
World
Population
Policies related to fertility
2021
Policies
UN DESA/POP/2021/TR/NO. 1
Department of Economic and Social Affairs
Population Division
World Population Policies 2021
Policies related to fertility
asdf
United Nations
New York, 2021
United Nations Department of Economic and Social Aairs, Population Division
e Department of Economic and Social Aairs of the United Nations Secretariat is a vital interface between
global policies in the economic, social and environmental spheres and national action. e Department
works in three main interlinked areas: (i) it compiles, generates and analyses a wide range of economic,
social and environmental data and information on which States Members of the United Nations draw to
review common problems and take stock of policy options; (ii) it facilitates the negotiations of Member
States in many intergovernmental bodies on joint courses of action to address ongoing or emerging
global challenges; and (iii) it advises interested Governments on the ways and means of translating policy
frameworks developed in United Nations conferences and summits into programmes at the country level
and, through technical assistance, helps build national capacities.
e Population Division of the Department of Economic and Social Aairs provides the international
community with timely and accessible population data and analysis of population trends and development
outcomes for all countries and areas of the world. To this end, the Division undertakes regular studies of
population size and characteristics and of all three components of population change (fertility, mortality
and migration). Founded in 1946, the Population Division provides substantive support on population and
development issues to the United Nations General Assembly, the Economic and Social Council and the
Commission on Population and Development. e Population Division also leads or participates in various
interagency coordination mechanisms of the United Nations system. It also contributes to strengthening the
capacity of Member States to monitor population trends and to address current and emerging population
issues.
Suggested citation
United Nations Department of Economic and Social Aairs, Population Division (2021). World Population
Policies 2021: Policies related to fertility. UN DESA/POP/2021/TR/NO. 1.
is report is available in electronic format on the Division’s website at www.unpopulation.org. For further
information about this report, please contact the Oce of the Director, Population Division, Department of
Economic and Social Aairs, United Nations, New York, 10017, USA, by Fax: 1 212 963 2147 or by email at
popula[email protected]g.
Copyright information
Front cover: Murje Netu and her son aer seeking services at the Wamba Local Government Primary
Health Care Centre in Wamba, Nigeria, by Dominic Chavez/e Global Financing Facility, 2018.
Back cover: Adolescent health in Mozambique, by the Global Financing Facility, 2019.
United Nations Publication
Sales No.: E.22.XIII.1
ISBN: 9789211483635
eISBN: 9789210000949
Copyright © United Nations, 2021.
Figures and tables in this publication can be reproduced without prior permission, made available under a
Creative Commons license (CC BY 3.0 IGO), http://creativecommons.org/licenses/by/3.0/igo/
Acknowledgements
is report was prepared by Guangyu Zhang, Stephen Kisambira and Karoline Schmid. e authors wish to
thank John Wilmoth, Jorge Bravo, Vinod Mishra and Bela Hovy for their input in reviewing the dra.
e assistance of Donna Culpepper and Neena Koshy in editing and desktop publishing is acknowledged.
Contents
Executive summary .......................................................................................................1
Introduction ......................................................................................................................3
Government fertility and family planning policies through 2019 ..............5
Government policies and related responses: Case studies ......................... 13
The impact of the COVID-19 pandemic on fertility ........................................ 27
Summary and policy considerations ..................................................................... 31
References ....................................................................................................................... 32
Annex table .................................................................................................................... 36
Notes on regions, development groups, countries and areas
e designations employed in this publication and the material presented in it do not imply the expression
of any opinions whatsoever on the part of the Secretariat of the United Nations concerning the legal status
of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or
boundaries. e term “country” as used in this report also refers, as appropriate, to territories or areas.
In this publication, data for countries and areas are oen aggregated in six continental regions: Africa,
Asia, Europe, Latin America and the Caribbean, Northern America, and Oceania. Further information on
continental regions is available from https://unstats.un.org/unsd/methodology/m49/. Countries and areas
have also been grouped into geographic regions based on the classication being used to track progress
towards the Sustainable Development Goals of the United Nations (see https://unstats.un.org/sdgs/
indicators/regional-groups/).
e designation of “more developed” and “less developed”, or “developed” and “developing”, is intended for
statistical purposes and does not express a judgment about the stage in the development process reached
by a particular country or area. More developed regions comprise all countries and areas of Europe and
Northern America, plus Australia, New Zealand and Japan. Less developed regions comprise all countries
and areas of Africa, Asia (excluding Japan), Latin America and the Caribbean, and Oceania (excluding
Australia and New Zealand).
e group of least developed countries (LDCs) includes 47 countries, located in sub-Saharan Africa (32),
Northern Africa and Western Asia (2), Central and Southern Asia (4), Eastern and South-Eastern Asia (4),
Latin America and the Caribbean (1), and Oceania (4). Further information is available at http://unohrlls.
org/about-ldcs/.
e group of Landlocked Developing Countries (LLDCs) includes 32 countries or territories, located in
sub-Saharan Africa (16), Northern Africa and Western Asia (2), Central and Southern Asia (8), Eastern
and South-Eastern Asia (2), Latin America and the Caribbean (2), and Europe and Northern America (2).
Further information is available at http://unohrlls.org/about-lldcs/.
e group of Small Island Developing States (SIDS) includes 58 countries or territories, located in the
Caribbean (29), the Pacic (20), and the Atlantic, Indian Ocean, Mediterranean and South China Sea
(AIMS) (9). Further information is available at http://unohrlls.org/about-sids/.
e classication of countries and areas by income level is based on gross national income (GNI) per capita
as reported by the World Bank (June 2018). ese income groups are not available for all countries and areas.
Further information is available at https://datahelpdesk.worldbank.org/knowledgebase /articles/906519-
world-bank-country-and-lending-groups.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
1
Executive summary
e report provides a brief overview of global fertility levels and trends since the early 1960s and explores
government’s views and policies related to fertility. e analysis of views and policies draws on data gathered
through 2019 and available in the World Population Policies Database (box 1), reecting the situation before
the outbreak of the coronavirus disease 2019 (COVID-19) pandemic. e report then presents ve case
studies of countries from dierent regions and with a range of fertility levels, exploring in more detail the
origin and evolution of national fertility policies. e case studies are followed by an assessment of known
or potential direct and indirect impacts of the COVID-19 pandemic on fertility patterns and trends. e
report concludes with an exploration of policy options that governments may wish to consider in the current
context.
Below are some key conclusions of the report:
• Globally, through 2019, nearly three quarters of governments had policies related to fertility. Of these,
69 governments had policies to lower fertility, 55 aimed to raise fertility, and 19 focused on maintaining
current levels of fertility. A total of 54 governments did not have an ocial fertility policy.
• e data suggest an association between the kinds of policies in place between 2015 and 2019 and
fertility levels observed in that period. Among the 69 countries with policies to lower fertility, 10 were
high-fertility countries in 2019, and 50 had intermediate fertility levels. Of the 55 countries with policies
to raise fertility, 40 had low levels of fertility in 2019, including 18 with very low levels.
1
• In developed countries with older populations, governments were more likely to have policies intended
to raise fertility. Among developing countries, nearly half had policies to lower fertility, while one quarter
did not have an ocial policy related to fertility. Among the least developed countries (LDCs), whose
combined population continues to grow rapidly, an increasing number of governments had policies
seeking to lower fertility.
• Fertility policies show considerable variation across regions. In sub-Saharan Africa and Oceania
(excluding Australia and New Zealand), governments were more likely to have policies to lower fertility,
whereas in Europe and Northern America and in Eastern and South-Eastern Asia, policies to raise
fertility were more prevalent. In Latin America and the Caribbean, around half of the countries had no
specic policy designed to inuence fertility levels.
• An overwhelming majority of governments (over 95 per cent, or 98 of 103 countries with available
data in 2019) provided family planning services to their populations, either directly through public
programmes or indirectly through non-governmental organizations. Direct support was provided by 80
governments, of which 68 reported supporting family planning both directly and indirectly. In addition,
18 governments provided only indirect support.
• For a large majority of the 11 countries with high levels of fertility and available data on policies in 2019,
governments had adopted one or more policy measures aimed at (a) raising the age of marriage or union
formation, (b) raising the age of the mother at the time of her rst birth, or (c) increasing the duration of
time between successive births. Of the 52 countries with intermediate fertility levels and available data
on policies, about half aimed to raise both the age of marriage or union formation and the age of the
mother at the time of her rst birth. Although nearly half of the governments in these two groups (45)
aimed to increase the time between successive births, only 31 did this in combination with the other
two measures.
1
In this report, “high fertility” refers to a level of total lifetime fertility of at least 5.0 births per woman; “intermediate fertility”, between 2.1 and
5.0 births; and “low fertility”, below 2.1 births. “Very low fertility”, a sub-category of “low fertility”, refers to a level below 1.5 births per woman, and
“moderately low fertility”, another sub-category of “low fertility”, refers to a fertility level between 1.5 and 2.1 births per woman.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
2
• Among the 81 countries with low fertility and available data on policies during 2015-2019, one measure
adopted by almost all governments was paid or unpaid maternity leave with job security. Beyond that,
the four most commonly adopted measures were (a) publicly subsidized childcare (88 per cent), (b) child
or family allowances (78 per cent), (c) paid or unpaid parental leave (73 per cent) and (d) paid or unpaid
paternity leave with job security (73 per cent). In addition, over half of these governments provided other
incentives, such as exible or part-time work hours for parents or tax credits for dependent children.
• Among the 102 countries with available data in 2019, 88 governments considered the fertility of
adolescents to be a matter of concern. is was true for almost all of the countries in sub-Saharan Africa
or in Latin America and the Caribbean that had adolescent fertility rates higher than 50 births per
1,000 women aged 15-19 years. Regardless of their specic views on adolescent fertility, the majority
of governments adopted measures to improve the sexual and reproductive health of adolescents by
providing school-based sexuality education and by raising rates of secondary school enrolment and
retention among girls and young women.
• e country case studies illustrate the link between fertility policies adopted by governments and
the fertility patterns and trends prevailing in their countries. Kenya, which had high levels of fertility
as recently as 2000-2005, became the rst country in sub-Saharan Africa to adopt a national family
planning programme in 1967, contributing to a reduction in the country’s fertility level from 8.1 births
per woman in 1965-1970 to 3.5 in 2015-2020. In Argentina, a country where low levels of total lifetime
fertility have been accompanied by high levels of adolescent fertility, government policies have focused
specically on lowering the adolescent birth rate.
• In Hungary, the Government has expressed concern about persistent low levels of fertility and has
adopted a range of policies that explicitly encourage childbirth. By contrast, Australia does not have
an ocial policy to raise the fertility level but has adopted a range of family policies that support
childbearing and childrearing. China, aer implementing a strict one-child policy for three decades,
has in recent years changed course in response to persistent low fertility and rapid population ageing; it
now allows all couples to have three children.
• e ongoing COVID-19 pandemic and resulting economic and social changes have aected fertility
levels in many countries, but this impact may be short-lived. Based on both historical experience and
available evidence about recent changes, it is expected that fertility uctuations from 2021 to 2023 will
be relatively minor and that fertility may return to pre-pandemic levels by around 2025. e COVID-19
pandemic is not expected to have a signicant impact on fertility patterns and trends in the long run.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
3
Introduction
National population policies and family planning programmes have a long history. Policies that aimed to
lower fertility and curb population growth were a response to the rapid growth in populations, particularly
in Asia, that became apparent aer data became available from population censuses conducted in the early
1950s and later. Population experts and national and international leaders began calling for action to stem
rapid population growth (May, 2012). Two academic conferences on population, organized or co-organized
by the United Nations, were held in Rome in 1954 and Belgrade in 1965. Attended mostly by technical
experts, including from less developed countries,
2
these meetings focused on the relationship between
population growth and economic and social development, particularly in less developed countries, and on
policies and programmes to lower fertility and slow population growth.
e World Population Conference, held in Bucharest in 1974, was the rst of three intergovernmental
conferences on population convened by the United Nations. It attracted a broader audience than the earlier
academic conferences, including government ocials from 135 countries, and led to the adoption of the
World Population Plan of Action. Two years aer the Bucharest meeting, the governments of 40 countries,
including the most populous developing countries, initiated family planning policies with the aim of
slowing population growth. By 2013, this number had risen to 160 (de Silva and Tenreyro, 2017). During the
International Conference on Population, convened in Mexico City in 1984, and the International Conference
on Population and Development, held in Cairo in 1994, governments continued to work towards building a
global consensus around an approach to population policies that de-emphasized the pursuit of demographic
targets in favour of promoting women’s empowerment and improving maternal and child health, with an
emphasis on the provision of sexual and reproductive health care, including for voluntary family planning
(May, 2012).
In 1952, India became the rst country to adopt an ocial population policy, committing the country to
reduce substantially its level of fertility and establishing a national family planning programme. Other
countries and areas of Asia, including Sri Lanka, Pakistan, Singapore, Taiwan Province of China and the
Republic of Korea, followed suit.
Some population policies, especially in past decades, included specic quantitative targets and were not
entirely voluntary, sometimes using strong incentives or coercion to ensure widespread adoption of family
planning practices and leading in the most extreme cases to the use of forced sterilization or abortion as
means of population control.
3
However, most national population policies were not coercive and focused
instead on promoting a desire for smaller families with fewer, healthier and better educated children.
Especially since the Cairo conference in 1994, it has been increasingly recognized that population objectives
can be reached faster by giving priority to the needs of couples and individuals instead of focusing on
demographic or numerical targets.
With declining fertility and the progressive ageing of many national populations, the discussion of population
policies has increasingly emphasized objectives of raising the fertility level and promoting population
growth. At the same time, rapid population growth remains a concern in countries with persistent high
levels of fertility, whose governments continue their eorts to promote smaller families and facilitate access
to sexual and reproductive health care and services (United Nations, 2013).
2
A/RES/1838 (XVII), 18 December 1962.
3
See https://publichealthreviews.biomedcentral.com/articles/10.1186/s40985-017-0060-9.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
4
In 1962, the General Assembly requested the Secretary-General to “conduct an inquiry among the
governments of States Members of the United Nations and members of the specialized agencies concerning
the particular problems confronting them as a result of the reciprocal action of economic development and
population changes”.
4
To implement this mandate, the Population Division, currently part of the United
Nations Department of Economic and Social Aairs, conducted the rst United Nations Inquiry among
Governments on Population and Development in 1963 and, since then, has periodically gathered information
on ocial government’s views and policies concerning a wide range of population issues, including fertility
and family planning.
World Population Policies 2021: Policies related to fertility, provides a brief overview of past and present
fertility trends and related policies. It features published data from the World Population Policies Database
(box 1) with more recent updates from the United Nations Twelh Inquiry conducted during 2018-2019.
In addition, the report includes an in-depth analysis of fertility trends and related family policies in ve
countries from dierent world regions and with varying fertility levels. e impact of the socioeconomic
disruptions caused by the COVID-19 pandemic on current and future fertility patterns and trends are
then discussed. e report concludes with a set of policy recommendations that governments may wish
to consider in the current context, taking into consideration possible impacts of the COVID-19 pandemic.
4
A/RES/1838 (XVII), 18 December 1962.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
5
Government fertility and family planning policies through 2019
Fertility levels and trends at the global and regional level
Global fertility started to decline since the early 1960s, from about 5.0 births per woman during 1960-1965
to about 3.0 births during 1990-1995 (United Nations, 2019). In 1994, when the landmark Cairo conference
was held, about 46 per cent of the global population, mostly in Europe and Northern America, lived in
countries with below-replacement fertility (under 2.1 births per woman). Total fertility continued to decline
during the decades following the Cairo conference, reaching just under 2.5 births per woman globally
during 2015-2020. In 2019, nearly half of the global population was living in countries with fertility below
the replacement level.
Nonetheless, there have been signicant variations in fertility by development level and by region. In many
developed countries, fertility had declined to below-replacement levels by 2015-2020. In some countries,
including Greece, Italy, Japan and Spain, fertility had been under 1.5 births per woman for several decades.
Whereas all developing countries experienced fertility declines, with many countries reaching replacement
or below-replacement levels, some 40 countries, mostly least developed countries (LDCs), still recorded
fertility levels of more than 4 births per woman.
During 2015-2020, four out of eight world regions had below-replacement fertility, namely Europe and
Northern America, Australia and New Zealand, Eastern and South-Eastern Asia, and Latin America and
the Caribbean. Fertility in sub-Saharan Africa was still high, with, on average, about 4.7 births per woman.
Average fertility levels in Northern Africa and Western Asia (3.5 births), Oceania excluding Australia and
New Zealand (2.9) and Central and Southern Asia (2.4) remained at the intermediate level.
Evolution of government policies on fertility
An increasing number of governments have undertaken eorts to inuence fertility levels over the past
four decades (table 1). While more than half of all countries (52 per cent) did not intervene or did not have
an ocial policy to inuence fertility in 1976, this share had decreased to just over one quarter (27 per
cent) during the period 2015-2019. Moreover, in 1976, only one out of every four countries aimed to lower
fertility and only 9 per cent of all countries undertook eorts to increase birth rates. e growing number
of countries that aim to increase birth rates appear to be a response to growing concerns about population
ageing. Between 1986 and 2019, the proportion of countries that aim to lower fertility has oscillated between
33 and 35 per cent. e share of governments who focus on maintaining their current fertility levels has
remained rather stable at around 10-15 per cent.
Policies concerning the current fertility level and support for family planning
Policies concerning the level of fertility
Globally, through 2019, nearly three quarters of the governments of the 197 Member and non-member
States of the United Nations had policies to inuence fertility levels. Among them, 69 governments had
policies to lower fertility, 55 governments sought to raise fertility, while another 19 governments aimed to
maintain current levels of fertility. Meanwhile, 54 governments did not have such ocial policies concerning
the level of fertility (appendix table).
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
6
Table 1
Government policies to inuence the level of fertility, 1976-2019 (in percentage)
Year Raise Maintain Lower
No intervention/No
ocial policy
1
Total
1976 9 13 27 52 100
1986 12 10 33 46 100
1996 14 10 42 34 100
2005 20 16 40 24 100
2019 28 10 35 27 100
e available data show a close association between the types of fertility policies adopted by governments
and the prevailing levels of fertility in the country. Among the 69 countries where governments adopted
policies to lower fertility, 10 countries had high levels of fertility and another 50 countries had intermediate
fertility levels. Also, for the 55 countries with policies to raise fertility, 40 had low fertility levels, of which 18
were lower than 1.5 births per woman on average. For the 19 countries that chose to maintain current levels
of fertility, most had fertility levels around the replacement level.
For governments with policies to lower fertility, one major underlying reason was to curb rapid population
growth. Conversely, the major reasons for governments with policies to raise fertility were to counter
population decline and address population ageing. Aside from these specic motivations, a signicant
number of governments stated that ensuring sustainability for future generations was a major driver for
their policies on fertility.
Governments in developed countries were more likely to adopt policies to raise levels of fertility. Most
of these countries had already reached below-replacement fertility levels many years ago. Some countries,
including Greece, Italy, Japan and Spain, have had fertility levels below 1.5 births per woman for decades.
However, 14 out of 30 developed countries with moderately low levels of fertility (between 1.5 and 2.1 births
per woman), such as Australia, Canada, Germany, Sweden, and the United States of America, had no ocial
policies to inuence fertility levels.
Nearly half of governments (46 per cent) in developing countries had policies to lower fertility levels,
whereas about one quarter did not have such policies.
5
Several developing countries from dierent parts
of the world and with varying fertility levels have adopted policies to maintain current fertility levels. ese
include Argentina (2.3 births per woman), Viet Nam (2.1) and the United Republic of Tanzania (4.9).
Most LDCs continue to experience rapid population growth driven mainly by high fertility, particularly in
sub-Saharan Africa. In recent decades, a growing number of governments of LDCs had policies to address
rapid population growth (United Nations, 2017). During the period 2015-2019, nearly 80 per cent of the
LDCs had policies to lower fertility. Some LDCs, which already reached below replacement-level fertility,
such as Bangladesh, Bhutan and Nepal, had policies in place to lower fertility.
Signicant regional variations exist in policies concerning present fertility levels (table 2). In sub-Saharan
Africa and Oceania (excluding Australia and New Zealand), where relatively high fertility and rapid
population growth are more common than in other regions, governments were more likely to adopt policies
to lower fertility. By contrast, countries with persistent low levels of fertility in Europe and Northern Africa,
5
Developing countries without policies to lower fertility included countries with low fertility, such as Brazil, and countries with intermediate fertility,
such as South Africa.
Source: World Population Policies Database, available at: www.un.org/development/desa/pd/data/world-population-policies.
1
Information on “No ocial policy” was gathered separately from “No intervention” starting with the 2015 revision of the World Population
Policies Database. In older revisions, “no ocial policy” was assumed to be included under “No intervention”.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
7
as well as in Eastern and South-Eastern Asia, were more likely to adopt policies to raise fertility. Several
countries with moderately low fertility in these two regions did not have an ocial policy to inuence the
level of fertility, including Canada, Czechia, Denmark, Germany, Norway, Sweden, the United Kingdom of
Great Britain and Nothern Ireland and the United States of America. Australia and New Zealand, also with
moderately low fertility, had no such policies in place. Most countries in Latin America and the Caribbean
either did not have policies targeting fertility levels or had policies to maintain current levels.
Table 2
Policies concerning the present fertility level of countries or areas, by region, 2015-2019
(Number of countries or areas in each region and the world)
Region
Policies concerning the present level of
fertility
No ocial
policy Total
(Number of countries or areas)
Raise Lower
Maintain
current
levels
Sub-Saharan Africa 3 35 2 8 48
Northern Africa and Western Asia 9 6 4 5 24
Central and Southern Asia 4 7 3 14
Eastern and South-Eastern Asia 7 3 1 5 16
Latin America and the Caribbean 3 8 6 16 33
Europe and Northern America 27 1 4 14 46
Australia and New Zealand 2 2
Oceania* 2 9 2 1 14
World 55 69 19 54 197
Government’s support to family planning
Access to family planning and reproductive health services is critical to the health of women and children
worldwide. Improving such access can help to prevent maternal deaths and reduce unwanted pregnancies.
Target 3.7 of the Sustainable Development Goal (SDG) 3 on “Good health and well-being: Ensure healthy
lives and promote well-being for all at all ages” calls on countries “to ensure universal access to sexual
and reproductive health-care services, including for family planning, information and education, and the
integration of reproductive health into national strategies and programmes by 2030”. In 2019, 80 governments,
or nearly 80 per cent of 103 governments with available data, reported providing direct support for family
planning. Of these governments, 68 provided both direct and indirect support.
6
In addition, another 18
countries supported the provision of family planning services through non-governmental organizations
only. Together, over 95 per cent of governments among those with available data (103) provided either direct
or indirect support for family planning.
6
Direct support for family planning refers to governments providing contraceptive methods directly through governmental sources, while indirect
support refers to governments providing nancial support for the provision of contraceptive methods by non-governmental organizations.
Source: World Population Policies Database, available at www.un.org/development/desa/pd/data/world-population-policies.
* Oceania excluding Australia and New Zealand.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
8
Box I. Data sources and limitations
Data used in preparing this report were obtained primarily from the World Population Policies Database,
maintained since 1976 by the Population Division of the United Nations Department of Economic and
Social Aairs. e most recent update of the database is based on the Twelh United Nations Inquiry among
Governments on Population and Development conducted between September 2018 and August 2019.
e World Population Policies Database provides comprehensive information on national population policies
and programmes for 197 countries or areas, including all 193 Member States, 2 Observer States (Holy See and
State of Palestine) and 2 non-member States (Cook Islands and Niue) of the United Nations. e database
shows the evolution of government’s views, policies and programmes with respect to population size and
growth; population age structure; spatial distribution of populations, internal migration and urbanization;
fertility, reproductive health and family planning; health and mortality; and international migration.
Between 1976 and 2015, the Database was updated biennially by conducting a detailed country-by-country
review of national plans and strategies, programme reports, legislative documents, ocial statements
and various international, inter-governmental and non-governmental sources, as well as by using ocial
responses to the United Nations Inquiry among Governments on Population and Development, conducted
quinquennially since 1963.
e 2017 revision of the Database focused on abortion laws and policies in all countries of the world, based
on a global survey on abortion issues and a careful assessment of legislative documents, conducted jointly
with the World Health Organization during 2016-2017.
Starting with the 2019 revision, the Database has been updated based entirely on ocial government’s
responses to the Inquiry. e 2019 revision of the Database was based on 86 government responses to the
ageing and urbanization module, 107 responses to the fertility, family planning and reproductive health
module, and 111 responses to the international migration module of the Twelh Inquiry, conducted during
2018-2019.
e most recent revision of the Database (2021) is based on 109 government responses to the reproductive
health module, and 89 responses to the international migration module of the irteenth Inquiry, conducted
between November 2020 and October 2021.
In this report, data on selected fertility-related policies from the 2015 and 2019 revisions of the Database have
been combined to create a pooled dataset for all 197 countries or areas covering the period 2015-2019. For
countries or areas with information available in both revisions, the more recent information from the 2019
revision was used. e pooled variables describing the policy situation during the 2015-2019 period include
(a) policies on fertility, (b) measures to improve family/work balance for childbearing and childrearing, and
(c) measures to improve sexual and reproductive health of adolescents.
For other policy questions discussed in this report, including (a) underlying reasons for the current fertility
policy, (b) policies concerning age of marriage or union formation, mother’s age at the time of her rst
birth, and spacing between successive births, (c) ocial views on adolescent childbearing, and (d) policies
concerning the provision of modern contraceptive methods, the data are from the 2019 revision of the
Database for 107 countries or areas that responded to the fertility, family planning and reproductive health
module of the Twelh Inquiry. e most recent (2021) revision of the Database based on the irteenth
Inquiry does not include data on fertility-related policies.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
9
Policy measures to lower fertility in high and intermediate fertility countries
Raising the age of marriage or union formation and the age at rst birth, increasing the spacing between
births, and expanding access to modern contraceptive methods are considered to be eective means to
improve sexual and reproductive health and to help reduce fertility levels. Many governments have adopted
some or all of these measures.
High fertility countries
In 2019, there were 11 countries (all LDCs in sub-Saharan Africa) with fertility levels above 5.0 births per
woman (United Nations, 2019). Nine of them also had relatively high adolescent birth rates (ABR), above
100 births per 1,000 women aged 15-19 years.
Among the 11 countries in sub-Saharan Africa with fertility higher than 5.0 births per woman, all except
Somalia had policies to lower fertility, mainly to curb rapid population growth and ensure sustainability for
future generations by: (a) raising the age of marriage or union formation, (b) raising the age of the mother
at the time of her rst birth, or (c) increasing the duration of time between successive births.
Ninety per cent of governments in high fertility countries provided contraceptive methods directly through
public programmes as well as indirectly through government’s permission (80 per cent) or nancial support
(50 per cent) to non-governmental sources. None of the governments in high fertility countries restricted
access to contraceptive methods (gure 1).
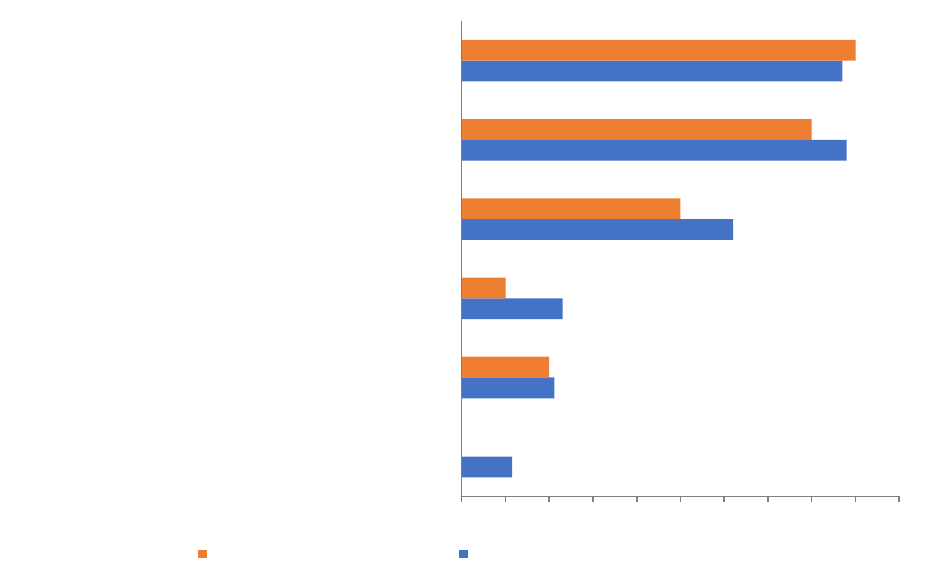
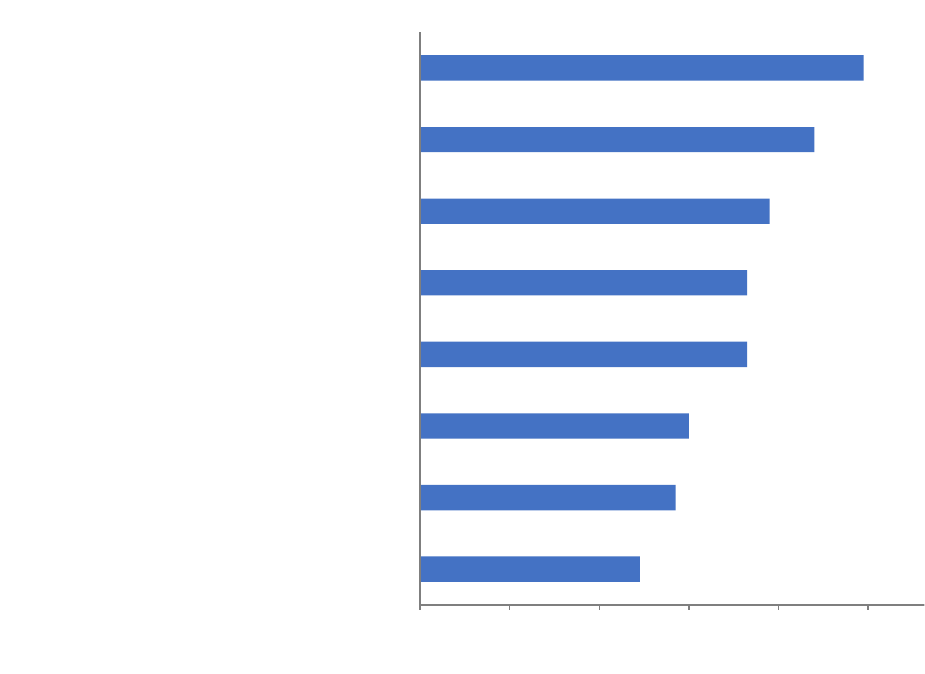
Figure 1
Policy measures taken by governments concerning the provision of modern contraceptive methods, 2019
(in percentage)
12
21
23
62
88
87
0
20
10
50
80
90
0 10 20 30 40 50 60 70 80 90 100
Restrict access to contraceptive methods
Charge clients for family planning service or commodities
provided through government sources
Subject family planning commodities to duties, import taxes or
other fees
Provide financial support for the provision of contraceptive
methods by non-governmental sources
Permit non-governmental sources to provide contraceptive
methods, without providing financial support to such sources
Directly provide contraceptive methods through government
sources
Countries with high fertility Countries with intermediate fertility
Source: World Population Policies Database, available at www.un.org/development/desa/pd/data/world-population-policies.
Note: Data refer to 10 high fertility countries and 52 intermediate fertility countries in 2019.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
10
Intermediate fertility countries
In 2019, for countries covered in the World Population Policies Database, there were 92 countries with
intermediate fertility (between 2.1 and 5 births per woman) (United Nations, 2019). Of these, 29 countries,
mostly in sub-Saharan Africa, had fertility levels higher than 4.0 births per woman. Meanwhile, there were
also a number of countries with fertility approaching the replacement level, including Argentina, India,
Iran, Mexico, Sri Lanka and Tunisia. Over half of these governments (50) had policies to lower fertility
during 2015-2019, while over one h (22) did not have ocial policies. During this time, governments in
a number of countries in Central Asia and Western Asia, had policies to raise the fertility level, including
Saudi Arabia, Iran, Israel, Kazakhstan, Kuwait, Kyrgyzstan, Mongolia and Turkmenistan.
About half of the 52 countries with intermediate fertility levels and available data on policy measures to
inuence fertility levels, located in sub-Saharan Africa, Central and Southern Asia, Eastern and South-
Eastern Asia, or Latin America and the Caribbean, sought to raise the age at marriage or union formation
as well as the age at rst birth. Although nearly half of the governments promoted the spacing of birth, few
adopted such a policy in combination with the other two measures.
Most countries with intermediate fertility levels facilitated the provision of modern contraceptive methods,
regardless of whether they had explicit policies targeting fertility. Nearly 90 per cent of these countries
or areas directly provided contraceptive methods through governmental sources, while also nearly 90 per
cent of governments permitted non-government organizations to provide contraceptive methods without
providing nancial support to these NGOs. In addition, over 60 per cent of governments provided nancial
support for the provision of contraceptive methods by non-governmental sources. About three quarters of
governments in intermediate fertility countries provided both direct and indirect support for the provision
of modern contraceptive methods. Only a few governments in these countries (6) applied restrictive policies
in the provision of contraceptive methods, with 12 subjecting family planning commodities to duties, import
taxes or other fees.
Policy measures to improve family/work balance for childbearing and
childrearing in low fertility countries
Among countries with available data on policy measures regarding family/work balance during 2015-2019,
81 countries had fertility below the replacement level (2.1 births per woman), of which 20 had fertility levels
below 1.5 births per woman. While most of these countries were developed countries located in Europe and
Northern America, plus Japan, Australia and New Zealand, some were developing countries located in Latin
America and the Caribbean, Northern Africa and Western Asia, or Eastern and South-Eastern Asia. About
half of the low-fertility countries had adopted policies to raise fertility, (gure 2), about one third of these
countries had no fertility-related policies, mostly in Europe and Northern America or in Latin America and
the Caribbean. Most of these countries were concerned about population decline and population ageing,
and some expressed concerns regarding sustainability for future generations.
All low-fertility countries, with the exception of the United States of America, had introduced paid or unpaid
maternity leave for childbirth with job security. e other four commonly adopted measures were publicly
subsidized childcare (88 per cent), child or family allowances (78 per cent), paid or unpaid parental leave
for childcare at home and paid or unpaid paternity leave for childbirth with job security (both 73 per cent).
In addition, over half of the countries oered exible or part-time work hours for parents or tax credits for
dependent children.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
11
Figure 2
Percentage of governments in low-fertility countries with policy measures to improve work/family balance,
2015-2019
49
57
60
73
73
78
88
99
0 20 40 60 80 100
120
Baby bonus (lump sum payment)
Tax credit for dependent children
Flexible or part-time work hours for parents
Paternity leave for childbirth with job security (paid or
unpaid)
Parental leave for childcare at home (paid or unpaid)
Child or family allowances
Publicly subsidized childcare
Maternity leave for childbirth with job security (paid or
unpaid)
Although many governments did not have ocially promulgated policies on fertility, the above measures
help balance work and family life and are therefore greatly benecial for childbearing and childrearing.
For example, maternity leave, publicly subsidized childcare and exible work arrangements can help many
working parents to have children and remain employed. Tax credits for dependent children and baby
bonuses are measures adopted by some governments as nancial incentives for childbearing.
Increasingly, governments in countries with high and intermediate levels of fertility have also adopted
measures to help balance work and family life. Almost all of these governments have instituted paid or
unpaid maternity leave with job security, while over half of these governments have instituted paid or unpaid
paternity leave with job security, or child allowances.
Measures to improve adolescent sexual and reproductive health
Adolescent pregnancies and births are closely associated with negative outcomes in sexual and reproductive
health and in the social and economic well-being of adolescents. Achieving SDG target 3.7, which calls for
universal access to sexual and reproductive health-care services, including for family planning, information
and education, is critical for improving adolescent sexual and reproductive health.
Source: World Population Policies Database, available at www.un.org/development/desa/pd/data/world-population-policies.
Note: Data refer to 82 countries or areas with below replacement fertility during 2015-2019. Multiple responses possible.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
12
Among the 102 countries with data available on government’s views on the fertility of adolescents in 2019,
a large majority (86 per cent) considered it as either a major or a minor concern. Sixty-eight governments,
mostly in countries with adolescent birth rates (ABRs) above 50 births per 1,000 women aged 15-19 years,
considered it as a major concern. is includes almost all governments of countries in sub-Saharan Africa
and in Latin America and the Caribbean that responded to the Inquiry. Another 20 governments, mostly
in countries with ABRs below 50 per 1,000, considered the ABR level to be a minor concern. Another 14
governments were not concerned about the level of the ABR in their countries.
Regardless of their views on adolescent fertility, most governments have adopted policies to improve the
sexual and reproductive health of adolescents, although this was more oen the case in countries with
relatively high levels of adolescent fertility. During 2015-2019, more than three quarters of governments
provided school-based sexuality education, and 55 per cent had adopted measures to expand girls’ secondary
school enrolment and retention, particularly in countries with high levels of adolescent fertility.
7
7
Over 50 births per 1,000 women aged 15 to 19 years.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
13
Government policies and related responses: Case studies
is chapter contains ve case studies of policies related to fertility and family planning for countries with a
range of fertility levels from dierent parts of the world, namely Kenya, Argentina, Hungary, Australia and
China. ese case studies provide a more detailed analysis of the evolution of policies related to fertility,
population and family planning that should be understood in the respective historical, cultural and political
context of a given country.
e rst case involves Kenya, a high-fertility country in sub-Saharan Africa with policies to lower fertility
and curb rapid population growth. Kenya was the rst country in sub-Saharan Africa to adopt a family
planning programme in 1967, which helped to bring the country’s fertility level down from 8.1 births per
woman during 1965-1970 to 3.5 births per woman during 2015-2020. e second case, Argentina, also
focuses on government’s eorts to reduce fertility, but with a specic focus on the country’s history of high
adolescent fertility. e third case is that of Hungary, which has experienced a steady decline in population
size since 1980 and has a long tradition pursuing pronatalist policies. e fourth case, Australia, concerns a
country with no ocial population policy but with a range of family policies that support childbearing and
childrearing. e h case, China, examines the renowned one-child policy that was in place from the late
1970s to the mid-2010s for the purpose of lowering the country’s fertility level, as well as its phasing out in
recent years in response to concerns about the rapid ageing of the population.
Policies to lower fertility: Kenya
Kenya has a long tradition of addressing rapid population growth, including eorts to reduce fertility
levels through the promotion of family planning and other indirect government interventions to inuence
demographic trends. Kenya was the rst sub-Saharan country to launch a family planning programme.
e use of modern contraception in the country dates back to the pre-independence period when, in
1957, the Family Planning Association of Kenya (FPAK) was formed. When the FPAK became an aliate
of the International Planned Parenthood Federation (IPPF) in 1962, the campaign to control fertility was
intensied (Ndeti and Koesoebjono, 1973). Shortly aer gaining independence in 1963, the Government had
several population concerns, rst and foremost of which was high population growth. In 1965, the Kenyan
Government invited the United States-based Population Council to make recommendations on the optimal
rate of population growth, on a programme for achieving this rate, on the administration of the programme,
and on procedures for obtaining funds and technical assistance for carrying out the programme (Population
Council of the United States of America, 1966).
National population policy
A delegation of the Population Council arrived in June 1965 and submitted its report three months later
to the Ministry of Economic Planning and Development (Republic of Kenya, 1967; Population Council of
the United States of America, 1966). e report and recommendations served as the basis for formulating a
national population policy. e aim of the family planning programme would be to achieve a decline in the
population growth rate by limiting the number of children. It recommended that the Government declare
its goal to reduce the population growth rate and to embark on a national programme “to make the means
of limiting the number of their children, as well as assistance to infertile women desiring children, available
to every family” with the ambitious goal of reducing fertility by as much as 50 per cent in 10 to 15 years.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
14
National family planning programme
e Kenyan Government incorporated many of the recommendations of the Population Council into
government directives and in the 1966-1970 and 1970-1974 development plans. A National Family Planning
Council was established in February 1967, followed by the launch of a national family planning programme
in May 1967 (Frank and McNicoll, 1987). e family planning programme would make information and
supplies available free of charge through government and private facilities to families wishing to avail
themselves of those services through voluntary means and within religious prescriptions. A timeline of
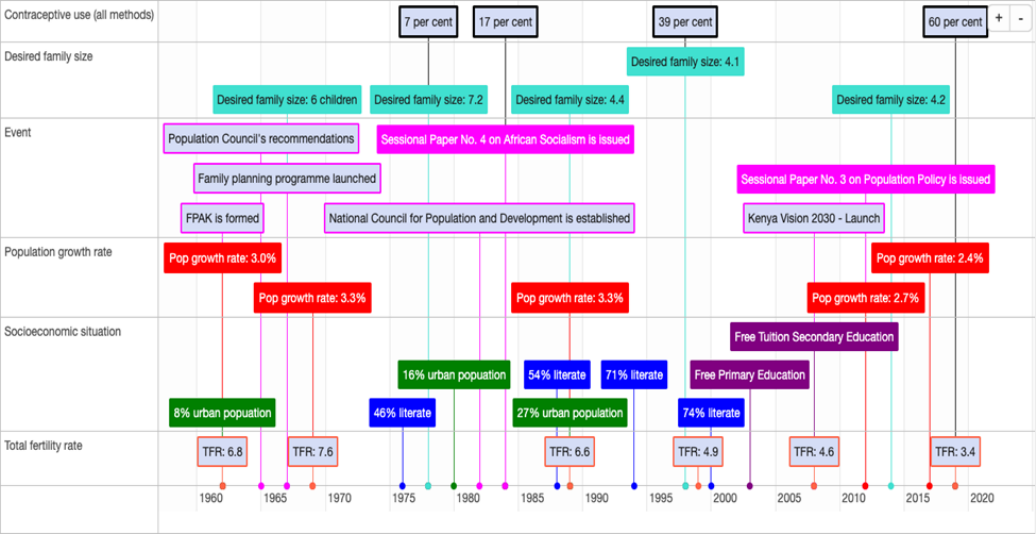
Kenya’s fertility policy is shown in gure 3.
Figure 3
Timeline of fertility policy in Kenya, 1960-2019
Kenya framed population growth and its implications primarily as a national development issue, emphasizing
the voluntary nature of family planning, taking into account individual and family needs as well as social,
cultural and other sensitivities. It integrated population issues in every sector of government and established
the National Council for Population and Development to guide the Government’s ministries, agencies and
sectors in identifying how to integrate population issues in their programmes. It provided the resources and
devolved its implementation down from the Oce of the Vice-President to district planning committees,
district population and family planning committees, and local communities. It encouraged and allowed
private entities and NGOs to participate in implementing the national family planning programmes and
tasked the National Council for Population and Development to coordinate the activities and eorts of the
Government, private agencies, NGOs, and donors. e partnership with the private sector helped to sustain
the family planning services and to reach remote rural areas, particularly when the number of new acceptors
stalled. Kenya became, in a way, a laboratory of policy development and programme implementation in sub-
Saharan Africa.
Source: Prepared by the Population Division of the United Nations Department of Economic and Social Aairs.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
15
Kenya accommodated the views of a foreign advisory mission, which stayed and assured the implementation
and modications of the policy. e delegation of the Population Council provided support in several areas
of programme implementation, including training of local personnel in population matters, funding and
supervising critical research. e uninterrupted presence and involvement of the Population Council in
implementing and adjusting the national population policy inspired several foreign agencies, institutions
and donors to participate in Kenya’s eort to manage its own population growth. Many of those entities still
have a physical presence in the country.
Although the family planning programme was conceived to contain population growth, it became eventually
an essential part of the country’s maternal and child health care programmes. Indeed, the implementation of
the national population policy shied to integrate family planning into the national health programme under
the umbrella of maternal and child health. Even as the Programme of Action from the Cairo conference in
1994 shied the emphasis of population policies and programmes towards improving the quality of people’s
lives, including by expanding access to sexual and reproductive health services, Kenya stayed the course in
its eorts to limit population growth and mitigate its negative impacts on national development. Consistent
with the Programme of Action, the high level of adolescent fertility was identied in 1997 as one of the key
challenges that needed to be addressed (Republic of Kenya, 1997).
e National Council for Population and Development and the Population Studies and Research Institute at
the University of Nairobi played critical roles in tracking the progress in the implementation of the national
population policy, assessing its challenges and constraints, providing modications to implementation and
governance, among other activities. ese two national institutions, together with other entities, produced
seminal papers and policy briefs that were the basis of programme implementation.
Perhaps the most critical factor in the evolution and implementation of the national population policy has
been the continued commitment of the Kenyan Government and its emphasis on a participatory process
in formulating, implementing and adjusting the policy. e Government’s eorts were buoyed, to this day,
by sustained donor funding and internal high-level political support. In particular, the government’s role in
population matters was enshrined in the 2010 Constitution (Constitution of Kenya, 2010). In accordance
with the Constitution, every Kenyan is guaranteed to receive health-care services, including for reproductive
health and family planning. e Constitution requires that the programmes and projects are implemented
in close consultation and collaboration with local governments.
In 2012, the Government launched consultations at the local, regional and national levels on the country’s
population policy for national development. Following those consultations, the Government launched a
new policy to manage its persistent rapid population growth and youthful population structure through
a multi-sectoral approach (National Council for Population and Development, 2012). Between 2009 and
2030, the new policy aims to reduce the number of children a woman has over her lifetime from 4.6 to
2.6; increase contraceptive use of modern methods from 40 to 70 per cent; reduce the population growth
rate from 2.5 to 1.5 per cent; reduce the dependency ratio from 87 to 54; and increase the median age of
the population from 17 to 25 years in line with Vision 2030, the 2010 Constitution, the SDGs and other
national goals and international aspirations. e United Nations Population Fund (UNFPA) has supported
Kenya’s population policies by strengthening reproductive health services, improving supply chains for
contraceptives, advocacy against gender-based violence, and facilitating integration of population dynamics
into policy formulation (UNFPA, 2021a).
8
8
See https://kenya.unfpa.org/en.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
16
Already, in 2019, the proportion of married women using modern methods of contraception was 56 per
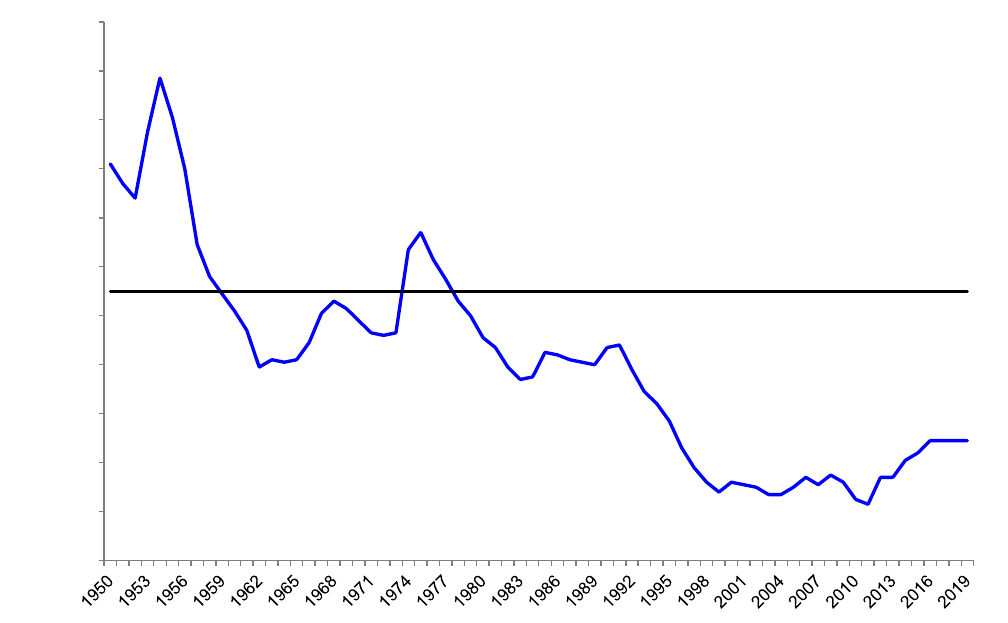
cent, up from 39 per cent in 2009, and the total fertility rate had declined to 3.4 children per woman,
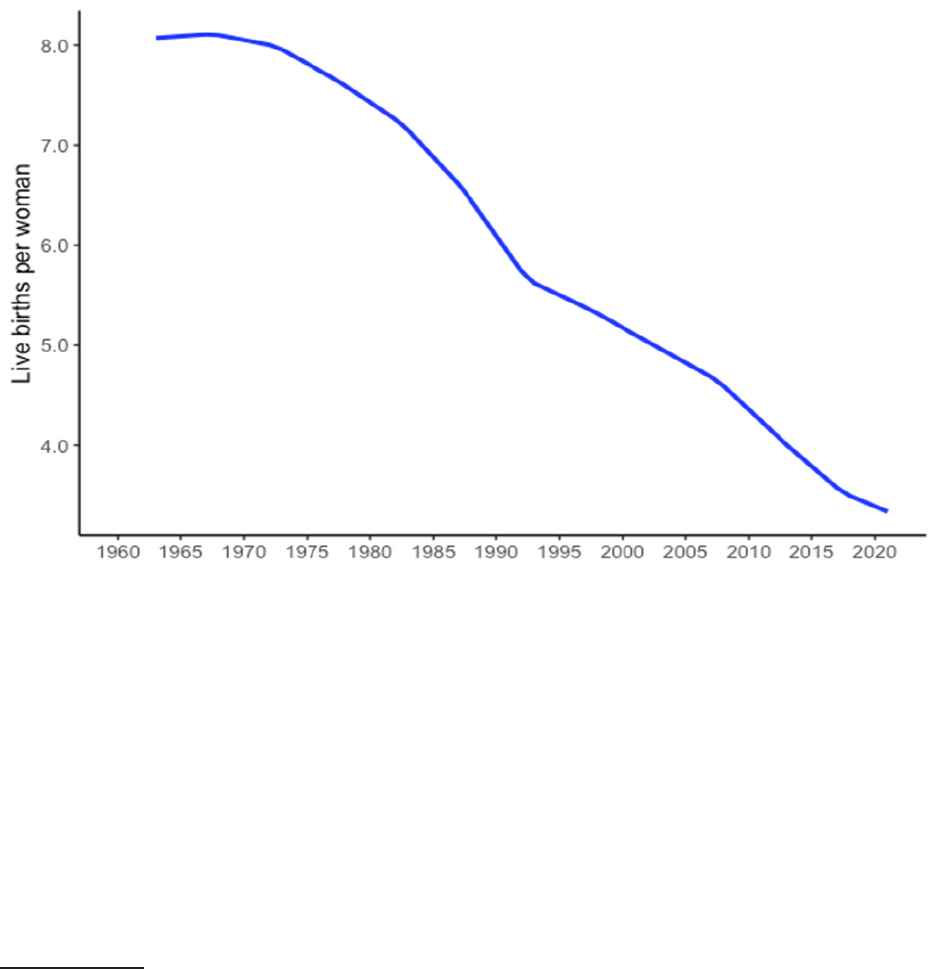
down from 4.5 children per woman in 2012 (gure 4). e Government is cognizant of the challenges
in implementing the policy, which includes the diminished share of resources for population and family
planning activities due to competing or new and emerging issues, such as the ght against HIV/AIDS, and
high levels of adolescent fertility partly attributed to early marriages and polygamy, and during the last two
years, eorts to contain the spread of COVID-19.
Figure 4
Total fertility rates in Kenya, 1960-2021
When the family planning programme was rst launched, the population was not ready in many ways,
including materially, culturally and psychologically. Nonetheless, the Government and donors consistently
supported the population policy and family planning programme. Generations have since been born and
grown up surrounded by ubiquitous family planning services and information that defy the shame associated
with the use of family planning services in many other sub-Saharan countries.
9
As the population became
more accepting, the family programme succeeded in more than halving the total fertility rate from 7.7 to
3.3 children per woman between 1984 and 2021. By all accounts, Kenya is deemed to have led a successful
family planning programme (Aliyu, 2018; May, 2017), alongside Ethiopia, Madagascar, Malawi, Rwanda,
South Africa and Zimbabwe.
9
A recent study associated the implementation of high-quality programmes in sub-Saharan Africa with rapid changes in reproductive behaviour
(Bongaarts, 2020).
Source: United Nations (2019).

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
17
Policies to discourage adolescent childbearing: Argentina
Today, Argentina is a low-fertility country that has historically been either a pronatalistor or pro-maternalistic
country, or both (Cepeda, 2014). Like most countries in Latin American and the Caribbean, a majority
of the country’s population ascribe to the Roman Catholic faith, a religion that inuenced many policies,
including those related to fertility. Historically, Argentina is also a country of immigrants, well beyond the
colonization period. Aer gaining independence in 1816, Argentina became one of the world’s top receivers
of immigrants, most of them from Spain, Italy and other European countries. Despite its relatively overall
low level of fertility since the twentieth century, Argentina exemplies the persistence of high fertility among
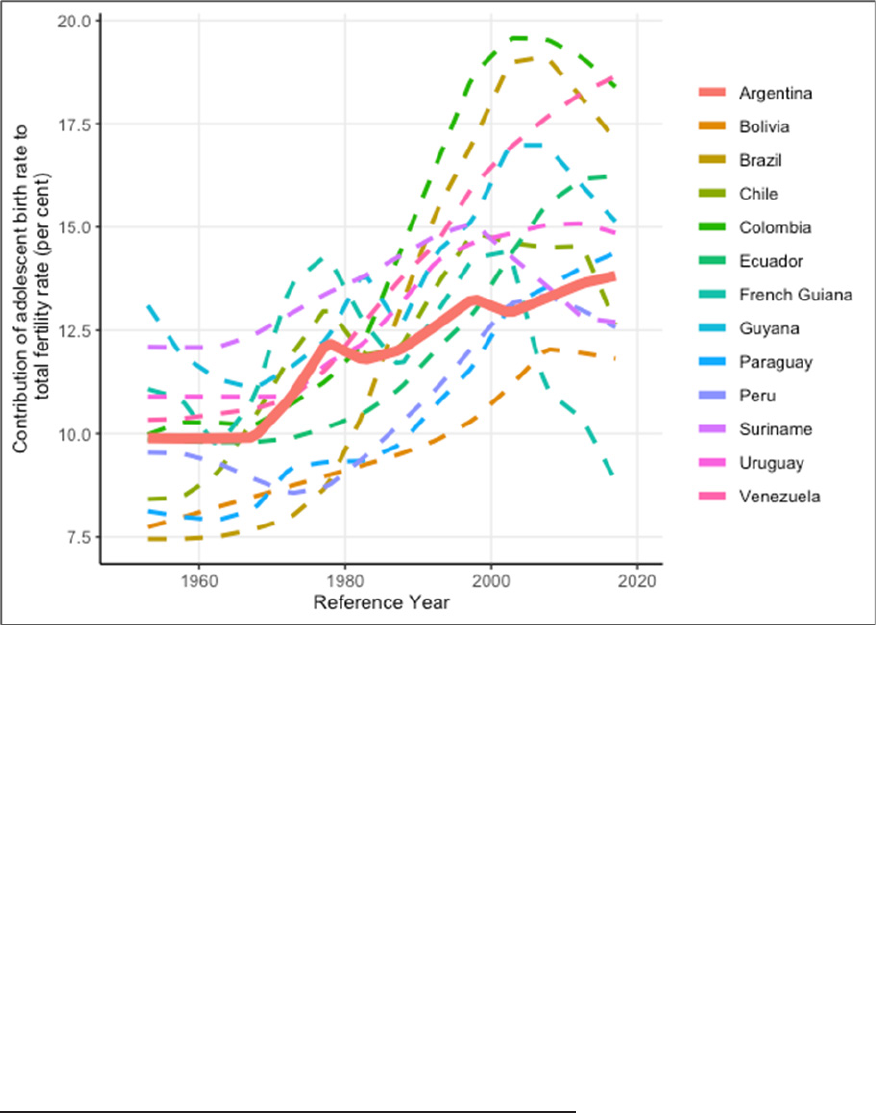
adolescents in the region (gure 5) and an increasing contribution of adolescent births to total fertility.
Population policies in the country should be placed within the larger context of major socio-political
changes in Argentina (Novick, 2001). In the period preceding 1930, women were mostly conned to family
roles. Aer 1930, women were granted some liberties and civil rights, were allowed into the labour force and
given certain protections in the workplace: their employment could not be terminated because of marriage,
they were granted maternity protection, including medical care and nancial compensation, and pregnant
women were prohibited to work during the 30 days preceding a birth and during the 45 days following a
birth.
First population congress, 1940
At the rst population congress, or Primer Congreso de la Población (PCP), convened in 1940, major concerns
were raised about the slowdown in population growth. During the period 1935-1940, the population growth
rate had declined to 1.6 per cent, down from 2.7 per cent for the period 1925-1930. e slow population
growth rate and the decline in fertility were seen as posing serious limitations for the future economic
growth of the nation (Novick, 2001).
e PCP generated a lot of media attention, editorial commentary and public discussions. It was a watershed
event that informed population policy in the ensuing years. During 1945-1955, the Government assumed
greater responsibility for women and children’s health (Novick, 2001; Ramacciotti, 2003). It provided
subsidies for births, granted employment preference in hiring and retention of parents and exempted
or reduced taxes for large families (Ramacciotti, 2003). Children previously classied as legitimate or
illegitimate were now classied as born in wedlock or out of wedlock, with other discriminatory categories
and designations phased out. For the rst time, parents who did not meet their paternal obligations could
be imprisoned (Novick, 2001).
From the 1950s through the early 1970s, the Government continued to expressly declare its responsibility
for the health of mothers and children, implementing a policy that guaranteed free medical care and basic
foodstus. In 1974, the Government created a national commission on demographic policy, the Comisión
Nacional de Política Demográca, to support population growth. In that same year, at the World Population
Conference in Bucharest, Argentina joined other countries in the argument against the Malthusian view of
population growth. In the meantime, however, adolescent fertility had begun to become a concern in the
1970s, a decade later than in Europe and the United States of America (Gogna and others, 2008), because of
the strong pronatalist sentiments in Argentina.
Petracci, Ramos and Szulik (2005) have summarized the evolution of policies on reproductive health in
Argentina since the 1980s as involving three phases. First, the gradual opening of public space and receptivity
of reproductive health issues. Second, the passing of a national sexual and reproductive health law. ird, the
successful development of public policy and programmes, despite the pressures from conservative groups
and contradicting policies over the lifetime of several dierent governments to date.
10
10
As Robinson and Ross (2007) have observed, governments implement policies by enacting laws, creating implementing agencies, and expending
public resources. ese actions provide the framework within which policy responses and endurance occur. Argentina is emblematic that the
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
18
Figure 5
Contribution of adolescent birth rate (births to women aged 15-19 years) to total fertility rate, South American
countries (in percentage)
International agreements
Following the ratication of the Convention on the Elimination of All Forms of Discrimination against
Women in 1985, and the agreements reached at the International Conference on Population and Development
in 1994 and the Fourth World Conference on Women in 1995, a strong public consensus emerged around
key reproductive health issues (Petracci, Ramos and Szulik, 2005). Aer the unsuccessful attempt to include
a section penalizing abortion in the amendment of the National Constitution in 1994, many provinces
and municipalities established local reproductive health programmes, undeterred by the position against
abortion adopted by the Argentine Government together with the Vatican in Cairo in 1994.
11
Adolescent fertility as an issue
e adolescent fertility rate rose and peaked towards the end of the 1980s at 80 births per 1,000 adolescent
girls.
12
By 2001, Argentina was experiencing a serious socioeconomic and political crisis, with almost half
of its population living in poverty and 19 per cent of the labour force unemployed. Millions of young people
were neither in school nor working (Reina and Castelo-Branco, 2014).
political and social context might change but, oen, the policy responses endure.
11
Novick (2001) has observed that the Argentine Government’s position against abortion at the Cairo conference in 1994 did not necessarily imply
a pro-birth policy at the domestic level.
12
Census and survey data show that half of adolescent mothers aged 15-19 were living with their spouse or consensual partner in 2001 and 1 in 10
were divorced or separated (Gogna and others, 2008; López, 2006).
Source: United Nations (2019).

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
19
In 2003, the Government created a National Programme for Sexual Health and Responsible Procreation,
which was tasked with the development and implementation of public policies on sexual and reproductive
health. e programme is aimed at the population in general, without discriminating against any sector
or population group.
13
e tasks specic to adolescents included the prevention of unwanted pregnancy
and the promotion of sexual health. is programme distributes contraceptive commodities free of charge
throughout the country. Under the 2006 National Comprehensive Sexual Education Programme, (Ministerio
de Justicia y Derechos Humanos, 2006), comprehensive sexual education became a right of all children,
adolescents and young people who attend the public and private schools at the primary and secondary levels
(Malnis, 2018).
14
Argentina launched a conditional cash transfer programme (Asignación Universal por Hijo) in 2009, a
monthly cash allowance for each unmarried child under the age of 18 years—or with no age limit for a child
with a disability—whose household members are unemployed or informal workers. e programme provides
the subsidy to only one of the parents, prioritizing the mother, and for up to ve children (Administración
Nacional de la Seguridad Social, 2021; Badaracco, Gasparini and Marchionni, 2016).
Discussion
Argentina experienced a peculiar trend in fertility levels. e fertility transition in Argentina occurred long
before hormonal contraceptives were available, indicating that fertility was traditionally controlled by the
use of periodic abstinence, withdrawal and abortion (Gogna and Pantelides, 2009). Despite the decades-
long pro-maternal and pronatalistpolicies and programmes, and the intermittent ban on family planning
activities and restrictions on abortion, the present fertility levels were reached, in part, by using modern
contraception and abortion. e overall fertility decline was associated mostly with a reduction in inequality
and poverty in Argentina and in Latin America more generally (Badaracco, Gasparini and Marchionni,
2016).
e current level of fertility in Argentina is comparable to average total fertility rates in the Latin American
and Caribbean region. Concern remains, though, about the trends in the adolescent fertility rate, which
are above the regional average, despite the policies and programmes that have been implemented. e
adolescent birth rate has declined at a slower pace than the total fertility rate and it remains high at 61.7 per
1,000 adolescent women, sustained by the high birth rates among girls in the poorer socioeconomic strata,
a reection of inequity (Reina, and Castelo-Branco, 2018). Estimates of the contribution of abortion to
fertility decline show that in the late 2000s, an average of 450,000 unsafe abortions per year were performed
in Argentina, or 0.64 abortions per birth, suggesting a shortfall in policy eectiveness or conicting impacts
on wanted fertility.
15
e availability of contraceptive commodities and services is not necessarily associated with fertility
intentions. Studies in Argentina and elsewhere have observed that many women and adolescents—especially
those in the lower socioeconomic strata—desire motherhood from a very young age because it increases self-
esteem, social approval and prestige within a woman’s family and community ( UNICEF, 2001; López, 2006;
Dyer, 2007; Ombelet and others, 2008; Kane and others, 2019). A study by López (2006) shows that three out
of ve sexually active adolescent girls aged 15-19 were using contraception in Argentina, although a majority
were already mothers, some with more than one child. Subsequent research shows that more than 80 per
cent of adolescents in Argentina were not using a contraceptive method when they became pregnant, even
though they did not necessarily want to have a child (Reina, and Castelo-Branco, 2018; Gogna and others,
2008). Also, access and use of contraception by adolescents in Argentina is still controversial, particularly in
13
e law that established the National Programme of Sexual Health and Responsible Procreation is reproduced in Reina and Castelo-Branco (2014).
14
However, 75 per cent of the adolescents in the last two years of high school indicate that the school does not oer them sex-education topics that
are of interest and relevant to them (Equipo Latinoamericano de Justicia y Género (ELA), 2020).
15
Even though abortion is legally restricted, studies in 2008 show that 5 per cent of adolescents in Argentina had an abortion (Gogna and others,
2008) and that 16 per cent of the hospital admissions for abortion complications were girls under 20 years of age (Reina and Castelo-Branco, 2014).
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
20
some poor provinces where the inuence of the Catholic Church and other conservative forces is still strong
(Gogna and Pantelides, 2009).
ere are suggestions that the high levels of adolescent fertility in Argentina could be partly the unintended
result of policies and programmes, such as the cash transfers for young mothers, that were designed to
mitigate the negative association between socioeconomic inequalities and adolescent fertility (ECLAC, 2012;
Garganta and others, 2017). Young mothers are then most likely to use family planning when the challenges
of parenthood dawn on them. Also, unlike countries such as Mexico, where adolescent births occur mostly
within marriage or a union (Quick, 2014), childbearing among adolescents in Argentina appears to have
become more socially tolerable, especially aer the Government ended the discrimination against children
born out of wedlock (Novick, 2001).
Policies to encourage childbearing and raise fertility: Hungary
Since the late 1940s, Hungary has continuously implemented policies to raise fertility, with short and
temporary changes towards less pronatalist approaches. Nonetheless, fertility in Hungary declined below
the replacement level for the rst time in 1960 and has continued to decline further to about 1.5 births per
women during 2015-2020. Unlike many other developed countries, Hungary experienced only a moderate
baby boom aer the Second World War. e total fertility rate was 2.6 births per woman in 1950, but quickly
declined below the replacement level in the 1960s, reaching a level of 1.8 births in 1962. e country’s
population size has been falling since 1980.
Policies intended to raise the fertility level and promote population growth were adopted by the Hungarian
Government both during the period of the centrally planned economy (1949-1989) and during the period
of the current market economy (1989 to present). ere were frequent changes in policies and programmes
associated with dierent political regimes during the 1990s and early 2000s (Spéder, 2015). e current
Government coalition, which has been in power since 2010, has steadily expanded policies to encourage
families to have more children.
Maternity and family allowances introduced in 1967 and 1973 may have been the cause of a rebound that
raised fertility levels for a short period even above the replacement level in the mid-1970s. However, past
medium-term trends towards lower fertility resumed quickly thereaer and stabilized around 1.8 births
until the early 1990s. e 1990s were marked by the collapse of the Soviet Union and the transition to
a new political system that also included economic reforms, including the adoption of a scal austerity
programme that led to a sharp economic downturn. e constraints and uncertainties associated with these
drastic political, social and economic transformations led many couples to delay the starting of a family and
childbearing in general. Total fertility dropped to a low level of 1.3 births per women in 1999 and stayed
around that level until 2011. e country’s total fertility rate has risen slightly to nearly 1.5 births per women
over the past ve years (gure 6).
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
21
Figure 6
Total fertility rates in Hungary, 1950-2019
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
3.2
Live births per woman
Responding to changing population dynamics, population and family policies in Hungary have evolved
over time. In the 1950s, the Government rst introduced policy measures restricting access to abortions
and contraception that were quickly relaxed in response to public objections to these measures. is led
to an increase in the number of abortions and a decline in the number of births until the early 1960s
(United Nations, 1989a). In 1967, the Government introduced the maternity allowance, a paid maternity
leave with job security for mothers to take care of a young child until the child’s third birthday. In 1973,
family allowances were introduced, whereby families and young couples received benets to improve their
housing conditions, such as low-rent public housing and interest-free housing loans. Later on, in 1985, the
Government adopted new population policies to address fertility decline and negative population growth.
e measures included a wage-adjusted parental leave, tax relief for large families and the expansion of the
family allowances to unemployed parents.
Following the end of socialism in Hungary, successive governments continued the family policies to support
families aimed at raising fertility, even though priorities and the extent of support evolved (Spéder, 2015).
e current Government, in power since 2010, has a strong demographic focus with an objective to raise
fertility to a level of 2.1 births per woman by 2030. e existing family welfare system has been modied and
expanded over the past decade and currently provides family allowances and tax credits as well as universal
maternity leave, childcare support and exible employment to help parents return to the labour market.
However, due to the complexity of the various programmes, many Hungarians are reportedly unfamiliar
with them (Albert, 2018). e current scope of public nancial support for families and children in Hungary
ranks second only aer France among OECD countries as a percentage of GDP (OECD, 2021).
Source: Hungary Central Statistical Oce (2021).

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
22
One characteristic of the Hungarian family policy is its support for families with three or more children. In
2016, a family “home creation” scheme was introduced to support couples who have or plan to have three
children, with an allowance equivalent to €32,250. Starting in 2018, families with three or more children and
who have a mortgage on their home can deduct their debt. e deduction is of one million Hungarian forint
(equivalent to €3,200) aer the birth of their third child, and a further 1 million forints aer the birth of each
subsequent child. On 1 January 2020, a new tax allowance was introduced for mothers raising four or more
children, applicable before any other tax allowance (Albert, 2018, 2020). In early 2020, the Government also
announced that Hungary would provide free in-vitro fertilization (IVF) treatment to couples at State-run
clinics.
It will take time to observe whether these latest family policies will have a lasting eect in raising fertility
towards the replacement level and reversing the trend of population decline. In the meantime, the total
fertility rate has increased to just under 1.5 births per woman, with the latest gure for 2020 was 1.56 births
(Hungary Central Statistical Oce, 2021).
Policies to support families and encourage childbearing: Australia
Australia has enjoyed a moderately low fertility for several decades compared to other developed countries.
Australia does not have an ocial policy concerning the fertility level, although the Government expressed
a desire to raise the fertility level in recent United Nations inquiries (United Nations, 2018). ere have been
various social security payments ranging from family tax benets and allowances for childcare aimed at
alleviating poverty, which are also benecial for families to raise children in Australia. ese measures have
been attributed to maintaining current levels of fertility (McDonald, 2015).
Australia experienced an extended baby boom from 1946 to 1964 with total fertility peaking at 3.6 births
per woman in 1961 (gure 7). Fertility declined shortly thereaer, reaching the below-replacement level
of 2.1 births per women in 1976. Fertility levels declined further and nally stabilized between 1.8 and 1.9
births since the late 1970s with a continued downward trend that was only interrupted briey in the period
between 2007 and 2009, when fertility increased to about 2 births per women. In 2019, the total fertility rate
reached a historic low of just below 1.7 (1.66) births per woman.
Australia has provided support to families with children since the early twentieth century. For example, a
maternity allowance of £5 (over two weeks wages for an unskilled worker) was introduced in 1912 (Daniels,
2009). Over the years, the Government has introduced various welfare payment schemes to help families
with children. Nonetheless, the type and strength of support vary depending on which major party is
in power (McDonald, 2015). e current family payment scheme, that consists of two components, was
instituted in the late 1990s: the Family Tax Benet Part A, an income-tested assistance for each dependent
child, and the Family Tax Benet Part B, a family-based payment to give extra help to single parents
and some couples with only one main income.
16
e Government started to provide an income-tested
childcare allowance in 1983. In the early 2000s, a childcare tax rebate was introduced for out-of-pocket
childcare costs, from which eligible families can claim 30 per cent tax rebate for up to 50 hours for each
child per week. Australia’s rst national paid parental leave scheme was introduced in 2011, and revised
in 2014, although many employers had already provided such a benet on a voluntary basis. In 2009, the
Australian Parliament passed the Fair Work Act 2009 which stipulated that a parent, or someone having
responsibility for the care of a child of school age or younger, can request exible working arrangements,
including the hours, patterns and locations of work, if she or he has worked with the same employer
forat least 12 months. ese family-friendly policies help women to participate in the labour force and to
16
More details about Australia’s family tax benets are available at www.servicesaustralia.gov.au/individuals/services/centrelink/family-tax-benet.
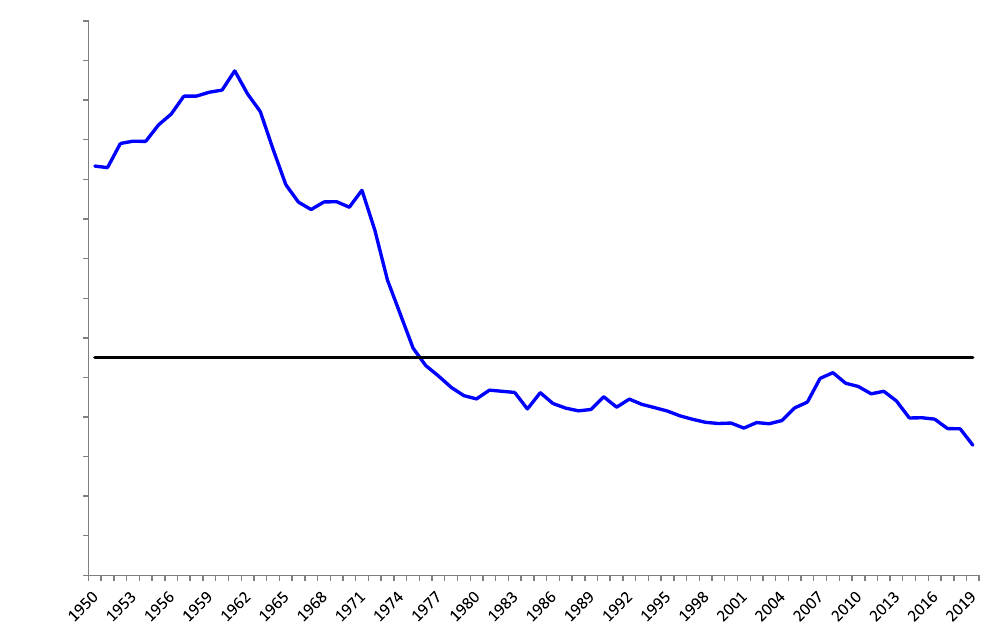
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
23
balance work and family life through exible work arrangements. For example, during 2019-20, 78 per cent
of women aged 30-39 years participated in the labour force and nearly 60 per cent of employed mothers
worked part-time (Australian Bureau Statistics, 2020).
Figure 7
Total fertility rates in Australia, 1950-2019
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
3.2
3.4
3.6
3.8
Live births per woman
For a decade (2004-2013), the Government directly paid a lump sum and non-means tested maternity
payment to all mothers for each newborn child and each young child adopted, in response to declining
fertility and population ageing. In 2001, total fertility had declined to 1.74 births per woman, the lowest
level since 1950. e Government released its rst intergenerational report in 2002 highlighting signicant
ageing-related challenges, such as potential labour supply shortages, reduced economic growth and domestic
revenue, increased medical costs and increased demand for old-age care, if no action would be taken. In this
context, in May 2004 the Government introduced a baby bonus for new mothers. e pronatalist motivation
was illustrated by the famous slogan coined by the Australian Treasurer at that time, Mr. Peter Costello,
who encouraged each couple to have three children: “one for mum, one for dad and one for the country”
(Costello, 2004). From 1 July 2004 onwards, all women with newborns or adopted children under the age
of two years, regardless of her marital status and household income, were to be paid AU$3,000, an amount
that increased to AU$4,000 in 2006 and to AU$5,000 in 2008. Because of its high cost, the policy generated
considerable controversy in the country and became a topic of debate in every election over the following
decade; it underwent a series of revisions that increasingly restricted the size of benets paid, until nally
the policy was revoked in 2013.
Source: Australian Bureau of Statistics (2021).
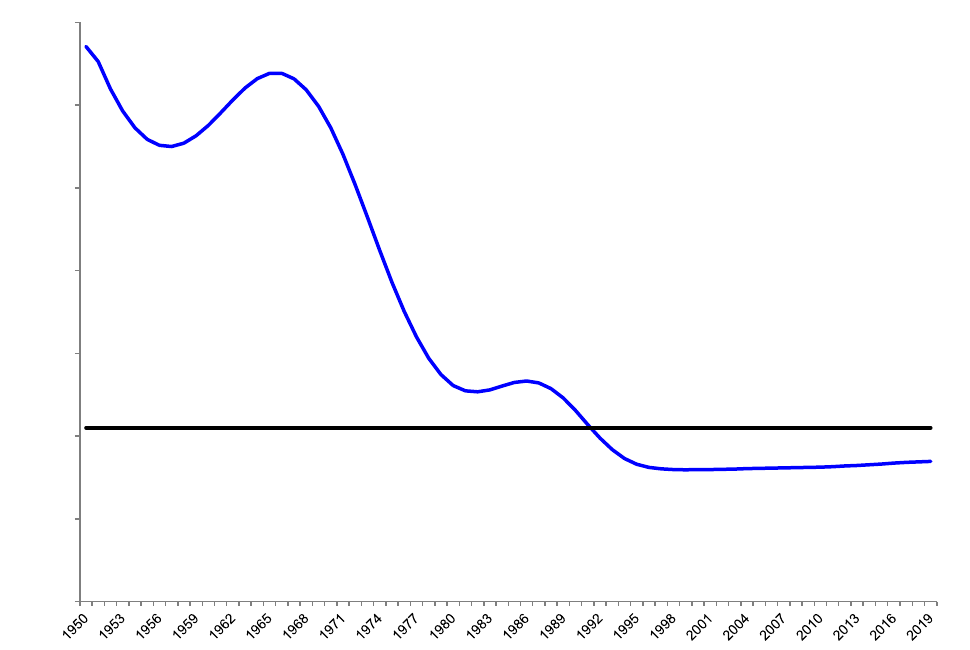
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
24
Policies to lower and then raise fertility: China
In China, the total fertility rate declined from 6.3 births per woman in 1965-1970, just before the start of
the nationwide family planning programme, to 1.7 births during 2015-2020 (gure 8). During the past
half century, China has developed, maintained and adjusted population policies with a family planning
programme focused on limiting the number of births per couple, with the intention to lower fertility. A strict
policy, allowing each couple to have only one child with few exceptions, termed the “one-child policy”, was
implemented between 1979 and 2015. In 2015, it was replaced by a policy allowing each couple to have two
children. Aer further revisions, the formal policy as of mid-2021 allows each couple to have up to three
children, with the explicit intention of raising the country’s fertility level and countering the situation of
sustained low fertility and rapid population ageing.
Figure 8
Total fertility rates in China, 1950-2019
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Live births per woman
Like most developing countries, China experienced rapid population growth in the 1950s and 1960s with its
total population increasing from 554 million in 1950 to 828 million in 1970 and its growth rate peaking at
2.7 per cent in 1968 (United Nations, 2019). Aer the implementation of the family planning programme,
the total fertility rate fell from 5.4 births per woman in 1971 to 2.8 births in 1979 (Coale, 1984). During
the following decade, total fertility rate uctuated well above the replacement level despite the strict “one
child” policy already referred to. In 1992, the total fertility rate declined below the replacement level and has
remained below this level since. Exactly how far below the replacement level did fertility decline aer the
Source: United Nations (2019).
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
25
early 1990s has been a topic of considerable debate. According to the latest census in 2020, the total fertility
rate had fallen to 1.3 births per woman in 2020, a level comparable to Italy, Japan, the Republic of Korea
and Spain. A continuation of the long-term trend of fertility decline is likely, possibly reinforced by the
COVID-19 pandemic (United Nations, 2021).
e national fertility policy during 1971-1979, termed the “later, longer and fewer” policy, had three
components: a) encouraging later marriage and childbearing, b) requiring longer birth spacing, and c)
allowing at most three children each couple can have (United Nations, 1989b). Despite a rapid fertility
decline during this period, the population kept increasing, to 1 billion people in 1980. In the late 1970s, the
Chinese Government started a “reform and open-up” policy making economic development a top priority
while considering rapid population growth a major impediment to economic advancement. As noted
above, in late 1979, the Government introduced a stricter policy, allowing each couple to have one child
only, with a few exceptions in urban areas and more exceptions in rural areas. e policy was in general
successful in cities but faced some resistance in rural areas. As a result, the Government relaxed the policy
in rural areas in 1984, allowing couples to have a second child if the rst one was a girl. is modied
policy was maintained until the mid-2010s. To accommodate the diversity in such a large country, the policy
was translated into regulations at the provincial level. It was estimated that the fertility level based on the
provincial regulations would be 1.6 births per woman (Gu and others, 2007). To legalize this policy at the
national level, a Population and Family Planning Law was enacted in 2001.
In response to the surprising results of the 1990 population census that revealed that China’s population had
increased to nearly 1.2 billion and its total fertility rate was still above the replacement level (2.4 births per
woman), the Chinese Government tightened the policy enforcement, requiring the heads of Government at
all levels to take personal responsibility for its strict implementation, and couples violating the policy to pay
a signicant “social compensation” fee (Greenhalgh and Winkler, 2002). ese practices were maintained
until the mid-2010s. Realizing the challenges arising from the growing labour shortage, rapid ageing and
the social consequences of the long-standing unbalanced sex ratio at birth (more males than females than
expected), the Chinese Government eased the policy in 2013, allowing couples to have two children if one
of the parents was from a single-child family, and later in 2015, replaced it with a universal policy allowing
each couple to have two children.
e policy relaxation brought a short-lived increase in the annual number of births in 2016 and 2017.
However, during the following three years, births continued to decline, which would result in zero or
negative population growth in the very near future. Following the release of the 2020 population census
results in May 2021, the Chinese Government decided to apply a three-child policy, aimed at raising the
fertility level to maintain population growth with a more balanced age structure. is occurred exactly 40
years aer introducing a fertility policy to lower fertility levels in an eort to curb rapid population growth.
It had long been argued that China’s low fertility was not the sole result of the one-child policy, and that rapid
socioeconomic development since the 1990s had played an important role in driving down fertility (Zhao
and Zhang, 2018). Realizing that many factors are at play, the Chinese Government also plans to take a range
of measures to support couples to have more children, including providing support for childcare through
widely available facilities, encouraging local governments to provide paid parental leave, and abolishing the
social compensation fee for those violating the policy. In August 2021, an amended Population and Family
Planning Law was passed to incorporate the new policy.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
26
Mothers and infants at Primary Health Centre, Madagascar, by UN Photo/Eskinder Debebe,
2006

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
27
The impact of the COVID-19 pandemic on fertility
Since early 2020, the COVID-19 pandemic has caused great economic disruptions, with major impacts
on people’s health and livelihoods. From a demographic perspective, COVID-19 has impacted all three
components of population change, namely fertility, mortality and migration. By the end of December
2021, more than 300 million people had been infected and more than 5 million people had died due to the
disease. e pandemic has hit countries across the world at dierent times and with a range of intensity and
duration. e eects on fertility appear to dier as a function of the severity and duration of the epidemic,
the country’s socioeconomic level and its policy responses.
17
While some countries have registered a decline
in births during the pandemic and may perhaps see a fertility rebound thereaer, other countries might
see a short-term increase in fertility from unintended pregnancies due to disruptions in access to family
planning services, which could pose challenges especially in sub-Saharan Africa and in some countries of
Latin America and the Caribbean.
How the COVID-19 pandemic aects fertility
Historically, the response of human fertility to external shocks such as famine, epidemics and economic
crises have followed a fairly common pattern: fertility declined in response to rising mortality, normally
with a nine-month lag, and rebounded one or two years aer the crisis (Lee, 1990; Livi Bacci, 2000). is
phenomenon was clearly observed in the 1918 inuenza pandemic and more recently in the context of 2015
Zika virus outbreak in Brazil (Mamelund 2004; Rangel, Nobles and Hamoudi, 2020).
Past experiences can help to understand the impact of the current pandemic on fertility. However, it is
important to recognize the dierences between the COVID-19 pandemic and previous pandemics and
epidemics in disease transmission, progression, morbidity and mortality proles as well as dierences in the
socioeconomic consequences of the related disease containment measures. While the inuenza and Zika
epidemics mainly aected younger people, in the early stages of the coronavirus disease 2019 pandemic,
COVID-19 morbidity, and especially mortality, has disproportionately aected older persons (Aassve and
others, 2020).
Existing research identies three major mechanisms through which the COVID-19 pandemic can aect
fertility. e rst mechanism is widespread fear and uncertainty about the future, particularly at the early
stage of the pandemic. Being confronted with a new and highly contagious virus-based illness for which
neither cure, treatment or vaccination were available, caused fear of infection, illness and death of individuals
and family members. In addition, concerns about an uncertain future resulting from strict and extended
lockdowns adopted to curb the spread of the disease triggered additional worries about the future in general.
e broad coverage of the socioeconomic as well as health related aspects of the pandemic in the mass
media and social media platforms may have contributed to the creation of a “pandemic of fear” (Mencarini,
2021; Mamelund, 2021) that could have led to postponement of childbearing at least temporarily, causing
a temporary dip in fertility levels, particularly in some of the countries that were aected in the early stages
of the pandemic.
e second possible factor that could continue to impact fertility is the increase in unemployment and rising
job insecurity. Since the start of the pandemic, unprecedented measures to control the spread of the virus
by governments across the world resulted in major economic and social disruptions. Global GDP fell by an
17
is chapter is based on the Expert Group Meeting on the Impact of the COVID-19 Pandemic on Fertility, organized virtually by the Population
Division in May 2021. e key ndings of the meeting, which brought together more than 100 experts from across the world, are provided here with
a view to providing Governments and other stakeholders with empirical information to assess and as needed, revise and adjust fertility and family
planning related policies and programmes in order to cope with the impact of the pandemic. Further information on the expert group meeting can
be found here.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
28
estimated 4.3 per cent in 2020, compared to a reduction of 1.7 per cent during the Great Recession in 2009
(United Nations, 2021). Hundreds of millions of people lost their jobs and income, and those who still have
jobs continue to face increasing job insecurity. Previous research shows that fertility decline was correlated
signicantly with a rise in unemployment at dierent reproductive ages during the Great Recession (Sobotka,
Skirbekk and Philipov, 2011; Matysiak, Sobotka and Vignoli, 2021). In the United States, the fertility decline
continued even aer the recession had ended (Seltzer, 2019).
e third possible mechanism is the increase in unintended pregnancies in less developed countries that have
experienced and continue to experience disruptions in the supply of and access to family planning services
and commodities. e 2014-2016 Ebola outbreak in Guinea, Liberia and Sierra Leone led to disruptions in
access to family planning services. Fertility data from Liberia point towards an early sign of an apparent “post-
Ebola baby boom” attributed to increased unintended pregnancies in January 2016 (McBain and others, 2016;
Sochas, Channon and Nam, 2017). Early in the pandemic, there were widespread concerns about a shortage
of and access to essential sexual and reproductive health-care services, including family planning. A more
recent study found that disruptions in family planning services were largely concentrated in April and May
2020. It was estimated that about 12 million women had experienced contraceptive interruptions, leading
to 1.4 million unintended pregnancies during 2020 across 115 low- and middle-income countries (UNFPA,
2021b). To secure access to sexual and reproductive health services many governments declared sexual
and reproductive health-care services to be essential services and service providers developed innovative
methods for service delivery, with broad support from international and non-governmental organizations.
Such joint eorts by the national entities and the international community are expected to help reduce the
risk of unintended pregnancies and births in parts of the less developed countries.
At this point in time, it is not known how the evolution of the pandemic, the increased availability of
vaccines and more recently, treatments, along with global eorts to rebuild global economies, will aect
people’s perceptions of the threats of the pandemic to their health and economic well-being, nor is it known
how all this will impact on couples’ decisions to start a family or expand an existing one. Learning to live
with the virus and building condence in a better post-COVID-19 world could trigger an uptick in births
when parents decide to catch up on postponed childbearing intentions. Intensied eorts to restore sexual
and reproductive health services, including access to family planning where the service supply chains were
severely disrupted, will hopefully limit the number of unintended pregnancies.
Early data from selected countries and regions
Early data from a number of low-fertility countries, mostly in Europe and Northern America, indicate a
fertility decline in 2020. For example, the Short-Term Fertility Data series available in the Human Fertility
Database,
18
showed that in many European countries the monthly number of births fell sharply between
October 2020 and March 2021, compared with the same period a year earlier (October 2019 to March 2020).
However, no fertility declines were noted in the Nordic countries. Data for March 2021 even point towards
unexpected upturns in the number of births in some countries. Overall, a continuation of the present
downward trajectory of fertility aer 2021 appears likely in most European countries (Sobotka, 2021). In
the United States of America, the total fertility rate declined from a previous low of 1.7 births per woman in
2019 to 1.6 births in 2020. It is expected that in the short term the United States of America will continue to
observe declines in both the number of births as well as the fertility level.
In line with the pre-pandemic declining fertility trends in Asia, China’s birth registration system reported
a signicant drop in fertility in late 2020, reaching an all-time low of 1.3 births per woman in 2020. ese
record low fertility levels were conrmed by the latest population census data (National Bureau of Statistics,
18
Human Fertility Database, available at www.humanfertility.org/cgi-bin/main.php.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
29
China, 2021). Continued fertility declines were also observed in Japan and the Republic of Korea. For these
three countries as well as for low- and middle-income countries in Eastern and South-Eastern Asia, available
data point towards a continuation of pre-pandemic fertility trajectories.
Australia and New Zealand had adopted strict zero-COVID-19 strategies
19
to contain the spread of the virus,
that included lockdowns, quarantines and border closures. Although both countries were not as heavily hit
by the pandemic as were Europe and Northern America, the pandemic appears to have had some eect on
the total fertility rate in both Australia and New Zealand, which fell from 1.66 to 1.58 births per woman and
from 1.72 to 1.66 birth per woman from 2019 to 2020, respectively (Australian Bureau of Statistics, 2021;
Statistics New Zealand, 2021).
In Latin America and the Caribbean, early evidence points to a decrease in fertility in some countries strongly
aected by the rst wave of the COVID-19 pandemic,
20
with preliminary data suggesting a postponement
of childbearing in Brazil and an accelerated drop in adolescent fertility in Chile. A signicant decline in the
number of births was also observed in Cuba and Peru (UNFPA, 2021c). However, in the longer term, the
region is expected to return to pre-pandemic fertility patterns and trends.
In countries with available data in sub-Saharan Africa, access to and use of family planning seem to have
been stable since the outbreak of the pandemic. In some instances, contraceptive use increased, and women
switched to more eective methods (implants and injectables) rather than to discontinue contraceptive use
altogether. However, early data for Northern Africa and Western Asia, Central and Southern Asia reported
disruptions to family planning services, with poorer women and women in remote rural areas being more
likely aected and therefore possibly exposed to a higher risk of unintended pregnancies. Early statistics
reported that Bangladesh experienced a signicant increase in the number of births in late 2020 and early
2021 (UNFPA, 2021c).
Caution is required in interpreting these early statistics. For low-income countries, timely and accurate
birth registration data are not available and high- and middle-income countries experienced delays in
timely registration of births. Also, it is important to take into consideration the lag of nine months between
conception and birth of a child, and that available fertility data reect births from conceptions during the
early stages of the pandemic. Continued monitoring of fertility data will be necessary to obtain a better
understanding of the impact of the pandemic on fertility levels and trends.
Post-pandemic fertility levels and trends
Judging from historical experiences, the current status of the pandemic and the available evidence to date (as
of May 2021), fertility uctuations during 2021 to 2023 are likely to be minor in general, and fertility levels
to likely return to pre-pandemic levels between 2023 and 2025. High vaccination rates in some countries
along with eorts to revitalize their economies, could lead some countries to focus on a post COVID-19
future, whereas in poorer countries, especially in some parts of Asia and sub-Saharan Africa, vaccination
drives could take years to complete, portending future waves of infection, the spread of new virus variants
and potentially a dierent or more prolonged impact on fertility.
19
Zero-COVID-19 strategies were ended in Australia on 31 August 2021 and in New Zealand on 5 October 2021.
20
Latin America was declared by the World Health Organization (WHO) as the epicenter of the COVID-19 pandemic in May 2020, accounting for
more than 40 per cent of the world’s COVID-19 death then, with the total infection rate exceeding 6.5 million cases and a loss of over 350,000 lives;
in: OECD (2020): Tackling coronavirus (COVID-19): Contributing to a global eort; COVID-19 in Latin America and the Caribbean: an overview
of government response to the crisis, 11 November 2020.

World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
30
People wait to receive a COVID-19 vaccine at Javits Center in New York City, by Spencer
Platt/Getty Images, 2021
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
31
Summary and policy considerations
Seventy years ago, with the adoption of the rst national population policy in India in 1952, the focus
of population and family policies in developing countries with rapidly growing populations, was to lower
fertility and curb population growth. According to the World Population Policies database, more than 20
years later, in 1976, 40 countries, accounting for almost two thirds of the world’s population at that time and
including almost all the largest developing countries, except for Nigeria, Ethiopia, Brazil and the Former
USSR, had explicit policies to reduce fertility levels.
Total fertility has fallen markedly over recent decades in many countries (United Nations, 2019), and it has
begun to fall even in countries where fertility levels remain high. It is dicult to determine the direct eects
of fertility and population policies on fertility levels within a country, since individual national policies are
generally embedded in a wider institutional, economic, social and cultural context. However, it seems likely
that direct measures, such as the provision of sexual and reproductive health care and broad access to family
planning, in combination with the indirect impact of broader developments, such as the advancement of
women in education and employment, the increased costs of raising a family and cultural shi towards more
egalitarian approaches by couples within households, have contributed to the global decline in fertility and
family size.
As of 2019, more than 60 per cent of governments globally (124 out of 197 countries or areas) had policies
attempting to inuence the current level of fertility with another 19 governments aiming to maintain its
current fertility level, albeit with a growing number adopting pronatalist measures (55 countries or areas out
of 143 countries or areas with such policies – see also table 1). Many governments have adopted implicit or
explicit pronatalist family policies, such as oering baby bonuses and parental leave and/or tax-incentives
as well as housing and income allowances related to the birth of a child. Subsidized fertility treatment, long-
term job guarantees for new mothers/parents and aordable childcare and aer-school care are some of the
additional incentives adopted to raise fertility.
While various approaches and initiatives to lower fertility have shown results globally (United Nations,
2019), reversing the long-term downward trends in total fertility that are the outcome of social, economic
and cultural transformations, has proven to be much more dicult (United Nations, 2015). While some
countries in Europe have been able to maintain their fertility levels or have even seen slight increases over a
relatively short period (for example, France, Germany, and Hungary), there is a lack of evidence that these
increases are stable and long term, and not merely a reaction by couples to take advantage of incentives
provided by advancing the birth of their next child without increasing their ultimate family size.
Even the COVID-19 pandemic, with direct and indirect implications for the health and socioeconomic
well-being of populations worldwide, appears not to have interrupted the global trend towards lower fertility
levels (United Nations, 2021).
In summary, governments should anticipate that fertility will continue to decline globally. is ongoing
trend is expected to lead, inevitably, to population ageing and also, potentially, to smaller populations
in many countries worldwide. Countries near the onset of this transition need to take advantage of the
demographic window of opportunity created by a shiing age distribution to bolster their economies, by
providing education and job opportunities to their growing working-age populations, whereas countries
with declining populations need to adjust to the new realities of an older and possibly smaller population.
Continued support by governments, the private sector, civil society and international development partners
to sustain sexual and reproductive health-care services, including access to family planning, is needed to
continue to enable men and women to freely decide on marriage and family formation, including the timing
and spacing of the children they wish to have.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
32
References
Aassve, Arnstein, and others (2020). e COVID-19 pandemic and human fertility. Science, vol. 369,
No. 6502, pp. 370-371, doi: 10.1126/science.abc9520.
Administración Nacional de la Seguridad Social (ANSES) (2021). Available at https://anses.gob.ar/. Accessed
on 25 October 2021.
Albert, F. (2018). Measures to ght demographic decline in Hungary. ESPN Flash Report 2018/19. European
Social Policy Network (ESPN): European Commission, Brussels.
_______ (2020). Hungary: Tax exemption for mothers of four or more children. ESPN Flash Report 2020/17.
European Social Policy Network (ESPN): European Commission, Brussels.
Aliyu, A. A. (2018). Family Planning Services in Africa: e Successes and Challenges. Available at www.
intechopen.com/chapters/58297.
Australian Bureau of Statistics (2020). Gender Indicators, Australia, December 2020. Available at www.abs.
gov.au/statistics/people/people-and-communities/gender-indicators-australia/latest-release#data-
download.
_______ (2021). Births, Australia 2021. cat. No. 33010DO001. Available at https://abs.gov.au/statistics/
people/population/births-australia/2020.
Badaracco, Nicolás, Leonardo Gasparini, and Mariana Marchionni (2016). Distributive implications of
fertility changes in Latin America. International Journal of Population Research, vol. 2016, pp. 1–11.
Bongaarts, John (2020). Trends in fertility and fertility preferences in sub-Saharan Africa: e roles of
education and family planning programs. Genus, vol. 76, No. 1, pp. 1–15.
Cepeda, Agustina (2014). In the days of the “Toad Test”: Justice and abortion in mid-twentieth-century
Argentina. Clio. Women, Gender, History, vol. 39, No. 1, pp. 239–254.
Coale, Ansley (1984). Rapid Population Change in China, 1952-1982. Washington, D. C.: National Academy
Press.
de Silva, Tiloka and Silvana Tenreyro (2017). Population control policies and fertility convergence. e
Journal of Economic Perspectives, vol. 31, No. 4, pp. 205-228.
Gogna, Mónica, and others (2008). Adolescent pregnancy in Argentina: Evidence-based recommendations
for public policies. Reproductive Health Matters, vol. 16, No. 31, pp. 192–201.
Gogna, Mónica and Edith Alejandra Pantelides (2009). e context of family p lanning in Argentina. In
Demographic Transformations and Inequalities in Latin America. Historical Trends and Recent Patterns,
Suzana Cavenaghi, ed.,rst edition., pp. 293–296. Rio de Janeiro, Brazil: UNFPA, CIPD/15 and
ALAP.
Costello, Peter (2004). Budget Speech 2004-05. Canberra: Australian Government. Available at http://budget.
gov.au/2004-05/speech/html/speech.htm.
Daniels, Dale (2009). Social Security payments for people caring for children, 1912-2008: A chronology. Social
Policy Section. Parliament Library. Parliament of Australia. Available at www.aph.gov.au /About_
Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/BN/0809/children#table1.
htm.
Dyer, Silke J. (2007). e value of children in African countries – insights from studies on infertility. Journal
of Psychosomatic Obstetrics and Gynecology, vol. 28, No. 2, pp. 69–77.
Economic Commission for Latin America and the Caribbean (ECLAC) (2012). Social Panorama of Latin
America 2011. Santiago, Chile: United Nations, ECLAC.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
33
Equipo Latinoamericano de Justicia Y Género (ELA) (2020). Country case-study: Sexual and reproductive
rights in Argentina. 2 June.
Garganta, Santiago, and others (2017). e eect of cash transfers on fertility: Evidence from Argentina.
Population Research and Policy Review, vol. 36, No. 1, pp. 1–24.
Frank, Odile, and Georey Mcnicoll (1987). An Interpretation of fertility and population policy in Kenya.
Population and Development Review, vol. 13, No. 2, pp. 209–243.
Greenhalgh, Susan, and Edwards Winkler (2001). Chinese State Birth Planning in the 1990s and Beyond.
Resource Information Center, Immigration and Naturalization Service (INS), US Department of
Justice, Perspective Series, September.
Gu, Baochang, and others (2007). China’s local and national fertility policies at the end of the twentieth
century. Population and Development Review, vol. 33, No. 1, pp. 129-147.
Hungary Central Statistical Oce (2021). Summary Tables: 22.1.1.6. Live births, total fertility rate (1900-
2020). Available at www.ksh.hu/stadat_les/nep/en/nep0006.html. Accessed on 29 September 2021.
Kane, Sumit, and other (2019). You have a child who will call you “mama”: Understanding adolescent
pregnancy in South Sudan. Global Health Action, vol. 12, No. 1, pp. 1553282.
Lee, Ronald (1990). e demographic response to economic crisis in historical and contemporary
populations. Population Bulletin of the United Nations, No. 29. ST/ESA/SER.N/29.
Livi Bacci, Massimo (2020). Mortality crises in a historical perspective: e European experience. In
e Mortality Crisis in Transitional Economies, G.A. Cornia and R. Paniccia, eds., pp. 38-58. Oxford
University Press.
López, Elsa (2006). La fecundidad adolescente en la Argentina: desigualdades y desafíos. Encrucijadas,
vol. 39, pp. 24–31.
Malnis, Soledad (2018). Posiciones docentes frente a la ESI: algunos desafíos para la capacitación continua.
Revista de Ciencias Sociales, vol. 4, No. 7, pp. 1–26.
Mamelund, Svenn-Erik (2004). Can the Spanish inuenza pandemic of 1918 explain the baby boom of 1920
in neutral Norway? Population, vol. 59, No. 2, pp. 229-260.
_______ (2021). Lessons from the 1918 inuenza pandemic. Presentation at the United Nations Expert
Group Meeting on the Impact of the COVID-19 Pandemic on Fertility, New York, 10 and 11 May
2021.
Matysiak, Anna, Sobotka Tomáš and Daniele Vignoli (2021). e great recession and fertility in Europe: A
sub-national analysis. European Journal of Population, vol. 37, No. 1, pp. 29-64. doi: 10.1007/s10680-
020-09556-y.
May, John (2012). World Population Policies: eir origin, evolution and impact. Springer.
_______ (2017). e politics of family planning policies and programs in sub-Saharan Africa. Population
and Development Review, vol. 43, S1, pp.308–329. doi:10.1111/j.1728-4457.2016.00165.x.
McDonald, Peter (2015). e Evolution of Population and Family Policy in Australia. In Low and Lower
Fertility: Variations across Developed Countries, Ronald R. Rindfuss and Minja Kim Choe, eds.
Springer.
Mencarini, Letizia (2021). COVID-19 and human fertility: A global perspective. Presentation at the United
Nations Expert Group Meeting on the Impact of the COVID-19 Pandemic on Fertility, New York,
10 and 11 May 2021.
Ministerio de Justicia y Derechos Humanos Ley 26.150: Nacional de Educación Sexual Integral. (2006).
Buenos Aires: El Senado y Cámara de Diputados de la Nación Argentina.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
34
National Bureau of Statistics (2021). Main Data of the Seventh National Population Census. News Release.
Available at www.stats.gov.cn/english/PressRelease/202105/t20210510_1817185.html. Accessed on
5 November 2021.
National Bureau of Statistics (2012). Sessional Paper Number 3 of 2012 on Population Policy for National
Development. Nairobi, Kenya: Ministry of Finance and Planning.
Novick, Susana (2001). Argentina’s Recent Population Policies and Political Changes. At 24th International
Population Conference, Bahia, Brazil, 18-24 August 2001, pp. 1–20. Bahia, Brazil: IUSSP.
Ombelet, Willem, and others (2008). Infertility and the provision of infertility medical services in developing
countries. e National Center for Biotechnology Information, vol. 14, No. 6, pp. 605–621.
Organization for Economic and Co-operation and Development (OECD) (2020). Tackling coronavirus
(COVID-19): Contributing to the global eort. Available at: www.oecd.org/dac/development-assistance-
committee/daccovid19statement.htm.
_______ (2021). OECD Family Database: PF1.1: Public spending on family benets. Available at www.oecd.
org/els/family/database.htm. Accessed on 29 September 2021.
Petracci, Mónica, Silvina Ramos, and Dalia Szulik (2005). A strategic assessment of the Reproductive
Health and Responsible Parenthood Programme of Buenos Aires, Argentina. Reproductive Health
Matters, vol. 13, No. 25, pp. 60–71.
Quick, Erica (2014). Adolescent pregnancy in Mexico. In International Handbook of Adolescent Pregnancy,
Medical, Psychosocial, and Public Health Responses, A.L. Cherryand M.E. Dillon, eds. New York, USA:
Springer.
Ramacciotti, Karina Inés (2003). El Museo Social Argentino y el Primer Congreso de Población de 1940.
Sociohistórica, pp. 231–236.
Rangel, Marcos, Jenna Nobles and Amar Hamoudi (2020). Brazil’s missing infants: Zika risk changes
reproductive behavior. Demography, vol. 57, pp. 1647–1680. doi:10.1007/s13524-020-00900-9.
Reina, María Fabiana and Camil Castelo-Branco (2014). In International handbook of adolescent pregnancy,
Medical, psychosocial, and public health responses, First edition, L.A. Cherry and M.E. Dillon, eds.
Boston, MA, United States: Springer.
_______ (2018). Teenage pregnancy: A Latin-American concern. Obstetrics and Gynecology Research,
vol. 1, No. 4, pp. 85–93.
Republic of Kenya (1997). Sessional Paper Number 1 of 1997 on National Population Policy for Sustainable
Development. Nairobi, Kenya: Republic of Kenya.
_______ (2010). Constitution of Kenya, 2010. Government of Kenya: e National Council for Law Reporting.
Available at http://kenyalaw.org:8181/exist/kenyalex/actview.xql?actid=Const2010. Accessed on 22
September 2021.
Robinson, Warren C., and John A. Ross (2007). Family Planning: e Quiet Revolution. In e Global Family
Planning Revolution: ree Decades of Population Policies and Programs, W.C. Robinson and J.A. Ross,
eds. Washington, D.C.: World Bank Publications.
Seltzer, Nathan (2019). Beyond the Great recession: labor market polarization and ongoing fertility decline
in the United States. Demography, vol. 56, pp. 1463‐1493. doi: 10.1007/s13524‐019‐00790‐6.
Sobotka, Tomáš, Vegard Skirbekk and Dimiter Philipov (2011). Economic recession and fertility in the
developed world. Population and Development Review, vol. 37, No. 2, pp. 67-306. doi: 10.1111/j.1728-
4457.2011.00411.x.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
35
Sochas, Laura, Andrew Amos Channon and Sara Nam (2017). Counting indirect crisis-related deaths in the
context of a low-resilience health system: e case of maternal and neonatal health during the Ebola
epidemic in Sierra Leone. Health Policy and Planning, vol. 32 (suppl. 3), pp. 32-39. doi: 10.1093/heapol/
czx108.
Spéder, Zsolt (2015). Fertility decline and the persistence of low fertility in a changing policy environment -
A Hungarian case study. In Low Fertility, Institutions, and their Policies. R.R. Rindfuss and M.K. Choe,
eds. Springer International Publishing.
Statistics New Zealand (2021). Births and deaths: Year ended December 2020. Available at https://stats.govt.
nz/information-releases/births-and-deaths-year-ended-december-2020-including-abridged-period-
life-table.
United Nations Children Fund (UNICEF) (2001). Early Marriage, Child Spouses. Innocenti Digest No. 7,
pp. 1–30.
United Nations Population Fund (UNFPA) (2021b). Impact of COVID-19 on Family Planning: What we
know one year into the pandemic. Available at www.unfpa.org/resources/impact-covid-19-family-
planning-what-we-know-one-year-pandemic.
_______ (2021c). How will COVID-19 impact fertility? Technical brief. Available at www.unfpa.org/
publications/how-will-covid-19-impact-fertility.
United Nations, Department of Economic and Social Aairs, Population Division (1989a). Case Studies in
Population Policy: Hungary. Population Policy Paper No. 19. ST/ESA/SER.R/87.
_______ (1989b). Case Studies in Population Policy: China. Population Policy Paper No. 20.
ST/ESA/SER.R/88.
_______ (2018). World Population Policies 2015. ST/ESA/SER.A/374. Available at www.un.org/
development/desa/pd/sites/www.un.org.developmentdesa.pd/files/files/documents/2020/Jan/
un_2015_worldpopulationpolicies.pdf.
_______ (2019). World Population Prospects 2019. Available at https://population.un.org/wpp/.
_______ (2021). Report of the United Nations expert group meeting on the impact of the COVID-19 pandemic
on fertility. ESA/P/WP/264. Available at www.un.org/development/desa/pd/event/egm-impact-covid-
19-fertility.
Zhao, Zhongwei, and Guangyu Zhang (2018). Socioeconomic factors have been the major driving force of
China’s fertility changes since the mid-1990s. Demography, vol. 55, No. 2, pp. 733-742.
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
36
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
SUB-SAHARAN AFRICA
Eastern Africa
Burundi 11531 5.5 55.6 Lower Yes Yes Yes Yes Yes
Comoros 851 4.2 65.4 Lower Yes Yes Yes
Djibouti 974 2.8 18.8 Lower Yes Yes Yes
Eritrea 3497 4.1 52.6 Lower Yes Yes Yes
Ethiopia 112079 4.3 66.7 Lower Yes Yes Yes
Kenya 52574 3.5 75.1 Lower Yes Yes Yes
Madagascar 26969 4.1 109.6 Lower Yes Yes Yes
Malawi 18629 4.3 132.7 Lower Yes Yes Yes Yes Yes
Mauritius 1270 1.4 25.7 Raise Yes Yes Yes Yes Yes
Mozambique 30366 4.9 148.6 Lower Yes Yes No Yes Yes
Rwanda 12627 4.1 39.1 Lower Yes Yes Yes
Seychelles 98 2.5 62.1 No policy Yes Yes
Somalia 15443 6.1 100.1 No policy Yes Yes No
South Sudan 11062 4.7 62.0 Raise Yes Yes No Yes Yes
Uganda 44270 5.0 118.8 Lower Yes Yes Yes
United Republic of Tanzania 58005 4.9 118.4 Maintain Yes Yes Yes Yes Yes
Zambia 17861 4.7 120.1 Lower Yes Yes Yes Yes Yes
Zimbabwe 14645 3.6 86.1 Lower Yes Yes Yes
Middle Africa
Angola 31825 5.6 150.5 Lower Yes Yes No Yes Yes
Cameroon 25876 4.6 105.8 Lower Yes Yes Yes Yes Yes
Central African Republic 4745 4.8 129.1 No policy Yes Yes Yes Yes Yes
Chad 15947 5.8 161.1 Lower Yes Yes Yes Yes
Congo 5381 4.5 112.2 No policy Yes Yes Yes Yes Yes Yes
Democratic Republic of the
Congo
86791 6.0 124.2 Lower Yes No Yes Yes Yes
Equatorial Guinea 1356 4.6 155.6 Lower Yes Yes Yes
Gabon 2173 4.0 96.2 Raise Yes Yes Yes Yes Yes Yes
Sao Tome and Principe 215 4.4 94.6 No policy Yes Yes No Yes Yes
Southern Africa
Botswana 2304 2.9 46.1 Maintain Yes Yes No Yes
Eswatini 1148 3.0 76.7 Lower Yes Yes Yes
Lesotho 2125 3.2 92.7 Lower Yes Yes Yes Yes
Annex table
Key indicators of Member and non-member States of United
Nations, globally through 2019
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
37
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
Namibia 2495 3.4 63.6 No policy Yes Yes Yes Yes Yes
South Africa 58558 2.4 67.9 No policy Yes Yes Yes Yes Yes
Western Africa
Benin 11801 4.9 86.1 Lower Yes Yes Yes Yes Yes Yes
Burkina Faso 20321 5.2 104.3 Lower Yes Yes Yes Yes Yes
Cabo Verde 550 2.3 73.8 Lower Yes Yes Yes
Côte d’Ivoire 25717 4.7 117.6 Lower Yes Yes Yes Yes Yes
Gambia 2348 5.3 78.2 Lower Yes Yes Yes No Yes Yes
Ghana 30418 3.9 66.6 Lower Yes Yes
Guinea 12771 4.7 135.3 Lower Yes Yes Yes Yes Yes Yes
Guinea-Bissau 1921 4.5 104.8 Lower Yes No Yes Yes Yes
Liberia 4937 4.4 136.0 No policy Yes No Yes Yes Yes
Mali 19658 5.9 169.1 Lower Yes Yes Yes Yes
Mauritania 4526 4.6 71.0 Lower Yes Yes Yes
Niger 23311 7.0 186.5 Lower Yes Yes Yes Yes Yes
Nigeria 200964 5.4 107.3 Lower Yes Yes No Yes Yes
Senegal 16296 4.7 72.7 Lower Yes Yes Yes Yes Yes
Sierra Leone 7813 4.3 112.8 Lower Yes Yes No Yes
Togo 8082 4.4 89.1 Lower Yes Yes Yes Yes Yes
NORTHERN AFRICA AND
WESTERN ASIA
Northern Africa
Algeria 43053 3.1 10.1 Lower Yes Yes Yes
Egypt 100388 3.3 53.8 Lower Yes Yes Yes Yes Yes Yes
Libya 6777 2.3 5.8 No policy Yes No No Yes
Morocco 36472 2.4 31.0 Maintain Yes Yes Yes Yes
Sudan 42813 4.4 64.0 No policy Yes Yes No .. Yes
Tunisia 11695 2.2 7.8 Maintain Yes Yes ..
Western Asia
Armenia 2958 1.8 21.5 Raise Yes Yes Yes Yes Yes
Azerbaijan 10048 2.1 55.8 Maintain Yes Yes Yes Yes
Bahrain 1641 2.0 13.4 Lower Yes Yes Yes
Cyprus 1199 1.3 4.6 Raise Yes Yes Yes
Georgia 3997 2.1 46.4 Raise Yes Yes No No Yes Yes
Iraq 39310 3.7 71.7 No policy Yes Yes No No Yes
Israel 8519 3.0 9.6 Raise Yes Yes Yes Yes
Jordan 10102 2.8 25.9 Lower Yes Yes
Kuwait 4207 2.1 8.2 Raise Yes
Lebanon 6856 2.1 14.5 No policy Yes Yes Yes
Oman 4975 2.9 13.1 Maintain Yes Yes Yes Yes
Qatar 2832 1.9 9.9 Raise Yes Yes
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
38
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
Saudi Arabia 34269 2.3 7.3 Raise Yes Yes Yes
State of Palestine 4981 3.7 52.8 No policy Yes Yes Yes Yes
Syrian Arab Republic 17070 2.8 38.6 Lower Yes Yes Yes Yes Yes Yes
Turkey 83430 2.1 26.6 Raise Yes Yes .. .. Yes
United Arab Emirates 9771 1.4 6.5 Raise Yes
Yemen 29162 3.8 60.4 Lower Yes Yes .. Yes
CENTRAL AND SOUTHERN
ASIA
Central Asia
Kazakhstan 18551 2.8 29.8 Raise Yes Yes No No
Kyrgyzstan 6416 3.0 32.8 Raise Yes Yes Yes No Yes
Tajikistan 9321 3.6 57.1 Lower Yes Yes Yes
Turkmenistan 5942 2.8 24.4 Raise Yes Yes Yes Yes
Uzbekistan 32982 2.4 23.8 No policy Yes Yes Yes No Yes Yes
Southern Asia
Afghanistan 38042 4.6 69.0 Lower Yes Yes Yes Yes Yes Yes
Bangladesh 163046 2.1 83.0 Lower Yes Yes No Yes Yes
Bhutan 763 2.0 20.2 Lower Yes Yes Yes
India 1366418 2.2 13.2 Lower Yes Yes Yes Yes Yes Yes
Iran (Islamic Republic of) 82914 2.2 40.6 Raise Yes Yes No Yes
Maldives 531 1.9 7.8 No policy Yes Yes No Yes
Nepal 28609 1.9 65.1 Lower Yes Yes No Yes Yes
Pakistan 216565 3.6 38.8 Lower Yes Yes Yes Yes Yes
Sri Lanka 21324 2.2 20.9 No policy Yes Yes No Yes Yes
EASTERN AND SOUTH-
EASTERN ASIA
Eastern Asia
China 1433784 1.7 7.6 Raise Yes Yes Yes Yes
Dem. People’s Republic of
Korea
25666 1.9 0.3 Raise Yes Yes Yes Yes Yes
Japan 126860 1.4 3.8 Raise Yes Yes No No Yes
Mongolia 3225 2.9 31.0 Raise Yes Yes Yes
Republic of Korea 51225 1.1 1.4 Raise Yes Yes
South-Eastern Asia
Brunei Darussalam 433 1.8 10.3 No policy Yes
Cambodia 16487 2.5 50.2 No policy Yes Yes No Yes Yes
Indonesia 270626 2.3 47.4 Lower Yes Yes Yes
Lao People’s Democratic
Republic
7169 2.7 65.4 No policy Yes Yes Yes Yes Yes
Malaysia 31950 2.0 13.4 No policy Yes Yes No Yes Yes
Myanmar 54045 2.2 28.5 No policy Yes Yes Yes No Yes Yes
Philippines 108117 2.6 54.2 Lower Yes Yes Yes Yes Yes Yes
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
39
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
Singapore 5804 1.2 3.5 Raise Yes Yes Yes
Thailand 69626 1.5 44.9 Raise Yes Yes Yes
Timor-Leste 1293 4.1 33.8 Lower Yes Yes Yes Yes
Viet Nam 96462 2.1 30.9 Maintain Yes Yes Yes Yes Yes
LATIN AMERICA AND THE
CARIBBEAN
Caribbean
Antigua and Barbuda 97 2.0 42.8 No policy Yes Yes Yes Yes Yes
Bahamas 389 1.8 30.0 No policy Yes Yes Yes
Barbados 287 1.6 33.6 No policy Yes Yes Yes Yes
Cuba 11333 1.6 51.6 Raise Yes Yes Yes
Dominica 72 No policy Yes Yes Yes
Dominican Republic 10739 2.4 94.3 Lower Yes Yes Yes
Grenada 112 2.1 29.2 Maintain Yes Yes Yes Yes
Haiti 11263 3.0 51.7 Lower Yes Yes Yes Yes Yes
Jamaica 2948 2.0 52.8 Lower Yes Yes
Saint Kitts and Nevis 53 No policy Yes Yes Yes
Saint Lucia 183 1.4 40.5 No policy Yes Yes Yes Yes Yes Yes
Saint Vincent and the
Grenadines
111 1.9 49.0 No policy Yes Yes Yes Yes Yes
Trinidad and Tobago 1395 1.7 30.1 Maintain Yes Yes Yes Yes Yes
Central America
Belize 390 2.3 68.5 No policy Yes Yes Yes Yes Yes
Costa Rica 5048 1.8 53.5 No policy Yes Yes .. .. Yes Yes
El Salvador 6454 2.1 69.5 Lower Yes Yes Yes No Yes Yes
Guatemala 17581 2.9 70.9 No policy Yes Yes Yes No Yes Yes
Honduras 9746 2.5 72.9 No policy Yes Yes No Yes Yes Yes
Mexico 127576 2.1 60.4 Lower Yes Yes Yes No Yes Yes
Nicaragua 6546 2.4 85.0 Lower Yes Yes Yes
Panama 4246 2.5 81.8 No policy Yes Yes
South America
Argentina 44781 2.3 62.8 Maintain Yes Yes Yes Yes
Bolivia (Plurinational State of) 11513 2.8 64.9 Maintain Yes Yes Yes
Brazil 211050 1.7 59.1 No policy Yes Yes Yes Yes
Chile 18952 1.7 41.1 Raise Yes Yes Yes Yes
Colombia 50339 1.8 66.7 Maintain Yes Yes Yes Yes Yes Yes
Ecuador 17374 2.4 79.3 Lower Yes Yes Yes Yes
Guyana 783 2.5 74.4 Raise Yes Yes Yes Yes
Paraguay 7045 2.4 70.5 Maintain Yes Yes Yes
Peru 32510 2.3 56.9 Lower Yes Yes No Yes Yes
Suriname 581 2.4 61.7 No policy Yes Yes Yes No Yes
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
40
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
Uruguay 3462 2.0 58.7 No policy Yes Yes Yes Yes Yes Yes
Venezuela (Bolivarian
Republic of)
28516 2.3 85.3 No policy Yes Yes Yes
AUSTRALIA/NEW ZEALAND
Australia 25203 1.8 11.7 No policy Yes Yes No Yes Yes
New Zealand 4783 1.9 19.3 No policy Yes Yes No Yes Yes Yes
OCEANIA (EXCLUDING
AUSTRALIA AND NEW
ZEALAND)
Melanesia
Fiji 890 2.8 49.4 Lower Yes Yes
Papua New Guinea 8776 3.6 52.7 Lower Yes Yes Yes
Solomon Islands 670 4.4 78.0 Lower Yes Yes Yes
Vanuatu 300 3.8 49.4 Lower Yes Yes Yes
Micronesia
Kiribati 118 3.6 16.2 Lower Yes Yes
Marshall Islands 59 Lower
Micronesia (Fed. States of) 114 3.1 13.9 Lower Yes Yes
Nauru 11 Maintain Yes Yes
Palau 18 No policy Yes Yes Yes
Polynesia
Cook Islands 18 Raise Yes Yes
Niue 2 Raise Yes Yes Yes
Samoa 197 3.9 23.9 Lower Yes Yes
Tonga 104 3.6 14.7 Maintain Yes Yes
Tuvalu 12 Lower Yes Yes Yes
EUROPE AND NORTHERN
AMERICA
EUROPE
Eastern Europe
Belarus 9452 1.7 14.5 Raise Yes Yes Yes No Yes
Bulgaria 7000 1.6 39.9 Raise Yes Yes Yes Yes
Czechia 10689 1.6 12.0 No policy Yes Yes No No Yes
Hungary 9685 1.5 24.0 Raise Yes Yes Yes
Poland 37888 1.4 10.5 Raise Yes Yes Yes
Republic of Moldova 4043 1.3 22.4 Raise Yes Yes Yes No Yes
Romania 19365 1.6 36.2 Raise Yes Yes .. .. Yes Yes
Russian Federation 145872 1.8 20.7 Raise Yes Yes No No
Slovakia 5457 1.5 25.7 Raise Yes Yes Yes
Ukraine 43994 1.4 23.7 Raise Yes Yes Yes No Yes
Northern Europe
Denmark 5772 1.8 4.1 No policy Yes Yes Yes No
World Population Policies 2021: Policies related to fertility
United Nations Department of Economic and Social Aairs, Population Division
41
Region, country or area
Population
(thousand)
Total
fertility
rate (live
births per
woman)
Adolescent
fertility
rate (live
births per
1,000 girls
aged 15-19
years)
Policy
concerning
current
fertility
level
Whether
providing
maternity
leave
Whether
providing
public
subsidized
childcare
Whether
providing
direct
support
for family
planning
Whether
providing
indirect
support
for family
planning
Whether
expanding
girls’
secondary
school
enrolment/
retention
Whether
providing
school-
based
sexuality
education
Reference period 2019 2015-20 2015-20 2015-19 2015-19 2015-19 2019 2019 2015-19 2015-19
Estonia 1326 1.6 7.7 Raise Yes Yes Yes
Finland 5532 1.5 5.8 Raise Yes Yes No No
Iceland 339 1.8 6.3 Maintain Yes Yes
Ireland 4882 1.8 7.5 No policy Yes Yes Yes
Latvia 1907 1.7 16.2 Raise Yes Yes No No Yes
Lithuania 2760 1.7 10.9 Raise Yes Yes Yes No Yes
Norway 5379 1.7 5.1 No policy Yes Yes Yes
Sweden 10036 1.9 5.1 No policy Yes Yes Yes Yes Yes
United Kingdom 67530 1.8 13.4 No policy Yes Yes Yes Yes
Southern Europe
Albania 2881 1.6 19.6 Raise Yes Yes Yes Yes Yes Yes
Andorra 77 Maintain Yes
Bosnia and Herzegovina 3301 1.3 9.6 No policy Yes Yes Yes Yes
Croatia 4130 1.4 8.7 Raise Yes Yes
Greece 10473 1.3 7.2 Raise Yes Yes .. ..
Holy See 1 Raise Yes
Italy 60550 1.3 5.2 Raise Yes Yes
Malta 440 1.5 12.9 Raise Yes Yes No No Yes
Montenegro 628 1.8 9.3 Lower Yes Yes No Yes Yes Yes
North Macedonia 2083 1.5 15.7 Raise Yes Yes
Portugal 10226 1.3 8.4 Raise Yes Yes Yes Yes
San Marino 34 No policy Yes Yes
Serbia 8772 1.5 14.7 Raise Yes Yes No Yes Yes Yes
Slovenia 2079 1.6 3.8 No policy Yes Yes Yes No Yes
Spain 46737 1.3 7.7 Raise Yes Yes Yes
Western Europe
Austria 8955 1.5 7.3 Raise Yes Yes Yes
Belgium 11539 1.7 4.7 Maintain Yes Yes No Yes Yes Yes
France 65130 1.9 4.7 Raise Yes Yes Yes
Germany 83517 1.6 8.1 No policy Yes Yes No Yes Yes
Liechtenstein 38 Raise Yes Yes Yes
Luxembourg 616 1.5 4.7 Raise Yes Yes Yes
Monaco 39 Maintain Yes Yes
Netherlands 17097 1.7 3.8 No policy Yes Yes No No Yes
Switzerland 8591 1.5 2.8 No policy Yes Yes No Yes
NORTHERN AMERICA
Canada 37411 1.5 8.4 No policy Yes Yes Yes
United States of America 329065 1.8 19.9 No policy Yes Yes
The World Population Policies 2021: Policies related to fertility, provides a brief overview of global fertility levels
and trends since the early 1960s and explores government’s views and policies related to fertility. The analysis of
views and policies draws on data gathered through 2019 and available in the World Population Policies Database,
reecting the situation before the outbreak of the coronavirus disease 2019 (COVID-19) pandemic. The report
then presents ve case studies of countries from dierent regions and with a range of fertility levels, exploring in
more detail the origin and evolution of national fertility policies. The case studies are followed by an assessment
of known or potential direct and indirect impacts of the COVID-19 pandemic on fertility patterns and trends. The
report concludes with an exploration of policy options that governments may wish to consider in the current
context.
ISBN 9789211483635
