Scope of Appointment Cover &
Instruction Sheet
In order to provide a comprehensive review of the Medicare
market, we are required to receive the following Scope of
Appointment form completed and signed by any Medicare
beneficiary at least 48 hours prior to a meeting (special
circumstances may apply).
Please complete the Scope of Appointment by in initialing
the boxes and adding your name and signature to the form in
the appropriate fields.
If you have any medications that need to be researched
please add them to the Doctor & RX assessment form.
Of you have any additional concerns please add them to the
optional NOTES section on the assessment form.
Please be advised that we cannot discuss any Medicare
Advantage plans without having received the scope of
appointment first! The other form is voluntary.
Please return the completed forms to our
secure fax at (888) 287-3186.
The
Centers for Medicare and Medicaid Se
rv
ices requires agents
to
document the scope
of
a marketing
appointment
before any in-person sales
meet
i
ng
to
ensure understanding
of
what
w
il
l be discussed.
All
in
formation provided on this form is confidential and should
be
completed
by
each person wi
th
Medicare or his/her authorized
rep
resentative.
S
ta
n
d-alone
Medicare Prescription
Drug Plans
(P
art D)
Medicare
Pre
scripti
on
Drug Plan (PDP) - A stand-
alone drug plan
that
adds prescription drug coverage
to
Original Medicare.
Medicare Advantage Plans (Part
C)
A Medicare Advantage Plan
that
provides all Original
Medicare Part A and Part B heal
th
coverage and
sometimes offers Part D prescription drug coverage
and other additional benefits.
Medicare
He
a
lt
h Maintenance O
rg
anizat
ion
(HMO)-
A Medicare Advantage Plan
that
typically requires you
to
see
only in-network providers and get referrals from
a primary care doctor.
Medicare Preferred Provider Organization
(P
P
O)
Pl
an - A Medicare Advantage
Plan
where
in
most
cases
you pay
less
if
you use in-netwark doctors, and
referrals from a pri
mary
care doctor are
not
required.
Med
ic
are
Pri
v
at
e Fee-
Fa
r-Service
(PFFS)
Plan -
A Medicare Advantage Plan in which you
may
go to
any Medicare-approved doctor, hospital and provider
that
accepts the plan's payment, terms and conditions
and agrees
to
treat
you -
not
all providers will.
Medicare Special Needs Plan (SNP) - A Medicare
Advantage
Plan
that
has a benefit package designed
for people wi
th
special health care needs. Examples
of
groups served include people wi
th
both Medicare and
Medicaid, reside in nursing homes, and have
ce
r
ta
in
chronic medical conditions.
Additi
on
al Related Products
Medicare Supplement - Medicare Supplement are
standardized plans
that
can
be
bought
wi
th
varying
coverage options. Medicare Supplement plans have no
provider networks and cover some costs
that
Original
Medicare does not pay.
Vision - Vision plans are available
at
varying levels
of
coverage
at
in-network and
out
-
of
-
network
provider
s.
Dental-
Dental plans are available available
at
varying
levels
of
coverage
at
in-network and
out
-of-network
providers.
Hospital Indemnity - Hospital
indemnity
plans cover
some
of
the costs associated
with
hospital stays
that
may
not
be
covered
by
a pri
mary
heal
th
plan.
Please
note,
the
person
who
will di
scuss
the products
is
either employed or contracted by a Medicare pl
an
.
They do
not
work directly for
the
Federal government.
This
individual may
also
be
paid based
on
your enrollment
in
a plan.
Signing this
form
does
NOT
obligate you
to
enroll
in
a plan, affect your curre
nt
enrollment, or enroll you
in
a M
ed
icare plan.
Y0040
GNHHVXDEN
Approved
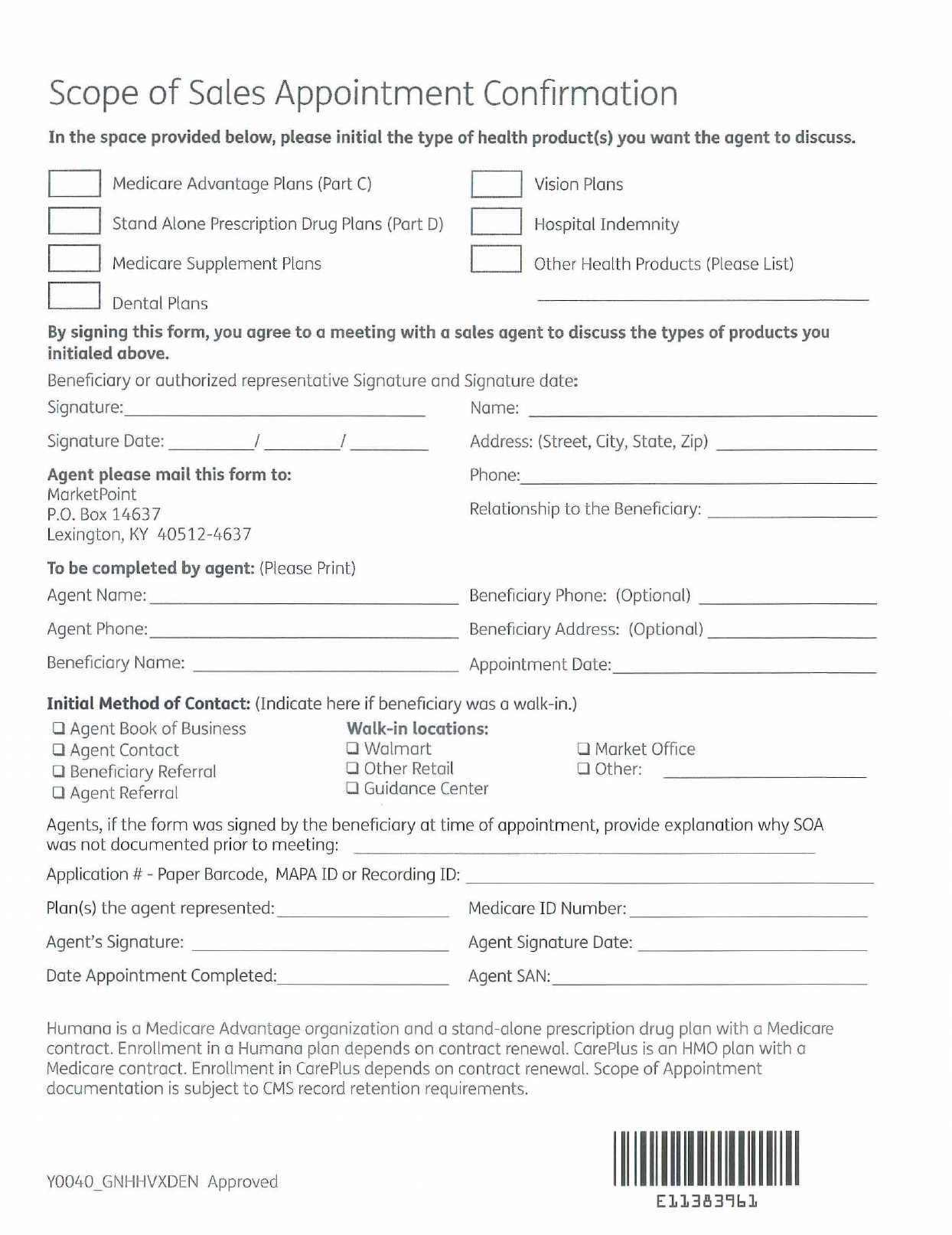
Scope
of
Sales
Appointment
Confirmation
In
the
space provided below, please
in
itial
the
type
of
health product(s) you want the agent
to
discuss.
D
D
D
D
Medicare Advantage Plans
(P
art
C)
Stand Alone
Presc
ri
ption
Dr
ug
Pl
ans (Part
D)
Medicare Supplement
Pla
ns
Dentol
Pla
ns
D
D
D
Vis
ion Plans
Hos
pital
Indemn
i
ty
Other Heol
th
Prod
ucts (Pleose List)
By
signing this form, you agree
to
a meeting with a sales agent to discuss the types
of
products you
initialed above.
Beneficiary or authorized
re
presentative Signature and
Sig
n
at
u
re
date:
Signatu
re:
______________
_
Signature Dat
e:
____
I
__
__
I
___
_
Agent please mail this form
to:
MarketPoi
nt
P.
O.
Box
14637
L
ex
ington, KY 40512-4637
To
be completed
by
agent:
(P
le
as
e Print)
Name:
_______________
_ _
Ad
d
ress:
(Street, C
it
y, State, Zip)
___
__
_ _
Phane:
_______________
_ _
Rela
tionship to
the
Beneficiary:
_____
_ _ _
Agent N
ame
:
____
____
_______
Be
nefi ciary Phone: (Optional)
_____
__
_ _
Agent Phone:
_______________
Bene
ficiary Address: (Optional)
_______
_
Beneficiary Name:
_____________
Appoi
ntm
ent
Date:
____________
_
Initial Method
of
Contact: (Indicate here if beneficiary was a walk-in.)
o Agent Book
of
Busi
n
ess
Walk-in locations:
o Agent Contact 0
Walmart
o Mark
et
Office
o Beneficiary Referral 0 Other Retail
o Agent Referral 0 Guidance Center
o Other:
Ag
e
nt
s,
if
th
e
form
was signed
by
the
benefi ciary
at
tim
e
of
appointment, provide explanati
on
why
SOA
was
nat
docum
e
nt
ed prior
to
meeting:
Application # -
Pop
er Barcode,
MAPA
ID or Recording ID:
__
_
____
_________
_
__
_
Plan(s)
the agent repre
se
nt
ed:
_______
_ Medicare ID Number: _
_________
_
Agent's Signature:
___
___
_
____
_
Agent Signature Date:
_________
_ _
Date Appaintm e
nt
Campleted: _ _
_____
_
Age
nt
SA
N:
____________
_ _
Humana
is
a Medicare Advantage organization and a stand-alone prescription drug plan with a Medicare
contract.
Enrol
lment
in
a Humana plan depends on contract renewal. CarePlus
is
an
HMO
plan wi
th
a
Medicare controct.
Enrollment in
CarePlus
depends
on
contract renewal. Scope
of
Appointment
documentation
is
subject
to
CMS
record retention requirements.
Y0040
GNHHVXDEN
Approved
1
11111111
1
111111
1
El13839
61
Edward MacConnell
(215)355-2121
1532737 NPN 2032257
Name:__________________________________________ Date:____________________________________________
HomeAddress:________________________________________________________________________________
DateofBirth:____________________________________HomeZip:_________________________________
Phone:_________________________________E‐Mail:________________________________________________
MedicationName
Brand/Generic
Dosage Frequency DoctorName City/Town
Notes:
QuestionsorconcernspleasecontactTotalBenefitSolutionsInc.(215)355‐2121
HealthInsuranceComparison&AssessmentForm
NOTE:Thisformisdesignedtohelpusthoroughlyresearchhealthinsurancecoverage.Disclosureisvoluntaryandnotrequiredtogeta
healthinsurancequote.Thisinformationcannotbeusedforeligibilitypurposes,itissimplyacourtesytoprovidethemost
compreŚĞnsivereview
oftheavailablehealthplans.
PLEASERETURN
THISFORMVIASECUREFAX(888)287‐3186
