© MDart10/Shutterstock.com
Average Annual Growth Rates of Spending, Utilization, and Prices for Hospitals’
and Physicians’ Services, 2013 to 2018
Percent
3.2
1.8
0.4
0.5
2.7
1.3
Spending per Person Utilization per Person Prices Paid to Providers
Inflation as
Measured by the
Gross Domestic
Product Price
Index (1.6)
Medicare Fee
for Service
Commercial
Insurers
JANUARY | 2022
The Prices That Commercial
Health Insurers and Medicare
Pay for Hospitals’ and
Physicians’ Services

At a Glance
Just over half of the total U.S. population receives health insurance through commercial plans that
are oered by employers or purchased by individuals. In recent years, commercial health insurers’
per-person spending on hospitals’ and physicians’ services has grown more quickly than analogous
spending by the Medicare fee-for-service (FFS) program, according to analysis by the Congressional
Budget Oce. e main reason for the growth of per-person spending by commercial insurers—and
for the dierence from the growth of per-person spending by Medicare FFS—has been rapid increases
in the prices that commercial insurers pay for hospitals’ and physicians’ services.
Prices paid by commercial insurers and Medicare FFS dier, and rise at dierent rates over time, in part
because of dierences in how the two sets of prices are determined. e prices that commercial insurers
pay for services from in-network health care providers result from negotiations between the insurers and
providers. Commercial insurers may try to obtain lower prices by excluding providers from their net-
works, but in many cases, their ability to do that is limited. e prices that Medicare FFS pays providers
are set administratively through laws and regulations, and providers can either take them or leave them.
CBO’s analysis and a review of the research literature found that commercial insurers pay much
higher prices for hospitals’ and physicians’ services than Medicare FFS does. In addition, the prices
that commercial insurers pay hospitals are much higher than hospitals’ costs. Paying higher prices
to providers can have several eects. First, it can increase insurers’ spending on claims, which may
lead to higher premiums, greater cost-sharing requirements for patients, reductions in the scope of
benets, or other adjustments to plans. Second, it can increase the federal government’s subsidies for
health care (that is, the government’s spending on health care plus forgone revenues from federal tax
preferences for health benets). And third, it can slow the growth of wages.
Compared with the prices paid by Medicare FFS, the prices paid by commercial insurers also vary
much more among and within geographic areas. Large variation in prices for similar services can be
evidence that markets are not operating eciently.
CBO examined potential explanations for why the prices paid by commercial insurers are higher
and more variable than those paid by Medicare FFS. CBO’s analysis and literature review suggest the
following conclusions:
•
Greater market power among providers consistently leads to prices for commercial insurers that
are higher than Medicare FFS’s prices and that vary more widely, both among and within areas.
Hospitals and physicians’ groups may have market power because they have a dominant share of
the market in an area or because an insurer sees them as essential to its network of providers.
•
Some of the variation in the prices that commercial insurers pay for hospitals’ and physicians’
services is explained by dierences in the prices of inputs needed to deliver those services.
•
Higher hospital quality is associated with higher prices paid by commercial insurers, although whether
there is a causal link between quality and prices, and the direction of any such link, is not clear.
•
e share of providers’ patients who are covered by Medicare and Medicaid is not related to higher
prices paid by commercial insurers. at nding suggests that providers do not raise the prices
they negotiate with commercial insurers to oset lower prices paid by government programs (a
concept known as cost shifting).
www.cbo.gov/publication/57422

Contents
Chapter 1: Levels of and Trends in Spending and Prices 1
Factors Driving the Growth of Per-Person HealthCareSpending 1
How Medicare’s Prices Are Determined 2
How Commercial Insurers’ Prices Are Determined 3
Sources of Upward and Downward Pressure on Prices 4
Average Prices for Hospitals’ Services 5
Average Prices for Physicians’ Services 6
How Payments to Hospitals Compare With Hospitals’ Costs 7
Chapter 2: The Implications of Price Increases 9
How Price Increases Aect People With Employment-Based Insurance 9
How Price Increases Aect Federal Subsidies for Commercial Health Insurance 10
Chapter 3: Variation in Prices Among and Within Geographic Areas 13
Prices for Hospitals’ Services: Variation Among States 13
Prices for Physicians’ Services: Variation Among States 14
Prices for Hospitals’ Services: Variation Within MetropolitanAreas 15
Prices for Physicians’ Services: Variation Within MetropolitanAreas 16
Chapter 4: Factors Aecting the Prices Paid by Commercial Insurers 17
Market Power and Commercial Insurers’ Prices 17
The Relationship Between Input Prices and Prices Paid toProviders 22
Quality of Care and Commercial Insurers’ Prices 24
Providers’ Administrative Spending and Commercial Insurers’Prices 25
Cost Shifting and Commercial Insurers’ Prices 26
Appendix A: Data Sources for Figures 29
Appendix B: Sources of Estimated Average Prices for Hospitals’ and Physicians’ Services 33
Appendix C: Studies Examining the Relationship Between Market Concentration for
Providers and Prices Paid by Commercial Insurers 39
About This Document 46

Notes
To produce this report, the Congressional Budget Oce adapted data and gures from a wide variety
of sources. Brief citations for the gures are included in the gures’ captions; full citations are listed in
Appendix A.
e Medicare data used in this report reect spending, utilization, and prices in the fee-for-service
(FFS) program. ey do not include data from the Medicare Advantage (MA) program, except
where noted. Although MA data are not as widely available as FFS data, published research suggests
that MA plans and the FFS program generally pay very similar prices for hospitals’ and physicians’
services. See Jared Lane K. Maeda and Lyle Nelson, “How Do the Hospital Prices Paid by Medicare
Advantage Plans and Commercial Plans Compare With Medicare Fee-for-Service Prices?” Inquiry,
vol. 55 (June 11, 2018), pp. 1–8, https://doi.org/10.1177/0046958018779654.
e prices paid by commercial insurers reect the actual amounts paid to providers, not providers’
billed charges (“list prices”). Depending on the data source, the prices paid by Medicare and com-
mercial insurers may or may not include cost-sharing amounts paid by patients. In most of the data
sources used in this report, spending and prices for physicians’ services also reect services provided
by other health care professionals, such as nurse practitioners and physician assistants.
Chapter 1: Levels of and Trends in
Spending and Prices
is chapter describes the growth of spending by commercial health insurers and Medicare’s fee-for-service (FFS)
program on hospitals’ and physicians’ services in recent years. It illustrates the role of price increases in fueling
thegrowth of spending by commercial insurers and describes how prices are determined for those insurers and
for Medicare. is chapter also discusses sources of upward and downward pressure on prices, compares prices for
Medicare and commercial insurers, and compares payments to hospitals with hospitals’ costs.
Factors Driving the Growth of Per-Person HealthCareSpending
From 2013 to 2018, commercial insurers’ spending per person on inpatient and out-
patient hospital care and physicians’ services grew by an average of 3.2 percent a year, the
Congressional Budget Oce estimates. at spending growth was driven by increases in the
prices that commercial insurers paid for such services. Prices rose by an average of 2.7percent
a year—about 1 percentage point faster than average ination during that period, as mea-
sured by the change in the gross domestic product (GDP) price index.
1
CBO estimated the
increase in the prices paid by commercial insurers per unit of service (visits, procedures, and
admissions) from the growth of per-person spending and the quantity of services. at quan-
tity—“utilization” in the gure—was measured as the number of services provided, adjusted
for their intensity (the amount of resources or physicians’ eort used to provide them).
Utilization grew by less than 0.5 percent per year, on average, during the 2013–2018 period.
Per-person spending grew more slowly for the Medicare FFS program than for commerical
insurers—by 1.8 percent a year, on average—from 2013 to 2018. at spending growth also
stemmed mostly from price increases. e FFS program’s prices for hospitals’ and physicians’
services, which are updated regularly by statute and regulation, rose by an average of 1.3per-
cent a year. e quantity and intensity of services provided per person (which CBO esti-
mated from the growth of per-person spending and from price updates) increased by an
average of 0.5 percent a year during the 2013–2018 period.
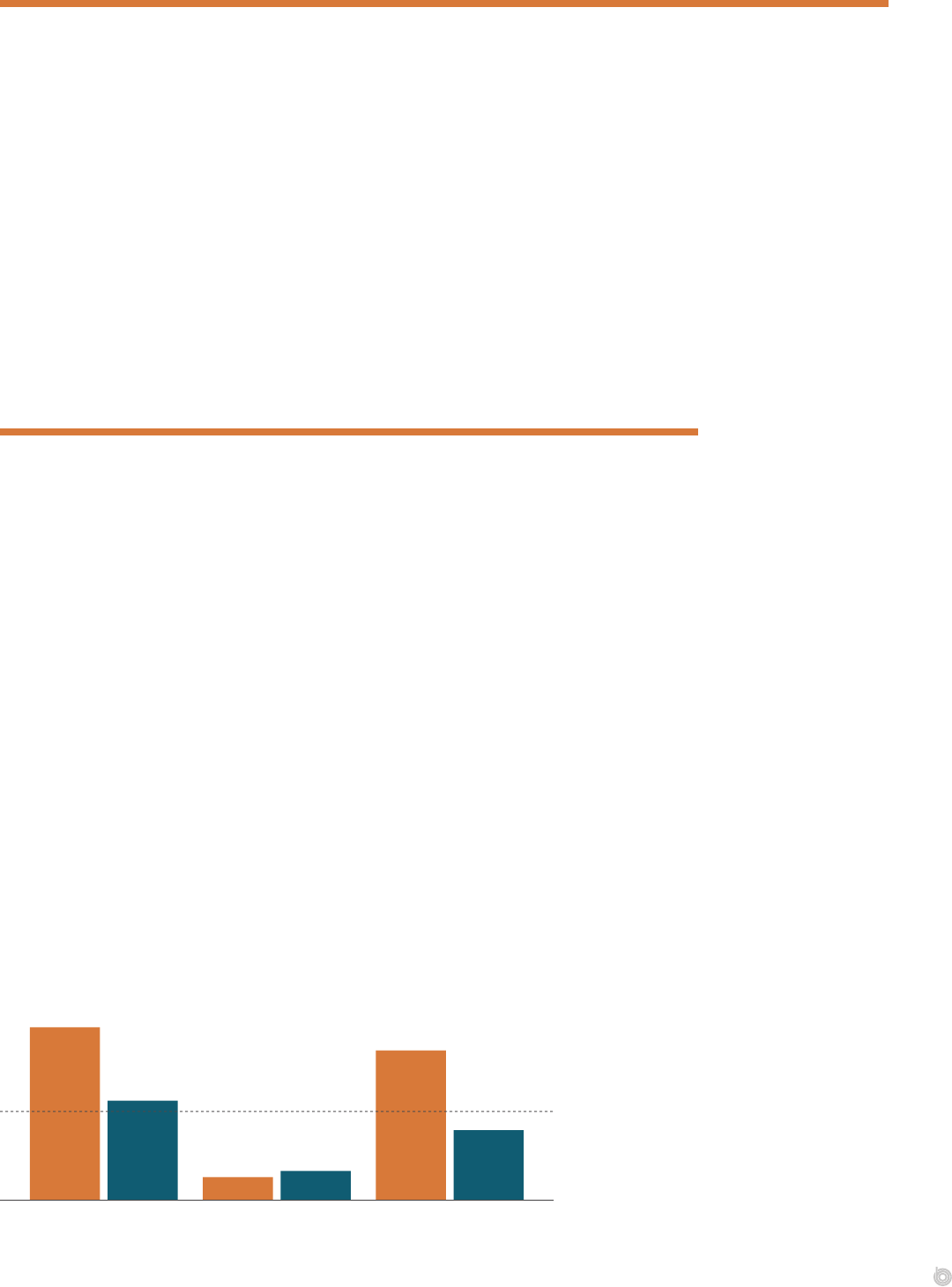
Average Annual Growth Rates of Spending, Utilization, and Prices for Hospitals’ and Physicians’
Services, 2013 to 2018
Percent
GDP Price Index (1.6)
Medicare Fee
for Service
Commercial
Insurers
3.2
1.8
0.4
0.5
2.7
1.3
Spending per Person Utilization per Person Prices Paid to Providers
Increases in the prices paid
by commercial insurers and
Medicare FFS were the major
reason for growth in their per-
person spending on hospitals’
and physicians’ services.
Price increases were larger
for commercial insurers,
exceeding the rate of inflation.
(Source: CBO’s analysis
of data from MedPAC, the
Medicare trustees, and the
Health Care Cost Institute.)
2 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
How Medicare’s Prices Are Determined
e prices that the Medicare FFS program pays providers are set administratively through
laws and regulations. e program uses various payment schedules for dierent kinds of
services. For hospitals’ services that are covered by the inpatient or outpatient prospective
payment systems, the amount that Medicare pays hospitals is predetermined. at amount
is based on a at base-payment rate, which Medicare adjusts to account for geographic
dierences in input costs, for the intensity of services, and for patients’ health (in the case of
inpatient services). Rates are also adjusted for patients who are transferred to another hospital
paid under the inpatient prospective payment system or who are discharged to a post-acute
care setting (for certain diagnoses).
In addition, Medicare makes hospital-specic adjustments for inpatient services at hospitals
that operate residency training programs or that treat a disproportionate share of low-
income patients. Medicare also makes “outlier payments”—additional payments for cases
that are extraordinarily costly—for inpatient or outpatient services. (Some hospitals, such as
certain small hospitals that Medicare considers “critical access hospitals,” are not paid under
Medicare’s prospective payment systems.)
For services covered by Medicare’s physician fee schedule, Medicare pays a xed amount per
service, with adjustments for the relative amount of resources (physicians’ eort, practice
expenses, and liability insurance) typically used to provide a given service and for geographic
dierences in the costs of delivering care. Payments are further adjusted if multiple similar
services are furnished by the same provider on the same day or for certain characteristics of
providers. For example, Medicare reduces prices if a service is provided by a nonphysician
professional, such as a nurse practitioner or social worker, or if a physician is serving as an
assistant during a surgery.
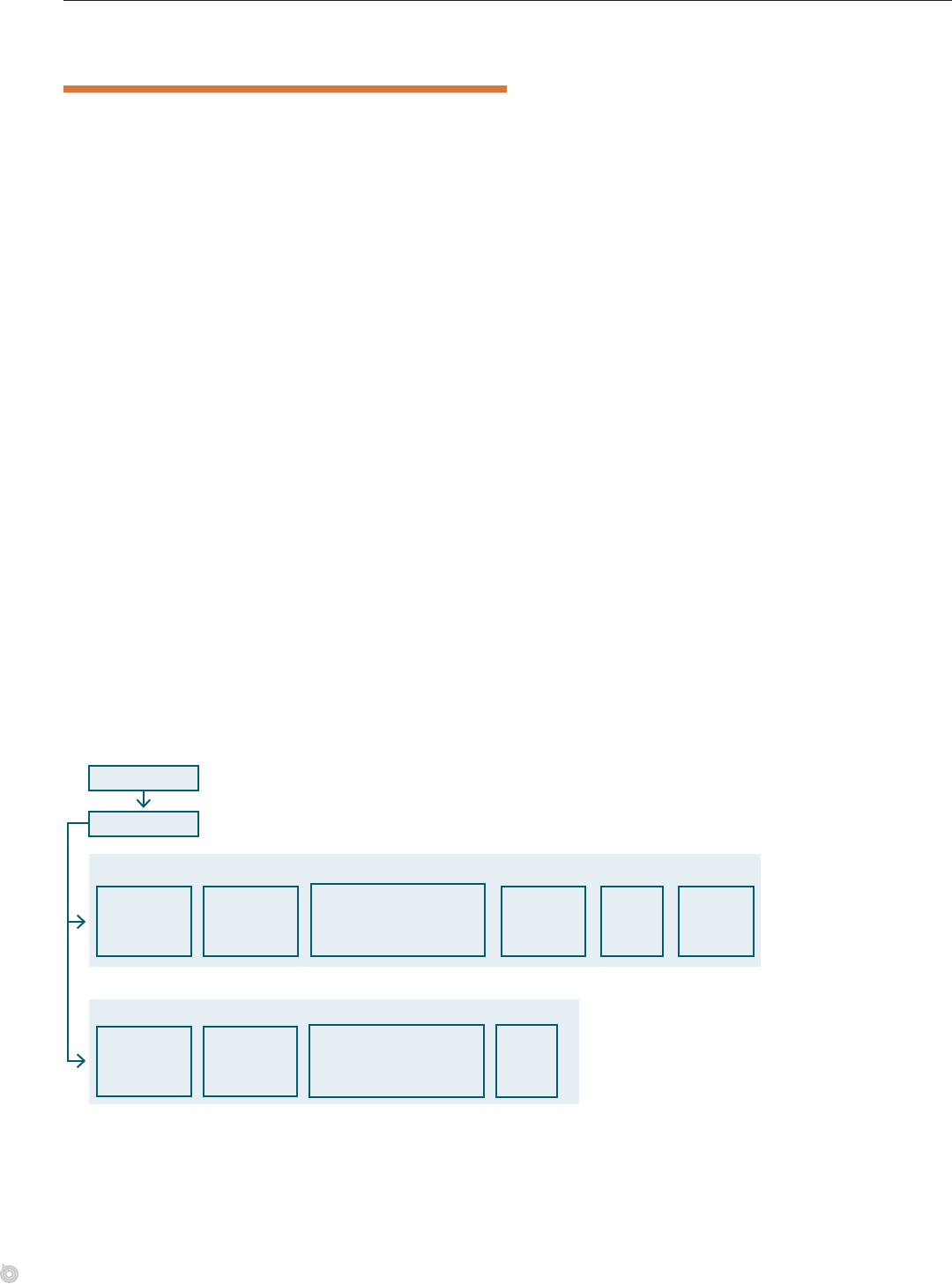
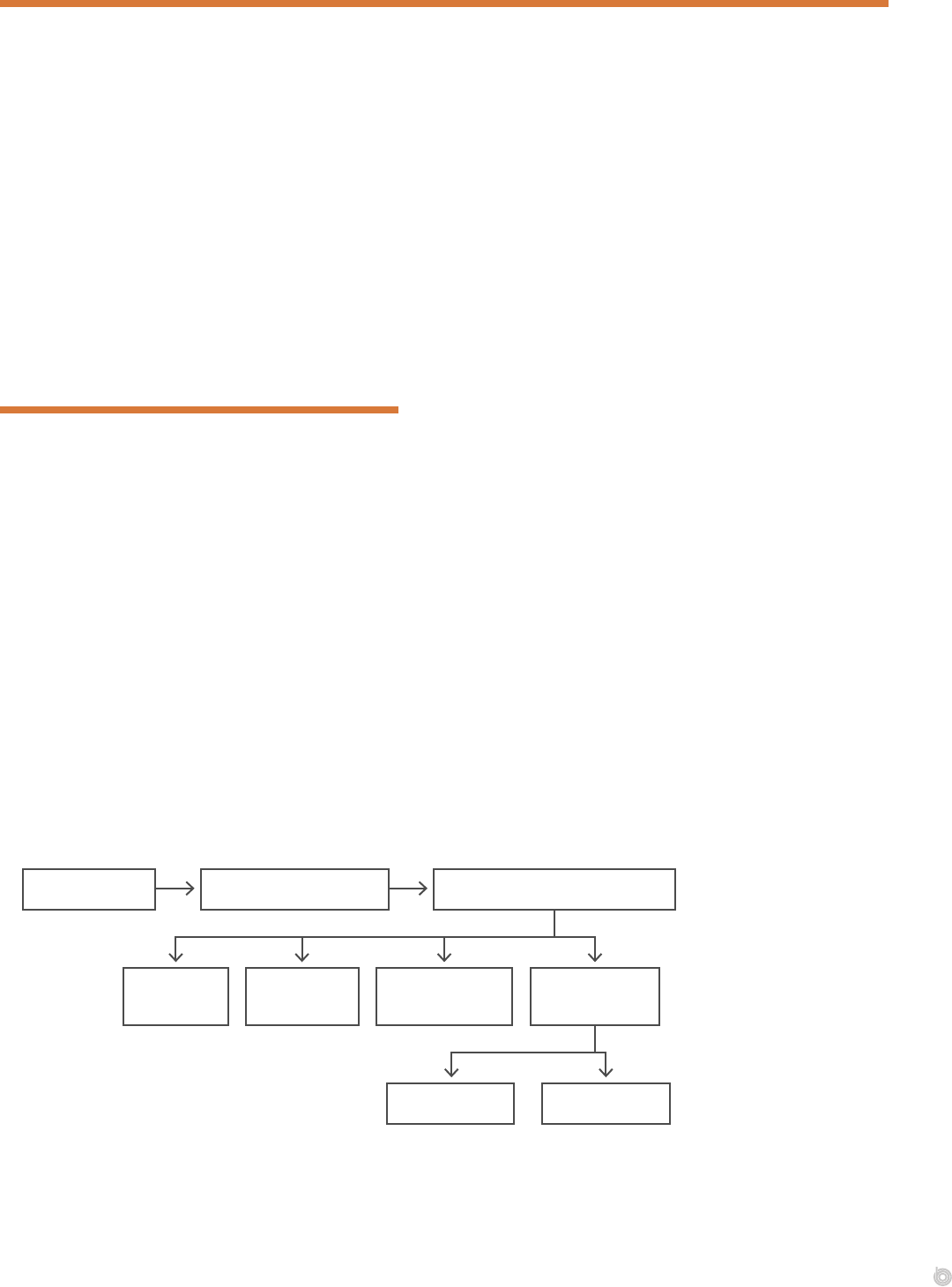
Stylized Illustration of How the Medicare FFS Program Determines Prices for Hospitals’ and
Physicians’ Services
’
’
Federal law
Final regulations
Base payment
(inpatient and
outpatient)
Intensity-
adjusted base
payment
Adjustment
for geographic
factors
Provider- or procedure-
specifi c adjustments
Price
Adjustment
for geographic
factors
× × ×
××
=
=
+
Adjustment for intensity of
services, patients’ health
(inpatient), and patients’
transfers (inpatient)
Hospital-
specifi c
adjustments
Price
Outlier
payment
The Medicare FFS
program’s prices for
inpatient, outpatient, and
physicians’ services are
set administratively by the
federal government. Base-
payment rates are adjusted
for specifics of the provider,
patient, orservice.
3CHAPTER 1 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
How Commercial Insurers’ Prices Are Determined
e prices that commercial health insurers pay in-network providers result from negotia-
tions between individual providers or provider groups and insurers. Providers agree to accept
lower in-network prices in exchange for having insurers steer patients to them and pay
claims promptly. In some instances, providers can negotiate higher prices by threatening to
stay out of an insurer’s network. at threat is more credible for providers that have a large
market share, provide high-quality services, or provide services that cannot be planned for in
advance. Such negotiations—and the contracts and prices that result from them—are often
considered trade secrets by both insurers and providers.
Insurers and providers also negotiate about the basis of payments. How hospitals are paid for
inpatient care can dier for each insurer and hospital. Methods include a at rate per stay
that varies by patients’ primary diagnosis and other health conditions (and may be set as a
percentage of the amount paid by Medicare for that service), a specied rate per day (known
as a per diem), or a specic discount from a hospital’s listed charges. Payments for hospitals’
outpatient care are frequently based on such discounts. Hospitals often prefer discounted
charges or per diems because a at rate can leave them at nancial risk for high-cost cases or
long stays. According to a recent study, hospitals with greater market power were more likely
to be paid on the basis of discounted charges.
2
Physicians are often paid by commercial insurers using the same structure as the Medicare
FFS program, but provider groups negotiate a multiplier that is applied to Medicare’s prices.
Some evidence suggests that physician groups with greater market power can negotiate
increases to that multiplier or have more ability to deviate from the Medicare FFS
paymentstructure.
3
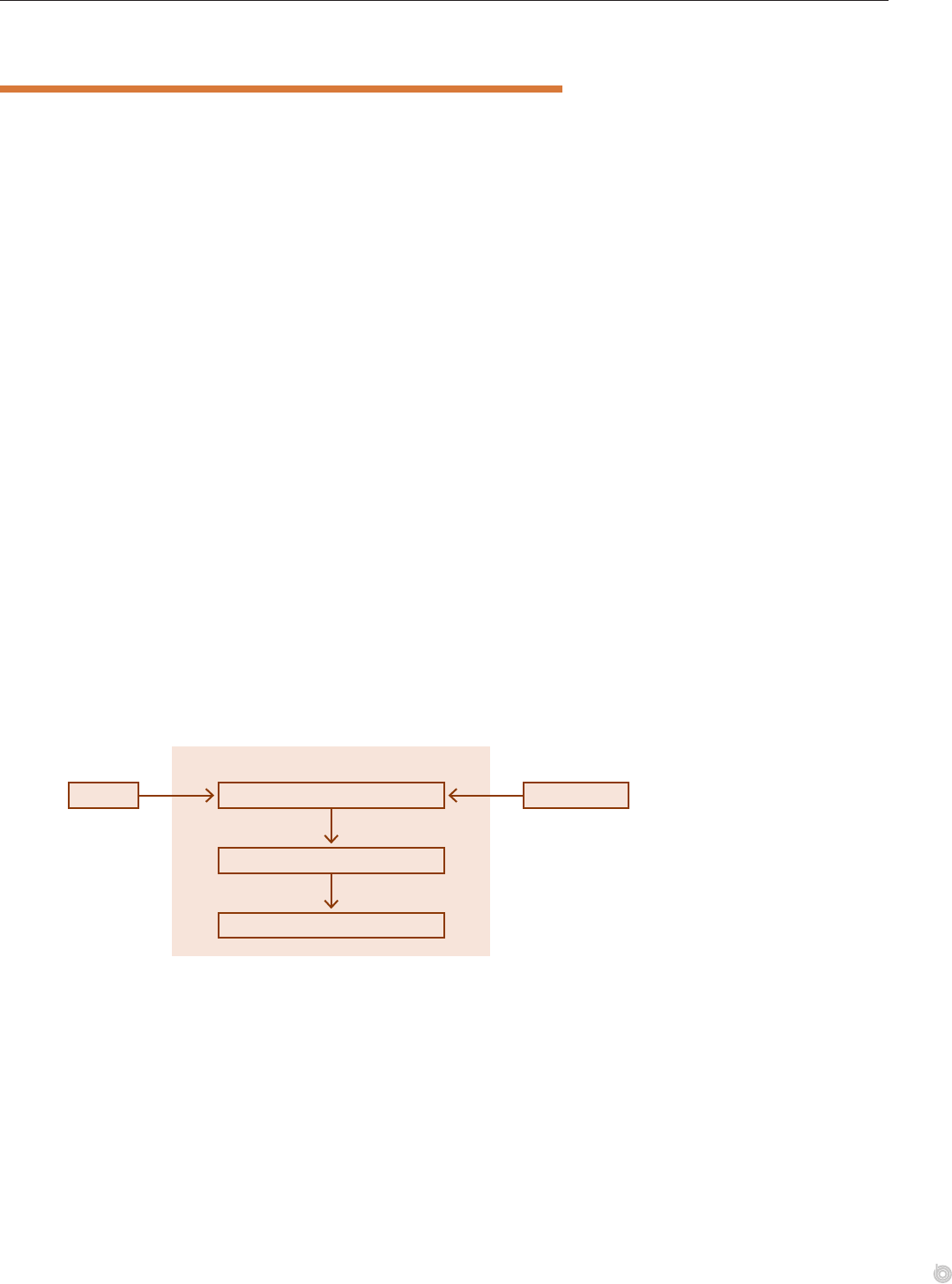
Stylized Illustration of How Commercial Insurers Determine Payments for Hospitals’ and
Physicians’Services
Providers Health insurers
Commercial insurers’ prices
Negotiations
Network contracts
The prices paid by
commercial insurers
are determined through
confidential negotiations
between individual insurers
and individual providers or
groups ofproviders.

4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Sources of Upward and Downward Pressure on Prices
e prices that commercial insurers pay for hospitals’ and physicians’ services are much
higher, and have grown much more rapidly in recent years, than the Medicare FFS program’s
prices. ose outcomes are the net result of competing factors that put upward or downward
pressure on prices. For commercial insurers, the upward pressures on prices are stronger than
the downward pressures. For Medicare FFS, prices do not rise as fast as commercial insurers’
prices because of factors that restrain their increases.
Compared with Medicare, commercial insurers are subject to fewer constraints on the prices
they pay. Private health insurance is mostly provided through employers, and private insur-
ers negotiate prices on employers’ behalf. Employers and insurers mainly try to negotiate
lower prices by threatening to exclude providers from their networks. eir ability to do
that is often limited, however, for several reasons: Providers’ market power is much greater
than employers’ in many markets; enrollees in employment-based plans tend to value having
access to broad networks; certain providers may be essential to a network in a given area; and
large insurers or employers may have enrollees in many locations with diverse medical needs,
making narrow-network plans hard to implement.
4
Employers have been slow to adopt other
methods to restrain price increases, such as reference pricing or other changes to the design of
insurance benets, because such designs are complex and could put enrollees at nancial risk.
5
In addition, the incentives for any one insurer or employer to push for lower prices are lim-
ited because the benets of doing so may not accrue directly to them. For example, insurers
have less incentive to negotiate lower prices because they can pass providers’ price increases
on to employers. A dominant insurer may even limit the discounts that a provider can oer
to other insurers, which can raise the prices paid by those other insurers and their premiums.
6
Negotiating lower prices may also involve trade-os for employers. For instance, employers
may be reluctant to reduce prices by adopting a plan with a narrower network or by reducing
health care benets if they use those benets to compete for high-value employees.
Conversely, one factor putting downward pressure on the prices paid by commercial insurers
is that employers may have to nance higher provider prices by raising premiums, limiting
wage increases, or reducing their plans’ benets. e strength of that downward pressure is
dampened, however, because premium contributions are generally excluded from federal
taxes and because the link between higher provider prices and lower wages or narrower bene-
ts is indirect, so most employees do not see it.
For Medicare FFS, price increases have been limited in part because annual updates to prices
are set through statute and regulation and have been modest in recent years. Prices for hos-
pitals’ inpatient and outpatient services are updated using a measure of changes in the prices
of hospitals’ key inputs, minus the increase in economywide productivity.
7
Price updates
for physicians’ services are set by law; those prices have risen by less than 0.5 percent a year
since 2015. In addition, Medicare oers payment rates to providers on a take-it-or-leave-it
basis. Providers that do not want to accept those rates can decline to participate. But because
Medicare accounts for a large share of U.S. health care spending, providers may have limited
nancial ability to opt out of the program.
Another source of downward pressure on Medicare’s prices is that, because Medicare is a fed-
eral program, proposals that would raise its spending must be nanced through higher taxes
or premiums, increases in federal debt, or cuts in Medicare benets or other spending. e
strength of that downward pressure is partly reduced, however, by concerns about providers’
nancial stability and Medicare beneciaries’ access to care.

5CHAPTER 1 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Average Prices for Hospitals’ Services
CBO reviewed a range of studies published between 2010 and 2020 that compared com-
mercial insurers’ and the Medicare FFS program’s prices for hospitals’ services. On average,
the ve studies that looked at overall prices for hospitals’ services suggest that the prices paid
by commercial insurers were more than twice those paid by Medicare FFS.
8
(e combined
average price ratio for inpatient and outpatient services reported by those studies ranged from
167 percent of Medicare FFS’s prices to 250 percent.) ose studies also generally reported
substantial variation in prices for the same service in dierent areas, in dierent hospitals,
and within the same hospital.
e ratio of commercial insurers’ prices to Medicare FFS’s prices was generally much higher
for outpatient services than for inpatient services. Averaged across the 6 studies on outpa-
tient services and 11 studies on inpatient services that CBO reviewed, commercial insurers’
prices were 240 percent of Medicare FFS’s prices for outpatient services and 182 percent of
Medicare FFS’s prices for inpatient services. e reasons for the higher price ratio for out-
patient services are not fully understood. ose reasons could include contracting practices:
Contracts based on discounted charges are more common for hospitals’ outpatient services
than for inpatient services, and that type of contract may encourage higher prices.
In its literature review, CBO included studies that compared commercial insurers’ prices with
Medicare FFS’s prices or that reported payment-to-cost ratios both for private sources
(including uninsured people) and for Medicare. CBO then calculated a simple average of the
studies’ results. ose studies’ estimates may have diered because of dierences in the
locations, time periods, or types of data used in the studies. For instance, estimates can dier
depending on whether a data source includes patients’ total cost-sharing responsibilities or
the amounts that were actually collected from patients.
Studies’ Estimates of Commercial Insurers’ Prices for Hospitals’ Services as a Percentage of
MedicareFFS’s Prices
Hospitals’ Services Overall Outpatient Services Inpatient Services
Average (223%)
Average (182%)
Average (240%)
Bai and Anderson, 2018 (250%)
AHA, 2020 (167%)
Whaley and Others,
2020 (231%)
White and Whaley,
2019 (293%)
Selden, 2020 (155%)
Fronsdal and Others,
2020 (137%)
For hospitals’ services as a
whole, the prices paid by
commercial insurers were
more than double the prices
paid by Medicare FFS, on
average, in recent years.
(Source: CBO’s review of
published literature; see
Appendix B.)
6 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Average Prices for Physicians’ Services
For physicians’ services overall, commercial insurers paid 129 percent of Medicare FFS’s
prices, on average, according to studies published between 2010 and 2020. (CBO reviewed
seven studies that looked at physicians’ services as a whole; their average price ratio ranged
from 118 percent of Medicare FFS’s prices to 163 percent.) ose studies also generally
reported substantial variation in prices for the same service among geographic areas, physi-
cian practices, and physician specialties.
Relative to Medicare FFS’s prices, the prices paid by commercial insurers for primary care
services and oce visits were generally lower than the prices paid for specialty services.
Among the ve studies of primary care services or oce visits and ve studies of specialty
services that CBO reviewed, commercial insurers’ prices were 117 percent of Medicare FFS’s
prices for primary care services or oce visits, on average, and 144 percent of Medicare
FFS’sprices for specialty services.
Higher prices for specialty services could stem from three factors: Fewer doctors provide any
one of those services; many doctors who do are employed in larger, multispecialty practices;
and more of those practices are aliated with hospitals. (In this analysis, average prices for
specialty services do not include emergency services or physicians’ services provided only in
inpatient settings.) Some of the variation in estimates among studies comes from dierences
in the types of physicians’ services included.
In its literature review, CBO looked only at studies that compared prices paid by commercial
insurers and Medicare FFS. CBO then calculated a simple average of the studies’ results. For
studies that reported prices separately for specic services or markets (such as employer-
sponsored plans versus individually purchased plans), CBO averaged those prices, weighting
them by the frequency of services or by estimates of premiums for dierent segments of the
market from CBO’s baseline budget projections. e studies’ estimates of relative prices for
physicians’ services may dier because of dierences in data sources, time periods, settings
ofservice (such as hospitals’ outpatient departments versus physicians’ oces), or the specic
services or markets included in the studies.
Studies’ Estimates of Commercial Insurers’ Prices for Physicians’ Services as a Percentage of
Medicare FFS’s Prices
Physicians’ Services Overall Primary Care Services
or Office Visits
Specialty Services
Average (129%)
Average (117%)
Average (144%)
Chernew and Others,
2020 (163%)
MedPAC, 2020 (128%)
Trish and Others,
2017 (179%)
Biener and Selden,
2017 (117%)
Pelech, 2020 (106%)
Ginsburg, 2010; Biener
and Selden, 2017 (118%)
On average, the prices paid
by commercial insurers for
physicians’ services as a
whole were about one-
quarter higher than the
prices paid by Medicare FFS
in recent years. (Source:
CBO’s review of published
literature; see Appendix B.)
7CHAPTER 1 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
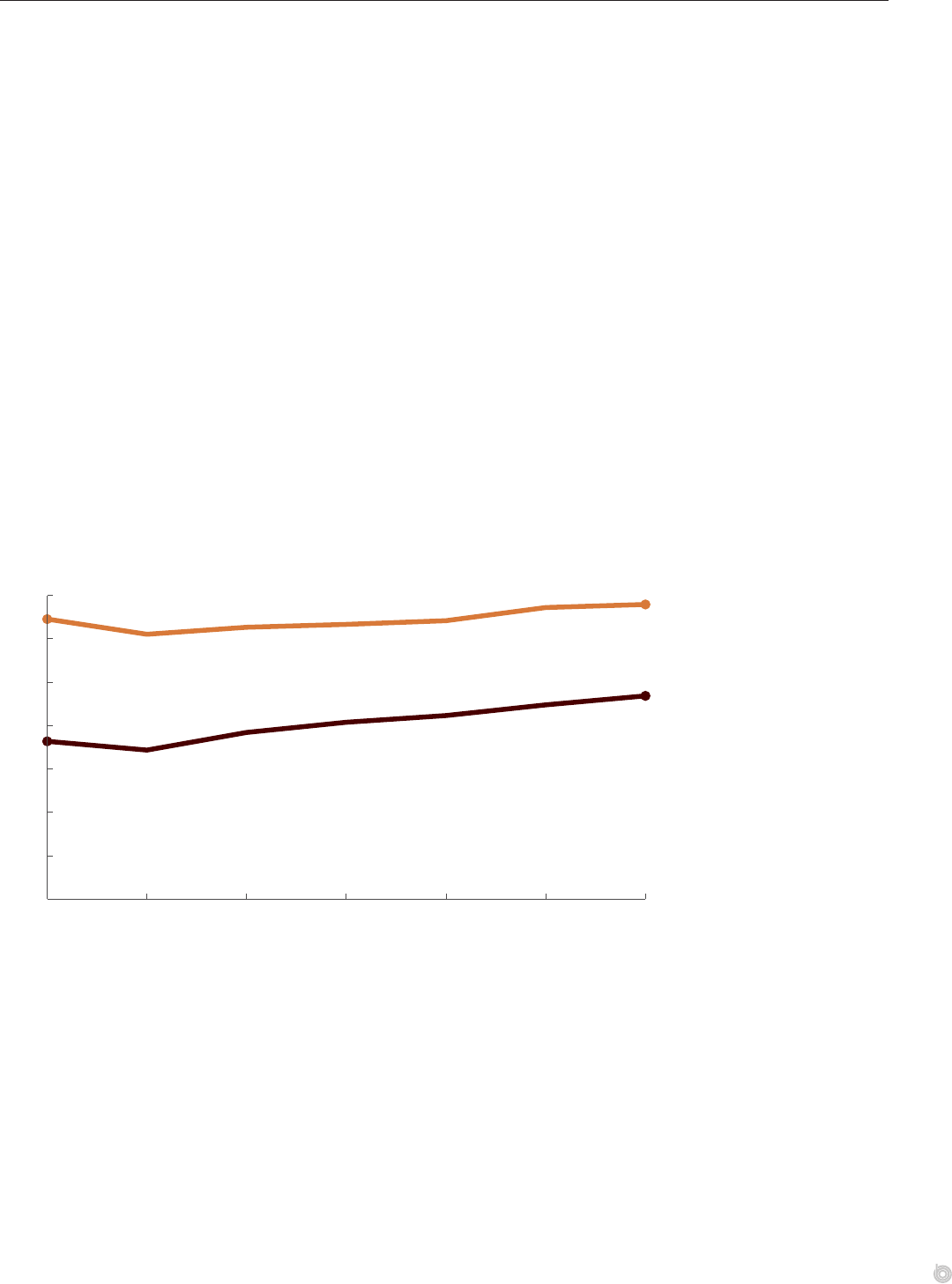
How Payments to Hospitals Compare With Hospitals’ Costs
According to data from the American Hospital Association (AHA), Medicare’s total pay-
ments for inpatient and outpatient services are lower than hospitals’ costs to provide those
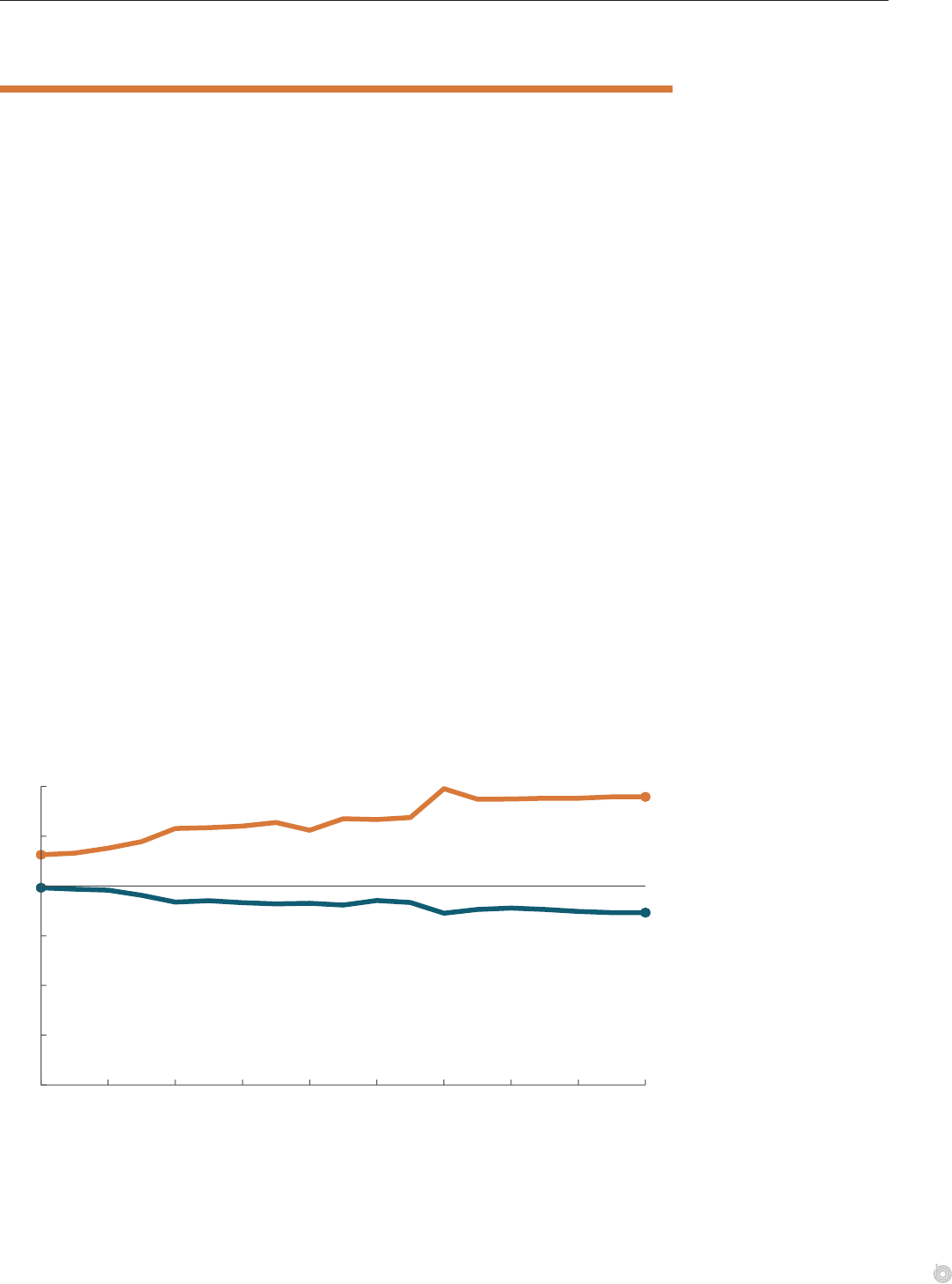
services. Private payers’ payments, by contrast, are much higher than hospitals’ costs. Between
2000 and 2018, private payers’ payments rose from 116 percent to 145 percent of hospitals’
costs, whereas Medicare’s payments fell from 99 percent to 87 percent of hospitals’ costs. (In
the AHA data, Medicare includes both the FFS program and Medicare Advantage plans, and
private payers consist of all nongovernment payment sources.)
e payment-to-cost ratios in the AHA data reect hospitals’ total costs for delivering care,
including stas’ salaries and the costs of buildings and equipment. ose total costs vary
because of external factors, such as local wages and utilities, and internal factors related to
hospitals’ behavior, such as how eciently they can manage their resources. Although pay-
ments by Medicare are lower than hospitals’ costs, on average, research suggests that hospi-
tals have some control over their cost structure and can adjust their expenses on the basis of
the nancial resources they have available.
9
e Medicare Payment Advisory Commission
(MedPAC) has identied a subset of hospitals as “ecient,” meaning that they perform well
in the areas of cost and quality. Such hospitals had positive Medicare margins from 2010
until about 2015, although they have had slightly negative Medicare margins since 2016.
10
Payments for hospitals’ services in the AHA data reect all payments made for care, not just
the prices negotiated by a subset of payers. Private payments, in particular, reect a wide
variety of sources—from uninsured people, who typically pay less than commercial payers, to
automobile liability insurance and workers’ compensation, which tend to pay more. Private
payments also reect patients’ unpaid debts, which tends to reduce private payers’ prices in the
AHA data relative to the prices reported in other studies. (CBO does not know of any regu-
larly updated source of data about costs or payment-to-cost ratios for physicians’ services.)
Payment-to-Cost Ratios for Hospitals, 2000 to 2018
Percent
0
25
50
75
100
125
150
2000 2002 2004 2006 2008 2010 2012 2014 2016 2018
86.6
144.8
99.1
115.7
Private Payers
Medicare FFS
Total payments for
hospitals’ services, as a
percentage of hospitals’
costs to deliver those
services, have increased
for private payers and
decreased for Medicare
since 2000. (Source: CBO’s
analysis of national-level
data from the AHA.)

8 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
1. CBO analyzed changes in per-person spending because they are not aected by growth in the number
of people with health insurance. Rather, changes in per-person spending among people with insurance
result from changes in utilization (including the amount and intensity of services), in prices, or in patients’
characteristics, such as age or sex (though the eect of those types of demographic changes is thought
to be limited). For information about the eects of demographic changes on Medicare spending, see
Laura M. Keohane, Lucas Stewart, and Melinda B. Buntin, e Slowdown in Medicare Spending Growth
for Baby Boomers and Older Beneciaries: Changes in Medicare Spending Levels and Growth by Age Group,
2007–2015(Commonwealth Fund, December 27, 2019), https://doi.org/10.26099/sy0d-xs78; and Michael
Levine and Melinda Buntin, Why Has Growth in Spending for Fee-for-Service Medicare Slowed? Working Paper
2013-06 (Congressional Budget Oce, August 2013), www.cbo.gov/publication/44513. e data from the
Health Care Cost Institute that CBO analyzed were weighted to be representative of the population with
employment-based insurance plans; thus, the eects of age and sex on those plans’ per-person spending
should be minimal.
2. See Zack Cooper and others, “e Price Ain’t Right? Hospital Prices and Health Spending on the
Privately Insured,” Quarterly Journal of Economics, vol. 134, no. 1 (February 2019), pp. 51–107,
https://doi.org/10.1093/qje/qjy020.
3. See Jerey Clemens, Joshua D. Gottlieb, and Tímea Laura Molnár, e Anatomy of Physician Payments:
Contracting Subject to Complexity, Working Paper 21642 (National Bureau of Economic Research, October
2015), www.nber.org/papers/w21642.
4. For comparisons of employers’ and providers’ market power, see Matthew D. Eisenberg and others, “Large
Self-Insured Employers Lack Power to Eectively Negotiate Hospital Prices,” American Journal of Managed
Care, vol. 27, no. 7 (July 2021), pp. 290–296, https://doi.org/10.37765/ajmc.2021.88702.
5. Reference pricing sets a benchmark price for certain services, and enrollees are responsible for the dierence
between providers’ negotiated price and the reference price. See Anna D. Sinaiko, Shehnaz Alidina, and Ateev
Mehrotra, “Why Aren’t More Employers Implementing Reference-Based Pricing Benet Design?” American
Journal of Managed Care, vol. 25, no. 2 (February 2019), pp. 85–88, https://tinyurl.com/ps7t2w93.
6. ose limits on the prices paid by rival insurers are the result of “most-favored nation” clauses in contracts.
See David Cutler and Leemore Dafny, “Designing Transparency Systems for Medical Care Prices,” New
England Journal of Medicine, vol. 364, no. 10 (March 10, 2011), pp. 894–895, https://doi.org/10.1056/
NEJMp1100540.
7. e Medicare FFS program’s adjustment for productivity reects the change in economywide multifactor
productivity in the private, nonfarm business sector. (Multifactor productivity measures the amount of goods
and services produced relative to the amount of inputs used to produce those goods and services.)
8. e estimate based on data from the AHA compared commercial insurers’ prices for hospitals’ services
with the prices paid by both the Medicare FFS program and Medicare Advantage (MA) plans. In CBO’s
assessment, the AHA’s estimate would be nearly unchanged if it only included FFS prices because MA plans’
prices for hospitals’ services are roughly equal to those paid by the Medicare FFS program, on average,
according to published research.
9. See Chapin White and Vivian Yaling Wu, “How Do Hospitals Cope With Sustained Slow
Growth in Medicare Prices?” Health Services Research, vol. 49, no. 1 (February 2014), pp. 11–31,
https://doi.org/10.1111/1475-6773.12101.
10. Medicare margins were calculated as total Medicare revenues minus total Medicare-allowable costs, divided
by revenues. Of the 1,878 hospitals that met MedPAC’s screening criteria over the 2015–2017 period, about
14 percent were found to be relatively ecient. See Medicare Payment Advisory Commission, “Hospital
Inpatient and Outpatient Services,” Chapter 3 in Report to the Congress: Medicare Payment Policy (March
2020), p. 92, https://tinyurl.com/yckkxfuy.
Chapter 2: The Implications of
PriceIncreases
is chapter describes how the high and rising prices that commercial insurers pay for hospitals’ and physicians’
servicesaect people with private health insurance and the federal budget.
How Price Increases Aect People
WithEmployment-BasedInsurance
A rise in providers’ prices would increase health insurers’ spending on claims, all else being
equal. Insurers could respond to such spending increases by raising premiums, increasing
cost-sharing requirements for patients, reducing the scope of benets, or making other
adjustments. In general, insurers’ greater spending would be passed on to employers that
purchase coverage on behalf of their employees.
1
Employers’ spending on health insurance
represents a large part of their employees’ nonwage compensation, so employers generally
take actions to oset increases in health insurance spending in order to maintain their prots.
A recent study found that price increases for hospitals’ services were associated with a rise in
employees’ out-of-pocket costs, an increase in the use of high-deductible health plans, and
slower wage growth for employees.
2
In addition, the Congressional Budget Oce analyzed
data from the Kaiser Family Foundation’s Employer Health Benets Survey and information
from the Bureau of Labor Statistics and found that between 2010 and 2020, average total
premiums rose by 55 percent for a family plan (from $13,770 to $21,342) and by 48 percent
for an individual plan (from $5,049 to $7,470), whereas median wages grew by only 32per-
cent over that period.
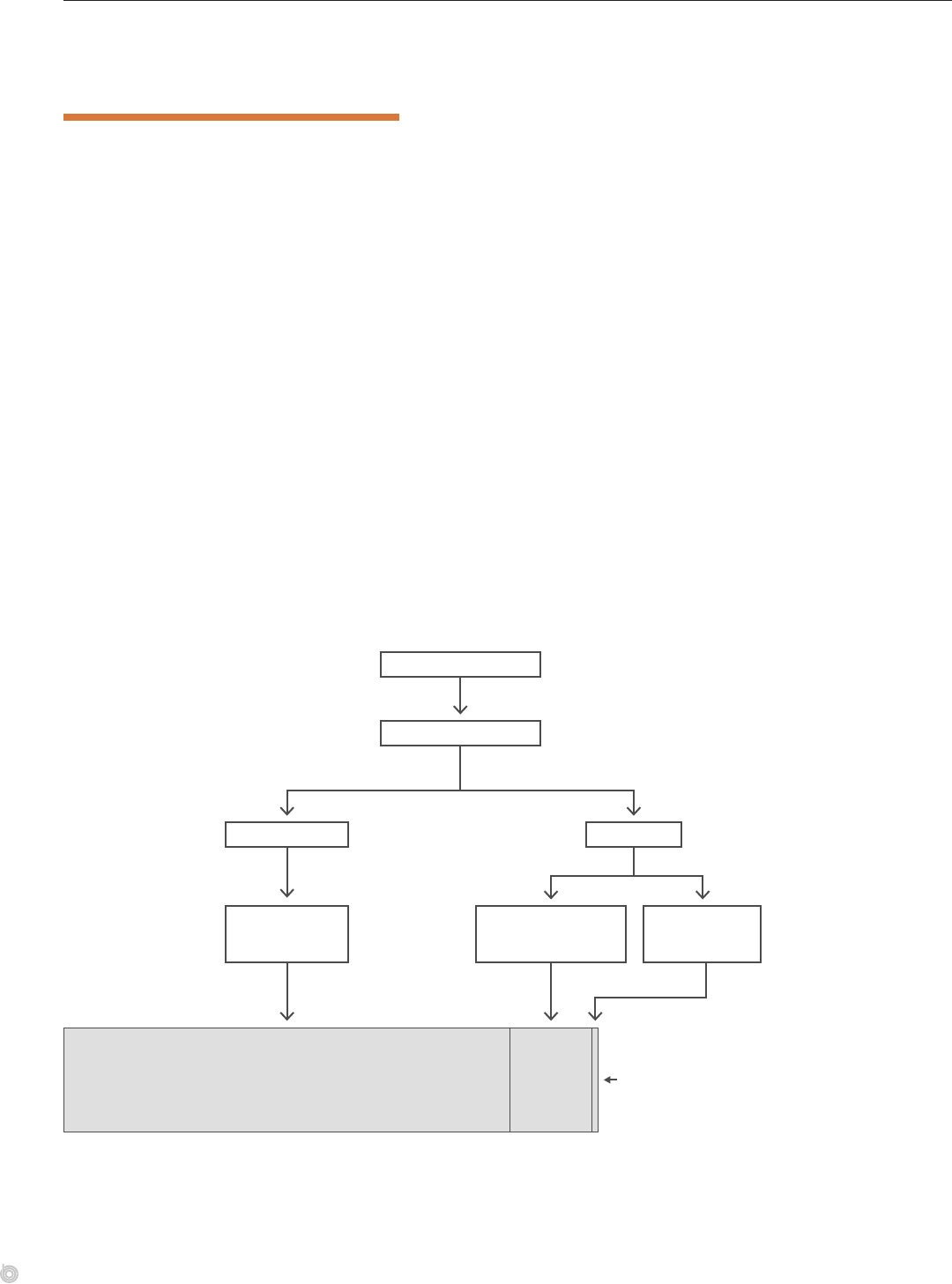
Eects of Higher Prices on Health Insurance Premiums and Benefits, Out-of-Pocket Costs, and Wages
When prices paid to
providers increase
Commercial health insurers’
spending on claims increases
Plans are adjusted in ways that have
one or more of the following results . . .
Employers’
premium payments
increase
Employees’ wages
grow more slowly
Firms’ profi ts
decline
Employees’
premium payments
increase
Covered
benefi ts are
narrowed
Patients’
out-of-pocket
costs increase
All else being equal,
increases in the prices
that commercial insurers
pay providers are
associated with increases
in premiums for employers
or employees, increases
in out-of-pocket costs
for enrollees, reductions
in covered benefits,
slowdowns in wage growth
for employees, or declines
in firms’ profits.
10 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
How Price Increases Aect Federal Subsidies for
CommercialHealthInsurance
e federal tax code contains various provisions that subsidize commercial health insur-
ance—both employment-based insurance and nongroup (individually purchased) plans.
For example, premiums for people with employment-based insurance are generally excluded
from federal income and payroll taxes. In addition, some out-of-pocket medical costs and
premium payments are subsidized through the tax deduction for itemized medical expenses.
efederal government also provides people who qualify with tax credits to reduce premiums
for nongroup health insurance purchased through the marketplaces established under the
Aordable Care Act. And the tax code allows some self-employed people who buy nongroup
insurance to deduct up to 100 percent of their premiums from their income. Because of
such provisions, increases in the prices that plans pay to providers aect federal subsidies for
commercial health insurance.
Insurers pass higher costs on to employers through premium increases or changes to plans’
benets. Since the tax code generally lets employers and employees contribute to the cost of
premiums with pretax dollars, higher premiums reduce taxable wages and increase federal
subsidies for employment-based insurance. Likewise, when premiums rise for the benchmark
plans oered in the federal or state health insurance marketplaces, tax credits for people who
buy insurance through those marketplaces rise as well.
Relationships Between Prices for Providers and Major Federal Subsidies for Commercial Health
Insurance in 2020
Federal subsidies for employment-based insurance
($288 Billion)
Marketplace
premium
subsidies
($53 Billion)
Subsidy for
self-employment
health insurance
($4 Billion)
Prices paid to providers
Health insurers’ costs
Employment-
Based Insurance
Nongroup
Plans
Premiums Premiums
Tax exclusion
for employment-
based insurance
Tax credit outlays and
revenue reductions
for nongroup plans
Tax deduction for
self-employment
health insurance
Major Federal Subsidies for
Commercial Health Insurance
Higher prices paid by
commercial insurers
to providers increase
federal subsidies for
health care because
of the tax preferences
for employment-based
insurance and premium
subsidies for nongroup
coverage. (Source: CBO.)

11CHAPTER 2 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
1. For people with nongroup insurance, increases in premiums or reductions in benets mainly aect the
covered individuals. e degree to which people with nongroup plans are aected by premium increases
depends on the size of the subsidies they receive from the federal government. ose who receive little or no
subsidy bear most of the cost of higher provider prices, whereas those who receive more subsidies are largely
shielded from price increases.
2. See Daniel Arnold and Christopher M. Whaley, Who Pays for Health Care Costs? e Eects of Health Care
Prices on Wages, Working Paper WR-A621-2 (RAND, July 2020), https://doi.org/10.7249/WRA621-2.
Chapter 3: Variation in Prices Among and
Within Geographic Areas
is chapter describes how prices for hospitals’ and physicians’ services vary among dierent areas, among hospitals
or provider groups in the same area, and within hospitals for the same or similar services. Prices can vary for many
reasons, but large variation in prices for similar services can be evidence of market ineciencies.
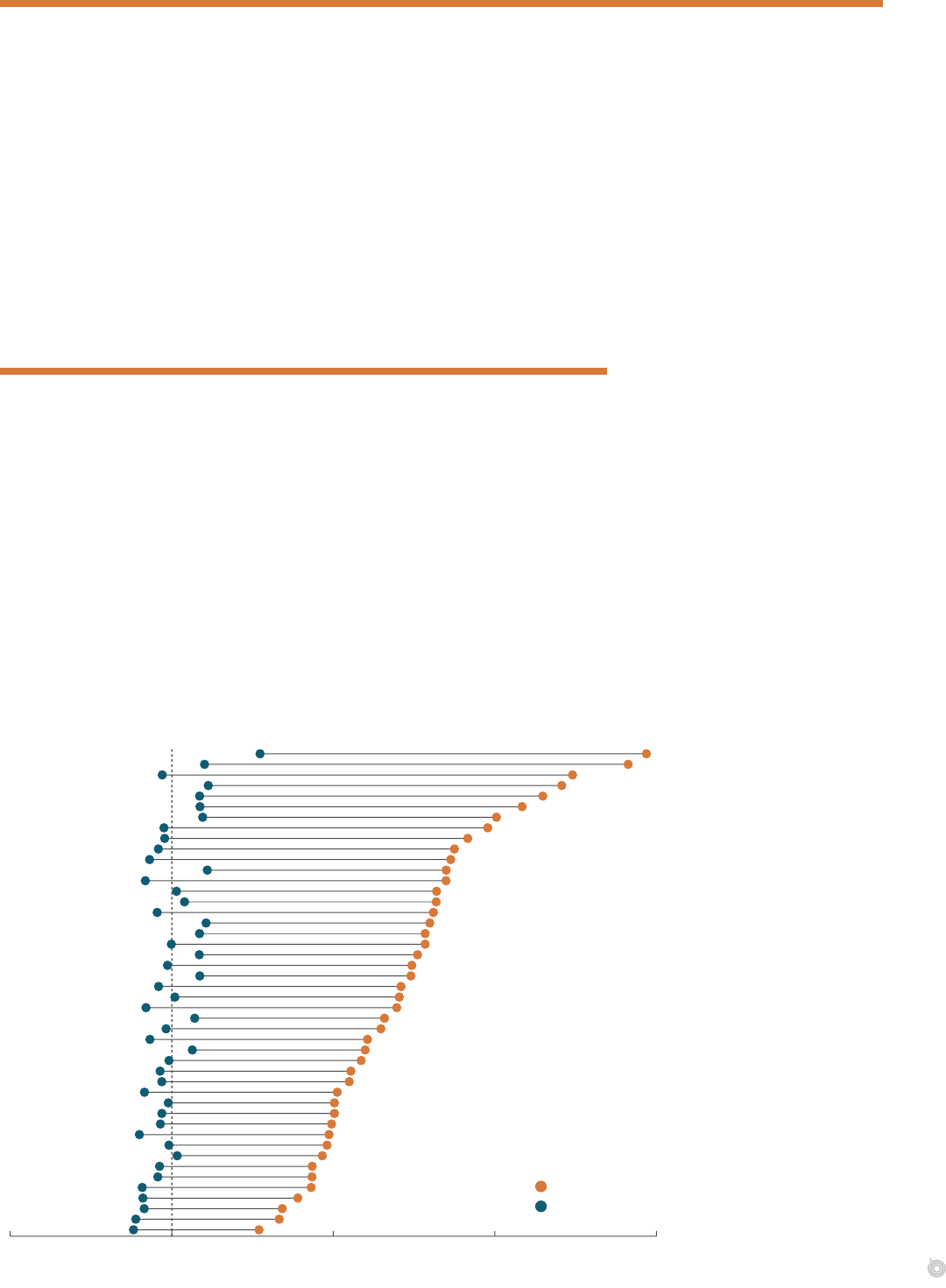
Prices for Hospitals’ Services: Variation Among States
e average prices that Medicare’s fee-for-service program and commercial employment-based
plans paid for hospitals’ inpatient services in 2018—relative to the national average price paid by
Medicare FFS—varied widely by state. e statewide average Medicare FFS price ranged from
24 percent lower than the program’s national average price in Arkansas to 55 percent higher
than the national average in Massachusetts. Prices for Medicare services diered among states
because of the location- and hospital-specic adjustments Medicare makes (see Chapter 1).
1
e degree of price variation was much greater for commercial insurers. e average state-level price
paid by commercial employment-based plans ranged from 54 percent higher than the national
average Medicare FFS price in Arkansas to 294 percent higher than that price in Massachusetts.
(e Congressional Budget Oce limited this analysis to employment-based plans because
price data are not as widely available for other types of commercial plans. Prices for inpatient
services are allowed amounts per stay, with stays adjusted to reect the intensity of the service.)
Average Prices for Hospitals’ Inpatient Services, by State, 2018
AR
NE
KY
KS
MO
MI
OK
PA
NV
MS
NM
CO
UT
LA
OH
TX
NC
NJ
ID
IL
CT
AL
AZ
IA
VT
WA
WY
MT
OR
RI
IN
DE
WI
SC
ME
FL
WV
VA
GA
CA
NH
AK
MN
TN
NY
MA
0 1x 2x 3x 4x
Price Relative to Medicare Fee-for-Service National Average
Commercial Insurers
Medicare FFS
Commercial insurers’ prices
for hospitals’ inpatient
services varied substantially
among states in 2018,
as did the gap between
commercial insurers’
and Medicare’s prices.
Commercial insurers’
prices were highest,
relative to Medicare’s, in
Massachusetts, New York,
and Tennessee. (Source:
CBO’s analysis of data from
Whaley and others,2020.)
14 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
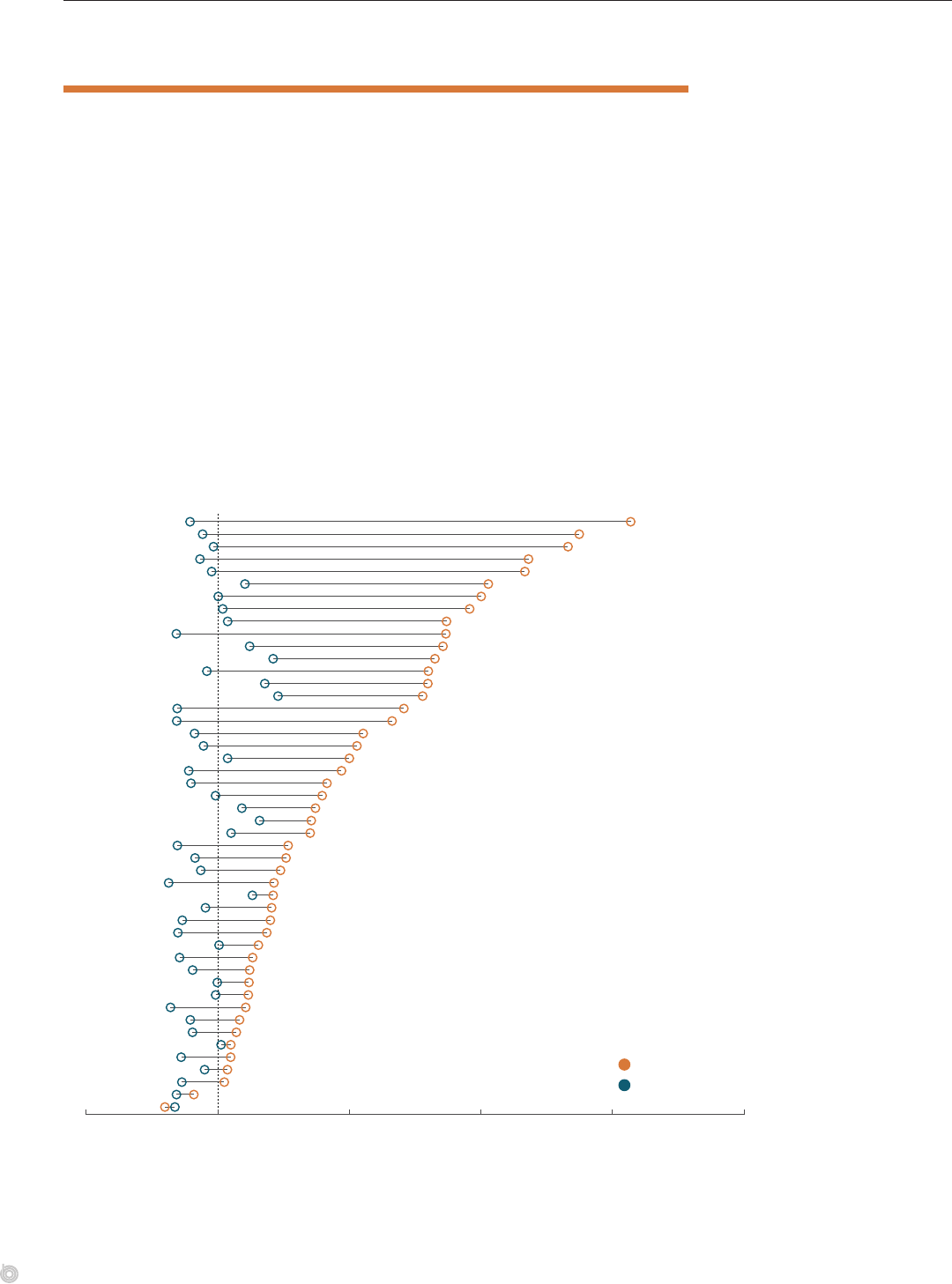
Prices for Physicians’ Services: Variation Among States
Relative to the national average Medicare FFS price for physicians’ services, the average price
paid by Medicare FFS and commercial insurers for a set of 500 common services in 2017
varied among states. (ose 500 services reect the service codes that appeared most often
in aggregate data drawn from employment-based plans in the claims database of the Health
Care Cost Institute, or HCCI. ey include services such as oce visits and knee replace-
ments.) e statewide average Medicare FFS price ranged from 9 percent lower than the
program’s national average price in Mississippi to 11 percent higher than the national average
in Washington, DC. In this analysis, average Medicare prices diered primarily because of
Medicare’s geographic adjustments for input prices.
e magnitude of the price variation was much larger for commercial insurers than for
Medicare FFS. e average state-level price paid by commercial insurers ranged from about
10 percent lower than the national average Medicare FFS price in Alabama to 78 percent
higher than that price in Wisconsin. Commercial insurers’ average price exceeded the average
state Medicare FFS price in every state except Alabama.
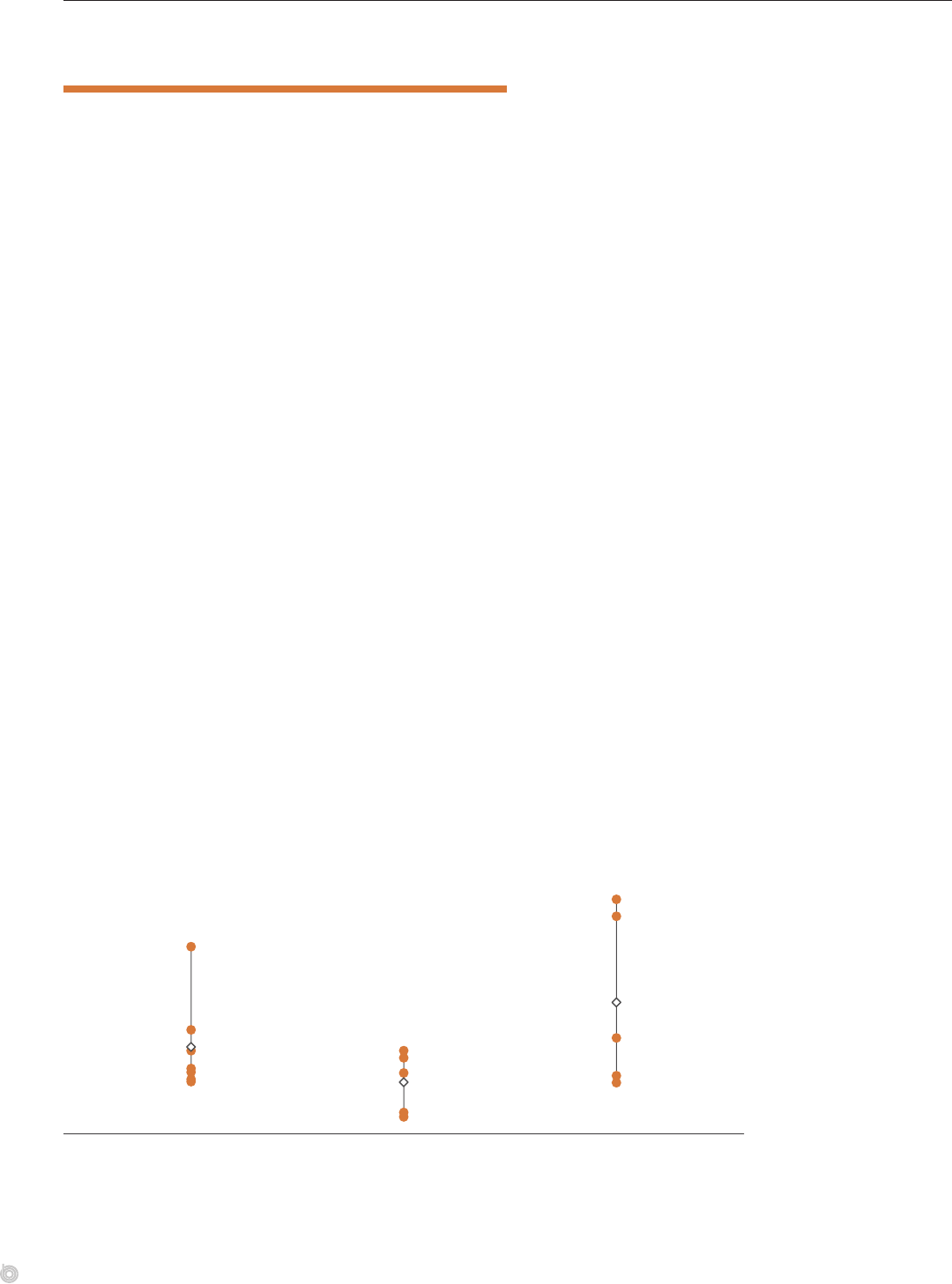
Average Prices for Physicians’ Services, by State, 2017
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
AL
KY
IN
AZ
KS
DE
MO
OH
AR
PA
FL
LA
OK
NV
WV
SC
MI
MD
MS
TX
UT
TN
VA
NJ
HI
CO
ME
NC
IL
GA
NM
IA
ID
DC
CA
VT
NY
CT
NE
WA
NH
MT
MA
WY
SD
OR
ND
WI
0.75x 1x 1.25x 1.5x 1.75x 2x
Price Relative to Medicare Fee−for−Service National Average
Commercial Insurers
Medicare FFS
Commercial insurers’ prices
for physicians’ services
varied substantially among
states in 2017. They
were highest, relative
to Medicare’s prices, in
Wisconsin, North Dakota,
and Oregon. (Source:
CBO’s analysis of data from
Johnson and others,2020.)
15CHAPTER 3 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
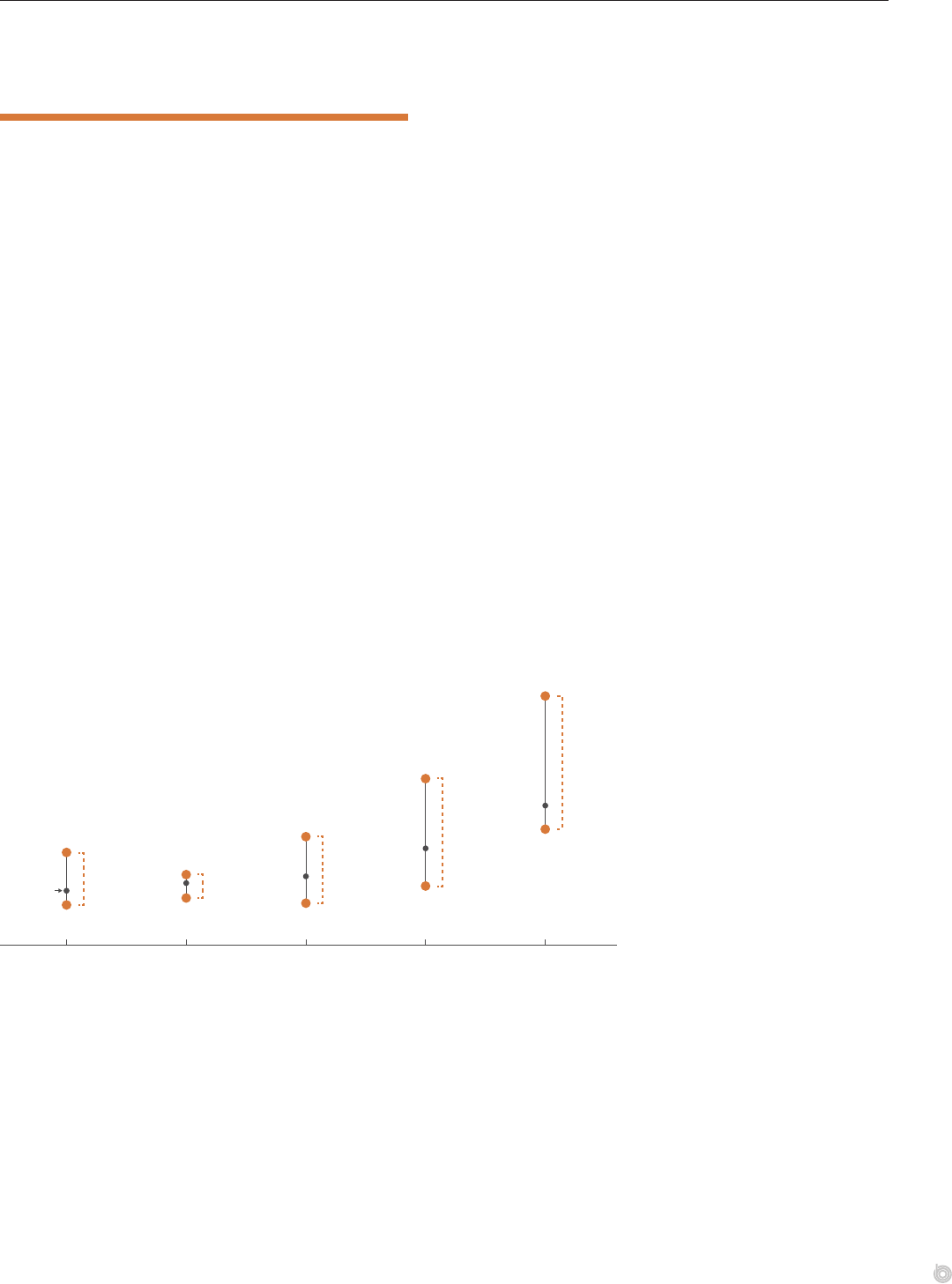
Prices for Hospitals’ Services:
VariationWithinMetropolitanAreas
Commercial insurers’ prices for hospitals’ services vary widely not only by state but also
within a given metropolitan statistical area, or MSA (a geographic area that generally con-
sists of one or more cities and the surrounding population). For example, the median price
that commercial insurers paid for a vaginal delivery of a baby—a well-dened and fairly
standardized service—in San Francisco in 2016 was $13,363. But the range of prices around
that median in the San Francisco area was quite broad: e price at the 90th percentile of
the distribution of prices ($23,880) was more than twice as high as the price at the 10th
percentile ($11,098). In Tucson, Arizona, the median price for a vaginal delivery was much
lower, $5,920, and the range of prices was much narrower: e price at the 90th percentile
($6,735) was only 50 percent higher than the price at the 10th percentile ($4,490).
Price variation within an MSA reects price dierences among hospitals in that area as well
as price dierences within the same hospital. e latter largely reect dierences in the
amounts that dierent commercial insurers pay for the same service at a particular hospital.
Price variation within and among hospitals could also reect dierences in patients’ health or
in the intensity of a service. However, most studies that examine price variation either control
for patients’ health or focus on variation for a relatively standardized service, such as mag-
netic resonance imaging (MRI) scans.
2
Commercial Insurers’ Prices for Vaginal Deliveries at Hospitals in Selected MSAs, 2016
Dollars
Median
The price for vaginal
deliveries at the 90th
percentile was 2.2
times the price at the
10th percentile
3,823
4,490
3,991
5,638
11,098
8,862
6,735
10,376
15,945
23,880
Kansas City, MO−KS Tucson, AZ Miami, FL Los Angeles, CA San Francisco, CA
2.8
2.6
1.5
2.3
Commercial insurers’
prices for the same hospital
service, such as a vaginal
birth, varied substantially
in 2016 within the same
geographic area. The extent
of the range of prices varied
among areas. (Source:
CBO’s analysis of data
fromKennedy and others,
2019.)

16 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Prices for Physicians’ Services:
VariationWithinMetropolitanAreas
Recent analyses have found that commercial insurers’ prices for a given physicians’ service
varied widely among providers in the same metropolitan statistical area. For instance, CBO’s
analysis of data about a specic type of colonoscopy (Current Procedural Terminology code
45385) found a roughly twofold variation in commercial insurers’ prices for that service
within ve MSAs in 2014.
3
In the Chicago-Naperville-Elgin area of Illinois, for example, the
price for that procedure for the provider at the 90th percentile of the distribution of pro-
viders by price ($660) was twice as high as the price for the provider at the 10th percentile
($330).
CBO found similar variation in prices within MSAs for all 20 of the physicians’ services that
it examined—including fairly standardized and narrowly dened services, such as echocar-
diograms and MRIs. For instance, in more than 85 percent of the 218 MSAs included in
CBO’s analysis, the price for a cranial MRI for the provider at the 90th percentile was more
than 1.5 times the price for the provider at the 10th percentile.
Commercial Insurers’ Prices for Colonoscopies Performed by Providers in Selected MSAs, 2014
Dollars
The price of the 90th
percentile provider
was 2.8 times the
price of the 10th
percentile provider
2.1
2.3
1.7
2.0
330
302
361
219
265
660
524
830
460
740
Chicago−
Naperville−Elgin,
IL−IN−WI
Cincinnati,
OH−KY−IN
Dallas−
Fort Worth−
Arlington, TX
Miami−
Fort Lauderdale−
West Palm Beach, FL
New York−Newark−
Jersey City,
NY−NJ−PA
Commercial insurers’
prices for the same
physicians’ service, such
as a colonoscopy, varied
substantially among
dierent providers in the
same geographic area
in 2014. (Source: CBO’s
analysis of data from
Pelech, 2018.)
1. ose adjustments include changes to Medicare’s base-payment rates for such things as an area’s wages and
other input prices as well as certain hospitals’ spending on graduate medical education or their share of
patient days that are for low-income patients.
2. See Daria Pelech, An Analysis of Private-Sector Prices for Physicians’ Services, Working Paper 2018-01
(Congressional Budget Oce, January 2018), www.cbo.gov/publication/53441; and Zack Cooper and
others, “e Price Ain’t Right? Hospital Prices and Health Spending on the Privately Insured,” Quarterly
Journal of Economics, vol. 134, no. 1 (February 2019), pp. 51–107, https://doi.org/10.1093/qje/qjy020.
3. To ease interpretation, CBO converted the ratios of commercial insurers’ prices to Medicare FFS’s prices from
that analysis to prices in dollars by multiplying those ratios by the national median price for a given service.

Chapter 4: Factors Aecting the Prices
Paid by Commercial Insurers
is chapter describes possible reasons that commercial insurers’ prices for hospitals’ and physicians’ services are
higher and more variable than the prices paid by Medicare’s fee-for-service program. Potential explanations include
market concentration for hospitals and physicians, the prices of various inputs for care, the quality of care, providers’
administrative spending, and their possible cost shifting from public to private payers.
Market Power and Commercial Insurers’ Prices
Market power is the ability of rms to raise prices above the level that would exist in a per-
fectly competitive market. It occurs for many reasons. Hospitals and physicians’ groups may
have market power because they have a dominant share of a particular market or because
an insurer sees them as essential to its network of providers. Being seen as essential can give
providers substantial leverage in price negotiations with insurers. us, prices may vary among
areas because of dierences in the relative market power of providers and insurers in each area.
Dierences in market power can also contribute to price variation within a geographic area.
Prices may vary among providers because of dierences in providers’ and insurers’ relative bar-
gaining power, or they may vary within a hospital or physicians’ group because of dierences
in insurers’ bargaining power. One study found that, within the same provider group, nego-
tiated prices for physicians’ oce visits were 21 percent lower, on average, for insurers with a
market share of at least 15 percent than for insurers with a market share of 5 percent or less.
1
Market concentration (the extent to which only a few rms provide a large share of the goods
or services in a market) can confer market power to rms with larger market shares. Evidence
suggests that concentration in the markets for hospitals’ and physicians’ services has been
growing and that, in many areas, those markets are now moderately or highly concentrated.
e percentage of physicians’ practices that are owned by or aliated with hospitals has also
increased. Such vertical integration can increase concentration in the market for physicians’
services (by consolidating physicians into larger groups) and can increase hospitals’ mar-
ket power (by steering physicians’ referrals to the acquiring hospital). In addition, evidence
suggests that a growing number of health care providers have been acquired by private equity
rms, which may leverage providers’ market power to raise prices.
Most of the studies that the Congressional Budget Oce reviewed (see Appendix C) suggest
that consolidation increases prices in the markets for both hospitals and physicians, as does
vertical integration among hospitals and physicians’ groups. ere is also a well-documented
correlation, across many areas, between concentration in the provider market and prices,
suggesting that some of the dierence in prices in dierent areas is attributable to providers’
market power.
2
Most studies focus on market share as a measure of providers’ market power,
but there is growing evidence that providers can also derive market power from providing spe-
cialized services, high-quality services, or services that a patient cannot shop for in advance.
3
18 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
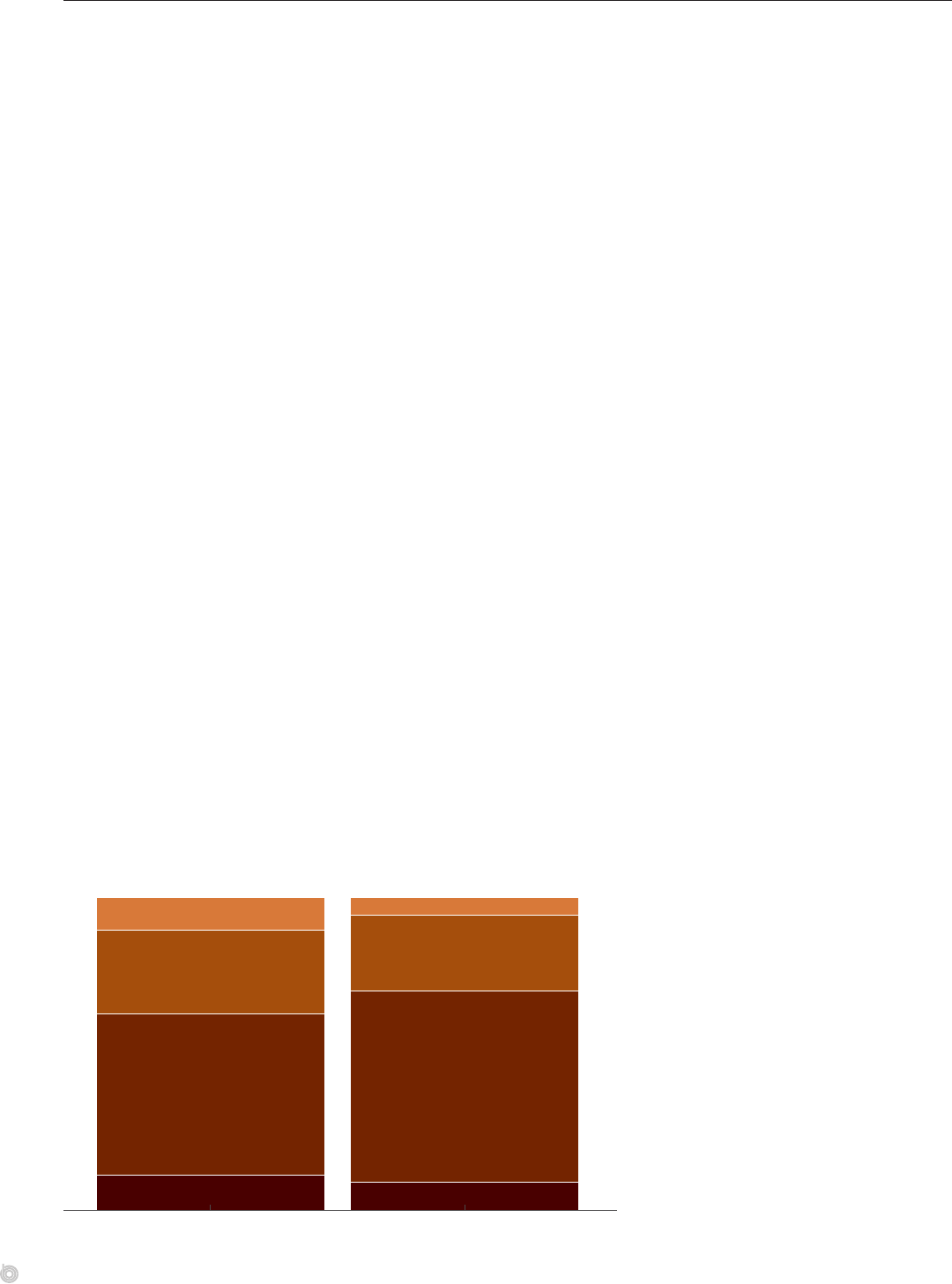
Concentration in Hospital Markets and Commercial Insurers’ Prices
CBO analyzed data from the Health Care Cost Institute for hospital markets in 42 states
and found that the percentage of metropolitan statistical areas with hospital markets that
were considered highly or very highly concentrated rose between 2010 and 2017. In 2010,
63percent of the 124 MSAs in the HCCI data had highly or very highly concentrated hospi-
tal markets. By 2017, that share had risen to 70 percent. (e MSAs that HCCI included in
that sample were selected on the basis of population, insurance coverage, and number of hos-
pitals.) Over that period, the average Herndahl-Hirschman index (HHI) for the MSAs in
that sample rose from 3,032, already in the “highly concentrated” range, to 3,338. (e HHI
is a common measure of market concentration; it indicates the extent to which a market is
dominated by one or a few participants.)
Greater market concentration has been linked to less price competition. CBO reviewed
13studies published since 2010 on the relationship between hospital market concentration
and prices for hospitals’ services (see Table C-1 in Appendix C). Of the four studies that
tested for correlations, three found a positive association between market concentration and
hospitals’ prices. Mergers between hospitals have also increased concentration and typically
led to higher prices. Of the ve studies that examined hospital mergers within a market, three
concluded that prices rose for insurers. (e other two studies showed price increases for
some insurers and decreases for others.) ere is also some recent evidence that mergers of
hospitals in dierent markets may result in price increases.
CBO focused on the research literature since 2010 because high-quality data on prices have
become more readily available since then. But a review of older studies also found a positive
association between market concentration and prices for hospitals’ services.
4
It also found
some evidence that growth in those prices is related to market concentration and that hospi-
tal mergers in concentrated markets typically result in much higher prices.
CBO also reviewed studies on the relationship between mergers and eciency gains for
hospitals.
5
e evidence about the relationship between mergers and hospitals’ costs is
inconsistent; some studies found that acquired hospitals have lower costs after their merger.
But lower costs do not necessarily translate into lower prices for hospitals’ services if hospitals
do not pass those eciency gains on to consumers.
Hospital Market Concentration, 2010 and 2017
Percentage of MSAs
10
6
27
24
52
61
11
9
2010 2017
Very Highly Concentrated
(HHI greater than 5,000)
Highly Concentrated
(HHI 2,501–5,000)
Moderately Concentrated
(HHI 1,500–2,500)
Competitive
(HHI less than 1,500)
The percentage of
metropolitan areas with
hospital markets that
were highly or very highly
concentrated (as measured
by a Herfindahl-Hirschman
Index of more than 2,500)
increased from 2010
to 2017. (Source: CBO’s
analysis of data from HCCI.)
19CHAPTER 4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Concentration in Physician Markets and Commercial Insurers’ Prices
Market concentration for physicians increased between 2010 and 2016, as measured by the
average of the Herndahl-Hirschman indexes for more than 370 metropolitan statistical
areas. During that period, the average HHI rose by nearly 29 percent for primary care phy-
sicians and by about 5 percent for four common types of specialist physicians (cardiologists,
oncologists or hematologists, radiologists, and orthopedists).
6
In addition, the percentage of
MSAs whose markets for primary care physicians were considered highly or very highly con-
centrated (an HHI of more than 2,500) increased from 20 percent in 2010 to 39 percent in
2016. Increases in market concentration were at least partly attributable to a rise in the share
of physicians employed by hospitals or hospital systems.
CBO reviewed eight studies on the relationship between market concentration for physicians
and prices for physicians’ services; all of the studies found that prices were related to market
structure in some way (see Table C-2 in Appendix C). Prices for most services were generally
higher in areas with more-concentrated physician markets, or increased more in areas with
higher initial levels of market concentration, or rose after mergers or acquisitions of physi-
cians’ practices. In addition, one of the studies found that an increase in the enforceability of
noncompete agreements for physicians (which make it harder for physicians to nd new
employment after leaving a practice) led to greater concentration among physicians’ groups
and higher prices.
Average Herfindahl-Hirschman Indexes for Primary Care and Specialist Physicians in Metropolitan
Statistical Areas, 2010 to 2016
Specialist Physicians
Primary Care Physicians
1,819
3,228
2,343
3,397
0
500
1,000
1,500
2,000
2,500
3,000
3,500
2010 2011 2012 2013 2014 2015 2016
Concentration in the
markets for specialist and
primary care physicians
has grown since 2010. An
HHI of 1,500 to 2,500 is
considered moderately
concentrated, and an
HHI of 2,501 to 5,000
is considered highly
concentrated. (Source:
CBO based on Exhibit 1 in
Fulton,2017.)
20 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
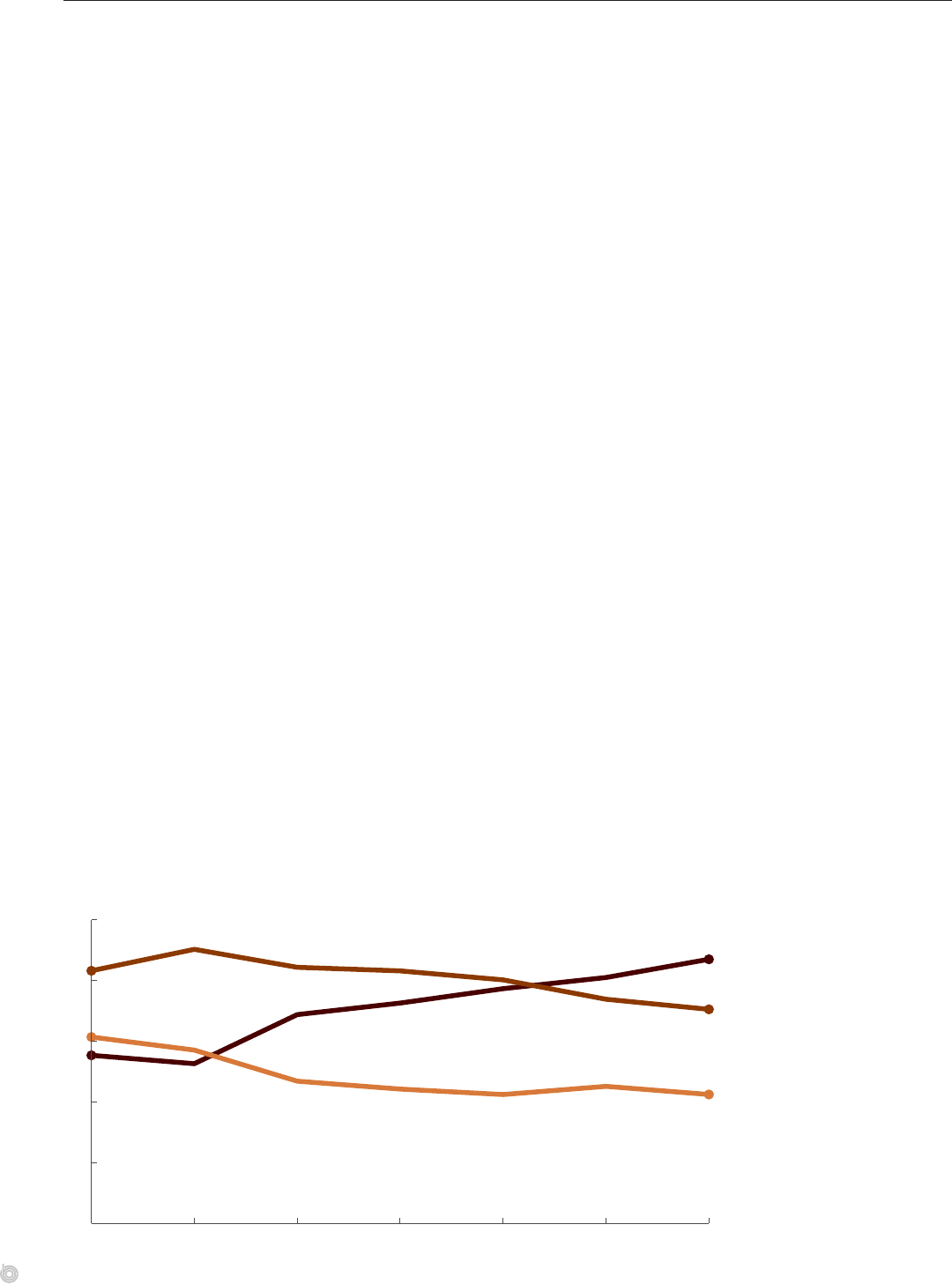
Employment of Physicians by Health Care Systems
Over the 2010–2016 period, the share of primary care physicians employed by a hospital
or health care system rose by 16 percentage points, from 28 percent to 44 percent.
7
At the
same time, the share of primary care physicians who were in a solo practice or were part of a
medical group declined. e trend of hospitals’ employing physicians may stem in part from
the fact that Medicare and many commercial insurers have tended to pay higher prices when
a service is billed in a hospital’s outpatient department rather than in a physician’s oce.
8
Physicians may also want to join larger, integrated practices to have more exible work
schedules, lower practice expenses per physician, access to expensive information technology
systems, or discounts on drugs they purchase for outpatient care.
Hospitals’ acquisitions of physicians’ practices have been found to result in greater use of
electronic health records and care management processes. Such acquisitions can also increase
hospitals’ market power in at least two ways. First, they increase the amount of care billed in
facilities owned by hospitals and reduce the amount billed in physicians’ oces. Second, they
lessen the ability of rival hospitals to refer patients to the acquired physicians’ practices and
increase the frequency of referrals within systems.
9
Such acquisitions can also increase market
concentration among physicians by consolidating them into larger groups.
CBO reviewed seven studies about whether vertical integration of providers relates to prices
for their services (see Table C-3 in Appendix C). Four of the studies looked at the relation-
ship between hospital-physician integration and prices for physicians’ services. All four
found that prices increased more in areas where vertical integration increased or that prices
rose after physicians’ practices were acquired by hospitals. (According to one of the studies,
almost half of those price increases were potentially attributable to the services’ being billed
as services provided in a facility and thus incurring a higher total fee.)
10
Another study looked
at integration between physicians of dierent specialties and found that prices for physicians’
services rose more in areas where that type of integration increased.
ree of the studies in CBO’s review examined the relationship between hospital-physician
integration and prices for hospitals’ services. Two found a signicant positive association
between increases in integration and hospitals’ prices. e other study’s ndings were incon-
clusive. (Although two of those studies used similar data sources, the three diered in their
time periods, measures of vertical integration, and methods.)
Share of Primary Care Physicians, by Ownership of Their Practice, 2010 to 2016
Percent
43.5
35.3
21.2
0
10
20
30
40
50
2010 2011 2012 2013 2014 2015 2016
Independent Solo Practice
Hospital or Health Care System
Medical Group
27.7
30.7
41.6
The percentage of primary
care physicians working
in a practice owned by
a hospital or health care
system rose during the
2010–2016 period. (Source:
CBO based on Exhibit 4 in
Fulton, 2017.)
21CHAPTER 4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
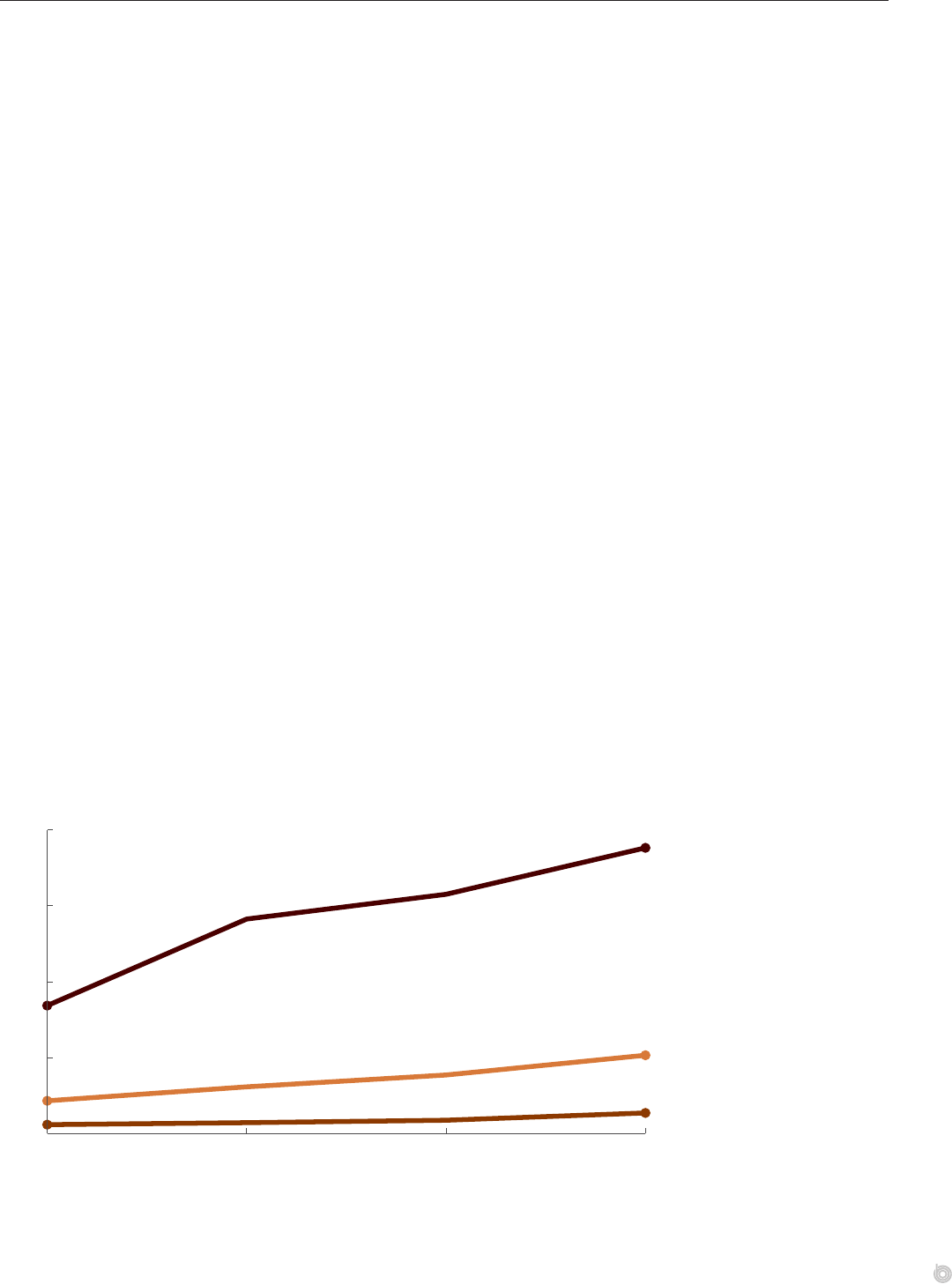
Acquisition of Health Care Providers by Private Equity Firms
In recent decades, some physicians’ practices and hospitals have been bought by private
equity rms (companies that purchase and take over other companies to generate short-term
prots for their investors). Several recent studies have documented the volume of such acqui-
sitions. According to one study, only about 2 percent of physicians’ practices were acquired
by private equity rms between 2013 and 2016, but such acquisitions more than doubled
in frequency during that period.
11
Anesthesiologists, emergency medicine specialists, family
practitioners, and dermatologists were the most common types of physicians in acquired
practices. Another study found that roughly 7 percent of short-term acute care hospitals,
responsible for 11 percent of total patient discharges, were acquired by private-equity-backed
ventures between 2003 and 2017.
12
More than half of those acquisitions (161) occurred
in 2006, when Bain Capital purchased Hospital Corporation of America. (HCA became
publiclytraded again in 2011.)
Evidence about the eects on prices when private equity rms acquire medical providers has
been mostly anecdotal, until recently. A recent study found that after private equity rms
acquired hospitals, the ratio of those hospitals’ charges to costs rose by 7 percent overall, and
by 16 percent in emergency rooms, relative to otherwise-similar hospitals not bought by pri-
vate equity rms.
13
(Hospitals’ charges dier from the negotiated prices paid by commercial
insurers. But they are often correlated with those prices because, in some contracts, negoti-
ated prices are dened as a percentage of a hospital’s charges.)
For physicians and other providers, another study found that after a private equity rm that
employed emergency physicians entered into contracts with hospitals, the percentage of
emergency care billed out of network at those hospitals rose by 83 percentage points, and the
prices paid to those emergency physicians rose by 114 percent.
14
A recent study of dermatol-
ogists found that among practices acquired by private equity rms, prices for a few common
services rose by 3 percent to 5 percent relative to prices at nonacquired practices, although
prices for other services were not signicantly aected.
15
In addition, a study found that air
ambulance companies owned by private equity rms charged 68percent more in 2017 than
other air ambulance companies did.
16
Number of Physicians’ Practices Acquired Each Year by Private Equity Firms, 2013 to 2016
136
516
1,882
0
500
1,000
1,500
2,000
2013 2014 2015 2016
Physicians
Practice Sites
Practices
59
216
843
Private equity firms’
acquisitions of physicians’
practices grew each year
between 2013 and 2016.
(Source: CBO based on data
from Zhu and others, 2020.)
22 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
The Relationship Between Input Prices and
PricesPaidtoProviders
Commercial insurers’ prices for hospitals’ and physicians’ services are correlated with various
measures of the prices of inputs needed to deliver those services (such as providers’ wages,
rent, and malpractice insurance premiums). e strength of those relationships, however, is
sensitive to the inclusion of a few areas with particularly high measures of input prices.
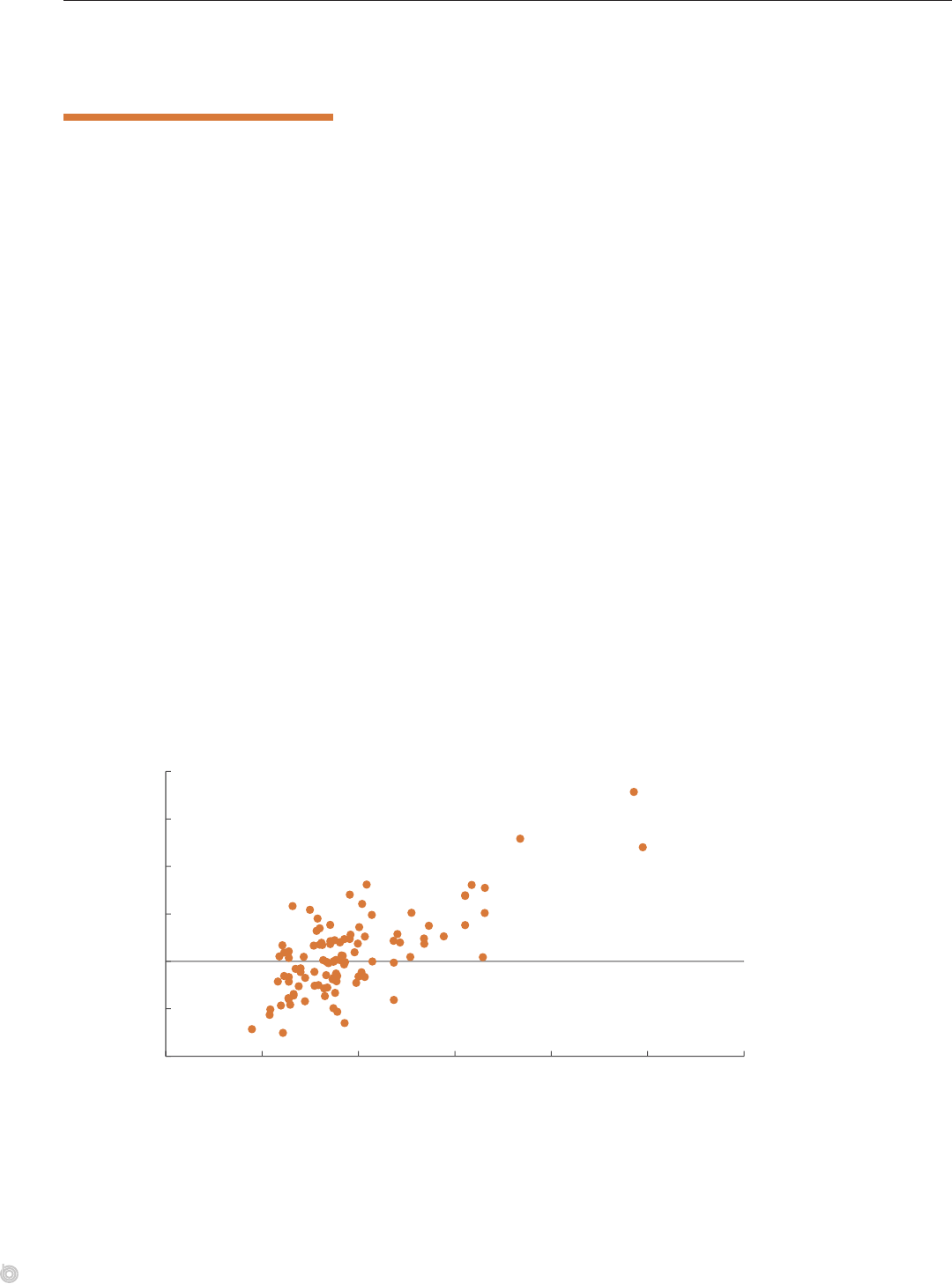
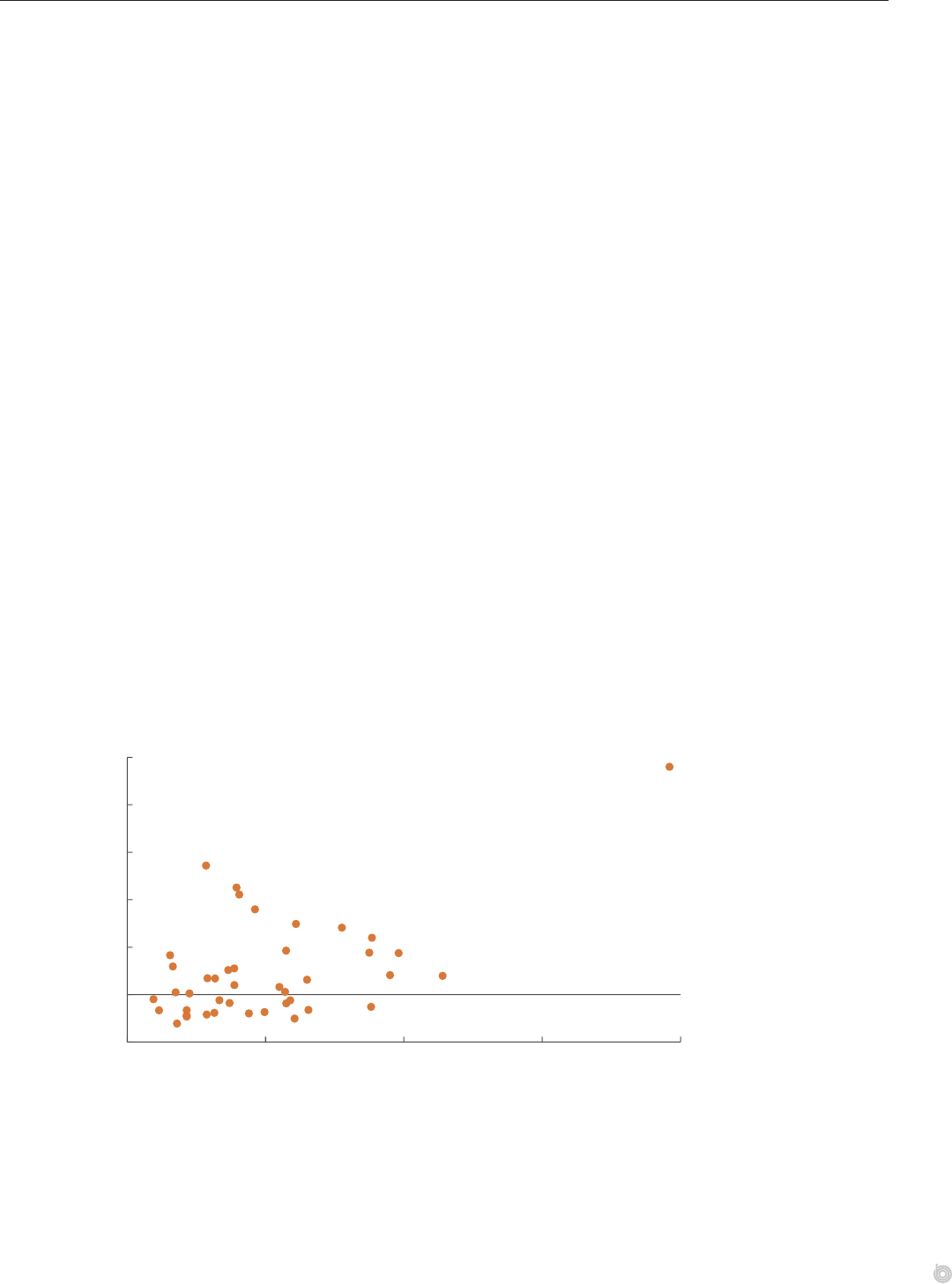
Hospitals’ Wages and Commercial Insurers’ Prices
Plotting an index of commercial insurers’ prices for hospitals’ inpatient services in a given
area against an index of hospitals’ wages in that area in 2017 shows a positive relation-
ship between wages and prices across 105 geographic areas. Of the variation in average
prices among those areas, 51 percent is explained by wages. at share falls to 33 percent
if the three outlier areas (Anchorage, Alaska; and San Francisco and San Jose, California)
areremoved.
In this analysis, the geographic areas are a subset of the nation’s core-based statistical areas
(CBSAs), which consist of metropolitan statistical areas and other areas with smaller popula-
tions, known as micropolitan statistical areas. Commercial insurers’ prices for inpatient
services are measured by a commercial price index, which represents the average price for a
basket of common services if people in each CBSA used services in the same proportions seen
at the national level. at index captures the percentage deviation from the national median
price paid by commercial insurers. Hospitals’ wages are measured by Medicare’s hospital wage
index. Medicare uses that index to adjust its prices for inpatient services to account for
geographic dierences in the wages that hospitals face in their local labor markets. Although
wages are a large part of hospitals’ input costs, Medicare adjusts its prices for other character-
istics of hospitals as well, such as whether they operate medical education programs or serve a
disproportionate share of low-income patients.
Relationship Between Hospitals’ Wages and Commercial Insurers’ Prices for Inpatient Services, 2017
-0.50
-0.25
0
0.25
0.50
0.75
1.00
0.50 0.75 1.00 1.25 1.50 1.75 2.00
Hospital Wage Index
Price
Index
Anchorage, AK
San Francisco, CA
San Jose, CA
Variation in the prices that
commercial insurers pay
for hospitals’ inpatient
services is associated
with variation in hospitals’
wages. (Source: CBO’s
analysis of aggregate
data from HCCI and the
Centers for Medicare &
MedicaidServices.)
23CHAPTER 4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Physicians’ Input Prices and Commercial Insurers’ Prices
Plotting an index of commercial insurers’ average prices for physicians’ services in each of
42states in 2017 against an index of average input prices for physicians’ services in those
states shows a positive relationship between input prices and the prices that commercial
insurers pay for physicians’ services. Dierences in input prices explain 27 percent of the
variation in commercial insurers’ prices among those states (the states for which the price
index that CBO used was available). However, that relationship is sensitive to the inclusion
of Alaska, which has high input prices. With Alaska excluded, only 3 percent of the variation
in commercial insurers’ prices is explained by dierences in input prices.
In this analysis, commercial insurers’ prices for physicians’ services are measured as the
state-level average commercial price index for a basket of 500 common physicians’ services
in 2017. As in the earlier discussion of how prices for physicians’ services vary by state, the
500 services included in that index reect the service codes most often seen in aggregate data
from HCCI’s database of claims by employment-based plans.
To measure input prices for physicians’ services, CBO used Medicare’s geographic adjustment
factor (GAF) as a proxy index for a state’s average input price for such services. at adjust-
ment factor accounts for geographic dierences in the prices of three inputs necessary for
delivering medical services: physicians’ wages (based on geographic dierences in the wages
of other professionals, such as architects, pharmacists, and computer scientists), practice
expenses (such as wages for administrative and clinical sta and rent), and malpractice
insurance premiums. For states with multiple geographic adjustment factors, CBO created a
state-level GAF by calculating a population-weighted average of the state’s factors. In addi-
tion, the Centers for Medicare & Medicaid Services (CMS) makes a number of legislatively
determined adjustments to the parts of the GAF that deal with physicians’ wages and practice
expenses, which aect the relationship between that measure and relative input prices.
Relationship Between Physicians’ Input Prices and Commercial Insurers’ Prices for
Physicians’Services, 2017
-0.2
0
0.2
0.4
0.6
0.8
1.0
0.9 1.0 1.1 1.2 1.3
Input Price Index (Measured by the GAF)
Physician
Price Index
Alaska
Variation in the prices that
commercial insurers pay
for physicians’ services is
associated with variation
in physicians’ estimated
input prices. (Source: CBO’s
analysis of aggregate data
from Johnson and others,
2020, and CMS.)
24 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
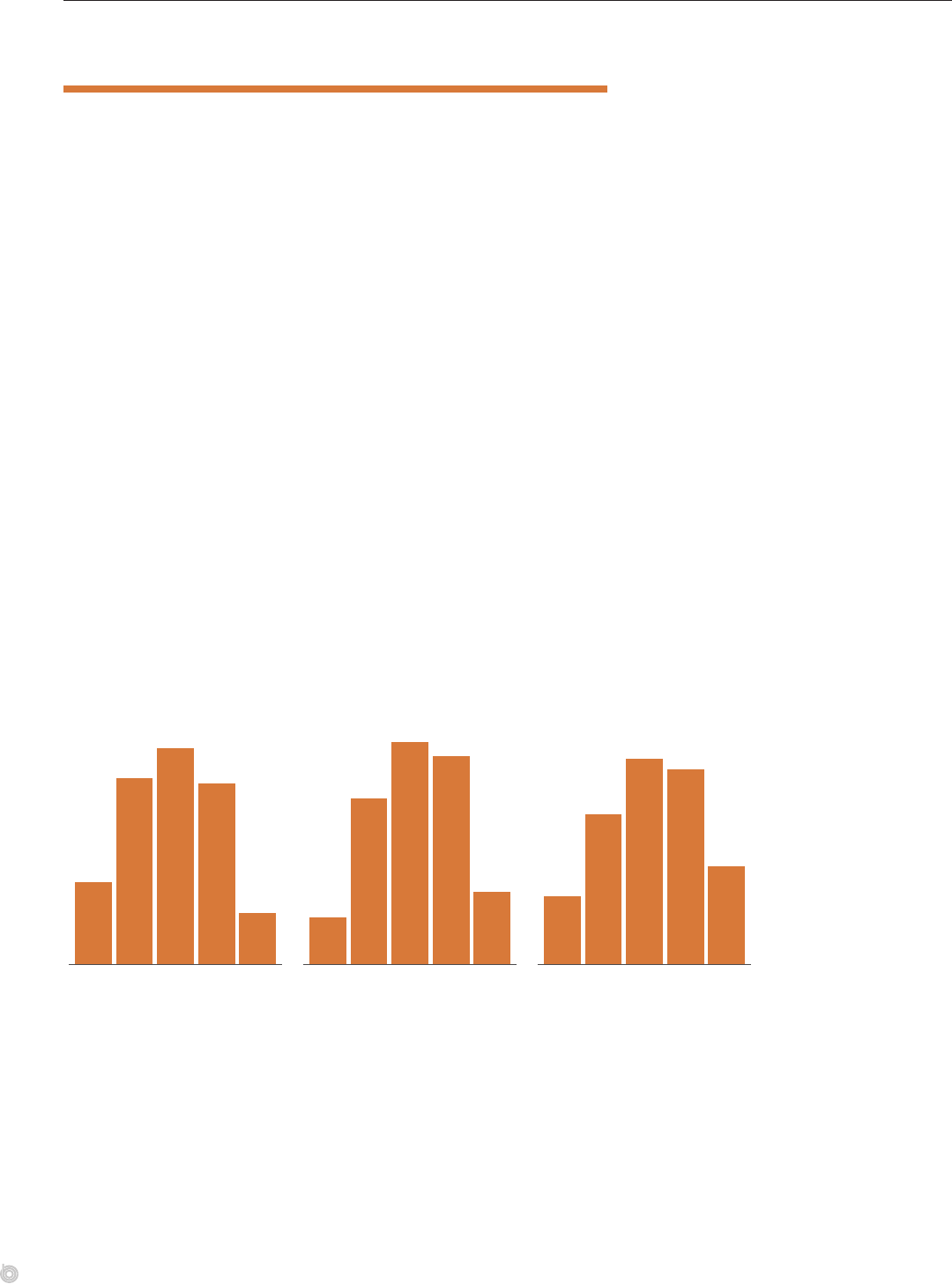
Quality of Care and Commercial Insurers’ Prices
Analyzing 2016–2018 pricing data from RAND and 2018 quality information from CMS
for more than 1,500 hospitals, CBO found a small positive correlation between the average
prices that commercial insurers paid for hospitals’ inpatient and outpatient services, relative
to Medicare FFS’s prices, and a summary measure of hospitals’ quality. In addition, when
hospitals were ranked by commercial insurers’ prices as a percentage of Medicare’s prices,
41percent of hospitals in the top third of that ranking (those with commercial prices greater
than 276 percent of Medicare FFS’s prices) received four or ve stars on CMS’s overall qual-
ity rating, compared with 32 percent of hospitals in the bottom third of the price ranking
(those with commercial prices less than 216 percent of Medicare FFS’s prices). Even among
hospitals in the bottom third, however, more than 60 percent received a quality rating of
three or more stars.
It is unclear whether hospitals with higher quality can command higher prices from commer-
cial insurers or whether hospitals with more market power, and thus higher prices, can spend
more to improve their quality. In addition, correlations between prices and quality scores
could both be associated with some other, unmeasured factor—such as a hospital’s size or the
health of its patients—that causes the observed correlations.
In the case of physicians’ services, commercial insurers’ prices were not found to be associated
with measures of quality for those services, according to a recent research study.
17
Quality Ratings for Hospitals, by Price Group, 2018
Percentage of Hospitals
12
26
30
25
7
7
23
31
29
10
10
21
29
27
14
Bottom Third
of Commercial Insurers' Prices
(<216% FFS)
Middle Third
(216−276% FFS)
Top Third
(>276% FFS)
1 2 3 4 5 1 2 3 4 5 1 2 3 4 5
Hospital Quality Rating (Number of stars)
Hospitals in the top third
when ranked by commercial
insurers’ average prices for
inpatient and outpatient
services, relative to
Medicare FFS’s prices, were
twice as likely to receive
the highest (five-star)
quality rating from CMS
in 2018 as hospitals in
the bottom third. (Source:
CBO’s analysis of hospital-
level data from Whaley and
others, 2020.)

25CHAPTER 4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Providers’ Administrative Spending and
CommercialInsurers’Prices
Many studies have documented the signicant costs of providers’ administrative activities,
which might contribute to higher prices for their services. Administrative spending can be
divided into spending on billing- and insurance-related (BIR) activities (such as processing
claims, updating patients’ medical records, and getting prior authorization from insurers) and
spending on non-BIR activities (such as general overhead, marketing, and eorts to monitor
and improve the quality of care).
In 2018, hospitals spent a total of $101 billion on BIR activities and $148 billion on
non-BIR activities, while physicians and clinics spent $94 billion on BIR activities and
$100billion on non-BIR activities. A study of BIR spending at a major academic medical
center found that providers’ administrative spending per encounter with a patient ranged
from $20 for a primary care visit to $215 for inpatient surgery.
18
Despite providers’ substantial administrative burden, the eect of that burden on prices for
providers’ services is unclear. Providers may pass the costs of their administrative activities on
to commercial insurers, but the relationship between administrative spending and prices has
not been documented by research studies.
Estimates of Providers’ Administrative Spending, 2018
Billions of Dollars
94 100
101 148
194
249
Physicians and Clinics
Hospitals
Billing- and Insurance-Related Not Billing- and Insurance-Related
Hospitals, physicians,
and clinics together spent
more than $440 billion on
administrative activities in
2018. But the eect of that
spending on prices paid
by commercial insurers
is unclear. (Source: CBO
based on Box Figure 1 from
Cutler, 2020.)
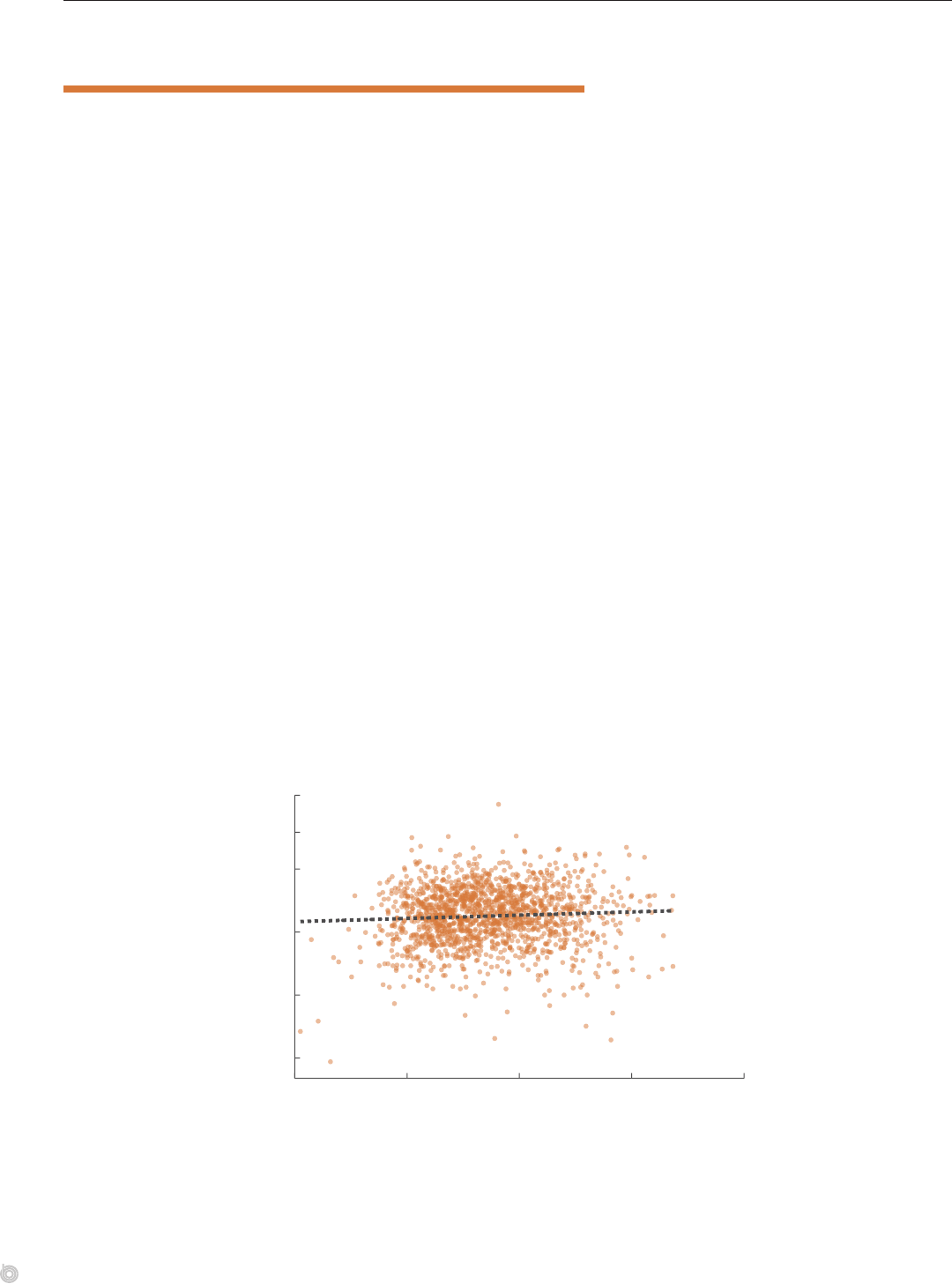
26 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Cost Shifting and Commercial Insurers’ Prices
Some observers assert that hospitals’ costs are inexible and that hospitals have to negotiate
higher prices with commercial insurers to oset smaller payments made by Medicare and
Medicaid—a concept known as cost shifting. ere is some evidence to support that asser-
tion in specic circumstances.
19
But the preponderance of the evidence suggests that hospi-
tals do not engage in cost shifting. Moreover, the idea of cost shifting is inconsistent with
economic theory: If hospitals could charge private payers more, it is unclear why they would
do so only after payment cuts from public payers.
If hospitals were able to cost shift, then hospitals with larger shares of Medicare and Medicaid
patients (for whom prices are relatively low) would be paid relatively high prices by commer-
cial insurers. However, CBO’s analysis of data for more than 1,500 hospitals indicates a weak
cross-sectional relationship between commercial insurers’ average prices for a hospital’s inpa-
tient and outpatient services during the 2016–2018 period and the percentage of Medicare
and Medicaid patients among the hospital’s discharges. (In this analysis, the average commer-
cial price reects the sum of commercial insurers’ allowed amounts for inpatient and outpa-
tient services relative to the simulated amount that Medicare would have paid for the same
services.) Each 1 percentage-point increase in a hospital’s share of Medicare and Medicaid
discharges is associated with only a 0.1 percent increase in commercial insurers’ prices rela-
tive to Medicare’s prices. A hospital’s share of discharges paid for by Medicare or Medicaid
explains just 0.4 percent of the variation among hospitals in commercial insurers’ prices.
CBO’s analysis is descriptive, however, and does not control for the many other factors that
aect hospitals’ costs. In addition, recent evidence suggests that hospitals with larger shares of
Medicare patients are more likely to close or be acquired over time, which could increase
concentration in their market and thus lead to higher prices for commercial insurers.
20
Relationship Between a Hospital’s Share of Medicare and Medicaid Patients and Commercial
Insurers’ Average Price for Its Services Over the 2016–2018 Period
Percent
50
100
200
400
600
900
0 25 50 75 100
Medicare and Medicaid Patients as a Share of a Hospital’s Discharges
Average Commercial Price for
a Hospital’s Services Relative
to Medicare FFS’s Price
(Natural log scale)
Predicted
Commercial
Price
The average price paid
by commercial insurers
for a hospital’s inpatient
and outpatient services
combined was weakly
associated with the
hospital’s share of
discharged patients
covered by Medicare or
Medicaid. (Source: CBO’s
analysis of hospital-
level data from Whaley
and others, 2020, and
White,2018.)

27CHAPTER 4 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
1. See Eric T. Roberts, Michael E. Chernew, and J. Michael McWilliams, “Market Share Matters: Evidence of
Insurer and Provider Bargaining Over Prices,” Health Aairs, vol. 36, no. 1 (January 2017), pp. 141–148,
https://doi.org/10.1377/hltha.2016.0479. Prices can also vary because of a patient’s health or the intensity
of services. However, most studies either adjust for variation in health status or focus on narrowly dened and
fairly standardized services, such as MRIs.
2. A study published in 2019 found that hospital market concentration was the strongest predictor of variation
in prices among hospitals, after controlling for patients’ health, measures of hospitals’ quality, the Medicare
base-payment rate (which reects some variation in hospitals’ input costs), and other characteristics of
hospitals, insurers, and counties. See Zack Cooper and others, “e Price Ain’t Right? Hospital Prices and
Health Spending on the Privately Insured,” Quarterly Journal of Economics, vol. 134, no. 1 (February 2019),
pp. 51–107, https://doi.org/10.1093/qje/qjy020.
3. For instance, hospitals with strong reputations have been shown to command high prices in competitive
markets, as do providers that insurers cannot credibly threaten to exclude from their networks, such as
anesthesiologists, emergency room physicians, and ambulance services.
4. See Martin Gaynor and Robert Town, e Impact of Hospital Consolidation—Update (Robert Wood Johnson
Foundation, June 2012), https://tinyurl.com/n8k8kft. at report updated an earlier study: William B. Vogt
and Robert Town, How Has Hospital Consolidation Aected the Price and Quality of Hospital Care? Research
Synthesis Report No. 9 (Robert Wood Johnson Foundation, February 2006), https://tinyurl.com/y4xjnuue.
5. For a review of that literature, see Hannah T. Neprash and J. Michael McWilliams, “Provider Consolidation
and Potential Eciency Gains: A Review of eory and Evidence,” Antitrust Law Journal, vol. 82, no. 2
(April 2019), pp. 551–578, https://tinyurl.com/dp4zs9jp.
6. See Brent D. Fulton, “Health Care Market Concentration Trends in the United States: Evidence and Policy
Responses,” Health Aairs, vol. 36, no. 9 (September 2017), pp. 1530–1538, https://doi.org/10.1377/
hltha.2017.0556.
7. Ibid.
8. See David Dranove and Christopher Ody, “Employed for Higher Pay? How Medicare Payment Rules
Aect Hospital Employment of Physicians,”American Economic Journal: Economic Policy,vol. 11, no. 4
(November2019), pp. 249–271, https://tinyurl.com/22j9r2y9; and Brady Post and others. “Hospital‐
Physician Integration and Medicare’s Site‐Based Outpatient Payments,” Health Services Research, vol. 56,
no.1 (February 2021), pp. 7–15, https://doi.org/10.1111/1475-6773.13613.
9. See Brent D. Fulton, “Health Care Market Concentration Trends in the United States: Evidence and Policy
Responses,” Health Aairs, vol. 36, no. 9 (September 2017), pp. 1530–1538, https://doi.org/10.1377/
hltha.2017.0556.
10. See Cory Capps, David Dranove, and Christopher Ody, “e Eect of Hospital Acquisitions of Physician
Practices on Prices and Spending,” Journal of Health Economics, vol. 59 (May 2018), pp. 139–152,
https://doi.org/10.1016/j.jhealeco.2018.04.001.
11. See Jane M. Zhu, Lynn M. Hua, and Daniel Polsky, “Private Equity Acquisitions of Physician Medical
Groups Across Specialties, 2013–2016,” JAMA, vol. 323, no. 7 (February 18, 2020), pp. 663–665,
https://doi.org/10.1001/jama.2019.21844.
12. See Anaeze C. Oodile II and others, “Private Equity Investments in Health Care: An Overview of Hospital
and Health System Leveraged Buyouts, 2003–17,” Health Aairs, vol. 40, no. 5 (May 2021), pp. 719–726,
https://doi.org/10.1377/hltha.2020.01535.
13. See Joseph D. Bruch, Suhas Gondi, and Zirui Song, “Changes in Hospital Income, Use, and Quality
Associated With Private Equity Acquisition,” JAMA Internal Medicine, vol. 180, no. 11 (August 2020),
pp.1428–1435, https://doi.org/10.1001/jamainternmed.2020.3552.
14. See Zack Cooper, Fiona Scott Morton, and Nathan Shekita, “Surprise! Out-of-Network Billing for
Emergency Care in the United States,” Journal of Political Economy, vol. 128, no. 9 (September 2020),
pp.3626–3677, https://doi.org/10.1086/708819.

28 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
15. See Robert Tyler Braun and others, “Private Equity in Dermatology: Eect on Price, Utilization,
and Spending,” Health Aairs, vol. 40, no. 5 (May 2021), pp. 727–735, https://doi.org/10.1377/
hltha.2020.02062.
16. See Loren Adler, Kathleen Hannick, and Sobin Lee, “High Air Ambulance Charges Concentrated in
Private Equity-Owned Carriers” (USC-Brookings Schaeer Initiative for Health Policy, October 13, 2020),
https://tinyurl.com/yhd6vuzu.
17. See Mark A. Unruh and others, “Physician Prices and the Cost and Quality of Care for Commercially
Insured Patients,” Health Aairs, vol. 39, no. 5 (May 2020), pp. 800–808, https://doi.org/10.1377/
hltha.2019.00237.
18. See Phillip Tseng and others, “Administrative Costs Associated With Physician Billing and Insurance-Related
Activities at an Academic Health Care System,” JAMA, vol. 319, no. 7 (February 20, 2018), pp. 691–697,
https://doi.org/10.1001/jama.2017.19148.
19. See Michael Darden, Ian McCarthy, and Eric Barrette, Who Pays in Pay for Performance? Evidence
From Hospital Pricing, Working Paper 24304 (National Bureau of Economic Research, August 2019),
www.nber.org/papers/w24304; and Austin Frakt, “Hospitals Don’t Shift Costs From Medicare or Medicaid to
Private Insurers,” JAMA Forum (January 4, 2017), https://tinyurl.com/me8b77f7.
20. See Michael E. Chernew and others, “Public Payment Rates for Hospitals and the Potential for
Consolidation-Induced Cost Shifting,” Health Aairs, vol. 40, no. 8 (August 2021), pp. 1277–1285,
https://doi.org/10.1377/hltha.2021.00201.

Appendix A: Data Sources for Figures
Chapter 1: Levels of and Trends in Spending and Prices
Average Annual Growth Rates of Spending, Utilization, and Prices for
Hospitals’ and Physicians’ Services, 2013 to 2018
Data sources: Growth rates for Medicare’s fee-for-service (FFS) program reect the
Congressional Budget Oce’s analysis of information from Medicare Payment Advisory
Commission, A Data Book: Health Care Spending and the Medicare Program (July 2020),
Section 1; Boards of Trustees of the Medicare Trust Funds, 2020 Annual Report of the Boards
of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust
Funds (April 2020), https://tinyurl.com/mb9666c8 (PDF, 2.7 MB); and other, miscellaneous
sources.
Growth rates for commercial insurers reect CBO’s analysis of aggregate data from Health
Care Cost Institute, 2017 Health Care Cost and Utilization Report (February 2019),
https://tinyurl.com/82jksnn3, and 2018 Health Care Cost and Utilization Report (February
2020), https://tinyurl.com/27v534jv.
CBO estimated total spending for Medicare FFS and for commercial insurers by summing
per-person spending on inpatient, outpatient, and physicians’ services but excluding spend-
ing on prescription drugs, home health care, and other types of care. In this analysis, com-
mercial insurers’ spending per patient reects the payments that insurers negotiated with
providers and excludes patients’ cost sharing.
Studies’ Estimates of Commercial Insurers’ Prices for Hospitals’ Services as a
Percentage of MedicareFFS’s Prices
Data sources: Sources are listed in Appendix B.
Studies’ Estimates of Commercial Insurers’ Prices for Physicians’ Services as a
Percentage of Medicare FFS’s Prices
Data sources: Sources are listed in Appendix B.
Payment-to-Cost Ratios for Hospitals, 2000 to 2018
Data source: CBO’s analysis of aggregate national-level data from American Hospital
Association, Trendwatch Chartbook 2020, Appendix 4, Table 4.4, https://tinyurl.com/
em4rjw9z (PDF, 3.6 MB).
Chapter 3: Variation in Prices Among and Within
GeographicAreas
Average Prices for Hospitals’ Inpatient Services, by State, 2018
Data source: CBO’s analysis of aggregate data from Christopher M. Whaley and
others, Nationwide Evaluation of Health Care Paid by Private Plans: Findings From
Round 3 of an Employer-Led Transparency Initiative, RR-4394-RWJ (RAND, 2020),
https://doi.org/10.7249/RR4394.

30 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Average Prices for Physicians’ Services, by State, 2017
Data source: CBO’s analysis of aggregate data from Bill Johnson and others, “Comparing
Commercial and Medicare Professional Service Prices: Public Use File” (Health Care Cost
Institute, August 13, 2020), https://tinyurl.com/3xux3hzj.
Commercial Insurers’ Prices for Vaginal Deliveries at Hospitals in Selected
MSAs, 2016
Data source: CBO’s analysis of aggregate data from Kevin Kennedy and others, “Past the
Price Index: Exploring Actual Prices Paid for Specic Services by Metro Area” (Health Care
Cost Institute, April 30, 2019), https://tinyurl.com/ap25xhr8.
Commercial Insurers’ Prices for Colonoscopies Performed by Providers in
Selected MSAs, 2014
Data source: CBO’s analysis of data from Daria Pelech, An Analysis of Private-Sector Prices for
Physicians’ Services, Working Paper 2018-01 (Congressional Budget Oce, January 2018),
www.cbo.gov/publication/53441.
Chapter 4: Factors Aecting the Prices Paid by
CommercialInsurers
Hospital Market Concentration, 2010 and 2017
Data source: CBO’s analysis of aggregate data from Health Care Cost Institute, “Healthy
Marketplace Index” (accessed December 2020), https://tinyurl.com/u86tw3x9.
Average Herfindahl-Hirschman Indexes for Primary Care and Specialist
Physicians in Metropolitan Statistical Areas, 2010 to 2016
Data source: CBO’s reproduction of Exhibit 1 in Brent D. Fulton, “Health Care Market
Concentration Trends in the United States: Evidence and Policy Responses,” Health
Aairs, vol. 36, no. 9 (September 2017), pp. 1530–1538, https://doi.org/10.1377/
hltha.2017.0556.
Share of Primary Care Physicians, by Ownership of Their Practice, 2010 to
2016
Data source: CBO’s reproduction of Exhibit 4 in Brent D. Fulton, “Health Care Market
Concentration Trends in the United States: Evidence and Policy Responses,” Health
Aairs, vol. 36, no. 9 (September 2017), pp. 1530–1538, https://doi.org/10.1377/
hltha.2017.0556.
Number of Physicians’ Practices Acquired Each Year by Private Equity Firms,
2013 to 2016
Data source: CBO, using data from Jane M. Zhu, Lynn M. Hua, and Daniel Polsky,
“Private Equity Acquisitions of Physician Medical Groups Across Specialties, 2013–2016,”
JAMA, vol. 323, no. 7 (February 18, 2020), pp. 663–665, https://doi.org/10.1001/
jama.2019.21844.
Relationship Between Hospitals’ Wages and Commercial Insurers’ Prices for
Inpatient Services, 2017
Data sources: CBO’s analysis of aggregate data from Health Care Cost Institute, “Healthy
Marketplace Index” (accessed December 2020), https://tinyurl.com/u86tw3x9; and Centers
for Medicare & Medicaid Services, “FY 2017 Proposed Rule Tables 2 and 3 (Wage Index
Tables) (ZIP),” Table 3 (accessed May 2021), https://tinyurl.com/cukuexa8.

31APPENDIX A THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Relationship Between Physicians’ Input Prices and Commercial Insurers’
Prices for Physicians’Services, 2017
Data sources: CBO’s analysis of aggregate data from Bill Johnson and others, “Comparing
Commercial and Medicare Professional Service Prices: Public Use File” (Health Care Cost
Institute, August 13, 2020), https://tinyurl.com/3xux3hzj; and Centers for Medicare &
Medicaid Services, “CY 2017 PFS Final Rule Addenda (ZIP),” Addendum D (accessed
December 2020), https://tinyurl.com/ywftbrad.
Quality Ratings for Hospitals, by Price Group, 2018
Data source: CBO’s analysis of aggregate data from Christopher M. Whaley and
others, Nationwide Evaluation of Health Care Paid by Private Plans: Findings From
Round 3 of an Employer-Led Transparency Initiative, RR-4394-RWJ (RAND, 2020),
https://doi.org/10.7249/RR4394.
Estimates of Providers’ Administrative Spending, 2018
Data source: CBO’s reproduction of Box Figure 1 in David M. Cutler, Reducing
Administrative Costs in U.S. Health Care, Policy Proposal 2020-09 (Hamilton Project,
Brookings Institution, March 2020), https://tinyurl.com/ap9mcczh.
Relationship Between a Hospital’s Share of Medicare and Medicaid Patients
and Commercial Insurers’ Average Price for Its Services Over the 2016–2018
Period
Data sources: CBO’s analysis of aggregate data from Christopher M. Whaley and
others, Nationwide Evaluation of Health Care Paid by Private Plans: Findings From
Round 3 of an Employer-Led Transparency Initiative, RR-4394-RWJ (RAND, 2020),
https://doi.org/10.7249/RR4394; and Chapin White, “RAND Hospital Data: Web-Based
Tool,” TL-303 (RAND, 2018), www.rand.org/pubs/tools/TL303.html.
Appendix B: Sources of Estimated
AveragePrices for Hospitals’ and
Physicians’Services
is appendix describes the sources that underlie the gures and discussion in Chapter 1 of average prices for hospitals’
and physicians’ services. For this analysis, the Congressional Budget Oce reviewed studies that compared commercial
insurers’ prices with the Medicare fee-for-service (FFS) program’s prices and studies that reported ratios of payments
to providers’ costs for private payers (including people without insurance) and for Medicare. (Studies that looked at
data before 2005 were not included because high-quality data on prices were not commonly available at that time.)
For each major type of service, CBO calculated a simple average of the studies’ estimates (see Table B-1). e estimates
of commercial insurers’ prices as a percentage of Medicare FFS’s prices may dier among the studies because of
dierences in the locations, data sources, and time periods they examined, as well as dierences in their methods for
adjusting for the health status of patients.
Table B-1 .
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Hospitals’ Services Overall
250% Ge Bai and Gerard F. Anderson, “Market Power: Price
Variation Among Commercial Insurers for Hospital Services,”
Health Aairs, vol. 37, no. 10 (October 2018), pp. 1615–1622,
https://doi.org/10.1377/hltha.2018.0567
Financial data for hospitals from the Florida Agency
for Health Care Administration
2016
247% Christopher M. Whaley and others, Nationwide Evaluation of
Health Care Prices Paid by Private Plans: Findings From Round
3 of an Employer-Led Transparency Initiative, RR-4394-RWJ
(RAND Corporation, 2020), www.rand.org/pubs/research_reports/
RR4394.html
Data from all states except Maryland. Sources
consist of self-insured employers and commercial
health plans, as well as all-payer claims databases
from Colorado, Connecticut, Delaware, Maine, New
Hampshire, and Rhode Island.
2018
241% Chapin White and Christopher M. Whaley, Prices Paid to
Hospitals by Private Health Plans Are High Relative to
Medicare and Vary Widely: Findings From an Employer-Led
Transparency Initiative, RR-3033-RWJ (RAND Corporation, 2019),
www.rand.org/pubs/research_reports/RR3033.html
Data from 25 states. Sources consist of self-insured
employers and commercial health plans, as well as
all-payer claims databases from Colorado and New
Hampshire.
2017
209% Richard Kronick and Sarah Hoda Neyaz, Private Insurance
Payments to California Hospitals Average More Than Double
Medicare Payments (West Health Policy Center, May 2019),
https://tinyurl.com/yb7kyxj6
Annual nancial disclosure reports led with the
California Oce of Statewide Health Planning and
Development
2015–
2016
167% American Hospital Association, Trendwatch Chartbook 2020
(accessed November 2020), Table 4.4, https://tinyurl.com/
em4rjw9z (PDF, 3.6MB)
Payment-to-cost ratios from all 50 states 2018
223% Simple Average for Hospitals’ Services Overall
Continued
34 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Hospitals’ Outpatient Services
293% Chapin White and Christopher M. Whaley, Prices Paid to
Hospitals by Private Health Plans Are High Relative to
Medicare and Vary Widely: Findings From an Employer-Led
Transparency Initiative, RR-3033-RWJ (RAND Corporation, 2019),
www.rand.org/pubs/research_reports/RR3033.html
Data from 25 states. Sources consist of self-insured
employers and commercial health plans, as well as
all-payer claims databases from Colorado and New
Hampshire.
2017
280% Paul B. Ginsburg, Wide Variation in Hospital and Physician
Payment Rates Evidence of Provider Market Power,
Research Brief 16 (Center for Studying Health System Change,
November 2010), www.hschange.org/CONTENT/1162
Data from Aetna, Anthem Blue Cross Blue Shield,
CIGNA, and UnitedHealth Group for 8 metropolitan
areas in 6 states
2005
267% Christopher M. Whaley and others, Nationwide Evaluation of
Health Care Prices Paid by Private Plans: Findings From Round 3
of an Employer-Led Transparency Initiative, RR-4394-RWJ (RAND
Corporation, 2020), www.rand.org/pubs/research_reports/
RR4394.html
Data from all states except Maryland. Sources
consist of self-insured employers and commercial
health plans, as well as all-payer claims databases
from Colorado, Connecticut, Delaware, Maine, New
Hampshire, and Rhode Island.
2018
227% Chapin White, Amelia M. Bond, and James D. Reschovsky, High
and Varying Prices for Privately Insured Patients Underscore
Hospital Market Power, Research Brief 27 (Center for Studying
Health System Change, September 2013), https://tinyurl.com/
yztwasr9
Claims data for auto workers from 13 markets in
6states
2011
216% Michael E. Chernew, Andrew L. Hicks, and Shivana A. Shah,
“Wide State-Level Variation in Commercial Health Care Prices
Suggests Uneven Impact of Price Regulation,” Health Aairs,
vol. 39, no. 5 (May 2020), pp. 791–799, https://doi.org/10.1377/
hltha.2019.01377
IBM MarketScan commercial claims data, which cover
all 50 states
2017
155% Thomas M. Selden, “Dierences Between Public and
Private Hospital Payment Rates Narrowed, 2012–2016,”
Health Aairs, vol. 39, no. 1 (January 2020), pp. 94–99,
https://doi.org/10.1377/hltha.2019.00415
Data from the Medical Expenditure Panel Survey, a
nationally representative survey. CBO’s estimate of
the price ratio for outpatient services from this study
is a weighted average of the study’s price ratios for
outpatient and emergency services.
2016
240% Simple Average for Hospitals’ Outpatient Services
Continued
Table B-1. Continued
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services
35APPENDIX B THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Hospitals’ Inpatient Services
231% Christopher M. Whaley and others, Nationwide Evaluation of
Health Care Prices Paid by Private Plans: Findings From Round
3 of an Employer-Led Transparency Initiative, RR-4394-RWJ
(RAND Corporation, 2020), www.rand.org/pubs/research_reports/
RR4394.html
Data from all states except Maryland. Sources
consist of self-insured employers and commercial
health plans, as well as all-payer claims databases
from Colorado, Connecticut, Delaware, Maine, New
Hampshire, and Rhode Island.
2018
220% Zack Cooper and others, “The Price Ain’t Right? Hospital Prices
and Health Spending on the Privately Insured,” Quarterly Journal
of Economics, vol. 134, no. 1 (February 2019), pp. 51–107,
https://doi.org/10.1093/qje/qjy020
The authors estimated risk-adjusted prices using
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover all
50states.
2011
206% Michael E. Chernew, Andrew L. Hicks, and Shivana A. Shah, “Wide
State-Level Variation in Commercial Health Care Prices Suggests
Uneven Impact of Price Regulation,” Health Aairs, vol. 39, no. 5 (May
2020), pp. 791–799, https://doi.org/10.1377/hltha.2019.01377
IBM MarketScan commercial claims data, which cover
all 50 states
2017
204% Chapin White and Christopher M. Whaley, Prices Paid to Hospitals
by Private Health Plans Are High Relative to Medicare and Vary
Widely: Findings From an Employer-Led Transparency Initiative,
RR-3033-RWJ (RAND Corporation, 2019), www.rand.org/pubs/
research_reports/RR3033.html
Data from 25 states. Sources consist of self-insured
employers and commercial health plans, as well as
all-payer claims databases from Colorado and New
Hampshire.
2017
189% Jared Lane K. Maeda and Lyle Nelson, “How Do the
Hospital Prices Paid by Medicare Advantage Plans and
Commercial Plans Compare With Medicare Fee-for-
Service Prices?” Inquiry, vol. 55 (June 11, 2018), pp. 1–8,
https://doi.org/10.1177/0046958018779654
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover all
50states
2013
178% Paul B. Ginsburg, Wide Variation in Hospital and Physician
Payment Rates Evidence of Provider Market Power, Research
Brief 16 (Center for Studying Health System Change,
November 2010), www.hschange.org/CONTENT/1162
Data from Aetna, Anthem Blue Cross Blue Shield,
CIGNA, and UnitedHealth Group for 8 metropolitan
areas in 6 states
2005
175% Thomas M. Selden and others, “The Growing Dierence Between
Public and Private Payment Rates for Inpatient Hospital Care,”
Health Aairs, vol. 34, no. 12 (December 2015), pp. 2147–2150,
http://dx.doi.org/10.1377/hltha.2015.0706
Data from the Medical Expenditure Panel Survey, a
nationally representative survey
2012
165% Laurence C. Baker and others, “Medicare Advantage
Plans Pay Hospitals Less Than Traditional Medicare Pays,”
Health Aairs, vol. 35, no. 8 (August 2016), pp. 1444–1451,
https://doi.org/10.1377/hltha.2015.1553
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover all
50states
2012
151% Chapin White, Amelia M. Bond, and James D. Reschovsky, High and
Varying Prices for Privately Insured Patients Underscore Hospital
Market Power, Research Brief 27 (Center for Studying Health
System Change, September 2013), https://tinyurl.com/yztwasr9
Claims data for auto workers from 13 markets in
6states
2011
150% Thomas M. Selden, “Dierences Between Public and
Private Hospital Payment Rates Narrowed, 2012–2016,”
Health Aairs, vol. 39, no. 1 (January 2020), pp. 94–99,
https://doi.org/10.1377/hltha.2019.00415
Data from the Medical Expenditure Panel Survey, a
nationally representative survey
2016
137% Toren L. Fronsdal, Jay Bhattacharya, and Suzanne Tamang,
Variation in Health Care Prices Across Public and Private Payers,
Working Paper 27490 (National Bureau of Economic Research,
May 2020), www.nber.org/papers/w27490
Data from the American Hospital Utilization Database;
all-payer data from 474 hospitals in 38 states and
estimates of risk- and hospital-adjusted prices
2009–
2016
182% Simple Average for Hospitals’ Inpatient Services
Continued
Table B-1. Continued
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services
36 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Physicians’ Services Overall
163% Michael E. Chernew, Andrew L. Hicks, and Shivana A. Shah,
“Wide State-Level Variation in Commercial Health Care Prices
Suggests Uneven Impact of Price Regulation,” Health Aairs,
vol. 39, no. 5 (May 2020), pp. 791–799, https://doi.org/10.1377/
hltha.2019.01377
IBM MarketScan commercial claims data, which cover
all 50 states
2017
135% Medicare Payment Advisory Commission, “Physician and
Other Health Professional Services,” Chapter 4 in Report to
the Congress: Medicare Payment Policy (March 2020), p. 132,
https://tinyurl.com/yckkxfuy
Claims data from a large preferred provider
organization with national coverage
2018
128% Daria M. Pelech, “Prices for Physicians’ Services in Medicare
Advantage and Commercial Plans,” Medical Care Research
and Review, vol. 77, no. 3 (June 2020), pp. 236–248,
https://doi.org/10.1177/1077558718780604
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover
all 50 states. To produce an overall estimate, CBO
calculated a weighted average of prices for various
services.
2014
122% Bill Johnson and others, “Comparing Commercial and Medicare
Professional Service Prices” (Health Care Cost Institute,
August 13, 2020), https://tinyurl.com/3xux3hzj
Average prices paid by commercial insurers (including
Aetna, UnitedHealthcare, and Humana) for the 500
most commonly provided physicians’ services in
metropolitan areas in 48 states and Washington, DC.
2017
121% Erin Trish and others, “Physician Reimbursement in Medicare
Advantage Compared With Traditional Medicare and Commercial
Health Insurance,” JAMA Internal Medicine, vol. 177, no. 9
(September 2017), pp. 1287–1295, https://doi.org/10.1001/
jamainternmed.2017.2679
Using data from a large national insurer, the authors
calculated average prices relative to Medicare for
each service in each year from 2007 to 2012 and
then averaged them across years. To produce an
overall estimate, CBO calculated a weighted average
of prices for professional services.
2007–
2012
118% Adam I. Biener and Thomas M. Selden, “Public and
Private Payments for Physician Oce Visits,” Health
Aairs, vol.36, no.12 (December 2017), pp. 2160–2164,
https://doi.org/10.1377/hltha.2017.0749
Data from the Medical Expenditure Panel Survey for
enrollees in employer-sponsored plans, nongroup
marketplace plans, and Medicare. To produce an
overall estimate, CBO calculated a weighted average
of prices paid by nongroup and employer-sponsored
plans (weighted by its 2020 baseline estimates of
premiums in those two segments of the market).
2014–
2015
118% Paul B. Ginsburg, Wide Variation in Hospital and Physician
Payment Rates Evidence of Provider Market Power, Research
Brief 16 (Center for Studying Health System Change,
November 2010), www.hschange.org/CONTENT/1162
Data from Aetna, Anthem Blue Cross Blue Shield,
CIGNA, and UnitedHealth Group for 8 metropolitan
areas in 6 states
2005
129% Simple Average for Physicians’ Services Overall
Continued
Table B-1. Continued
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services
37APPENDIX B THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Primary Care Services or Oce Visits
128% Medicare Payment Advisory Commission, “Physician and
Other Health Professional Services,” Chapter 4 in Report to
the Congress: Medicare Payment Policy (March 2020), p. 132,
https://tinyurl.com/yckkxfuy
Claims data from a large preferred provider
organization with national coverage
2018
126% Adam I. Biener and Thomas M. Selden, “Public and
Private Payments for Physician Oce Visits,” Health
Aairs, vol. 36, no. 12 (December 2017), pp. 2160–2164,
https://doi.org/10.1377/hltha.2017.0749
Data from the Medical Expenditure Panel Survey for
enrollees in employer-sponsored plans, nongroup
marketplace plans, and Medicare. CBO calculated
a weighted average of prices paid by nongroup
and employer-sponsored plans (weighted by its
2020 baseline estimates of premiums in those two
segments of the market).
2014–
2015
120% Bill Johnson and others, “Comparing Commercial and Medicare
Professional Service Prices” (Health Care Cost Institute,
August 13, 2020), https://tinyurl.com/3xux3hzj
The authors published commercial insurers’ prices for
primary care services in 320 metropolitan and state
areas and compared them with what Medicare would
have paid for the same services under the Medicare
fee schedule. CBO calculated a weighted average
of prices for those services (weighted by the volume
of commercial insurers’ claims in each core-based
statistical area).
2017
107% Erin Trish and others, “Physician Reimbursement in Medicare
Advantage Compared With Traditional Medicare and Commercial
Health Insurance,” JAMA Internal Medicine, vol. 177, no. 9
(September 2017), pp. 1287–1295, https://doi.org/10.1001/
jamainternmed.2017.2679
Using data from a large national insurer, the authors
calculated average prices relative to Medicare for
each service in each year from 2007 to 2012 and
then averaged them across years.
2007–
2012
106% Daria M. Pelech, “Prices for Physicians’ Services in Medicare
Advantage and Commercial Plans,” Medical Care Research
and Review, vol. 77, no. 3 (June 2020), pp. 236–248,
https://doi.org/10.1177/1077558718780604
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover
all 50states. CBO calculated a weighted average of
prices for visits to physicians’ oces.
2014
117% Simple Average for Primary Care Services or Oce Visits
Continued
Table B-1. Continued
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services
38 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Estimate of
Commercial
Insurers’ Prices
as a Percentage
of Medicare
FFS’s Prices Source Description of Data
Data
Period
Specialty (Nonemergency) Physicians’ Services
179% Erin Trish and others, “Physician Reimbursement in Medicare
Advantage Compared With Traditional Medicare and Commercial
Health Insurance,” JAMA Internal Medicine, vol. 177, no. 9
(September 2017), pp. 1287–1295, https://doi.org/10.1001/
jamainternmed.2017.2679
Using data from a large national insurer, the authors
calculated average prices relative to Medicare for
each service in each year from 2007 to 2012 and
then averaged them across years.
2007–
2012
173% Daria M. Pelech, “Prices for Physicians’ Services in Medicare
Advantage and Commercial Plans,” Medical Care Research
and Review, vol. 77, no. 3 (June 2020), pp. 236–248,
https://doi.org/10.1177/1077558718780604
Health Care Cost Institute data, which include
Aetna, UnitedHealthcare, and Humana and cover
all 50states. CBO calculated a weighted average of
prices for various specialty services.
2014
132% Jacob Wallace and Zirui Song, “Traditional MedicareVersus
Private Insurance: How Spending, Volume, and Price Change
at Age Sixty-Five,” Health Aairs, vol. 35, no. 5 (May 2016),
pp.864–872, https://doi.org/10.1377/hltha.2015.1195
The authors used MarketScan data to estimate
prices for imaging and surgical procedures using
a regression-discontinuity exploiting the change in
spending that occurs for people aging into Medicare.
2007–
2013
120% Bill Johnson and others, “Comparing Commercial and Medicare
Professional Service Prices” (Health Care Cost Institute,
August 13, 2020), https://tinyurl.com/3xux3hzj
The authors published commercial insurers’ prices for
non-primary-care services in 320 metropolitan and
state areas and compared them with what Medicare
would have paid for the same services under the
Medicare fee schedule. CBO calculated a weighted
average of prices for those services (weighted by the
volume of commercial insurers’ claims in each core-
based statistical area).
2017
117% Adam I. Biener and Thomas M. Selden, “Public and
Private Payments for Physician Oce Visits,” Health
Aairs, vol. 36, no. 12 (December 2017), pp. 2160–2164,
https://doi.org/10.1377/hltha.2017.0749
Data from the Medical Expenditure Panel Survey for
enrollees in employer-sponsored plans, nongroup
marketplace plans, and Medicare. CBO calculated
a weighted average of prices paid by nongroup
and employer-sponsored plans (weighted by its
2020 baseline estimates of premiums in those two
segments of the market).
2014–
2015
144% Simple Average for Specialty (Nonemergency) Physicians’ Services
Table B-1. Continued
Studies Comparing Prices Paid by Commercial Insurers and the Medicare Fee-for-Service
Program for Various Hospitals’ and Physicians’ Services

Appendix C: Studies Examining
the Relationship Between Market
Concentrationfor Providers and
PricesPaidbyCommercial Insurers
is appendix describes the sources that underlie the discussion in Chapter 4 of how concentration in the markets for
hospitals’ services (see Table C-1) and physicians’ services (see Table C-2) aects prices for those providers’ services.
is appendix also describes studies that examine the relationship between prices and vertical integration of hospitals
and physicians—that is, when physicians’ practices are owned by or aliated with hospitals (see Table C-3).
40 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Table C-1 .
Studies of the Relationship Between Hospital Market Concentration and Prices
Source Data Period Experiment or Methods Findings
Eric Barrette, Gautam Gowrisankaran,
and Robert Town, “Countervailing
Market Power and Hospital
Competition,” Review of Economics
and Statistics (February 2021),
https://doi.org/10.1162/rest_a_01020
2011–2014 Estimated models of consumers’
willingness to pay (WTP) for
hospitals’ services in dierent
metropolitan areas. Using the mean
WTP of 1.26, and assuming that a
typical hospital merger increases
WTP by 14.4 percent, the authors
examined the expected price
change from hospital mergers in
areas with dierent concentrations
of insurers.
•
A typical hospital merger would increase prices
by 4.3 percent at the 25th percentile of insurer
concentration but by only 0.97 percent at the
75thpercentile of insurer concentration.
Daniel Arnold and Christopher M.
Whaley, Who Pays for Health Care
Costs? The Eects of Health Care
Prices on Wages, WR-A621-2 (RAND
Corporation, 2020), www.rand.org/
pubs/working_papers/WRA621-2.html
2010–2016 Estimated the eects on hospitals’
prices from nearly all U.S. hospital
mergers that occurred during the
2010–2016 period
•
Hospital mergers were associated with an
increase of $521 in the mean price of hospitals’
services, which is about equal to a 2.6 percent
relative increase in price.
Leemore Dafny, Kate Ho, and Robin
S. Lee, “The Price Eects of Cross-
Market Mergers: Theory and Evidence
From the Hospital Industry,” RAND
Journal of Economics, vol. 50, no.2
(Summer 2019), pp. 286–325,
https://doi.org/10.1111/
1756-2171.12270
1996–2012 Examined hospital mergers and
compared price changes for
three groups: hospitals that were
acquired by a new system in the
same state (but not in the same
market), hospitals that were
acquired by a new system in a
dierent state, and hospitals that
were neither acquired nor part of
an acquiring system
•
Hospital mergers across markets within a state
resulted in price increases of about 7 percent
to 10 percent.
•
Out-of-state hospital mergers did not result in
price increases.
Zack Cooper and others, “The Price
Ain’t Right? Hospital Prices and Health
Spending on the Privately Insured,”
Quarterly Journal of Economics,
vol. 134, no. 1 (February 2019),
pp.51–107, https://doi.org/10.1093/
qje/qjy020
2007–2011 Examined the cross-sectional
correlation between the structure
of hospital markets and prices for
hospitals’ services. Also estimated
the eects on hospitals’ prices from
nearly all U.S. hospital mergers that
occurred during the 2007–2011
period by comparing the price
changes at merged hospitals with
those at control hospitals.
•
Hospitals in monopoly markets had 12.5percent
higher prices than those in markets with at least
four hospitals.
•
Prices increased by more than 6 percent at
merged hospitals that were geographically close
(5 miles or less) but did not increase at merged
hospitals that were geographically distant (more
than 25 miles apart).
Laurence C. Baker, M. Kate
Bundorf, and Daniel P. Kessler,
“Competition in Outpatient
Procedure Markets,” Medical Care,
vol. 57, no. 1 (January 2019),
pp.36–41, https://doi.org/10.1097/
MLR.0000000000001003
2008–2012 Estimated the relationship between
prices and market concentration
for outpatient services provided by
hospitals’ outpatient departments
or ambulatory surgical centers
(ASCs)
•
Prices for outpatient services were 9.9 percent
higher in the least competitive inpatient markets
than in the most competitive markets.
•
Prices for ASC services were 7.7 percent higher
in the least competitive ASC markets than in the
most competitive markets. The number of ASCs
per capita in an area was also associated with
lower prices for hospitals’ outpatient services.
•
Competition in markets for hospitals’ outpatient
services had no statistically signicant eect
on prices for those services.
Seidu Dauda, “Hospital and Health
Insurance Markets Concentration
and Inpatient Hospital Transaction
Prices in the U.S. Health Care Market,”
Health Services Research, vol. 53,
no. 2 (April 2018), pp. 1203–1226,
https://doi.org/10.1111/
1475-6773.12706
2005–2008 Examined the eects on prices from
concentration in the markets for
hospitals and insurers
•
A 10 percent increase in hospital market
concentration resulted in a 1.4 percent to
5percent increase in prices.
•
A merger of two hospitals in a market with
ve equally sized hospitals would result in a
4.9percent to 18.4 percent increase in prices.
Continued

41APPENDIX C THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Source Data Period Experiment or Methods Findings
Matthew S. Lewis and Kevin E.
Pum, “Hospital Systems and
Bargaining Power: Evidence From
Out-of-Market Acquisitions,” RAND
Journal of Economics, vol. 48,
no. 3 (Fall 2017), pp. 579–610,
https://doi.org/10.1111/
1756-2171.12186
1998–2010 Examined price changes at
hospitals acquired by an out-of-
market health system (more than
45 miles away) relative to price
changes at control hospitals that
did not join a health system
•
Out-of-market mergers resulted in price
increases for merging hospitals as well as for
their local rivals.
•
When independent hospitals were acquired by
an out-of-market system, prices rose by about
17 percent.
Gautam Gowrisankaran, Aviv Nevo,
and Robert Town, “Mergers When
Prices Are Negotiated: Evidence From
the Hospital Industry,” American
Economic Review, vol. 105, no.1
(January 2015), pp. 172–203,
https://doi.org/10.1257/aer.20130223
2003–2006 Simulated the eects of the
proposed merger of Prince William
Hospital and Inova Health System in
northern Virginia using a bargaining
model of competition
•
If the Federal Trade Commission had permitted
it, the proposed merger would have increased
prices by about 3 percent, on average.
Glenn A. Melnick, Yu-Chu Shen, and
Vivian Yaling Wu, “The Increased
Concentration of Health Plan
Markets Can Benet Consumers
Through Lower Hospital Prices,”
Health Aairs, vol. 30, no. 9
(September 2011), pp.728–
1733, https://doi.org/10.1377/
hltha.2010.0406
2001 and 2004 Examined the association between
hospitals’ prices and market
concentration for health plans and
hospitals among all nonfederal,
general, acute care hospitals
located in metropolitan statistical
areas
•
A 1,000-point increase in the concentration of a
hospital market (as measured by the Herndahl-
Hirschman index) was associated with an
8.3percent increase in prices.
Deborah Haas-Wilson and Christopher
Garmon, “Hospital Mergers
and Competitive Eects: Two
Retrospective Analyses,” International
Journal of the Economics of Business,
vol. 18, no. 1 (February 2011), pp.17–
32, https://doi.org/10.1080/
13571516.2011.542952
Fiscal years
1999 and 2002
Examined price changes for
two hospital mergers in the
Chicago metropolitan area,
Evanston Northwestern–Highland
Park Hospital and Vista Health
(St.Therese–Victory Memorial
Hospital), relative to price changes
for control hospitals in that area
•
After the Evanston merger, price increases were
at least 10 percentage points larger at the
merged hospitals than at control hospitals for
four of the ve insurers included in the study.
•
After the Vista Health merger, three of the ve
insurers experienced smaller price increases at
the merged hospital than at the control hospitals.
Only one insurer experienced a larger price
increase at the merged hospital than at the
controls.
Steven Tenn, “The Price Eects of
Hospital Mergers: A Case Study of
the Sutter–Summit Transaction,”
International Journal of the
Economics of Business, vol. 18,
no. 1 (February 2011), pp. 65–82,
https://doi.org/10.1080/
13571516.2011.542956
1999 and 2001 Examined price changes for the
Sutter Alta Bates–Summit hospital
merger in California relative to
price changes for a set of control
hospitals in that state
•
After the merger, price increases at Summit
were 28 percent to 44 percent higher,
depending on the insurer, than the average price
increase at the control group, but prices at Alta
Bates did not change signicantly.
Aileen Thompson, “The Eect of
Hospital Mergers on Inpatient Prices:
A Case Study of the New Hanover–
Cape Fear Transaction,” International
Journal of the Economics of Business,
vol. 18, no. 1 (February 2011),
pp.91–101, https://doi.org/10.1080/
13571516.2011.542958
1997–1998 and
2001–2002
Examined price changes for the
New Hanover–Cape Fear hospital
merger in North Carolina relative to
price changes for a control group of
similar urban hospitals in that state
•
After the merger, prices increased for some
insurers and decreased for others. For two
insurers, prices increased by 56.5 percent and
65.3 percent, respectively, while for another
insurer, prices declined by 30 percent.
Asako S. Moriya, William B. Vogt,
and Martin Gaynor, “Hospital
Prices and Market Structure in the
Hospital and Insurance Industries,”
Health Economics, Policy, and
Law, vol. 5, no. 4 (October 2010),
pp.459–479, https://doi.org/10.1017/
S1744133110000083
2001–2003 Examined the association between
hospitals’ prices and changes in
market concentration for insurers
and hospitals across health service
areas
•
The relationship between increases in hospital
market concentration and prices was not
signicant.
Table C-1. Continued
Studies of the Relationship Between Hospital Market Concentration and Prices
42 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Table C-2 .
Studies of the Relationship Between Physician Market Concentration and Prices
Source Data Period Experiment or Methods Findings
Naomi Hausman and Kurt Lavetti,
“Physician Practice Organization
and Negotiated Prices: Evidence
From State Law Changes,” American
Economic Journal: Applied
Economics, vol. 13, no. 2 (April 2021),
pp.258–296, https://doi.org/10.1257/
app.20180078
1996–2007 Examined the relationship between
market concentration (as measured
by the Herndahl-Hirschman index,
or HHI) and prices, using changes in
judicial policies about noncompete
agreements as a source of
exogenous variation in the structure
of physician markets
•
A 100-point increase in the rm-based HHI
(which could mainly aect providers’ bargaining
power) increased prices by 1.7percent to
2.1percent.
•
A 100-point increase in the practice-location-
based HHI (which could mainly aect practices’
eciency) decreased prices by 1.4 percent to
1.9 percent.
•
A decrease of 10 percent in the enforceability
of noncompete agreements caused physicians’
prices to decline by 4.3 percent.
Thomas Koch and Shawn W. Ulrick,
“Price Eects of a Merger: Evidence
From a Physicians’ Market,” Economic
Inquiry, vol. 59, no. 2 (April 2021),
pp.790–802, https://doi.org/10.1111/
ecin.12954
2008–2013 Compared prices of services
provided by orthopedists before
and after a merger of six orthopedic
practices into one, relative to prices
in nearby areas
•
Prices increased by 10 percent to 20 percent,
relative to prices for the same services in nearby
areas, for two of the three payers in the study.
•
Prices did not increase for the third payer.
Caroline S. Carlin, Roger Feldman,
and Bryan Dowd, “The Impact
of Provider Consolidation on
Physician Prices,” Health Economics
(United Kingdom), vol. 26, no. 12
(December 2017), pp.789–1806,
https://doi.org/10.1002/hec.3502
2006–2011 Compared prices of physicians’
services before and after three
large, multispecialty clinics were
acquired by two hospital-owned
integrated delivery systems.
Compared prices at practices
controlled by the acquiring systems
with prices at practices controlled
by a competing system.
•
Four years after a merger, average prices had
increased by 32 percent to 47 percent at the
newly acquired systems and had increased by
14 percent to 20 percent at clinics that had
already been acquired.
•
Prices increased for physicians’ services
delivered in hospitals’ inpatient and outpatient
settings but did not increase for some services
provided in physicians’ oces.
Daniel R. Austin and Laurence C.
Baker, “Less Physician Practice
Competition Is Associated With Higher
Prices Paid for Common Procedures,”
Health Aairs, vol.34, no. 10
(October 2015), pp.1753–1760,
https://doi.org/10.1377/
hltha.2015.0412
2010 Examined the relationship between
prices for 15 common, high-priced
specialty services and market
concentration in the previous year
for specialists providing those
services
•
For 11 of the 15 services, prices were 8percent
to 26 percent higher in the counties with the
most market concentration than in the counties
with the least concentration.
•
For the other 4 services, prices were not
statistically related to market concentration.
Eric Sun and Laurence C. Baker,
“Concentration in Orthopedic Markets
Was Associated With a 7Percent
Increase in Physician Fees for
Total Knee Replacements,” Health
Aairs, vol. 34, no. 6 (June 2015),
pp.916–921, https://doi.org/10.1377/
hltha.2014.1325
2001–2010 Examined the relationship
between changes in physicians’
prices for knee replacements and
concentration in the market for
orthopedic surgery in 311 counties
throughout the United States
•
Prices for knee replacements were 7 percent
higher in the most concentrated markets than in
the least concentrated markets.
Samuel A. Kleiner, William D. White,
and Sean Lyons, “Market Power and
Provider Consolidation in Physician
Markets,” International Journal of
Health Economics and Management,
vol. 15, no. 1 (January 2015),
pp.99–126, https://doi.org/10.1007/
s10754-014-9160-y
2009 Used data on consumers’ demand
(willingness to pay) for cardiology
and ophthalmology services in
three metropolitan areas to model
the incremental value of including a
physician in a network. Compared
that incremental value with prices
and modeled hypothetical mergers.
•
Prices were positively correlated with higher
willingness to pay in the two most concentrated
markets.
•
A hypothetical merger between the two
largest practices in an area increased prices
by 5.7percent to 5.9 percent in the most
concentrated market.
•
In the other two markets, simulated mergers had
small or insignicant eects, increasing prices
by less than 1.5 percent.
Continued
43APPENDIX C THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Source Data Period Experiment or Methods Findings
Laurence C. Baker and others,
“Physician Practice Competition
and Prices Paid by Private Insurers
for Oce Visits,” JAMA, vol. 312,
no. 16 (October 2014), pp. 1653–
1662, https://doi.org/10.1001/
jama.2014.10921
2003 and 2010 Examined the relationship between
physicians’ prices for oce visits
in 2010 for 10 common specialties
and market concentration in the
previous year. Also examined the
relationship between changes
in concentration and changes in
prices between 2003 and 2010.
•
Prices were 8 percent to 16 percent higher in
the most concentrated markets than in the least
concentrated markets.
•
Prices increased more in places that had more
market concentration initially.
Abe Dunn and Adam Hale
Shapiro, “Do Physicians Possess
Market Power?” Journal of Law
and Economics, vol.57, no. 1
(February 2014), pp.159–193,
https://doi.org/10.1086/674407
2005–2008 Examined the relationship between
prices for cardiology and orthopedic
services and market concentration
in the previous year for specialists
providing those services. Also
examined the relationship between
changes in concentration and
changes in prices over time.
•
Prices were 14 percent to 30 percent higher in
the most concentrated markets than in the least
concentrated markets.
•
The eect of concentration on prices became
larger as markets became more concentrated.
Table C-2. Continued
Studies of the Relationship Between Physician Market Concentration and Prices
44 THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES JANUARY 2022
Table C-3 .
Studies of the Relationship Between Providers’ Vertical Integration and Prices
Source Data Period Experiment or Methods Findings
Haizhen Lin, Ian M. McCarthy, and
Michael Richards, “Hospital Pricing
Following Integration With Physician
Practices,” Journal of Health
Economics, vol. 77 (May 2021),
https://doi.org/10.1016/
j.jhealeco.2021.102444
2009–2015 Examined the relationship between
changes in prices for hospital
discharges and changes in whether
a hospital owned a physicians’
practice in the same hospital
referral region. Also examined the
relationship between price changes
and changes in the number of
physicians working in those
practices.
•
On average, hospitals’ prices increased by
about 3 percent after integration of a hospital
with a physicians’ practice.
•
Prices were about 4 percent higher at the
75thpercentile of the number of physicians
working in local practices owned by a given
hospital than at the 25th percentile.
Laurence C. Baker, M. Kate Bundorf,
and Daniel P. Kessler, “Does
Multispecialty Practice Enhance
Physician Market Power?” American
Journal of Health Economics, vol. 6,
no. 3 (Summer 2020), pp. 324–347,
https://doi.org/10.1086/708942
2008–2012 Examined the relationship over
time between changes in prices
for oce visits with general
practitioners or specialists
and prior-year changes in the
prevalence of integration between
those physicians
•
On average, prices were 2.7 percent higher for
general practitioner oce visits and 2.0 percent
higher for specialist oce visits in zip code areas
in the top one-quarter of generalist-specialist
physician integration than in areas in the bottom
one-quarter of such integration.
Richard M. Scheer, Daniel R.
Arnold, and Christopher M. Whaley,
“Consolidation Trends in California’s
Health Care System: Impacts on
ACA Premiums and Outpatient Visit
Prices,” Health Aairs, vol.37, no.9
(September 2018), pp.1409–1416,
https://doi.org/10.1377/hltha.2018.0472
2011–2016 Examined the association between
changes in prices for primary care
and specialist physicians’ oce
visits in California and prior-year
changes in the percentage of
primary care or specialist physicians
in practices owned by a hospital
•
On average, prices were 5.0 percent higher for
primary care oce visits and 9.1 percent higher
for specialty oce visits in counties where
all practices were owned by hospitals than in
counties that had the average level of vertical
integration (33 percent integrated for primary
care physicians and 35percent integrated for
specialty care physicians).
Cory Capps, David Dranove, and
Christopher Ody, “The Eect of
Hospital Acquisitions of Physician
Practices on Prices and Spending,”
Journal of Health Economics,
vol.59 (May 2018), pp. 139–152,
https://doi.org/10.1016/
j.jhealeco.2018.04.001
2007–2013 Compared changes in prices of
physicians’ services in several
states before and after physicians’
vertical integration with a hospital,
relative to price changes for
physicians’ services at practices
that never integrated
•
On average, prices for physicians’ services
increased by 14.1 percent after integration of a
physicians’ practice with a hospital.
Hannah T. Neprash and others,
“Association of Financial Integration
Between Physicians and Hospitals
With Commercial Health Care Prices,”
JAMA Internal Medicine, vol.75,
no.12 (December 2015), pp.1932–
1939, https://doi.org/10.1001/
jamainternmed.2015.4610
2008 and 2012 Examined the association between
changes in spending for and
use of inpatient and outpatient
hospitals’ and physicians’ services
in a metropolitan statistical
area (MSA) and changes in the
proportion of physicians in that area
billing exclusively with a hospital
outpatient department code
•
On average, spending increased by
3.1percent for outpatient services in MSAs
where the amount of integration increased by
about 5 percentage points (equivalent to the
75th percentile of changes that occurred in
MSAs). There was no statistically signicant
increase in the use of services, which suggests
that the spending increase was driven almost
entirely by price increases.
•
There was no statistically signicant change
in spending or utilization for inpatient services
associated with increases in vertical integration,
but those results were inconsistent when
alternative measures of physician-hospital
integration were used.
Continued
45APPENDIX C THE PRICES THAT COMMERCIAL HEALTH INSURERS AND MEDICARE PAY FOR HOSPITALS’ AND PHYSICIANS’ SERVICES
Source Data Period Experiment or Methods Findings
Laurence C. Baker, M. Kate Bundorf,
and Daniel P. Kessler, “Antitrust for
Accountable Care Organizations,”
Journal of Competition Law and
Economics, vol. 11, no. 2 (June 2015),
pp. 317–329, https://doi.org/10.1093/
joclec/nhv002
2001–2007 Examined the association between
changes in prices for outpatient
physicians’ services in 639 counties
and changes in the share of the
market served by hospitals in
one of four hospital-physician
integration categories
•
On average, prices increased by 1.7 percent
for outpatient physicians’ services in areas
where the type of organization with the most
vertical integration increased its market share
by 10percentage points and where there had
initially been low levels of integration.
Laurence C. Baker, M. Kate Bundorf,
and Daniel P. Kessler, “Vertical
Integration: Hospital Ownership of
Physician Practices Is Associated With
Higher Prices and Spending,” Health
Aairs, vol. 33, no. 5 (May 2014),
pp. 756–763, https://doi.org/10.1377/
hltha.2013.1279
2001–2007 Examined the association between
changes in prices for hospital
admissions in 639 counties and
changes in the share of the market
served by hospitals in one of four
hospital-physician integration
categories
•
On average, prices increased by 3.2 percent
for hospital admissions in areas where the type
of organization with the most vertical integration
increased its market share by one standard
deviation.
Table C-3. Continued
Studies of the Relationship Between Providers’ Vertical Integration and Prices
About This Document
is report was prepared at the request of the Chairman of the House Committee on the Budget. In
keeping with the Congressional Budget Oce’s mandate to provide objective, impartial analysis, the
report makes no recommendations.
Michael Cohen, Jared Maeda (formerly of CBO), and Daria Pelech wrote the report with guidance
from Lyle Nelson (formerly of CBO) and Chapin White. Yiqun Gloria Chen, Carrie H. Colla,
Noelia Duchovny, Caroline Hanson, Tamara Hayford, and Ian McCarthy of CBO oered comments.
Christian Henry and Joshua Varcie fact-checked the report.
Comments were also provided by Zack Cooper of the Yale University School of Public Health; Paul
Ginsburg of the Price School of Public Policy, University of Southern California; Aditi Sen and Zhera
Valencia of the Health Care Cost Institute; and Jerey Stensland and Ariel Winter of the Medicare
Payment Advisory Commission. e assistance of external reviewers implies no responsibility for the
nal product; that responsibility rests solely with CBO.
Jerey Kling and Robert Sunshine reviewed the report. Christian Howlett edited it, and Casey
Labrack created the graphics and prepared the report for publication. e report is available at
www.cbo.gov/publication/57422.
CBO seeks feedback to make its work as useful as possible. Please send comments to
Phillip L. Swagel
Director
January 2022
