U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES

Page 2 | Advancing American Kidney Health
CONTENTS
Introduction .......................................................................................................................................................................
I. Executive Summary ......................................................................................................................................................
II. Goals and Objectives ....................................................................................................................................................
III. HHS Initiatives ............................................................................................................................................................
Technical Appendix ........................................................................................................................................................

Page 3 | Advancing American Kidney Health
INTRODUCTION
One of the top healthcare priorities of the Trump Administration—and many other stakeholders in
American healthcare—has been the shift from paying for sickness and procedures to paying for health
and outcomes.
There is no better example of an area that needs this transformation than the way we prevent and treat
kidney disease. Approximately 37 million Americans have kidney disease, and, in 2017 kidney disease was
the ninth-leading cause of death in the United States. The primary form of treatment for kidney failure is
dialysis, which is one of the most burdensome, draining long-term treatments modern medicine has to
oer. I know this personally—as so many Americans do—because my father was on dialysis for years.
Dialysis is also far from sustainable: One hundred thousand Americans begin this treatment each
year, and approximately one in five of them are likely to die within a year. Further, the best option we
currently have to oer those with kidney failure is a kidney transplant, but there are almost 100,000
Americans currently on a waiting list for new kidneys. A kidney transplant saved my father’s life; we
want to make that same outcome possible for many more Americans, while also looking to the future to
develop new, better options.
Today’s status quo in kidney care also carries a tremendous financial cost. In 2016, Medicare fee-for-
service spent approximately $114 billion to cover people with kidney disease, representing more than
one in five dollars spent by the traditional Medicare program.
But there is hope. A system that pays for kidney health, rather than kidney sickness, would produce
much better outcomes, often at a lower cost, for millions of Americans. The Trump Administration
plans to eect this transformation through a new vision for treating kidney disease—Advancing
American Kidney Health—laid out in this document.
We have set three particular goals for delivering on this vision, with tangible metrics to measure
our success:
1. We need more eorts to prevent, detect, and slow the progression of kidney disease, in part by
addressing upstream risk factors like diabetes and hypertension. We aim to reduce the number
of Americans developing end-stage renal disease by 25 percent by 2030.
1. We need to provide patients who have kidney failure with more options for treatment, from
both today’s technologies and future technologies such as artificial kidneys, and make it easier
for patients to receive care at home or in other flexible ways. We aim to have 80 percent of new
American ESRD patients in 2025 receiving dialysis in the home or receiving a transplant.
2. We need to deliver more organs for transplants, so we can help more Americans escape the burdens
of dialysis altogether. We aim to double the number of kidneys available for transplant by 2030.
With the help of many stakeholders, inside and outside of government, HHS has diagnosed the prob-
lems with our system, detailed what success looks like, and laid out how to get there. Over the next
several years, we will execute on the strategies laid out in the following pages: pioneering new payment
models, updating regulations, educating and empowering patients, and supporting new paths for re-
search and development.
This eort will build on the work underway throughout many HHS agencies including ASPR, CDC, CMS,
FDA, HRSA, IHS, and NIH, and will engage outside kidney-care stakeholders and innovators in other fields.
By executing on this bold, comprehensive vision, we can achieve our goals, bring kidney care for all
Americans into the 21
st
century, and show that some of the most stubborn, costly problems in American
healthcare can be solved.
Alex M. Azar II
Secretary of Health and Human Services
Page 4 | Advancing American Kidney Health
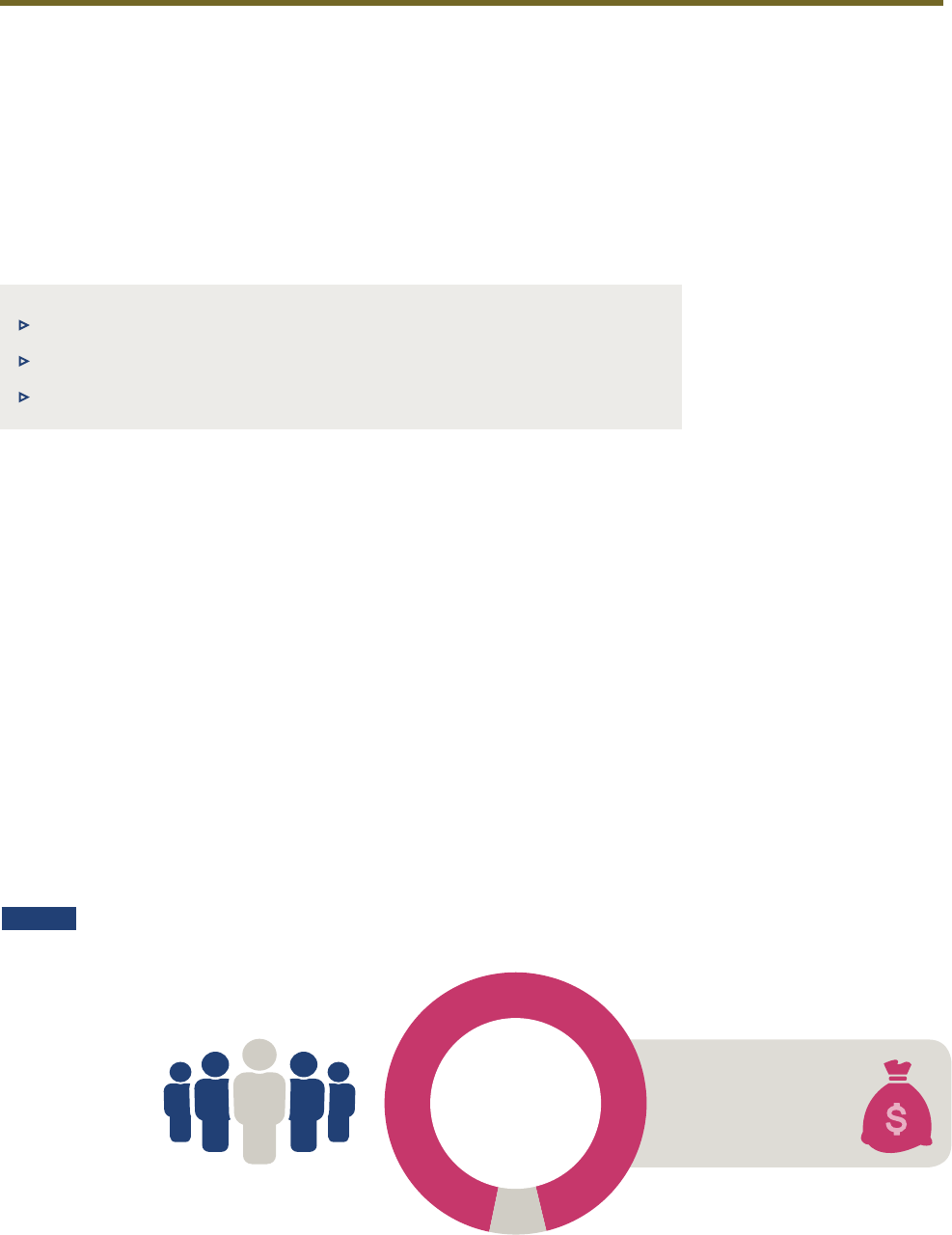
of the total Medicare population
1%
ESRD beneficiaries comprise less than
$35.4
BILLION IN 2016
7%
T
O
T
A
L
M
E
D
I
C
A
R
E
F
F
S
S
P
E
N
D
I
N
G
Medicare spending for ESRD beneficiaries
FIGURE 1
SOURCE: 2018 U.S. Renal Data System Annual Data Report.
I. EXECUTIVE SUMMARY
Goals for Advancing Kidney Health in America
As part of the Administration’s focus on improving person-centered care, the U.S. Department of
Health and Human Services (HHS) is announcing its vision for advancing kidney health to revolution-
ize the way patients with chronic kidney disease and kidney failure are diagnosed, treated, and most
importantly, live. The initiatives discussed in this paper are designed to tackle the challenges people
living with kidney disease face throughout the stages of kidney disease, while also improving the lives
of patients, their caregivers, and family members. The overall goals of these eorts are to:
▶ GOAL 1: Reduce the Risk of Kidney Failure
▶ GOAL 2: Improve Access to and Quality of Person-Centered Treatment Options
▶ GOAL 3: Increase Access to Kidney Transplants
Brief Context on Kidney Disease
Approximately 37 million Americans, or 15 percent of the nation’s adults, have kidney disease.
1
Kidney
disease reduces the ability of a person’s kidneys to filter blood, causing wastes to build up in the body.
In 2017, the ninth leading cause of death in the United States was kidney disease.
2
Major risk factors for kidney disease include uncontrolled diabetes, high blood pressure, and a fam-
ily history of kidney failure. In some individuals, kidney disease progresses to kidney failure, often
referred to as end-stage renal disease (ESRD), which requires dialysis or transplantation to survive.
3
ESRD is a life-threatening illness with a death rate (50 percent mortality in 5 years) worse than most
cancers that significantly aects quality of life. Even ESRD that is well managed with dialysis can
result in premature death or severe disability, heart disease, bone disease, arthritis, nerve damage, in-
fertility, and malnutrition.
4
Infections, including those related to the dialysis procedure, are frequent
causes of hospitalization and death among persons with ESRD. Dialysis treatments also pose a risk of
non-infectious complications. Currently, the only treatment alternative that can restore some or most
of normal kidney function is transplantation, which requires immunosuppressive therapy (to prevent
rejection of the kidney by the recipient’s body) and therefore places recipients at risk for infection and
malignancy due to immunosuppression.
Page 5 | Advancing American Kidney Health
Another indicator of the burden of kidney disease is the financial cost of treatment. Most individuals
with kidney failure are eligible for Medicare coverage, regardless of age.
5
Many Medicare beneficia-
ries with kidney failure suer from poor health status, often resulting from disease complications and
multiple co-morbidities that can lead to high rates of hospital admissions and readmissions.
6
Total
Medicare spending for beneficiaries with chronic kidney disease (CKD) and ESRD, including spending
on comorbidities and other health care services that may be unrelated to ESRD, was over $114 billion in
2016, representing 23 percent of total Medicare fee-for-service (FFS) spending, of which $35.4 billion
was spent on beneficiaries living with ESRD.
7
While less than 1 percent of the total Medicare popula-
tion has ESRD, spending on ESRD beneficiaries accounts for approximately 7 percent of total Medicare
FFS spending.
8
Figure 1 (previous page) shows the proportion of Medicare FFS spending attributable to
Medicare beneficiaries living with ESRD.
Over the past 70 years, there has not been the same level of innovation in treatments for people living
with kidney failure compared to treatments for other health conditions.
9
To improve quality of life
among people living with kidney failure, it is clear that new technological advances and alternatives to
dialysis for renal replacement therapy are urgently needed.
Additional information about kidney disease and its risk factors can be found in the Appendix.
Examples of Key Initiatives to Achieve Goals of the Kidney Care Vision
Eorts across HHS to advance kidney disease prevention and care in the United States include scaling
programs nationwide to optimize screening for kidney diseases, educating patients on care options with
coordinated care networks and other tools, supporting ground-breaking research to inform the next
generation of targeted therapies, creating new payment models and financial incentives to encourage
utilization of home dialysis and increase access to kidney transplants, encouraging accelerated develop-
ment of innovative products such as an artificial kidney, and undertaking a variety of eorts to increase
the number of kidneys available for transplant from both living and deceased donors.
Goal 1: Reduce the Risk of Kidney Failure
Examples of how HHS is addressing Goal 1 include the Indian Health Service’s (IHS’) eorts to adopt a
person-centered approach to care to improve outcomes for American Indians and Alaska Natives (AI/
ANs) at risk for diabetes complications such as kidney failure. The incidence of diabetes-related ESRD
(ESRD-D) among AI/AN populations decreased by over 40 percent between 2000 and 2015, resulting in
lower levels of disease burden for patients and lower spending on ESRD care.
10
The Centers for Disease
Control and Prevention (CDC) is updating its Hypertension Control Change Package for Clinicians to
improve CKD detection and care quality among persons at high risk for CKD progression. CDC is also
investing in state and local eorts to develop a public health response to CKD risk factors such as dia-
betes and heart disease.
11
Goal 2: Improve Access to and Quality of Person-Centered Treatment Options
HHS’ eorts to address Goal 2 include the National Institutes of Health (NIH) Kidney Precision
Medicine Project, which will use kidney biopsies to help redefine kidney disease into new molecu-
lar subgroups, paving the way for personalized treatments. The Oce of the Assistant Secretary for
Preparedness and Response’s (ASPR’s) programs are working to ensure individuals who need dialysis
treatment have ready access to treatment in the aftermath of disaster situations, through the availabil-
ity of portable dialysis technologies. The U.S. Food and Drug Administration (FDA) has cleared devices
for home hemodialysis, and FDA actively supports innovative eorts to improve the quality of current
dialysis treatment and to develop new alternatives to dialysis for renal replacement therapy through its
Breakthrough programs and participation in KidneyX, the Kidney Innovation Accelerator. The Centers
for Medicare & Medicaid Services (CMS) has reviewed potential refinements to the ESRD-Prospective
Payment System to facilitate Medicare beneficiaries’ access to certain innovative treatment options
and, through the Center for Medicare and Medicaid Innovation (Innovation Center), is providing
Page 6 | Advancing American Kidney Health
financial incentives to help clinicians better manage care aligned with beneficiaries’ preferences re-
garding home dialysis and kidney transplantation. CDC is working to translate evidence-based recom-
mendations into practical strategies to improve the quality and safety of care for patients undergoing
dialysis. CDC formed the Making Dialysis Safer for Patients Coalition, through which it collaborates
with partner organizations and patient representatives to implement core interventions proven to re-
duce dialysis bloodstream infections.
12
Goal 3: Increase Access to Kidney Transplants
To advance Goal 3, The Office of the Assistant Secretary for Health (OASH) is considering recom-
mendations from the Advisory Committee on Blood and Tissue Safety and Availability regarding
updating the U.S. Public Health Service Guideline for Reducing Human Immunodeficiency Virus,
Hepatitis B Virus, and Hepatitis C Virus Transmission Through Organ Transplantation, which may
increase available options for individuals who need kidney transplants. The Health Resources and
Services Administration (HRSA) is working to provide additional support for individuals who are
considering living donation by reducing financial barriers. In addition, new Innovation Center
models include financial incentives for health care providers to help Medicare beneficiaries move
through the kidney transplantation process.
Given the substantial burden kidney disease places on patients and their caregivers, it is imperative
that HHS continues to advance improvements and innovations in kidney disease prevention and care.
This paper outlines HHS’ goals for improving kidney care, finding alternatives to current dialysis
treatment, and increasing access to kidney transplants, and it describes agency initiatives designed to
address these goals.

Page 7 | Advancing American Kidney Health
II. GOALS AND OBJECTIVES
Goal 1: Reduce the Risk of Kidney Failure
The number of people with kidney failure has been growing in recent years, aicting more than
726,000 Americans in 2016.
13
Yet, 90 percent of adults with kidney disease and nearly half in advanced
stages of CKD are unaware they have the condition.
14
Associations have been found between diabetes,
hypertension, and CKD. For example, roughly 1 out of 5 adults with hypertension, and 1 out of 3 adults
with diabetes, may have kidney disease.
15
Moreover, among U.S. adults aged 18 years or older, diabetes
and high blood pressure are the primary reported causes of ESRD. Kidney disease usually progress-
es slowly in most individuals, and blood and urine tests can be used to monitor the progression of the
disease. Depending on the person and the stage of the disease, interventions can sometimes slow this
progression. Lifestyle and medication treatment for risk factors including diabetes and hypertension
are also important factors to address the progression of CKD. Two objectives for HHS’ eorts to reduce
the risk of kidney failure are:
OBJECTIVE 1. Advance public health surveillance capabilities and research to improve identification
of populations at risk and those in early stages of kidney disease
OBJECTIVE 2. Encourage adoption of evidence-based interventions to delay or stop progression
to kidney failure
Goal 2: Improve Access to and Quality of Person-Centered
Treatment Options
More than 100,000 Americans begin dialysis each year.
16
Approximately one in five will die with-
in one year, and half within five years.
17
Those with kidney failure typically must undergo dialysis
(often at a dialysis center) at least three times per week for three to four hours per session, or through
daily home peritoneal dialysis or home hemodialysis, and maintain an extremely restrictive diet.
Infections are a serious adverse outcome related to dialysis. Each year, approximately 29,500 blood-
stream infections occur in hemodialysis outpatients, and as many as one in two peritoneal dialysis
patients develops peritonitis.
18
These types of infections can lead to sepsis and can compromise the
patient’s treatment options, including ability to receive a kidney transplant. Eighty-seven percent
of Americans with kidney failure start treatment with hemodialysis. Of those on hemodialysis, the
majority (98 percent) receive in-center hemodialysis and only 2 percent use home dialysis.
19
Up to
85 percent of patients are eligible for home dialysis,
20
and in one study, 25 to 40 percent of patients
reported that they would select home dialysis if given the opportunity.
21
Higher survival has been
reported among individuals in the U.S. receiving home dialysis when compared to individuals receiv-
ing in-center hemodialysis treatment.
22
,
23
,
24
,
25
Supporting person-centered treatment options means
increasing the number of treatment modalities available for individuals living with kidney failure,
including home modalities, transplantation, and other alternatives to in-center hemodialysis still
under development.
Rapidly emerging technologies oer hope that new treatment options can improve patient outcomes
and lower the cost of care. HHS therefore supports eorts to develop and bring to market novel treat-
ments such as wearable, implantable, and/or biohybrid artificial kidneys as well as other biological and
drug-based alternatives to current dialysis treatments.
HHS aims to reduce morbidity and mortality among people living with advanced kidney disease and
increase the proportion of those with kidney failure receiving optimal treatment aligned with their
individual needs and preferences, based on informed patient choice.
OBJECTIVE 1. Improve care coordination and patient education for people living with kidney disease
Page 8 | Advancing American Kidney Health
and their caregivers, enabling more person-centric transitions to safe and eective treatments for
kidney failure
OBJECTIVE 2. Introduce new value-based kidney disease payment models that align health care pro-
vider incentives with patient preferences and improve quality of life
OBJECTIVE 3. Catalyze the development of innovative therapies including wearable or implant-
able artificial kidneys with funding from government, philanthropic and private entities through
KidneyX, and coordinating regulatory and payment policies to incentivize innovative product
development
Goal 3: Increase Access to Kidney Transplants
Nearly 95,000 patients are on the waiting list to receive a kidney transplant.
26
Kidney transplanta-
tion is generally associated with better outcomes compared to dialysis,
27
but only 30 percent of indi-
viduals who have experienced kidney failure are living with a functioning kidney transplant.
28
Many
Americans never have the chance to receive a kidney transplant due to shortages of available kidneys.
Objectives to improve access to kidney transplants are:
OBJECTIVE 1. Increase the utilization of available organs from deceased donors by increasing organ
recovery and reducing the organ discard rate
OBJECTIVE 2. Increase the number of living donors by removing disincentives to donation and ensur-
ing appropriate financial support

Page 9 | Advancing American Kidney Health
III. HHS INITIATIVES
By coordinating across HHS and partnering with people living with kidney disease, their caregivers,
organ donors, health care providers, and other stakeholders, HHS will enhance the ability of people
with kidney disease to improve their day-to-day well-being and quality of life. The specific activities
and initiatives HHS is undertaking to address the goals of this vision are described below.
Goal 1: Reduce the Risk of Kidney Failure
OBJECTIVE 1. Advance public health surveillance capabilities and research to improve identification
of populations at risk and those in early stages of kidney disease
In recent years, HHS has increasingly focused on developing better capabilities to identify kidney
disease early among high-risk patient populations and to support new research to uncover clinical-
ly-useful biomarkers that allow better prediction of the course of CKD and identify patients who could
be helped by particular therapies, or who should not be given specific drugs.
▶ CDC created and manages the national CKD Surveillance System, the only interactive and most
comprehensive collection of CKD-related data in the United States, helpful for monitoring prog-
ress toward achieving national Healthy People
29
objectives. Through its investments in the CKD
Surveillance System and innovative epidemiological research, CDC continues to strengthen
understanding of kidney disease prevalence, risk factors, and health consequences.
Find more information on the CKD Surveillance System at: https://nccd.cdc.gov/ckd/default.aspx
▶ The NIH-funded Chronic Renal Insuciency Cohort (CRIC) Study is examining risk factors
for progression of CKD and cardiovascular disease among patients with established CKD.
Additionally, the study is developing predictive models to identify high-risk subgroups,
informing future treatment trials, and examining the eect of ongoing clinical management
on outcomes. For example, CRIC researchers defined mortality risk subgroups in patients with
CKD based on whether levels of the hormone FGF23 in the blood change over time. FGF23 levels
in the blood were stable over time in most patients with CKD, but distinct subpopulations with
rising FGF23 levels over time were linked to higher risk of death.
Find more information about CRIC at: https://www.niddk.nih.gov/about-niddk/research-areas/
kidney-disease/eects-chronic-kidney-disease-adults-study-cric
▶ Hypertension is a leading cause of kidney disease and is the second leading cause of ESRD,
accounting for 26 percent of ESRD cases.
30
Heart disease can lead to and exacerbate CKD.
Hypertension can lead to kidney disease, which in turn can lead to worsened hypertension. It is
a dangerous cycle that, if not stopped, can lead to a heart attack, stroke, heart failure, or kidney
failure. The landmark NIH-funded Systolic Blood Pressure Intervention Trial (SPRINT) study
showed that lower blood pressure targets decrease the risk of death in high-risk patients with
cardiovascular disease (CVD) and CKD.
31
Find more information on the SPRINT trial at: https://www.nhlbi.nih.gov/science/
systolic-blood-pressure-intervention-trial-sprint-study
▶ Diabetes is another major risk factor for kidney disease. Although testing for kidney disease
is recommended for people with diabetes, almost 60 percent of Medicare beneficiaries with a
diabetes diagnosis are not screened for kidney-damage (albuminuria), and approximately 93
Page 10 | Advancing American Kidney Health
percent of those with hypertension only (a risk factor for kidney disease) are not being tested
for this disease.
32
CDC is collaborating with NIH on the Longitudinal Study of Markers of
Kidney Disease, and with the National Centers for Health Statistics to investigate and validate
new markers for early kidney disease and identify new treatment options for diabetes-related
kidney disease.
Find more information on the Longitudinal Study of Markers of Kidney Disease at: https://www.cdc.
gov/kidneydisease/about-the-ckd-initiative.html
▶ The NIH-funded Kidney Precision Medicine Project seeks to uncover the biological root causes
of kidney disease through high throughput molecular, genetic, and cellular techniques from
research kidney biopsies. This will lead to new biomarkers, disease subgroups, molecular
targets, and most importantly the development of new drugs to treat and possibly forestall
kidney disease. Recruitment of patients for renal biopsy will start in Summer 2019.
Find more information on the NIH-funded Kidney Precision Medicine Project at: https://www.niddk.nih.
gov/research-funding/research-programs/kidney-precision-medicine-project-kpmp
▶ The NIH-funded Preventing Early Renal Loss in Diabetes (PERL) Study is a randomized, dou-
ble-blind trial to test whether the medication allopurinol can slow the progression of kidney
disease in people with type 1 diabetes and early diabetic kidney disease. Results from this study
are expected to be available at the end of 2019.
Find more information about PERL at: http://www.perl-study.org/
▶ Identification of patients with CKD for population health management, research and surveil-
lance using data available in electronic health records (EHRs) is challenged by poor recogni-
tion and resulting under-diagnosis of the disease, particularly in its early stages. As a result,
diagnosis codes cannot be used to accurately identify patients with CKD from the EHR. The
NIH convened researchers, clinicians, and informaticists to develop and validate an electronic
phenotype for CKD. An electronic phenotype is a defined set of data elements and rules that
help identify groups of patients using a computerized query. The resulting NIH CKD pheno-
type uses laboratory measures commonly available in the EHR to identify patients likely to
have CKD.
Find more information on the electronic phenotype at: https://www.niddk.nih.gov/health-information/
communication-programs/nkdep/working-groups/health-information-technology
Looking forward, HHS will further intensify its eorts to make kidney disease detection more accessi-
ble, including:
▶ As part of its CKD Initiative, CDC will continue to collaborate with other government agen-
cies, universities, and national organizations to support a robust portfolio of epidemiological
studies, including cost-eectiveness studies of the long-term ecacy of public health in-
terventions for CKD, and the Systematic Review on Barriers to CKD Screening Project, which
identifies and synthesizes current evidence on kidney disease screening and screening rates in
the United States. These activities support eorts to raise awareness of CKD and its complica-
tions, promote prevention and control of risk factors for CKD, and improve early diagnosis and
treatment among people living with kidney disease.
▶ The CKD Epidemiology in the Military Health System (MHS), a collaborative eort between
the CDC and the Uniformed Services University of the Health Sciences, aims to describe the
epidemiology of kidney disease among the active duty and non-active duty populations and
assess their risk factors for developing kidney disease. Specifically, this project examines 1)

Page 11 | Advancing American Kidney Health
the eects of maintaining good physical and psychological health on risk of CKD, and 2) the
long-term eects of non-sedentary lifestyle on risk of chronic conditions, including CKD.
Because the project includes non-active duty persons, i.e., family members of active duty
individuals and retirees from active duty, the findings will have implications beyond military
personnel.
Find more information on CKD Epidemiology in the MHS at: https://www.cdc.gov/kidneydisease/
about-the-ckd-initiative.html
OBJECTIVE 2. Encourage adoption of evidence-based interventions to delay or stop progression
to kidney failure
In the United States, 30 million individuals have diabetes, 84 million adults have prediabetes (are at
high risk for type 2 diabetes), and 75 million adults have high blood pressure.
33,34
HHS has supported
the development of several evidence-based national models for better managing kidney disease and
risk factors for its progression. These models aim to reduce the national rate of kidney failure.
▶ American Indian/Alaska Native (AI/AN) populations have the highest prevalence of diabetes
of any U.S. racial/ethnic group.
35
The Special Diabetes Program for Indians (SDPI) represents
an important part of this broader approach to providing team-based care and care manage-
ment. The program has included a number of dierent components over time such as com-
munity directed grants that focus on locally developed solutions to improve diabetes preven-
tion and care, demonstrations and initiatives such as the SDPI Diabetes Prevention Initiative,
which built on the findings of an earlier clinical trial at NIH, the diabetes audit which collects
data on diabetic care provided by grantees to track outcomes, dissemination of diabetes
treatment algorithms and standards of care, and ongoing educational programs such as
webinars, periodic meetings and conferences, and consultations with health professionals
that have expertise in diabetes. Since its implementation, the incidence of diabetes-relat-
ed kidney failure among AI/AN populations decreased by over 40 percent between 2000 and
2015, resulting in lower spending for programs that cover the costs of AI/AN ESRD care.
36
The
SDPI and related eorts have also contributed to improvements in other diabetes-related
outcomes, including childhood obesity trends,
37
hospitalizations for uncontrolled diabetes,
38
and diabetic retinopathy.
39
Find more information on the SDPI at: https://www.ihs.gov/sdpi
▶ The CDC’s National Diabetes Prevention Program (National DPP) is a partnership of public and
private organizations working together to build a nationwide delivery system for a 12-month
lifestyle change program proven to prevent or delay onset of diabetes.
40
Congress specifically
authorized the National DPP in 2010 because of previous research—including the NIH-funded
Diabetes Prevention Program (DPP) and the DPP Outcomes Study —that demonstrated the
potential of the CDC-recognized lifestyle change program to prevent or delay the onset of type
2 diabetes. The National DPP is founded on four key pillars: 1) a trained workforce of lifestyle
coaches; 2) national quality standards supported by the CDC Diabetes Prevention Recognition
Program; 3) a network of program delivery organizations sustained through health benefit
coverage; and 4) participant engagement and referral. CDC also supports states’ eorts to
make the NDPP and other diabetes management interventions available to high-burden pop-
ulations and communities. These eorts include strengthening community-clinical linkages
to screen, test, and refer people with prediabetes to CDC-recognized organizations oering the
National DPP lifestyle change program; providing support to enroll and retain participants in
the program; and supporting pharmacist-patient care processes that help people with diabetes
better manage their medications.
Find more information on the CDC’s National DPP at: http://www.cdc.gov/diabetes/prevention

Page 12 | Advancing American Kidney Health
▶ The NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) promotes an
integrated health system model of team-based clinical care based on the pragmatic experience
of the IHS’ Kidney Disease Program. NIDDK has developed new clinical tools and educational
programs that improve the care of people with kidney disease in primary care settings. NIDDK
works in collaboration with government, nonprofit, and health care organizations to raise
awareness about screening for individuals at risk for kidney disease; educate individuals about
how to manage their disease; provide information, training, and tools that help health care
providers; and support important health systems changes.
Find more information on the NIH NIDDK at: http://www.niddk.nih.gov
▶ The Innovation Center’s Medicare Diabetes Prevention Program (MDPP) expanded model is
a structured behavior change intervention that aims to prevent the onset of type 2 diabetes
among Medicare beneficiaries with an indication of prediabetes. This model is an expansion of
the Diabetes Prevention Program model test under the authority of section 1115A of the Social
Security Act.
Find more information on the MDPP at: https://innovation.cms.gov/initiatives/medicare-diabetes-
prevention-program/
Looking forward, HHS will continue to support these programs and look for known and innovative
ways to scale their adoption, in partnership with communities.
▶ In late 2017, CDC announced a new five-year cooperative agreement to scale up the National
DPP in underserved areas and populations including Medicare beneficiaries, men, African
Americans, Asian Americans, Hispanics, American Indians, Alaska Natives, Pacific Islanders,
and noninstitutionalized people with visual impairments or physical disabilities.
▶ In late 2019, CDC will update its Hypertension Control Change Package for Clinicians (HCCP) to
include tools and resources to support CKD screening and early diagnosis among persons with
hypertension. This eort, part of CDC’s broader Million Hearts® initiative,
41
will better sup-
port clinician eorts to end the pernicious cycle between CKD and hypertension.
Find more information on the Hypertension Control Change Package for Clinicians at:
https://millionhearts.hhs.gov/files/HTN_Change_Package.pdf
Find more information on the Million Hearts initiative at: https://millionhearts.hhs.gov
▶ CDC has begun a collaboration with local health departments to develop innovative approaches
to increase the reach and eectiveness of public health strategies for diabetes, heart disease,
and stroke, including the use of clinical decision support tools within EHRs to promote early
detection of kidney disease.
▶ HHS supports continued funding for the SDPI, as reflected in the President’s Fiscal Year (FY)
2020 budget that proposes reauthorizing the SDPI at $150 million per year through FY 2021.
▶ NIH has recently funded the Improving Chronic Disease Management with Pieces (ICD-Pieces)
study, testing whether computer-generated reminders working in tandem with clinicians can
reduce hospitalizations in patients with coexisting CKD, diabetes, and hypertension, and im-
prove use of innovative and proven interventions.
Find more information on the ICD-Pieces study at: http://icd-pieces.com/
▶ ASPR is launching a new initiative called ExaHealth, to develop collaborative tools to acceler-
ate discovery of new therapies. The ExaHealth initiative will be one of many partnerships with
the Department of Energy to develop artificial intelligence tools and new methods for studying
Page 13 | Advancing American Kidney Health
complex biological functions in a concerted way, in order to develop new and more eective med-
ical interventions. These interventions will focus on acute onset of disease during pandemics and
man-made disasters, as well as and chronic diseases, whose onset can occur throughout a per-
son’s lifetime, including patients at risk for progression towards CKD and ESRD.
Goal 2: Improve Access to and Quality of Person-Centered
Treatment Options
OBJECTIVE 1. Improve care coordination and patient education for people living with kidney disease
and their caregivers, enabling more person-centric transitions to safe and eective treatments for
kidney failure
HHS supports the data and knowledge infrastructure necessary to inform more person-centric transi-
tions to safe and eective care for kidney failure.
▶ For example, the NIH supports production of the annual U.S. Renal Data System (USRDS) Atlas,
which provides up-to-date statistics on incidence, morbidity, and mortality for patients transi-
tioning through kidney failure. These data have been used to inform clinical practice for kidney
disease patients and development of targeted interventions for specific populations. In 2018,
USRDS published a special transitions section that describes the transition from CKD to ESRD
in greater detail using linked data from the Veterans Health system. Key summary findings
include the finding that heart failure and acute kidney injury (AKI) are the most common cause
of hospitalizations in the six months before the start of hemodialysis, and infectious compli-
cations (vascular access infection, septicemia) are the most common causes of hospitalizations
after the start of hemodialysis.
42
Future eorts of the USRDS include a detailed investigation
of causes of early mortality among patients who start hemodialysis, as well as expanded ex-
ploration of data sets other than Medicare data to support additional analyses related to kidney
disease and kidney care.
Find more information on the USRDS at: https://www.usrds.org/
▶ Through its Making Dialysis Safer for Patients Coalition, CDC coordinates a wide array of orga-
nizations and individuals to promote implementation of evidence-based interventions to pre-
vent dialysis bloodstream infections. Best practices and strategies for implementation of these
interventions include provider training and feedback, patient engagement and empowerment,
and use of audit tools, checklists, and other resources. These interventions have been shown to
significantly reduce dialysis-related bloodstream infections (by 30 to 50 percent) and associat-
ed outcomes.
43
Find more information on the Making Dialysis Safer for Patients Coalition at: https://www.cdc.gov/
dialysis/coalition/index.html
▶ Through the National Healthcare Safety Network (NHSN), CDC tracks bloodstream infections –
including those caused by antibiotic resistant organisms, vascular access infections, and other
outcomes among hemodialysis patients treated in clinics, and gives clinics immediate access
to the data reported. CDC produces standardized infection ratios that are posted publicly on
Medicare’s Dialysis Facility Compare website. National aggregate rates of infection are used for
benchmarking and in quality improvement initiatives.
Find more information on NHSN at: https://www.cdc.gov/nhsn/dialysis/index.html
▶ ASPR and CMS have formed a collaboration to improve access to dialysis care during every di-
saster and have launched the emPOWER program. emPOWER provides data and mapping tools

Page 14 | Advancing American Kidney Health
to help communities protect the health of more than 4.1 million Medicare beneficiaries who rely
on electricity-dependent medical equipment and healthcare services, including nearly 400,000
dialysis patients. In the wakes of Hurricanes Irma and Maria, the emPOWER Program helped
ASPR, CMS, and territorial public health ocials identify healthcare and resource gaps for dial-
ysis patients and immediately engage with End-Stage Renal Networks
44
and dialysis providers
to ensure continuity of their life-maintaining healthcare services.
Find more information on the emPOWER Program at: https://empowermap.hhs.gov/Fact Sheet_
emPOWER_FINALv5_508.pdf
Looking forward, HHS will continue to strengthen patient voices in policy development, address the
needs of vulnerable populations with portable dialysis technologies, and use payment incentives to
support patients making choices about their kidney care modalities.
▶ The Innovation Center has announced four new optional kidney care models: Kidney Care
First (KCF) for nephrology practices and Comprehensive Kidney Care Contracting (CKCC)
which oers three distinct payment options. These models will build on the existing
Comprehensive ESRD Care (CEC) Model, which began in 2015 and will end in 2020, and incor-
porate design elements from the recently announced Direct Contracting and Primary Care
First models. One of the key lessons learned from the CEC Model was the need to increase
coordinated care for beneficiaries with late-stage chronic kidney disease and beneficiaries
transitioning onto dialysis. These models will provide strong incentives to better manage
and coordinate care for beneficiaries with kidney disease. Model participants will be incen-
tivized through utilization measures and cost incentives to avoid unplanned dialysis starts in
the hospital, in an eort to avoid the cost and high mortality that occurs when beneficiaries
abruptly start dialysis. Additionally, CMS will also establish measures to demonstrate wheth-
er kidney disease is being delayed by the Model’s interventions and develop a quality measure
to incentivize better managing beneficiaries with late-stage CKD to avoid the more expensive
and burdensome dialysis process.
Find more information on the CKC Model at: https://innovation.cms.gov/initiatives/voluntary-
kidney-models/
▶ The FDA is developing a new survey to gain insight into patient preferences for new kidney
failure treatments. Information collected will be used by FDA and its partners including
device developers, patients, providers, payers, and other researchers to inform the develop-
ment of new treatments, including alternatives to dialysis. The patient preferences survey
will be an important example of how patient engagement can contribute to building infra-
structure for expanded patient-centered outcomes research and how patient input can be
used in FDA’s review processes. Results and methods will also be shared with those involved
in data collection efforts for other disease conditions to similarly inform the development of
new treatments.
▶ NIH is developing and testing an interoperable open-source electronic care plan tool for peo-
ple with multiple chronic conditions, including diabetes and kidney disease, to better coordi-
nate their care. In the context of kidney care, this tool will enable patients, physicians, nurses,
pharmacists, dieticians, and other health professionals, as well as community health workers,
to transfer critical, person-centered kidney care information across multiple settings of care
with diverse electronic health record systems using uniform data standards, supporting better
coordination of kidney care and research.
▶ Dialysis facilities are currently required to inform patients of their care options. To strengthen
patient education and support for patients’ selection of treatment modalities, CMS is consid-
ering options for new ways to improve quality of life for dialysis patients while also reducing
Medicare costs and minimizing regulatory burden.

Page 15 | Advancing American Kidney Health
▶ ASPR is working to ensure people living with kidney failure have access to readily available
portable dialysis technologies and access to treatments in any situation. Currently, treatment
options are limited following disaster events, and individuals on dialysis must be evacuated
and provided temporary housing to continue treatments. Beginning in 2019, ASPR will procure
and test portable dialysis units that can provide support to people living with kidney failure in
low-resource settings or within their homes, so that they can have access to dialysis with min-
imal power and from publicly-available water sources, allowing them to return home sooner
when a disaster occurs.
▶ CMS supports person-centered optimal starts for individuals living with ESRD. An “optimal
start” reflects adequate patient preparation resulting in pre-emptive transplant, initiation
of renal replacement with peritoneal dialysis or initiation of hemodialysis with a functioning
permanent vascular access. The Innovation Center is announcing the ESRD Treatment Choices
(ETC) Model, which will include financial incentives for ESRD facilities and Managing Clinicians
selected to participate in the model to better align with beneficiary choice on modalities such as
home dialysis or kidney transplants.
Find more information on the ETC Model at: https://innovation.cms.gov/initiatives/
esrd-treatment-choices-model/
OBJECTIVE 2. Introduce new value-based kidney disease payment models that align health care pro-
vider incentives with patient preferences and improve quality of life
As part of HHS’ commitment to transition to payment and delivery models that focus on patient out-
comes, preferences, and lowering costs, CMS is introducing a new payment model and has proposed
another payment model to encourage more coordinated care to delay kidney failure and ensure that
people living with kidney failure have access to the best available care options. Additionally, Medicare
will continue to support payment rule changes for the ESRD PPS that focus on patient care, support
innovation, reduce burdens, and lower costs.
▶ The Innovation Center’s ETC Model includes financial incentives for ESRD facilities and
Managing Clinicians selected to participate in the model to better align with patient choice
regarding home dialysis and kidney transplantation. The ETC Model will test the eective-
ness of outcomes-based payment adjustments to health care providers to increase utiliza-
tion of home dialysis and kidney/kidney-pancreas transplants. The Home Dialysis Payment
Adjustment (HDPA) would be in eect for the first three years of the Model, and would in-
crease payment for home dialysis and home dialysis-related services. The Performance
Payment Adjustment (PPA) would decrease or increase payment for dialysis and dialysis-re-
lated services based on a participating ESRD facility or Managing Clinician’s rate of home di-
alysis and transplants. The goal of the Model is to increase the transplant and home dialysis
rate across the country.
▶ The Innovation Center’s optional kidney care models (KCF and CKCC) include incentives for
health care providers to better manage the care for beneficiaries with kidney disease including
incentives for pre-emptive transplants, improving beneficiaries’ transition to dialysis, and en-
suring dialysis initiation is appropriately timed. The Model also includes incentives to manage
the total cost and quality of care for beneficiaries with kidney disease and kidney failure, and
strong financial incentives to move beneficiaries through the transplant process. Together
with the new ETC Model, the optional kidney care models demonstrate CMS’ commitment to
supporting high quality, coordinated care for people living with ESRD.
▶ CMS is considering ways to encourage ESRD facilities to furnish new and innovative drugs and bi-
ological products for the treatment of ESRD. The Transitional Drug Add-on Payment Adjustment
(TDAPA) is an add-on payment adjustment under the ESRD PPS intended to facilitate this goal for

Page 16 | Advancing American Kidney Health
Medicare beneficiaries. This is done by encouraging ESRD facilities to furnish certain qualifying
new renal dialysis drugs and biological products by allowing additional payment for them while
utilization data is collected.
▶ CMS recognizes that continual refinement of the ESRD PPS is necessary to benefit people living
with ESRD, and is therefore working with an analytical contractor to perform payment analysis
and develop potential refinements to the ESRD PPS. CMS plans to ask for stakeholder input on
data collection.
▶ Based on comments received during and after the CY 2019 ESRD PPS rulemaking, CMS is con-
sidering issues related to payment for new and innovative supplies and equipment that are renal
dialysis services furnished by ESRD facilities for ESRD beneficiaries.
OBJECTIVE 3. Catalyze the development of innovative therapies including wearable or implant-
able artificial kidneys with funding from government, philanthropic and private entities through
KidneyX, and coordinating regulatory and payment policies to incentivize innovative product
development
Ultimately, the best way to improve care for people living with kidney failure is to support the devel-
opment of novel therapies extending beyond the choices available today. Investing in foundational
research at the NIH, catalyzing rapid product development through public-private partnerships, and
creating clear and forward-looking guidelines for marketing approval for emerging technologies like
organ preservation may unleash innovation for years to come.
▶ KidneyX was ocially launched in 2018 as a public-private partnership with the American Society
of Nephrology to support the development of innovative therapies and diagnostics. KidneyX
is designed to leverage rapidly emerging technologies in areas such as regenerative medicine,
nanotechnology, and advanced materials to support early-stage development and lower the risk
of commercialization. KidneyX’s first prize, Redesign Dialysis, oers $2.6M for kidney failure
treatments beyond currently available options of dialysis and transplantation. Included among
the 15 winning teams announced in April 2019, were companies developing advanced nanofiltra-
tion for toxin removal, miniaturized wearable dialyzers, real-time infection and clotting sensors,
cell-based implantable dialyzers, and regenerative kidneys. The second phase currently under-
way will seek testable prototypes and announce winners in April 2020.
Find more information on KidneyX at: https://www.kidneyx.org
▶ In June 2019, the HHS Chief Technology Ocer signed an agreement with the heads of CMS,
NIH, FDA, and CDC to work closely together on KidneyX to ensure that unnecessary barriers to
patient access for innovative technologies are addressed. In July 2019, KidneyX is also launch-
ing a patient innovator prize focused on identifying and scaling new products and practices that
patients and caregivers have developed for their own care, recognizing that innovation often
happens at the frontlines of health. In 2020, KidneyX plans to launch Redesign Dialysis Phase
III to advance new products into human clinical trials, another prize focused on helping dialysis
patients manage fluids, a leading cause of ESRD hospitalizations, and a prize focused on spur-
ring development of therapies to slow progression of kidney disease.
▶ HHS and the Department of Veterans Aairs (VA) are exploring a partnership to streamline and
expedite clinical trials for kidney care-related treatments using the VA health system, similar
to the National Cancer Institute (NCI) and VA Interagency Group to Accelerate Trials Enrollment
(NAVIGATE), a partnership between the VA and the NCI to facilitate enrollment of veterans with
cancer into NCI-funded clinical trials.

Page 17 | Advancing American Kidney Health
▶ In May 2019, FDA issued final guidance that industry should consider when utilizing animal
studies to evaluate organ preservation devices. This guidance will help support the develop-
ment of next-generation organ preservation devices and systems, potentially capable of in-
creasing the supply of transplantable kidneys by salvaging and maintaining more kidneys. In
addition to recommendations that could be considered relevant for most animal studies such
as developing animal study protocols with consideration of the applicability of anatomical,
physiological, and immunological factors for humans, studies should include a control group
as a comparator. Specifically, for kidney preservation devices, animal studies should consid-
er three phases of the organ for transplantation: procurement, preservation, and reperfusion.
Following these recommendations will speed the review of kidney preservation devices, as well
as potentially improving the quality and functionality of these devices.
Find the FDA’s final guidance at: https://www.fda.gov/regulatory-information/search-fda-guidance-
documents/utilizing-animal-studies-evaluate-organ-preservation-devices
Goal 3: Increase Access to Kidney Transplants
OBJECTIVE 1. Increase the utilization of available organs from deceased donors by increasing organ
recovery and reducing the organ discard rate
From 2007 through 2017, the annual rate of kidneys procured but not transplanted has ranged between
18-20 percent. In 2017, the discard rate of 18.9 percent reflected 3,534 kidneys that were procured but
not transplanted into waiting patients.
45
Some donor kidneys are not transplanted due to medically
justifiable reasons; however, it is estimated that thousands of discarded kidneys could provide benefit
to people on dialysis.
46
Education about the appropriate clinical use of kidneys would help maximize
the limited supply of donated organs used.
47
,
48
Addressing the availability and utilization of kidneys is
one of the ways HHS can help people living with ESRD through transplantation.
▶ HRSA supported a Collaborative Innovation and Improvement Network (COIIN) pilot project
through the Organ Procurement and Transplantation Network (OPTN) with a limited number of
participating kidney transplant programs. The goal was to increase transplantation and reduce
the number of discarded kidneys, with a particular focus on increasing utilization of kidneys
deemed to be moderate-to higher-risk due to their clinical characteristics. In addition to sup-
porting education of transplant program sta, patients, and referring physicians on the eec-
tive use of these organs, the COIIN pilot also modified OPTN performance monitoring criteria
to reduce the risk-avoidance behaviors associated with the current monitoring system. Initial
results suggest that the COIIN pilot has resulted in increased utilization of kidneys among the
first cohort of participating transplant programs. It is possible that a recent decline in the dis-
card rate of moderate-risk kidneys may in part be related to the COIIN pilot.
Find more information on the HRSA COIIN at: https://optn.transplant.hrsa.gov/resources/coiin/
▶ The OPTN implemented a policy change in June 2018 to expedite the process of allocating organs
and improve the eciency of organ placement. This change reduces the amount of time a trans-
plant program has to accept or refuse an organ oer, as well as reduces bottlenecks in the system
by limiting the number of organ oers a program can accept for any candidate at the same time.
▶ CMS added a transplant waitlist measure to the ESRD Quality Incentive Program (QIP) for di-
alysis facilities via rulemaking in 2018 as a measure of dialysis center performance. The goal
of the ESRD QIP is to promote high-quality services in ESRD facilities treating patients with
ESRD. Under this value-based purchasing program, CMS pays for ESRD treatment by linking
a portion of payment directly to dialysis facilities’ performance on quality of care measures.
A list of CMS quality measures for ESRD care is included in the Appendix.
Page 18 | Advancing American Kidney Health
Looking forward, HHS plans to take a number of actions directly aimed at increasing the utilization
and availability of organs.
▶ HHS is updating the PHS Guideline for Reducing Human Immunodeficiency Virus, Hepatitis
B Virus, and Hepatitis C Virus Transmission Through Organ Transplantation. The goal of the
existing 2013 Guideline was to reduce risk of unintended HIV, HBV, and HCV transmission, while
preserving availability of high quality organs: Since 2013, however, shifts in the composition of
the donor pool, as well as advances in testing and treatment technologies, have created oppor-
tunities to revise the Guideline. The current initiative will re-evaluate and, where warranted,
revise elements of the Guideline based on current risks to patients and improvements in tech-
nology. HHS is also considering the April 2019 recommendations of the Advisory Committee
on Blood and Tissue Safety and Availability concerning revising the Guideline. The revised
Guideline is intended to strengthen the overall process for assessing, communicating, and
managing donor risk for HIV, HBV, and HCV.
Find the current PHS Guideline at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3675207/pdf/
phr128000247.pdf
▶ HRSA has funded the OPTN to expand the COIIN pilot project in 2020, allowing more kidney
transplant programs to participate in this OPTN quality improvement activity focused on
changing program waitlist management and organ acceptance practices.
49
▶ The Innovation Center’s ETC Model includes a learning collaborative operated by the Center
for Clinical Standards and Quality (CCSQ), designed in collaboration with HRSA and informed
by the HRSA OPTN COIIN, to reduce the disparity in performance among Organ Procurement
Organizations (OPOs) and transplant centers with the goal of increasing recovery of kidneys
by OPOs and utilization of kidneys by transplant centers. This quality improvement learning
component will bring HRSA, CMS, transplant centers, OPOs, and the nation’s largest donor
hospitals together to generate increased quality and cost-savings to Medicare through the use
of systematic quality and process improvement. Additionally, this activity will directly engage
patients and families to motivate, activate and empower them to drive the requirement/demand
for utilization of viable kidneys.
▶ HHS is organizing a federal workshop to discuss considerations related to the use of Hepatitis
C virus positive (HCV+) donor organs in recipients who do not have HCV. Due to the recent
increase in the number of deaths from the opioid epidemic, more HCV+ potential organs are
available. HCV is now considered to be largely curable with the advent of direct acting anti-vi-
ral (DAA) therapy. Ten clinical trials are in process or have been completed to study whether
intentional use of HCV+ donor organs in HCV uninfected recipients is safe and eective when
recipients are proactively treated with DAA agents. The planned federal workshop is intended
to help facilitate a proactive and coordinated approach to developments in this area of study,
specifically with regards to potential changes in the standard of clinical care in transplantation.
▶ NIH research led to the seminal discovery of the APOL1 gene, which explains why kidney disease
progresses faster among African Americans compared to Caucasians. Building on the discovery
of the APOL1 gene in African Americans, NIH founded the APOLLO initiative, which will produce
information about the best use of donor kidneys with APOL1 gene variants and also improve do-
nor-recipient matching to decrease the rate of organ discard. OPOs nationwide are participating in
this study. Recruitment began in 2019 and will continue at least through 2021. More precise quan-
tification of risks of poor outcomes related to donor/recipient genetic architecture will enhance the
ecacy of the allocation of precious donor kidneys. Study results are anticipated in 2023.
Find out more information on the APOLLO initiative at: https://theapollonetwork.org/info.cfm

Page 19 | Advancing American Kidney Health
▶ HRSA, through the OPTN, is developing a new model to test accelerated placement of certain
kidneys that are at high risk for discard. Following recommendations from the National Kidney
Foundation Consensus Conference,
50
the OPTN Organ Center will develop and test a proof of
concept for expediting allocation of these organs with safety monitoring. The OPTN will evalu-
ate the concept for safety and improvements in allocation eciency.
▶ HHS is analyzing and improving transplantation metrics with a focus on increasing organ utili-
zation while maintaining good outcomes.
▶ HRSA, through the OPTN, convened an Ad Hoc System Performance Committee, which among
other issues, has discussed new potential performance metrics that monitor patient safety
while encouraging innovative practice.
▶ Per the 2019 OMB regulatory agenda, CMS is reviewing the OPO conditions for coverage and will
be proposing changes to the standards used to evaluate OPOs to ensure proper data collection
on the availability of transplantable organs and transplants.
▶ CMS has begun to develop and test new dialysis facility transplant referral measures, which, if
approved, could be added to Quality Incentive Program (QIP) through rulemaking in the future
and then via the Consolidated Renal Operations in a Web-enabled Network (CROWNWeb) sys-
tem and ultimately, Dialysis Facility Compare.
51
OBJECTIVE 2. Increase the number of living donors by removing disincentives to donation and en-
suring appropriate financial support
Living donors account for 30 percent of all kidney transplants in the U.S. However, many financial and
risk-based disincentives to donation persist, which may serve as barriers for individuals who would
otherwise be willing to donate a kidney.
▶ To further support living donors, HRSA is planning to expand the Reimbursement of Travel
and Subsistence Expenses toward Living Organ Donation program by increasing the eligibility
income threshold. HRSA is implementing a pilot to expand the qualifying expenses to include
coverage for lost wages and family expenses. The expansion of the current reimbursement pro-
gram will reduce financial barriers to organ donation and support the goal of increasing living
donor transplants.
Find more information on the Reimbursement of Travel and Subsistence Expenses toward Living
Organ Donation program at: https://grants.hrsa.gov/2010/Web2External/Interface/Common/
EHBDisplayAttachment.aspx?dm_rtc=16&dm_attid=49472bf1-7438-42-b406-d597fcf3b498
▶ In FY 2019, HRSA awarded a demonstration cooperative agreement to provide for reimburse-
ment of up to $5,000 in lost wages related to donor evaluation and surgical procedures regard-
less of the donor’s income. Findings from this three-year demonstration project will inform
whether expansion of the Reimbursement of Travel and Subsistence Expenses toward Living
Organ Donation program has a positive eect on kidney donation.
Page 20 | Advancing American Kidney Health
TECHNICAL APPENDIX
Background Information on Kidney Disease
Prevalence of Chronic Kidney Disease (CKD) and End-Stage Renal Disease (ESRD)
Kidney disease occurs when kidneys are damaged and become unable to filter blood optimally, causing
wastes to build up in the body. The condition is clinically categorized into five stages as the disease
progresses. The last stage of the disease occurs when the kidneys stop working altogether, which is of-
ten referred to as ESRD. Individuals in this stage of the disease require ongoing dialysis, if a transplant
is not available, in order to filter wastes out of the body.
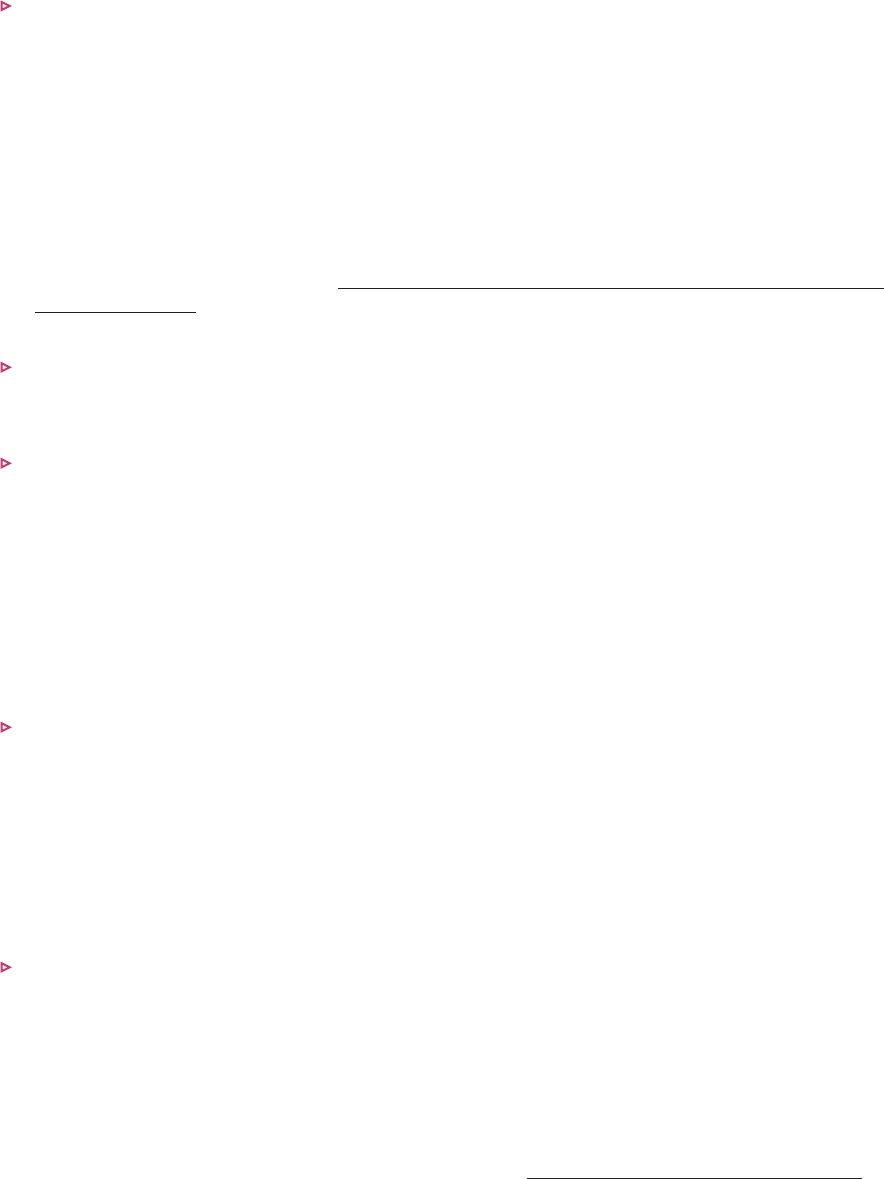
Figure 2 shows the prevalence of CKD in the U.S. population for stages 1 through 4 of the disease.
52
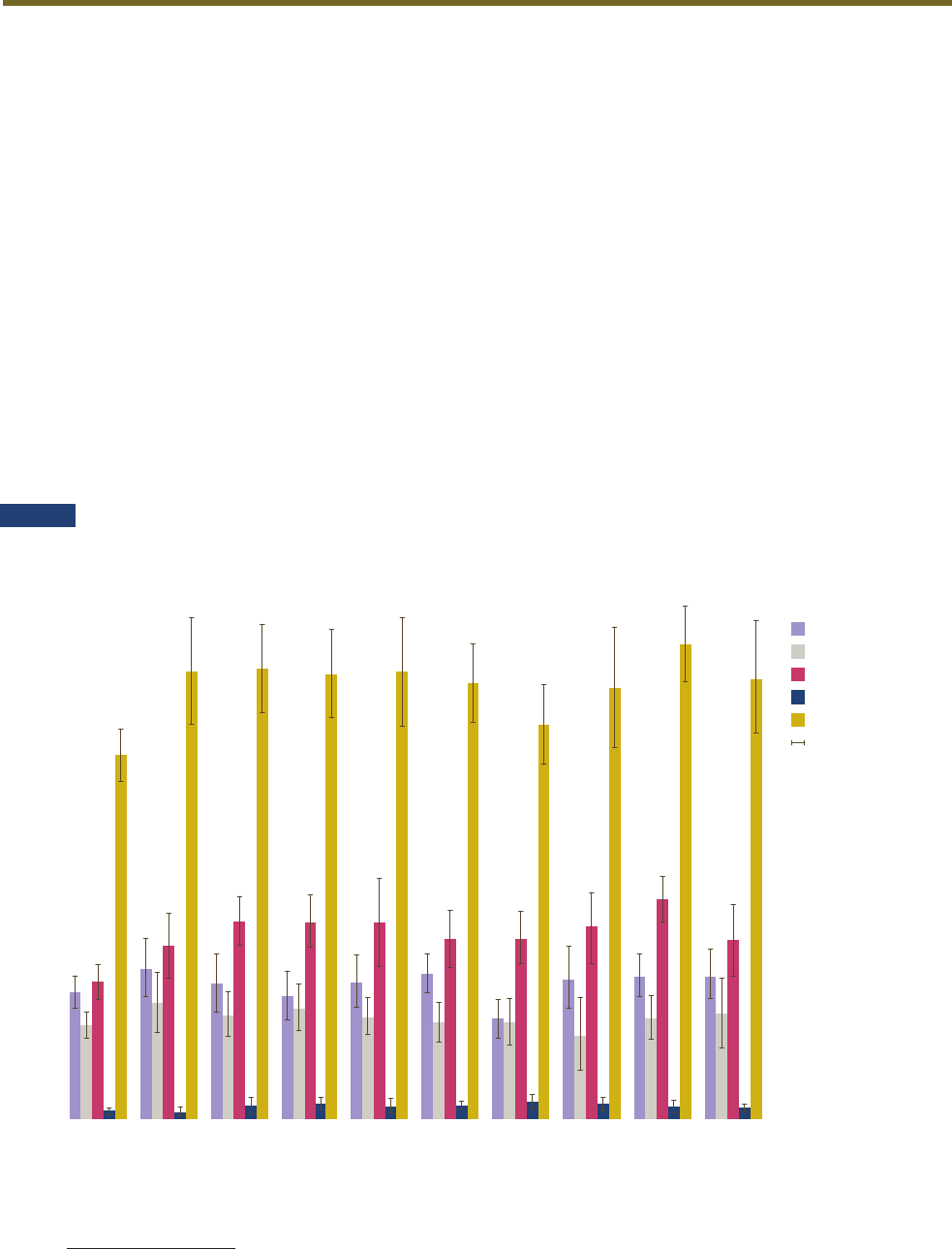
Figure 3 shows the disproportionate prevalence of the disease among older and minority individuals.
Prevalence of CKD by Stage, 1988-2016
FIGURE 2
SOURCE: Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States.
Website. https://nccd.cdc.gov/CKD.
YEAR
PERCENTAGE/PREVALENCE
1999-2000
2001-2002
2003-2004
2005-2006
2007-2008
2009-2010
2013-2014
2011-2012
2015-2016
1988-1994
CKD Stage 1
CKD Stage 2
CKD Stage 3
CKD Stage 4
Stages 1-4
Confidence Intervals
Page 21 | Advancing American Kidney Health
FIGURE 3
Percentage of CKD Among U.S. Adults Aged 18 Years and Older, by Sex and Race/Ethnicity
18-44
45–64
65+
Men
Women
Non-Hispanic whites
Non-Hispanic blacks
Non-Hispanic Asians
Hispanics
0 5 10 15 20 25 30 35 40
PERCENTAGE
SOURCE: Centers for Disease Control and Prevention. Percentage of CKD stages 1–4 among US adults aged 18 years or older using data
from the 2013–2016 National Health and Nutrition Examination Survey and the CKD Epidemiology Collaboration (CKD-EPI) equation.
NIH research led to the seminal discovery of the APOL1 gene, which explains why CKD progresses faster
among African Americans compared to Caucasians.
53
As of December 31, 2015, the prevalence of dialysis treatment was 1,470 per million U.S. population.
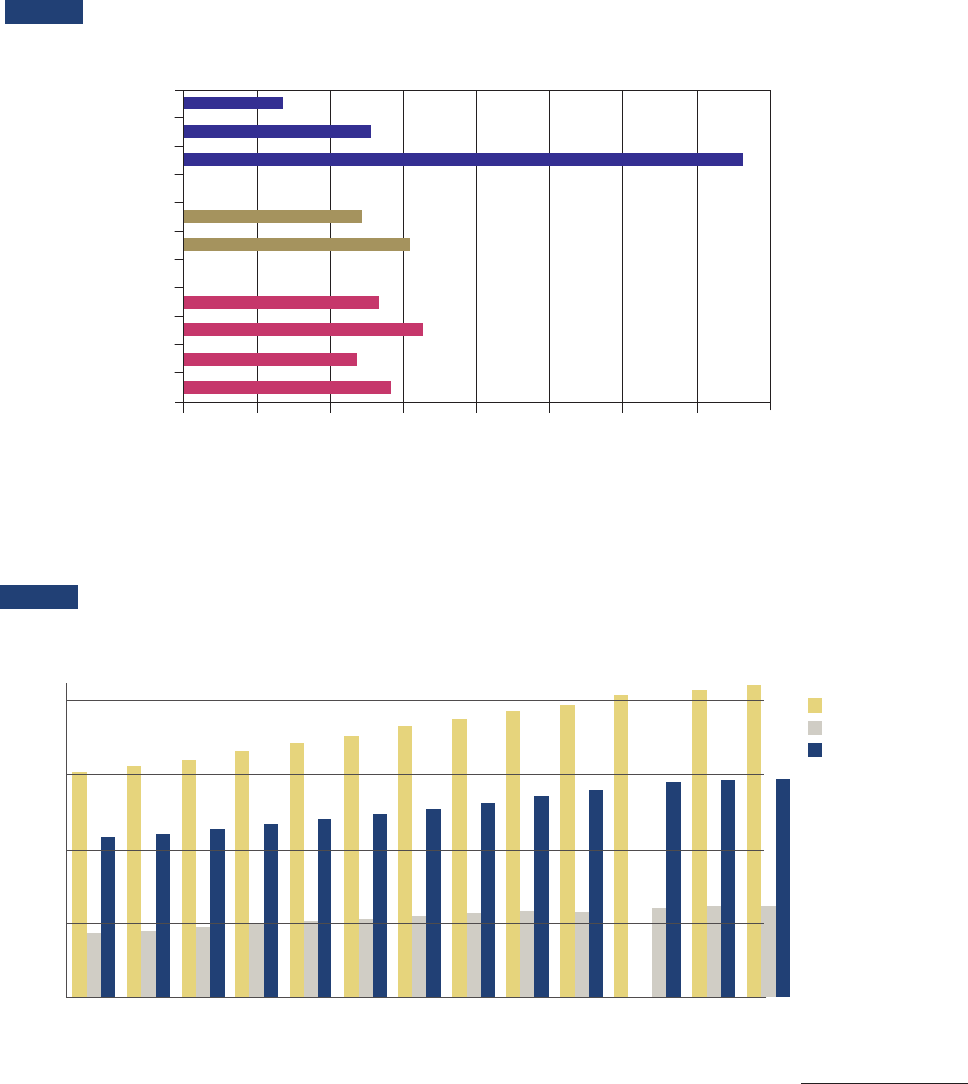
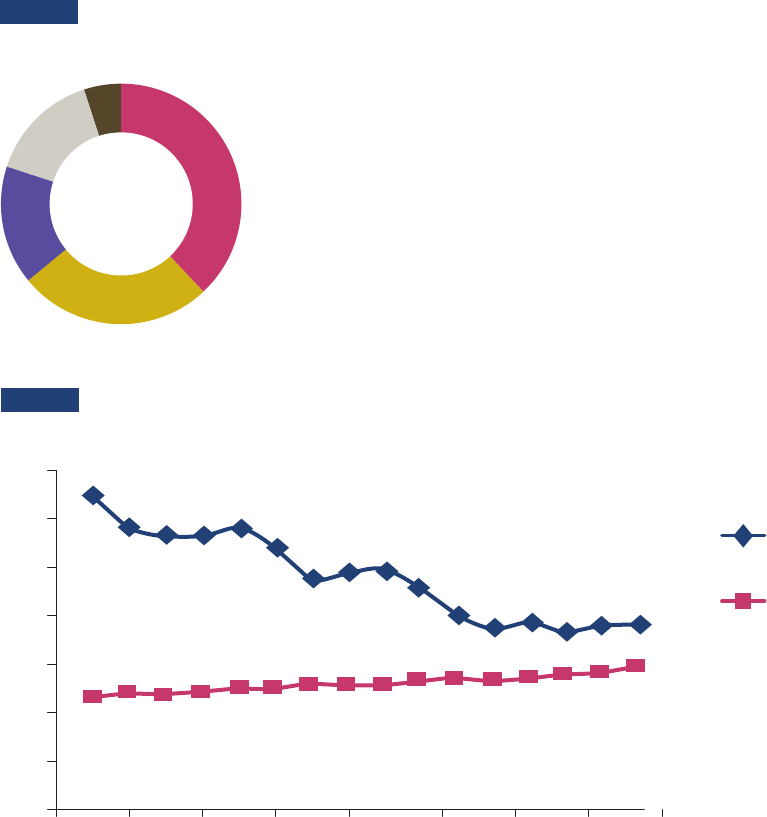
Figure 4 shows that the prevalence of ESRD has been increasing over time. The prevalence of ESRD
more than doubled between 1990 and 2015, and the number of prevalent ESRD cases has continued to
rise by approximately 20,000 cases per year, reaching 726,331 prevalent cases by 2016.
54
,
55
FIGURE 4
Prevalence of Treated ESRD, 2003-2015
POINT PREVALENCE PER MILLION RESIDENTS
SOURCE: Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. Website.https://nccd.cdc.gov/CKD.
YEAR
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
2000
1500
1000
500
0
All treated ESRD
Functioning transplant
Receiving dialysis
Page 22 | Advancing American Kidney Health
Similar to trends for CKD, Figure 5 shows that the prevalence of ESRD is higher among racial minori-
ties.
56
Compared to Whites, ESRD prevalence in 2016 was approximately 9.5 times greater in Native
Hawaiians and Pacific Islanders (NH PI), 3.7 times greater in African Americans (Black Af/Am), 1.5 times
greater in American Indians and Alaska Natives (AI/AN), and 1.3 times greater in Asians.
57
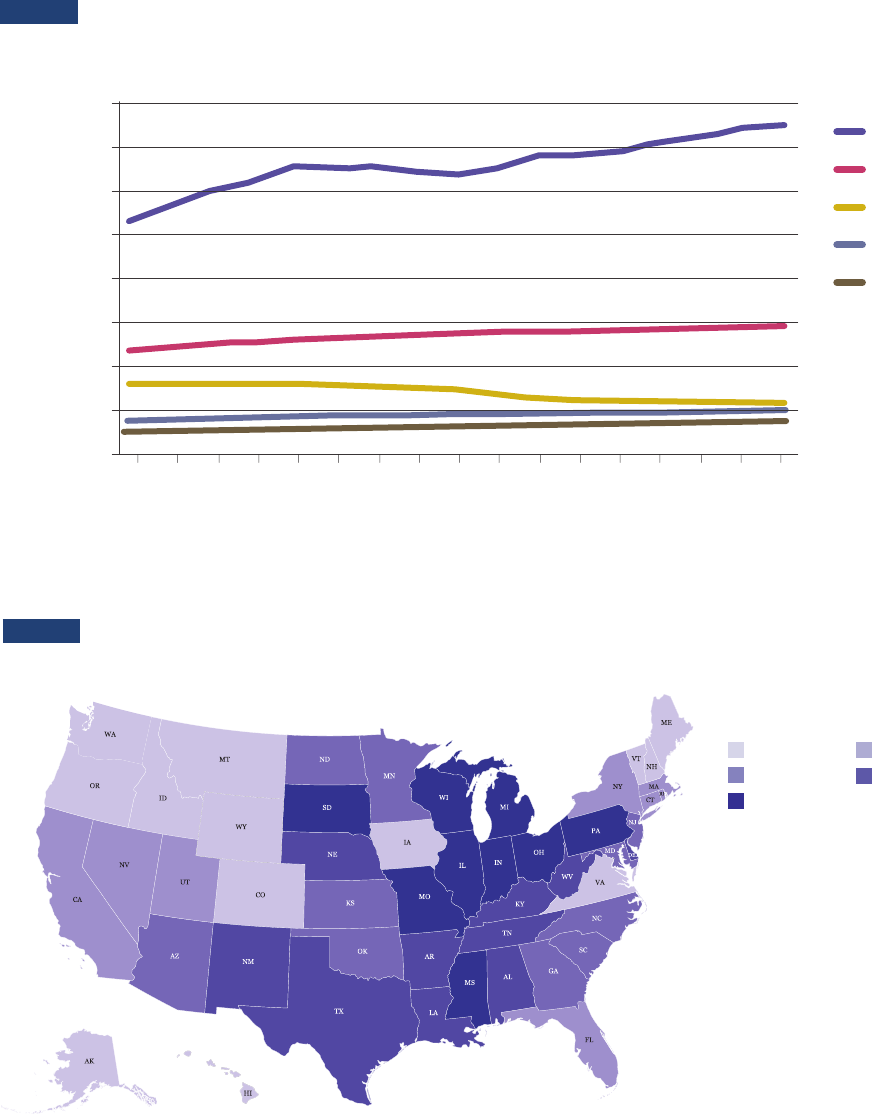
Figure 6 shows that the burden of ESRD varied significantly by state in 2015, ranging from highs of
2,428.8 per million residents in the District of Columbia, 2,212.6 in Illinois, and 2,203.6 in South Dakota
to lows of 1,185.8 per million residents in Vermont, 1,175.6 in Maine, and 1,155.7 in New Hampshire.
58
Trends in the Standardized Prevalence of ESRD, by Race, 2000-2016
White
Black/Af Am
AI/AN
Asian
NH/PI
SOURCE: USRDS Annual Data Report. Special analyses, USRDS ESRD Database. Point prevalence on December 31 of each year. Standardized
to the age-sex distribution of the 2011 U.S. population. Special analyses exclude unknown age, sex, and unknown/other race. Abbreviations
NH/PI: Native Hawaiian/Pacific Islander; AI/AN: American Indian/Alaska Native.
FIGURE 5
16,000
14,000
12,000
10,000
8,000
6,000
4,000
2,000
0
POINT PREVALENCE PER MILLION RESIDENTS
00 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16
Prevalence of ESRD by U.S. State for 2016
FIGURE 6
PREVALENCE PER MILLION
1,146 to 1,593 1,658 to 1, 90 9
1,921 to 2,016 2 ,019 to 2,107
2,163 to 2,563
Page 23 | Advancing American Kidney Health
Risk Factors
Major risk factors for ESRD include diabetes and high blood pressure (see Figure 7), in addition to hav-
ing a family history of kidney failure. Approximately 48 percent of individuals with severely reduced
kidney function who are not on dialysis, are not even aware they have CKD.
59
One positive trend is the decreasing rate of ESRD among American Indians and Alaska Natives (AI/ANs).
The incidence of diabetes-related ESRD (ESRD-D) among AI/AN populations decreased by over 40 per-
cent between 2000 and 2015, resulting in lower levels of disease burden for patients and reduced spend-
ing for programs that cover the costs of AI/AN health care.
60
Measures related to the assessment and
treatment of ESRD-D risk factors showed more improvement during this period in AI/ANs than in the
general U.S. population.
61
This reduction in ESRD rates occurred after the Indian Health Service (IHS)
began implementing public health and population management approaches to diabetes and improve-
ments in clinical care in the mid-1980s. The approach taken by IHS to reduce diabetes may be a model
for reducing ESRD risk factors in other health care systems.
Figure 8 shows the significant decline in ESRD-D incidence in AI/ANs compared to Whites between
2001 and 2015.
Reported Causes of ESRD in the United States
Diabetes
High blood pressure
Glomerulonephritis
Other cause
Unknown cause
N=726,331 (all ages, 2016).
Includes polycystic kidney disease, among other causes.
SOURCE: US Renal Data System.
38%
16%
15%
26%
5%
FIGURE 7
Incidence per Million of Diabetes-Related ESRD in AI/AN and White Populations
FIGURE 8
350
300
250
200
150
100
50
0
1999
2003
2009
2001
2007
2005
2011
2013
2015
AI/AN
White
SOURCE: ASPE Analysis of USRDS 2017 Annual Data Report Reference Tables.
Page 24 | Advancing American Kidney Health
Treatment Options for ESRD
USRDS data indicate that at the end of 2016, approximately 63.1 percent of all prevalent ESRD patients
were receiving hemodialysis (HD) therapy, 7.0 percent were treated with peritoneal dialysis, and 29.6
percent had a functioning kidney transplant. Among HD cases, 98.0 percent used in-center HD, and 2.0
percent used home HD.
62
While home-based dialysis may not meet the needs of every patient, home di-
alysis has clear benefits for those who are suitable candidates. In addition to being more convenient for
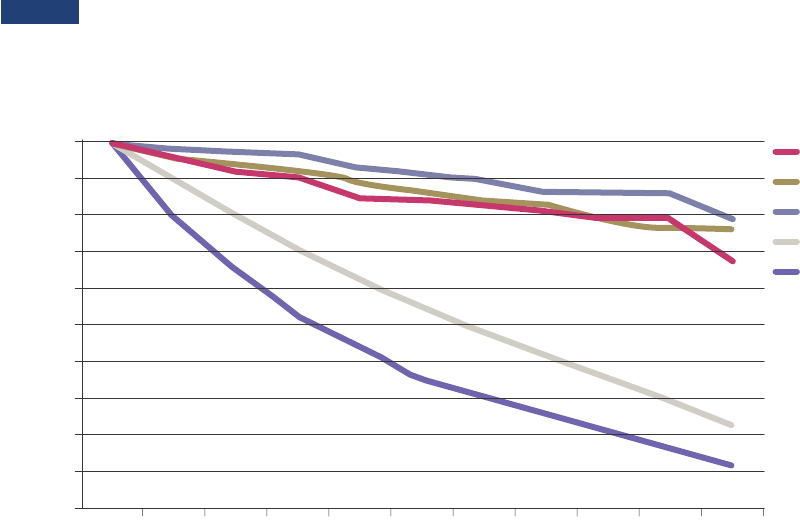
many people living with ESRD, Figures 9 (below) and 10 (following page) show that survivability rates
for home dialysis are comparable to those of transplant recipients and hemodialysis.
63
,
64
A 2015 Government Accountability Oce (GAO) report found that facilities have financial incentives
in the short term to increase provision of hemodialysis in facilities rather than increasing home dial-
ysis.
65
For example, hemodialysis facilities may be able to increase the number of in-center patients
without adding a dialysis machine because each machine can be used by six to eight in-center patients.
However, for each new home patient, facilities may need to pay for the cost of an additional dialysis
machine. GAO also reported that facilities might be less inclined to provide home dialysis depending
on the adequacy of Medicare’s payments for home dialysis training and because Medicare’s monthly
payments to physicians for managing the care of home dialysis patients are often lower than for man-
aging in-center patients.
66
The CMS Innovation Center is announcing five new payment models, which include incentives to opti-
mize care for Medicare beneficiaries with kidney disease. These models represent important eorts by
HHS to improve care for patients with chronic kidney disease in the near future. Looking further into the
future, investments in research and new technology may be able to increase access to even better treat-
ment options. Innovations in kidney disease treatments include technology such as wearable, implant-
able, and biohybrid dialysis units, which could substantially improve quality of life for people living with
ESRD. NIH funding for biomedical research related to kidney disease totaled approximately $600 mil-
lion in fiscal year 2018.
67
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
Survivability Rates for Nocturnal Home Hemodialysis (NHD)
vs. Other Treatment Modalities
SOURCE: USRDS 2018 Annual Data Report.
FIGURE 9
100
90
80
70
60
50
40
30
20
10
0
PATIENTS SURVIVING (%)
NHD: Avg age 46.4 years
Deceased donor transplant
Living donor transplant
Dialysis: 40-49 year (USRDS)
Dialysis: all ages (USRDS)
0 1 2 3 4 5 6 7 8 9 10
YEARS
Page 25 | Advancing American Kidney Health
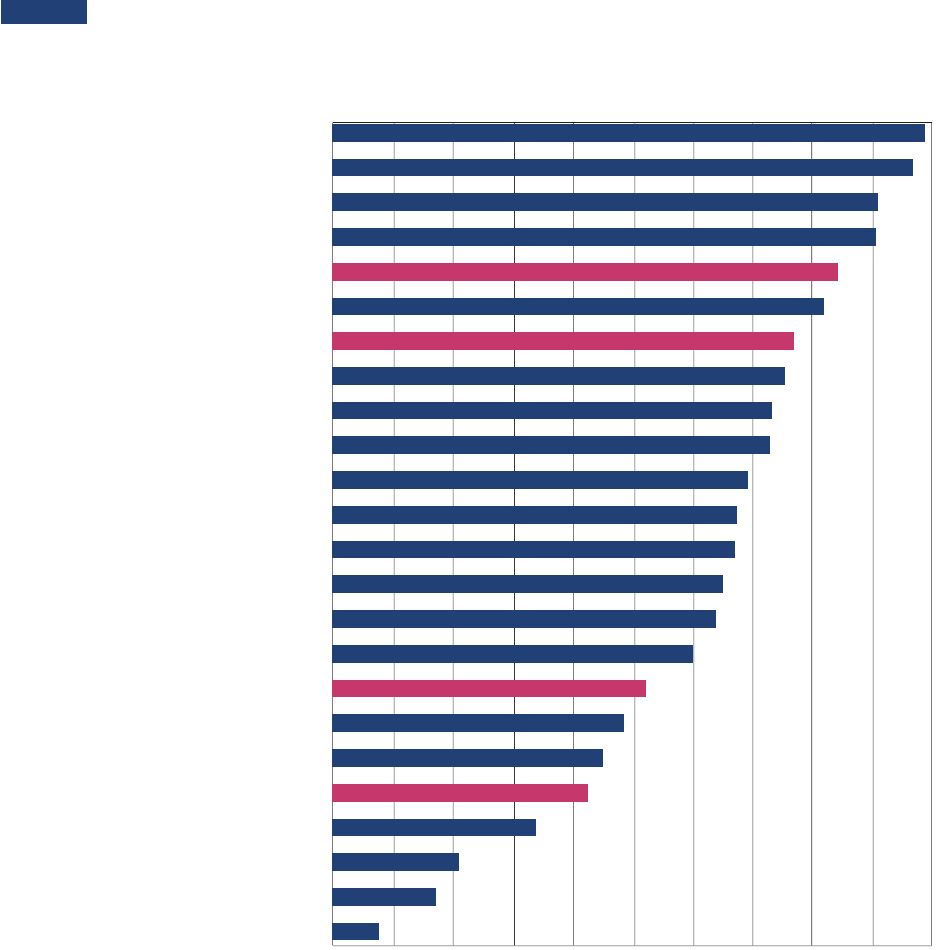
5-Year Survival of Cancers and ESRD by Treatment Type
FIGURE 10
Male Genital Cancer
Endocrine Cancer
Breast Cancer
Skin Cancer
ESKD–LD Txp*
Eye/Orbit Cancer
ESKD-DD Txp*
Urinary System Cancer
Kaposi Sarcoma
Lymphoma
Female Genital Cancer
Bones/Joint Cancer
All Cancer
So Tissue Cancer
Oral/Pharynx Cancer
Leukemia
ESKD–PD*
Myeloma
Digestive System Cancer
ESKD–HD*
Brain/CNS Cancer
Respiratory Cancer
Liver & Intrahepatic Bile Duct Cancer
Pancreatic Cancer
0 10 20 30 40 50 60 70 80 90 100
5-YEAR SURVIVAL RATE (PERCENTAGE)
*Reference population: incident ESKD patients, 2011. Adjusted for age, sex, race, Hispanic ethnicity, and primary
diagnosis
LEGEND
ESKD-LD Txp: end-stage kidney disease, received living donor transplant
ESKD-DD Txp: end-stage kidney disease, received deceased donor transplant
ESKD-PD: end-stage kidney disease, receiving peritoneal dialysis
ESKD-HD: end-stage kidney disease, receiving hemodialysis
SOURCES: United States Renal Data System, 2018 USRDS annual data report; SEER Cancer Statistics Review, 1975-2015.
Page 26 | Advancing American Kidney Health
provides the majority of NIH’s funding for biomedical research on kidney disease, ESRD treatment, and
kidney donation.
68
HHS, in partnership with the American Society of Nephrology, also supports KidneyX,
which is designed to improve kidney care by investing in the development of new products and technolo-
gies like wearable and implantable dialyzers and regenerative kidneys.
Health Care Spending on CKD and ESRD
When Medicare entitlement was first extended to individuals with ESRD in 1972, approximately 10,000
individuals were receiving dialysis. By 2016, excluding transplant patients, there were 511,270 benefi-
ciaries being treated for ESRD. While ESRD patients comprise less than 1 percent of the total Medicare
population, they accounted for approximately 7 percent of Medicare FFS spending, totaling over $35.4
billion in 2016.
69
Medicare spending on CKD and ESRD was over $114 billion in 2018, representing 23
percent of total Medicare FFS spending.
70
Growth in total CKD spending has primarily been driven
by an increase in the number of identified cases, particularly those in the earlier disease stages (CKD
Stages 1-3).
71
In 2016, Medicare patient obligations – which may be paid by the patient, by a second-
ary insurer, or may be uncollected – represented 9.6 percent, or approximately $4 billion, of total FFS
Medicare Allowable Payments.
72
Between 2015 and 2016, average per person per year spending for hemodialysis (HD) care increased
from $88,782 to $90,971, or 2.5 percent, while total spending on HD care rose from $26.8 billion to $28.0
billion, or 4.5 percent (similar to the total growth in ESRD spending of 4.6 percent).
73
Total spending for
patients who have received kidney transplants increased from $3.3 billion to $3.4 billion, or 3 percent,
and per capita spending increased from $34,080 to $34,780, or 2.1 percent.
74
Kidney Transplantation
For some people living with ESRD, a transplant using a healthy kidney from a donor may be an option.
The Innovation Center’s ETC Model will support the goal of increasing access to kidney transplants
through financial incentives for ESRD facilities and Managing Clinicians. A functioning transplanted
kidney does a better job of filtering wastes than dialysis,
75
and transplant recipients have improved life
expectancy compared to individuals on dialysis.
76
Of the 36,529 organ transplants performed in the
U.S. in 2018, approximately 21,000 were kidney transplants.
77
Of these, approximately 30.4 percent were
from living donors and 69.6 percent from deceased donors.
78
One-year patient survival rates are simi-
lar for individuals who received transplants from living kidney donors and from deceased donors: 98.8
percent and 96.3 percent, respectively. Five years after transplantation, the patient survival rate among
those who received a kidney transplant from a living donor is 92.1 percent, compared to 83.2 percent for
those who received a kidney transplant from a deceased donor.
79
The OPTN reports there are nearly 95,000 candidates on the waiting list to receive a kidney trans-
plant. On average, twenty candidates die each day while waiting for an organ transplant.
80
One
important factor contributing to the size of the waiting list is the number of discarded kidneys from
deceased donors.
Figure 11 (see following page) is a chart displaying the demand for kidney transplants and the policy
options that can optimize the availability of donor kidneys for transplantation.
Organ Donation and Procurement
More than 145 million Americans are registered to become organ donors.
81
However, signing up to be
a donor does not guarantee that the donor’s organs or tissues will be suitable for transplantation, and
registering as a donor usually takes place many years before donation becomes possible. In the case
of living donation, transplant centers evaluate potential living donors to determine whether they are
suitable to be a donor and to avoid the occurrence of any adverse physical, psychological, or emotional
outcome before, during, or after the donation.
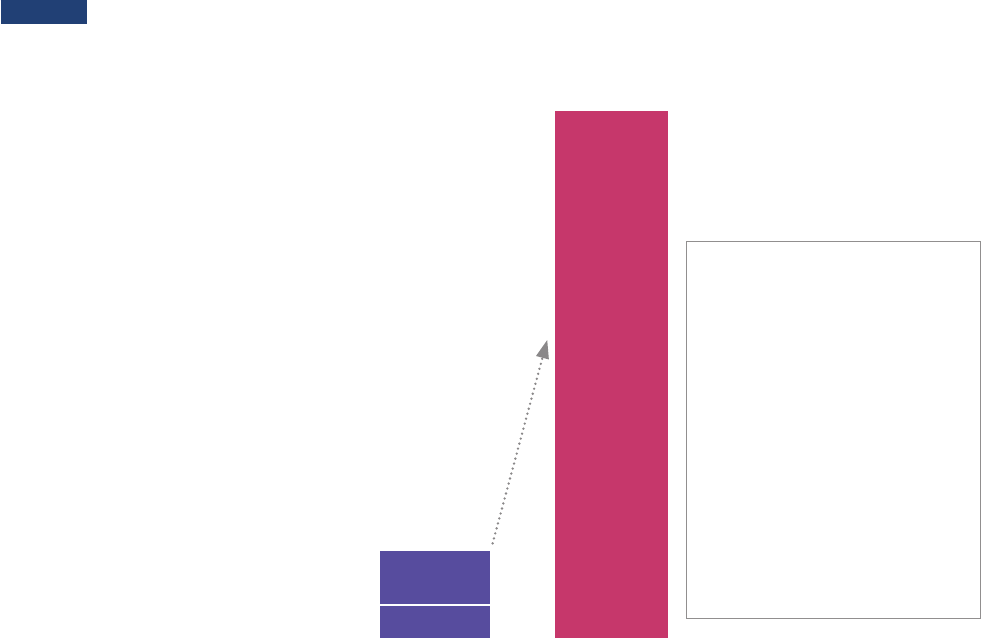
Page 27 | Advancing American Kidney Health
To become a deceased donor, an individual has to die under specific circumstances, such as after an ac-
cident involving severe head trauma, or a brain aneurysm or stroke. In such cases where an individual
is severely injured and unresponsive, physicians attempt to save the individual’s life and then perform
tests to determine whether the individual is brain dead and cannot breathe on his or her own. Organ
donation occurs only after the donor is legally declared dead. In accordance with federal regulations,
hospitals notify the local Organ Procurement Organization (OPO) of every patient who has died or is
nearing death and provide information to the OPO to determine whether deceased patients have the
potential to be an organ donor.
82
The OPO transplant coordinator searches the organ donor registries to see if the deceased person is
registered as a donor. If so, that registration serves as legal consent for organ donation. If the deceased
person has not registered as a donor and there was no other legal consent for donation such as a nota-
tion on the driver’s license, the OPO asks the deceased individual’s spouse or next of kin for authori-
zation. After authorization, a medical evaluation takes place, including obtaining information about
the deceased person’s medical history from his or her family. If the deceased person is determined
to be an eligible donor based on the medical evaluation, the OPO contacts the Organ Procurement and
Transplantation Network (OPTN).
83
,
84
The OPTN operates the national database of all patients in the U.S. waiting for a transplant. OPTN’s
computer system matches the donor’s organs to potential recipients. The network has policies that
define how donor organs are matched and allocated to patients on the waiting list. The OPTN policies
take into consideration the unique medical needs of children and provide priority to children for some
organs. OPTN policy also addresses the needs of patients with a highly sensitized immune system and
therefore at higher risk of rejecting a donor organ.
Gap between Supply and Demand for Kidney Transplantation
FIGURE 11
KEY STRATEGIES TO INCREASE
ACCESS TO KIDNEY TRANSPLANTS
Change the standards
used to evaluate Organ
Procurement Organizations
Update the PHS Guideline
for Reducing HIV, HBV, and
HCV Transmission Through
Organ Transplantation
Expand the Reimbursement of Travel
and Subsistence Expenses toward
Living Organ Donation program
Individuals on Waiting List to Receive
a Kidney as of June 18, 2019
Deceased Donor Kidney Transplants in 2018
Living Donor Kidney Transplants in 2018
94,754
5,645
14,516
SUPPLY DEMAND
SOURCE: Organ Procurement and Transplantation Network data
Page 28 | Advancing American Kidney Health
When matching organs from deceased donors to patients on the waiting list, many of the factors taken
into consideration are the same for all organs. These usually include:
• Blood type
• Body size
• Severity of patient’s medical condition
• Distance between the donor’s hospital and the patient’s hospital
• The patient’s waiting time
• Whether the patient is available (for example, whether the patient can be contacted and has no
current infection or other temporary reason that transplant cannot take place)
However, depending on the organ, some factors become more important, so there is a dierent policy
for each organ. For example, some organs can survive outside the body longer than others, so the dis-
tance between the donor’s hospital and the potential recipient’s hospital may be given greater weight
than other factors in certain situations.
After the OPO enters information about a deceased donor into the database, the computer system gen-
erates a list of patients who match the donor, by organ. Each available organ is then oered to the best-
matched patient for evaluation by the patient’s transplant team.
After a match is identified, the transplant team determines whether the available organ is medical-
ly suitable for the matched patient. Even if an organ is suitable, the transplant team may decline the
organ oer for example, if the patient is too sick to undergo a transplant, has an untreated infection,
or is unavailable for transplant. In these situations, the organ is then oered to the next patient on
the waiting list. During the organ matching process, organs are maintained on artificial support, and
the hospital medical sta and the OPO procurement coordinator closely monitor the condition of the
donated organs. After removal from the donor, organs remain viable for transplantation for only a lim-
ited period of time, which varies by organ type, so the OPO must arrange timely transportation of the
organs to the hospitals of the intended recipients. Figure 12 is a list of the reasons recovered kidneys
are not used.
FIGURE 12
Reported reasons why recovered kidneys are not used for transplantation:
• infection
• organ trauma
• too old on pump
• too old on ice
• ureteral damage
• deceased organ
• vascular damage
• biopsy findings
• positive hepatitis
• donor social history
• poor organ function
• donor medical history
• organ not as described
• anatomical abnormalities
• warm ischemic time
too long
• no recipient located –
list exhausted
• recipient determined to be
unsuitable for transplant
in the operating room
SOURCE: OPTN/SRTR 2016 Annual Data Report: Deceased Organ Donation
Page 29 | Advancing American Kidney Health
Current Quality Measures Relevant to Kidney Care
Calendar Year 2019 Quality Payment Program (QPP) Measures
for Clinicians by Reporting Method
QPP # Measure Name Claims Registry QCDR
Web
Interface EHR
1
Diabetes: Hemoglobin A1c (HbA1c)
Poor Control (>9%) ü ü ü ü
46 Medication Reconciliation Post-Discharge ü ü
47 Advance Care Plan ü ü
119
Diabetes: Medical Attention for
Nephropathy ü ü
167
Coronary Artery Bypass Gra (CABG):
Postoperative Renal Failure ü
325
Adult Major Depressive Disorder (MDD):
Coordination of Care of Patients with
Specific Comorbid Conditions ü
327
Pediatric Kidney Disease: Adequacy
of Volume Management ü
328
Pediatric Kidney Disease: ESRD Patients
Receiving Dialysis: Hemoglobin Level
< 10g/dL ü
329
Adult Kidney Disease: Catheter Use
at Initiation of Hemodialysis ü
330
Adult Kidney Disease: Catheter Use
for Greater Than or Equal to 90 Days ü
403 Adult Kidney Disease: Referral to Hospice ü
405
Appropriate Follow-up Imaging for
Incidental Abdominal Lesions ü ü
Page 30 | Advancing American Kidney Health
Qualified Clinical Data Registry (QCDR) Measures
QCDR Measure ID Measure Name
MUSIC15 Kidney Stones: SWL in patients with total renal stone burden > 2 cm or > 1 cm lower pole stones
ACRad26 Appropriate venous access for hemodialysis
RPAQIR9 Advance Care Planning (Pediatric Kidney Disease)
RPAQIR4 Arteriovenous Fistula Rate
RCOIR7 Improved Access Site Bleeding
RCOIR5 End Stage Renal Disease (ESRD) Initiation of Home Dialysis or Self-Care
RPAQIR13 Rate of Timely Documentation Transmission to Dialysis Unit/Referring Physician
RPAQIR5 Transplant Referral
RPAQIR16 Peritoneal Dialysis Catheter Success Rate
RPAQIR17 Peritoneal Dialysis Catheter Exit Site Infection Rate
RPAQIR18 Advance Directives Completed
RCOIR10 Upper Extremity Edema Improvement
RCOIR1 CKD 3-5 Patients Seen at the Recommended Frequency Levels
CLLC5 Monitoring for albuminuria in patients with CKD
RCOIR3 CKD 3-5 Patients with a Urine ACR or Urine PCR Lab Test
PPRNET13 Chronic Kidney Disease (CKD): eGFR Monitoring
PPRNET14 Chronic Kidney Disease (CKD): Hemoglobin Monitoring
RPAQIR1 Angiotensin Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy
RCOIR4 CKD 4-5 Patients with Transplant Referral
CLLC7 Renal Dysfunction: New Oral Anticoagulants (NOACs) Management
AQUA15 Stones: Urinalysis documented 30 days before surgical stone procedures
AQUA14 Stones: Repeat Shock Wave Lithotripsy (SWL) within 6 months of treatment

Page 31 | Advancing American Kidney Health
Quality Incentive Program (QIP) Measures for Dialysis Facilities by Data Source
SHORT NAME MEASURE NAME
PY
2021
PY
2022
PY
2023
DATA COLLECTION PERIOD
CY 2021 /CY 2022 /CY 2023
CLAIMS-BASED MEASURES
SRR Standardized Readmission Ratio ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
STrR Standardized Transfusion Ratio ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
SHR Standardized Hospitalization Ratio ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
VAT-Fistula Standardized Fistula Rate ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
VAT-Catheter Long-Term Catheter Rate ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
CROWNWEB BASED MEASURES
Depression
Clinical Depression Screening
and Follow-up ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
VAT-Fistula Standardized Fistula Rate ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
VAT-Catheter Long-Term Catheter Rate ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
UFR Ultrafiltration Rate ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
Kt/V Comprehensive Dialysis Adequacy ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
Hyp Hypercalcemia ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
PPPW Percentage of Prevalent Patients Waitlisted x ü ü
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
MedRec Medication Reconciliation x ü ü
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
NHSN BASED MEASURES
NHSN BSI
Reporting NHSN Dialysis Event Reporting ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
NHSN BSI Clinical
NHSN Bloodstream Infection
in Hemodialysis Patients ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
ICH_CAHPS BASED MEASURES
ICH_CAHPS
In-center Hemodialysis Consumer Assessment
of Healthcare Provider and Systems ü ü ü
January 1, 2019 – December 31, 2019
January 1, 2020 – December 31, 2020
January 1, 2021 – December 31, 2021
Page 32 | Advancing American Kidney Health
List of Acronyms
AI/AN American Indian/Alaska Native
APOL1 Apolipoprotein L1
ASPE Assistant Secretary for Planning and Evaluation
ASPR Assistant Secretary for Preparedness and Response
CDC Centers for Disease Control and Prevention
CEC Comprehensive ESRD Care
KCF Kidney Care First
CKCC Comprehensive Kidney Care Contracting
CKD Chronic Kidney Disease
CMS Centers for Medicare and Medicaid Services
COIIN Collaborative Improvement and Innovation Networks
CROWNWeb Consolidated Renal Operations in a Web-enabled Network
CTO Chief Technology Ocer
DAA Direct-acting Anti-viral
DPP Diabetes Prevention Program
EMP ESA Monitoring Policy
ESA Erythropoietin Stimulating Agent
ESRD End Stage Renal Disease
ESRD-D Diabetes-related ESRD
ETC ESRD Treatment Choices
FDA Food and Drug Administration
FFS Fee-for-Service
FY Fiscal Year
GAO Government Accountability Oce
HD Hemodialysis
HHS Health and Human Services
HRSA Health Resources and Services Administration
IHS Indian Health Service
MHS Military Health System
NIH National Institutes of Health
NIDDK National Institute of Diabetes and Digestive and Kidney Diseases
NKF National Kidney Foundation
OASH Oce of the Assistant Secretary for Health
ONC Oce of the National Coordinator for Health Information Technology
OPO Organ Procurement Organization
OPTN Organ Procurement and Transplantation Network
PHS Public Health Service
PPS Prospective Payment System
QCDR Qualified Clinical Data Registry
QIP Quality Incentive Program
QPP Quality Payment Program
SDPI Special Diabetes Program for Indians
USRDS U.S. Renal Data System

Page 33 | Advancing American Kidney Health
Endnotes
1. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: U.S.
Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
2. Heron M. Deaths: Leading causes for 2017. National Vital Statistics Reports; vol 68 no 6. Hyattsville, MD: National
Center for Health Statistics. 2019.
3. National Institute of Diabetes and Digestive and Kidney Diseases (2016). Kidney Disease Statistics for the United States.
Available online at https://www.niddk.nih.gov/health-information/health-statistics/kidney-disease
4. Ibid.
5. To be entitled to Medicare based on ESRD, patients must either individually or through a spouse or parent have accu-
mulated a sucient amount of work history to qualify for Social Security Disability Insurance (SSDI) or Social Security
Retirement Benefits or Railroad Retirement benefits or railroad disability annuity, and meet other requirements.
6. Centers for Medicare & Medicaid Services (2019). Comprehensive ESRD Care Model. Available online at https://innova-
tion.cms.gov/initiatives/comprehensive-ESRD-care/
7. United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States.
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018.
Available online at https://www.usrds.org
8. United States Renal Data System. 2018 Annual Data Report, Chapter 9, Healthcare Expenditures for Persons with ESRD.
Available online at https://www.usrds.org
9. Watnick, S. The Kidney Accelerator: Innovation Wanted, Nephrologists Needed. Clin J Am Soc Nephrol 13: 1750-1752,
2018. doi: https://doi.org/10.2215/CJN.04720418
10. HHS Oce of the Assistant Secretary for Planning and Evaluation (2019). The Special Diabetes
Program for Indians: Estimates of Medicare Savings. Available online at https://aspe.hhs.gov/pdf-report/
special-diabetes-program-indians-estimates-medicare-savings
11. CDC’s Innovative State and Local Public Health Strategies to Prevent and Manage Diabetes and Heart Disease and
Stroke (CDC-RFA-DP18-1817) is a collaboration between CDC and health departments to develop innovative approaches to
increase the reach and eectiveness of evidence-based public health strategies in populations and communities with a
high burden of diabetes, heart disease, and stroke. More information is available at https://www.cdc.gov/diabetes/pro-
grams/stateandlocal/funded-programs/1817.html
12. More information can be found at: https://www.cdc.gov/dialysis/coalition/index.html
13. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US
Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
14. Ibid.
15. Ibid.
16. Ibid.
17. United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States.
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018.
Available online at https://www.usrds.org
18. Internal communications with CDC.
19. United States Renal Data System (2018). 2018 Annual Data Report: Trends in Incident Counts: By Renal Replacement
Therapy Modality. Available online at https://www.usrds.org/2018/view/v2_01.aspx
20. Mendelssohn DC. Mujais SK, Soroka, SD, et al. A prospective evaluation of renal replacement therapy modality eligi-
bility. Nephrology Dialysis Transplantation. 2009; 24(2): 555-561. doi: https://doi.org/10/1093/ndt/gfn484
21. Maaroufi A, Fafin C, Mougel S, Favre G, Seitz-Polski P, Jeribi A, Vido S, Dewismi C, Albano L, Esnault V, Moranne O.
Patient preferences regarding choice of end-stage renal disease treatment options. American Journal of Nephrology.
2013; 37(4): 359-369.
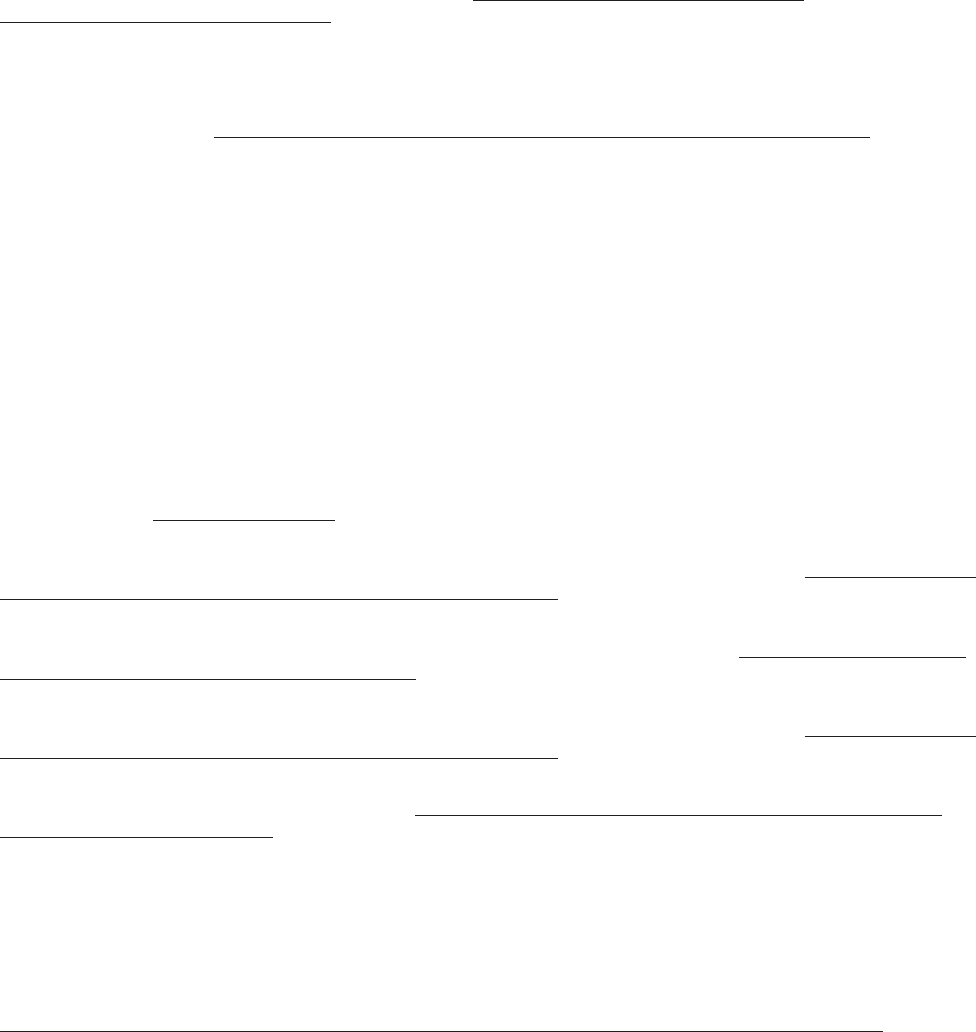
Page 34 | Advancing American Kidney Health
22. Wong B, Ravani P, Oliver MJ, Holroyd-Leduc J, Venturato L, Garg AX, Quinn RR. Comparison of Patient Survival
Between Hemodialysis and Peritoneal Dialysis Among Patients Eligible for Both Modalities. American Journal of Kidney
Diseases. 2018; 71(3) 344-351.
23. Walker, R., Howard, K., & Morton, R. (2017). Home hemodialysis: a comprehensive review of patient-centered and
economic considerations. Clinicoeconomics and Outcomes Research; Volume 9, 149-161.
24. Kumar VA, Sidell MA, Jones JP, Vonesh EF. Survival of propensity matched incident peritoneal and hemodialysis pa-
tients in a United States health care system. Kidney International; 2014; 86: 1016-1022.
25. Mehrotra R, Chiu YW, Kalantar-Zadeh K, Bargman J, Vonesh E. Similar outcomes with hemodialysis and peritoneal
dialysis in patients with end-stage renal disease. Archives of Internal Medicine; 2011; 171(2): 110-8.
26. United Network for Organ Sharing (2019). Waiting List Candidates by Organ Type – All Patient States
Based on OPTN data as of June 23, 2019. Available online at https://unos.org/data/transplant-trends/
waiting-list-candidates-by-organ-type/
27. Tonelli M, Wiebe N, Knoll G et al. Systematic Review: Kidney Transplantation Compared With Dialysis in Clinically
Relevant Outcomes. American Journal of Transplantation 2011; 11:2093-2109.
28. National Institute of Diabetes and Digestive and Kidney Diseases (2016). Kidney Disease Statistics for the United
States. Available online at https://www.niddk.nih.gov/health-information/health-statistics/kidney-disease
29. Healthy People provides science-based, 10-year national objectives for improving the health of all Americans. For
three decades, Healthy People has established benchmarks and monitored progress over time in order to encourage
collaborations across communities and sectors, empower individuals toward making informed health decisions, and
measure the impact of prevention activities.
30. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US
Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
31. Based in part on the results of the SPRINT trial, in 2017, the American College of Cardiology, the American Heart
Association, and other related organizations revised clinical practice guidelines for hypertension. They redefined the
definition of hypertension to lower blood pressure cut points and updated treatment guidelines. See Whelton PK, Carey
RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA, PCNA guideline for the prevention,
detection, evaluation, and management of high blood pressure in adults A report of the American College of Cardiology/
American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e13-e115. DOI: 10.1161/
HYP.0000000000000065.
32. United States Renal Data System. 2018 Annual Data Report, Chapter 2, Identification and care of patients with CKD.
Available online at https://www.usrds.org
33. Centers for Disease Control and Prevention (2017). National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for
Disease Control and Prevention, U.S. Department of Health and Human Services. Available online at https://www.cdc.gov/
diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
34. Centers for Disease Control and Prevention (2016). High Blood Pressure Fact Sheet. Atlanta, GA: Centers for Disease
Control and Prevention, U.S. Department of Health and Human Services. Available online at https://www.cdc.gov/dhdsp/
data_statistics/fact_sheets/fs_bloodpressure.htm
35. Centers for Disease Control and Prevention (2017). National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for
Disease Control and Prevention, U.S. Department of Health and Human Services. Available online at https://www.cdc.gov/
diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
36. HHS Oce of the Assistant Secretary for Planning and Evaluation (2019). The Special Diabetes Program for Indians:
Estimates of Medicare Savings. Available online at https://aspe.hhs.gov/pdf-report/special-diabetes-program-indi-
ans-estimates-medicare-savings
37. Bullock A, She K, Moore K, Manson S. Obesity and overweight in American Indian and Alaska Native children, 2006-
2015. American Journal of Public Health 2017;107:1502-1507.
38. Bursell SE, Fonda SJ, Lewis DG, Horton MB. Prevalence of diabetic retinopathy and diabetic macular edema in a pri-
mary care-based teleophthalmology program for American Indians and Alaska Natives. PLoS ONE 2018;13(6):e0198551.
39. Agency for Healthcare Research and Quality. Data Spotlight: Hospital admissions for uncontrolled diabetes improving
among American Indians and Alaska Natives. AHRQ Publication No. 18(19)-0033-7-EF. December 2018. Available online at
https://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/nhqrdr/dataspotlight-aian-diabetes.pdf
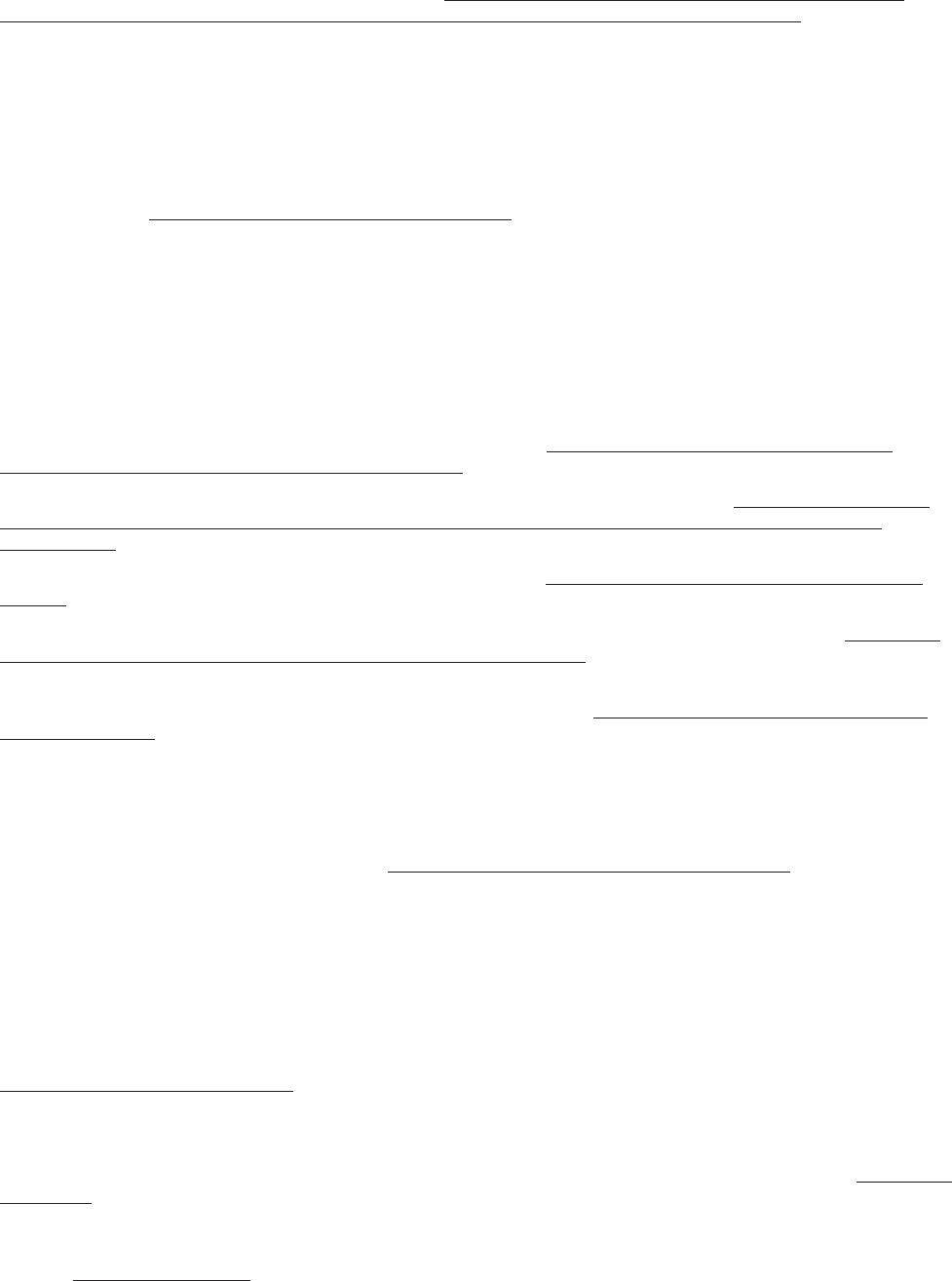
Page 35 | Advancing American Kidney Health
40. Additional information about the DPP is available at https://www.cdc.gov/diabetes/prevention/milestones.htm and
https://www.niddk.nih.gov/about-niddk/research-areas/diabetes/diabetes-prevention-program-dpp
41. The Million Hearts® 2022 initiative is co-led by the Centers for Disease Control and Prevention (CDC) and the Centers
for Medicare and Medicaid Services (CMS). Million Hearts® has a goal of preventing 1 million heart attacks, strokes,
and related cardiovascular events in the U.S. by 2022. It is carried out by a variety of governmental and nongovernmental
partners at local, state, and federal levels. Key priority areas include keeping people healthy, optimizing care for those at
risk for cardiovascular disease, and improving outcomes for priority population who suer worse outcomes of cardiovas-
cular disease.
42. United States Renal Data System. 2018 Annual Data Report: Chapter 9: Transition of Care in Chronic Kidney Disease.
Available online at https://www.usrds.org/2018/view/v1_09.aspx
43. Patel PR, Yi SH, Booth S, Bren V, et al. Bloodstream infection rates in outpatient hemodialysis facilities partic-
ipating in a collaborative prevention eort: a quality improvement report. American Journal of Kidney Diseases 2013;
Aug;62(2):322-30.
44. An ESRD Network is defined in the Code of Federal Regulations (CFR), at 42 CFR Part 405, Subpart U as all Medicare-
approved ESRD facilities in a designated geographic area specified by CMS. These regulations require ESRD treatment
facilities to be organized into groups called Networks in order to promote a system of eective coordination. As an
organized Network, dialysis and transplant providers can coordinate patient referral and access to resources in a more
ecient manner.
45. OPTN/SRTR 2017 Annual Data Report: Kidney. Available online at https://srtr.transplant.hrsa.gov/annual_re-
ports/2017/Kidney.aspx#KI_37_discard_rate_dm_1_b64
46. The Bridgespan Group (2019). Reforming Organ Donation in America. Available online at https://www.bridgespan.
org/bridgespan/Images/articles/reforming-organ-donation-in-america/reforming-organ-donation-in-ameri-
ca-01-2019.pdf
47. OPTN/SRTR 2017 Annual Data Report: Kidney page 4. Available at https://onlinelibrary.wiley.com/doi/epdf/10.1111/
ajt.15274;
KAS Turns Four: The State of Deceased Donor Kidney Allocation in the U.S. OBM Transplantation. Available at http://www.
lidsen.com/journals/transplantation/transplantation-03-01-041#Abstract
48. Sapiano, MRP, Jone, JM, et al. (2019). Impact of US Public Health Service increased risk deceased donor designa-
tion on organ utilization. American Journal of Transplantation; 2019;00:1–10. https://doi-org.ezproxyhhs.nihlibrary.nih.
gov/10.1111/ajt.15388
49. Tosoc-Haskell H, Sisaithong K, Carrico R. “The Collaborative Improvement and Innovation Network Project to Drive
Quality Improvement” Co-Transplantation Volume 24 Number 1 (February 2019).
50. Matthew Cooper, Richard Formica, John Friedewald, Ryutaro Hirose, Kevin O’Connor, Sumit Mohan, Jesse Schold,
David Axelrod, Stephen Pastan; Report of National Kidney Foundation Consensus Conference to Decrease Kidney
Discards, Clinical Transplantation, October 2018, https://onlinelibrary.wiley.com/doi/10.1111/ctr.13419
51. Dialysis Facility Compare is the ocial CMS source for information about the quality of dialysis facilities and pub-
lishes data on thousands of Medicare-certified dialysis centers across the country. The End-Stage Renal Disease (ESRD)
Quality Incentive Program (QIP) promotes high-quality services in outpatient dialysis facilities treating people living
with ESRD by changing the way CMS pays for the treatment of ESRD by linking a portion of Medicare ESRD Prospective
Payment System (PPS) payment directly to facilities’ performance on quality of care measures. CROWNWeb is the web-
based, national ESRD patient registry and quality measure reporting system mandated by CMS to enable dialysis facilities
to submit clinical and administrative data.
52. Centers for Disease Control and Prevention. Chronic Kidney Disease (CKD) Surveillance System—United States.
https://nccd.cdc.gov/ckd/default.aspx
53. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: U.S.
Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
54. Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. http://www.
cdc.gov/ckd;
United States Renal Data System. 2017 Annual Data Report: Epidemiology of kidney disease in the United States. National
Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2017. Available
online at https://www.usrds.org
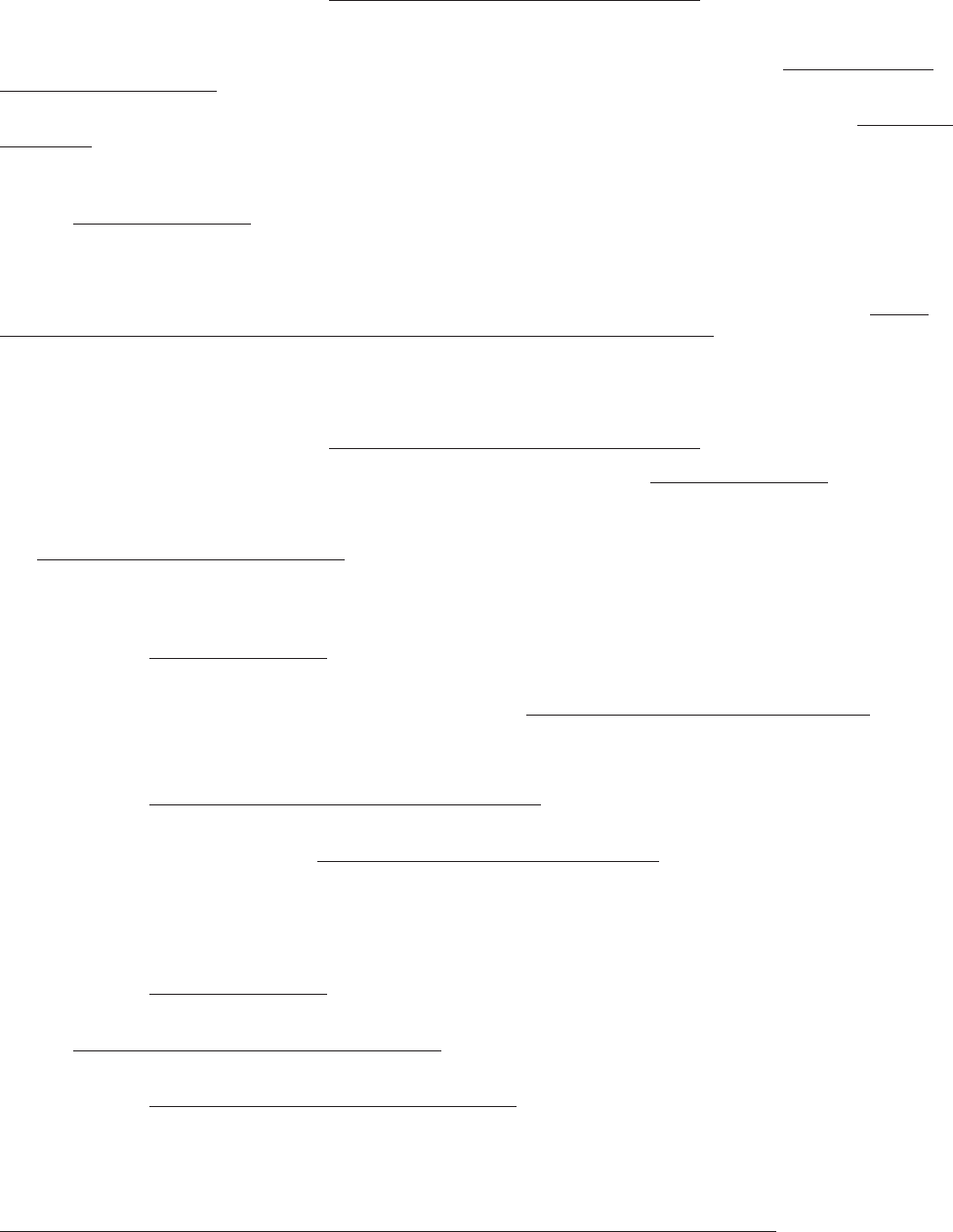
Page 36 | Advancing American Kidney Health
55. United States Renal Data System. 2018 Annual Data Report: ESRD Incidence, Prevalence, Patient Characteristics, and
Treatment Modalities. Available online at https://www.usrds.org/2018/view/Default.aspx
56. Ibid.
57. United States Renal Data System. 2018 Annual Data Report, Vol 2, Figure 1.12. Available online at https://www.usrds.
org/2018/view/Default.aspx
58. Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. http://www.
cdc.gov/ckd;
United States Renal Data System. 2017 Annual Data Report: Epidemiology of kidney disease in the United States. National
Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2017. Available
online at https://www.usrds.org
59. Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US
Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
60. ASPE, 2019. The Special Diabetes Program for Indians: Estimates of Medicare Savings. Available online at https://
aspe.hhs.gov/pdf-report/special-diabetes-program-indians-estimates-medicare-savings
61. Bullock A, Rios Burrows N, Narva AS, et al. (2017). Vital Signs: Decrease in Incidence of Diabetes-Related End-Stage
Renal Disease among American Indians/Alaska Natives - United States, 1996-2013. MMWR, Vol 66(1): 26-32.
62. United States Renal Data System. 2018 Annual Data Report: ESRD Incidence, Prevalence, Patient Characteristics, and
Treatment Modalities. Available online at https://www.usrds.org/2018/view/Default.aspx
63. United States Renal Data System. 2018 Annual Data Report. Available online at https://www.usrds.org
64. Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis
DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2014, National Cancer Institute. Bethesda,
MD, https://seer.cancer.gov/csr/1975_2014/, based on November 2016 SEER data submission, posted to the SEER web-
site, April 2017;
United States Renal Data System. 2016 USRDS annual data report: Epidemiology of kidney disease in the United States.
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2016.
Available online at https://www.usrds.org
65. Government Accountability Oce (2015). GAO-16-125: End Stage Renal Disease: Medicare Payment Refinements
Could Promote Increased Use of Home Dialysis. Available online at https://www.gao.gov/assets/680/673140.pdf
66. Ibid.
67. National Institutes of Health (2019). Estimates of Funding for Various Research, Condition, and Disease Categories.
Available online at https://report.nih.gov/categorical_spending.aspx
68. Government Accountability Oce (2016). GAO-17-121: National Institutes of Health Kidney Disease Research Funding
and Priority Setting. Available online at https://www.gao.gov/assets/690/681714.pdf
69. Centers for Medicare & Medicaid Services (2019). Center for Medicare & Medicaid Innovation analysis of United States
Renal Data System data.
70. United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States.
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018.
Available online at https://www.usrds.org
71. United States Renal Data System. 2018 Annual Data Report: Health Care Expenditures for Persons with CKD. Available
online at https://www.usrds.org/2018/view/Default.aspx
72. United States Renal Data System. 2018 Annual Data Report: Health Care Expenditures for Persons with ESRD.
Available online at https://www.usrds.org/2018/view/Default.aspx
73. Ibid.
74. Ibid.
75. National Institute of Diabetes and Digestive and Kidney Diseases (2018). Kidney Transplant. Available online at
https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/kidney-transplant
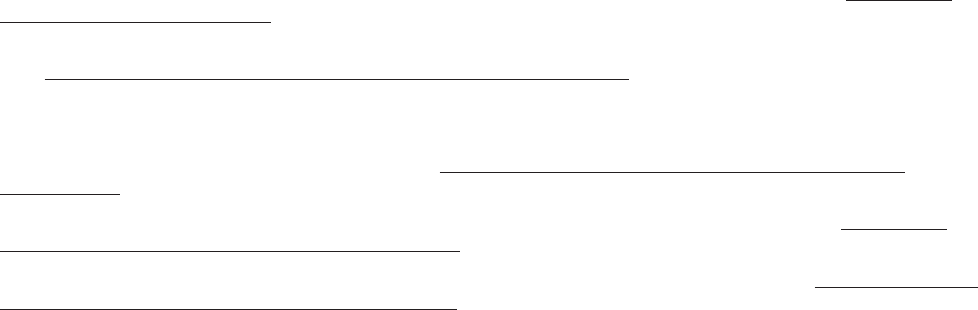
Page 37 | Advancing American Kidney Health
76. United States Renal Data System (2018). 2018 Annual Data Report: ESRD Mortality. Available online at https://www.
usrds.org/2018/view/Default.aspx
77. Organ Procurement and Transplantation Network (2019). Transplants by Donor Type, U.S. Transplants Performed,
2018. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/
78. Ibid.
79. Organ Procurement and Transplantation Network (2019). Kidney Kaplan-Meier Patient Survival Rates for
Transplants Performed 2008-2015. Available online at https://optn.transplant.hrsa.gov/data/view-data-reports/
national-data/
80. Health Resources and Services Administration (2019). Organ Donation Statistics. Available online at https://www.
organdonor.gov/statistics-stories/statistics.html#glance
81. Health Resources and Services Administration (2019). Registration Statistics. Available online at https://www.organ-
donor.gov/statistics-stories/statistics.html#registration
82. OPOs evaluate potential donors, discuss donation with surviving family members, and arrange for the surgical
removal and transport of donated organs. There are 58 OPOs in the U.S., each with its own designated service area. OPOs
must be certified by the Centers for Medicare and Medicaid Services (CMS) and abide by CMS regulations.
83. An eligible death is defined as per OPTN Policy 1.2 as death of a person aged 70 years or younger who is legally de-
clared brain dead according to hospital policy and does not exhibit any of the following indications: tuberculosis, hu-
man immunodeficiency virus (HIV) infection with specified conditions, Creutzfeldt-Jacob Disease, herpetic septicemia,
rabies, reactive hepatitis B surface antigen, any retrovirus infection, active malignant neoplasms (except primary central
nervous system tumors and skin cancers), Hodgkin disease, multiple myeloma, leukemia, miscellaneous carcinomas,
aplastic anemia, agranulocytosis, fungal and viral encephalitis, gangrene of bowel, extreme immaturity, or positive sero-
logical or viral culture findings for HIV.
84. The purpose of the OPTN is to improve the eectiveness of the nation’s organ procurement, donation, and transplan-
tation system by increasing the availability of and access to donor organs for patients with end-stage organ failure. The
OPTN is administered by United Network for Organ Sharing (UNOS) under contract to the U.S. Department of Health and
Human Services.

