommendations. Therefore, as evidence was being gathered on alcohol and health, parallel
activities were undertaken to better understand people’s views about guidelines and to obtain
insight on alcohol, health and issues of well-being that matter most and are most useful to people
living in Canada.
Three different types of evidence were collected to inform experts’ deliberations and final decisions
for the updated guidelines: an update of a systematic review, a public consultation and interviews
with stakeholders.
2.6.1 Summary of Evidence on Understanding and Response to Alcohol
Guidelines
To learn about the acceptability and feasibility of the updated guidelines, the systematic review
previously prepared for the behavioural evidence expert group for the U.K. guidelines (Jones & Bellis,
2013) was updated with a focus on understandings and responses to official public health
guidelines. The update was prepared by Cochrane Canada. (See the full report:
Update of Canada’s
Low-Risk Alcohol Drinking Guidelines: Summary of Evidence on Understanding and Response to
Alcohol Consumption Guidelines.) Some of the results have proven to be of great importance to the
experts charged with making judgments about the acceptability and feasibility of recommendations.
• There appears to be little understanding among the public about what a standard drink is, and
most times people overestimated the standard drink size. The public also overestimated the
number of daily and weekly standard drinks recommended in guidelines. Typically, people indicated
that those recommendations were unrealistic and did not want to count standard drinks.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 39
• Views about the amount of alcohol consumption that was not sensible or that was harmful were
often associated with excessive intake or “problem drinking,” but people often noted that their
own drinking was not a problem.
• Less than half the people who responded to surveys were aware of the harms of alcohol intake,
and there was less awareness in people who drink at high- or very high-risk levels. While some
people were aware of the harms, they still had a positive attitude toward alcohol use, especially
in social situations.
• People suggested that guidelines should include strategies to help apply the low-risk drinking
recommendations, such as refusing drinks when not really wanted or eating while drinking.
• The applicability to their own lives of guidelines generally and guidelines specifically for low-risk
drinking was questioned by the public with many reasons given for why guidelines might not be
applicable. For example, individual tolerance levels and physical reactions to alcohol can differ,
and the effects of different types of alcohol on an individual can also differ.
• While participants in the studies indicated that a health agency should provide
recommendations, they preferred advice rather than strict rules or patronizing messages.
• Overall, the experts considered these findings to indicate that regardless of the scientific quality
of the guidelines, to be credible updated guidelines must meet people where they are at. They
would have to bridge the gap between the way people consume alcohol and the evidence on the
health impacts by providing them with actionable guidance.
2.6.2 Public Consultation on Alcohol Guidelines
In spring 2021, CCSA held an online public consultation in which 4,845 people living in Canada
participated. (See the full report:
Update of Canada’s Low-Risk Alcohol Drinking Guidelines:
Summary of Findings from Public Consultation.) The consultation focused on the experiences of
people living in Canada with the current LRDGs and their needs and expectations for updated
guidelines. The public consultation revealed alcohol-related topics of importance to people living in
Canada that, in return, influenced the topics for which it was decided to conduct rapid reviews (see
Section 2.4). The experts also retained two major lessons in terms of the type of information to be
emphasized and prioritized in the development of resources to promote the new guidelines:
• Among contributors who said they had used the 2011 LRDGs in the past, the most often cited
challenge with using the guidelines was “not wanting to follow the LRDGs.”
• The contributors shared an interest in understanding their risk of experiencing alcohol-related
harms and receiving information about long-term risks and benefits of alcohol use.
Both these results point to the importance of not only informing people about the existence of the
guidelines, but also about the reasons for their existence. Without fully understanding the risks
associated with alcohol use, people are unlikely to understand why they should follow the guidelines.
2.6.3 Interviews with Stakeholders
To explore the familiarity and understanding of the 2011 LRDGs, and to discuss specific knowledge
mobilization recommendations including ideal messaging and communication strategies, Leger was
contracted to assist in the completion of eight virtual focus groups. A total of 48 persons representing
various health-related organizations were interviewed. The summary report,
Commissioned Report:
Update on Canada’s Low-Risk Alcohol Drinking Guidelines: Summary of Stakeholder Focus Groups,
is available on CCSA’s LRDG webpage.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 40
Overall, stakeholders were familiar with the LRDGs. They mentioned frequently referencing the
guidelines, which they found to be particularly useful to start a conversation about alcohol use and
drinking patterns. Still, they mentioned that encouraging people to follow alcohol guidelines was
challenging because awareness of the dangers of alcohol was low and people living in Canada
tended to normalize consuming alcohol.
Stakeholders mentioned that the goal of the updated guidelines should be to get people rethinking
their alcohol consumption. They requested a focus on the adverse effects of alcohol on overall
health and wellness, including information on alcohol being a known teratogen and carcinogen, and
its association with mental health and social harms. Messaging for teens and young adults should
focus on the immediate short-term impacts of drinking. Finally, many participants mentioned the
importance for updated guidelines to challenge the alcohol-centred culture and to include messaging
promoting a non-drinking culture. Participants also mentioned keeping the guidelines as simple as
possible and providing standard drink measurements that are easy to follow as the ideal approach to
conveying the guidelines.
In terms of resources, stakeholders said they wanted a variety of different types of information. They
also viewed infographics as important for communicating the updated guidelines. The guidelines
should be kept as simple as possible, and providing standard drink measurements that are easy to
follow is viewed as the ideal approach to conveying them. In fact, the interviews further revealed a
firm belief among stakeholders that the public should be provided with information about standard
drink size, nutritional information and potential health risks related to consuming alcohol. Hence,
they expressed support for the addition of mandatory enhanced alcohol container labels with a
health message, drink guidelines, standard drink information and nutrition information.
Standard Drink Labelling: A Necessary Condition for the Adoption of the Guidance
on Alcohol and Health by the Public
The concept of standard drink is central to understanding the Guidelines on Alcohol and Health.
To adhere to the guidance and reduce the risk of negative consequences due to alcohol,
consumers need consistent, easy-to-use information when serving alcohol to accurately track and
monitor their drinking.
In Canada, a standard drink is 17.05 ml or 13.45 grams of pure alcohol, which is equivalent to:
• A bottle of beer (12 oz., 341 ml, 5% alcohol)
• A bottle of cider (12 oz., 341 ml, 5% alcohol)
• A glass of wine (5 oz., 142 ml, 12% alcohol)
• A shot glass of spirits (1.5 oz., 43 ml, 40% alcohol)
In practice, people in Canada have a limited understanding of a standard drink (Osiowy et al.,
2015; Public Health Ontario, 2017b). According to this project’s public consultation (Update of
Canada’s Low-Risk Alcohol Drinking Guidelines: Summary of Findings from Public Consultation),
38% of contributors said they had previously heard of the 2011 LRDGs. Among those who
reported using the guidelines, less than half (43%) said they were extremely familiar with the
concept of standard drink. When asked about challenges associated with using the 2011 LRDGs,
two of the three most popular answers were that it was not clear to them “what a standard drink
is” and that the standard drinks in the guidelines did not represent the types of alcoholic
beverages they typically drink. These results echo those of other studies showing that a lack of
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 41
knowledge about standard drinks can preclude people from adhering to guidelines, even if they
are aware of them and motivated to monitor and regulate their alcohol consumption (de Visser &
Birch, 2012; Dowling et al., 2006; Hawks, 1999).
Percent alcohol by volume (%ABV) information is mandated on alcohol beverage containers in
Canada. However, communicating alcohol content on beverage containers using %ABV
information is problematic because alcohol drinking guidelines are expressed in terms of standard
drinks. The inconsistency in messaging causes consumer confusion and creates barriers for
consumers to adhere to alcohol guidance. Standard drink labelling (SDL) can help consumers to
accurately monitor their alcohol use in terms of standard drinks (Osiowy et al., 2015; Wettlaufer,
2018). According to a 2022 systematic review of the impacts of alcohol container labels on
consumer outcomes, the evidence consistently suggests that compared to %ABV labels, exposure
to SDL results in more accurate estimates of the amount of alcohol in a standard drink, the
number of standard drinks in an alcohol container, and the number of standard drinks to reach
drink limit guidelines (Hobin et al., 2022). Evidence also indicates that by providing information at
the point of pour, SDL better supports accurately pouring one standard drink of alcohol relative to
%ABV labels (Brunk et al., 2020; Wettlaufer, 2018). In the only real-world experimental study
testing alcohol container labels, results suggest when consumers are exposed to SDL, they are
more likely to use the labels to drink within guidelines and accurately estimate the number of
standard drinks in their preferred drink (Schoueri‐Mychasiw et al., 2021).
Considering that:
• The concept of standard drink is central to understanding and following Canada’s Guidance on
Alcohol and Health;
• SDL can help consumers follow alcohol guidelines by monitoring their personal alcohol use;
and
• A fundamental idea underlying this project is that people living in Canada have a right to clear
information about alcohol;
A corollary of this project is highlighting that a particular effective policy change could be the
mandatory labelling of all alcoholic beverages to indicate the number of standard drinks in a
container.
2.6.4 Focused Discussions with Indigenous People
Throughout the project, focused discussions were held with Indigenous people serving on the LRDG
executive committee or scientific expert panels. These experts included Dr. Carol Hopkins, Lenape
Nation, Chief Executive Officer, Thunderbird Partnership Foundation; the late Harold Johnson,
Nehiyaw lawyer and author; and Dr. Christopher Mushquash, Anishinabek Professor, Lakehead
University, and Canada Research Chair in Indigenous Mental Health and Addiction.
The discussions began very broadly with regards to Indigenous peoples’ historical relationship with
alcohol (Johnson, 2016). The participants reflected on how alcohol has been used as a tool or
weapon of colonization from its first introduction during the fur trade. They recalled that the negative
impacts were so severe that the numbered treaties included a clause to ban alcohol from Indigenous
territory and communities. This prohibition led to the criminalization of alcohol sales, transportation
and consumption that in turn contributed to high levels of incarceration of Indigenous people,
negative stereotyping, racism and stigma. In the frontier context, binge drinking and related harms
like violence, injuries and accidents became pervasive (Ehrlander, 2010). Drinking alcohol became a

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 42
coping mechanism for dealing with trauma and grief resulting from the losses of self-government,
cultural practices, ceremonies, language and a viable economy, as well as the apprehension,
isolation and abuse of children in the Indian Residential Schools. Indigenous people’s situation
illustrates that the effects of alcohol are not the same for all people and communities.
In this larger context it is important to recognize the bi-modal drinking pattern amongst Indigenous
people. Compared to other adults in Canada, there are proportionately more First Nations adults who
do not use alcohol (42.6%) or engage in binge drinking (50.5%) (First Nations Information
Governance Centre, 2018). Using alcohol without binge drinking is uncommon (6.9%) and generally
confined to those who are urban and have more education and greater career responsibilities. In
most communities, tribal councils and Indigenous organizations, the emphasis has been on
abstinence-based treatment programs with a strong cultural content. The latter serves to reinforce
Indigenous identity with the exploration of hope, belonging, meaning and purpose (Assembly of First
Nations et al., 2011; Thunderbird Partnership Foundation, 2015). Nevertheless, pragmatic harm
reduction strategies have also been embraced by Indigenous communities.
Because of the above considerations, the Indigenous experts questioned the relevance of the LRDGs
for Indigenous people, in terms of the enormity of the challenges with alcohol, the inequity in resources
to address alcohol at the community level, and the cultural and historical contexts surrounding
alcohol. They emphasized that in most Indigenous communities wellness is more oriented toward
abstinence than low-risk alcohol use (Thunderbird Partnership Foundation, 2015). They further
expressed concern that an Indigenous commentary or takeaway, without the correct context, would
simply reinforce systemic racism, negative stereotyping and stigma. Instead, it was suggested that
broad social determinants of health need to be recognized and linked to policies, like addressing
epistemic racism through poverty reduction, income security, accessible employment, colonialism
diminishment, and ensuring Indigenous culture is the foundation of policy (Czyzewski, 2011).
On a smaller scale, Indigenous experts agreed that Indigenous peoples should be involved in
developing knowledge mobilization practices for their people and the following initiatives should be
prioritized for development:
• A risk-based approach to increase alcohol literacy, aligned with the culturally congruent focus on
wellness;
• A harm reduction initiative to promote substance use health among those who choose to use
alcohol, focused on how to reduce the harms of alcohol consumption to self, families and
Indigenous communities; and
• Community-based alcohol interventions, framed as community-based alcohol strategies, with
appropriate guidance, knowledge mobilization and resources.
A narrative approach identifying risk factors, resiliency and the success of different communities was
encouraged. Evaluation resources should accompany the development of these initiatives to ensure
they meet their intended goals. Each objective should be funded to ensure that alcohol issues are
explored and addressed in the appropriate historical and cultural context, guided by an evidence-
based, culturally relevant approach, and using enhanced community-based resources.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 43
Part 3: Experts’ Recommendations
Canada’s LRDGs were originally published in November 2011 and the evidence since then on the
association between drinking alcohol and physical, mental and social harms has continuously
evolved. An update of the guidelines was required to take into account these advancements in what
we know about the risks and benefits associated with alcohol. In July 2020, with the support of
Health Canada, CCSA was mandated to update Canada’s LRDGs. The project has been guided by a
public health perspective and its stated focus has been to provide people living in Canada with the
latest evidence-based advice on alcohol to support them in making informed decisions about its use,
and reduce the risk of harms from alcohol.
When the update of Canada’s LRDGs was initiated, it was anticipated that the new guidelines would
set lower limits for alcohol use. This was, in part, due to several trends that have emerged since the
guidelines were released in 2011: that alcohol use was a risk factor for an increasing number of
diseases; an important proportion of alcohol-attributable deaths in Canada were among people
adhering to the 2011 guidelines; and alcohol guidelines coming from other countries in recent years
had all recommended limits below the 2011 Canadian guidelines. What was not anticipated was
that the evidence review would reveal the extent to which even very small amounts of alcohol can be
harmful to people’s health and well-being. In this context, the experts have agreed to replace
Canada’s LRDGs with
Canada’s Guidance on Alcohol and Health.
Canada’s Guidance on Alcohol and Health
To reduce the risk of harm from alcohol,
it is recommended that people in Canada consider
reducing their alcohol use
.
The reasons to do so derive from the following facts:
a. There is a continuum of risk associated with weekly alcohol consumption where the risk of
harm from alcohol is:
• Low for individuals who consume
2
standard drinks or less per week;
• Moderate for those who consume between
3 and 6
standard drinks per week; and
• Increasingly high for those who consume
7
standard drinks or more per week.
b. Consuming more than
2
standard drinks per drinking occasion is associated with an increased
risk of harms to self and others, including injuries and violence.
c. When pregnant or trying to get pregnant, there is no known safe amount of alcohol use.
d. When breastfeeding, not drinking alcohol is safest.
Sex and Gender
Above the upper limit of the moderate risk zone for alcohol consumption, the health risks
increase more steeply for females than males.
Far more injuries, violence and deaths result from men’s alcohol use, especially in the case of
per occasion drinking.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 44
3.1 Canada’s Guidance on Alcohol and Health
Throughout the life course, there are established thresholds of mortality risk that people are willing
to accept (BMJ Best Practice, n.d.; Starr, 1969). For voluntary activities like unprotected sexual
practices or smoking cigarettes, that level is a 1 in 1,000 mortality risk (i.e., people are willing to
accept a 1 in 1,000 risk of premature death when participating in these activities). For alcohol,
people appear willing to accept a higher risk of death associated with consumption as compared
with other voluntary activities. It is not uncommon for countries to base their guideline
recommendations on a 1 in 100 mortality risk limit (e.g., Australia, France, U.K.). This project revealed
that in Canada, the limit associated with a 1 in 1,000 chance of premature death related to an
alcohol condition is two standard drinks per week, while the 1 in 100 risk limit is six standard drinks
per week.
There is a continuum of risk whereby the risk for those who consume two standard drinks or less per
week is low; it is moderate for those who consume between three and six standard drinks per week;
and it is increasingly high for those who consume more than six standard drinks per week, with
increasing risk conferred by every additional drink.
7
In light of results obtained through this project’s knowledge mobilization activities and with a view to
meet people where they are at, the experts agreed that instead of providing people with strict rules
and recommendations, people in Canada should be presented with a continuum of risk associated
with various levels of alcohol use. The experts anticipate that a continuum of risk will allow people to
situate themselves where they are on that continuum and understand in which risk zone their
alcohol use places them. It is hoped that this will lead people to develop intentions to adopt healthier
and safer behaviours — that is, to move toward a less risky drinking zone along that continuum.
Presenting people in Canada with a continuum is also a direct response to stakeholders’ wishes for
the new guidance to be broadly relatable to all segments of the population, reflecting the different
ways people in Canada use alcohol and the unique health and social outcomes associated with
those patterns of use.
The weekly number of standard drinks that delineate the
continuum’s risk zones align with weekly recommendations in
the U.K. (8.3 standard drinks), Australia, Denmark, France
(7.4
standard drinks) and the Netherlands (5.2 standard drinks). In
Canada, among persons aged 15 and older, about a fifth of
females (23%) and males (21%) do not drink alcohol, 27% of
females and 16% of males usually consume two standard
drinks or less per week; 19% of females and 15% of males
consume three to six standard drinks per week on average and
a third of females (32%) and half of males (49%) usually
consume more than six standard drinks per week. These
proportions are based on data sources from the World Health
Organization (2021) and Statistics Canada (2021).
The continuum of risk is based on average quantities of alcohol people consume per week and the
impact it has on their physical health. The experts looked at other types of evidence to support
people in Canada who may wonder about the consequences of occasional drinking or the immediate
effects that could fall outside the realm of physical health. This line of inquiry uncovers a second
7
Guidelines from BMJ on how to talk about risk were followed to qualify the risk zones (BMJ Best Practice, n.d.).
Among people living in Canada
aged 15 and older, one fifth
(20%) do not drink alcohol,
another fifth (21%) consume
two standard drinks or less per
week on average, 17% consume
three to six standard drinks per
week and 40% consume more
than six standard drinks per
week.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 45
reason behind the recommendation to consider reducing alcohol use: consuming more than two
standard drinks per drinking occasion is associated with an increased risk of harms to self and
others, including injuries and violence.
The experts on this project are aware that the new Guidance on Alcohol and Health with its
continuum of risk will be surprising and unsettling to large segments of the population, including
members of the media, policy makers and those in the alcohol industry. However, the project is
based on the principles of pragmatism and autonomy in harm reduction (Hawk et al., 2017) and the
fundamental idea behind these principles is that
people have the right to know. Alcohol is a
carcinogen related to at least seven types of cancer, including common ones like colon and breast
cancer (Canadian Cancer Society, 2022). It is a main cause of liver diseases, which are on the rise in
Canada (Frolkis et al., 2022; Shaheen et al., 2022). Furthermore, in contrast to common perceptions,
current evidence shows that drinking a little alcohol neither decreases nor increases the risk of
ischemic heart disease. In fact, alcohol consumption is a risk factor for most types of cardiovascular
diseases (Arora et al., 2022) and lower respiratory infections (Morojele et al., 2021), as well as
injuries resulting from violence (see
Update of Canada’s Low-Risk Alcohol Drinking Guidelines:
Overview of Reviews of the Association Between Alcohol Use and Aggression and Violence) and road
crashes (Lyon et al., 2019). It is clear that people should not start to use alcohol or increase their
alcohol use for health benefits. Hence, this project has confirmed that when it comes to drinking
alcohol,
less consumption means less risk of harm from alcohol and from this fact, it is necessary to
promote the message that
it is okay not to drink alcohol.
An encouraging fact associated with this new evidence is that every standard drink counts and any
reduction in alcohol use is beneficial. Research demonstrates that many harms related to chronic
disease caused by alcohol are reversible. People who decrease their alcohol consumption
experience improvements in liver function, insulin resistance, weight, blood pressure and cancer-
related growth factors (Mehta et al., 2018; Thomes et al., 2021). Reductions in alcohol consumption
also decrease hypertension (Roerecke et al., 2017), and reduce the risk of cancer, atrial fibrillation,
stroke, diabetes, pancreatitis and liver cirrhosis (Heckley et al., 2011; Lee et al., 2021; Nikkola et al.,
2013; Verrill et al., 2009; Voskoboinik et al., 2020; Wu et al., 2021). In addition, the risk of infectious
diseases, epilepsy and injuries are affected by the acute effects of alcohol and reductions in alcohol
consumption will immediately decrease the risk of these outcomes (Imtiaz et al., 2017; Samokhvalov
et al., 2010a; Samokhvalov et al., 2010b; Taylor et al., 2010).
The fact that any reduction in alcohol consumption is beneficial is all the more encouraging because
it also applies to those who are unable or unwilling to reduce their risk to low or moderate levels. In
fact, those consuming high levels of alcohol have even more to gain by reducing their consumption
by as much they are able. It should also be noted that those who, regardless of their level of alcohol
use, wish to reduce consumption but are unable to, may want to speak with a primary care provider
about the various evidence-based approaches, including medications and treatment options, that
are available to help reduce alcohol consumption (Regier & Jensen, 2021).
The project's work on the differences between women and men revealed some surprising results,
namely that at low levels of consumption, the physiological differences between females and males
as they affect the lifetime risk of death due to alcohol are minimal. However, the experts are
unequivocal in stating that this should not distract from the evidence that
above the upper limit of
the moderate risk zone for alcohol consumption, the lifetime risk of harm increases more steeply for
women than for men. On the one hand, biological factors enhance the impact of alcohol, causing
more harm and faster intoxication on lesser amounts in females. For example, females sustain more
liver damage on lesser amounts of alcohol compared to males. On the other hand, girls and women

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 46
suffer disproportionately from social factors that contribute to the negative impacts of alcohol in real
life, such as increasing vulnerability to marketing exploitation, stigma, sexual assault and IPV.
On this note, the experts find it imperative to highlight that men’s vulnerability to alcohol should not
be overlooked. The work completed in this project has shown that men are more likely than women
to experience and cause alcohol-related harms. Men drink more alcohol than women do (80% vs.
77%) and are more likely to drink in excess (28% vs 20%) (Government of Canada, 2022). As a
consequence, they are over-represented among drivers involved in alcohol-related serious injury
crashes (75% vs 22%) (Brown et al., 2021). They are also more likely to be treated in hospitals and
hospitalized for alcohol-related medical emergencies and health problems (355 vs 165
hospitalizations per 100,000) (Canadian Institute for Health Information, 2022), to be diagnosed
with an alcohol use disorder (4.7% vs 1.7%) (Pearson et al., 2013), and to die from alcohol-related
causes (7.7% vs 2.6%) (World Health Organization, 2022). Alcohol is also more strongly associated
with perpetration of violence for men then for women.
Far more injuries, violence and deaths result
from men’s drinking, especially in the case of per occasion drinking.
Furthermore, reproductive health is compromised by alcohol use. People in Canada need to be
aware that alcohol is a teratogen or agent that can cause malformation of the fetus. It can lead to
learning, health and social effects with lifelong impact as well as brain injury, birth defects,
behavioural problems, learning disabilities and other health problems typically referred to as FASD.
These adverse effects are observed at relatively low levels of exposure or short-term exposure to
high levels of consumption. For this reason,
when pregnant or trying to get pregnant, there is no
known safe amount of alcohol use.
Alcohol consumption can also negatively impact breastfeeding by causing a decrease in milk
production, early cessation of breastfeeding and effects on infant sleep patterns. Alcohol enters
breast milk through passive diffusion within 30 to 60 minutes following ingestion, so breastfeeding
infants can be exposed to alcohol through breastmilk. However, infants are less able to metabolize
alcohol. Therefore,
when breastfeeding, no alcohol use is safest for the baby.
Finally, it should be pointed out that there are circumstances, other than those related to
reproductive health, where the guidance's main recommendation does not apply and where no
alcohol is safest. That is when driving a motor vehicle, using machinery and tools, taking medicine or
other drugs that interact with alcohol, doing any kind of dangerous physical activity, being
responsible for the safety of others or making important decisions.
3.2 Limitations
This project represents a synthesis of the best available evidence about the relationship between
alcohol use and health outcomes. However, the current evidence base has limitations that are
important to acknowledge. Specifically, there have been no randomized trials of alcohol consumption
for any morbidity or mortality outcome. As noted in section 2.1.3, the observational studies that
comprise the bulk of the evidence incorporated in this report are subject to a variety of threats to
validity, mainly not controlling for confounding variables, only adjusting to age and sex. However, this
is not to imply that observational studies are not helpful or valid when there is growing explicit
acknowledgement in epidemiology that observational studies can also aim to estimate causal effects
(Boon et al., 2022; Hernán, 2018).
Genetic (Mendelian) randomization studies were not included in our evidence base because they do
not generally provide risk estimates in small enough increments of consumption to be useful for
guidelines, and because there are few meta-analyses of genetic randomization studies. However,
genetic studies do not find protective effects from low volume alcohol consumption for coronary

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 47
heart disease or ischemic strokes, contradicting findings from observational studies, including when
the two analytic methods are compared side-by-side using the same data (Au Yeung et al., 2013;
Chen et al., 2008; Cho et al., 2015; Holmes et al., 2014; Lawlor et al., 2013). On this basis, because
coronary heart disease and ischemic stroke are important contributors to total mortality, it is
possible that we are underestimating the impact of alcohol on the risk of premature death compared
to not drinking, particularly at lower levels of consumption.
Most studies included in the meta-analyses used for this project assessed alcohol-outcomes based
on weekly average levels of alcohol use and failed to account for the effects of drinking patterns
(e.g., binge drinking or spacing out drinking over time) within those average levels. Hence, we were
unable to directly model how binge drinking affects the risk of disease and injury. However, binge
drinking is indirectly accounted for in our models as weekly alcohol consumption is correlated with
the probability of binge drinking (Stahre et al., 2006).
Our report focuses mainly on health conditions that result in death. Existing literature was not
adequate to characterize the relationship between alcohol use and important non-lethal conditions.
These conditions would include those related to mental health but also several outcomes within the
social realm. While this project reviewed the association between alcohol, aggression and violence,
future alcohol guidelines should aim to incorporate other social issues such as neglect, crime, and
job or school performance. Our report also does not cover the intangible effects of alcohol use,
including suffering related to adverse outcomes or social enjoyment from alcohol consumption.
This project and its conclusions are based largely on population averages, and do not necessarily
apply to any individual and their unique socio-behavioural, genetic and medical circumstances, nor
do they account for risk and protective factors at the community, familial or individual levels. As
mentioned below, these issues should be addressed in the next phase of this project, which will
focus on the guidance’s dissemination, appropriation and use. Individualizing risk should be an
important goal of this project’s knowledge mobilization activities.
Finally, the parameters of the project did not allow for a detailed analysis of the relationship between
alcohol use and harm among youth, especially those under the legal drinking age, an area that
should be pursued. It is well established that alcohol is the most common psychoactive substance
used by youth and that it is a leading behavioural risk factor for death and social problems in this
age group (American College Health Association, 2016; Health Canada, 2015, 2021; Pearson et al.,
2013). A high proportion of alcohol consumed by youth is consumed through binge drinking with its
attendant risks of alterations to brain development and cognitive function (Carson, 2015; Crews
et al., 2016; Spear, 2018). Binge drinking also increase the risk of injury, aggression, violence and
other age-related consequences such as dating violence and worsening academic performance
(American College Health Association, 2016; Health Canada, 2015, 2021). Even for the same
number of drinks consumed per drinking occasion, the risk of adverse outcomes from alcohol
consumption is greater for youth than for adults. This may be due to several factors, including
greater impulsivity and less emotional maturity among youth, lower body mass on average, less
experience doing complex tasks that are made more dangerous by alcohol, and faster drinking
speeds (Crews et al., 2016). For these reasons,
the prudent advice to youth is to delay alcohol use
for as long as possible.
3.3 Moving Forward
In light of the new Guidance on Alcohol and Health and the fact that alcohol literacy in the population
is low (Canadian Centre on Substance Use and Addiction, 2021),
substantial and sustained efforts
will be required to develop messaging that speaks directly to the unique concerns of people with

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 48
diverse backgrounds and personal experiences who ultimately will make their own choices. For
example, work developed in parallel with this project has shown that alcohol consumers aged 18 to
30 may be more receptive to health messaging about the effects of their alcohol use on life
expectancy, than to messages that simply present a guideline (Stockwell et al., 2022). Others may
want to direct their prevention efforts toward young adults, particularly boys and young men among
whom drinking to intoxication is normalized. For example, there is a need to address the belief among
men that alcohol serves as an excuse for risky and aggressive behaviours. The message needs to be
sent to men that that they should take extra care when they drink alcohol so that they and others are
not injured or hurt because of their alcohol use. Other recommendations and suggestions, particularly
in relation to sex and gender, have been prepared in connection with this project and are available to
those who would like to build a campaign around them (see Appendix 3).
Furthermore, the individualization of risk should be an important goal of this project’s knowledge
mobilization. Health professionals, family doctors and nurses, who are crucial allies with credibility in
explaining the continuum of risks associated with alcohol to patients and the general public, will need
to be involved. They could make a valuable contribution to health care by reducing direct alcohol-
related costs; we will return to this issue below.
People in Canada should “Learn the facts. Parse the fictions. Act accordingly.”
8
To do so, they will
need more than plain and clear information, no matter how effective newly developed target
campaigns may be. Alcohol, like tobacco or processed foods, has been termed a “sinful good,”
meaning that when people use it they get the pleasure now and suffer the consequences later. To
make wise decisions about such goods, people need encouragement (Thaler & Sunstein, 2008).
People in Canada who want to move toward the lower end of the continuum of alcohol-related risks
need an environment that supports healthier and safer decisions. There needs to be a cultural shift
away from an alcogenic culture (Johnston, 2014). Therefore
, a corollary to the current project is for
governments to design a healthier environment to make it easier for people to make difficult
decisions about alcohol.
First and foremost, evidence shows that, to adhere to the Guidance on Alcohol and Health,
consumers will need consistent, easy-to-use information on alcohol containers to accurately track
and monitor their alcohol use in terms of standard drinks. While beer remains the alcoholic beverage
of choice for people in Canada, the growing craft movement is producing beer with a variety of
alcohol content levels and in a variety of sizes of cans and bottles for consumption at home. Now,
more than ever, to count how many standard drinks they consume, people need information at the
point of pour. While Canada is a world leader in mandating enhanced labels on tobacco and
cannabis packages, alcohol containers are exempt from these requirements. Enhanced alcohol
container labels are an increasingly popular strategy for providing information to consumers, and a
key recommendation by national and international health organizations (Jané-Llopis et al., 2020;
Vallance et al., 2021; World Health Organization, 2022). A direct consequence of the current project
is the recognition that an especially effective policy change could be
the mandatory labelling of all
alcoholic beverages with the number of standard drinks in a container.
Many studies have shown that people are most likely to follow guidance if they know the reasons
why they should (Pettigrew et al., 2021; Wakefield et al., 2018). Our public consultation revealed
that without understanding the risks and benefits associated with alcohol use, people are unlikely to
understand why they should follow the guidelines. Therefore,
mandatory labelling of all alcoholic
beverages with health warnings and Canada’s Guidance on Alcohol and Health would also be
adequate and effective. Labelling can be an important intervention in a more comprehensive alcohol
8
These words are used by Alec Bruce in an op-ed published in The Globe and Mail on Nov. 12, 2021 (Bruce, 2021, Nov. 12).
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 49
strategy (Kokole et al., 2021). Evidence has shown that adding health warnings to alcohol labels can
increase public awareness of the causal link with cancer and reduce per capita alcohol consumption.
Health warning labels can also strengthen public support for policies that are often unpopular but
known to reduce population-level alcohol-caused harms (Weerasinghe et al., 2020).
To support people living in Canada who want to move toward the less risky end of the continuum,
governments will need to be involved on other policy fronts. Cost-effective policies and feasible
interventions that reduce the overall level of alcohol consumption are well documented at the global,
national and provincial levels (Vallance et al., 2021; World Health Organization, 2022). For example,
work conducted by the Canadian Alcohol Policy Evaluation
committee and the National Alcohol
Strategy Advisory Committee has highlighted that measures such as strengthened regulations of
alcohol advertising and marketing, restrictions on the physical availability of alcohol, and the
adoption of a minimum price for alcohol sold are all beneficial to public health. If the new Guidance
on Alcohol and Health were to facilitate policy discussions and initiatives, the effects could be
considerable and extend beyond the public health sphere to include economic benefits.
Alcohol is a leading preventable cause of death, disability injuries, accidents and social problems. In
2017, it caused 18,000 deaths in Canada, and the year before, there were about 77,000
hospitalizations due to conditions entirely caused by alcohol, an average of 212 a day (Canadian
Institute for Health Information, 2022). According to the Canadian Substance Use Costs and Harms
study (Canadian Substance Use Costs and Harms Scientific Working Group, 2020), the annual direct
costs of alcohol are $16.7 billion, with $5,4 billion of that sum being spent on health care. This is far
more than the direct costs associated with tobacco ($12.3 billion), opioids ($5.9 billion) or cannabis
($3.2 billion), and far exceeding the value of the revenue produced by alcohol sales and taxation,
which was last estimated to be $13.5 billion (Statistics Canada, 2021).
Hence, by adopting policies
to support healthier and safer decisions around alcohol use, government may save money and
reduce per-person costs attributable to alcohol use in Canada, most recently estimated at $455 per
year (Canadian Substance Use Costs and Harms Scientific Working Group, 2020).
3.4 Future Update of Canada’s Guidance on Alcohol and
Health
We recommend that the Guidance on Alcohol and Health be regularly reviewed as the field of alcohol
epidemiology develops. More specifically, an update should be requested when:
• Emerging or improved methods are available to address the previously mentioned limitations;
• The availability of evidence changes. For example, when high-quality studies on alcohol-caused
conditions like mental health become available, or when evidence identifies new alcohol-caused
conditions that are currently unappreciated or wholly recognized. This could be the case for
conditions such as melanoma and prostate, pancreatic, gastric and stomach cancers, for which
evidence is accumulating that alcohol consumption could be a risk factor.
• The prevalence of alcohol consumption changes within the population, new segments of the
population become particularly at risk or new consumption patterns such as polysubstance use
emerge.
3.5 Conclusion
Canada’s Guidance on Alcohol and Health reflects the conclusions drawn from global evidence
reviews, mathematical modelling, consultations with the public and experts, and discussion among

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 50
the experts on the project. It is hoped that this work will be useful to people in Canada who are
health conscious and want to know more about the effects of alcohol consumption on their well-
being. The Guidance on Alcohol and Health was developed to help them make informed decisions
about their alcohol use.
The Guidance on Alcohol and Health requires a cultural shift that, by and large, can only be
orchestrated by governments through policies and collaboration with employers, healthcare
providers and community stakeholders to make people aware of and better at managing their risks.
The evidence reviewed and presented here should influence provincial and federal governments to
implement alcohol policies focused on reducing alcohol-related harms and promoting health and
wellness. Information and advice are useful and necessary for people in Canada, but an environment
supporting healthier and more informed-behaviour choices around alcohol is an absolute pre-requisite
for a healthy society.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 51
References
Alpert, H. R., Slater, M. E., Yoon, Y. H., Chen, C. M., Winstanley, N., & Esser, M. B. (2022). Alcohol
consumption and 15 causes of fatal injuries: A systematic review and meta-analysis. American
Journal of Preventive Medicine, 63(2), 286–300.
https://doi.org/10.1016/j.amepre.2022.03.025
American College Health Association. (2016). National College Health Assessment II: Canadian
reference group, executive summary, spring 2016. Hanover, MD: Author.
https://www.acha.org/documents/ncha/NCHA-
II%20SPRING%202016%20CANADIAN%20REFERENCE%20GROUP%20EXECUTIVE%20SUMMAR
Y.pdf
Assembly of First Nations, National Native Addictions Partnership Foundation & Health Canada.
(2011). Honouring our strengths: A renewed framework to address substance abuse issues
among First Nations people in Canada.
https://thunderbirdpf.org/wp-
content/uploads/2014/02/Honouring-Our-Strengths-2011_Eng1.pdf
Arora, M., ElSayed, A., Beger, B., Naidoo, P., Shilton, T., Jain, N., … Champagne, B.M. (2022). The
impact of alcohol consumption on cardiovascular health: Myths and measures. Global Heart,
17(1), Article 45. https://doi.org/10.5334/gh.1132
Au Yeung, S.L., Jiang, C., Cheng, K.K., Cowling, B.J., Liu, B., Zhang, W., … Schooling, C.M. (2013).
Moderate alcohol use and cardiovascular disease from Mendelian randomization. Plos One, 8(7),
e68054. https://doi.org/10.1371/journal.pone.0068054
Bagnardi, V., Rota, M., Botteri, E., Tramacere, I., Islami, F., Fedirko, V., … La Vecchia, C. (2015).
Alcohol consumption and site-specific cancer risk: A comprehensive dose–response meta-
analysis. British Journal of Cancer, 112(3), 580–593. https://doi.org/10.1038/bjc.2014.579
Bergeron, C.D., Tremblay-Antoine, C., Dufresne, Y., Morin, R., April, N., Lelair, V., … Ouellet, C. (2021).
La consommation d’alcool: qu’en pense la population du Québec? Québec, Qué.:
https://www.inspq.qc.ca/sites/default/files/publications/2772-consommation-alcool-
population-quebec.pdf
Biemer P. P., Groves, R. M., Lyberg, L. E., Mathiowetz, N. A., & Sudman, S. (Eds.). (2013).
Measurement errors in surveys. Hoboken, NJ: John Wiley & Sons.
Blomberg, R. D., Peck, R. C., Moskowitz, H., Burns, M., & Fiorentino, D. (2009). The Long Beach/Fort
Lauderdale relative risk study. Journal of Safety Research, 40(4), 285–292.
https://doi.org/10.1016/j.jsr.2009.07.002
BMJ Best Practice. (n.d.). Understanding risk. https://bestpractice.bmj.com/info/toolkit/practise-
ebm/understanding-risk/
Boon, M. H., Burns, J., Craig, P., Griebler, U., Heise, T. L., Katikireddi, S. V., … Bero, L. (2022). Value
and challenges of using observational studies in systematic reviews of public health
interventions. American Journal of Public Health, 112(4), 548–552.
https://doi.org/10.2105/ajph.2021.306658
Brabete, A. C., Greaves, L., Hemsing, N., & Stinson, J. (2020). Sex- and gender-based analysis in
cannabis treatment outcomes: A systematic review. International Journal of Environmental
Research and Public Health, 17(3), Article 872. https://doi.org/10.3390/ijerph17030872
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 52
Brewer, R. D., & Swahn, M. H. (2005). Binge drinking and violence. JAMA, 294(5), 616–618.
https://doi.org/10.1001/jama.294.5.616
Broholm, K., Galluzzo, L., Gandin, C., Ghirini, S., Ghiselli, A., Jones, L., … Mäkelä, P. (2016). Good
practice principles for low risk drinking guidelines. Helsinki, Finland: National Institute for Health
and Welfare.
https://www.julkari.fi/bitstream/handle/10024/131322/WP5%20Good%20practice%20low%2
0risk%20guidelines.pdf?sequence=1&isAllowed=y
Brown, S. W., Vanlaar, W. G. M., Robertson, R. D., & The Traffic Injury Research Foundation of
Canada. (2021). The Alcohol and Drug Crash Problem in Canada 2016 Report. Ottawa, Ont.:
Canadian Council of Motor Transport Administrators.
https://www.ccmta.ca/web/default/files/PDF/CCMTA.2016%20Alcohol%20and%20Drug%20Cr
ash%20Problem%20Report.EN.MAR2021.pdf
Bruce, A. (2021, Nov. 12). Drinking skyrocketed during COVID-19. Why’s it so hard to learn the facts
about alcohol? Globe and Mail.
https://www.theglobeandmail.com/opinion/article-drinking-
skyrocketed-during-covid-19-whys-it-so-hard-to-learn-the/
Brunk, E., Becker, M. W., & Bix, L. (2020). Empirical evaluation of the presence of a label containing
standard drinks on pour accuracy among US college students. PloS one, 15(11), Article
e0241583. https://doi.org/10.1371/journal.pone.0241583
Butt, P., Beirness, D., Gliksman, L., Paradis, C., & Stockwell, T. (2011). Alcohol and health in Canada:
A summary of evidence and guidelines for low-risk drinking. Ottawa, ON: Canadian Centre on
Substance Abuse.
https://www.ccsa.ca/sites/default/files/2019-04/2011-Summary-of-
Evidence-and-Guidelines-for-Low-Risk%20Drinking-en.pdf
Canadian Cancer Society. (2022). Some sobering facts about alcohol and cancer risk.
https://cancer.ca/en/cancer-information/reduce-your-risk/limit-alcohol/some-sobering-facts-
about-alcohol-and-cancer-risk
Canadian Centre on Substance Abuse. (2014). Recalculating risky drinking in women. Ottawa, Ont.:
Author.
Canadian Centre on Substance Use and Addiction. (2021). Update of Canada’s Low-Risk Alcohol
Drinking Guidelines: Summary of findings from public consultation. Ottawa, Ont.: Author.
https://www.ccsa.ca/sites/default/files/2021-09/CCSA-Lower-Risk-Drinking-Guidelines-
Summary-Findings-Public-Consultation-2021-en_0.pdf
Canadian Institute for Health Information. (2022). Hospitalizations entirely caused by alcohol.
https://yourhealthsystem.cihi.ca/hsp/inbrief?lang=en#!/indicators/061/hospitalizations-
entirely-caused-by-alcohol/;mapC1;mapLevel2;/
Canadian Substance Use Costs and Harms Scientific Working Group. (2020). Canadian substance
use costs and harms 2015–2017. (Prepared by the Canadian Institute for Substance Use
Research and the Canadian Centre on Substance Use and Addiction.) Ottawa, Ont.: Canadian
Centre on Substance Use and Addiction.
https://csuch.ca/publications/CSUCH-Canadian-
Substance-Use-Costs-Harms-Report-2020-en.pdf
Carson, A. (2015). Alcohol and the developing adolescent brain: Evidence review. Journal of the
Royal College of Physicians of Edinburgh, 45(1), 12-14.
https://doi.org/10.4997/JRCPE.2015.103
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 53
Centers for Disease Control and Prevention. (2022). Binge drinking.
https://www.cdc.gov/alcohol/fact-sheets/binge-drinking.htm
Chen, L., Davey Smith, G., Harbord, R. M., & Lewis, S. J. (2008). Alcohol intake and blood pressure: a
systematic review implementing a Mendelian randomization approach. PLoS Medicine, 5(3),
e52. https://doi.org/10.1371/journal.pmed.0050052
Cherpitel, C. J., Ye, Y., Bond, J., Borges, G., & Monteiro, M. (2015). Relative risk of injury from acute
alcohol consumption: modeling the dose–response relationship in emergency department data
from 18 countries. Addiction, 110(2), 279–288. https://doi.org/10.1111/add.12755
Chikritzhs, T., Stockwell, T., Naimi, T., Andreasson, S., Dangardt, F., & Liang, W. (2015). Has the
leaning tower of presumed health benefits from ‘moderate’ alcohol use finally collapsed?
Addiction, 110(5), 726–727. https://doi.org/10.1111/add.12828
Cho, Y., Shin, S.-Y., Won, S., Relton, C. L., Davey Smith, G., & Shin, M.-J. (2015). Alcohol intake and
cardiovascular risk factors: A Mendelian randomisation study. Scientific Reports, 5, Article
18422. https://doi.org/10.1038/srep18422
Choenni, V., Hammink, A., & van de Mheen, D. (2017). Association between substance use and the
perpetration of family violence in industrialized countries: A systematic review. Trauma Violence
Abuse, 18(1), 37–50. https://doi.org/10.1177/1524838015589253
Compton, R. P. & Berning, A. (2015). Drug and Alcohol Crash Risk. (Traffic Safety Facts Research
Note. DOT HS 812 117). Washington, DC: National Highway Traffic Safety Administration.
https://www.nhtsa.gov/staticfiles/nti/pdf/812117-Drug_and_Alcohol_Crash_Risk.pdf
Crews, F.T., Vetreno, R.P., Broadwater, M.A., & Robinson, D.L. (2016). Adolescent alcohol exposure
persistently impacts adult neurobiology and behavior. Pharmacological Reviews, 68(4), 1074–
1109. https://doi.org/10.1124/pr.115.012138
Czyzewski, K. (2011). Colonialism as a broader social determinant of health. International
Indigenous Policy Journal,2(1), Article 5. https://doi.org/10.18584/iipj.2011.2.1.5
Dawson, D. A., Grant, B. F., & Li, T. K. (2005). Quantifying the risks associated with exceeding
recommended drinking limits. Alcoholism, Clinical and Experimental Research, 29(5), 902–908.
https://doi.org/10.1097/01.alc.0000164544.45746.a7
de Visser, R. O., & Birch, J. D. (2012). My cup runneth over: Young people’s lack of knowledge of low-
risk drinking guidelines. Drug and Alcohol Review, 31(2), 206–212.
https://doi.org/10.1111/j.1465-3362.2011.00371.x
Devries, K. M., Child, J. C., Bacchus, L. J., Mak, J., Falder, G., Graham, K., Watts, C., & Heise, L.
(2014). Intimate partner violence victimization and alcohol consumption in women: A systematic
review and meta-analysis. Addiction, 109(3), 379–391. https://doi.org/10.1111/add.12393
Dietary Guidelines Advisory Committee. (2020). Scientific report of the 2020 Dietary Guidelines
Advisory Committee. Washington, DC: U.S. Department of Agriculture, Agricultural Research
Service. https://doi.org/10.52570/DGAC2020
Dowling, N., Clark, D., & Corney, T. (2006). Responsible drinking knowledge: A comparison of
Australian apprentices and university students. Youth Studies Australia, 25(3). 42–48
Ehrlander, M. (2010). The historical roots of a frontier alcohol culture: Alaska and northern Canada.
The Northern Review, 32, 63–103. https://thenorthernreview.ca/index.php/nr/article/view/14
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 54
Exum, M. L. (2006). Alcohol and aggression: An integration of findings from experimental studies.
Journal of Criminal Justice, 34(2), 131–145. https://doi.org/10.1016/j.jcrimjus.2006.01.008
Fillmore, M.T. & Jude, R. (2011), Defining “binge” drinking as five drinks per occasion or drinking to a
.08% BAC: Which is more sensitive to risk? American Journal on Addictions, 20, 468–475.
https://doi.org/10.1111/j.1521-0391.2011.00156.x
First Nations Information Governance Centre. (2018). National report of the First Nations Regional
Health Survey, Phase 3: Volume One. Ottawa, Ont.: Author.
https://fnigc.ca/wp-
content/uploads/2020/09/713c8fd606a8eeb021debc927332938d_FNIGC-RHS-Phase-III-
Report1-FINAL-VERSION-Dec.2018.pdf
Frolkis, A., Borman, M., Sadler, M., Congly, S., Nguyen, H., Lee, S., … Shaheen, A. A. (2022).
Increased hospital admissions for alcohol-associated hepatitis during the COVID-19 pandemic in
Alberta, Canada: A retrospective cohort study. Journal of Hepatology, 77, S143.
https://doi.org/10.1016/S0168-8278(22)00665-1
Government of Canada. (2022). Alcohol use among Canadians.
https://health-infobase.canada.ca/alcohol/ctads/
Graham, K., Wells, S., & West, P. (1997). A framework for applying explanations of alcohol-related
aggression to naturally occurring aggressive behavior. Contemporary Drug Problems, 24(4),
625–666. https://doi.org/10.1177/009145099702400402
Graham, K., Leonard, K., Room, R., Wild, T. C., Pihl, R. O., Bois, C., & Single, E. (1998). Current
directions in research on understanding and preventing intoxicated aggression. Addiction, 93(5),
659–676. https://doi.org/10.1046/j.1360-0443.1998.9356593.x
Greaves, L., Poole, N., & Brabete, A. C. (2022). Sex, gender, and alcohol use: implications for women
and low-risk drinking guidelines. International Journal of Environmental Research and Public
Health, 19(8), Article 4523. https://doi.org/10.3390/ijerph19084523
Hawk, M., Coulter, R., Egan, J., Fisk, S., Friedman, M., Tula, M., & Kinsky, S. (2017). Harm reduction
principles for healthcare settings. Harm Reduction Journal, 14(1), Article 70.
https://doi.org/10.1186/s12954-017-0196-4
Hawks, D. (1999). Not much to ask for, really! The introduction of standard drink labelling in
Australia. Addiction, 94(6), 801–811. https://doi.org/10.1046/j.1360-0443.1999.9468014.x
Health Canada. (2015). Summary of results: Canadian Student Tobacco, Alcohol and Drugs Survey
2014-15
https://www.canada.ca/en/health-canada/services/canadian-student-tobacco-
alcohol-drugs-survey/2014-2015-summary.html
Health Canada. (2019). Canadian Alcohol and Drugs Survey (CADS): Summary of results for 2019.
https://www.canada.ca/en/health-canada/services/canadian-alcohol-drugs-survey/2019-
summary.html
Health Canada. (2021). Canadian Postsecondary Education Alcohol and Drug Use Survey,
2019/2020. https://health-infobase.canada.ca/alcohol/cpads/
Heckley, G. A., Jarl, J., Asamoah, B. O., & G-Gerdtham, U. (2011). How the risk of liver cancer changes
after alcohol cessation: a review and meta-analysis of the current literature. BMC Cancer, 11,
Article 446. https://doi.org/10.1186/1471-2407-11-446
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 55
Hernán, M.A. (2018). The C-word: Scientific euphemisms do not improve causal inference from
observational data. National Library of Medicine, 108(5), 616–619.
https://doi.org/10.2105/AJPH.2018.304337
Hobin, E., Jansen, R., Vanderlee,. L., & Berenbaum, E. (2022). Enhanced alcohol container labels: A
systematic review. Ottawa, Ont.: Canadian Centre on Substance Use and Addiction.
https://www.ccsa.ca/sites/default/files/2022-02/CCSA-Enhanced-Alcohol-Container-Labels-
Systematic-Review-Report-en.pdf
Holmes, J., Angus, C., Meier, P. S., Buykx, P., & Brennan, A. (2019). How should we set consumption
thresholds for low risk drinking guidelines? Achieving objectivity and transparency using
evidence, expert judgement and pragmatism. Addiction, 114(4), 590–600.
https://doi.org/10.1111/add.14381
Holmes, M. V., Dale, C. E., Zuccolo, L., Silverwood, R. J., Guo, Y., Ye, Z., Prieto-Merino, D., … Casas,
J.P. (2014). Association between alcohol and cardiovascular disease: Mendelian randomisation
analysis based on individual participant data. BMJ, 349, g4164.
https://doi.org/10.1136/bmj.g4164
Imtiaz, S., Shield, K. D., Roerecke, M., Samokhvalov, A. V., Lönnroth, K., & Rehm, J. (2017). Alcohol
consumption as a risk factor for tuberculosis: meta-analyses and burden of disease. European
Respiratory Journal, 50(1), Article 1700216. https://doi.org/10.1183/13993003.00216-2017
Institute for Health Metrics and Evaluation. (2018). Data visualizations: GBD compare. Seattle,
Washington: Author. https://vizhub.healthdata.org/gbd-compare/
International Agency for Research on Cancer. (2012). Personal habits and indoor combustions,
Volume 100 E: A review of human carcinogens. Lyon, France: Author.
https://monographs.iarc.who.int/wp-content/uploads/2018/06/mono100E.pdf
Jané-Llopis, E., Kokole, D., Neufeld, M., Hasan, O. S. M., & Rehm, J. (2020). What is the current
alcohol labelling practice in the WHO European Region and what are barriers and facilitators to
development and implementation of alcohol labelling policy? Copenhagen: WHO Regional Office
for Europe. https://www.ncbi.nlm.nih.gov/books/NBK558550/
Johnson, H. (2016). Firewater: How alcohol is killing my people (and yours). Regina, Sask.: University
of Regina Press.
Johnston, A. D. (2014). Drink: The intimate relationship between women and alcohol. Harper Collins.
Jones, L., & Bellis, M. A. (2013). CMO alcohol guidelines review: A summary of the evidence on
understanding and response to public health guidelines. Liverpool, England: Centre for Public
Health.
https://www.drugsandalcohol.ie/25026/1/LJMU_CMO-Alcohol-Guidelines-Behavioural-
Review.pdf
King, A. C. (1994). Enhancing the self-report of alcohol consumption in the community: Two
questionnaire formats. American Journal of Public Health, 84(2), 294–296.
https://doi.org/10.2105/ajph.84.2.294
Knott, C., Bell, S., & Britton, A. (2015). Alcohol consumption and the risk of type 2 diabetes: A
systematic review and dose-response meta-analysis of more than 1.9 million individuals from 38
observational studies. Diabetes Care, 38(9), 1804–1812. https://doi.org/10.2337/dc15-0710
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 56
Kokole, D., Anderson, P., & Jané-Llopis, E. (2021). Nature and potential impact of alcohol health
warning labels: A scoping review. Nutrients, 13(9), Article 3065.
https://doi.org/10.3390/nu13093065
Larsson, S. C., Burgess, S., Mason, A. M., & Michaëlsson, K. (2020). Alcohol consumption and
cardiovascular disease: A Mendelian randomization study. Circulation: Genomic and Precision
Medicine, 13(3), Article e002814. https://doi.org/10.1161/CIRCGEN.119.002814
Larsson, S. C., Drca, N., & Wolk, A. (2014). Alcohol consumption and risk of atrial fibrillation: a
prospective study and dose-response meta-analysis. Journal of the American College of
Cardiology, 64(3), 281–289. https://doi.org/10.1016/j.jacc.2014.03.048
Larsson, S. C., Wallin, A., Wolk, A., & Markus, H. S. (2016). Differing association of alcohol
consumption with different stroke types: A systematic review and meta-analysis. BMC Medicine,
14, Article 178. https://doi.org/10.1186/s12916-016-0721-4
Laslett, A.-M., Room, R., Waleewong, O., Stanesby, O., & Callinan, S. (Eds.). (2019). Harm to others
from drinking: Patterns in nine societies. Geneva: World Health Organization.
https://apps.who.int/iris/handle/10665/329393
Lawlor, D. A., Nordestgaard, B. G., Benn, M., Zuccolo, L., Tybjaerg-Hansen, A., & Davey Smith, G.
(2013). Exploring causal associations between alcohol and coronary heart disease risk factors:
findings from a Mendelian randomization study in the Copenhagen General Population Study.
European Heart Journal, 34(32), 2519–2528. https://doi.org/10.1093/eurheartj/eht081
Lee, S.-R., Choi, E.-K., Jung, J.-H., Han, K.-D., Oh, S., & Lip, G. Y. H. (2021). Lower risk of stroke after
alcohol abstinence in patients with incident atrial fibrillation: A nationwide population-based
cohort study. European Heart Journal, 42(46) 4759–4768.
https://doi.org/10.1093/eurheartj/ehab315
Liu, F., Liu, Y., Sun, X., Yin, Z., Li, H., Deng, K., … Hu, D. (2020). Race- and sex-specific association
between alcohol consumption and hypertension in 22 cohort studies: A systematic review and
meta-analysis. Nutrition, Metabolism and Cardiovascular Diseases, 30(8), 1249–1259.
https://doi.org/10.1016/j.numecd.2020.03.018
Liu, Y., Nguyen, N., & Colditz, G. A. (2015). Links between alcohol consumption and breast cancer: A
look at the evidence. Women’s Health, 11(1), 65-77. https://doi.org/10.2217/WHE.14.62
Llerena, S., Arias-Loste, M. T., Puente, A., Cabezas, J., Crespo, J., & Fábrega, E. (2015). Binge
drinking: Burden of liver disease and beyond. World Journal of Hepatology, 7(27), 2703–2715.
https://doi.org/10.4254/wjh.v7.i27.2703
Lu, P.-Y., Shu, L., Shen, S.-S., Chen, X.-J., & Zhang, X.-Y. (2017). Dietary patterns and pancreatic
cancer risk: A meta-analysis. Nutrients, 9(1), Article 38. http://dx.doi.org/10.3390/nu9010038
Lyon, C., Brown, S., Vanlaar, W., & Robertson, R. (2019). Road Safety Monitor 2019: Drinking and
driving attitudes & practices in Canada. Ottawa, Ont.: Traffic Injury Research Foundation.
Mehta, G., Macdonald, S., Cronberg, A., Rosselli, M., Khera-Butler, T., Sumpter, C., … Moore, K. P.
(2018). Short-term abstinence from alcohol and changes in cardiovascular risk factors, liver
function tests and cancer-related growth factors: A prospective observational study. BMJ Open,
8(5), Article e020673. https://doi.org/10.1136/bmjopen-2017-020673
Midanik, L. T. (1999). Drunkenness, feeling the effects and 5+ measures. Addiction, 94(6), 887–
897. https://doi.org/10.1046/j.1360-0443.1999.94688711.x
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 57
Miller, W. R., Heather, N., & Hall, W. (1991). Calculating standard drink units: International
comparisons. British Journal of Addiction, 86(1), 43–47.
https://doi.org/10.1111/j.1360-
0443.1991.tb02627.x
Morojele, N.K., Shenoi, S.V., Shuper, P.A., Braithwaite, R.S., & Rehm, J. (2021). Alcohol use and the
risk of communicable diseases. Nutrients, 13(10), Article 3317.
https://doi.org/10.3390/nu13103317
Mukamal, K. J., Maclure, M., Muller, J. E., & Mittleman, M. A. (2005). Binge drinking and mortality
after acute myocardial infarction. Circulation, 112(25), 3839–3845.
https://doi.org/10.1161/CIRCULATIONAHA.105.574749
Naimi, T. S., Blanchette, J., Nelson, T. F., Nguyen, T., Oussayef, N., Heeren, T. C., … Xuan, Z. (2014). A
new scale of the U.S. alcohol policy environment and its relationship to binge drinking. American
Journal of Preventive Medicine, 46(1), 10–16. https://doi.org/10.1016/j.amepre.2013.07.015
Naimi, T. S., Brewer, R. D., Mokdad, A., Denny, C., Serdula, M. K., & Marks, J. S. (2003). Binge
drinking among US adults. JAMA, 289(1), 70–75. https://doi.org/10.1001/jama.289.1.70
National Health and Medical Research Council. (2020). Australian guidelines to reduce health risks
from drinking alcohol. Canberra, Australia: Author.
https://www.nhmrc.gov.au/about-
us/publications/australian-guidelines-reduce-health-risks-drinking-alcohol
National Institute of Alcohol Abuse & Alcoholism. (2004). NIAAA council approves binge drinking
definition. NIAAA Newsletter, 2004(3), 3.
http://pubs.niaaa.nih.gov/publications/Newsletter/winter2004/Newsletter_Number3.pdf
Newton, S., Morona, J., Salinger, K., & Merlin, T. (2018). Systematic literature review on the
association between alcohol consumption and mental health disorders. Adelaide, South
Australia: Adelaide Health Technology Assessment.
https://www.nhmrc.gov.au/sites/default/files/documents/attachments/Alcohol/4-tech-report-
systematic-review.pdf
Nikkola, J., Räty, S., Laukkarinen, J., Seppänen, H., Lappalainen-Lehto, R., Järvinen, S., Nordback, I.,
& Sand, J. (2013). Abstinence after first acute alcohol-associated pancreatitis protects against
recurrent pancreatitis and minimizes the risk of pancreatic dysfunction. Alcohol and Alcoholism,
48(4), 483–486. https://doi.org/10.1093/alcalc/agt019
Osiowy, M., Stockwell, T., Zhao, J., Thompson, K., & Moore, S. (2015). How much did you actually
drink last night? An evaluation of standard drink labels as an aid to monitoring personal
consumption. Addiction Research & Theory, 23(2), 163–169.
https://doi.org/10.3109/16066359.2014.955480
Paradis, C. (2016). Canada’s National Alcohol Strategy: It’s time to assess progress. Canadian
Journal of Program Evaluation, 31(2), 232–241.
https://journalhosting.ucalgary.ca/index.php/cjpe/article/view/31045
Parrott, D. J., & Eckhardt, C. I. (2018). Effects of alcohol on human aggression. Current Opinion in
Psychology, 19, 1–5. https://doi.org/10.1016/j.copsyc.2017.03.023
Paula, T., Chagas, C., Martins, L. B., & Ferri, C. P. (2020). Low-risk drinking guidelines around the
world: An overview of the current situation. Addictive Disorders & Their Treatment, 19(4), 218–
227. https://doi.org/10.1097/ADT.0000000000000225
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 58
Pearson, C., Janz, T., & Ali, J. (2013). Mental and substance use disorders in Canada. Ottawa, Ont.:
Statistics Canada.
Pettigrew, S., Booth, L., Jongenelis, M. I., Brennan, E., Chikritzhs, T., Hasking, P., … Wakefield, M.
(2021). A randomized controlled trial of the effectiveness of combinations of ‘why to reduce’ and
‘how to reduce’ alcohol harm-reduction communications. Addictive Behaviors, 121, Article
107004. https://doi.org/10.1016/j.addbeh.2021.107004
Public Health Ontario. (2017a). Alcohol: Awareness and knowledge of Canada’s Low Risk Drinking
Guidelines (LRDG) [infographic].
https://www.publichealthontario.ca/-
/media/Documents/A/2017/alcohol-lrdg.pdf?sc_lang=en
Public Health Ontario. (2017b). Alcohol: Awareness of alcohol-related health risks and support for
health and nutrition labels [infographic].
https://www.publichealthontario.ca/-
/media/Documents/A/2017/alcohol-health-risks-labels.pdf?sc_lang=en .
Regier, L., & Jensen, B. (2021). Substance use disorder (SUD)/addiction: Overview & tx
considerations. https://www.rxfiles.ca/rxfiles/uploads/documents/CHT-Substance-Abuse.pdf
Rehm, J., Gmel, G. E., Sr., Gmel, G., Hasan, O. S. M., Imtiaz, S., Popova, S., … Shuper, P. A. (2017)
The relationship between different dimensions of alcohol use and the burden of disease—an
update. Addiction, 112(6), 968–1001. https://doi.org/10.1111/add.13757
Rehm, J., Lachenmeier, D. W., & Room, R. (2014). Why does society accept a higher risk for alcohol
than for other voluntary or involuntary risks? BMC Medicine, 12, Article 189.
https://doi.org/10.1186/s12916-014-0189-z
Roerecke, M., Kaczorowski, J., Tobe, S. W., Gmel, G., Hasan, O., & Rehm, J. (2017). The effect of a
reduction in alcohol consumption on blood pressure: A systematic review and meta-analysis.
Lancet Public health, 2(2), e108–e120. https://doi.org/10.1016/S2468-2667(17)30003-8
Roerecke, M., & Rehm, J. (2010). Irregular heavy drinking occasions and risk of ischemic heart
disease: a systematic review and meta-analysis. American Journal of Epidemiology, 171(6),
633–644. https://doi.org/10.1093/aje/kwp451
Roerecke, M., & Rehm, J. (2014). Alcohol consumption, drinking patterns, and ischemic heart
disease: a narrative review of meta-analyses and a systematic review and meta-analysis of the
impact of heavy drinking occasions on risk for moderate drinkers. BMC Medicine, 12, 182.
https://doi.org/10.1186/s12916-014-0182-6
Roerecke, M., Vafaei, A., Hasan, O. S. M., Chrystoja, B. R., Cruz, M., Lee, R., Neuman, M. G., & Rehm,
J. (2019). Alcohol consumption and risk of liver cirrhosis: A systematic review and meta-Analysis.
American Journal of Gastroenterology, 114(10), 1574–1586.
https://doi.org/10.14309/ajg.0000000000000340
Samokhvalov, A. V., Irving, H. M., & Rehm, J. (2010a). Alcohol consumption as a risk factor for
pneumonia: A systematic review and meta-analysis. Epidemiology and Infection, 138(12), 1789–
1795. https://doi.org/10.1017/S0950268810000774
Samokhvalov, A. V., Irving, H., Mohapatra, S., & Rehm, J. (2010b). Alcohol consumption, unprovoked
seizures, and epilepsy: A systematic review and meta-analysis. Epilepsia, 51(7), 1177–1184.
https://doi.org/10.1111/j.1528-1167.2009.02426.x
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 59
Samokhvalov, A. V., Rehm, J., & Roerecke, M. (2015). Alcohol consumption as a risk factor for acute
and chronic pancreatitis: A systematic review and a series of meta-analyses. eBioMedicine,
2(12), 1996–2002. https://doi.org/10.1016/j.ebiom.2015.11.023
Santé publique France & Institut national du cancer. (2017). Avis d’experts relatif à l'évolution du
discours public en matière de consommation d'alcool en France. Saint-Maurice: Santé publique
France.
https://www.santepubliquefrance.fr/les-actualites/2017/avis-d-experts-relatif-a-l-
evolution-du-discours-public-en-matiere-de-consommation-d-alcool-en-france-organise-par-sante-
publique-france-et-l-insti
Schoueri‐Mychasiw, N., Weerasinghe, A., Stockwell, T., Vallance, K., Hammond, D., Greenfield, T. K.,
McGavock, J., & Hobin, E. (2021). Use as directed: do standard drink labels on alcohol
containers help consumers drink (ir) responsibly? Real‐world evidence from a quasi‐
experimental study in Yukon, Canada. Drug and Alcohol Review, 40(2), 247–257.
https://doi.org/10.1111/dar.13165
Schünemann, H., Brożek, J., Guyatt, G., & Oxman, A. (2013) GRADE handbook for grading quality of
evidence and strength of recommendations.
http://gdt.guidelinedevelopment.org/app/handbook/handbook.html
Shaheen, A.A., Kong, K., Ma, C., Doktorchik, S., Coffin, C.S., Swain, M.G., Burak, K.W., … Abraldes,
J.G. (2022). Impact of the COVID-19 pandemic on hospitalizations for alcoholic hepatitis or
cirrhosis in Alberta, Canada. Clinical Gastroenterology and Hepatology, 20(5), e1170–e1179.
https://doi.org/10.1016/j.cgh.2021.10.030
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., … Henry, D. A. (2017).
AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-
randomised studies of healthcare interventions, or both. BMJ, 358.
https://doi.org/10.1136/bmj.j4008
Sherk, A., Thomas, G., Churchill, S., & Stockwell, T. (2020). Does drinking within low-risk guidelines
prevent harm? Implications for high-income countries using the International Model of Alcohol
Harms and Policies. Journal of Studies on Alcohol and Drugs, 81(3), 352–361.
https://doi.org/10.15288/jsad.2020.81.352
Spear, L.P. (2018). Effects of adolescent alcohol consumption on the brain and behaviour. Nature
Review Neuroscience, 19(4), 197–214. https://doi.org/10.1038/nrn.2018.10
Stahre, M., Naimi, T., Brewer, R., & Holt, J. (2006). Measuring average alcohol consumption: The
impact of including binge drinks in quantity–frequency calculations. Addiction, 101(12), 1711–
1718. https://doi.org/10.1111/j.1360-0443.2006.01615.x
Starr, C. (1969). Social benefit versus technological risk: What is our society willing to pay for safety?
Science, 165(3899), 1232–1238. https://doi.org/10.1126/science.165.3899.1232
Statistics Canada. (2021). Table 13-10-0096-11 Heavy drinking, by age group.
https://doi.org/10.25318/1310009601-eng
Stockwell, T., Butt, P., Beirness, D., Gliksman, L., & Paradis, C. (2012). The basis for Canada’s new
low-risk drinking guidelines: A relative risk approach to estimating hazardous levels and patterns
of alcohol use. Drug Alcohol Review, 31(2), 126–134.
https://doi.org/10.1111/j.1465-
3362.2011.00342.x
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 60
Stockwell, T., Priore, B., Churchill, S., Goulet-Stock, S., Naimi, T., Sherk, A., Shield, K., & Zhao, J.
(2022, May 30–June 3). Calling time on low-risk drinking guidelines: An evaluation of alternative
methods to communicate risks of alcohol use to consumers. 47th Annual Alcohol Epidemiology
Symposium of the Kettil Bruun Society, Warsaw, Poland.
Stockwell, T., Zhao, J., Sherk, A., Rehm, J., Shield, K., & Naimi, T. (2018). Underestimation of alcohol
consumption in cohort studies and implications for alcohol's contribution to the global burden of
disease. Addiction. 113(12), 2245–2249. https://doi.org/10.1111/add.14392
Sun, Q., Xie, W., Wang, Y., Chong, F., Song, M., Li, T., Xu, L., & Song, C. (2020). Alcohol consumption
by beverage type and risk of breast cancer: A dose-response meta-analysis of prospective cohort
studies. Alcohol and Alcoholism, 55(3), 246–253. https://doi.org/10.1093/alcalc/agaa012
Sundell, L., Salomaa, V., Vartiainen, E., Poikolainen, K., & Laatikainen, T. (2008). Increased stroke
risk is related to a binge-drinking habit. Stroke, 39(12), 3179–3184.
https://doi.org/10.1161/STROKEAHA.108.520817
Taylor, B., Irving, H. M., Kanteres, F., Room, R., Borges, G., Cherpitel, C., Greenfield, T., & Rehm, J.
(2010). The more you drink, the harder you fall: A systematic review and meta-analysis of how
acute alcohol consumption and injury or collision risk increase together. Drug and Alcohol
Dependence, 110(1-2), 108–116. https://doi.org/10.1016/j.drugalcdep.2010.02.011
Taylor, B., & Rehm, J. (2012). The relationship between alcohol consumption and fatal motor vehicle
injury: High risk at low alcohol levels. Alcoholism, Clinical and Experimental Research, 36(10),
1827–1834. https://doi.org/10.1111/j.1530-0277.2012.01785.x
Thaler, R. H., & Sunstein, C. R. (2008). Nudge: Improving decisions about health, wealth, and
happiness. New Haven, Connecticut: Yale University Press.
Thomas, G., Poole, N., Greaves, L., Bialystok, L., & Dell, C. (2014). Patterns of alcohol use among
women of childbearing years in Canada: Implications for FASD prevention. Toronto, Ont.: Public
Health.
Thomes, P. G., Rasineni, K., Saraswathi, V., Kharbanda, K. K., Clemens, D. L., Sweeney, S. A., …
Casey, C. A. (2021). Natural recovery by the liver and other organs after chronic alcohol use.
Alcohol Research: Current Reviews, 41(1), Article 05. https://doi.org/10.35946/arcr.v41.1.05
Thunderbird Partnership Foundation. (2015). The native wellness assessment. Bothwell, Ont.:
Author. https://thunderbirdpf.org/about-tpf/scope-of-work/native-wellness-assessment/
U.K. Chief Medical Officers. (2016). UK Chief Medical Officers’ Low Risk Drinking Guidelines.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_dat
a/file/545937/UK_CMOs__report.pdf
Vallance, K., Stockwell, T., Wettlaufer, A., Chow, C., Giesbrecht, N., April, N., … Thompson, K. (2021).
The Canadian Alcohol Policy Evaluation project: Findings from a review of provincial and
territorial alcohol policies. Drug and Alcohol Review, 40(6), 937–945.
https://doi.org/10.1111/dar.13251
Vernooij, R. W. M., Sanabria, A. J., Solà, I., Alonso-Coello, P., & Martínez García, L. (2014). Guidance
for updating clinical practice guidelines: A systematic review of methodological handbooks.
Implementation Science, 9(1), Article 3. https://doi.org/10.1186/1748-5908-9-3
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 61
Verrill, C., Markham, H., Templeton, A., Carr, N. J., & Sheron, N. (2009). Alcohol-related cirrhosis—
early abstinence is a key factor in prognosis, even in the most severe cases. Addiction, 104(5),
768–774. https://doi.org/10.1111/j.1360-0443.2009.02521.x
Vieira, A. R., Abar, L., Chan, D., Vingeliene, S., Polemiti, E., Stevens, C., Greenwood, D., & Norat, T.
(2017). Foods and beverages and colorectal cancer risk: a systematic review and meta-analysis
of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project.
Annals of Oncology, 28(8), 1788–1802. https://doi.org/10.1093/annonc/mdx171
Vinson, D. C., Maclure, M., Reidinger, C., & Smith, G. S. (2003). A population-based case-crossover
and case-control study of alcohol and the risk of injury. Journal of Studies on Alcohol, 64(3),
358–366. https://doi.org/10.15288/jsa.2003.64.358
Voas, R. B., Torres, P., Romano, E., & Lacey, J. H. (2012). Alcohol-related risk of driver fatalities: An
update using 2007 data. Journal of Studies on Alcohol and Drugs, 73(3), 341–350.
https://doi.org/10.15288/jsad.2012.73.341
Voskoboinik, A., Kalman, J. M., De Silva, A., Nicholls, T., Costello, B., Nanayakkara, S., … Kistler, P. M.
(2020). Alcohol abstinence in drinkers with atrial fibrillation. New England Journal of Medicine,
382(1), 20–28. https://doi.org/10.1056/NEJMoa1817591
Wagenaar, A. C., Salois, M. J., & Komro, K. A. (2009). Effects of beverage alcohol price and tax levels
on drinking: a meta-analysis of 1003 estimates from 112 studies. Addiction, 104(2), 179–190.
https://doi.org/10.1111/j.1360-0443.2008.02438.x
Wagenaar, A. C., Tobler, A. L., & Komro, K. A. (2010). Effects of alcohol tax and price policies on
morbidity and mortality: a systematic review. American Journal of Public Health 100, 2270–
2278. https://doi.org/10.2105/AJPH.2009.186007
Wakefield, M. A., Brennan, E., Dunstone, K., Durkin, S. J., Dixon, H. G., Pettigrew, S., & Slater, M. D.
(2018). Immediate effects on adult drinkers of exposure to alcohol harm reduction
advertisements with and without drinking guideline messages: Experimental study. Addiction,
113(6), 1019–1029. https://doi.org/10.1111/add.14147
Wechsler, H., & Austin, S. B. (1998). Binge drinking: the five/four measure. Journal of Studies on
Alcohol, 59(1), 122–124. https://doi.org/10.15288/jsa.1998.59.122
Weerasinghe, A., Schoueri-Mychasiw, N., Vallance, K., Stockwell, T., Hammond, D., McGavock, J., …
Hobin, E. (2020). Improving knowledge that alcohol can cause cancer is associated with
consumer support for alcohol policies: Findings from a real-world alcohol labelling study.
International Journal of Environmental Research and Public Health, 17(2), Article 398.
https://doi.org/10.3390/ijerph17020398
Wettlaufer, A. (2018). Can a label help me drink in moderation? A review of the evidence on
standard drink labelling. Substance Use & Misuse, 53(4), 585–595.
https://doi.org/10.1080/10826084.2017.1349798
White, A. J., DeRoo, L. A., Weinberg, C. R., & Sandler, D. P. (2017). Lifetime alcohol intake, binge
drinking behaviors, and breast cancer risk. American Journal of Epidemiology, 186(5), 541–549.
https://doi.org/10.1093/aje/kwx118
Whiting, P., Davies, P., Savović, J., Caldwell, D., & Churchill, R. (2013). Evidence to inform the
development of ROBIS, a new tool to assess the risk of bias in systematic reviews. Bristol, U.K.:
School of Social and Community Medicine, University of Bristol.
https://www.bristol.ac.uk/media-
library/sites/social-community-medicine/robis/ROBIS%20Report%204_9.pdf
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 62
World Cancer Research Fund International. (2018). Diet, nutrition, physical activity and cancer: a
global perspective. London, U.K.: Author.
https://www.wcrf.org/diet-activity-and-cancer/global-
cancer-update-programme/table-of-contents/
World Health Organization. (2021). Global Information System on Alcohol and Health.
https://www.who.int/data/gho/data/themes/global-information-system-on-alcohol-and-health
World Health Organization. (2022). Alcohol: Fact sheet. https://www.who.int/en/news-room/fact-
sheets/detail/alcohol
Wu, X., Liu, X., Liao, W., Kang, N., Dong, X., Abdulai, T., … Li, Y. (2021). Prevalence and
characteristics of alcohol consumption and risk of type 2 diabetes mellitus in rural China. BMC
Public Health, 21(1), Article 1644. https://doi.org/10.1186/s12889-021-11681-0
Zhao, J., Stockwell, T., Roemer, A., Naimi, T., & Chikritzhs, T. (2017). Alcohol consumption and
mortality from coronary heart disease: An updated meta-analysis of cohort studies. Journal of
Studies on Alcohol and Drugs, 78(3), 375–386. https://doi.org/10.15288/jsad.2017.78.375
Zhao, J., Stockwell, T., & Thomas, G. (2015). An adaptation of the Yesterday Method to correct for
under-reporting of alcohol consumption and estimate compliance with Canadian low-risk drinking
guidelines. Canadian Journal of Public Health, 106(4), e204–e209.
https://doi.org/10.17269/cjph.106.4753

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 63
Appendix 1: Lifetime Risk of Alcohol-Attributable
Death and Disability: Shadow Analysis
Purpose
To inform decisions regarding the formation of Canadian drinking guidelines, a primary analysis was
performed whose results were a collection of risk relationships that estimated the risk of death and
disability as a function of average daily alcohol use by those who live in Canada.
Toward ensuring accuracy of the primary analysis, this shadow analysis process was designed and
undertaken. The general objective of a shadow analysis is for the main and shadow analysts to come
together and share the desired project input and broad methodology. The two analyses are
conducted independently, in parallel, and results are compared to ensure accuracy of the primary
collection of results.
Method
The primary and shadow researchers met several times to discuss strategy and determine raw input
that would be shared by both analyses. Shared inputs were as follows:
• Relative risk function definitions: Each alcohol-attributable condition considered was assigned a
dose–response relative risk function, and the source and definition of these risk functions was
shared. Relative risk functions were prepared by the primary researcher.
• Prevalence and consumption data: Raw survey data for Canada was transformed into total and
relative population alcohol consumption, where relevant population strata were sex and age.
Prevalence and consumption data were prepared by the primary researcher.
• Deaths, years lived with disability, and incidence in the population, by condition: Raw data were
aggregated and summarized into alcohol-attributable condition categories for each outcome
category. Death data was prepared by the primary researcher and also the shadow researcher.
Years lived with disability and incidence were prepared by the primary researcher.
The two analysts discussed the broad methodologies. The implementation of the lifetime risk
methodology was then performed in R in both the primary and shadow analyses. Researchers wrote
their scripts and/or packages independently. Primary and shadow analysis results were compared
with an eye toward whether differences would have an impact on the quantitative guidelines
endeavour.
Summary of the Comparison of Findings
The shadow analysis is a very near-match with the primary analysis, with differences accounted for
by expected, random differentials in the model-building exercise, the random draws employed
throughout the process and slight differences in methodological choices between analysts. Small
differences between the shadow analyses and the primary analysis
are not expected to lead to
differences in interpretations of results for the quantitative guidelines endeavour.
Figures 1 and 2 compare the results of the primary and shadow analyses. Figure 1 displays lifetime
deaths per 1,000 people at each level of consumption up to an average of 100 g ethanol/day.
Figure 2 displays the same statistic on the range of up to an average of 40 g ethanol/day. In each
figure, the results of the primary analysis (and associated 95% confidence intervals [CIs]) are shown
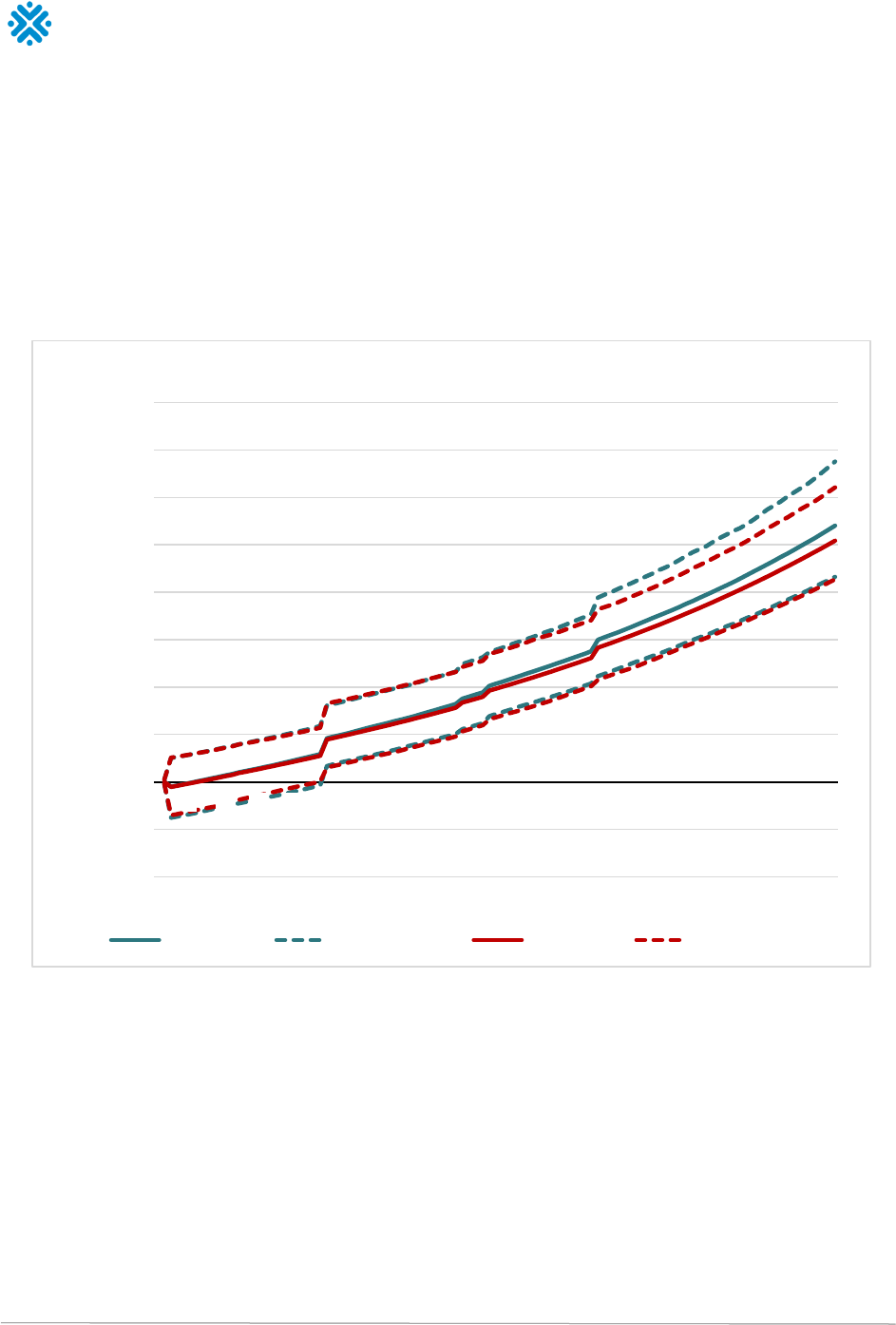
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 64
in red and the shadow analyses in blue. In Figure 2, it is clear that the shadow analysis produced
results that would not lead to substantive differences in interpretation when designing alcohol use
guidelines for people who live in Canada. A high similarity between the shadow and primary analysis
is observed for all levels of average daily alcohol use, and in particular the match is near-perfect at
levels of average daily alcohol use below 50 g ethanol/ day. This behaviour is consistent throughout
the remainder of the shadow results, distributed separately.
Figure 1: Visual comparison between primary results and shadow results in the category of male death, range of
average consumption of from 1 to 100 g ethanol/day
-100
-50
0
50
100
150
200
250
300
350
400
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Lifetime deaths
per 1000 people
Average alcohol intake (grams /day)
Shadow analysis - Male Deaths
Shadow PE Shadow 95% CI Primary PE Primary 95% CI
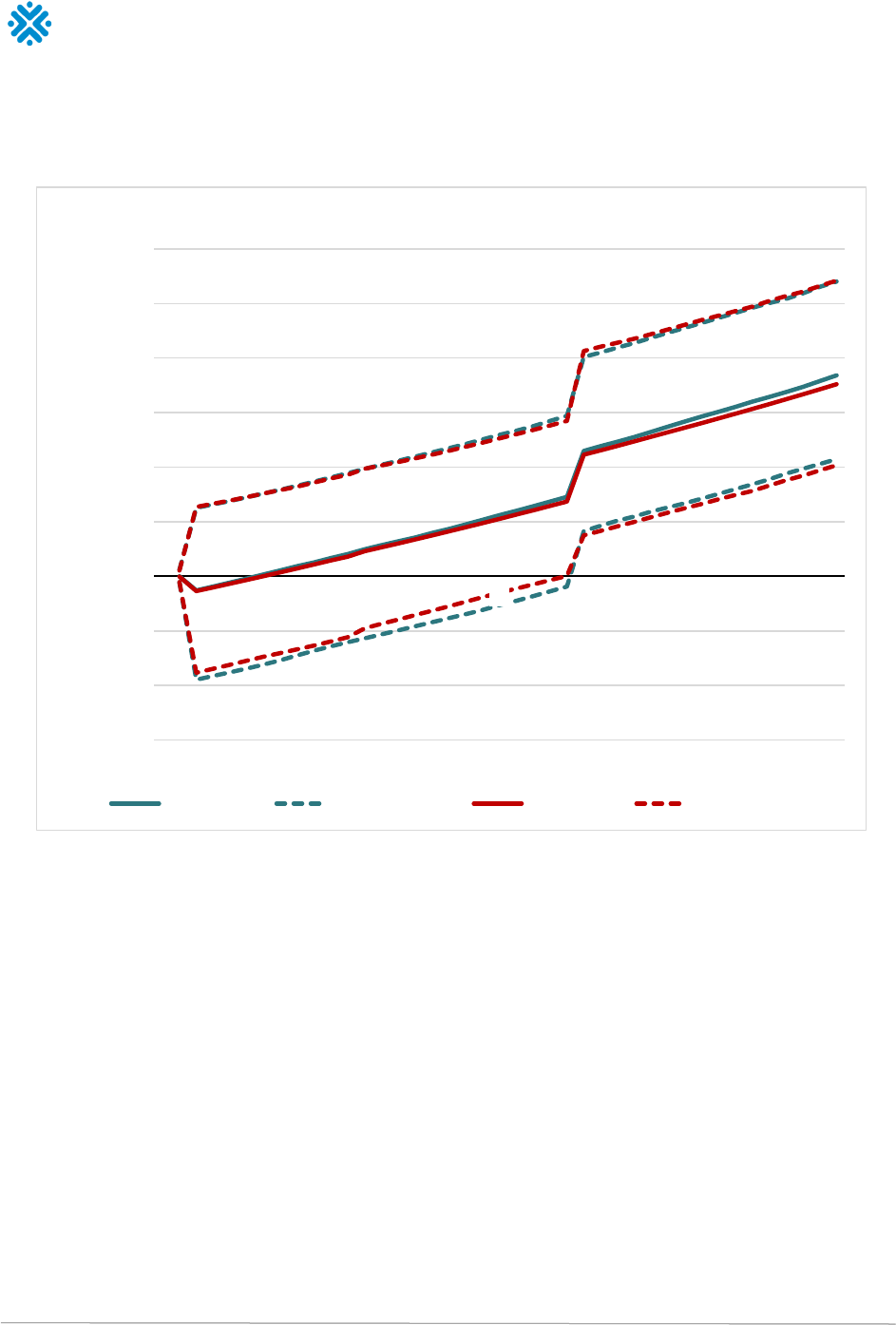
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 65
Figure 2: Visual comparison between primary results and shadow results in the category of male death, range of
average consumption of from 1 to 40 g ethanol/day
-60
-40
-20
0
20
40
60
80
100
120
0 5 10 15 20 25 30 35 40
Lifetime deaths
per 1000 people
Average alcohol intake (grams /day)
Shadow analysis - Male Deaths
Shadow PE Shadow 95% CI Primary PE Primary 95% CI
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 66
Appendix 2: Confidence Intervals for Risk of Disease and Injury
Table 1. Increased risk of diseases and injuries, with 95% confidence intervals, for females, based on average daily alcohol use
Condition or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 1.04
(1.01, 1.07)
1.07
(1.01, 1.14)
1.11
(1.02, 1.21)
1.15
(1.03, 1.29)
1.20
(1.03, 1.38)
1.24
(1.04, 1.47)
1.26
(1.04, 1.52)
1.62
(1.09, 2.38)
2.05
(1.14, 3.61)
3.33
(1.25, 8.60)
Lower respiratory
infections
1.01
(1.00, 1.02)
1.02
(1.00, 1.03)
1.03
(1.01, 1.05)
1.04
(1.01, 1.07)
1.05
(1.01, 1.09)
1.06
(1.01, 1.10)
1.06
(1.01, 1.11)
1.14
(1.03, 1.25)
1.21
(1.04, 1.39)
1.38
(1.07, 1.74)
Oral cavity and pharynx
cancer
1.05
(1.04, 1.06)
1.10
(1.09, 1.12)
1.16
(1.13, 1.18)
1.22
(1.18, 1.25)
1.28
(1.23, 1.31)
1.34
(1.28, 1.39)
1.37
(1.31, 1.42)
1.89
(1.74, 2.04)
2.52
(2.24, 2.80)
4.38
(3.68, 5.15)
Oesophagus cancer 1.03
(1.03, 1.03)
1.05
(1.05, 1.06)
1.08
(1.08, 1.09)
1.11
(1.11, 1.12)
1.14
(1.13, 1.15)
1.17
(1.16, 1.18)
1.19
(1.18, 1.20)
1.43
(1.40, 1.45)
1.69
(1.64, 1.74)
2.39
(2.28, 2.50)
Colorectal cancer 1.01
(1.01, 1.02)
1.03
(1.02, 1.04)
1.04
(1.03, 1.05)
1.06
(1.04, 1.07)
1.07
(1.05, 1.09)
1.08
(1.06, 1.11)
1.09
(1.06, 1.12)
1.20
(1.14, 1.26)
1.31
(1.21, 1.42)
1.57
(1.38, 1.79)
Liver cancer 1.01
(1.00, 1.01)
1.02
(1.01, 1.02)
1.02
(1.01, 1.04)
1.03
(1.02, 1.05)
1.04
(1.02, 1.06)
1.05
(1.02, 1.07)
1.05
(1.03, 1.08)
1.11
(1.05, 1.17)
1.17
(1.08, 1.26)
1.30
(1.14, 1.48)
Breast cancer 1.02
(1.01, 1.02)
1.04
(1.03, 1.05)
1.06
(1.04, 1.07)
1.08
(1.06, 1.09)
1.10
(1.07, 1.12)
1.12
(1.09, 1.15)
1.13
(1.09, 1.16)
1.28
(1.21, 1.36)
1.44
(1.32, 1.57)
1.84
(1.60, 2.14)
Larynx cancer 1.03
(1.02, 1.04)
1.06
(1.04, 1.07)
1.09
(1.07, 1.11)
1.12
(1.09, 1.15)
1.16
(1.11, 1.19)
1.19
(1.14, 1.24)
1.21
(1.15, 1.26)
1.46
(1.34, 1.59)
1.74
(1.54, 1.95)
2.43
(2.02, 2.91)
Pancreatitis 0.95
(0.91, 0.99)
0.90
(0.82, 0.98)
0.85
(0.74, 0.98)
0.81
(0.68, 0.97)
0.77
(0.62, 0.97)
0.74
(0.58, 0.97)
0.73
(0.56, 0.97)
0.79
(0.53, 1.21)
1.15
(0.69, 1.94)
2.74
(1.05, 7.47)
Diabetes Mellitus 0.85
(0.80, 0.89)
0.80
(0.75, 0.86)
0.77
(0.71, 0.84)
0.75
(0.68, 0.83)
0.73
(0.65, 0.82)
0.72
(0.63, 0.81)
0.71
(0.63, 0.80)
0.66
(0.56, 0.78)
0.65
(0.53, 0.80)
0.67
(0.52, 0.86)
Liver cirrhosis 1.61
(1.51, 1.72)
1.94
(1.77, 2.12)
2.24
(2.00, 2.50)
2.53
(2.23, 2.87)
2.82
(2.44, 3.24)
3.11
(2.66, 3.61)
3.25
(2.76, 3.81)
5.45
(4.30, 6.82)
7.85
(5.90, 10.32)
14.37
(9.92, 20.47)
Atrial fibrillation and
flutter
1.01
(1.01, 1.02)
1.03
(1.02, 1.03)
1.04
(1.03, 1.05)
1.05
(1.04, 1.07)
1.07
(1.05, 1.08)
1.08
(1.06, 1.10)
1.09
(1.07, 1.11)
1.19
(1.14, 1.24)
1.29
(1.22, 1.38)
1.54
(1.39, 1.71)
Hypertension 1.01
(1.00, 1.02)
1.02
(1.00, 1.04)
1.04
(1.01, 1.06)
1.05
(1.01, 1.09)
1.06
(1.01, 1.11)
1.07
(1.02, 1.12)
1.08
(1.03, 1.13)
1.16
(1.06, 1.26)
1.25
(1.12, 1.39)
1.45
(1.20, 1.74)
Ischemic heart disease 0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
1.04
(0.81, 1.34)
1.04
(0.81, 1.34)
1.15
([0.86, 1.52)
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 67
Ischemic stroke 0.90
(0.85, 0.95)
0.90
(0.85, 0.95)
0.90
(0.85, 0.95)
0.90
(0.85, 0.95)
0.90
(0.85, 0.95)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
1.08
(1.01, 1.16)
1.08
(1.01, 1.16)
1.14
(1.01, 1.28)
Intracerebral
hemorrhage
0.92
(0.77, 1.10)
0.92
(0.77, 1.10)
0.92
(0.77, 1.10)
0.92
(0.77, 1.10)
0.92
(0.77, 1.10)
0.99
(0.83, 1.19)
0.99
(0.83, 1.19)
1.25
(0.92, 1.69)
1.25
(0.92, 1.69)
1.67
(1.26, 2.25)
Subarachnoid
haemorrhage
1.21
(0.48, 3.06)
1.21
(0.48, 3.06)
1.21
(0.48, 3.06)
1.21
(0.48, 3.06)
1.21
(0.48, 3.06)
1.11
(0.33, 3.90)
1.11
(0.33, 3.90)
1.39
(0.32, 5.94)
1.39
(0.32, 5.94)
1.82
(0.38, 10.12)
Epilepsy 1.03
(1.02, 1.04)
1.06
(1.04, 1.07)
1.08
(1.06, 1.10)
1.11
(1.08, 1.14)
1.14
(1.10, 1.17)
1.17
(1.13, 1.21)
1.18
(1.14, 1.23)
1.40
(1.30, 1.51)
1.64
(1.46, 1.84)
2.29
(1.89, 2.76)
Road injuries 1.02
(1.01, 1.03)
1.04
(1.02, 1.06)
1.06
(1.03, 1.09)
1.08
(1.04, 1.13)
1.10
(1.04, 1.16)
1.12
(1.05, 1.20)
1.13
(1.06, 1.21)
1.30
(1.12, 1.50)
1.47
(1.19, 1.82)
1.90
(1.34, 2.73)
Other unintentional
injuries
1.02
(1.01, 1.02)
1.03
(1.02, 1.04)
1.05
(1.03, 1.06)
1.06
(1.05, 1.08)
1.08
(1.06, 1.10)
1.10
(1.07, 1.13)
1.11
(1.07, 1.14)
1.23
(1.16, 1.31)
1.36
(1.25, 1.49)
1.68
(1.45, 1.95)
Intentional injuries 1.05
(1.04, 1.06)
1.10
(1.08, 1.13)
1.16
(1.12, 1.20)
1.22
(1.17, 1.28)
1.28
(1.21, 1.36)
1.35
(1.26, 1.44)
1.38
(1.29, 1.49)
1.96
(1.69, 2.28)
2.71
(2.17, 3.39)
5.32
(3.66, 7.73)
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 68
Table 2. Increased risk of diseases and injuries, with 95% confidence intervals, for males, based on average daily alcohol use
Condition or injury
1
2
3
4
5
6
7
14
21
35
Tuberculosis 1.04
(1.01, 1.07)
1.07
(1.02, 1.14)
1.11
(1.02, 1.21)
1.15
(1.03, 1.30)
1.20
(1.04, 1.38)
1.24
(1.05, 1.48)
1.26
(1.05, 1.52)
1.62
(1.11, 2.40)
2.05
(1.17, 3.66)
3.33
(1.30, 8.77)
Lower respiratory infections 1.01
(1.00, 1.02)
1.02
(1.00, 1.04)
1.03
(1.01, 1.05)
1.04
(1.01, 1.07)
1.05
(1.01, 1.09)
1.06
(1.01, 1.11)
1.06
(1.01, 1.12)
1.14
(1.03, 1.27)
1.21
(1.04, 1.42)
1.38
(1.07, 1.80)
Oral cavity and pharynx cancer 1.05
(1.04, 1.06)
1.10
(1.09, 1.12)
1.16
(1.14, 1.18)
1.22
(1.19, 1.25)
1.28
(1.24, 1.32)
1.34
(1.29, 1.39)
1.37
(1.32, 1.43)
1.89
(1.75, 2.06)
2.52
(2.25, 2.83)
4.38
(3.69, 5.19)
Oesophagus cancer 1.03
(1.03, 1.03)
1.05
(1.05, 1.06)
1.08
(1.08, 1.09)
1.11
(1.10, 1.12)
1.14
(1.13, 1.15)
1.17
(1.16, 1.18)
1.19
(1.18, 1.20)
1.43
(1.40, 1.46)
1.69
(1.64, 1.74)
2.39
(2.28, 2.51)
Colorectal cancer 1.01
(1.01, 1.02)
1.03
(1.02, 1.04)
1.04
(1.03, 1.05)
1.06
(1.04, 1.07)
1.07
(1.05, 1.09)
1.08
(1.06, 1.11)
1.09
(1.07, 1.12)
1.20
(1.15, 1.26)
1.31
(1.22, 1.41)
1.57
(1.40, 1.79)
Liver cancer 1.01
(1.00, 1.01)
1.02
(1.01, 1.02)
1.02
(1.01, 1.04)
1.03
(1.02, 1.05)
1.04
(1.02, 1.06)
1.05
(1.02, 1.07)
1.05
(1.03, 1.08)
1.11
(1.06, 1.17)
1.17
(1.08, 1.26)
1.30
(1.14, 1.48)
Breast cancer 1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
Larynx cancer 1.03
(1.02, 1.04)
1.06
(1.04, 1.07)
1.09
(1.07, 1.11)
1.12
(1.09, 1.15)
1.16
(1.11, 1.20)
1.19
(1.14, 1.24)
1.21
(1.15, 1.26)
1.46
(1.33, 1.59)
1.74
(1.53, 1.97)
2.43
(2.03, 2.94)
Pancreatitis 1.04
(1.02, 1.05)
1.07
(1.04, 1.10)
1.11
(1.06, 1.16)
1.15
(1.08, 1.22)
1.19
(1.10, 1.28)
1.23
(1.12, 1.34)
1.25
(1.13, 1.38)
1.60
(1.30, 1.94)
2.00
(1.47, 2.67)
3.20
(1.91, 5.17)
Diabetes Mellitus 1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.00)
1.00
(1.00, 1.01)
1.00
(1.00, 1.01)
1.00
(0.99, 1.01)
1.00
(0.99, 1.01)
1.01
(0.98, 1.05)
1.02
(0.97, 1.09)
1.06
(1.01, 1.11)
Liver cirrhosis 1.06
(1.05, 1.07)
1.12
(1.11, 1.14)
1.19
(1.16, 1.22)
1.26
(1.22, 1.30)
1.33
(1.28, 1.38)
1.40
(1.34, 1.47)
1.44
(1.38, 1.52)
2.14
(1.94, 2.37)
3.07
(2.66, 3.57)
6.53
(5.13, 8.41)
Atrial fibrillation and flutter 1.01
(1.01, 1.02)
1.03
(1.02, 1.03)
1.04
(1.03, 1.05)
1.05
(1.04, 1.06)
1.07
(1.05, 1.08)
1.08
(1.06, 1.10)
1.09
(1.07, 1.11)
1.19
(1.14, 1.24)
1.29
(1.21, 1.37)
1.54
(1.38, 1.69)
Hypertension 1.03
(1.02, 1.04)
1.06
(1.03, 1.08)
1.09
(1.05, 1.13)
1.12
(1.07, 1.17)
1.15
(1.09, 1.22)
1.17
(1.10, 1.24)
1.17
(1.11, 1.25)
1.29
(1.21, 1.40)
1.36
(1.27, 1.48)
1.47
(1.37, 1.60)
Ischemic heart disease 0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
0.95
(0.75, 1.21)
1.04
(0.81, 1.34)
1.04
(0.81, 1.34)
1.15
([0.86, 1.52)
Ischemic stroke 0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
0.92
(0.87, 0.97)
1.08
(1.02, 1.15)
1.08
(1.02, 1.15)
1.14
(1.01, 1.27)
Intracerebral hemorrhage 0.92
(0.78, 1.11)
0.92
(0.78, 1.11)
0.92
(0.78, 1.11)
0.92
(0.78, 1.11)
0.92
(0.78, 1.11)
0.99
(0.82, 1.19)
0.99
(0.82, 1.19)
1.25
(0.93, 1.68)
1.25
(0.93, 1.68)
1.67
(1.24, 2.22)
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 69
Condition or injury
1
2
3
4
5
6
7
14
21
35
Subarachnoid haemorrhage 1.21
(0.51, 2.81)
1.21
(0.51, 2.81)
1.21
(0.51, 2.81)
1.21
(0.51, 2.81)
1.21
(0.51, 2.81)
1.11
(0.32, 4.00)
1.11
(0.32, 4.00)
1.39
(0.25, 6.42)
1.39
(0.25, 6.42)
1.82
(0.32, 10.36)
Epilepsy 1.03
(1.02, 1.04)
1.06
(1.04, 1.07)
1.08
(1.07, 1.10)
1.11
(1.09, 1.14)
1.14
(1.11, 1.17)
1.17
(1.13, 1.21)
1.18
(1.14, 1.23)
1.40
(1.31, 1.52)
1.64
(1.48, 1.85)
2.29
(1.93, 2.78)
Road injuries 1.03
(1.02, 1.04)
1.06
(1.05, 1.07)
1.09
(1.07, 1.11)
1.12
(1.10, 1.15)
1.16
(1.12, 1.20)
1.19
(1.15, 1.24)
1.21
(1.16, 1.26)
1.49
(1.37, 1.62)
1.80
(1.60, 2.04)
2.68
(2.19, 3.30)
Other unintentional injuries 1.02
(1.01, 1.02)
1.03
(1.02, 1.04)
1.05
(1.03, 1.06)
1.06
(1.05, 1.08)
1.08
(1.06, 1.10)
1.10
(1.07, 1.13)
1.11
(1.08, 1.14)
1.23
(1.16, 1.31)
1.36
(1.25, 1.49)
1.68
(1.45, 1.95)
Intentional injuries 1.05
(1.04, 1.06)
1.10
(1.08, 1.13)
1.16
(1.12, 1.20)
1.22
(1.17, 1.28)
1.28
(1.21, 1.36)
1.35
(1.26, 1.44)
1.38
(1.28, 1.48)
1.96
(1.68, 2.27)
2.71
(2.16, 3.38)
5.32
(3.63, 7.67)

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 70
Appendix 3: Specific Messages for Girls and
Women to Supplement the Guidance on Alcohol
and Health
It is important for girls and women to know:
• There are risks of alcohol use for both men and women, but it is not a level playing field, as
alcohol affects women’s bodies more negatively
• Alcohol is processed by women’s bodies differently, causing more negative health effects, earlier,
after lesser amounts of alcohol
• Women become intoxicated faster after drinking less than men due to smaller bodies and
organs, less body water, hormonal effects, and different enzyme actions that break down alcohol
• Alcohol has more serious health effects on females than males, due to body size, body fat/water
ratio, hormonal effects and differing actions of enzymes that break down alcohol
• Alcohol consumption increases risk of breast cancer, a very common cancer in Canadian women
• Women experience more liver injuries on lower levels of alcohol, compared to men
It is also important for girls and women to know:
• Perpetrators of sexual assault often target someone who has been drinking alcohol or is
intoxicated
• Women often use alcohol to cope with the stress of trauma, intimate partner violence and
caregiving, which can lead to poorer, not better health
• Girls and women with histories of childhood abuse progress more quickly from starting to drink to
becoming alcohol dependent
And some ideas for the pregnancy-related messages:
• Alcohol use in pregnancy negatively affects both women’s and fetal health
• There is no safe level of alcohol use in pregnancy, so it is safest not to drink at all while pregnant
• The more alcohol consumed, the greater the risk of harm for women’s and fetal health
• Alcohol use in pregnancy especially when combined with poor nutrition and tobacco use can
result in infant death, birth defects, and lifelong behavioural and cognitive problems
• Alcohol use in pregnancy can increase the risk of miscarriage.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 71
Appendix 4: Update of Canada’s Low-Risk Alcohol
Drinking Guidelines: Open Consultation
A total of 886 completed submissions for the open consultation on the update of Canada’s Low-Risk
Alcohol Drinking Guidelines were received. Respondents were mostly individuals who are concerned
about the effects of alcohol use on themselves, their family or their friends (75.3%). Others identified
themselves as professionals who use alcohol guidelines in their work (15%) or as representatives of
an organization (4.7%). Five percent of the respondents preferred not to disclose this information.
Among respondents, 746 indicated they would like to answer questions related to the public
summary, 377 indicated they would like to answer questions related to the technical summary and
307 mentioned they would like to answer questions related to the technical report.
Public Summary
Please indicate how strongly you agree with the following statement: The Public Summary is clear,
simple, and easy to understand.
Level of agreement
Frequency
Percent
Strongly agree 276 37.0
Agree 311 41.7
Neither agree nor disagree 63 8.4
Disagree 55 7.4
Strongly disagree 31 4.2
Prefer not to answer 10 1.3
Total 746 100.0
Technical Summary
Please indicate how strongly you agree with the following statement: The Technical Summary is
clear, simple, and easy to understand.
Level of agreement
Frequency
Percent
Strongly agree 111 29.4
Agree 171 45.4
Neither agree nor disagree 51 13.5
Disagree 20 5.3
Strongly disagree 15 4.0
Prefer not to answer 9 2.4
Total 377 100.0
Please indicate how strongly you agree with the following statement: The information presented in
the
Technical Summary is likely to make people reconsider their alcohol drinking habits.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 72
Level of agreement
Frequency
Percent
Strongly agree 73 19.4
Agree 146 38.7
Neither agree nor disagree 88 23.3
Disagree 35 9.3
Strongly disagree 22 5.8
Prefer not to answer 13 3.4
Total 377 100.0
Please indicate how strongly you agree with the Technical Summary’s Policy Implications.
Level of agreement
Frequency
Percent
Strongly agree 140 37.1
Agree 117 31.0
Neither agree nor disagree 44 11.7
Disagree 32 8.5
Strongly disagree 30 8.0
Prefer not to answer 14 3.7
Total 377 100.0
Technical Report
Takeaway 1: All levels of alcohol consumption are associated with some risk, so drinking less is
better for everyone.
Please indicate how strongly you agree with takeaway 1.
Level of agreement
Frequency
Percent
Strongly agree 166 54.1
Agree 77 25.1
Neither agree nor disagree 21 6.8
Disagree 16 5.2
Strongly disagree 21 6.8
Prefer not to answer 6 2.0
Total 307 100.0
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 73
Takeaway 2: There is a continuum of risk whereby the risk for those who consume 2 standard drinks
or less per week is negligible to low; it is moderate for those who consume between 3 and 6
standard drinks per week; and it is high for those who consume more than 6 standard drinks per
week, with increasingly higher levels of risk with every additional drink.
Please indicate how strongly you agree with takeaway 2.
Level of agreement
Frequency
Percent
Strongly agree 129 42.0
Agree 83 27.0
Neither agree nor disagree 34 11.1
Disagree 30 9.8
Strongly disagree 25 8.1
Prefer not to answer 6 2.0
Total 307 100.0
Takeaway 3: On any occasion, any level of consumption has risks, and with more than two standard
drinks, most individuals will have an increased risk of injuries or other problems.
Please indicate how strongly you agree with takeaway 3.
Level of agreement
Frequency
Percent
Strongly agree 126 41.0
Agree 85 27.7
Neither agree nor disagree 39 12.7
Disagree 29 9.4
Strongly disagree 23 7.5
Prefer not to answer 5 1.6
Total 307 100.0
Takeaway 4: Disproportionately more injuries, violence and deaths result from men’s drinking.
Please indicate how strongly you agree with takeaway 4.
Level of agreement
Frequency
Percent
Strongly agree 151 49.2
Agree 88 28.7
Neither agree nor disagree 27 8.8
Disagree 14 4.6
Strongly disagree 18 5.9
Prefer not to answer 9 2.9
Total 307 100.0
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 74
Takeaway 5: Above low levels of alcohol consumption, the health risks increase more steeply for
women than for men.
Please indicate how strongly you agree with takeaway 5.
Level of agreement
Frequency
Percent
Strongly agree 122 39.7
Agree 83 27.0
Neither agree nor disagree 55 17.9
Disagree 18 5.9
Strongly disagree 19 6.2
Prefer not to answer 10 3.3
Total 307 100.0
Takeaway 6: It is safest to not drink while pregnant and during the preconception period.
Please indicate how strongly you agree with takeaway 6.
Level of agreement
Frequency
Percent
Strongly agree 219 71.3
Agree 57 18.6
Neither agree nor disagree 16 5.2
Disagree 3 1.0
Strongly disagree 5 1.6
Prefer not to answer 7 2.3
Total 307 100.0
Takeaway 7: For women who are breastfeeding, it is safest not to use alcohol.
Please indicate how strongly you agree with takeaway 7.
Level of agreement
Frequency
Percent
Strongly agree 188 61.2
Agree 78 25.4
Neither agree nor disagree 20 6.5
Disagree 7 2.3
Strongly disagree 5 1.6
Prefer not to answer 9 2.9
Total 307 100.0

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 75
Public Consultation: Summary of Key Actions Taken
The responses received from the open consultation were analyzed and categorized. The table below
presents the main categories of comments as well as the actions taken by the LRDG-Scientific Expert
Panel (LRDG-SEP) to address comments which fell within the scope of this project’s mandate.
There were several suggestions made for knowledge mobilization activities, including knowledge
synthesis, dissemination, transfer and exchange. These suggestions have been recorded but are not
listed here as they could not be considered for action (i.e., could not lead to edits and revisions of
the final report).
Consultation comment or suggestion
Action taken
Public Summary
Provide more information about specific cancers. There are already many consequences of different types
presented in the public summary, the suggested
consequences were not added. However, the public
summary was edited to link the average amount of weekly
use with examples consequences.
In general, some respondents want to see more statistics. The objective of the document is to communicate
information without statistics that would need contextual
information and more explanations to be easily
understood. No statistics were added.
Explain and provide a graphic about the effect of alcohol
on the body.
Adding this information would require including
information that would be too detailed for a public
summary.
Mention that alcohol is an addictive substance. The focus of the public summary is on low- and moderate-
risk alcohol drinking.
In general, some respondents want to see different social
harms mentioned going beyond one own’s health.
Mention of social harms added in the public summary.
Mention of consequences for others added as well.
Clearly show the cumulative and long-term effects. Rephrasing done to show the cumulative effects of the
consequences. Information about long-term small
amounts not included for lack of space.
Mention the consequences of binge drinking vs having
drinks across the week.
No mention on binge drinking but a highlighted statement
added stating do not drink more than two drinks on one
occasion.
Mention the social aspect of drinking. Out of scope for this summary.
Emphasize sobriety and its benefits. Information about the benefits of not drinking or reduced
consumption has been added in the document.
More emphasis on specific consequences related to the
number of drinks.
The consequences of drinking are now paired with the
number of drinks in the graphic. Colours used to show the
continuum will be emphasized to make this information
even clearer.
Mention the risk of dying for a young person so young
people feel concerned.
There is already a mention that alcohol can shorten one’s
life.
Present clearly what are safe amount. The colours on the continuum are adjusted to avoid
indicating that 1 to 2 drinks per week is not without risk.
Specifically, a hint of yellow is added in the circled
numbers under 1 and 2 drinks.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 76
Consultation comment or suggestion
Action taken
Respondents mention wanting to see other consequences:
State clearly that there is no protective effect to alcohol.
The public summary was comprehensively edited to link
the average amount of weekly use with examples
consequences.
Include more information about alcohol use and
reproductive health.
It was decided to maintain the focus of the summary on
pregnancy and to put more emphasis on zero alcohol
during pregnancy.
Request for a gender-inclusive language. The content was rephrased to be more gender inclusive.
Provide information about different types of alcoholic
beverages, their specific effects and their ingredients.
No information about specific products was added.
People requested clarification on what is a standard drink. The word “standard” was added whenever relevant.
Mention if lifestyle factors and predispositions influence
the causality between alcohol use and consequences.
Information added in the content mentioning that lifestyle
does not prevent alcohol caused consequences.
Many comments are about the guidelines in relation to
various socio-demographic variables.
The content already mentions that the consequences are
the same regardless of age, gender, sex or lifestyle.
Some respondents want more tips to reduce drinking. A clear and highlighted statement about not drinking more
than two drinks per occasion will be included in the public
summary. Tips will remain in the summary.
Add a tool or a link to help cut down drinking. It is not possible to include a tracking tool in the public
summary.
There were mixed feelings about the main title. The main title was revised.
Some respondents criticized the use of “we.” When relevant, the pronoun “we” was removed.
Some respondents would like more white space. The text was reduced and the graphic and the
“Consequences” section were combined, which reduces
visual overload.
Some respondent expressed concerns about the way the
drinks, the various levels of risks and the consequences
were presented.
The image and colours depicting the continuum of risk
have been modified.
Respondents made different comments about the layout
and made suggestions about highlighting specific
information.
Layout was reorganized to combine the graphic and the
“Consequences” section.
Some respondents mentioned that the font was a bit too
small, and the resolution was poor.
This will not be an issue when the document is in a poster
size.
Technical Summary
Some submissions requested additional information and
specifications.
The technical summary was entirely revised with additional
statistics, information and sections.
Some submissions noted some contradictions between
key messages.
The key messages have been revised.
Some submissions requested greater clarity about the
thresholds.
The section on the risks associated with weekly levels of
alcohol use has been clarified.
Takeaway 1:
All levels of alcohol consumption are associated with some risk, so drinking less is better for everyone.
Several submissions queried clarity and nuances. This takeaway has been modified into a more nuanced
message that better reflects the complexity of the issue.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 77
Consultation comment or suggestion
Action taken
Takeaway 2:
There is a continuum of risk whereby the risk for those who consume 2 standard drinks or less per week is
negligible to low; it is moderate for those who consume between 3 and 6 standard drinks per week; and it is high for
those who consume more than 6 standard drinks per week, with increasingly higher levels of risk with every additional
drink.
Some submissions mentioned that the terms used in the
continuum of risk were misleading.
The takeaway has been revised and the term “negligible”
has been removed.
Some requested a clearer figure to accompany the
takeaway.
The format, the design and the colours of the figure
presented in the public summary and the technical
summary have been modified.
Make this statement more clear, concise and to the point. The takeaway and the accompanying text have been
revised to provide more clarity.
Some requested more details about the evidence behind
this takeaway.
No action required. The evidence and details about the
methodology used to develop this takeaway are available
in the technical report and the background report
available here:
Lifetime Risk of Alcohol-Attributable Death and Disability
https://ccsa.ca/lifetime-risk-alcohol-attributable-death-
and-disability-report
Takeaway 3:
On any occasion, any level of consumption has risks, and with more than two standard drinks, most
individuals will have an increased risk of injuries or other problems.
Requires simplifying and specifying. Takeaway has been revised with greater emphasis on per
occasion alcohol use and the fact that the risk for harm is
to oneself and others.
Takeaway 4:
Disproportionately more injuries, violence and deaths result from men’s drinking.
Some statistics comparing men and women’s alcohol-
related outcomes requested.
Statistics were added throughout.
Requires clarifying the pattern of alcohol use. This takeaway has been moved into a sex and gender box
that specifies that it is especially in the case of per
occasion drinking that far more harms result from men’s
alcohol use.
Some submissions queried Information about factors that
can influence alcohol use and its impact such as motives
for drinking, context, personality traits, socialization, the
pandemic, etc.
No action required. This is out of scope for the mandate.
Other gender-related harms from alcohol could be
considered and noted (e.g., sexual violence, domestic and
gender-based violence).
No action required. The report includes a section on the
association between alcohol use, aggression and violence.
For the “Association Between Alcohol Use, Aggression and
Violence,” it should be noted that alcohol is not the unique
cause of violence.
A paragraph acknowledging aggravating factor has been
added to the section of the report on the association
between alcohol use, aggression and violence.
A submission raised concerns about creating a victim
blaming dynamic.
This section of the report was reviewed by two of the
LRDG-SEP members with expertise in this area. Special
attention will be given to this concern when knowledge
mobilization activities are developed.
Takeaway 5:
Above low levels of alcohol consumption, the health risks increase more steeply for women than for men
Provide more details and statistics showing the
differences between men and women.
Statistics were added in the technical report.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 78
Consultation comment or suggestion
Action taken
Men and women should not be compared and the term
"everyone" should be used instead.
No action required. This request does not reflect current
scientific knowledge as alcohol use has sex- and gender
specific risks.
Requires clarifying low levels and the type of risks. This statement has been moved into a sex and gender box
that specifies that it is above the upper limit of the
moderate risk zone for alcohol consumption that the
health risks increase more steeply more women.
Takeaway 6:
It is safest to not drink while pregnant and during the preconception period
This statement is not inclusive and needs to speak to
other genders (i.e., people who are pregnant).
The report has been revised to avoid sex or gender
specific statements.
One submission suggested the promotion of early
pregnancy awareness.
No action required. Out of scope.
The term "preconception period" needs to be defined.
The term has been replaced with “planning to be
pregnant.”
The wording of this statement should be strengthened and
simplified.
The statement now specifies that there is no known safe
amount of alcohol use.
FASD should be mentioned. The fact that FASD can be a consequence of alcohol use
when pregnant is now clearly stated.
The conclusion ignores the benefits of alcohol
consumption on women who are pregnant (e.g., stress
reduction, decreased blood pressure).
The research questions that guided this project were
formulated to encompass all effects, so that studies
focusing on both positive and negative effects could be
identified. The recommendations do not include the
benefits because overall results of systematic reviews did
not show a significant beneficial effect even at low levels
of alcohol use.
Takeaway should address the impact of alcohol use on
male reproductive capacity.
No action required. No high-quality systematic review has
been found to support this claim.
Clarify what studies were used to come up with this
statement.
A detailed account and description of studies that form the
basis of this statement are available here:
Sex, Gender and Alcohol: What Matters for Women in Low-
Risk Drinking Guidelines?
https://ccsa.ca/sites/default/files/2022-08/CCSA-LRDG-
Sex-Gender-and-Alcohol-what-matters-for-Women-in-
LRDGs-en.pdf
Information on how to minimize the risk if women choose
to drink should be provided.
This report aims to review evidence to update the LRDGs.
Harm reduction tips will be the focus of eventual
knowledge mobilization activities.
Takeaway 7:
For women who are breastfeeding, it is safest not to use alcohol
Sentence should be adjusted to reflect that babies do
metabolize alcohol.
The report now accurately states that babies are “less
able” instead of “unable” to metabolize alcohol.
The benefits of alcohol consumption are missing. The research questions that guided this project were
formulated to encompass all effects, so that studies
focusing on both positive and negative effects could be
identified. The recommendations do not include the
benefits because overall, results of systematic reviews did
not show a significant beneficial effect even at low levels
of alcohol use.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 79
Consultation comment or suggestion
Action taken
The message should be improved by adding information
about how long alcohol stays in the breastmilk.
The message has been revised with additional information
regarding the time it takes for alcohol to leave the body
and breastmilk.
Overall Comments for the entire report
Some submissions requested more details about the
increased risk according to the number of standard drinks.
All tables and statistics throughout the report were revised
to present risk according to standard drinks.
Submissions queried more information about absolute risk
and years of life lost per specific cause of death.
To aid readers to better understand risk, tables with
cause-specific risk of death have been added (see tables
3 and 4).
One submission queried why the J shaped curve is
obsolete.
A specification was added to the technical report.
A comparison of the health risks between people who
consume alcohol to those who do not should be added.
No action required. The information is presented in the
technical report (tables 1 and 2), which describes the
increased percentage risk of diseases and injuries of
people who use alcohol compared to lifetime abstainers
(i.e., those who have never consumed alcohol).
There should be a "zero limit" section. The report now includes a section listing circumstances
when no alcohol use is the safest.
One submission asked for more information about which
specific risk curves were retrieved from meta-analyses and
how they were used.
We have added a footnote to Table 1 of the document
“Lifetime Risk of Alcohol-Attributable Death and Disability”
to indicate source of this relative risk function.
Some submissions queried risk curves based on the
frequency of drinking.
A sentence was added to the document “Lifetime Risk of
Alcohol-Attributable Death and Disability” noting the
absence of reliable evidence on how abstinence days
increase or decrease people’s risk of alcohol-attributable
disease.
The quality of the evidence (i.e., GRADE) should be
reported.
A paragraph about the quality of the evidence was added
to the technical report.
Submissions found it difficult to understand where the
threshold of 17.5 years of life comes from when the rest of
the text speaks of 1 in 100 or 1,000.
An explanation was added noting how the risk thresholds
of 17.5 YLLs in 100 and 1,000 lifetimes were derived.
Some submissions questioned how the risk zones were
named.
A reference has been added.
One submission requested clarification on how the CCMTA
data were reworked to create the risk curves.
A reference on the process of creating relative risk curves
from CCMAT BAC data was added to the document
“Lifetime Risk of Alcohol-Attributable Death and Disability.”
Some submissions requested clarification about the non-
protective effects of alcohol use on heart disease.
Throughout the report, text has been edited to better
reflect the nuances of the results on this topic.
One submission requested a clarification as to why two
specific studies used to revise the Australian alcohol
guidelines (Patra et al, 2010; Yang et al, 2016) were not
used here.
No action required. Patra et al. (2010) was replaced by
Larsson et al. (2016), which is of equal quality (as
assessed by GRADE) and more recent. Yang et al. (2016)
was replaced by Zhao et al. (2017), which is of higher
quality (as assessed by GRADE) and more recent.
One submission requested references on the
mathematical modelling methods.
All models are based on peer-reviewed methodology and
are cited in the document “Lifetime Risk of Alcohol-
Attributable Death and Disability.”
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 80
Consultation comment or suggestion
Action taken
A submission questioned the quality of the data on death,
disability and alcohol exposure that were used in the
modelling.
No action required. Only original public data files were
used for both the original modelling analyses and the
shadow analyses.
The use of controlled correlational prospective studies
does not allow to eliminate several alternative
explanations and limitations (e.g., publication bias and the
fact that studies focus little on the beneficial effects of
alcohol).
Causality for all diseases included and excluded from the
analyses were determined based on recent animal,
mechanistic and epidemiological evidence, which taken
together allow elimination of alternative explanations.
Moreover, all relative risks were assessed for bias through
the GRADE criteria.
One submission questioned methodological decision
(inflation of self-reported alcohol use, restrictive selection
of risk curves for certain diseases), which may have
contributed to an overestimation of the risk associated
with low levels of alcohol use.
First, correction of population survey for under-reporting
was done based on peer-reviewed studies cited in the
report. Second, the relative risks obtained from systematic
reviews were not adjusted for misestimation of alcohol
use. Although there is hypothesized to be a slight
underestimation of alcohol use in medical epidemiology
studies, the direction of alcohol use measurement bias in
cohort studies is unknown. We have added a note to the
technical report acknowledging this limitation.
The methodological limitations and uncertainties need to
be reported.
A limitation section has been added to the final report.
Provide an explanation as to why only systematic reviews
were included.
As per GRADE guidelines.
Some submissions noted that the recommendations were
too general and should consider other individual factors
and special populations.
This report aims to provide general recommendations to
the general population. This consideration will be taken
into the knowledge mobilization phase of this project,
when resources will be dedicated to the development of
messaging that speaks directly to the unique concerns of
people with diverse backgrounds and personal
experiences.
There should be a clear numerical recommendation. Key takeaways have been revised for clarity. However,
considering the results obtained through this project, the
experts have agreed that instead of providing people with
strict rules and recommendations, people should be
presented with a continuum of risk.
Some requested that the information in the report should
be presented by age group.
The experts agreed to adopt a lifetime approach to alcohol
use, which is much more in alignment with the way people
consume alcohol throughout the lifetime. For example,
people do not start to drink at 45 or 65 years old. We have
added a sentence to the document “Lifetime Risk of
Alcohol-Attributable Death and Disability” justifying the use
of the lifetime approach based on empirical studies of life
course alcohol use.
Provide an explanation as to why the binge-drinking
amounts have not changed.
Revisiting the definition of binge-drinking is out of scope of
the mandate. Moreover, the definition remains relevant in
other contexts and for other types of interventions.
The recommendation should address the benefits of
alcohol consumption.
The research questions that guided this project were
formulated to encompass all effects, so that studies
focusing on both positive and negative effects could be
identified. The recommendations do not include the
benefits because overall, our model did not show a
significant beneficial effect even at low levels of alcohol use.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 81
Consultation comment or suggestion
Action taken
Some submissions requested stronger message that no
drinking is the only safe option, others queried messaging
that alcohol is as important as abstinence, while others
requested less abstinence-oriented messages.
The language was revised throughout the report to be
more nuanced.
While there is acknowledgment that sex and gender are
different, women/females and men/males seem to be
used interchangeably in some contexts that are referring
to physiological risks. If the statement refers to sex
assigned at birth use the terms "males" and "females."
Throughout the report, text has been reviewed to clarify
the biological (sex) and social concepts (gender). A note on
terminology was added to the report.
The report is gender-biased and needs to be more
inclusive of other genders.
Throughout this project, there has been a commitment to
integrate sex-, gender- and diversity-based analysis
(SGBA+). However, sex and gender science is nascent, the
literature incomplete, and many effects and impacts of sex
and gender on alcohol use, especially among sub-
populations such as Indigenous Peoples, older people,
sexual minorities and gender minorities, remain under-
researched or unknown. The experts recognize that it will
be important for people with various sex and gender
identities to find themselves in the Guidance. As such, it
will be crucial for the knowledge mobilization phase of this
project to create resources that speak to gender or
sexually diverse populations.
Request to remove the policy implications section.
The policy implications are evidence-based. They are
included in the report as they suggest a path forward to
increase awareness and support people who may want to
follow the Guidance on Alcohol and Health.
A more specific definition of a standard drink should be
reported in the beginning of the report.
A definition of a standard drink was added at the
beginning of the report and an image was added to the
technical summary.
Some submissions queried the impacts of alcohol use
among youth.
This is a limitation that is now mentioned in the concluding
part of the report. The message that youth under the legal
drinking age should delay drinking as much as possible
has also been added.
Provide more statistics on how many people die from
alcohol-related diseases and experience health issues due
to alcohol consumption, as well as the cost to the health
care system.
More references and statistics were added throughout the
report.
A discussion around the changes in outcomes if reducing
alcohol consumption should be added.
A paragraph in the technical report devoted to this issue
has been enhanced.
A discussion around mental health (e.g., depression
suicide) and social (e.g., loneliness, isolation) risks is
needed.
The experts commissioned a review on this topic. Effect of
Alcohol Consumption on the Development of Depression,
Anxiety and Suicidal Ideation: Update of a Systematic
Review is available here:
https://ccsa.ca/effect-alcohol-
consumption-development-depression-anxiety-and-
suicidal-ideation-update-systematic. The final report
provides a summary and presents the limitations and
implications of the review.
Some submissions requested a greater focus on harm
reduction.
This project was based on the principle of autonomy in
harm reduction, and this has now been made clearer. The
public summary highlights safer drinking tips.

Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 82
Consultation comment or suggestion
Action taken
Request for a mention of evidence-based treatment
available for alcohol use disorder and that people should
see their doctor for more information on treatment options
A note was added in the report.
Some submissions queried the impact of alcohol on the
brain.
The project’s focus has been on the risk relationships
between alcohol use and the occurrence of and mortality
from all disease or injury categories causally related to
alcohol consumption and for which high quality systematic
reviews were available.
One submission requested more precision about province-
specific data.
Details and precisions have been added throughout the
report.
Some submissions requested more consultations and co-
construction of messages with stakeholders.
The public was invited to provide input o
n two separate
occasions. Representatives from different health-related
organizations were invited to discuss ideal messaging and
communication strategies. It is hoped that the conclusions
of the update will be useful to experts and partners who
should work together to create interventions and
messaging that will speak directly to the unique concerns
of people with diverse backgrounds and personal
experiences.
Specify where to find the evidence from which the
recommendations are derived.
A figure was revised. Links to all background reports are
available in that figure and throughout the document.
A submission questioned the decision to include three
documents in the final report.
Three documents were designed to meet the needs of as
many people as possible. The three documents were
designed with particular audiences in mind but are not
restricted to the intended audiences.
One submission requested focus on responsible safer use
rather than low-risk guidance.
The experts agreed that presenting a continuum of risk
associated with various levels of alcohol use should allow
people to situate themselves where they are on that
continuum and understand in which risk zone their alcohol
use places them. It is hoped that this will lead people to
develop intentions to adopt healthier and safer
behaviours.
General typographical or grammatical errors and
formatting suggestions.
Numerous grammatical, formatting and typographical
edits were made to improve the clarity of the report.
A total of 19 articles were submitted as evidence to be considered for mathematical modelling. None
of the submitted evidence was retained; the reasons are presented in the table below.
Articles submitted to be included as evidence
Action taken
Bryazka, D., Reitsma, M. B., Griswold, M. G., Abate, K. H., Abbafati, C.,
Abbasi- Kangevari, M., ... & Diress, M. (2022). Population-level risks of
alcohol consumption by amount, geography, age, sex, and year: a
systematic analysis for the Global Burden of Disease Study 2020. The
Lancet, 400(10,347), 185–235. https://doi.org/10.1016/S0140-
6736(22)00847-9
This article was excluded at step 2 of the
screening process as it failed to meet at
least two of the methodological quality
criteria. The characteristics of the included
studies were not reported, and the quality
of the included studies was not assessed.
Daviet, R., Aydogan, G., Jagannathan, K., Spilka, N., Koellinger, P.D.,
Kranzler, H.R., Nave, G., Wetherill, R.R. (2022). Associations between
alcohol consumption and gray and white matter volumes in the UK
Biobank. Nature Communications, 13(1), Article 1175.
https://doi.org/10.1038/s41467-022-28735-5
Not a systematic review.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 83
Articles submitted to be included as evidence
Action taken
Demoury, C., Karakiewicz, P., & Parent, M. E. (2016). Association
between lifetime alcohol consumption and prostate cancer risk: A case-
control study in Montreal, Canada. Cancer Epidemiology, 45, 11–17.
https://doi.org/10.1016/j.canep.2016.09.004
Not a systematic review.
Leong, C., Bolton, J. M., Ekuma, O., Prior, H. J., Singal, D., Nepon, J.,
Konrad, G., Paille, M., Finlayson, G., & Nickel, N. (2022). Association of
alcohol use disorder on alcohol-related cancers, diabetes, ischemic heart
disease and death: A population-based, matched cohort study. Addiction,
117, 368–381. https://doi.org/10.1111/add.15646
Not a systematic review.
Ma, H., Li, X., Zhou, T., Sun, D., Shai, I., Heianza, Y., Rimm, E. B., Manson,
J. E., & Qi, L. (2021). Alcohol consumption levels as compared with
drinking habits in predicting all-cause mortality and cause-specific
mortality in current drinkers. Mayo Clinic proceedings, 96(7), 1758–
1769. https://doi.org/10.1016/j.mayocp.2021.02.011
Not a systematic review.
Marcus, G. M., Vittinghoff, E., Whitman, I. R., Joyce, S., Yang, V., Nah, G.,
Gerstenfeld, E. P., Moss, J. D., Lee, R. J., Lee, B. K., Tseng, Z. H.,
Vedantham, V., Olgin, J. E., Scheinman, M. M., Hsia, H., Gladstone, R.,
Fan, S., Lee, E., Fang, C., … Hahn, J. A. (2021). Acute consumption of
alcohol and discrete atrial fibrillation events. Annals of Internal Medicine,
174(11), 1503–1509. https://doi.org/10.7326/M21-0228
Not a systematic review.
McIntosh, J. (2017). Alcohol and Canadian health. Global Journal of
Health Science, 9(5), 96-104. https://doi.org/10.5539/gjhs.v9n5p96
Not a systematic review.
McIntosh, J. (2019). The truth about alcohol and health. European
Journal of Medical and Health Sciences, 1(2).
https://doi.org/10.24018/ejmed.2019.1.2.35
Not a systematic review.
Mørch, L. S., Johansen, D., Thygesen, L. C., Tjønneland, A., Løkkegaard,
E., Stahlberg, C., & Grønbaek, M. (2007). Alcohol drinking, consumption
patterns and breast cancer among Danish nurses: A cohort study.
European Journal of Public Health, 17(6), 624–629.
https://doi.org/10.1093/eurpub/ckm036
Not a systematic review.
Patra, J., Taylor, B., Irving, H., Roerecke, M., Baliunas, D., Mohapatra, S.,
& Rehm, J. (2010). Alcohol consumption and the risk of morbidity and
mortality for different stroke types--a systematic review and meta-
analysis. BMC Public Health, 10, Article 258.
https://doi.org/10.1186/1471-2458-10-258
The study on stroke by Larsson et al.
(2016) was included instead of the Patra
et al. (2010) study as it was more recent
and of similar quality as assessed by
GRADE.
Perreault, K., Bauman, A., Johnson, N., Britton, A., Rangul, V., &
Stamatakis, E. (2017). Does physical activity moderate the association
between alcohol drinking and all-cause, cancer and cardiovascular
diseases mortality? A pooled analysis of eight British population cohorts.
British Journal of Sports Medicine, 51(8), 651–657.
https://doi.org/10.1136/bjsports-2016-096194
Not a systematic review.
Schaefer, S. M., Kaiser, A., Behrendt, I., Eichner, G., & Fasshauer, M.
(2022). Association of alcohol types, coffee and tea intake with mortality:
prospective cohort study of UK Biobank participants. British Journal of
Nutrition, 1–11. Advance online publication.
https://doi.org/10.1017/S000711452200040X
Not a systematic review.
Van Heertum, K., & Rossi, B. (2017). Alcohol and fertility: How much is
too much?. Fertility Research and Practice, 3, 10.
https://doi.org/10.1186/s40738-017-0037-x
Not a systematic review.
Canada’s Guidance on Alcohol and Health: Final Report
Canadian Centre on Substance Use and Addiction • Centre canadien sur les dépendances et l’usage de substances Page 84
Articles submitted to be included as evidence
Action taken
Veldhuis, C. B., Hughes, T. L., Drabble, L., Wilsnack, S. C., Riggle, E., &
Rostosky, S. S. (2019). Relationship status and drinking-related
outcomes in a community sample of lesbian and bisexual women. Journal
of Social and Personal Relationships, 36(1), 244–268.
https://doi.org/10.1177/0265407517726183
Not a systematic review.
White, A. J., DeRoo, L. A., Weinberg, C. R., & Sandler, D. P. (2017).
Lifetime alcohol intake, binge drinking behaviors, and breast cancer risk.
American Journal of Epidemiology, 186(5), 541–549.
https://doi.org/10.1093/aje/kwx118
Not a systematic review.
White, H. R., Fite, P., Pardini, D., Mun, E.-Y., & Loeber, R. (2013).
Moderators of the dynamic link between alcohol use and aggressive
behavior among adolescent males. Journal of Abnormal Child Psychology,
41(2), 211–222. https://doi.org/10.1007/s10802-012-9673-0
Not a systematic review.
Willett, W. C., Stampfer, M. J., Colditz, G. A., Rosner, B. A., Hennekens, C.
H., & Speizer, F. E. (1987). Moderate Alcohol Consumption and the Risk
of Breast Cancer. New England Journal of Medicine, 316(19), 1174–
1180. https://doi.org/10.1056/NEJM198705073161902
Not a systematic review.
Wood, A. M., Kaptoge, S., Butterworth, A. S., Willeit, P., Warnakula, S.,
Bolton, T., Paige, E., Paul, D. S., Sweeting, M., Burgess, S., Bell, S., Astle,
W., Stevens, D., Koulman, A., Selmer, R. M., Verschuren, W. M. M., Sato,
S., Njølstad, I., Woodward, M., … Danesh, J. (2018). Risk thresholds for
alcohol consumption: Combined analysis of individual-participant data for
599 912 current drinkers in 83 prospective studies. The Lancet,
391(10129), 1513–1523. https://doi.org/10.1016/S0140-
6736(18)30134-X
This article was excluded at step 2 of the
screening process as it failed to meet at
least two of the methodological quality
criteria. There was no comprehensive
search of the literature, the characteristics
for each of the included studies were not
reported, and the quality of the included
studies was not assessed.
Yang, Y., Liu, D. C., Wang, Q. M., Long, Q. Q., Zhao, S., Zhang, Z., Ma, Y.,
Wang, Z. M., Chen, L. L., & Wang, L. S. (2016). Alcohol consumption and
risk of coronary artery disease: A dose-response meta-analysis of
prospective studies. Nutrition, 32(6), 637–644.
https://doi.org/10.1016/j.nut.2015.11.013
The more recent study on ischaemic heart
disease by Zhao et al. (2017) was included
instead of the Yang et al. (2016) study as it
was of higher quality as assessed by
GRADE.
