ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
PB
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
427
Impact of Scribes on Physician Satisfaction, Patient
Satisfaction, and Charting Efficiency: A Randomized
Controlled Trial
ABSTRACT
PURPOSE Scribes are increasingly being used in clinical practice despite a lack of
high-quality evidence regarding their effects. Our objective was to evaluate the
effect of medical scribes on physician satisfaction, patient satisfaction, and chart-
ing efciency.
METHODS We conducted a randomized controlled trial in which physicians in an
academic family medicine clinic were randomized to 1 week with a scribe then
1 week without a scribe for the course of 1 year. Scribes drafted all relevant
documentation, which was reviewed by the physician before attestation and sign-
ing. In encounters without a scribe, the physician performed all charting duties.
Our outcomes were physician satisfaction, measured by a 5-item instrument that
included physicians’ perceptions of chart quality and chart accuracy; patient sat-
isfaction, measured by a 6-item instrument; and charting efciency, measured by
time to chart close.
RESULTS Scribes improved all aspects of physician satisfaction, including over-
all satisfaction with clinic (OR = 10.75), having enough face time with patients
(OR = 3.71), time spent charting (OR = 86.09), chart quality (OR = 7.25), and
chart accuracy (OR = 4.61) (all P values <.001). Scribes had no effect on patient
satisfaction. Scribes increased the proportion of charts that were closed within
48 hours (OR =1.18, P = .028).
CONCLUSIONS To our knowledge, we have conducted the rst randomized con-
trolled trial of scribes. We found that scribes produced signicant improvements
in overall physician satisfaction, satisfaction with chart quality and accuracy, and
charting efciency without detracting from patient satisfaction. Scribes appear
to be a promising strategy to improve health care efciency and reduce physi-
cian burnout.
Ann Fam Med 2017;15:427-433. https://doi.org/10.1370/afm.2122.
INTRODUCTION
E
lectronic health records (EHRs) have radically transformed the
practice of medicine. Driven by federal meaningful use incentives
and penalties,
1,2
more than 95% of US hospitals and 56% of office-
based physicians have adopted EHRs.
3,4
Electronic health records hold
promise to improve patient safety, quality of care, physician efficiency and
performance, patient-physician communication, patient participation, cost
of care, and health outcomes.
5-9
There is also growing evidence, however,
that in their current state, EHRs are associated with decreased physician
productivity and revenue,
10
negative patient-physician interactions and
relationships,
11
and widespread physician dissatisfaction.
12-14
More than one-half of all US physicians experience burnout, with pri-
mary care physicians having one of the highest rates.
15
Among the largest
contributors to burnout is a growing clerical workload.
16-18
For every hour
physicians provide direct face time to patients, 2 more hours are spent on
EHR and desk work.
19
Many physicians leave most charting to the end of
Risha Gidwani, DrPH
1,2
Cathina Nguyen, MPH
3
Alexis Kofoed, MPH
2
Catherine Carragee, BA
2
Tracy Rydel, MD
2
Ian Nelligan, MD, MPH
2
Amelia Sattler, MD
2
Megan Mahoney, MD
2
Steven Lin, MD
2
1
Center for Health Policy and Center for
Primary Care and Outcomes Research,
Stanford University School of Medicine,
Stanford University, Stanford, California
2
Division of Primary Care and Population
Health, Department of Medicine, Stanford
University School of Medicine, Stanford
University, Stanford, California
3
Division of Epidemiology, Department
of Health Research and Policy, Stanford
University School of Medicine, Stanford
University, Stanford, California
Conflicts of interest: authors report none.
CORRESPONDING AUTHOR
Steven Lin, MD
Suite 405, 211 Quarry Rd
MC 5985
Palo Alto, CA 94304
stevenlin@stanford.edu
IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
428
the day, and spend 1 to 2 hours each night working on
the EHR.
19
One strategy to decrease clerical burden is the
use of scribes. Scribes are nonlicensed team members
trained to document patient encounters in real time
under the direct supervision of a physician.
20
Scribes
do not act independently but may assist with chart-
ing, recording laboratory and radiology results, and
supporting physician workflow with EHR data entry.
21
Although the use of scribes as physician extenders in
emergency departments has been reported as early
as the 1970s, it is only recently that the popularity of
scribes has skyrocketed.
22
Scribes are currently being
used in more than 1,000 hospitals and clinics across
44 states.
23
It is estimated that by 2020, there will be
100,000 scribes in the United States, or 1 scribe for
every 9 physicians.
23
Despite the increasing presence of scribes, method-
ologically rigorous studies regarding their impact are
lacking. Two systematic reviews found, using data from
observational studies, that scribes may improve rev-
enue, patient and physician satisfaction, productivity,
efficiency, and the quality of patient-physician interac-
tions.
24,25
There has been no randomized controlled
study of scribes, and few studies have been undertaken
in the primary care setting. Given that most office
visits are to primary care physicians,
26
research in this
setting is particularly warranted.
METHODS
Design
Physicians were randomly assigned to 1 week practic-
ing with a scribe then 1 week without a scribe for the
course of 52 weeks. Randomization at the physician-
week level was chosen instead of randomizing at the
level of patients, as variations in length of patient
appointments posed challenges for proper allocation
of scribes across patients and was too disruptive to
normal clinic flow. We also chose not to randomize
at the physician level, as the small number of physi-
cians included in this study would not properly protect
against imbalance in the scribe and no-scribe groups.
During the week in which a physician was assigned
a scribe, the scribe attended all appointments and
drafted all relevant documentation, including the his-
tory and physical findings, objective examination find-
ings, laboratory and radiology results, assessment and
plan, and patient instructions. The physician reviewed
the note, attested to its accuracy, and signed it before
the chart was closed. During the week in which the
physician was not assigned a scribe, the physician per-
formed all charting duties. The EHR used was the out-
patient version of Epic (Epic Systems Corporation).
The study was conducted from July 2015 to June
2016. Four physicians and 2 scribes participated in
the study, which was undertaken in a family medi-
cine clinic associated with a large academic medical
center in Northern California. All physicians were
board-certified in family medicine and had an aver-
age of 6 years of practice experience. None had prior
experience working with scribes. As part-time clini-
cians, each physician in the study had 4, 4-hour clinic
sessions per week when data were collected. Both
scribes were college graduates who completed an
80-hour training course administered by a commercial
scribe company (Elite Medical Scribes). One scribe
was assigned to 2 physicians in the first 6 months of
the study; in the second 6 months, that scribe was
assigned to the other 2 physicians. This allowed us to
test for any learning effects that may have occurred in
the physician-scribe dyads.
Physician Satisfaction
Physician satisfaction was measured by a self-
administered 5-item questionnaire. Answers were
recorded using a 7-point Likert scale, with a value of
1 indicating strong disagreement (strongly dissatis-
fied) and 7 indicating strong agreement (strongly
satisfied). Physicians were offered 1 questionnaire
after each 4-hour clinic session. For data analyses, we
dichotomized each answer into strongly satisfied vs
non–strongly satisfied (7 vs 1 to 6) because of skewness
in results. In sensitivity analyses, we tested alternate
ways to characterize the outcome by dichotomizing
scores from 1 to 5 and 6 to 7. To investigate the effect
of scribes on aspects of physician satisfaction, each
item was assessed using its own fixed-effects logistic
regression equation with the physician questionnaire
as the unit of analysis and accommodating multiple
observations per physician. We adjusted for whether
the interaction was new so we could test any learning
effects over time within physician-scribe dyads. Specifi-
cally, we investigated whether a physician paired with a
scribe had significantly lower satisfaction scores during
the first quarter than during the second quarter that the
same physician and scribe were paired. We adjusted for
multiple hypothesis testing using the conservative Bon-
ferroni correction, resulting in an α of .01.
27
Patient Satisfaction
Patient satisfaction was measured using a shortened,
validated, 6-item questionnaire designed for the pri-
mary care setting.
28
Each patient was asked to complete
the questionnaire immediately after the appointment.
To encourage completion, questionnaires were made
anonymous. Answers were recorded using a 7-point
Likert scale, with 1 indicating strong disagreement
IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
429
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
428
(strongly dissatisfied) and 7 indicating strong agreement
(strongly satisfied). Each response was dichotomized
into strongly satisfied (7) vs non–strongly satisfied (1 to
6) because of skewness of the distribution. In sensitivity
analyses, we tested alternate ways to characterize the
outcome, specifically dichotomizing scores from 1 to 5
and 6 to 7. We investigated each item separately using
its own fixed-effects logistic regression equation with
the patient questionnaire as the unit of analysis, clus-
tering questionnaires within physician. All tests were
evaluated against a Bonferroni-corrected α of .007.
Charting Efciency
Physician efficiency was measured as the time to chart
close, which is calculated as the time from appointment
start to the physician signing the chart note, which is
marked by timestamps in the EHR. Industry standards
(Medicare documentation guidelines)
29
state that charts
should be completed within 48 hours; therefore, we
dichotomized time to close chart into 48 hours or less
vs more than 48 hours. We ran fixed-effects logistic
regression with chart as the unit of analysis, accommo-
dating clustering of charts within physician.
This study was exempted from formal review by
the Institutional Review Board of Stanford University
School of Medicine.
RESULTS
Physician Satisfaction
A total of 361 physician satisfaction questionnaires
were completed, for a 73.1% response rate (Table 1).
Physicians were more likely to complete a question-
naire when a scribe was present (53.2%) than when a
scribe was not (46.8%). Scribes produced significantly
higher physician satisfaction in all aspects of care
and charting (Tables 2-4). Physicians who worked
with a scribe had 10.75 the adjusted odds of express-
ing high satisfaction with their clinic that day, 3.71
the adjusted odds of having enough face time with
patients, and 86.09 the adjusted odds of expressing
high satisfaction with the amount of time they spent
charting (all P <.001). Scribes increased physician
satisfaction with the quality and accuracy of their
charts. Physicians reported 7.25 the adjusted odds of
being satisfied with their chart quality when a scribe
was present (P <.001). There was no
difference in satisfaction with quality
when the physician-scribe dyad was
new vs established (P = .451). Physi-
cians reported 4.61 the adjusted odds
of being satisfied with chart accuracy
when a scribe was present (P < .0 01).
Physicians did report being less
satisfied with chart accuracy when
the physician-scribe dyad was new
(adjusted OR = 0.39) vs established,
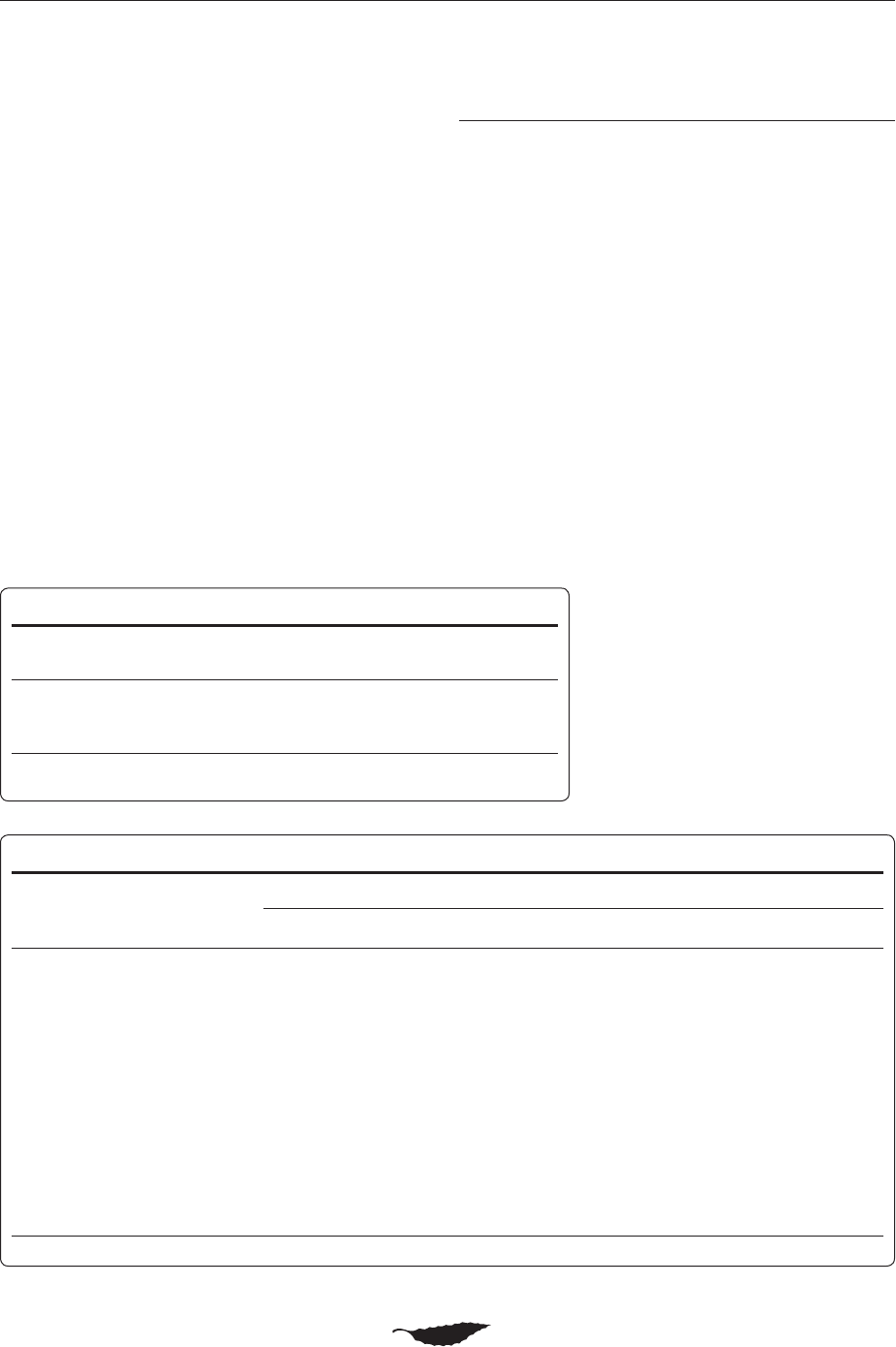
Table 1. Survey Questionnaire Completion
Characteristic
Scribe
No. (%)
No Scribe
No. (%)
Total
No.
Patient satisfaction questionnaires completed 808 (54.8) 667 (45.2) 1,475
a
Physician satisfaction questionnaires completed 192 (53.2) 169 (46.8) 361
b
Charts analyzed for efciency 1,381 (52.4) 1,255 (47.6) 2,636
a
Of 1,681 questionnaires distributed, 87.7% were returned.
b
Of 494 questionnaires distributed, 73.1% were returned.
Table 2. Physician and Patient Questionnaire Results, Unadjusted
Characteristic
Questionnaire Score
a
1
No. (%)
2
No. (%)
3
No. (%)
4
No. (%)
5
No. (%)
6
No. (%)
7
No. (%)
Physician questionnaire (n = 361)
Overall satisfaction 2 (0.6) 8 (2.2) 16 (4.4) 39 (10.8) 69 (19.1) 122 (33.8) 105 (29.1)
Face time with patients 2 (0.6) 6 (1.7) 16 (4.4) 34 (9.4) 69 (19.1) 90 (24.9) 144 (39.9)
Charting time 8 (2.2) 13 (3.6) 26 (7. 2) 67 (18.6) 66 (18.3) 87 (24.1) 94 (26.0)
Chart quality 3 (0.8) 5 (1.4) 14 (3.9) 27 (7.5) 69 (19.1) 114 ( 31.6) 129 (35.7)
Chart accuracy 2 (0.6) 4 (1.1) 10 (2.8) 36 (10.0) 68 (18.8) 106 (29.4) 135 ( 37.4)
Patient questionnaire (n = 1,475)
Physician explains things to me 8 (0.5) 0 (0.0) 1 (0.1) 2 ( 0.1) 8 (0.5) 84 (5.7) 1,372 (93.0)
Physician listens to me 8 (0.5) 0 (0.0) 1 (0.1) 3 (0.2) 10 (0.7) 67 (4.5) 1,386 (94.0)
Physician cares about me 7 (0.5) 1 (0.1) 0 (0.0) 5 (0.3) 17 (1.2) 72 (4.9) 1,366 (93.1)
Physician encourages me to talk 7 (0.5) 1 (0.1) 1 (01) 5 (0.3) 19 (1.3) 84 (5.7) 1,354 (92.0)
Physician spends enough time with me 7 (0.5) 1 (0.1) 1 (0.1) 6 (0.4) 22 (1.5) 97 (6.6) 1,341 (90.9)
I would recommend this physician 7 (0.5) 1 (0.1) 1 (0.1) 5 (0.3) 10 (0.7) 75 (5.1) 1,375 (93.3)
a
Responses scored on a scale from 1 to 7 where 1 indicates least satisfaction, and 7 indicates most satisfaction.
IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
430
but results were not significant using a Bonferroni-
corrected α of .01 (P = .019). There was no difference
in significance of the impact of scribes on physician
survey results when we dichotomized the responses
into 1 to 5 vs 6 to 7.
Patient Satisfaction
A total of 1,475 patient satisfaction questionnaires
were completed for an 87.7% response rate (Table 1).
Patients were more likely to complete a questionnaire
when a scribe was present (54.8%) than when a scribe
was not (45.2%). In adjusted analyses, there
were no significant differences in any aspect
of patient satisfaction between physician
visits in which a scribe was or was not pres-
ent (Table 2 and Table 5). Satisfaction across
patient questionnaires, however, was high
with or without a scribe, with more than
91% of patients in either group reporting
being highly satisfied with their care. There
was no difference in significance of the
impact of scribes on patient survey results
when we dichotomized the responses into 1
to 5 vs 6 to 7.
Charting Efciency
Scribes improved time to close chart. In
unadjusted analyses, 28.5% of charts that
were drafted by physicians were closed in 48
hours relative to 32.6% of charts drafted by
scribes. In adjusted analyses, scribed charts
had 1.18 the adjusted odds of being closed
within 48 hours compared with physician-
only charts (P = .028) (Table 6).
DISCUSSION
To our knowledge, we have undertaken the
first randomized controlled trial evaluating
the effects of medical scribes. We found
that scribes significantly improved physi-
cian satisfaction across all measured aspects
of patient care and documentation. Scribes
improved physician-perceived chart qual-
ity and chart accuracy, as well as charting
efficiency as measured by the likelihood of
closing a chart within 48 hours.
When working with a scribe, physicians
were much more satisfied with how their
clinic went, the length of time they spent
face-to-face with patients, and the time
they spent charting. These findings suggest
that scribes may have a protective effect on
physicians’ well-being. Implementation of
team documentation is an important com-
ponent of achieving the Quadruple Aim,
30
a
patient-centered approach to care that also
emphasizes improving the work life of physi-
cians. Spending less time on documentation
frees up the physician to pursue direct clini-
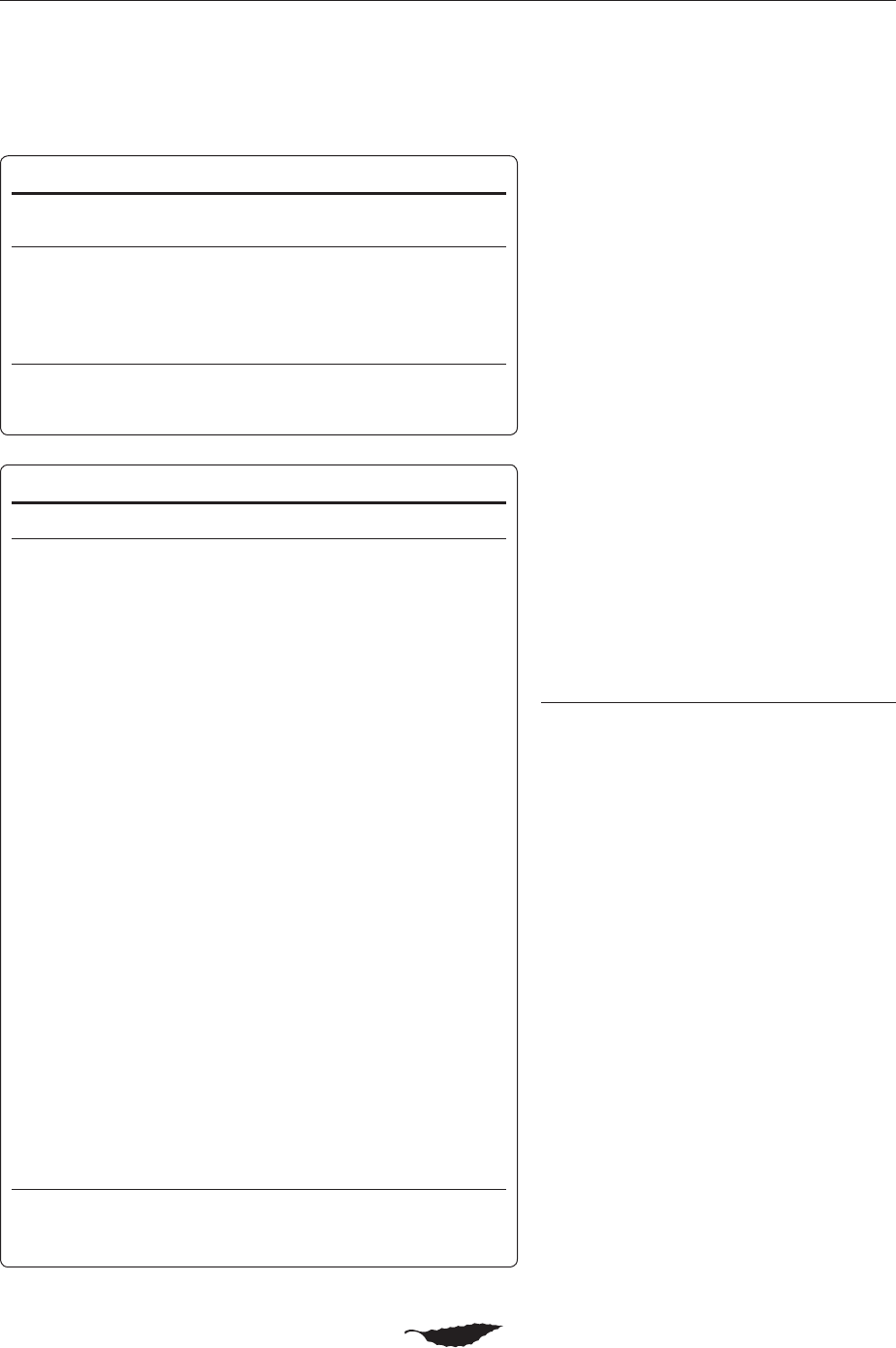
Table 3. Physician Satisfaction, Unadjusted Results
Characteristic
Scribe Present
Median Score (IQR)
a
Scribe Not Present
Median Score (IQR)
a
Overall satisfaction 6 (6-7) 5 (4-6)
Face time with patients 6.5 (6-7) 5 (4-7)
Charting time 6 (6-7) 4 (3-5)
Chart quality 6 (6-7) 5 (5-6)
Chart accuracy 6 (6-7) 6 (5-7)
IQR = interquartile range.
a
Responses scored on a scale from 1 to 7 where 1 indicates least satisfaction, and 7 indicates
most satisfaction.
Table 4. Physician Satisfaction, Adjusted Results
Outcome OR 95% CI P Value
Overall satisfaction
Scribe 10.75 5.36-21.58 <.0 01
Physician 1, new interaction
a
0.51 0.27-0.96 .038
Physician 2 0.78 0.36-1.71 .539
Physician 3 1.49 0.71-3.12 .288
Physician 4 0.15 0.06-0.41 <.0 01
Face time with patients
Scribe 3.71 1.91-7.21 <.0 01
Physician 1, new interaction
a
0.73 0.37-1.46 .375
Physician 2 1.28 0.63-2.60 .498
Physician 3 4.71 2.35-9.44 <.0 01
Physician 4 0.11 0.04-0.31 <.001
Charting time
Scribe 86.09 19.58 -378.41 <.0 01
Physician 1, new interaction
a
1.04 0.56 -1.96 .891
Physician 2 1.75 0.70-4.35 .228
Physician 3 1.31 0.55 -3.16 .542
Physician 4 0.15 0.05-0.46 .001
Chart quality
Scribe 7.25 3.42-15.39 <.0 01
Physician 1, new interaction
a
0.75 0.36-1.55 .435
Physician 2 1.34 0.60-3.01 .475
Physician 3 10.18 4.53-22.85 <.0 01
Physician 4 0.13 0.04-0.44 .001
Chart accuracy
Scribe 4.61 2.11-10. 0 6 <.0 01
Physician 1, new interaction
a
0.38 0.17-0.85 .018
Physician 2 0.81 0.36 -1.81 .611
Physician 3 15.19 6.9-33.44 <.001
Physician 4 0.09 0.02-0.34 <.001
OR = odds ratio.
Note: Model B.
a
First interaction between scribe and physician.
IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
431
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
430
cal care and care coordination, thus enhancing joy of
practice and preventing burnout. In academic centers,
scribes provide faculty physicians more time to teach
medical students and residents.
31
We found that not only were physicians satisfied
with the quality and accuracy of charting done by
scribes, they were more satisfied with scribed charts
than with their own. This finding is consistent with a
study suggesting that scribed notes are of higher qual-
ity than physician-only notes.
32
Patient encounters in
primary care are often highly complex; scribes enable
physicians to capture all the important details in the
note while communicating effectively with the patient
in the room.
During a typical day in the ambulatory setting,
49% of physician time is spent on EHR and desk work,
whereas only 27% is spent face-to-face with patients.
19
Physicians can use EHR shortcuts, such as copy and
paste,
33
but these actions are associated with a risk
of documentation error that can jeopardize patient
safet y.
34,35
In addition, documentation competes with
panel management and EHR inbox completion. It is
estimated that the average primary care physician
receives 76.9 EHR inbox notifications daily, requiring
an investment of approximately 66.8 minutes
per day.
36
Eliminating the burden of writing
notes affords more time for physicians to
attend to the tasks of panel management dur-
ing, not after, their workday.
Our study found no difference in patient
satisfaction between visits with or without
a scribe, perhaps because of ceiling effects;
patients expressed high satisfaction both
during visits with and without a scribe. Nev-
ertheless, we found that the presence of a
scribe did not decrease patient satisfaction.
This finding has been found in other nonran-
domized studies, even in settings as sensitive
as a urology practice.
37
Our study is the first to evaluate charting
efficiency in a randomized controlled man-
ner. We found that scribed charts were more
likely to be closed within 48 hours compared
with charts completed by physicians alone.
Charts that are completed in a timely man-
ner allow patient data to be accessed by
other physicians in the health care system,
which is particularly important to safety and
effective care coordination. Charts com-
pleted in a timely manner may also be more
accurate than those completed multiple days
after the patient’s visit.
This randomized controlled trial was con-
ducted at a single family medicine clinic in an
academic medical center. Although our unit
of analysis was a physicians’ day or patient
encounter, our study’s biggest limitation is
the relatively few physicians and scribes. Our
findings are positive with respect to physi-
cian satisfaction and efficiency, but future
randomized studies should be conducted
with large sample sizes and across multiple
institutions to improve the generalizability
of these findings. The physician satisfaction
instrument we used measured markers related
to joy of practice and was deemed feasible
Table 5. Patient Satisfaction, Adjusted Results
Outcome OR 95% CI P Value
Physician explains things to me
Scribe 0.82 0.48-1.40 .468
Physician 1, new interaction
a
0.81 0.48-1.36 .429
Physician 2 0.40 0.22-0.71 .002
Physician 3 1.54 0.72-3.32 .266
Physician 4 0.97 0.50-1.87 .920
Physician listens to me
Scribe 0.88 0.49-1.58 .681
Physician 1, new interaction
a
0.75 0.42-1.32 .319
Physician 2 0.64 0.36 -1.11 .113
Physician 3 2.63 1.18-5.87 .018
Physician 4 1.58 0.82-3.04 .717
Physician cares about me
Scribe 1.15 0.67-1.97 .609
Physician 1, new interaction
a
0.66 0.38 -1.13 .130
Physician 2 0.39 0.22-0.69 .001
Physician 3 2.19 0.96-5.00 .061
Physician 4 0.79 0.43-1.47 .459
Physician encourages me to talk
Scribe 1.07 0.63-1.80 .808
Physician 1, new interaction
a
0.58 0.35-0.97 .037
Physician 2 0.39 0.22-0.68 .001
Physician 3 2.09 0.95-4.60 .068
Physician 4 0.68 0.38-1.23 .202
Physician spends enough time
with me
Scribe 1.12 0.70-1.79 .642
Physician 1, new interaction
a
0.92 0.06-1.50 .725
Physician 2 0.53 0.33-0.85 .008
Physician 3 3.20 1.57-6.53 .001
Physician 4 1.55 0.90-2.68 .116
I would recommend this physician
Scribe 1.06 0.60-1.89 .825
Physician 1, new interaction
a
0.59 0.34-1.04 .066
Physician 2 0.34 0.18-0.62 .001
Physician 3 1.79 0.76 - 4.19 .183
Physician 4 0.75 0.38-1.47 .405
OR = odds ratio.
Note: Model B.
a
First interaction between scribe and physician.
IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
432
for repeated use, but it was not a validated survey of
joy of practice or burnout. Our findings of improved
efficiency, as measured by time to chart close, would
be strengthened by future work using other objective
approaches, such as time and motion analyses. Our
data show that physicians reported higher satisfaction
with the quality and accuracy of charting when scribes
were present; future work should evaluate chart qual-
ity in an objective way with blinded observers using a
validated instrument. We also found that patient sat-
isfaction was not affected by the presence of a scribe,
but we believe that qualitative work would better elu-
cidate patients’ perceptions of scribes. Other worthy
avenues of research include evaluating team-based care
models using medical assistants or nurses as scribes,
38
the effect of scribes on physician productivity and rev-
enue, as well as cost-benefit analyses, which have been
described by others
39-41
but warrant further research in
the primary care setting.
The challenge of modifying physicians’ practices to
accommodate EHRs without sacrificing quality of care
or quality of physician-patient interactions is not trivial.
Some have suggested that scribes are not an appropriate
solution, arguing that they are no substitute for better
functioning EHRs or may remove some of the pressure
on EHR designers to improve their systems.
23
We ag ree
that scribes are not a replacement for EHR redesign,
but we do consider them an immediate solution that
can be implemented while the more onerous and time-
consuming problem of EHR redesign is also tackled.
We also believe scribes can serve as a complement to a
high-functioning EHR, as the latter will still require the
mundane capture of information that does not require
a physician. By reducing the time that physicians spend
on clerical tasks, scribes serve an important function in
a multidisciplinary health care team.
To read or post commentaries in response to this article, see it
online at http://www.AnnFamMed.org/content/15/5/427.
Key words: medical scribes; electronic health records; work satisfac-
tion; patient satisfaction; efciency; primary care physicians; random-
ized controlled trial
Submitted December 6, 2016; submitted, revised, April 15, 2017;
accepted May 3, 2017.
Funding support: This study was supported by a grant to the senior
author (S.L.) from the Pisacano Leadership Foundation, the philan-
thropic foundation of the American Board of Family Medicine.
Disclaimer: The Foundation had no role in the design of the study; the
collection, analysis, and interpretation of the data; and the decision to
approve publication of the nished manuscript.
Previous presentations: A portion of this manuscript was presented at
the Stareld Summit, April 23-26, 2016, Washington, DC; and the Soci-
ety of Teachers of Family Medicine (STFM) Annual Spring Conference,
April 30-May 4, 2016, Minneapolis, Minnesota.
Acknowledgments: The authors wish to thank Sang-ick Chang, MD,
MPH, associate dean for primary care; Tim Engberg, RN, MA, vice
president for primary care; Juno Vega, RN, clinic manager; and Therese
Truong, RN, assistant clinic manager, for their support of the scribe
program.
References
1. Blumenthal D. Wiring the health system—origins and provisions of
a new federal program. N Engl J Med. 2011; 365(24): 2323-2329.
2. Blumenthal D. Implementation of the federal health information
technology initiative. N Engl J Med. 2011; 365(25): 2426-2431.
3. Ofce of the National Coordinator for Health Information Technol-
ogy. Hospitals Participating in the CMS EHR Incentive Programs,
Health IT Quick-Stat #45. http: //dashboard.healthit.gov/quickstats/
pages/FIG-Hospitals-EHR-Incentive-Programs.php. Updated Feb
2016. Accessed Nov 1, 2016.
4. Ofce of the National Coordinator for Health Information Tech-
nology. Ofce-based Health Care Professionals Participating
in the CMS EHR Incentive Programs, Health IT Quick-Stat #44.
http: //dashboard.healthit.gov/quickstats/pages/FIG-Health-Care-
Professionals-EHR-Incentive-Programs.php. Updated Feb 2016.
Accessed Nov 1, 2016.
5. Institute of Medicine, Committee on Patient Safety and Health
Information Technology. Health IT and Patient Safety: Building Safer
Systems for Better Care. Washington, DC: National Academies Press;
2011.
6. Holroyd-Leduc JM, Lorenzetti D, Straus SE, Sykes L, Quan H. The
impact of the electronic medical record on structure, process, and
outcomes within primary care: a systematic review of the evidence.
J Am Med Inform Assoc. 2011; 18(6): 732-737.
7. King J, Patel V, Jamoom EW, Furukawa MF. Clinical benets of elec-
tronic health record use: national ndings. Health Serv Res. 2014;
49(1 Pt 2): 392-404.
8. Health IT. gov. Benets of electronic health records (EHRs). http: //
www.healthit.gov/providers-professionals/benets-electronic-health-
records-ehrs. Updated Jul 2015. Accessed Nov 1, 2016.
9. Slight SP, Berner ES, Galanter W, et al. Meaningful use of electronic
health records: experiences from the eld and future opportunities.
JMIR Med Inform. 2015; 3(3): e30.
10. Fleming NS, Becker ER, Culler SD, et al. The impact of electronic
health records on workow and nancial measures in primary care
practices. Health Serv Res. 2014; 49(1 Pt 2): 405-420.
Table 6. Charting Efciency, Adjusted Results for
Less Than 48 Hours to Close Chart
Variable OR 95% CI P Value
Scribe 1.18 1.02-1.36 .028
Physician 1, new
interaction
a
1.01 0.86 -1.18 .950
Physician 2 6.26 5.04 -7.76 <.001
Physician 3 8.35 6.75-10.33 <.0 01
Physician 4 4.80 3.85-5.99 <.0 01
OR = odds ratio.
Note: Model B.
a
First interaction between scribe and physician.

IMPACT OF SCRIBES
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
433
ANNALS OF FAMILY MEDICINE
✦
WWW.ANNFAMMED.ORG
✦
VOL. 15, NO. 5
✦
SEPTEMBER/OCTOBER 2017
432
11. Shachak A, Reis S. The impact of electronic medical records on
patient-doctor communication during consultation: a narrative lit-
erature review. J Eval Clin Pract. 2009; 15(4): 641-649.
12. Friedberg MW, Chen PG, Van Busum KR, et al. Factors Affecting Phy-
sician Professional Satisfaction and Their Implications for Patient Care,
Health Systems, and Health Policy. Santa Monica, CA: Rand Corpora-
tion; 2013.
13. Menachemi N, Collum TH. Benets and drawbacks of electronic
health record systems. Risk Manag Healthc Policy. 2011; 4: 47-55.
14. Boonstra A, Broekhuis M. Barriers to the acceptance of electronic
medical records by physicians from systematic review to taxonomy
and interventions. BMC Health Serv Res. 2010; 10: 231.
15. Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and
satisfaction with work-life balance in physicians and the general US
working population between 2011 and 2014. Mayo Clin Proc. 2015;
90(12): 1600-1613.
16. Gottschalk A, Flocke SA. Time spent in face-to-face patient
care and work outside the examination room. Ann Fam Med.
2005;3(6):488-493.
17. Gilchrist V, McCord G, Schrop SL, et al. Physician activi-
ties during time out of the examination room. Ann Fam Med.
2005;3(6):494-499.
18. Chen MA, Hollenberg JP, Michelen W, Peterson JC, Casalino LP.
Patient care outside of ofce visits: a primary care physician time
study. J Gen Intern Med. 2011; 26(1): 58-63.
19. Sinsky C, Colligan L, Li L, et al. Allocation of physician time in
ambulatory practice: a time and motion study in 4 specialties. Ann
Intern Med. 2016; 165(11): 753-760.
20. Campbell LL, Case D, Crocker JE, et al. Using medical scribes in a
physician practice. J AHIMA. 2012; 83(11): 64-69.
21. Joint Commission. Clarication: Safe use of scribes in clinical set-
tings. Jt Comm Perspect. 2011; 31(6): 4-5.
22. Lin S, Khoo J, Schillinger E. Next big thing: integrating medi-
cal scribes into academic medical centres. BMJ Simulation & Tech
Enhanced Learning. 2016; 2(2): 27-29.
23. Gellert GA, Ramirez R, Webster SL. The rise of the medical scribe
industry: implications for the advancement of electronic health
records. JAMA. 2015; 313(13): 1315-1316.
24. Shultz CG, Holmstrom HL. The use of medical scribes in health care
settings: a systematic review and future directions. J Am Board Fam
Med. 2015; 28(3): 371-381.
25. Heaton HA, Castaneda-Guarderas A, Trotter ER, Erwin PJ, Bellolio
MF. Effect of scribes on patient throughput, revenue, and patient
and provider satisfaction: a systematic review and meta-analysis.
Am J Emerg Med. 2016; 34(10): 2018-2028.
26. Centers for Disease Control and Prevention. National Ambulatory
Medical Care Survey: 2012 State and National Summary Tables.
http: //www.cdc.gov/nchs/data/ahcd/namcs_summary/2012_namcs_
web_tables.pdf. Updated 2012. Accessed Nov 1, 2016.
27. Bland JM, Altman DG. Multiple signicance tests: the Bonferroni
method. BMJ. 1995; 310(6973): 170.
28. Hojat M, Louis DZ, Maxwell K, Markham FW, Wender RC, Gonnella
JS. A brief instrument to measure patients’ overall satisfaction with
primary care physicians. Fam Med. 2011; 43(6): 412-417.
29. Centers for Medicare and Medicaid Services. Medicare Claims
Processing Manual. Chapter 12 – Physicians/Nonphysician Practi-
tioners. http: //www.cms.gov/Regulations-and-Guidance/Guidance/
Manuals/Downloads/clm104c12.pdf. Updated Mar 2016. Accessed
Nov 1, 2016.
30. Bodenheimer T, Sinsky C. From triple to quadruple aim: care
of the patient requires care of the provider. Ann Fam Med.
2014;12(6):573-576.
31. Hess JJ, Wallenstein J, Ackerman JD, et al. Scribe impacts on pro-
vider experience, operations, and teaching in an academic emer-
gency medicine practice. West J Emerg Med. 2015; 16(5): 602- 610.
32. Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: How
do their notes stack up? J Fam Pract. 2016; 65(3): 155 -159.
33. O’Donnell HC, Kaushal R, Barrón Y, Callahan MA, Adelman RD,
Siegler EL. Physicians’ attitudes towards copy and pasting in elec-
tronic note writing. J Gen Intern Med. 2009; 24(1): 63-68.
34. Siegler EL, Adelman R. Copy and paste: a remediable hazard of
electronic health records. Am J Med. 2009; 122(6): 495-496.
35. Markel A. Copy and paste of electronic health records: a modern
medical illness. Am J Med. 2010; 123(5): e9.
36. Murphy DR, Meyer AN, Russo E, Sittig DF, Wei L, Singh H. The
burden of inbox notications in commercial electronic health
records. JAMA Intern Med. 2016; 176(4): 559-560.
37. Koshy S, Feustel PJ, Hong M, Kogan BA. Scribes in an ambulatory
urology practice: patient and physician satisfaction. J Urol. 2010;
184(1): 258-262.
38. Yan C, Rose S, Rothberg MB, Mercer MB, Goodman K, Misra-
Hebert AD. Physician, scribe, and patient perspectives on clinical
scribes in primary care. J Gen Intern Med. 2016; 31(9): 990-995.
39. Bank AJ, Obetz C, Konrardy A, et al. Impact of scribes on patient
interaction, productivity, and revenue in a cardiology clinic: a pro-
spective study. Clinicoecon Outcomes Res. 2013; 5: 399-406.
40. Bank AJ, Gage RM. Annual impact of scribes on physician produc-
tivity and revenue in a cardiology clinic. Clinicoecon Outcomes Res.
2015; 7: 489 -495.
41. Walker KJ, Dunlop W, Liew D, et al. An economic evaluation of the
costs of training a medical scribe to work in Emergency Medicine.
Emerg Med J. 2016; 33(12): 865-869.
