A
SURVEY
AND
ANALYSIS
OF
TECHNIQUES
USED
IN
ATTRACTING
THE
BLACK
MIDDLE.CLASS
PATIENT
Sydney
Barnwell,
MD,
and
Walter
F.
LaMendola,
PhD
Greenville,
North
Carolina
This
study
presents
a
survey
which
is
based
upon
the
black
physician's
perception
of
the
expectations
of
the
black
middle-class
patient.
This
perception
is
that
the
middle-class
ex-
pectations
are
low;
hence,
satisfaction
is
low,
and
the
result
is
that
prospective
patients
tend
to
utilize
the
services
of
white
physi-
cians.
The
survey
was
designed
to
sample
opinions
of
physicians
attending
the
1983
an-
nual
meeting
of
the
National
Medical
Associ-
ation
in
Chicago,
and
it
determined
the
most
useful
techniques
in
attracting
black
middle-
class
patients.
These
investigators
believe
that
there
is
an
immediate
need
of
a
market-
concept
approach
utilizing
the
results
of
this
study
to
help
the
black
doctor
market
his
serv-
ices
more
effectively.
Such
a
market
concept
approach
is
presented.
Dr.
Barnwell
is
Assistant
Dean
for
Minority
Affairs
and
Dr.
Mendola
is
Associate
Professor,
Division
of
Social
Work,
School
of
Allied
Health
and
Social
Work,
East
Carolina
Uni-
versity.
Requests
for
reprints
should
be
addressed
to
Dr.
Sydney
Barnwell,
1709
Lincoin
Street,
New
Bern,
NC
28560.
Black
doctors
represent
2.6
percent
of
the
na-
tion's
physicians.
They
are
well-organized
and
well-represented
by
the
National
Medical
Associ-
ation.
In
this
changing
practice
environment
where
Diagnosis-Related
Groups
(DRGs),
Pro-
spective
Payment,
and
Preferred
Provider
Organi-
zations
(PPOs)
are
the
order
of
the
day,
the
black
physician
has
to
sharpen
his
competitive
edge
in
order
to
survive.
This
is
made
more
urgent
by
the
increasing
oversupply
of
physicians,
which
will
peak
by
the
end
of
this
decade.
These
pressures
make
it
critical
that
black
practitioners
make
use
of
market
concepts
in
order
to
alter
public
percep-
tion,
increase
the
likelihood
that
prospective
pa-
tients
will
choose
to
use
them,
and
positively
in-
fluence
middle-class
patient
satisfaction.
Four
types
of
independent
variables
relating
to
patient
satisfaction
have
been
studied
by
research-
ers.
These
are
patient
characteristics,
organiza-
tional
characteristics,
doctor-patient
interaction
characteristics,
and
the
physician's
sociodemo-
graphic
characteristics.
This
study
presents
a
sur-
vey
of
the
black
physician's
perception
of
the
expectations
of
the
black
middle-class
patient.
We
propose
a
fifth
type
of
independent
variable,
one
which
states
that
the
racial
characteristics
of
the
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,
1985
379
BLACK
MIDDLE-CLASS
PATIENTS
black
physician
tend
to
influence
negatively
the
black
middle-class
patient's
satisfaction
by
not
meeting
the
latter's
preconceived
expectation
of
quality.
INDEPENDENT
VARIABLES
RELATING
TO
PATIENT
SATISFACTION:
A
REVIEW
OF
THE
LITERATURE
Patient
characteristics
are
usually
discussed
in
terms
of
attitudes-expectations
and
sociodemo-
graphic
factors.
The
more
positive
the
attitude
about
a
given
service,
the
more
satisfied
the
pa-
tient
tends
to
be.I
The
patient's
sociodemographic
characteristics
(including
age,
sex, race,
religion,
education,
occupation,
income,
and
marital
status)
tend
to
be
more
equivocal;
these
do
not
consistent-
ly
affect
satisfaction.1
But
when
the
determinants
of
patient
satisfaction
in
the
sociodemographic
characteristics
of
fee-for-service
solo
practices
are
studied
against
large
prepaid
organized
groups,
there
is
one
consistent
finding,
and
that
is
that
upper-class
patients
are
not
satisfied
with
large
prepaid
organized
groups.2
Organizational
characteristic
determinants
show
that
patient
satisfaction
is
lower
in
large
pre-
paid
organized
groups
than
in
fee-for-service
solo
practices.3
The
doctor-patient
interaction
depends
largely
upon
the
quality
of
such
interaction
affecting
pa-
tient
satisfaction.
Patients
tend
to
be
more
satis-
fied
when
the
physician
is
concerned,
comforting,
and
communicates
openly.4'5
The
sociodemographic
characteristics
of
the
physician
are
very
important
when
patient
expec-
tations
are
studied
vis-a-vis
patient
satisfaction.
Ross
and
his
co-workers
have
shown
that
patients
"halve
expectations
concerning
physicians'
status
characteristics:
that
clients
have
images
not
just
of
what
a
physician
does,
but
of
who
a
physician
is."6
These
authors
have
also
shown
that
images
of
physician
status
characteristics
are
based
on
statistical
norms.
For
example,
patients
expect
doc-
tors to
be
middle-aged,
white
men.
The
mean
is
ac-
cepted
as
the
norm,
and
the
norm
is
equated
with
being
good
and
appropriate.
Thus,
we
expect
that
if
most
physicians
are
white,
middle-aged
men
from
status
backgrounds,
and
of
Protestant
or
Jewish
religions,
then
clients
will
expect
physicians
to
have
these
status
char-
acteristics.
When
these
expectations
are
not
met,
satis-
faction
will
be
low.6
The
review
of
the
literature
indicates
that
a
fifth
type
of
independent
variable-black
physician
in-
teraction
with
the
black
middle-class
patient-has
not
been
examined
as
a
potential
determinant
of
patient
satisfaction.
We
propose
that
the
image
of
the
black
physi-
cian
does
not
fit
the
"great
white
father
image"
as
far
as
the
black
middle-class
patient
is
concerned
and
that
the
physician
does
not
fit
the
norm
which
is
equated
with
the
good
and
the
appropriate.
Therefore,
black
middle-class
patients'
expecta-
tions
are
low
at
the
outset
and
satisfaction
remains
low,
causing
many
black
patients
to
seek
out
white
physicians.7
The
Lloyd
and
Johnson
study7
limits
itself
to
black
medical
alumni
and
compares
re-
sults
of
practicing
patterns
for
graduating
classes
from
1955-1970
and
1973-1975.
According
to
this
study,
the
first
subgroup,
in
their
private
prac-
tices,
takes
care
of
67
percent
black
patients,
while
the
second
subgroup
takes
care
of
77
percent.
When
the
economic
status
of
these
patients
is
studied,
the
results
demonstrate
that
the
tendency
towards
caring
for
patients
from
lower
socio-
economic
backgrounds
predominates,
with
only
6.8
percent
and
6.2
percent
of
the
patients,
re-
spectively,
considered
well-to-do.
NATURE
OF
THE
PROBLEM
Gunnar
Myrdal
identified
the
problem
quite
clearly
in
1944
when
he
wrote
that
"The
Negro
doctor,
in
the
main,
must
depend
on
Negro
pa-
tronage.
And
the
overwhelming
majority
of
both
the
white
and
the
Negro
patients
of
the
Negro
doc-
tor
are
poor.
8
Furthermore,
Myrdal
cited
Carter
G.
Woodson
who
estimated
the
proportion
of
Negro
trade
that
goes
to
the
Negro
doctor
to
be
60
percent.
Wood-
son
went
on
to
say
more
bluntly
that
"the
large
number
of
Negro
leaders
who
after
preaching
race
380
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,1985
BLACK
MIDDLE-CLASS
PATIENTS
patronage
and
even
boasting
of
our
competent
physicians
and
surgeons
as
proof
of
race
progress,
nevertheless
have
employed
white
surgeons
in
undergoing
operations."9
In
1969,
Michel
Richard10
published
a
well-
documented
study
which
examined
the
profes-
sional
experiences
of
98
doctors
practicing
in
New
York
City.
Richard
found
that
many
Negro
pa-
tients
and
Negro
doctors
were
in
unwitting
collu-
sion
to
send
Negro
patients
to
white
doctors.
A
quotation
from
this
work
bears
out
the
point:
Sadly
enough,
it
has
been
observed
that
black
patients
and
Negro
physicians
themselves
have
helped
to
hold
down
the
number
of
specialists.
In
the
past,
at
any
rate,
Negro
patients
preferred
white
specialists
because
they
believe
them
to
be
more
competent,
and
Negro
doctors
often
referred
their
black
patients
to
white
specialists
on
the
assumption
that
they
would
be
reluctant
to
see
such
patients
on
a
continuing
basis,
whereas
the
Negro
spe-
cialist
might
"steal"
them.10
Additionally,
Richard
gave
the
incomes
of
the
doctors,
and
observed
that
although
the
average
Negro
doctor
in
the
sample
received
a
higher
in-
come
than
the
average
American
citizen,
his
in-
come
was
much
smaller
than
that
of
the
average
white
doctor.
10
What
was
true
in
1934
and
1969
is
still
true
to-
day:
the
black
middle-class
has
a
great
tendency
to
gravitate
to
the
white
physician.
Patients
have
expectations
not
just
of
what
a
physician
does
but
of
who
a
physician
is;
these
expectations
influence
satisfaction.
These
problems
resolve
themselves
as
marketplace
problems
and
involve
managing
a
service
or
a
product
so
that
it
can
be
sold
to
cus-
tomers
(patients).
The
customer's
perception
is,
as
much
if
not,
more
important
than
the
actual
qual-
ity
of
the
product.
METHODOLOGY
A
survey
was
designed
to
sample
opinions
of
physicians
attending
the
annual
meeting
of
the
National
Medical
Association,
Chicago,
July
30-
August
4,
1983.
The
survey
was
constructed
in
two
steps.
First,
attendees
at
a
Region
III
meeting
of
the
National
Medical
Association
at
Jackson-
ville,
Florida,
June
23-26,
1983,
were
asked
to
con-
tribute
descriptions
of
techniques
they
used
to
attract
the
black
middle-class
patient.
The
20
re-
spondents
contributed
86
descriptions.
Second,
the
descriptions
were
grouped
by
three
judges
into
25
areas.
The
three
judges
included
a
black
physi-
cian,
a
social
scientist,
and
a
data
analyst.
The
25
areas
were
placed
on
the
survey
form
to
be
rated
by
respondents.
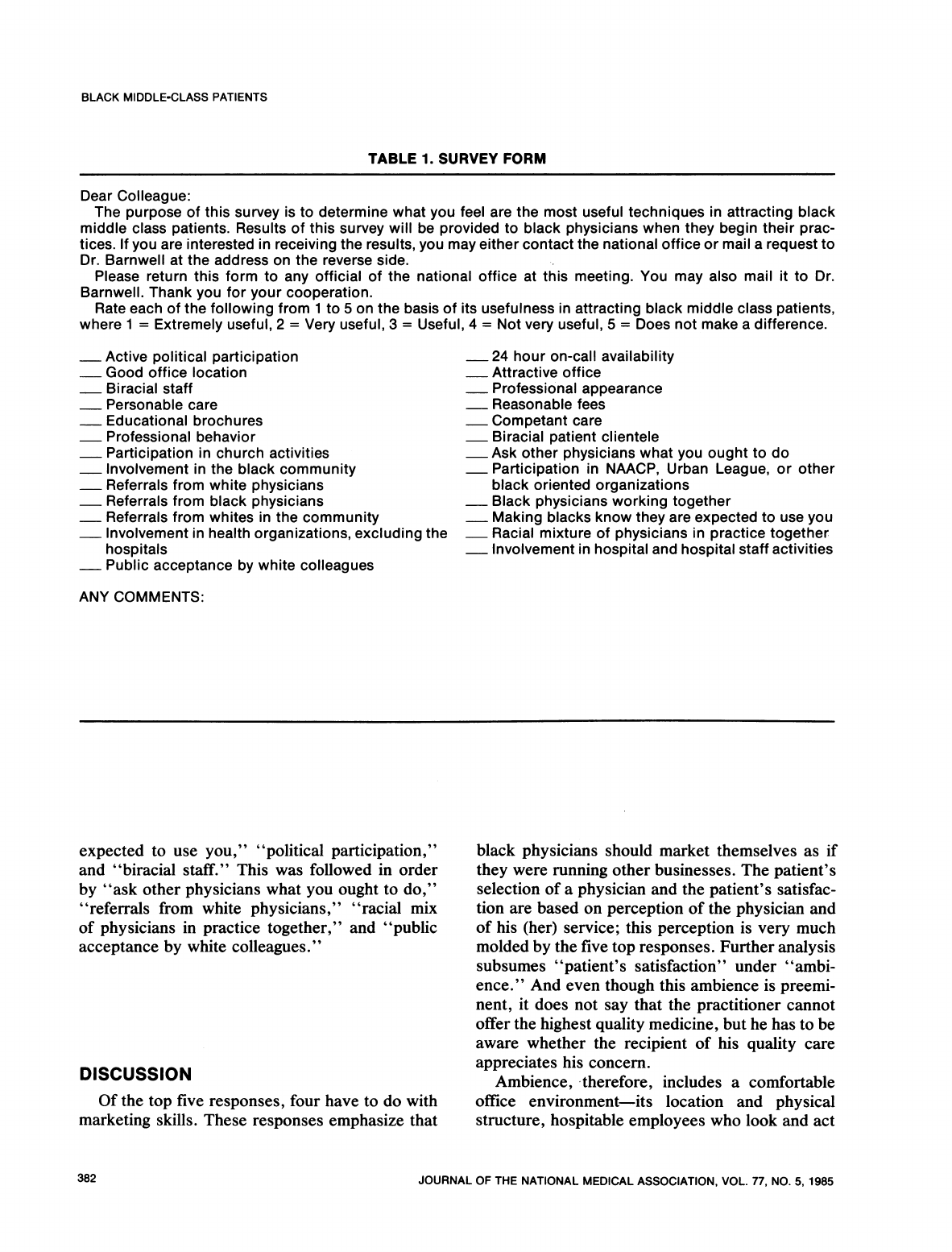
A
copy
of
the
survey
form
is
in-
cluded
as
Table
1.
A
rating
scale
was
constructed
to
assess
the
respondent's
opinion
of
the
item's
utility
in
attracting
black
middle
class
patients.
The
scale
asked
the
respondent
to
rate
the
scale
as
"1
=
Extremely
Useful"
to
"4
=
Not
Very
Use-
ful."
The
respondent
could
have
also
rated
the
item
as
"5
=
Does
not
make
a
difference."
One
hundred
copies
of
the
single
sheet
survey
form
were
distributed
at
the
registration
desk
at
the
Na-
tional
Medical
Association
meeting
in
Chicago.
Respondents
could
have
returned
the
form
at
the
meeting
or
by
mail.
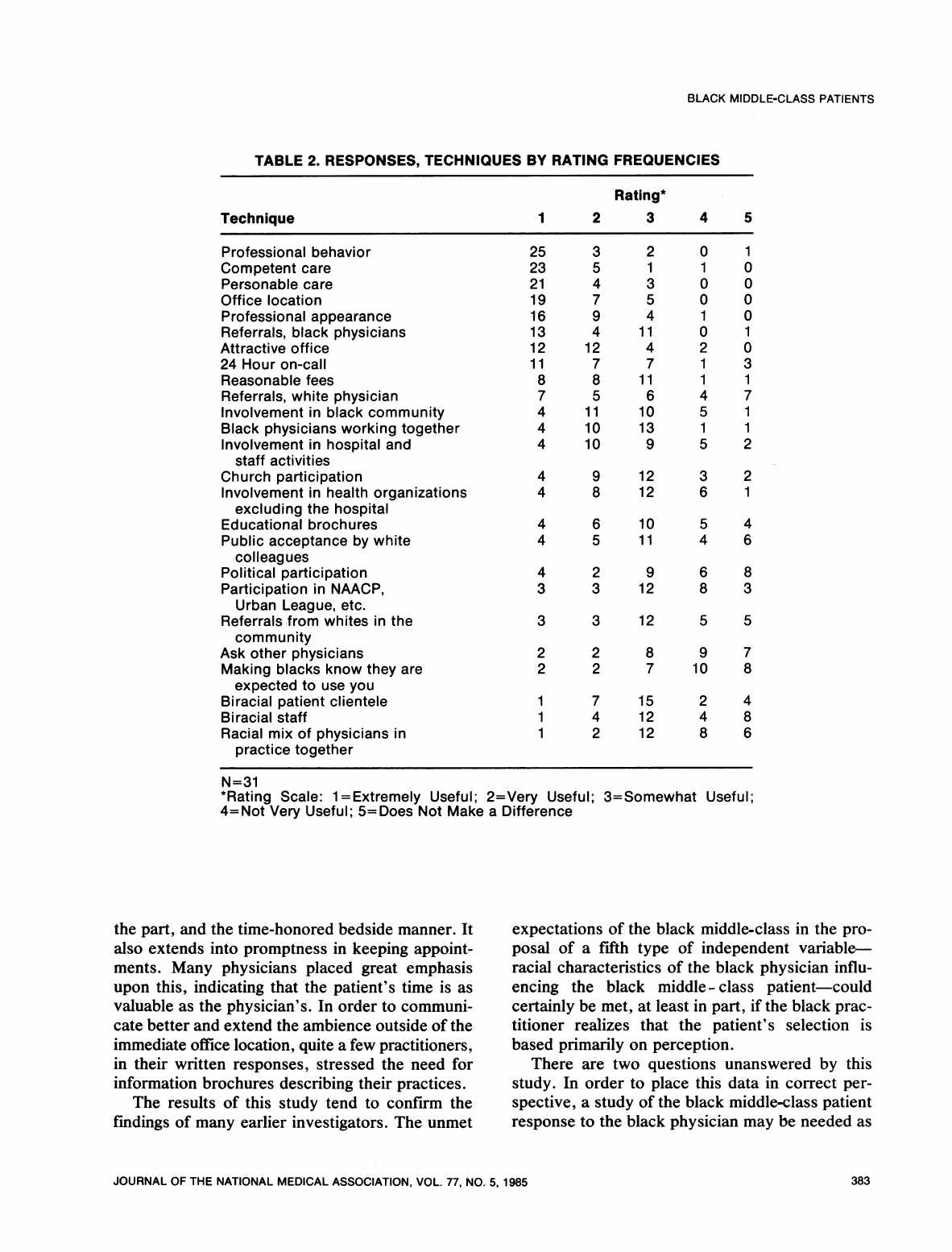
RESULTS
Thirty-one
survey
forms
were
returned.
The
low
rate
of
response
may
be
attributable,
in
part,
to
attitudes
physicians
have
toward
marketing
their
services.
Table
2
presents
the
results,
ranked
by
techniques
rated
as
most
useful.
Professional
behavior
was
judged
most
useful,
followed
by
competent
and
personable
care.
Office
location
and
attractiveness
were
also
judged
to
be
effective
techniques.
Of
all
sources
of
referrals
asked
to
be
rated,
referrals
from
black
physicians
were
judged
to
be
most
effective.
The
technique
judged
least
effective
was
"mak-
ing
blacks
know
they
are
expected
to
see
you."
"Ask
other
physicians
what
you
ought
to
do"
was
next
in
order
of
least
favorable
ratings.
"Partici-
pation
in
the
NAACP,
Urban
League,
or
other
black
oriented
organizations"
and
"racial
mix
of
physicians
in
practice
together"
were
tied
for
the
third
least
useful
rating.
The
techniques
most
often
rated
as
not
making
a
difference
were
"making
blacks
know
they
are
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,
1985
381
BLACK
MIDDLE-CLASS
PATIENTS
TABLE
1.
SURVEY
FORM
Dear
Colleague:
The
purpose
of
this
survey
is
to
determine
what
you
feel
are
the
most
useful
techniques
in
attracting
black
middle
class
patients.
Results
of
this
survey
will
be
provided
to
black
physicians
when
they
begin
their
prac-
tices.
If
you
are
interested
in
receiving
the
results,
you
may
either
contact
the
national
office
or
mail
a
request
to
Dr.
Barnwell
at
the
address
on
the
reverse
side.
Please
return
this
form
to
any
official
of
the
national
office
at
this
meeting.
You
may
also
mail
it
to
Dr.
Barnwell.
Thank
you
for
your
cooperation.
Rate
each
of
the
following
from
1
to
5
on
the
basis
of
its
usefulness
in
attracting
black
middle
class
patients,
where
1
=
Extremely
useful,
2
=
Very
useful,
3
=
Useful,
4
=
Not
very
useful,
5
=
Does
not
make
a
difference.
Active
political
participation
24
hour
on-call
availability
Good
office
location
Attractive
office
Biracial
staff
Professional
appearance
_
Personable
care
Reasonable
fees
Educational
brochures
Competant
care
Professional
behavior
Biracial
patient
clientele
Participation
in
church
activities
Ask
other physicians
what
you
ought
to
do
Involvement
in
the
black
community
Participation
in
NAACP,
Urban
League,
or
other
Referrals
from
white
physicians
black
oriented
organizations
Referrals
from
black
physicians
Black
physicians
working
together
Referrals
from
whites
in
the
community
Making
blacks
know
they
are
expected
to
use
you
Involvement
in
health
organizations,
excluding
the
Racial
mixture
of
physicians
in
practice
together
hospitals
Involvement
in
hospital
and
hospital
staff
activities
_
Public
acceptance
by
white
colleagues
ANY
COMMENTS:
expected
to
use
you,"
"political
participation,"
and
"biracial
staff."
This
was
followed
in
order
by
"ask
other
physicians
what
you
ought
to
do,"
"referrals
from
white
physicians,"
"racial
mix
of
physicians
in
practice
together,"
and
"public
acceptance
by
white
colleagues."
DISCUSSION
Of
the
top
five
responses,
four
have
to
do
with
marketing
skills.
These
responses
emphasize
that
black
physicians
should
market
themselves
as
if
they
were
running
other
businesses.
The
patient's
selection
of
a
physician
and
the
patient's
satisfac-
tion
are
based
on
perception
of
the
physician
and
of
his
(her)
service;
this
perception
is
very
much
molded
by
the
five
top
responses.
Further
analysis
subsumes
"patient's
satisfaction"
under
"ambi-
ence."
And
even
though
this
ambience
is
preemi-
nent,
it
does
not
say
that
the
practitioner
cannot
offer
the
highest
quality
medicine,
but
he
has
to
be
aware
whether
the
recipient
of
his
quality
care
appreciates
his
concern.
Ambience,
therefore,
includes
a
comfortable
office
environment-its
location
and
physical
structure,
hospitable
employees
who
look
and
act
382
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,
1985
BLACK
MIDDLE-CLASS
PATIENTS
TABLE
2.
RESPONSES,
TECHNIQUES
BY
RATING
FREQUENCIES
Rating*
Technique
1
2
3
4
5
Professional
behavior
25
3
2
0
1
Competent
care
23
5
1
1
0
Personable
care
21
4
3
0
0
Office
location
19
7
5
0 0
Professional
appearance
16
9
4
1
0
Referrals,
black
physicians
13
4
11
0
1
Attractive
office
12
12
4
2
0
24
Hour
on-call
11
7
7
1
3
Reasonable
fees
8
8
11
1
1
Referrals,
white
physician
7
5
6
4 7
Involvement
in
black
community
4
11
10
5
1
Black
physicians
working
together
4
10
13
1
1
Involvement
in
hospital
and
4
10
9
5
2
staff
activities
Church
participation
4
9
12
3
2
Involvement
in
health
organizations
4
8
12
6
1
excluding
the
hospital
Educational
brochures
4
6
10
5
4
Public
acceptance
bywhite
4
5
11
4
6
colleagues
Political
participation
4
2
9
6 8
Participation
in
NAACP,
3
3
12
8
3
Urban
League,
etc.
Referrals
from
whites
in
the
3
3
12
5
5
community
Ask
other
physicians
2 2
8
9
7
Making
blacks
know
they
are
2
2
7
10
8
expected
to
use
you
Biracial
patient
clientele
1
7
15
2
4
Biracial
staff
1
4
12
4
8
Racial
mix
of
physicians
in
1
2
12
8
6
practice
together
N=31
*Rating
Scale:
1=Extremely
Useful;
2=Very
Useful;
3=Somewhat
Useful;
4=Not
Very
Useful;
5=Does
Not
Make
a
Difference
the
part,
and
the
time-honored
bedside
manner.
It
also
extends
into
promptness
in
keeping
appoint-
ments.
Many
physicians
placed
great
emphasis
upon
this,
indicating
that
the
patient's
time
is
as
valuable
as
the
physician's.
In
order
to
communi-
cate
better
and
extend
the
ambience
outside
of
the
immediate
office
location,
quite
a
few
practitioners,
in
their
written
responses,
stressed
the
need
for
information
brochures
describing
their
practices.
The
results
of
this
study
tend
to
confirm
the
findings
of
many
earlier
investigators.
The
unmet
expectations
of
the
black
middle-class
in
the
pro-
posal
of
a
fifth
type
of
independent
variable-
racial
characteristics
of
the
black
physician
influ-
encing
the
black
middle
-
class
patient-could
certainly
be
met,
at
least
in
part,
if
the
black
prac-
titioner
realizes
that
the
patient's
selection
is
based
primarily
on
perception.
There
are
two
questions
unanswered
by
this
study.
In
order
to
place
this
data
in
correct
per-
spective,
a
study
of
the
black
middle-class
patient
response
to
the
black
physician
may
be
needed
as
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,
1985
383

BLACK
MIDDLE-CLASS
PATIENTS
a
corollary.
The
authors
believe
that
this
is
not
necessary
because
the
literature
is
replete
with
studies
of
consumer
responses
and
such
a
study
would
be
a
replication
that
would
yield
little
addi-
tional
information.
A
second
unanswered
question
is
that
raised
by
Carter
G.
Woodson
50
years
ago.
He
wrote
about
the
lack
of
confidence
of
black
people
in
the
com-
petence
of
the
black
physician.
He
observed
that
white
physicians
have
to
talk
to
black
patients
to
make
them
believe
that
doctors
of
their
own
race
are
any
good.9
This
observation
is
not
a
superficial
one
but
one
that
goes
to
the
bone;
when
this
is
combined
with
Reitzes's
assertion
that
black
doc-
tors
often
refer
their
black
patients
to
white
spe-
cialists,
it
goes
even
deeper
to
the
very
marrow
of
the
soul
of
black
people."
The
authors
believe
that
there
is
an
immediate
need
of
a
market
concept
approach
in
the
doctor-
patient
interaction.
This
is
a
"physician-needs"
approach
that
involves
analytic,
diagnostic,
and
prescriptive
techniques
to
help
a
doctor
market
his
service
more
effectively.
The
results
of
this
pres-
ent
study
would
be
valuable
for
this
prescription.
Lenox
has
described
the
effective
use
of
such
an
approach
for
use
in
nonprofit
organizations.'2
A
first
step
is
to
construct
goals,
target
audiences,
identify
needs
and
resources,
and
then
consider
how
congruent
these
are
with
one
another.
A
"'marketing
audit"
provides
a
tool
for
developing
and
controlling
market
activities
by
helping
to
identify
factors
to
be
considered
and
by
putting
them
in
measurable
terms.
Creation
of
a
marketing
program
for
black
physicians
would
include:
a
physician
working
with
a
marketing
firm
to
iden-
tify
the
goals
of
the
practice,
targeting
an
audi-
ence,
and
a
marketing
audit.
The
physician
then
should
be
able
to
proceed
with
a
clear
customer
orientation.
CONCLUSIONS
The
results
of
this
study
make
it
clear
that
black
physicians
understand
the
importance
of
marketing-
based
skills
in
the
development
of
a
successful
practice.
In
order
to
be
competitive,
survive,
and
thrive,
black
physicians
should
consider
the
use
of
marketing
specialists
to
assist
them
in
implement-
ing
specific
marketing
goals.
This
is
especially
true
when
one
reflects
upon
the
public
perception
of
the
black
physician's
competence,
and
the
reluc-
tance,
documented
by
other
investigators,
that
some
black
physicians
display
in
referring
their
patients
to
other
black
practitioners.
The
findings
seem
to
indicate
that
black
doctors
do
not
differ
much
from
their
white
counterparts
in
their
per-
ceptions
of
what
it
takes
to
"sell"
a
practice.
Be-
cause
of
societal
beliefs,
ones
that
are
so
institu-
tionalized
that
even
blacks
accept
them,
black
doctors
face
especially
difficult
marketing
prob-
lems.
Indeed,
these
problems
seem
so
severe
that
they
are
reflected
in
dramatic
wage
differentials
between
black
and
white
practitioners
in
compa-
rable
specialites.
Literature
Cited
1.
Greenley
JR,
Schoenherr
RA.
Organizational
effects
on
client
satisfaction
with
humaneness
of
service.
J
Health
Soc
Behav
1981;
22:2-18.
2.
Shortell
S,
Richardson
W,
Lo
Gerfo
J,
et
al.
The
re-
lationship
among
dimensions
of
health
services
in
two
provider
systems:
A
causal
model
approach.
J
Health
Soc
Behav
1977;
18:139-159.
3.
Tessler
R,
Mechanic
D.
Consumer
satisfaction
with
prepaid
group
practice:
A
comparative
study.
J
Health
Soc
Behav
1975;
16:95-113.
4.
Ben-Sira
Z.
The
function
of
the
professional's
affec-
tive
behavior
in
client
satisfaction:
A
revised
approach
to
social
interaction
theory.
J
Health
Soc
Behav
1976;
17:3-11.
5.
Ben-Sira
Z.
Affective
and
instrumental
components
in
the
physician-patient
relationship.
J
Health
Soc
Behav
1980;
21:170-180.
6.
Ross
CE,
Mirowsky
J,
Duff
RS.
Physician
status
characteristics
and
client
satisfaction
in
two
types
of
medi-
cal
practice.
J
Health
Soc
Behav
1982;
23:317-329.
7.
Lloyd
SM,
Johnson
DG.
Practice
patterns
of
black
physicians:
Results
of
a
survey
of
Howard
University
Col-
lege
of
Medicine
Alumni.
J
Nat
Med
Assoc
1982;
74:129-
141.
8.
Myrdal
G.
An
American
Dilemma.
New
York:
Harper
and
Row,
1944,
p
323.
9.
Woodson
C.
The
Negro
Professional
Man
and
the
Community.
Washington,
DC:
The
Association
for
the
Study
of
Negro
Life
and
History,
Inc.,
1934,
p
96.
10.
Richard
MP.
The
Negro
Physician:
Babbitt
or
Revo-
lutionary?
J
Health
Soc
Behav
1969;
10:265-274.
11.
Reitzes
D.
Negroes
and
Medicine.
Cambridge:
Har-
vard
University
Press,
1958,
pp
117,
277-278,
347.
12.
Lenox
C.
Marketing
of
community
information
serv-
ices.
The
Information
Community:
An
Alliance
for
Progress
1981;
18:123-135.
384
JOURNAL
OF
THE
NATIONAL
MEDICAL
ASSOCIATION,
VOL.
77,
NO.
5,
1985
